Article Text

Statistics from Altmetric.com
Respiratory muscles
P1 MULTIDISCIPLINARY MOTOR NEURONE DISEASE CLINICS: DO THEY IMPROVE PATIENT CARE?
B.V. Prathibha, C. Wylie, N. Pease, F.J. Thomas. Nevill Hall Hospital, Brecon Road, Abergavenny, South Wales, UK
Motor neurone disease is a progressive neurological disorder which results in respiratory failure eventually. Currently the respiratory input into the management of these patients occurs at the terminal stages of their life. In addition, these patients need input from other specialties including palliative care and gastroenterology. We describe here a multidisciplinary approach with a new type of clinic set up so that the patients are seen by these specialists early on in the illness in the hope of improving the quality of care.
Aim: The aim was to set up a one stop clinic providing combined respiratory, neurological, and palliative care advice with input from voluntary organisations (MND association) and social workers and to assess any perceived benefits from the patients and carers point of view.
Design: The clinic is scheduled once a month and the three physicians (respiratory, neurology, and palliative care) sit in the same room with the other organisation representatives in the next room. The patients are offered an appointment in the specialist MND clinic following confirmation of the diagnosis by the neurologist. A special proforma has been designed to include the neurological, respiratory, gastroenterological, and social aspects of care. At each visit, the different variables including spirometry and blood gases are recorded. All patients undergo baseline overnight sleep study. The subject of NIPPV and intubation is introduced during these visits depending on the symptoms. The patients then make informed choices about their treatment. A patient feedback questionnaire has been designed and is given to each new patient.
Results: The clinic was established in November 2001 and to date 11 patients (7 males and four females) have been seen. The median age is 63 for men and 62 for women. The median FVC at presentation is 89 % predicted and median Po2 and Pco2 are 11.5 and 4.8 respectively. The decline in the FVC over 9 months is associated with increasing Pco2 and symptoms. Three have been opted for NIPPV for symptom palliation. All patients rated the clinic highly, preferred to come to a single clinic than to three different ones and felt that they had adequate time to discuss all their concerns and have them allayed.
Conclusion: MND patients need specialised input from many professionals and too often this is patchy and unsatisfactory. The organisation of a combined clinic of the type described above has improved patient care and communication between the different specialists and has resulted in the efficient use of time and other limited resources.
P2 OUTCOMES OF ASSISTED VENTILATION IN MOTOR NEURONE DISEASE
S. Sundaram, I.E. Smith, J.M. Shneerson. Respiratory Support And Sleep Centre, Papworth Hospital, Cambridge, UK
Assisted Ventilation may prolong survival in patients with respiratory failure in motor neurone disease (MND), but there are few published reports.
We performed a retrospective study of all patients referred to our tertiary care centre between 1993 and 2002.
We identified 109 patients; mean age 60 (SD 9.0) years, 74% of whom were male. Fifty-one per cent had bulbar symptoms. Sixteen patients were transferred from intensive care units elsewhere with tracheostomy ventilation (TV). Fifty-five patients were offered non-invasive ventilation (NIV), of whom 43 accepted and 12 declined treatment. Thirty seven patients were assessed at our unit and were thought not to require any assisted ventilation. One patient required only a tracheostomy with no assisted ventilation. Nine of the TV patients were weaned to NIV. Patients who still required TV at the time of discharge managed to self ventilate by day, but within three months were once again continuously dependent on it. Among patients offered NIV de novo, 36 had hypercapnia (mean Paco2 8.0 kPa) and 19 had orthopnoea causing sleep disturbance. The arterial blood gases while self ventilating on air improved in patients treated with NIV. At first follow up, the mean fall in Paco2 (95% CI) was 2.3 kPa (1.2 to 3.4; p<0.001) and the mean rise in Pao2 was 1.1 kPa (0.30 to 2.0; p<0.01). Bulbar weakness was as frequent in patients given NIV as those that declined (p=0.66).
There have been 86 deaths. Using the Kaplan-Meier method, the median survival was four months in patients who declined treatment and 11 months in those thought not to need NIV. There was no difference in survival between patients transferred intubated from ICU (12 months) and other subjects who started assisted ventilation (14 months; p=0.89).
Many MND patients treated with tracheostomy ventilation can be weaned to NIV. In our cohort bulbar weakness did not preclude NIV. Survival was best for patients using assisted ventilation and worst for those who declined treatment.
P3 OUTCOME OF NON-INVASIVE DOMICILIARY VENTILATION FOR PREVIOUS POLIOMYELITIS: IMPACT OF SCOLIOSIS
Y. Tai, D. McKeon, I.E. Smith, J.M. Shneerson. Respiratory Support and Sleep Centre, Papworth Hospital, Cambridge, UK
Survivors of poliomyelitis can develop new respiratory disability many years after the acute illness. Scoliosis, muscle weakness, and decreased respiratory drive may all contribute. We examined the effect of scoliosis on survival in 51 patients (20 women) with previous poliomyelitis established on home mechanical ventilation (HMV) in our centre.
Poliomyelitis was contracted at a median age of 6.5 years; 82% of the patients had a thoracic scoliosis. The mean interval from contracting poliomyelitis to HMV was 46 (SD 8.8) years. Arterial blood gases on room air prior to HMV showed Pao2 7.2 kPa and Paco2 8.6 kPa, which significantly improved (p<0.05) after one month of treatment to Pao2 9.5 kPa and Paco2 6.6 kPa. The improvement was maintained at a mean follow up of 58 months. The Kaplan-Meir plot for life expectancy from initiation of ventilation is shown in the figure: survival was 7.35 years for subjects without scoliosis (solid line) v 12.1 years for subjects with scoliosis (dashed line) (p=0.048).

Kaplan-Meir plot for life expectancy from initiation of ventilation.
Comparing subjects with and without scoliosis there were no differences in blood gases or overnight monitoring at presentation or during follow up on HMV; those with scoliosis had a smaller vital capacity 1.18 L v 1.49 L (p=0.013) and were younger when they had contracted poliomyelitis (median age 5 v 20 years; p=0.003); the time interval from poliomyelitis to HMV was similar for the two groups and so those with scoliosis started ventilation at an earlier age. Recalculating life expectancy from birth there was no difference between the two groups (p=0.989).
This study confirms that HMV can normalise arterial blood gas tensions in patients with previous poliomyelitis and the improvement is maintained. Overall survival is good. Compared to subjects with a scoliosis survival from the initiation of HMV is worse for subjects without a scoliosis largely because they are older when they develop ventilatory failure.
P4 COMPARISON OF PRESSURE AND VOLUME TARGETED NON-INVASIVE VENTILATION IN CHEST WALL DEFORMITY
J.M. Tuggey, M.W. Elliott. St James’s University Hospital, Leeds, UK
Introduction: The use of domiciliary non-invasive ventilation (NIV) in chest wall deformity is established and of proven benefit in terms of arterial blood gas tensions, sleep quality and daytime function. Previous studies have compared in the short term, volume, and pressure targeted ventilation. As part of a larger study, we investigated the effect of ventilation mode on minute ventilation and mask leak.
Method: 10 patients (mean age 64; mean FVC 0.55 l) with chest wall deformity, established on home NIV completed a randomised crossover study comparing pressure support and volume ventilation using the Breas PV403 ventilator. Ventilator parameters were set following a daytime titration period according to patient comfort and so that MVe was identical for both PSV and VCV. Patients used the machine at home for four weeks for each modality. At the end of each period, patients were admitted for a sleep study, including measurement of ventilation using a pneumotachometer connected to the ventilator circuit, adjacent to the nasal mask. Delivered tidal volume (Vti), expired tidal volume (Vte), expired minute volume (MVe) and respiratory rate (fR) were measured throughout the night. Minute leak was calculated by (Vti−Vte) × fR.
Results: See figure.

Ventilation was slightly greater in the volume group. There was significantly more leak during PSV than compared to VCV (16 v 6 l/min).
Conclusion: Volume cycled ventilation results in less leak without compromising ventilation compared to PSV. Excessive amounts of leak during PSV may result in greater arousals and sleep fragmentation.
JT is funded by the NHS Northern & Yorkshire Executive
P5 COMPARISON OF PRESSURE AND VOLUME CYCLED VENTILATION IN KYPHOSCOLIOSIS (A RANDOMISED, SINGLE BLIND, CROSSOVER, PILOT STUDY)
S.E. Higgins, R. Russell, B.E.A. Lams, A.J. Williams, A.C. Davidson. Lane-Fox Respiratory Unit, St Thomas’ Hospital, London, UK
Introduction: This study compared pressure controlled (PCV) and volume controlled ventilation (VCV) in patients with kyphoscoliosis (KS). Two previous studies have been published with conflicting results. One suggests that some more severe patients were inadequately treated with PCV (
). The second study found no differences between the modes but suggested that patient fatigue was reduced using PCV (
).
Patients & methods: Twelve patients (three female, nine male) with KS and longstanding chronic respiratory failure (CRF) (Paco2 at enrolment was 5.96 + 0.73 kPa) were recruited into the study, (mean age 59 (8.9) years). All patients were receiving domiciliary nocturnal pressure ventilation. We measured the following at base line; ABGs, overnight Pulse Oximetry and transcutaneous CO2, FVC, FEV1, SNIP, Psychomotor Vigilance (PVT), OSLER Sleep latency, Epworth Sleepiness Scale, and Actigraphy & Sleep Diary for 10 days. Each patient was then randomised to one month of PCV or VCV using the BREAS PV403 ventilator. The subjects were blinded to the mode of ventilation. At the end of one month all of the above parameters were remeasured, the mode changed and the parameters remeasured after a further month. At the end of the study the subjects were asked to express a preference for month one or month two.
Results: Five subjects were excluded (three due to underlying OSA, one due to an unrelated illness, and one was unable to tolerate VCV). In the remaining seven no significant differences were found between PCV and VCV in most of the physiological variables. The hours of ventilator use was greater during PCV compared with VCV (8:22 v 7:49), but this did not reach statistical significance (p=0.07). Actigraphy revealed a significantly lower sleep fragmentation index in the PCV limb of the study (32.6 v 38.5; p=0.04). This was supported by the subjects reported sleep quality during PCV (2.17 v 2.45; p=0.01). In addition, subjects preferred PCV to VCV (p<0.0002).
Conclusions: Patients with KS and CRF are adequately ventilated with both PCV and VCV modes. However patients prefer PCV, and subjective and objective sleep quality is improved with PCV.
P6 COMPARISON OF PRESSURE V VOLUME CYCLED VENTILATION IN KYPHOSCOLIOSIS A RANDOMISED SINGLE BLIND CROSSOVER STUDY: QUALITY OF LIFE OUTCOME DATA
R.E.K. Russell, S.E. Higgins, B. Lams, A.J. Williams, A.C. Davidson. Lane Fox Respiratory Unit, St Thomas’ Hospital, London, UK
Introduction: Patients with kyphoscoliosis (KS) may require long term ventilatory support as disease progression occurs. The ventilator used may be either volume (VC) or pressure controlled (PC). It is unclear which strategy is most beneficial for patients with KS.
Patients and methods: 12 subjects with KS (nine males, mean age 59 (8)) who were receiving long term ventilatory support were enrolled in a single blind randomised crossover pilot study. Ventilators were provided by the manufacturer (Breas PV403) and were set to provide the same minute volume in either volume or pressure control mode. Subjects completed the St George’s Respiratory Questionnaire (SGRQ), the SF-36 health questionnaire, and the Beck depression score pre treatment and after four weeks on the trial ventilator at each setting.
Results: One subject was excluded due to intercurrent illness, three due to obstructive sleep apnoea, and one subject could not tolerate VC. Pulmonary function and QoL data are shown in table 1. There were no significant differences between pre treatment values and those obtained after four weeks on the two ventilator settings. However these subjects scored on all values much greater than healthy normals, indicating significant impairment of QoL. Beck depression scores were within the normal range.
Beck, SGRQ and SF-36 following PC or VC ventilation for four weeks.
Conclusions: Patients with KS on long term ventilation have significantly impaired QoL and the ventilator strategy used (VC or PC) does not affect this.
P7 ADDUCTOR POLLICIS AND QUADRICEPS STRENGTH IN COPD
M.G.G. Soliman1, W.D-C. Man1, D. Nikoletou1, M.L. Harris1, G.F. Rafferty1, N. Mustfa1, M.I. Polkey2, A.J. Williams3, J. Moxham1. 1Respiratory Muscle Laboratories, King’s College Hospital, UK; 2Royal Brompton Hospital, UK; 3St Thomas’ Hospital, London, UK
Background: Peripheral muscle weakness is common in COPD, but the cause remains controversial. Better understanding of the distribution of muscle weakness may reveal the underlying pathological process; chronic inactivity and disuse atrophy should lead to preferential involvement of the muscles with the greatest decrease in utilisation—that is, the lower limbs—whereas the loss of muscle function should be equally distributed if the underlying pathology is a more generalised process such as inflammation or malnutrition. To address this question, we used the non-volitional technique of supramaximal magnetic nerve stimulation to assess the strength of the adductor pollicis and quadriceps muscles.
Methods: 14 patients with stable COPD (not on oral corticosteroids) and 14 age matched healthy controls were recruited. Twitch adductor pollicis tension (TwAP) and twitch quadriceps tension (TwQ) were determined following supramaximal magnetic stimulation of the ulnar and femoral nerves respectively.
Results: Patients and controls were well matched for age, weight, height, and BMI. Mean FEV1 and FEV1predicted for the COPD patients were 0.86l and 37% respectively. TwAP was similar in the COPD and healthy elderly groups (7.04 v 7.30N; p=0.69). However TwQ was significantly lower in the COPD group (68.2 v 104N; p=<0.001).
Discussion: In non-weight losing, stable COPD patients, quadriceps strength is significantly reduced compared with age matched healthy controls, whereas the strength of the adductor pollicis is normal. This is indirect evidence that there is not a generalised weakness in stable COPD, and that disuse atrophy is an important contributor towards peripheral muscle weakness.
WDCM is a Clinical Research Training Fellow of the MRC (UK).
P8 THE RELATIONSHIP BETWEEN RESPIRATORY MUSCLE STRENGTH AND NEED FOR VENTILATORY SUPPORT IN POST-POLIO PATIENTS
M.G.G. Soliman, S.E. Higgins, D.R. El-Kabir, B. Pereira, W.D-C. Man, A.C. Davidson, R.S. Howard, A.J. Williams. The Lane-Fox Respiratory Unit, St Thomas’ Hospital, London, UK
Respiratory failure requiring nocturnal ventilatory support is a recognised late complication of previous poliomyelitis and is probably secondary to respiratory muscle weakness. Respiratory muscle strength was measured in 50 post-polio patients to assess the relationship between the need for ventilatory support and the degree of respiratory muscle weakness. Tests included forced vital capacity (FVC), maximum inspiratory (MIP) and expiratory pressures (MEP), and sniff nasal pressure (SNIP).
During the time of testing, 21 patients were using nocturnal ventilatory support (VS) compared with 29 on no support (NS). No significant differences in age, BMI, or time since acute episode, were found between the two groups. Respiratory muscle strength (mean (SD)) are presented in the table.
Of the patients requiring no support, those who had been ventilated during the acute episode had a significantly lower SNIP than those who had never been ventilated (48.8 (17.6) v 65.8 (27.4); p=0.04).
