Article Text

Abstract
Mesenchymal Stem cells (MSCs) are stromal cells that can be readily harvested from adult bone marrow and adipose tissue, but also umbilical cords. With respect to respiratory disease, the therapeutic potential of these cells lies in their paracrine effects which underlie their ability to enhance tissue regeneration and modulate immune responses. MSCs have been shown to be effective in a range of murine models of respiratory disease, and there are currently five clinical trials involving the administration of MSCs for respiratory diseases, including COPD and emphysema. This paper summarises the features of MSCs.
- Asthma
- cytokine biology
- neutrophil biology
Statistics from Altmetric.com
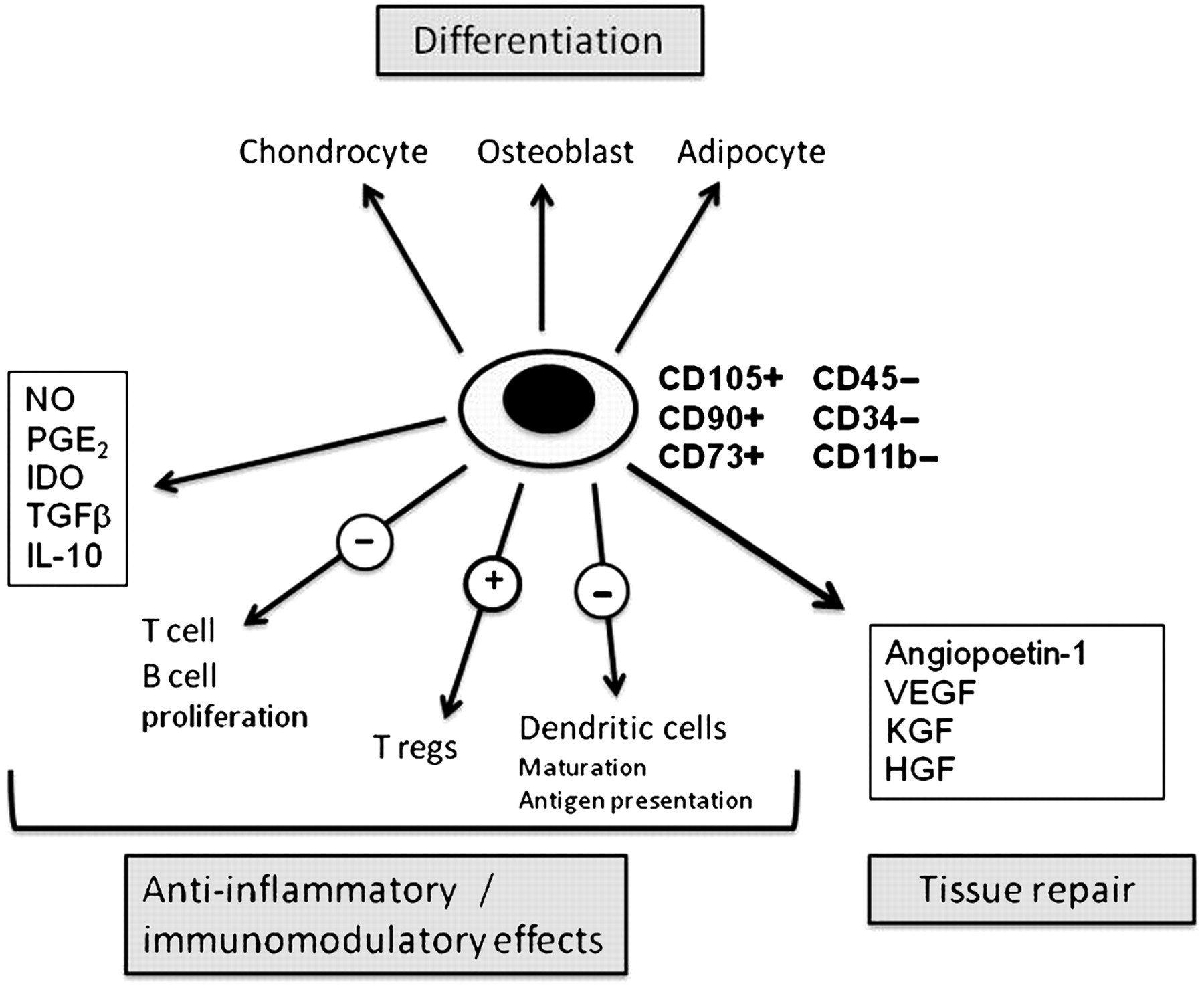
Mesenchymal stem cells (MSCs) are stromal cells that are found in many tissues but can be readily harvested from adult bone marrow and adipose tissue. There are no specific markers for MSCs, therefore they are identified by their expression of a range of markers and their functional characteristics. MSCs have been defined by the International Society for Stem Cell Research as plastic adherent cells that can be differentiated into adipocytes, chondrocytes and osteoblasts. For cells to be classified as MSCs they must express the mesenchymal markers CD105, CD90 and CD73, but importantly not express the haematopoietic markers CD45, CD34, CD14 and CD11b (figure 1).1 In addition to these markers, MSCs are generally reported to express CD13, CD29, CD44, CD166 and platelet-derived growth factor receptor α. It is important to note that fibrocytes, which are often referred to as MSCs, express the haematopoietic markers CD18, CD11b and CD45, and as such, by definition, are not MSCs.