Post-polio patients requiring nocturnal ventilatory support have a greater degree of inspiratory muscle weakness. SNIP is the most sensitive non-invasive test of inspiratory muscle weakness, and may prove to be a potentially useful tool in monitoring the progression of respiratory muscle weakness and subsequent ventilatory failure in post-polio patients.
P9 COPD ALTERS THE DIAPHRAGM MOTOR AREA RESPONSE TO TRANSCRANIAL MAGNETIC STIMULATION
N.S. Hopkinson, T. Sharshar, E. Ross, M.J. Dayer, A.H. Nickol, J. Moxham2, M.I. Polkey. Muscle Lab, Royal Brompton Hospital; 2King’s College Hospital, London, UK
Background and methods: The threshold and stimulus response curve to transcranial magnetic stimulation (TMS) of the diaphragm motor area can provide information about cortical excitability in health and disease. We studied five patients with severe COPD (mean FEV1 20.2%predicted) and eight healthy controls. Stimulation series were delivered over the vertex using a 110mm double cone coil (Magstim 200 mono-pulse) at a variety of intensities in random order and the surface diaphragm motor evoked potential (MEP) recorded. Series were performed at resting end expiration and then, facilitated, during inspiratory manoeuvres at 20% and 40% of maximum inspiratory pressure (MIP) and then again at rest. Healthy subjects also performed a run at 60% MIP. The stimulus response curves for COPD patients are shown in the figure. This group showed a significant increase from rest to 20% facilitation but no further increase at 40%. By contrast controls showed a stepwise increase in MEP to 40% with no further increase at 60%.
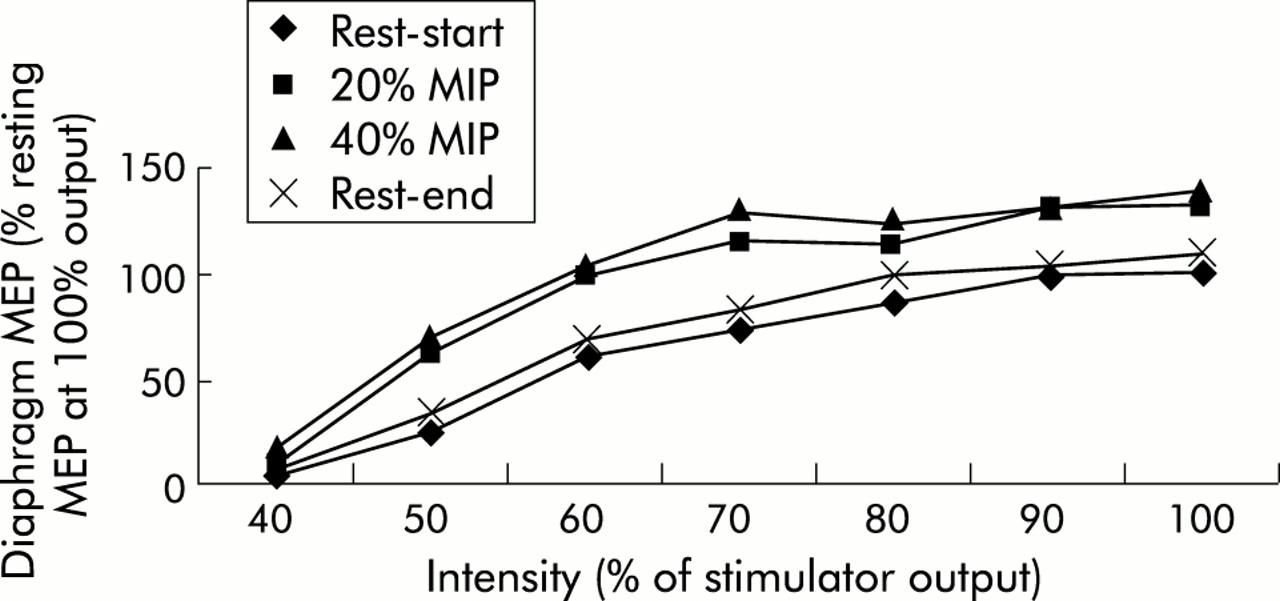
The stimulus response curves for COPD patients are shown.
Conclusion: COPD patients have a reduced cortical reserve perhaps because they are already facilitated at rest by an increased work of breathing.
This study was funded by the Wellcome Trust.
P10 THE EFFECT OF LONG TERM DOMICILIARY NON-INVASIVE POSITIVE PRESSURE VENTILATION (NIPPV) ON RESPIRATORY MUSCLE FUNCTION IN CHRONIC TYPE 2 RESPIRATORY FAILURE
A.D. Gething, E.M. Williams, A. Phillips, B.V. Prathibha.2School of Applied Science, University of Glamorgan; 2Respiratory Department, Nevill Hall Hospital, Abergavenny
In subjects with acute and chronic type 2 respiratory failure (due to kyphoscoliosis, sleep hypoventilation, and chronic obstructive pulmonary disease) application of nasal intermittent positive pressure ventilation (NIPPV) helps to restore arterial blood gases to normal levels, and aid breathing by unloading inspiratory muscles.(1) The effect of NIPPV on inspiratory muscle strength (IMs) and endurance (IMe) was tested.(2)
Methods: Two patient groups were studied, group one (n=6, age 63 (7) years; mean (SD)) who had just started with NIPPV and group two (n=6, 66 (14) years) who had undergone domiciliary ventilation (dNIPPV) for longer than six months. Group one patients were tested twice, once soon after the initiation of NIPPV and again after three months of dNIPPV. Inspiratory muscle strength and endurance were tested by asking the patient to perform three maximal inspiratory manoeuvres (a measure of IMs) followed by repeated submaximal (80%) manoeuvres with ever decreasing intermittent rest periods until task failure (a measure of IMe).(2) All patients were naïve to the IMe testing procedure.
Results: Group one patients (dNIPPV <1 month) had significantly (p<0.05) lower Pao2 than group two (dNIPPV >6 month) of 6.7 (2.5) v 8.6 (1.9) kPa respectively. The Paco2 was not significantly different at 7.5 (1.3) v 6.4 (0.9) kPa respectively. The maximal inspiratory pressure (MIP) a measure of IMs was highest in group two (Group1 32 (4) v Group 2 47 (9) cmH2O) as was sustainable MIP, a measure of IMe (Group1 102 (50) v Group2 158 (50) time/pressure units). In group 1, three months of dNIPPV improved MIP from 32 (4) to 48 (14) cmH2O but had no effect on sustainable MIP.
Conclusions: These data show that using dNIPPV for three months and longer improves inspiratory muscle strength. Improving inspiratory muscle endurance takes longer to achieve and can only be seen in the patients receiving dNIPPV for over six months (Group two). There are no long term benefits of using dNIPPV in terms of increasing inspiratory muscle strength but there are for endurance. How these improvements in endurance relate to general health status have yet to be evaluated.
1. Vitacca M, et al.
2. Gething, et al.
COPD exacerbations: ITU to discharge
P11 DEVELOPMENT OF A RESPIRATORY HIGH DEPENDENCY UNIT: EXPERIENCE FROM THE FIRST 20 MONTHS
D.M.G. Halpin, A. Jackson, C.D. Sheldon, N.J. Withers, S. Dodds. Royal Devon & Exeter Hospital, Exeter, Devon, UK
Non-invasive ventilation (NIV) has been used at the Royal Devon & Exeter Hospital since the early 1990s. Patients receiving NIV were treated on the specialist respiratory ward and as awareness of the benefits spread, NIV became the treatment of choice for patients admitted in hypercapnic respiratory failure secondary to COPD. The number of patients requiring NIV grew steadily and a business case was prepared for an appropriately staffed and equipped respiratory high dependency unit (rHDU). Eventually funding was secured from money allocated to critical care services and the unit opened in November 2000. Here we present an analysis of our experience over the first 20 months.
The unit has four beds and is staffed with a nurse:patient ratio of 1:2. It is located in one bay of the respiratory ward. Two hundred and twenty three patients have been admitted, with 33 admitted more than once. The mean age was 64.5 yrs (range 18 to 91) and 51% of patients were male. Most admissions (71%) occurred between 8am and 8pm and were mainly transfers of patients admitted acutely to the Emergency Medical Unit. Fifty one admissions (20%) were patients transferred out of the ITU and 38 had tracheostomies. The median length of stay was 4.04 days (range 1 to 37).
One hundred and nine patients received NIV, with 19 ventilated more than once. The mean age was 69.3 yrs (range 18 to 91) and 50% were male. The median duration of NIV therapy was 25.0 hours (range 0.5 to 505). There were 29 deaths in patients treated with NIV. In most of these it had been agreed in advance that more invasive treatment would not be undertaken. Ten patients were transferred to ITU because of failure to respond to NIV.
Twenty six patients received CPAP therapy, with one being treated more than once. The mean age was 70.2 yrs (range 32 to 88) and 64% were male. The median duration of CPAP therapy was 9.5 hours (range 0.5 to 134). There were five deaths and four patients were transferred to ITU because of failure to respond to CPAP.
The opening of the rHDU has allowed significant numbers of patients with respiratory failure to be managed effectively. Many of these patients would previously have been admitted to ITU. Appropriate staffing of the unit has allowed admissions to be accepted throughout the day and night and nearly one in three admissions occurred outside the normal working day. The rHDU has significantly enhanced the service we are able to offer patients.
P12 VARIATION IN CONSULTANT’S PROGNOSTIC ESTIMATES FOR IDENTICAL PATIENTS MAY EXPLAIN VARIATION IN COPD INTENSIVE CARE UNIT (ICU) ADMISSION: SIMULATION STUDY FROM ONE CRITICAL CARE NETWORK
M.J. Wildman2, J. O’Dea, S. Walia, M. Tindall, O. Kostopoulou, Z. Khan. Critical Care Units City Hospital and University Hospital Birmingham; 2London School Of Hygiene & Tropical Medicine, London, UK
Introduction: Anecdotal evidence suggests variation in gatekeeping decisions for COPD patients with respiratory failure considered for ICU.(1) However little is known about the approach of different doctors to the management of identical patients and the causes for the suggested variability. This study exploits the fact that consultants on call will occasionally make ICU admitting decisions on the basis of information conveyed over the phone. Simulation of such phone calls allows many clinicians to make decisions about identical patients in a way that mimics real life.
Methods: One hundred and twenty consultants caring for acute admissions in the Heart of England Critical Care Network were invited to take part. An investigator in the role of a registrar who had just assessed a COPD patient requiring ICU admission phoned consultants who were told that the patient was likely to arrest soon if not intubated. All relevant clinical information about the patient was available from the investigator. Clinicians were asked whether they would admit the patient to ICU and asked to predict ICU, hospital, and 180 day survival following admission. The probability of survival for the patients was subsequently calculated using the SUPPORT model.(2) Doctors considered three patients all of whom had single organ failure, but who varied in characteristics shown in multivariate analysis to be predictive of outcome.(2)
Results: Out of 120 clinicians, 98 (82%) took part. Patient one: 88.8% of doctors admitted patient one, with admitters giving a mean predicted hospital survival of 46.1% and non-admitters a significantly lower mean predicted hospital survival of 12.7% (p<0.00005). Patient one’s SUPPORT probability of 30 day survival was 89%. Patient two: 64.3% of clinicians admitted patient two, with admitters giving a mean predicted hospital survival of 37.9% v 11.8% for non-admitters (p<0.00005). Patient two’s SUPPORT probability of 30 day survival was 94%. Patient three: 39.8% admitted patient three, with admitters giving a mean predicted hospital survival of 28.2% v 13.0% for non-admitters (p<0.00005). Patient three’s SUPPORT probability of 30 day survival was 68%.
Conclusion: Predicted hospital survival for identical patients following ICU admission differed significantly between clinicians who would admit compared to those who would not. This study suggests that an important source of variability in ICU admission may arise from marked variation in predictions of survival and that objective models of patient outcome might reduce variability and support equity.
1. Wildman M.
2. Conners AF Jr, et al.
.
P13 CLINICAL DECISION MAKING: VENTILATING PATIENTS WITH EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
F.M.R. Perrin1, C.W.G. Turton1, M. Renshaw2. 1Respiratory Department, 2Clinical Effectiveness Unit, Brighton and Sussex University Hospital, Eastern Road, Brighton, UK
Introduction: The decision to institute mechanical ventilation in a patient presenting in acute respiratory failure secondary to an exacerbation of COPD can be difficult and controversial. This study aimed to determine whether there is a real difference in the views held between respiratory physicians, general physicians, and intensivists, whether there are significant differences in practice between individual clinicians and which clinical factors most influence decision making.
Method: A questionnaire was circulated by post to 600 consultants (200 in each specialty) selected randomly and at meetings to 125 SpRs. It included 25 different demographic, chest and comorbid variables that were each scored 0 to 3 according to the perceived relevance of the variable in the decision to embark on a trial of ventilation (where 0 was irrelevant and three contraindicated ventilation). The total score for all the variables was calculated for each clinician (0 to 75).
Results: 356 questionnaires were returned; 321 were completed fully and analysed (120 respiratory, 109 general medicine, 92 intensive care). The total scores for the clinicians in each specialty were: respiratory: mean 37.5, 95% CI 358 to 39.3, range 15 to 68; general medicine: mean 39.5, 95% CI 37.7 to 41.4, range 12 to 65; intensive care: mean 38.8, 95% CI 36.9 to 40.8, range 16 to 64. The importance placed on the different variables were ordered similarly across specialties. The most influential factors in deciding not to ventilate a patient were documented permanent cognitive dysfunction needing constant supervision, nursing home resident failing all activities of daily living, lung cancer deemed inoperable due to COPD, previous CVA such that patient chair bound or aphasic, and previous difficulty weaning from ventilation. The factors regarded as being least important were documented depression requiring treatment, osteoporosis with vertebral body collapse, continued smoking >20 cigarettes/day, plasma albumin <30g/l, and an above knee amputation for peripheral vascular disease.
Conclusions: There were no significant differences in clinical decision making between the specialties but there was wide variation between individual clinicians. Few of the factors investigated would contraindicate ventilation alone.
P14 CARDIOVASCULAR COMORBIDITY IS ASSOCIATED WITH HIGHER MORTALITY IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) PATIENTS ADMITTED TO AN INTENSIVE CARE UNIT
K.S. Srinivasan, A. Spiliopopolous, M.K. Sridhar. Staffordshire General Hospital, Stafford, UK
Background: 30–50% of patients admitted to an Intensive Care Unit (ICU) with respiratory failure due to COPD die in hospital.(1) (2) Studies have highlighted the difficulty of predicting mortality in this patient group from standard clinical and other scoring systems.(3) We present results of a retrospective analysis of data examining mortality in an unselected group of COPD patients admitted to the ICU in a district general hospital in England.
Patients and methods: Fifty nine patients (31 male, 28 female; mean age 66.2 years (50 to 86)) with COPD, who had been admitted with respiratory failure to the ICU at Stafford General Hospital in the last five years were studied. Of these patients, 17 (8 male, 9 female; mean age 72 years (52 to 86)) died while on ICU and 12 (5 male, 7 female) died within a year of their discharge. Age, smoking history (past or present), usage of oxygen or nebulisers at home, and associated cardiovascular diseases (ischaemic heart disease, heart failure, or hypertension), were studied as predictors of mortality. We do not know the severity of COPD before admission (FEV1) in these patients. Patients with associated cardiovascular conditions were found to have the highest mortality. Of the 59 patients, 24 had heart disease (40%) and the death rate in this group was 54% (13 of 24). Of these nine died during their stay in ICU.
Conclusion: COPD patients with cardiovascular comorbidity suffer a higher mortality following admission to ICU with respiratory failure. This information may have a bearing on prognostication and decision making in COPD patients being considered for invasive ventilation and admissions to ICU.
1. Hill AT, et al.
.
2. Sonell MG, et al.
.
3. Kaelin RM, et al.
.
P15 REFERRAL AND OUTCOME OF PATIENTS WITH AN EXACERBATION OF COPD REQUIRING ADMISSION TO INTENSIVE CARE
A. MacDuff1, I.S. Grant2, S. MacKenzie2, P.T. Reid1. 1Depts of Respiratory Medicine, and 2Intensive Care, Lothian University Health Trust, Edinburgh
Exacerbations of COPD complicated by acidotic respiratory failure which fail to respond to medical management, including non-invasive ventilation (NIV), are associated with a high mortality rate. When a reversible aetiological factor is not present the decision to refer to ICU is difficult with reservations on outcome and pressure on ICU resources (
). To examine our own practice, we performed a retrospective audit of admissions to the Intensive Care Units in our Trust. We identified 56 consecutive patients between April 1999 to April 2001 in whom a primary diagnosis of COPD was recorded. Of these, 37 were excluded as having a reversible cause of respiratory failure or an alternative diagnosis.
The median age was 64.5 years (range 49 to 78). Nine patients were previously unknown to respiratory physicians. It was the first admission with respiratory failure requiring ventilatory support in five of the nine previously admitted patients. Previous lung function was only available on five patients: median FEV1 0.7l (range 0.35 to 1.7). Prior to ICU referral median [H+]= 65.25mmol/l (IQR 61.33–77.7), Paco2=12.82kPa (IQR 8.93–15.6) and Pao2=8.2kPa (IQR 6.2–9.0). The median duration of assessment prior to ICU admission was 5.5 hours (IQR 2–10.1). Seventeen patients required invasive ventilation, one non-invasive ventilatory support. Two patients died in ICU (one of respiratory failure, one of refractory hypotension). The median duration of ICU stay for study patients was three days (IQR 2–6.23) compared to 2.7 days for all ICU patients at the Royal Infirmary and Western General. Sixteen were successfully discharged to respiratory unit. One patient died in respiratory failure but 15 patients were discharged and 14 were alive at one year. The median hospital stay was 13 days (IQR 9–19.3) (mean stay acute exacerbations of COPD in Lothian Trust=8.3 days).
Our data suggest that severe respiratory failure may be the first presentation of COPD to hospital. Limited time and information may be available to make an informed decision on referral to ITU, but length of stay and outcome are comparable to other ICU admissions.
P16 AN AUDIT OF THE USE OF NON INVASIVE VENTILATION IN ACUTE EXACERBATIONS OF COPD
C.J. Jolley, R. Savine, S. Ellum, O. Gilleard, B.E.A. Lams, A.C. Davidson. Lane-Fox Respiratory Unit, St. Thomas’ Hospital, London, UK
Introduction: The benefits of non-invasive ventilation (NIV) in the treatment of acute type 2 respiratory failure secondary to chronic obstructive pulmonary disease (COPD) are well documented (
).
Guidelines for the use of NIV have been published by the British Thoracic Society (BTS) (
). We investigated whether all patients with an acute exacerbation of COPD who fulfil the BTS’s criteria for NIV are being referred for this treatment.
Methods: We identified 203 patients who were admitted to St Thomas’s Hospital, London, with an acute exacerbation of COPD between 1/11/2001 and 10/7/2002 by searching the Accident & Emergency (A&E) register, High Dependency Unit (HDU), and Patient At Risk Team databases. The results of arterial blood gas (ABG) analysis on presentation to A&E were obtained from the patients’ A&E notes. We noted whether the patient was admitted to a general ward, received NIV on the HDU, or was intubated in A&E.
Results: Fifty four patients were excluded because their admission ABGs were not available from their A&E notes, leaving 147 patients’ data for analysis. Of 147 patients, 110 were admitted to a general ward, 33/147 received NIV on the High Dependency Unit, and 4/147 patients were intubated in A&E. The mean (SD) pH of patients admitted to a general ward was 7.38 (0.06). The mean (SD) pH on admission of patients referred for NIV was 7.27 (0.09). Of 147 patients admitted via A&E, 18 did not receive NIV despite meeting the BTS criteria on the basis of their arterial blood gas analysis on initial presentation. Their mean (SD) pH was 7.28 (0.05).
Conclusion: A significant proportion of patients with acute type 2 respiratory failure secondary to COPD who meet the criteria for NIV do not receive it. Strategies are required to improve the pick up rate of patients who would benefit from NIV at the time of their presentation to A&E.
P17 NON-INVASIVE VENTILATION IN PATIENTS WITH RESPIRATORY FAILURE: EXPERIENCE FROM A DEVELOPING COUNTRY
F. Hussain, J. Iqbal, R. Haqqee. Aga Khan University Hospital, Karachi, Pakistan
Objective: Non-invasive ventilation (NIV) has been found to be effective in the management of respiratory failure. In developing countries there is severe shortage of ICU beds and NIV service is still in early stages of development. Studies are needed, from developing countries, to determine its effectiveness among patients with different types of respiratory failure. In this study we have evaluated Asian patients with both types of respiratory failure as well as patients with respiratory distress and impending respiratory failure.
Method: The study was conducted at Aga Khan University Hospital Karachi, Pakistan. All patients who were treated with NIV during 1999–2000 were evaluated. Demographic details, history, and physical examination of patients were recorded. Laboratory data included serial arterial blood gas (ABG) analysis, chest radiograph, blood count, and electrolytes. Details of medical treatment, of NIV and their outcome were recorded.
Results: A total of 68 patients (35 males) were evaluated. Their Mean (SD) age was 60 (16.75) (range 16 to 90) yrs. The commonest indication for the use of NIV was Type II respiratory failure due to COPD exacerbation. There was significant improvement of mean Paco2 within two hours of treatment (76 v 70 mm Hg, p = 0.001) and of mean pH at 24 hours (7.30 v 7.36, p<0.001). Out of 37 patients, 25 (68%) improved with NIV alone, five (14%) needed invasive ventilation, and seven (19%) were considered unsuitable for invasive ventilation despite deterioration. Mortality was 30% (11 patients). NIV was applied to 17 patients with Type I respiratory failure; pneumonia, asthma, and pulmonary oedema were the common underlying diseases. The mean Pao2 improved within two hours of treatment (53 v 87 mm Hg, p = 0.003). Ten (59%) patients were successfully treated with NIV alone, six (35%) needed subsequent invasive ventilation, and one (6%) was considered inappropriate for invasive ventilation despite deterioration. Six patients died (mortality 35%). Neuromuscular diseases and pulmonary oedema were the common causes among 14 patients with respiratory distress (respiratory rate >30 along with use of accessory muscles and laboured breathing). NIV was successful in 9 (64%) patients, 3 (22%) needed invasive ventilation, and two (14%) died. At the time of admission 16 (24%) patients were considered inappropriate for invasive ventilation, based on the nature of medical illnesses, prior physical health, and patient’s wishes. In this group 14 (88%) patients had Type II respiratory failure and two (12%) had Type I respiratory failure. Overall 8 (50%) out of 16 had a successful outcome with NIV.
Conclusion: NIV can be used effectively in developing countries to treat patients with respiratory failure. It can be applied outside ICU and can obviate the need of invasive mechanical ventilation in responders. It can be used, with good effect, in patients not suitable for invasive mechanical ventilation.
P18 RELATIONSHIP BETWEEN AQ20, SGRQ, AND EXACERBATION FREQUENCY IN PEOPLE WITH COPD IN PRIMARY CARE
A. Choudhury, C.M. Dawson, H.E. Kilvington, C.J. Griffiths, G.S. Feder, J.A. Wedzicha. Department of General Practice and Academic Respiratory Medicine, St Bartholomew’s and Royal London School of Medicine and Dentistry, London, UK
Health related quality of life (HRQoL) is closely related to exacerbation frequency in patients with chronic obstructive pulmonary disease (COPD). The main obstacle to measuring HRQoL in primary care is their size and complex nature. The Airways Questionnaire 20 (AQ20) (Barley EA, et al.
) is a short, simple, disease specific questionnaire. Dimensions range from 0 to 20 (worst health).
Patients were recruited from general practices in East London. Patients were aged 40 and above, current or ex-smokers and were prescribed regular inhaled steroids. We asked patients to complete the AQ20 and the St George’s Respiratory Questionnaire (SQRQ) simultaneously at interview.
One hundred and thirty one patients (68 male) of median age 66 years (range 48 to 87) with COPD were recruited from 12 general practices. Mean (SD) FEV1 was 1.28 (0.55) l, FEV1 predicted 50.0 (18.0)%, mean FEV1/FVC ratio was 57.0 (16.0)%. Patients had a yearly exacerbation rate of 2.4 (2.5). The median AQ20 score was 11 with a range of one to 19. The median SGRQ total score was 51.0 with a range of 7.7 to 93.3. The AQ20 was strongly correlated to the SGRQ (Spearman rank correlation); SGRQ symptom (0.548), activities (0.681), impacts (0.742), and total (0.749).p<0.001. Other statistically significant findings with AQ20 were predicted FEV1 (−0.271) and pack years smoked (0.242) p<0.005. Patients were divided into those who had less than three COPD exacerbations per year (infrequent exacerbators) and those who had three or more exacerbations per year (frequent exacerbators).
The AQ20 shows a strong relationship to yearly exacerbation rate. The AQ20 is simple to implement and can be used to assess health status for patients with COPD in primary care where time and resources are limited.
AQ20, SGRQ, and exacerbation frequency
P19 USING A PRIVATE SECTOR PARTNERSHIP TO PROVIDE SUPPORTED EARLY DISCHARGE FOR ACUTE EXACERBATIONS OF COPD IN A DISTRICT GENERAL HOSPITAL
C. Fehrenbach1, E. Neville1, W.F. Holmes2. 1Portsmouth NHS Trust; 2Nestor Healthcare PLC, UK
Home care is successful in about 25% patients hospitalised with an exacerbation of COPD,(1) though nursing resources are not always available to provide it. Encouraged by the government’s endorsement of partnerships between the NHS and the private sector,(2) a six month home care service was commissioned from Nestor Primecare, for nurse led 24hr care for selected patients following early hospital discharge. The Trust Respiratory nurses reviewed patients one month after discharge in clinic.
Following medical assessment in hospital (protocol available), the nurse accompanied and transported the patient home, and thereafter provided care over a 10 day period, (mean attendance: five hours). During the day, patients had direct access to the nurses, and at night through a dedicated telephone support line. When thought necessary, readmissions were organised by the nurse, not the patient’s general practitioners.
In Portsmouth, about 580 000 patients are served by two district general hospitals and three Primary Care Trusts. During the six months to July 2002 there were 276 admissions to the Trust coded J44.1 (exacerbation of COPD). The average hospital stay for this condition locally is eight days. Of these patients, 124 (44%) (50% male) received supported discharge within 1–2 days of admission. Fifty four calls for support came from 34 patients but none needed referral to their GP. There were 18 readmissions during the period of home care (14%). Seven patients died during readmission, but none of those remaining at home. Patient satisfaction was high, and only one person refused home care.
Conclusion: This 10 day service was successful in a higher proportion of patients than in previous studies, and at a total cost of £85 000.
1. Gravil JH, et al.
.
2. DoH. NHS Plan. London: Department of Health, 2001.
P20 A REGULAR VISIT TO PATIENTS ADMITTED WITH COPD REDUCES FURTHER HOSPITAL ADMISSIONS
R. Rowles, R. Bennett, A. Hill, S. Jones, J. Goldman. Heart and Lung Unit, Torbay Hospital, Torquay, TQ2 7AA UK
The Torbay Hospital Outreach Respiratory Team (THORT) has been supporting the early discharge of patients with exacerbations of COPD since December 1999. It was noted that certain patients were having frequent admissions often with minor exacerbations that were then managed at home by THORT. It was proposed that regular maintenance visits by the team on patients identified as having frequent admissions or significant problems with anxiety would reduce these.
The first of these visits was in July 2001. In total 12 patients have been placed on the maintenance list and data has been collected on admissions pre and post the start of visits. For the purpose of this study 10 patients were selected who had complete sets of admission data for 12 months prior to the visits, and had been receiving maintenance visits for at least two months. Total bed days and THORT days were averaged over the previous 12 month period, and for the period since the onset of maintenance visits to give an indication of whether admissions had subsequently reduced.
The results show that in the year prior to the start of visits the average number of bed days and facilitated discharge days under THORT per month for the 10 patients studied was 40.1. After the introduction of maintenance visits the average number of days was 8.7 per month. The average number of maintenance visits undertaken per month was 12.8.
Although this study has comparable data on a small number of patients, preliminary results suggest that regular maintenance visits to patients with COPD identified as having frequent exacerbations do have a positive impact on their ability to cope at home and avoid admission to hospital. In conclusion directing resources towards providing regular support to appropriate patients with COPD would be seen to be a cost effective way of reducing the use of healthcare resources by COPD patients over the winter months.
P21 PRIMARY CARE EXPERIENCE OF PATIENTS ADMITTED TO HOSPITAL WITH AN EXACERBATION OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE
A. Coe, A.O.C. Johnson. Pontefract General Infirmary, Pontefract, West Yorkshire, UK
Although `Hospital at Home’ schemes for early facilitated discharge of patients with exacerbations of chronic obstructive pulmonary disease (COPD) have become more prevalent, schemes to prevent admission are less widespread. AC was awarded a Health Action Zone fellowship to investigate the role of a respiratory therapist in assessing and triaging potential admissions with exacerbations of COPD into those who require admission, early facilitated discharge (by referral to our Hospital at Home Scheme) or conventional discharge. This survey was done to inform the design of the potential new service.
Fifty three patients (mean age 71) admitted to hospital with exacerbations of COPD were questioned about their contact with primary care prior to admission. There were 26 men and 27 women. Symptoms which prompted admission included increased breathlessness (92%), wheeze (72%), cough (55%), increased sputum volume (49%), sputum colour change (45%), fever (38%). Three patients denied any change in symptoms. Prior to admission, 25% of the patients had had no contact with primary care services, 25% had telephone contact only, 34% were seen at home, and 17% were seen in the GP surgery. Of the 40 patients who had some contact with primary care, 40% had contact in the morning, 40% in the afternoon and only 12.5% out of hours (no data on three patients). Only 8 patients were seen twice with the same exacerbation prior to admission.
When asked why they had bypassed primary care most patients said either that they or a relative thought the situation too urgent for a GP to manage, or that previous experience was that the GP would send them to hospital anyway. The three patients with no change in symptoms had all bypassed primary care and were admitted because of anxious relatives. In contrast to the time of primary care contact, attendance at hospital was mostly out of hours (51%) or afternoon (36%). About half of the admissions were arranged by GPs, a quarter saw the GP but self presented to A&E anyway, and a quarter bypassed primary care altogether.
We conclude that many patients and relatives admitted with COPD have little confidence in primary care’s ability to deal with exacerbations, especially out of hours. A 24 hour service with specialist training may be able to deal with some patients with exacerbations and prevent unnecessary admission to hospital.