{kind=link}
Mesenchymal stem cells. HGF, hepatocyte growth factor; IDO, indoleamine 2,3-dioxygenase; KGF, keratinocyte growth factor; IL-10, interleukin 10; NO, nitric oxide; PGE2, prostaglandin E2; TGFβ, transforming growth factor β; VEGF, vascular endothelial growth factor.
Therapeutic applications of MSCs were originally focused on their tri-lineage differentiation capacity and hence their possible applications for tissue repair and tissue engineering, for example, generating cartilage for the treatment of arthritis or bone for non-healing fractures. Notably in 2008 a successful trachea transplant was performed in a man with a tissue-engineered trachea, using a de-celluarised donor trachea as a scaffold, seeded with autologous bone-marrow-derived MSCs that had been expanded ex vivo and differentiated into cartilage.2
In addition to these more obvious applications it was discovered that MSCs exhibited potent anti-inflammatory and immunomodulatory activities both in vitro and in vivo. Mechanistically the evidence suggests that these effects are mediated predominantly through paracrine factors, MSCs secreting a range of immunomodulators, including transforming growth factor β, prostaglandin E2, interleukin 10, indoleamine 2,3-dioxygenase. MSC-mediated immunosuppression may also result from the recruitment of other immunoregulatory networks. In vitro MSCs have been shown to inhibit T-cell and B-cell proliferation, to support the development of T-regulatory cells, to downregulate the lytic activity of natural killer cells and cytotoxic T lymphocytes, inhibit the differentiation of monocytes into dendritic cells, and impair their antigen-presenting function. Currently it is not known which of these pathways is critical for the immunosuppressive actions of MSCs in vivo and it is likely that different mechanisms may operate dependent on the disease state.
Impressive immunosuppressive effects of these cells have been reported in a wide range of animal models of disease, including acute graft versus host disease (GvHD), collagen-induced arthritis, experimental autoimmune encephalomyelitis and autoimmune diabetes. With respect to respiratory disease there are now a number of publications that report a reduction in disease pathology when MSCs are administered in the context of bleomycin-induced fibrosis, bacterial infection and allergic airways disease.
Recent studies have also provided evidence that MSCs can promote tissue repair through their production of cytokines and growth factors, including vascular endothelial growth factor, angiopoietin 1, keratinocyte growth factor, and hepatocyte growth factor.
Human MSCs can be readily harvested from bone marrow or adipose tissue and culture expanded. Following intravenous injection, these cells have been shown to home to sites of inflammation or tissue damage. As MSCs appear to be largely non-immunogenic (due to their low constitutive expression of major histocompatibility complex I and II proteins, and the lack of T-cell costimulatory molecules) culture-expanded allogeneic MSCs may represent a practical, cost-effective stem cell therapy that does not have the ethical issues associated with embryonic stem cells.
MSCs are currently being evaluated in several clinical trials for a variety of diseases, including Crohn's disease, multiple sclerosis, diabetes mellitus and acute GvHD disease, with promising results already reported from some of these trials.3
While MSCs hold huge potential for the treatment of a range of lung diseases, currently there are many gaps in our scientific knowledge with respect to the biology of these cells. These relate to our understanding of exactly how they modulate inflammatory processes and promote tissue repair, and also with respect to practical issues such as determining the best source, expansion methodology, route and timing of administration of these cells. Effective translation into humans will, therefore, require rigorous scientific experimentation to elucidate mechanisms and establish optimal protocols.
Linked Articles
- Acute lung injury
- Editorial
- Respiratory infection
- Airwaves