Bronchoscopic and other lung investigations
P22 Bronchoscopy practice in england and Wales, 2002
J. Pickles, M. Jeffrey, A. Datta, A.A. Jeffrey. Chest Clinic, Northampton General Hospital, Northampton NN1 5BD, UK
Aims: To assess current practice in bronchoscopy preparation in England and Wales.
Methods: Questionnaires were faxed to respiratory consultants listed in The BTS Directory.(1) We looked at the population, number of consultants and bronchoscopies undertaken, topical anaesthetic use, sedative use and how adequate sedation is judged.
Results: There was a response rate of 76% (344 responses to 452 questionnaires). Median consultant numbers per hospital was three (IQR 4–6), median population served per consultant was 116 00 (IQR 90–150 000). The majority of bronchoscopists use lignocaine spray to the throat (70%), sometimes with spray to the nose (43%), together with gel to the nose (65%). The majority use 4% lignocaine to the vocal cords (54%) and 2% to the bronchi (71%). Atropine is used routinely by 13%. Sedation with midazolam (78%) or other combinations (22%) is routine. The option of sedation is only discussed with the patients by 8.4% of consultants. Only three operators use formal sedation scores to assess patient level of sedation. Oxygen saturation was the commonest measurement used (n=98) to judge sedation. Otherwise, response to sedation was judged by clinical experience (n=60), patient response (n=57), and conscious level (n=50).
Conclusion: Despite the recent BTS guidelines there is considerable variation in bronchoscopy practice, particularly in sedation practice. Patient level of sedation is not formally assessed and combinations of sedatives and analgesics are used contrary to the recent guidelines on safe sedation practice.(2) Sedation options are not routinely discussed. The wide variations in practice may reflect the lack of consistent evidence based guidance on sedation techniques for bronchoscopy. Further study to determine optimal technique is required.
1. BTS/Astra Zeneca. The directory of respiratory medicine [7th ed]. Hawker Publishing, 2002.
2. Safe sedation practice. Academy of Medical Royal Colleges and their Faculties, 2001.
P23 FLUORESCENCE BRONCHOSCOPY IN PATIENTS WITH ABNORMAL SPUTUM CYTOLOGY
A.K. Banerjee1, P.H. Rabbitts1, P.J.M. George2. 1Molecular Oncology Group, University Of Cambridge, UK; 2The Middlesex Hospital, London, UK
Introduction: Patients at risk of lung cancer with abnormal sputum cytology or bronchial washings but no other evidence of lung cancer present a management dilemma. Autofluorescence bronchoscopy detects preinvasive endobronchial lesions and carcinomas with greater sensitivity than conventional bronchoscopy. We present a series of patients with abnormal sputum cytology or bronchial wash cytology investigated further with autofluorescence bronchoscopy.
Methods: Patients selected had no clinical or radiological evidence of invasive carcinoma and no bronchoscopic abnormality within the preceding two months. The visible bronchial tree was inspected with white light and autofluorescence using the Storz bronchoscope. Biopsies were taken of all areas appearing abnormal bronchoscopically.
Results: Ten patients were studied, eight males with a mean age of 66.5yrs (range 51 to 79 yrs). All were smokers, mean exposure 47 pack years (range 18.5 to 79). The table shows the bronchoscopy results and outcomes for the study patients.
Bronchoscopy results and outcomes for the study patients
Conclusions: In this group of patients, no abnormality detectable at fluorescence bronchoscopy suggests a good outcome, with no evidence of carcinoma at up to 42 months. Abnormal fluorescence may reveal the presence of radiologically occult carcinoma, or high grade preinvasive lesion, but may also be a false positive finding. High grade preinvasive lesions may exfoliate cells that resemble squamous carcinoma cells. Fluorescence bronchoscopy may provide useful information in this difficult group of patients. This study is limited by the small numbers and relatively short duration of follow up, but suggests that a larger study should be undertaken.
P24 ENDOBRONCHIAL MIMICS OF LUNG CANCER: A CASE REPORT AND REVIEW OF BRONCHOSCOPY DATA BASE
S. Lohani, P.R. Chadwick, G.R. Armstrong, B.R. O’Driscoll, S.C.O. Taggart. Respiratory Medicine Department, Hope Hospital, Salford M6 8HD, UK
Case report: A 72 year old ex-smoker and retired fireman with previous asbestos exposure, presented with a six week history of cough, breathlessness, and wheeze. Clinical examination revealed a small basal effusion. CXR examination confirmed the clinical findings. ESR was 122 mm/hour. CT scanning revealed a loculated effusion and loss of volume in right lower lobe (RLL) with associated distal consolidation. Initial and subsequent bronchoscopies demonstrated an endobronchial RLL “tumour” but biopsies were negative for cancer. The patient was informed that cancer seemed the most likely cause of his symptoms. However, ultrasound guided aspiration of the fluid revealed an empyema which grew Actinomyces israelii. This was subsequently demonstrated to be present in both previous biopsy specimens. The patient made a full clinical and bronchoscopic recovery after six weeks of penicillin treatment.
Review of bronchoscopy data base: Over the past 10 years, our team has performed 4199 bronchoscopies of which 1122 (27%) were found to have lesions suspicious of lung cancer. Of these 1004 (89.5%) have had cancer confirmed by histology or cytology and 101 (9.0%) have been treated as cancer although the biopsies were negative. Of patients with suspicious bronchoscopies, 17 (1.5%) had a specific non-malignant diagnosis (see table).
Conclusions: Endobronchial mimics of lung cancer account for >1% of suspicious bronchial lesions. We recommend caution in informing patients of cancer until either histological confirmation is obtained or other causes are excluded.
P25 BRONCHOALVEOLAR LAVAGE, NON-INVASIVE INVESTIGATIONS AND RADIOLOGY: IMPACT ON TREATMENT IN PATIENTS WITH HAEMATOLOGICAL MALIGNANCIES AND PULMONARY INFILTRATES
A.R. Benjamin, E.F. Bowen. Respiratory Medicine Unit, Hammersmith Hospital, London W12 ONN, UK
Pulmonary infiltrates are a frequent complication in immunosuppressed patients with haematological malignancies requiring early diagnosis with prompt appropriate treatment. We investigated the diagnostic yield of bronchoalveolar lavage (BAL) and non-invasive sampling (NIS) in this population over a 12 month period and evaluated their impact on treatment modification.We compared high resolution computed tomography (HRCT) findings with these results. Twenty five bronchoscopies (FOBs) (21 patients) were performed during this period. Seventeen out of 21 patients were post bone marrow transplant and 4/21, on high dose chemotherapy. Pre FOB, 16/25 cases were neutropenic and/or lymphopenic, 15/25 were thrombocytopenic, 22/25 were pyrexial, and 22/25 were on empirical antibiotics. All were hypoxic and required supplemental oxygen periprocedure. Post FOB, 1/21 patient required admission to the intensive care unit.
Blood cultures, sputum cultures, and nasopharyngeal aspirates were positive in 3/41, 4/21, and 1/3 samples respectively and treatment was modified in 2/25, 2/25, and 1/25 cases respectively. Overall, NIS was positive in 8/25 (32%) cases with subsequent treatment modification in 5/25 (20%) cases. BAL was positive in 10/25 (40%) cases. (7/25 bacterial, 2/25 viral, 1/25 PCP) and treatment was modified in 8/25 (32%) cases. Where NIS was positive, BAL confirmed the diagnosis only once and in one case revealed another organism that changed management further.
In 2/25 cases, chest radiograph (CXR) was not done prior to HRCT. CXR was abnormal in 16/25 cases, 13 of which proceeded to HRCT with subsequent treatment modification in 5/13 cases. In 7/25 cases, CXR was normal of which all had abnormal HRCTs with treatment modification in 1/7 case. Overall, HRCT led to treatment modification in 6/22 cases, in which BAL confirmed the suspected aetiology in 2/22 cases.
This data indicates that the sequential use of NIS and BAL gives the highest diagnostic yield of pulmonary infiltrates. At our institution, HRCT was not sensitive enough to allow for its confident use as a diagnostic tool in place of BAL. Although FOB is a high risk procedure in this population, this data supports BAL as a safe and useful investigation.
P26 CT GUIDED LUNG BIOPSIES: DO THEY PROVIDE THE DIAGNOSIS?
P.L. Williams, R.K. Rajakulasingam. Department of Respiratory Medicine, Homerton University Hospital, London, UK
When requesting CT guided lung biopsies we are frequently asked “Will the patient tolerate a pneumothorax?”. With this in mind we performed an audit of this technique to assess the success rate of the procedure, frequency of complications, and the sensitivity and specificity for diagnosing lung cancer.
Using the CT record book to identify cases we recorded details of all (n=68) patients recorded as having had “lung biopsy” over the previous four year period. We used patient case notes, the lung cancer database, and the computer based histology records and CT reports to record, where possible, the indication, histology obtained, whether or not further investigative procedures had been required, any documented complications, and the final diagnosis.
Of the 68 patients recorded as “lung biopsy”, 1% actually had pleural biopsy and 4% lung aspirate. Of these there were no complications and the procedure provided the diagnosis. Sixty four patients were scheduled for the procedure: percutaneous core needle biopsy under CT guidance, following infiltration with subcutaneous lignocaine. 1-”multiple” passes were made as required/tolerated. Each patient had a postprocedure CT check for pneumothorax. Of the 64, 6% were cancelled due to radiological improvement and 6% abandoned due to technical difficulties, leaving 56.
The indication for biopsy was suspected lung cancer in 91%. We wanted to know whether the procedure provided the final diagnosis or if further measures needed. Of the 46 patients in whom adequate information was available, the histological sample from biopsy was successful in providing the final diagnosis in 71%. Histology was obtained but further investigations were needed in 26%. No histology was obtained in 4%. Of the 56 patients who underwent any procedure pneumothorax preventing biopsy occurred in just 2%. Smaller pneumothoraces occurred in 13%, and the remaining 85% experienced no complications.
The sensitivity of the procedure for diagnosing lung cancer was 90%, specificity 100%, and false negative rate 8%. These and the complication rate compared favourably with other published studies of lung biopsy. In a DGH this procedure is still useful and we have demonstrated a relatively low complication rate.
P27 GENERAL PRACTICE OPEN ACCESS SPIROMETRY: WHO WAS REFERRED IN 2001?
A.H. Kendrick, D. Smith, M.R. Hetzel, J.R. Catterall, G. Laszlo. Department of Respiratory Medicine, Bristol Royal Infirmary, Bristol, UK
We provide an Open Access spirometry service to primary care. Patients attend from 09:30 to 11:30 Mon to Fri. A technologist obtains a history, spirometry pre and post β2-agonist via spacer and pulse oximetry. A report and recommendations are sent to the GP.
Aim: To review the throughput of this service in 2001.
Methods: The records of all patients attending the service were reviewed. Data are given as median (range).
Results: 706 patients attended, with 55 having further studies after a trial of steroids. Age was 54.7 yr (10 to 91), 366 were female and body mass index (BMI) was 27.4 kg.m-2 (14.9 to 52.6). 198 had a BMI ≥30 kg.m-2. History: 274 were smokers, 438 had cough, 368 had wheeze, and 397 had sputum production. MRC dyspnoea grade (n = 696) was Grade 1–110, Grade 2–230, Grade 3–223, Grade 4–116, and Grade 5 – 17. One hundred and ninety six patients had no medication, 49 were on antibiotics, 261 on a β2 agonist, 24 on an anti-muscarinic, 177 on oral/inhaled steroids, 32 on a β blocker, 57 on a blood pressure tablet, and 203 patients were on other therapies. Lung Function: FEV1%predicted was 84.7 (15 to 143), FVC%predicted was 89.1 (14.7 to 144) and FEV1%FVC was 74.9 (23.9 to 100). Sixty one studies showed submaximal/variable efforts. One hundred and fifteen patients had normal spirometry, 68 reversible airflow obstruction, 438 irreversible airflow obstruction, and 24 a restrictive defect. For reversibility, absolute change in FEV1 was 0.4 l (0.2 to 1.45) and % change was 29.8% (15.4 to 271). Nine out of 55 steroid trials showed a positive response with the absolute change in FEV1 (post β2 agonist) of 0.45 l (0.2 to 0.8) and % change of 29.8% (15.1 to 64.0). Pulse oximetry (n = 676) showed 34 patients had an O2 saturation ≤92%. Recommendations: 25 patients with airflow obstruction to change from β blockers, 145 patients for a trial of inhaled steroids with repeat spirometry, 40 to be prescribed a β2 agonist, 184 to be referred for further investigations—LTOT (n = 34), ?occupational lung disease (n = 36), ?EIA (n = 27), excessive dyspnoea for spirometry (n = 63), and restrictive defect (n = 24).
Conclusion: This service (1) accurately assesses simple lung function, (2) identifies groups of patients requiring further investigation or a change in therapy, and (3) provides recommendations to assist the primary care physicians to manage their patients.
P28 SERIAL PEAK FLOW MEASUREMENTS FOR THE DIAGNOSIS OF OCCUPATIONAL ASTHMA: IMPROVING THE QUALITY
V. Huggins1, W. Anees1, C. Pantin2, P.S. Burge1. 1Occupational Lung Disease unit, Birmingham Heartlands Hospital, UK; 2Department of Respiratory Medicine, North Staffordshire Hospital, Stoke-on-Trent, UK
Serial measurements of peak expiratory flow (PEF) are usually the most appropriate first step in the investigation of occupational asthma.
Different centres have reported widely different success in obtaining records of sufficient data quantity for diagnosis. We have investigated different methods of instruction and determined the return rate and quality of the resulting record for the diagnosis of occupational asthma using predefined criteria.
Methods: Three instruction methods have been investigated: 159 were instructed by post (postal group), 86 were personally instructed by a PEF specialist (personal group), and 40 were instructed by others—for example, GPs, occupational health physicians, or nurses.
Results: The postal return rate was 56% and the personal return rate 85%, adequate data quantity was similar in the postal and personal groups (54.8% and 58.8% respectively). Pre-existing records plotted from graph charts were only adequate in 23%, compared with pre-existing records plotted from occupational forms (61% adequate). Failure of the record to contain consecutive periods of ≥3 workdays was the most common reason for inadequate data quantity.
Conclusion: The quality and return rate of PEFs for diagnosing occupational asthma is better when patients have been given specific instructions from a PEF specialist and recording is on a dedicated form.
P29 DIFFERENCES IN INDICES OF PEAK EXPIRATORY FLOW VARIABILITY BETWEEN WORKERS WITH OCCUPATIONAL ASTHMA AND IRRITANT (GRAIN DUST) EXPOSED HEALTHY SUBJECTS
W. Anees1, D. Blainey2, V. Huggins1, K. Robertson2, P.S. Burge1. 1Occupational lung disease unit, Birmingham Heartlands Hospital, Birmingham, UK; 2Broomfield hospital, Chelmsford, Essex, UK
Introduction and Aims: Serial peak expiratory flow (PEF) records have been recommended as a first line investigation in workers suspected as having occupational asthma. It is unclear, however, to what extent they can differentiate between workers with occupational asthma and healthy workers exposed to irritant agents, and which index of PEF variability is best at doing so.
Methods: Indices of PEF variability were compared in three groups of subjects. (1) Forty healthy grain exposed farmers and dockers. (2) Forty two consecutive subjects with independently confirmed occupational asthma. (3) Forty eight non-occupational asthmatics.
Results: The index of PEF variability that best separated the occupational asthmatic workers from the others was the difference in mean PEF between rest and work periods. The upper 95% confidence limit of this index for the grain workers was 2.8% of predicted PEF (16 L/min), for non-occupational asthmatics 3.3% predicted PEF (15 L/min). Sensitivity for diagnosing occupational asthma using this index was 70%. Only 40% of workers with confirmed occupational asthma had a PEF diurnal variability >17% of predicted, the upper limit for grain workers. An increase in diurnal variation on work days of >7% (the upper 95% limit for non-occupational asthmatics) had a sensitivity of only 27% for the diagnosis of occupational asthma. The difference between maximum PEF on work days and minimum PEF on rest days was poor at separating occupational asthmatic workers from those with non-occupational asthma.
Conclusion: Difference in mean PEF between work and rest days is the best simple index for differentiating subjects with occupational asthma from those with non-occupational asthma or irritant exposed healthy subjects.
P30 REPEATABILITY OF CHLORIDE LEVELS IN EXHALED BREATH CONDENSATE (EBC)
A. Zacharasiewicz, N. Wilson, A.M. Li, CH. Lex, J. Hooper, A. Bush. Department of Paediatric Respiratory Medicine, Royal Brompton Hospital, UK
Background: Reproducibility of measurements of EBC is controversial (Effros, et al.
). It has been suggested that there is a wide variation in dilution of the collected sample, which would make interpretation of measurements difficult.
Aim: to assess the repeatability of Sodium [Na] and Chloride [Cl] measurements in EBC in healthy adults and in asthmatic and cystic fibrosis (CF) children.
Methods: EBC were collected for 10 minutes using a Condenser (Ecoscreen (Jaeger) and wearing a nose clip. [Na] and [Cl] were measured with a CIBA Corning M 644 NaCl Analyser. Samples of five healthy adults were collected five times within one day with a 20 minute interval each. To measure period repeatability, the collection was repeated on another day within eight weeks. Technical repeatability was measured by aliquoting each sample into two tubes. Within day repeatability was also assessed in seven asthmatic and eight CF children from two collections within two hours. Repeatability was calculated according to Chinn (Chinn S.
).
Results: Na could not be detected in >30% EBC, so was not analysed further. For normals, the mean (SD) [Cl] was 4 (0.95) mmol/L; the technical repeatability within one sample, calculated by the single determination range was ±1.96 mmol/L, and the within subject day repeatability assessed as the 95% range for change within a day was ±1.16 mmol/L, the within period (eight weeks) range of change was ±2.18 mmol/L. For asthmatics, the mean [Cl] was 4.4 (0.9) mmol/L with a range of change of ±2.98, in CF patients the mean [Cl] was 5 (1.5) mmol/L and 95% range for change was ±3.38 mmol/L.
Conclusion: The variability of measured levels is similar for within test (paired estimates of the same sample), within day and between visits, for both normals and children with asthma and CF. Thus our data suggest that the major source of variability of [Cl−] can be explained by limitation of the measurement assay method used, rather than as an effect of intrinsic variability in EBC collection per se. The wide use of EBC is most likely dependant on the development of highly sensitive and reproducible assays, rather than further refinements of the collection technique.
P31 DOES AIRFLOW OBSTRUCTION OR INHALATION OF SALBUTAMOL INCREASE THE VOLUME OF EXHALED BREATH CONDENSATE COLLECTED IN STABLE COPD AND ASTHMA?
S. Manney1, J.G. Ayres1, J. Baker2. 1Air Pollution Laboratory, Heartlands Research Institute, Birmingham Heartlands & Solihull NHS Trust, Bordesley Green East, Birmingham, B9 5SS, UK; 2Division of Environmental Health & Risk Management, University of Birmingham, Edgbaston, Birmingham, B15 2TT, UK
Introduction: Exhaled breath condensate (EBC) collection, although widely accepted as a method for measuring molecules in exhaled breath, is not well characterised methodologically. Factors such as airflow obstruction, bronchodilator therapy, or respiratory rate may affect the volume of EBC volume achieved. The main aims of this study were to examine whether EBC volume collected could be increased post salbutamol inhalation, and whether EBC volume collected was directly linked to airflow obstruction as assessed by FEV1.
Methods: Eighteen volunteers were studied (10 COPD, eight asthmatics). Each completed six collections over three days. On each occasion, subjects were asked to refrain from taking short acting bronchodilators for six hours before the study. Two collections were made on each day (breathing via mouthpiece and two way valve into two Teflon tubes in ice for 15 minutes), pre and post inhalation of 200 μg salbutamol. Spirometry was completed on all volunteers at the end of both collections. On each of the three days, volunteers completed the same protocol for reproducibility of volumes.
Results: There was no correlation between airflow obstruction and EBC volume collected.
There was no significant difference in EBC volume pre and post bronchodilator when considering all 18 patients (2.26 ml (SD)(0.35) pre; 2.31 ml (0.35) post) (p=0.46). For patients with COPD the respective volumes were 2.21 ml (0.30) and 2.35 ml (0.32) (NS) while for asthma they were 2.33 ml (0.42) and 2.22 ml (0.37) (p=0.04).
Conclusion: EBC volume was not related to the degree of airflow obstruction and bronchodilator inhalation did not increase EBC volume.

FEV1v EBC volume produced.
P32 A NOVEL DEVICE FOR THE PRECISE MEASUREMENT OF RESPIRATORY HEAT AND MOISTURE LOSS
J.B. McCafferty1, P.K. Kew2, A. Haston2, J.A. Innes1. 1Respiratory Unit, Western General Hospital, Edinburgh; 2Department of Mechanical and Chemical Engineering, Heriot-Watt University, Edinburgh
Background: It is proposed that respiratory heat and moisture loss (RHML) are altered by airway inflammation and that measurements of RHML may yield a useful non-invasive marker of such inflammation. Simple exhaled temperature and humidity measurements are however insufficient to characterise RHML as heat and moisture loss are affected by respiratory pattern and inspirate temperature and humidity. To precisely measure RHML in normal subjects and patients with airway disease we have developed a novel device which can control inspired air temperature, humidity, minute ventilation, and tidal volume.
Methods: The device is a compact trolley mounted air conditioning module delivering air at up to 1500 ml/s with a controllable temperature (3°C to 40°C) and moisture content (5 to 40 g/kg dry air). Air is delivered to the inspiratory side of a 2 way valve by means of a flow past configuration. Temperature and humidity sensors located on inspiratory and expiratory sides of the breathing valve allow accurate, continuous recording of the thermodynamic state of air entering and leaving the respiratory tract. A computer linked to an ultrasonic flowmeter in the expiratory limb is used to generate auditory and visual feedback cues to help subjects control respiratory rate and flow respectively, allowing standardisation of ventilatory pattern between subjects. RHML at steady state is calculated as the product of mass flowrate and “enthalpy” difference between inspired and expired air. Six normal volunteers breathed inspirate at 7°C at a target minute ventilation of 15 l/min with either a slow deep pattern (rate 10/min, tidal volume 1455 (101) ml (SD)) or rapid shallow pattern (30/min, tidal volume 525 (36) ml).
Results: Mean respiratory heat loss was 15.7 (1.4) Watts during rapid shallow breathing and increased to 18.3 (1.3) Watts during the slow deep pattern (p=0.009). At the same tidal volumes respiratory water loss was measured as 334 (30) μl/min and 408 (46) μl/min respectively (p=0.008).
Conclusions: This new measurement device was sufficiently sensitive to detect a significant increase in RHML with increasing tidal volume at fixed minute ventilation in normal subjects. When normal ranges are defined it will be used to measure RHML under matching conditions in patients with COPD, asthma, and cystic fibrosis.
P33 EFFECT OF VARYING RESPIRATORY PATTERN ON EXHALED BREATH CONDENSATE COLLECTION
S. Tate, J. McCafferty, J.A. Innes, A.P. Greening. Respiratory Medicine Unit, Western General Hospital, Edinburgh
Background: Exhaled breath condensate (EBC) has been proposed as a non-invasive means of measuring pulmonary inflammation. At present little is known about how the respiratory pattern during collection influences the properties of the EBC sample. We hypothesised that variations in respiratory pattern would have significant effects on volume and concentration of EBC.
Methods: Ten control subjects had EBC collected three times for six minute periods each on the same day. For the three collections subjects were instructed to follow constant respiratory rates (RR) for the six minutes (10, 20, and 30 breaths per minute in random order), at a constant flow rate (500 mls/s) resulting in three different tidal volumes (Vt), (1500, 750, and 500 mls) but constant total respired volume for the three collections (90 L). A custom built air conditioning unit was used which allowed inspired air temperature and humidity to be kept constant. The expiratory limb of the unit housed heat and humidity sensors which allowed determination of heat (W) and moisture loss (mg/g dry air) from the respiratory tract. The system was linked to a flow meter and computer with an audiovisual cue so that the subjects could maintain the necessary RR and flow rate. A commercial breath condenser system (Jaeger) was fixed to the expiratory port to allow collection of EBC. Total volume achieved and solute concentration (nitrite) were measured for each collection.
Results: A strong correlation was found between EBC volume (μl) and Vt (r = 0.73, p<0.0001). However nitrite concentration was unaffected by Vt (r = 0.04, p=0.83) or total volume collected (r = −0.1, p=0.62). There was a strong correlation between moisture loss from the respirator tract and Vt (r = 0.7, p=0.0001). Calculated total water loss in six minutes related to actual EBC volume collected gave a measure of efficiency of collection. This calculated efficiency was also related to Vt (r = 0.5, p=0.018).
Conclusion: Collected EBC volume is enhanced significantly at higher tidal volumes. This appears a function of increased moisture loss with higher Vt but also increased condenser efficiency. Increased yield of EBC volume does not result in dilution of non-volatile solutes in the sample. The influence of other variables such as flow rate and inspired temperature on EBC collection need to be examined.
COPD: Assessment and treatment
P34 MECHANISMS OF BRONCHIAL HYPER-RESPONSIVENESS IN COPD
P.P. Walker, P.M.A. Calverley. Department of Medicine, University Hospital Aintree, Liverpool, UK
Bronchial hyper-reactivity (BHR) is a hallmark feature of asthma and a common, though not fundamental, feature of COPD. In asthma the response represents narrowing of the airway lumen due to contraction of airway smooth muscle (ASM). In COPD there is a relationship between BHR and airflow obstruction and we hypothesise that responsiveness is related less to changes in ASM and resistance and more to increase in hyperinflation. Hence an increase in residual volume (RV) will reduce the ability of the airway-parenchymal interface to overcome narrowing of the airway lumen.
We studied 10 subjects with mild to moderate COPD—baseline FEV1 1.59l (SD) (0.45l), FEV1 % predicted 55% (16%), FEV1/FVC ratio 0.49 (0.1)—who underwent standard methacholine challenge testing. At baseline subjects had moderate increases in airway resistance measured by body plethysomnography (Raw 3.04 − predicted 1.86), moderate increases in resistance (R5Hz 0.67 − predicted 0.32) and impedance (Z5Hz 0.77 − predicted 0.32) measured by IOS and moderate reduction in inspiratory capacity (2.53l − predicted 2.91l). Median PC20 was 0.54 (range 0.1 to >16) and all but one subject achieved a PC20 at <2 mg/ml.
After challenge mean FEV1 fell by 34% to 1.05l (p<0.01), mean FVC fell by 38% to 2.08l (p<0.01), mean SVC by 30% from 3.74l to 2.61l (p<0.04), and IC by 38% to 1.60l (p<0.01). TLC, when measured, was constant therefore these changes represent significant increases in RV. Airway resistance by body plethysomnography (Raw) increased overall (3.04 v 12.16) but showed minimal change in three subjects while measurement in five other subjects was technically difficult. IOS measurements showed an overall modest increase in impedance (0.77 v 1.01; p<0.01) which was due to a fall in reactance (−0.35 v −0.55; p<0.04). There was no significant change in resistance (0.67 v 0.83; p<0.12).
In individuals with COPD who are subject to bronchial challenge assessment of changes in FEV1 does not give a true measure of change in respiratory system resistance. BHR is likely to be determined less by ASM contraction and more by increases in hyperinflation, which in turn alter the ability of the lung to overcome airway narrowing.
P35 CHRONIC BRONCHITIS, SMOKING AND SOCIOECONOMIC STATUS IN THE NHANES III DATASET
M. Sridhar1, G. Netuveli2, A. Sheikh2. 1NHLI Division of Faculty of Medicine; 2Department of Primary Health Care & General Practice, Charing Cross Hospital, UK; Imperial College of Science, Technology & Medicine, London, UK
Background: While some studies have suggested that differences in the prevalence of chronic bronchitis in the various socioeconomic groups is due to differences in smoking habits, others suggest an explanation unrelated to smoking.
Methods: We have examined the relation between the prevalence of chronic bronchitis, smoking and socioeconomic status (SES) in a subset of the extracted from the US NHANES III data set representing a population of 115 million adults between the ages of 30 and 75 years. A measure of SES was constructed using household income and education. Current smoking status, duration of smoking, and intensity of smoking were also noted. Symptom identified bronchitis (SIB) and doctor diagnosed bronchitis (DDB) were used as outcome measures. Data was analysed using logistic regression analysis with appropriate population weighting.
Results: SIB was significantly related to age above 70 years, African and Hispanic ethnicity, upper SES, and smoking. DDB was related to age, being male, African and Hispanic ethnicity, SES, and smoking. Of these, being male, ethnicity, and higher SES were protective. In SIB, within each stratum of SES, the only consistently significant variable was current smoking status. No significant interaction between smoking and SES was detected. When DDB was used as outcome measure, the current smoking status was significantly associated only in the upper middle SES strata. For both outcomes, stratification according to current smoking status revealed SES to be significant in current smokers only.
Conclusions: Socioeconomic status had a significant influence on the prevalence of SIB that was independent of cigarette smoking. The protective effect of higher socioeconomic status was most significant for current smokers. This effect seemed to be independent of smoking behaviour in the different SES strata and merits further scrutiny.
Acknowledgements: An NHS R&D National Primary Care Fellowship supports AS. GN is supported by a grant from the National Asthma Campaign, UK.
P36 MEDICAL RESEARCH COUNCIL DYSPNOEA SCALE IS A MEASURE OF FUNCTIONAL CAPACITY AND GLOBAL PERCEIVED HEALTH STATUS
C. McAlpine1, W. Cochrane1,2, B. Watson2, M. Heatley1, S. Dogan1, G. Dovey-Pearce1, G. Afolabi1. 1Northumbria Healthcare NHS Trust, Northumbria, UK; 2Northumbria University, Northumbria, UK
Introduction: The Medical Research Council Dyspnoea scale (MRCD) has been used to categorise disability in patients with COPD, though it remains unclear what the scale measures.
Participants: All 218 participants had stable COPD. Sixty per cent reported MRCD scale grade 3, 29% grade 4, and 11% grade 5. Forty four per cent were male and mean (95% CI) age was 68.8 (67.8 to 69.7) years.
Methods: Participants were graded on the MRCD scale on the basis of self report information. Incremental shuttle walking test (ISWT) distance, spirometric, and anthropometric measurements were recorded. Self report data were recorded to assess: perceived health status (Chronic Respiratory Disease Questionnaire (CRDQ)); personal cognitions of illness (Illness Perceptions Questionnaire); affect (Hospital Anxiety and Depression Scale); and self efficacy (COPD Self Efficacy Scale). χ2 And Oneway and Kruskal Wallis ANOVA analysis were carried out to assess differences in respondent characteristics across MRCD grade.
Results: Mean percent predicted FEV1 was 9.93% higher people with grade 3 than those with grade 5 (F = 4.33, p=0.01). Resting oxygen saturation was significantly higher in people with grade 3 compared with those with grades 4 and 5 (F = 9.11, p<0.001). People with grade 3 had a mean ISWT of 235.0 m compared with 153.0 and 117.7 m for grades 4 and 5 respectively (F = 20.05, p<0.001). On the CRDQ, mastery, and emotional functioning were significantly higher, and fatigue and dyspnoea were significantly lower, in people with grade 3 compared with those with grade 4 and 5 (p<0.02). Anxiety was significantly higher in people with grade 3 compared with those with grade 4 (χ2 = 6.13, p=0.04) and people with grade 5 had a higher perception of treatment control compared with those with grade 4 (χ2 = 8.24, p=0.016). Of people with grade 3, 31.8% regarded themselves as being in good health, compared with 16.7% with grade 4, and only 4.5% with grade 5 (χ2 = 10.38, p=0.006). There were no significant differences across MRCD grade in body mass index, age, depression, self efficacy, or gender.
Conclusion: Only the ISWT and patients’ Global Perceived Health showed significant differences across all three grades of MRCD scale. The MRCD scale reflects patients’ functional capacity but also their global perceived health status.
P37 THE INFLUENCE OF BMI ON LUNG CT DENSITOMETRY IN EMPHYSEMA
D.G. Parr1, M. Needham1, B. Stoel2, J. Stolk2, R.A. Stockley1. 1Lung Investigation Unit, University Hospital, Birmingham, UK; 2Division of Image Processing, Leiden University Medical Centre, Leiden, the Netherlands.
Lung CT densitometry correlates well with pathological and physiological measures of emphysema and is the most sensitive measure for detecting disease progression in alpha-1 antitrypsin deficiency (AATD) (Dowson, et al.
). Long term reproducibility is subject to errors arising from limitations in the reconstruction algorithm, with changes in denser tissues affecting lung density measurements by altering beam hardening effects. Emphysematous lung is of similar density to air, and therefore changes in air densitometry reflect influences on lung densitometry. We looked at the effect of body mass index (BMI) on measured values for air density within the patient. Using a lung phantom, we then measured the effects on lung densitometry of an increase in chest wall thickness as would occur with increasing BMI.
Methods: We performed voxel densitometry of tracheal air on single slice inspiratory high resolution CT images at the level of the aortic arch in 41 patients with AATD (PiZ) and related the results to BMI. In addition, a thoracic phantom containing fixed, whole dog lung (KCARE, KCH, London) was imaged before and after attaching to the outer surface two flexible water filled containers of total volume 3.5L (Durex,UK) simulating increased chest wall mass. Lung densitometry was performed on two images taken from each series using the PULMO-CMS software (B Stoel, Leiden University). Three techniques were used; relative area at a threshold of –910 HU, the 15th percentile point and the mean lung density.
Results and conclusions: Tracheal air density measurements correlated well with BMI (Spearman’s rho = 0.55, p<0.001). Lung phantom densitometry was influenced by chest wall thickness as shown in the table.
A change in BMI over time will alter measured lung density. The effect of an increase in BMI could therefore be to reduce apparent emphysema severity
P38 CT SCANNING IN SUBJECTS WITH COPD AND THEIR RELATIVES
P.P. Walker1, J. Griffiths1, J. Curtis2, E. Thwaite2, P.M.A. Calverley1. 1Department of Respiratory Medicine; 2Department of Radiology, University Hospital Aintree, Liverpool, UK
Participants in a prospective COPD genetics study underwent thoracic HRCT scanning. Ninety two scans were performed in 71 subjects with COPD and 21 smoking siblings. We documented the frequency of lung nodules and other abnormalities and assessed their follow up to identify possible tumours. We also correlated spirometry and presence of visually scored emphysema on CT and compared the presence of bronchiectesis with clinical symptoms. Mean FEV1 was 1.46l, % predicted FEV1 50%. COPD severity by GOLD criteria: grade 1= 9(10%), grade 2A= 20(22%), grade 2B= 30(33%), grade 3= 12(13%), no COPD= 21(23%).
Twenty one (23%) subjects had lung nodules—4/21 in siblings without COPD. No malignancies have to date been confirmed. Ten (11%) subjects required investigation for other abnormalities including lobar collapse and asbestosis. Thirty nine additional radiology investigations have been completed so far (29 CT). Twenty one (23%) subjects had bronchiectesis on CT scan. In this population 42/92 subjects had chronic bronchitis clinically but only 6/21 subjects with bronchiectesis had symptoms of chronic bronchitis—no positive correlation.
The worse the spirometry the more likely emphysema was to be present but 33% of smokers with normal spirometry had CT evidence of emphysema. Pulmonary nodules were common and hence resource implications high. Spirometry was imprecise in identifying mild-moderate emphysema but severe obstruction correlated well with CT findings. In subjects without a recent infection bronchiectesis is frequently present without symptoms.
P39 MULTIDIMENSIONAL (IDS) ASSESSMENT OF COPD IN THE COMMUNITY: CLINICAL IMPACT IS UNDERESTIMATED BY CURRENT GUIDELINES
A.D. Lawrence, N.P. Keaney. Chest Clinic, Sunderland Royal Hospital, Sunderland, Tyne & Wear, UK
The staging of the severity of COPD is based on the degree of airflow limitation. Specific FEV1 cut points are used by the BTS, ATS, and ERS Guidelines. GOLD mentions the impact of COPD, and the imperfect relationship between impaired spirometric values and symptomatology, COPD also has systemic consequences. The IDS system of classifying COPD incorporates airflow limitation (impairment), dyspnoea (disability) and nutritional depletion (BMI-systemic involvement).
Our community database provided information on 401 patients (203 female) attending COPD clinics in eight general practices in Sunderland. Airflow limitation was classified according to standard BTS, ATS, ERS, and GOLD criteria using pre and post bronchodilator FEV1, and compared with IDS.
Use of post bronchodilator FEV1 does not perturb the IDS classification. All guidelines significantly underestimate the impact of COPD with their methods of classifying severity from spirometric impairment alone.
Table 1
Table 2
P40 A COMPARISON OF INTENSIVE, MDI-DELIVERED AND NEBULISED BRONCHODILATOR THERAPY IN SEVERE COPD
T.K. Rogers, A. Venners, H. Drayton, P. Camplin, G. Segust, R. McCook. Chest Clinic, Doncaster Royal Infirmary, Armthorpe Road, Doncaster, S. Yorks, DN2 5LT, UK
Background: We have investigated whether nebulised therapy provides superior bronchodilation to a combination of high-dose anticholinergic and long acting β2 agonist therapy, delivered via MDI and large volume spacer, in a well characterised group of stable patients with severe COPD (FEV1<40% predicted).
Methods: We undertook a comparison of three regimes of four times daily nebulised therapy (salbutamol 5 mg /ipratropium bromide 500 μg / Combivent 1 nebule) each used for a week in randomised order, against combined therapy with salmeterol 50 μg twice daily and ipratropium bromide 160 μg four times daily via MDI and large volume spacer, in an open label, sequential, cross over study. The outcome measure was self recorded peak flow rates, measured in the morning, pretreatment (am), afternoon (pm) and night time (nocte).
Results: Seventy three patients were enrolled, until the required number of 42 subjects with adequate data was obtained. Each of the three nebulised regimens was highly significantly, and probably clinically, superior to the MDI therapy, but there was no significant difference between them (ANOVA and paired t tests), see table.
Conclusions: Overall in this group of patients with severe COPD, nebulised therapy produced greater improvement in peak expiratory flow rate than could be achieved with intensive MDI-based therapy.
P41 ECONOMIC IMPLICATIONS OF REDUCTIONS IN COPD REHOSPITALISATION DUE TO TREATMENT WITH INHALED CORTICOSTEROIDS (ICS)
M.D. Spencer. GlaxoSmithKline, Greenford, UK
Background: A study in an Ontario observational database has demonstrated reductions in the rate of COPD rehospitalisation and death of 24% and 29% respectively using ICS (Sin, et al.
). Based on Hospital Episode Statistics there were 78 908 admissions for COPD in the year 2000/1 in England & Wales, with an average length of stay of 9.1 days, Sin and Tu’s data suggest over 15 000 of these would have been rehospitalisations (assumes current ICS usage 50%). This equates to a hospitalisation cost of over £155.8 m with over £31 m for rehospitalisations.
Methods: The economic implications of reductions in exacerbations have been assessed by modelling these risk reductions on a hypothetical population of 1000 patients, accounting for uncertainty in parameters by second order “Monte Carlo” simulation techniques. The implications of a hypothetical increase in the use of ICS by patients with an initial hospitalisation from 50% to 100% in England & Wales are then considered.
Results: For the hypothetical cohort of 1000 patients a comparison with and without ICS produces a reduction in hospital days of 622 (95% CI 494 to 760) equivalent to a cost saving of £135.6K (95% CI 95K to 189K). Applying this to an increase in ICS use from 50% to 100% for all patients with an initial hospitalisation, would result in a reduction in hospital days of 19 751 (95% CI 15 799 to 24 256) equivalent to a cost saving of £4.29m (95% CI £3.08m to 5.74m), thus offsetting a considerable portion of the drug purchase cost.
Conclusion: These results suggest that, additional to the obvious clinical benefits of avoiding COPD hospitalisation and mortality, valuable NHS resources may also be freed. In addition the financial cost (over £4m) of these hospital days may undervalue these resources during periods of high hospital bed occupancy.
P42 THE ASSOCIATION OF SURVIVAL WITH THE USE OF INHALED CORTICOSTEROIDS (ICS) SEEN IN OBSERVATIONAL STUDIES OF COPD CANNOT BE EXPLAINED BY UNOBSERVED MARKERS OF DISEASE SEVERITY (FEV1% PREDICTED, HEALTH STATUS, BODY MASS INDEX)
M.D. Spencer. GlaxoSmithKline, Greenford, UK
Background: Recent COPD studies performed in observational databases have shown benefits of ICS and ICS + LABA in terms of reductions in mortality and of hospitalisation (Sin, et al. 2001; Soriano, et al. 2002). A criticism of such studies, is the lack of randomisation and hence potential bias caused by the confounding of unobserved factors. This study investigates the relationship of a number of potential markers of disease severity in COPD to ICS prescription, and hence the potential for confounding.
Methods: The Health Survey for England 95, 96, and 97 (96 only for health status) forms the population for this study. Respondents with an FEV1/FVC ratio <70% and an FEV1% predicted of <70% were selected for analysis. Mean age = 65.9 and 42.2% were women. The relationship between disease severity and ICS prescription in COPD was investigated and the statistical significance tested using the independent t test.
Results: No statistically significant relationship was found between ICS prescription and BMI (p=0.518), whilst in the case of FEV1% predicted and of health status measured by both the EQ-5D and by the SF-6D patients taking ICS had on average worse scores than those not taking ICS (all p<0.001). See table.
Conclusions were unchanged when the population was limited to only those patients receiving at least one respiratory medicine.
Conclusions: In respondents to The Health Survey for England with objective airflow obstruction there was no association between ICS prescription and FEV1, BMI or health status that could explain benefits seen in other studies. The benefits of ICS seen in observational studies are unlikely to be explained by these differences between those taking and not taking ICS.
P43 AUDIT OF LTOT PRESCRIPTIONS IN BLAENAU GWENT
B. Perreira, S. Venn, B.V. Prathibha. Nevill Hall Hospital, Brecon Road, Abergavenny, South Wales, UK
Introduction: The ex-mining area of Blaenau Gwent has a high incidence of occupational and smoking related lung diseases. Provision of high quality clinical care to those individuals with severe disease includes the appropriate prescription of LTOT along with education to facilitate compliance. This audit was conducted with the aim of establishing whether the prescription and use of long term oxygen therapy in Blaenau Gwent complies with established guidelines.
Method: Audit criteria and standards were set using guidelines given in the Royal College of Physicians report Domiciliary Oxygen therapy services. Patients in Blaenau Gwent using oxygen concentrators in June 2000 were identified from Health Authority records. Criteria were measured from a review of hospital notes and by using a short postal questionnaire.
Results: Fifty patients were identified as using oxygen concentrators in Blaenau Gwent in June 2000. Notes were obtained for 48 of these patients (96%) and questionnaires were returned from 44 patients (88%). Thirty five (73%) of the patients were under the care of a respiratory physician. Only 15 (31.2%) had documented evidence of complete adherence to the guidelines prior to LTOT prescription (all under the care of a respiratory physician), although 39 (81.3%) of the patients had blood gases recorded. Thirty three (69%) had documented evidence of prescription for 15 hours a day, although the information given to patients was not recorded in the majority of cases. Of the respondents to the questionnaire, 38 (86.4%) reported using their oxygen for long periods of time rather than intermittently and 34 (77.3%) reported daily use of 15 hours or more. Thirty six (81.8%) understood to use the oxygen correctly and 22 (50%) were able to give a written explanation for their need of oxygen therapy.
Conclusion: The majority of patients who are prescribed LTOT report using it appropriately, although fewer understand the reason for treatment. However, it is of concern that appropriate assessment prior to LTOT prescription can only be confirmed in 31% cases and a chest physician had not seen 27% of the patients receiving LTOT. Following this audit a specially designed nurse led LTOT clinic has been started with referral to the chest physician. A patient information booklet has been introduced along with a blood gases record. A further audit will be conducted in one year to assess the impact of the clinic on the quality of care that patients using LTOT receive.
P44 WEIGHT CHANGE IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD): NOT JUST A PROBLEM OF UNDERNUTRITION
C.E. Weekes1, N.T. Bateman2. 1Departments of Nutrition & Dietetics; 2Respiratory Medicine, Guy’s and St Thomas’ Hospital NHS Trust, London, UK
Weight loss is frequently reported in patients with COPD and is associated with increased morbidity and mortality. In contrast, for the past 30 years the general population has become more overweight and therefore at increased risk for heart disease and diabetes. While reviewing patients for a nutrition intervention study it was noted that many patients presenting to chest clinic were overweight. The aims of this study were to establish the number of outpatients with COPD who were overweight, obese, or at risk as a result of weight loss.
Two hundred and seventy six consecutive patients with COPD (143 male; 133 female) were reviewed by the dietitian during a routine visit to the chest clinics at Guy’s and St Thomas’ Hospitals. Weight, height, and history of weight change were recorded, together with smoking status, presence of oedema, and steroid use. Medical records were reviewed to establish the length of chest related hospital stays and mortality. Mean age was 67.3 (10.3) years and body mass index (BMI) 26.2 (6.7) kg/m2. Patients were categorised as underweight, acceptable, overweight, or obese (BMI <20.0, 20.0 – 24.9, 25.0 – 29.9 or ≥30.0 kg/m2). Weight change was considered significant if it exceeded 5% in either direction.
Approximately half the patients were overweight (n = 80 (29%)) or obese (n = 61 (22%)) while one in six (n = 43 (16%)) were underweight. Sixty one (22%) patients reported significant weight loss and 53 (19%) reported weight gain. Oedema was noted in 26 (9%) patients.
Recent weight loss was associated with chest infection in 25 (9%) patients, gastrointestinal symptoms in nine (3%), and social reasons in five (2%), while 22 (8%) patients reported gradual weight loss over one to two years. Twenty two (8%) patients with significant weight loss had BMI ≥20.0 kg/m2, and 15 (5%) had BMI ≥25.0 kg/m2.
Recent weight gain was associated with smoking cessation in 17 (6%) patients, oedema in six (2%) and recent oral steroid use in two (<1%). The remaining 28 (10%) reported a gradual increase over several years.
There was a non-significant trend for increasing BMI to be associated with shorter length of hospital stay (5.9 (12.7) days for underweight to 2.9 (8.4) for obese) but neither BMI nor weight change were associated with mortality.
The majority of publications on COPD are on the undernourished, yet it would appear from this study that about half the outpatients with COPD seen in this Trust were overweight or obese. The effect of being overweight on patients with COPD deserves further study.
P45 BRONCHOSCOPIC LUNG VOLUME REDUCTION (BLVR) WITH ENDOBRONCHIAL VALVE IMPLANTS
T.P. Toma, N.S. Hopkinson, N. Shen, J. Hillier, P. Goldstraw, C. Morgan, D.M. Hansell, M.I. Polkey, D.M. Geddes. Royal Brompton Hospital, Imperial College, London, UK
Background: Surgical lung volume reduction (LVRS) can palliate symptoms in selected patients with advanced emphysema. We hypothesised that a similar effect could be achieved by blocking segmental bronchi leading to areas of bullous emphysema.
Aim: In this study we investigated the safety and efficacy of BLVR using the Emphasys™ valve implant and delivery system, in patients unsuitable for surgical LVRS.
Methods: Three male patients have undergone so far unilateral BLVR under general anaesthesia. Three valves were placed in each patient in the most affected lobe as evaluated on ventilation/perfusion scans and CT scans.
Results: See table. BVR was effective in shrinking emphysematous lung and expanding a collapsed lobe in one patient. The effect was sustained at one month follow up. Post procedure complications included: one pneumothorax at day 36 which resolved without drainage, and one COPD exacerbation at day 40 treated with antibiotics and steroids. None of the implants became dislodged.
Conclusion: This pilot study suggests that lung volume reduction can be achieved in humans with flexible bronchoscopy and specific valve implants. The implants are safe and easy to place and have the potential for extending indications and reducing morbidity, mortality and costs in patients with severe emphysema.
Sleep assessment and treatment
P46 AN ATTEMPT TO ASSESS THE DURATION OF PROBABLE MORBIDITY PRIOR TO THE DIAGNOSIS OF OBSTRUCTIVE SLEEP APNOEA SYNDROME (OSAS)
R. Ghiassi, M.R. Partridge. The Sleep Laboratory, Imperial College of Science, Technology and Medicine, NHLI Division at Charing Cross Hospital, London, UK
Recent work from Canada has suggested that hospital admissions and physician costs in the two years prior to diagnosis of OSAS was significantly higher in those with OSAS than in a control group.1 In the year prior to diagnosis it has also been shown that prescribed medication costs were significantly higher; medication being needed for hypertension, ischaemic heart disease, and congestive heart failure.2 The rate of road traffic crashes and occupational accidents is also higher amongst those with untreated OSAS.
To gain an insight into the duration of possible prediagnosis morbidity, we administered a questionnaire to 117 consecutive OSAS patients being treated with CPAP who attended this laboratory for review. Of these 107/117 (91.5%) reported that prior to diagnosis someone had complained about loud snoring and responders recorded that first mention of this had been a median of 12 years prior to diagnosis (range 2 to 47). Also 91/117 (77.8%) reported witnessed apnoea prior to diagnosis and this had been observed a median eight years prior to diagnosis (range 1 to 49). Ninety seven out of 117 (82.9%) reported sleepiness in the day time now or in the past and this had been present for a median of seven years (range 0.5 to 62 years). Seventy eight respondents were in employment and 37.2% of these reported having had two or more jobs in the last five years. Of the respondents, 85 were drivers and 21 of these (24.7%) reported having had a road traffic accident in the previous five years with five respondents having had two and one having had four such crashes. Overall these results suggest the likelihood of significant prediagnosis morbidity and greater public and primary care awareness of OSAS is needed.
1. Kryger M H, et al.
.
2. Otake K, et al.
.
P47 URINARY SYMPTOMS DO NOT CORRELATE WITH SEVERITY OF OBSTRUCTIVE SLEEP APNOEA OR COMPLIANCE WITH CPAP
K.E. Lewis1, A.J. Watkins2, L. Seale1, I.E. Bartle1, P. Ebden1. 1Prince Philip Hospital, Dafen, Llanelli, Wales, SA14 8QF, UK
Introduction: Studies have found increased urinary disturbance in patients with obstructive sleep apnoea (OSA). The reason remains unclear and may be due to in part to prostatic symptoms in middle aged men. We examined whether higher urinary symptom scores prior to treatment are correlated with more respiratory disturbance in OSA, and if more symptoms reduce compliance by interfering with machine use.
Methods: Seventy four consecutive males with OSA, mean (SD) age of 55.2 (9.0) years, mean BMI 34.5 (5.9), mean Epworth Sleepiness Score 15.4 (5.2), mean AHI 28.1 (22.8) per hour and mean 5% dip rate of 31 (21.7) per hour were prospectively studied. They completed the International Prostate Symptom Score and American Urological Questionnaire prior to CPAP therapy. Machine clock timers were hidden and machine on time was checked at one month. Correlations between the various subscores for urinary symptoms and measures of respiratory disturbance and machine on time were assessed using Spearman’s rho.
Results: Our patients had a mean Total Urinary Score of 5.72 (4.27), range 0 to 19. The correlation between Urinary Obstructive Scores and AHI was rho −0.229 (p=0.121). The correlation between Urinary Irritative Scores and AHI was rho −0.100 (p=0.506). The correlation between Urinary Total Scores and AHI was rho −0.197 (p=0.185).
Machine on-time was correlated to Urinary Obstructive Scores with rho −0.221 (p=0.301) to Urinary Irritative Scores with rho −0.030 (p=0.798) and Total Urinary Scores rho 0.032 (p=0.790).
Conclusion: Patients with OSA have Urinary Scores similar to the normal population as measured by standard urology tools, and any increased urinary disturbance, prior to CPAP is not significantly correlated with either the respiratory disturbance or reduced compliance with CPAP.
P48 APOLIPOPROTEIN E: A ROLE IN SLEEP DISORDERED BREATHING?
R.L. Riha, P. Brander, M. Vennelle, N.J. Douglas. Dept of Medicine, University of Edinburgh, Royal Infirmary, Edinburgh
Apolipoprotein E e4 (Apo E e4) is an important risk factor for the development of early onset Alzheimer’s disease, as well as being an independent risk factor for cardiovascular disease. A recent study by Kadotani et al1 demonstrated a correlation of Apo E e4 with a higher apnoea/hypopnoea index in a population with sleep disordered breathing (SDB). The aim of our study was to examine the distribution of Apo E alleles and genotype in patients in the UK with SDB compared to controls.
Method: A case control study was undertaken from 1997–2002. One hundred consecutive patients with SDB were recruited randomly from the clinic register. Each case was matched to a sibling. All cases and controls were asked to complete a self administered questionnaire and underwent clinical examination. All subjects underwent routine PSG or home monitoring. Studies were scored manually. All subjects had 20 ml of blood taken. Genotyping was performed on DNA extracted from peripheral blood lymphocytes using PCR-RFLP with polymorphisms for the three Apo E alleles determined according to published techniques.
Results: Results for 38 matched pairs are presented. Male:female ratio was 46:30. Mean age did not differ significantly between index patients and siblings (50.5 (SD)(8) v 60 (10)) nor did BMI (27 (2) v 28 (4)). AHI was significantly higher for cases (41 (IQR 27–52) v 13 (IQR 10–20). There was no significant difference in the distribution of either alleles or genotypes of Apo E between cases and controls (genotypes shown). See table.
The K statistic for alleles between cases and controls was 0.35 (p<0.0001) and for genotypes was 0.32 (p=0.002). Allelic frequency in the population was equivalent to that of the UK population: E2 (0.13); E3 (0.71); E4 (0.16).
Discussion: There is no difference in distribution of Apo E alleles and genotypes between subjects with SDB and their siblings. Our results are supported by two other studies looking at Apo E in relation to SDB.2 3 Further samples will be genotyped both for Apo E and other candidate genes in this ongoing study.
Acknowledgements: nursing staff & technicians of the Scottish National Sleep Laboratory; Dr N McArdle; Genetics Core, Wellcome Trust Clinical Research Facility, Edinburgh.
Supported by: Helen Bearpark Scholarship; AFUW fund; ERS LTT fellowship.
1.
.
2.
.
3.
.
P49 REACTION TIME (RT) TESTS IN OBSTRUCTIVE SLEEP APNOEA (OSA) AND NARCOLEPSY PATIENTS: THE PSYCHOMOTOR VIGILANCE TASK (PVT) IS A BETTER DISCRIMINATOR THAN THE SIMPLE UNPREPARED REACTION TIME (SURT)
D.C. Randall, S.N. Pilsworth, M.A. King, J.M. Shneerson, I.E. Smith. Papworth Hospital Sleep Centre, Cambridge, UK
RT tests are commonly used to assess performance of patients with sleep disorders and healthy subjects who undergo sleep deprivation but it is unclear which is most suitable for use in the clinical setting as an additional tool for assessing the effectiveness of treatment. The aim of this study was to compare the performance of four groups: healthy volunteers, treated narcolepsy patients, OSA patients treated with nCPAP, and untreated OSA patients (desaturation index = 15, Epworth Sleepiness Scale score = 10) on two different tests of sustained attention used in our lab: the PVT and the SURT.
Methods: Subjects completed the 10 min tasks in the afternoon, in random order. Subject demographics are presented in the table.
Results: One way ANOVA showed that there was a significant difference between the four groups on PVT slope (time on task decrement) (F(3,48) = 6.3, p<0.005). Bonferroni post hoc tests revealed that both narcolepsy and untreated OSA patients showed more reaction fatigue—that is, an increase of reaction time over time—on this task than did healthy volunteers (p<0.01). Mann-Whitney tests also revealed significant differences between the groups on SURT mean RT and number of gaps. These were due to narcolepsy patients having slower reaction times and a greater number of gaps (RT > 1s) (for both, p<0.05) than both healthy volunteers and treated OSA patients. There were no significant differences between the untreated OSA patients and the other groups on this task.
Discussion: Despite treatment, narcolepsy patients showed impairments on both tasks of sustained attention. Unlike the PVT, the SURT did not distinguish between untreated patients with OSA and healthy volunteers or those on nCPAP and may not be appropriate to follow treatment effects.
P50 ANALYSIS OF SLEEP STAGE USING A NEURAL NETWORK: COMPARISON TO MANUAL SCORING IN PATIENTS WITH OBSTRUCTIVE SLEEP APNOEA (OSA)
F. Buchanan, N. Wiltshire, J.R. Catterall A.H. Kendrick. Sleep Unit, Dept Respiratory Medicine, Bristol Royal Infirmary, Bristol, UK
Sleep is a continuum, often with short 2–3s events. Traditional scoring using Rechtschaffen & Kales (R&K) uses multiple channels and assigns one of seven sleep stages to each 30s epoch with further analysis for arousals. Neural net analysis uses 1s epochs and analyses sleep using one EEG channel, assigning a probability of a sleep stage to each epoch.
Aim: To compare R&K scoring to neural net in patients with OSA.
Methods: Patients underwent one night’s full polysomnography (SleepLab 1000e, Jaeger). A single scorer manually scored the study using R&K and American Sleep Disorders Association arousals criteria. Data files were converted into European Data Format (EDF) and analysed using a neural network (Bio Sleep v4.0, Oxford BioSignals) using a single EEG channel. Median filter was set to 15s and a threshold of 0.25 was used to score arousals, which had a minimum duration of 3s. Data are median (range).
Results: Twenty two patients (two female) were compared. Median Apnoea index was 2.45 (0 to 67.1) and Apnoea-hypopnoea index was 16.6 (0.7 to 93.2). The conversion to EDF took 40 mins and analysis 15 mins, as against a median of 120 mins using R&K. The EEG analysis is summarised below (see table).
Conclusion: The differences observed between R&K and Neural Net reflect the shorter epoch analysis time of 30s against 1s. Neural network analysis provides (1) a simple computerised scoring of overnight sleep studies; (2) a more sensitive analysis of the sleep continuum, and (3) reduces the overall time of analysis of sleep studies as compared to R&K.
P51 COMPARISON OF R&K AND BIOSLEEP SYSTEMS FOR ANALYSIS OF OBSTRUCTIVE SLEEP APNOEA
F. Diamantea, P.P. Walker, S. Lowe, D. Barr, T. Mckown, P.M.A. Calverley. Department of Medicine, University Hospital Aintree, Liverpool, UK
At present the gold standard in the objective assessment of sleep apnoea is still polysomnography with data analysis using the Rechtschaffen & Kales (R&K) guidelines for 20–30 second sleep epochs. This is time consuming, expensive and relates poorly to symptoms. An attractive alternative based on neural net technology is the BioSleep system. It is a single channel method, which provides second by second measurements and classifies sleep as awake, light or deep using probability assessment rather than the traditional 6–7 point staging system. This may provide better analysis of microarousals and also shortens technician analysis time to less than five minutes.
We compared BioSleep to R&K analysis using the same data set from 28 patients with moderate or severe OSA (Mean AHI = 52.4 (SD 18.4)) during split night polysomnography in which therapeutic CPAP was administered for half the night. BioSleep (B) was as good as R&K (R) at detecting differences between CPAP and air in terms of arousals (B: 44 v 80; p<0.001, R: 51 v 79; p<0.02), arousal index (B: 12 v 22; p<0001, R: 18 v 29; p<0.005), deep sleep % time (B: 30% v 8%; p<0.0001, R: 24% v 7%; p<0.0001) and light sleep % time (B: 70% v 92%; p<0.001, R: 76% v 93%; p<0.0002). BioSleep found greater differences in number of awakenings (B: 24 v 36; p<0.02, R: 2.8 v 3.2; p=0.53) and total time awake (B: 0.9hrs v 1.27hrs; p<0.05, R: 0.46hrs v 0.35hrs; p=0.15) but was inferior at detecting differences in sleep onset latency (B: 0.12 v 0.14; p=0.80, R: 0.26 v 0.10; p<0.001). BioSleep gave a more detailed picture of sleep architecture that was clearly different with therapy. Direct comparison showed that BioSleep predictably scored more awakenings and less total sleep time and sleep maintenance efficiency but there were no significant differences in % light or deep sleep, number of arousals or arousal index.
BioSleep is a method of sleep analysis comparable to R&K for several important parameters. While not replacing R&K for investigation of REM related and complex sleep disorders BioSleep provides additional information compared to R&K while shortening analysis time and this makes it an attractive analysis method for more widespread use.
P52 THE EFFECT OF RECORDING SITE IN ACOUSTIC ANALYSIS OF SNORING
M.J. Drinnan1, A.M. MacDonald1, M. Reda2, J.A. Wilson2, G.J. Gibson3. Departments of 1Medical Physics; 2ENT surgery; 3Respiratory Medicine Freeman Hospital, Newcastle upon Tyne, UK
Introduction: Several groups have investigated acoustic analysis of snoring, in order to investigate the mechanism of snoring, to distinguish obstructive sleep apnoea from non-apnoeic snoring and to predict the outcome of corrective surgery. However, the recording site has varied, and it is not known how this affects the acoustic parameters measured.
Methods: We studied 47 subjects prior to laser-assisted palatoplasty for severe snoring. All underwent preoperative polysomnography and patients with AHI > 25/h were excluded. Sound was recorded continuously from a throat microphone and an external microphone 1m above the patient’s head. We analysed all snores, defined as sound level peaks during sleep, lasting 0.1 to 3 seconds, and at least 45dBA in amplitude measured 1m above the patient’s head, and calculated three acoustic parameters for each snore: centre frequency, SD frequency (a measure of spread about the centre frequency) (
), and peak factor ratio (the ratio of peak to RMS sound energy) (
). For each subject we calculated the mean value for each of the three parameters, for the external and throat microphones separately.
Results: We analysed an average of 1018 snores per subject. The mean values for each acoustic parameter are given in the table.
Discussion: Clearly, the recording site has a profound influence on the acoustic qualities of snoring sounds. In particular, frequency-domain indices (centre and SD frequency) are affected, implying the throat microphone preferentially attenuates the higher frequencies.
Conclusion: When performing acoustic analysis of snoring sounds, it is essential that the recording site is selected with care.
Acknowledgements: We wish to than the British Lung Foundation for their financial support of this work.
P53 EFFECTS OF SIMULATED OBSTRUCTIVE APNOEA ON THE CAROTID BARORECEPTOR: VASCULAR RESISTANCE REFLEX
C.M. Bowker, V.L. Cooper, S. Davis, S.B. Pearson, M.W. Elliott, R. Hainsworth. Leeds University Teaching Hospitals, Leeds, UK
Obstructive sleep apnoea may lead to hypertension. This study was designed to determine whether the changes in inspiratory pressure and the asphyxia that occurs in this condition can change the gain and/or setting of the carotid baroreflex to maintain arterial pressure at a higher level.
In eight healthy subjects (aged 21–62) we changed the stimulus to carotid baroreceptors using a neck chamber and graded pressures of −40 to +60 mmHg and assessed vascular resistance responses in the forearm from changes in the blood pressure (Finapres) divided by brachial flow velocity (Doppler ultrasound). Stimulus response curves were defined during (a) sham (no additional stimulus), (b) inspiratory resistance (∼10 mmHg), (c) breathing asphyxic gas (12% O2, 5% CO2), and (d) resistance and asphyxia. Sigmoid functions were applied to the curves and the maximal differential (equivalent to peak gain) and the corresponding carotid pressure (equivalent to “set point”) were determined.
The sham test had no effect on either the gain or the “set point”. Inspiratory resistance alone had no effect on blood pressure. However it reduced the gain from −3.0 (0.6) to −2.1 (0.4) units (p<0.5) but the curve was not displaced. Asphyxia alone increased blood pressure (+7.0 (1.1) mmHg, p<0.0005) and displaced the curve to higher pressures by +16.8 (2.1) mmHg (p<0.0005) but had no effect on gain. The combination of resistance and asphyxia both reduced gain and displaced the curve to higher pressures.
These results show that inspiratory resistance decreases the gain of the baroreceptor reflex and in combination with asphyxia also shifts the curve to higher blood pressure levels. If these changes were sustained, they would provide a mechanism to link hypertension with obstructive sleep apnoea.
P54 PREVALENCE OF SLEEP DISORDERED BREATHING IN PATIENTS WITH CONGESTIVE HEART FAILURE
A. Rashid, J. Chambers, A.J. Williams. Sleep Disorders Centre and Dept of Cardiology, St. Thomas’ Hospital, London, UK
Introduction: Despite recent advances in medical and surgical therapy, congestive heart failure (CHF) remains a common and serious condition. CHF has been associated with sleep disordered breathing (SDB) in 51% patients (
), including Cheyne-Stokes respiration (CSR) in 40%, and obstructive sleep apnea (OSA) in 11%. SDB is associated with frequent arousals, leading to a persistent activation of the sympathetic nervous system and elevation of catecholamines with deleterious effects on left ventricular function. Heart rate variability (HRV) is considered to be a surrogate for arousals and serves as an independent prognostic indicator for cardiovascular events (Narkiewicz et al.
).
Methods: Patients suffering from CHF were selected on the basis of echocardiographic findings of ejection fraction (EF) less than 35%. We contacted 72 patients by letter, out of whom 36 patients (32 male and four female) agreed to participate in the study. Patients were sent portable pulse oximeters with a digital probe to wear overnight. The oximeters returned were studied for episodes of desaturations, and an oxygen desaturation index (ODI) was calculated. Desaturations were defined as dips in oxygen saturation greater than 3% and SDB was defined as an ODI greater than five.
Results: The overall prevalence of SDB in CHF patients was found to be 47.2% (17/36) and the mean ODI amongst these patients was 22.2/hr. The prevalence in patients with an EF less than or equal to 25% was 53.8% (7/13) with a mean ODI of 26.2/hr, whereas in patients with an EF between 25% and 35%, it was 43.5% (10/23) with an ODI of 19.5/hr. Increased heart rate variability was noted but was not found to correlate with SDB in our study. Twenty four out of 36 patients had increased HRV associated with concomitant dips in oxygen saturation in only 13. The remaining 11 patients having no SDB as defined here and raising the question as to additional burden of “subclinical” respiratory disturbance.
Conclusion: Our study confirms that nearly half the patients affected by CHF, even in stable condition, have severe nocturnal respiratory disturbances, which increase with increasing severity of CHF.
P55 IS MORE CPAP BETTER IN CLINICAL PRACTICE IN THE MEDIUM/LONG TERM?
E. Morrish, S.N. Pilsworth, M.A. King, J.M. Shneerson, I.E. Smith. Papworth Hospital, Cambridge, UK
Background: In a trial setting, hours of continuous positive airway pressure (CPAP) use by obstructive sleep apnoea (OSA) patients is correlated with the fall in subjective sleepiness at one month.(1) Our aim was to examine this relationship in a clinical setting after a longer follow up.
Methods: A retrospective review of patients who (a) were diagnosed with OSA according to the criteria as in(1) (oxygen desaturation >4% index (DI) ≥10/hr and Epworth Sleepiness Scale (ESS) score ≥10); and (b) were started on CPAP in the year 2000 and continued to use it for an average of ≥1 hour each night after ≥100 days. Correlation was assessed using Kendall’s tau_b coefficient.
Results: One hundred and three subjects (82 male) met the study criteria (table). Hours of CPAP use per night and change in ESS were not significantly correlated (r = −0.094; p=0.170).
Study group baseline demography and outcome measures
Discussion: In a month long trial setting only 4% of subjects withdrew from using CPAP.(1) In our experience approximately 15–20% discontinue CPAP in the long term. Those who use CPAP very little and gain no benefit will increase the correlation between hours of CPAP use and change in ESS early on. After a longer period of time these people have stopped using CPAP. The hours of use of long term compliers with CPAP may be more dependent on intrinsic sleep requirement, the benefits gained from decreased snoring and the level of belief in a decreased risk from cardiovascular events rather than a simple relationship with perceived change in daytime sleepiness.
1.
.
P56 TREATMENT OF SLEEP APNOEA/HYPOPNOEA SYNDROME (SAHS): A RANDOMISED TRIAL OF STANDARD CARE VERSUS ENHANCED NURSE INTERVENTION IN A DISTRICT GENERAL HOSPITAL
S. Palmer1, S. Selvaraj1, C. Dunn1, L.M. Osman2, J. Cairns3, D. Franklin4, G. Hulks4, D.J. Godden1. 1Highlands and Islands Health Research Institute; 2University of Aberdeen; 3Health Economics Research Unit; 4Highland Acute Hospitals NHS Trust
Background: Patients commencing CPAP therapy in Inverness (DGH) undergo a hospital titration study, telephone nurse review at four days and consultant review at six weeks (standard care). A study carried out at the Scottish National Sleep Laboratory found that enhanced nurse intervention after diagnosis improved outcome after CPAP therapy (
). Our randomised trial compared impact of standard care versus an enhanced nurse intervention on symptoms and quality of life in patients treated in the DGH setting.
Methods: Seventy consecutive SAHS patients were randomised to receive standard care (SC, n=35) or standard care plus a specialist nurse home visit at seven days (HV, n=35). Patients completed a symptom score, Epworth score, Hospital Anxiety and Depression Score (HADS), and SF-36 at baseline and three months after initial review. CPAP hours of use were recorded.
Results: CPAP therapy resulted in significant improvements in symptoms, Epworth, HADS (table), and in the energy/vitality and mental component summary scores of the SF-36 in both groups. There was no difference between groups in any outcome measure or in hours of use of CPAP.
Conclusion: CPAP led to marked improvement in patients with SAHS treated in the DGH setting. There was no difference between our two groups, both obtaining a similar magnitude of improvement to that reported in the enhanced care group from the National Sleep Laboratory.
Funded by the William Sutherland Trust.
P57 CONTINUOUS POSITIVE AIRWAYS PRESSURE (CPAP) TREATMENT CAN REDUCE ANXIETY AND DEPRESSION IN OBSTRUCTIVE SLEEP APNOEA
K.E. Lewis1, A.J. Watkins2, L. Seale1, I.E. Bartle1, P. Ebden1. 1Prince Philip Hospital, Dafen, Llanelli, Wales SA14 8QF; 2EBMS, University of Wales Swansea, Swansea, Wales SA2 8PP, UK
Introduction: We tested the hypothesis that CPAP treatment will improve anxiety and depression scores and if effects are correlated to machine use.
Methods: Eighty consecutive patients (74 male), age 51.2 (9.7) (mean (SD)) years, mean BMI 35.5 (5.7), mean Epworth Sleepiness Score 14.4 (5.2), mean AHI 25.1 (22.8), and mean 5% dip-rate of 31 (21.7) per hour, were prospectively studied. They completed the Hospital Anxiety and Depression Score at autotitration and after approximately one month of treatment with CPAP. Clock timers were hidden and machine “on time” was recorded at one month as a surrogate marker for machine use.
One sample t tests assessed if change in anxiety and depression were statistically significantly different from zero. Pearson’s correlation assessed the relationship between “on time” and changes in HAD scores.
Results: Patients were followed for a mean of 33.7 (13.4) days. Data was available on 70 patients. No patients reported life events or medication changes over this period. The mean anxiety score fell from 7.8 (3.7) to 6.3 (4.2) and the mean value for depression fell from 6.0 (3.7) to 4.9 (3.4) post treatment. Test statistics are −4.03 and −4.11 for hypotheses of zero change in anxiety and depression, respectively; p<0.001 in both cases. Pearson’s correlations between change in anxiety and depression with machine use are r= −0.297 (p=0.012) and r = −0.382 (p=0.001), respectively.
Conclusion: OSA patients have similar anxiety and depression scores to the normal population but there were statistically significant improvements in both scores after only a short period of treatment. We conclude that CPAP has a graded effect, with the greatest benefits observed in those using their machines the most.
Lung cancer
P58 OUTCOME OF A CODED X RAY SYSTEM TO FACILITATE REFERRAL OF CASES OF SUSPECTED LUNG CANCER
J. Hughes, C. Garvey, C. Smyth, M.J. Ledson, M.J. Walshaw. Liverpool Lung Cancer Unit, Royal Liverpool University Hospital, Liverpool, UK
Chest radiography is an important investigation in patients with persistent chest symptoms, and can be an early indication of malignant disease. This is of particular importance when the x ray abnormality is an incidental finding, for example on a preoperative routine film. In order to ensure the rapid investigation of patients with suspected lung cancer, we have introduced a coded x ray reporting system for chest x ray taken in Liverpool, including those performed in the community. When lung cancer is suspected, the reporting radiologist codes the report accordingly and the result is faxed to the relevant clinician, with a suggestion that the patient is referred to the rapid access service. In addition, all reports are electronically sent to the lung cancer specialist nurse, who monitors the referrals and ensures that the clinician acts on the report. We have audited the outcome of the first 477 patients in whom the radiologist flagged as suspected lung cancer using this coding system. Two hundred and fifty six were GP requests; nine of these were subsequently admitted to hospital, 215 were referred to the rapid access outpatient service, 24 were referred to a chest outpatient clinic, and eight refused further investigation. Within the secondary care sector, 206 were taken: 41 were admitted from the A&E department, one was a clinic attendee, and 164 were inpatients of whom 74 were discharged to attend the rapid access outpatient service. Eight of the latter group were surgical patients in whom the finding of a suspicious x ray lesion was incidental. In the remaining 15 cases, further investigation was not deemed necessary by the supervising clinician. Mean time from chest x ray to attendance at the rapid access outpatient clinic was 14 days, and mean time from referral to first appointment was 8.5 days. Overall 268 patients (56%) were subsequently diagnosed with lung cancer. Thus, we have shown that this x ray coding system allows the rapid access of patients with suspected lung cancer to the relevant service. Furthermore, processing the reports through the dedicated lung cancer nurse acts as a safety net and ensures that cases are not missed by busy clinicians. We recommend the use of such coding systems to clinicians charged with providing rapid access lung cancer services.
P59 AVOIDING LATE PRESENTATION OF LUNG CANCER: A PROACTIVE APPROACH TO MANAGEMENT OF ABNORMAL CHEST RADIOGRAPH REPORTS
J. Brown, P. Murphy, A. Bramwell, J. Wide, J. Corless, J. Hendry. St.Helens and Knowsley Hospitals NHS Trust, Whiston Hospital, Warrington Road, Prescot, Merseyside L35 5DR, UK
Late presentation with lung cancer may preclude radical treatment. System breakdowns may result in abnormal chest radiograph (CXR) reports not reaching the necessary clinician or being acted upon. In January 2000 we introduced a more pro-active approach to the handling of CXR reports that raise the possibility of lung cancer via a “failsafe” system. In partnership with our radiologists a coding system was used for CXR’s requested both from primary and secondary care. CXR’s with features strongly suggestive of a bronchial neoplasm were coded “TCXX” by the radiologist. Where neoplasia could not be excluded, a repeat film after 4–6 weeks was advised and a “TPXX” coding was given. All abnormal reports were immediately forwarded to the lung cancer team. Typically we would contact the patients’ GP by telephone to discuss the report and requested an urgent referral from the GP. We later audited all new patients attending our rapid access lung cancer clinic over a one year period to assess the impact of this system.
Results: The codes were initially not applied to all abnormal CXRs, especially by trainee and locum radiologists. Of 228 new patients seen, 102 (45%) had CXRs coded TCXX/TPXX and 126 (55%) had abnormal CXRs with no coding. The percentage of patients later confirmed to have lung cancer were: TCXX (71%), TPXX (23%), and no code (63%). The mean (range) time from day of CXR to clinic attendance was 8.5 (1 to 21) days in the TCXX group and 16 (1 to 162) days in the no code group (p<0.001). A survey of 66 local GPs found that 86% felt that the failsafe system was helpful and should be continued. A recent re-audit has found that 69% of abnormal CXR’s now receive the appropriate code.
Conclusions: A “failsafe” chest radiograph system is an effective tool that helps to ensure that patients with lung cancer are seen promptly and do not “slip through the net”.
P60 COMPULSORY REFERRAL FOLLOWING ABNORMAL CHEST X RAY VERSUS CHOICE
S.M. Jones1, J. Hammond2, A. Dunn2, A. Healey2, I. Ryland1, J. Curtis2, C.J. Warburton1, J.E. Earis1. 1Aintree Chest Centre; 2Department of Radiology, University Hospital Aintree, Liverpool, UK
The British Thoracic Society recommends that General Practitioners should immediately refer patients to a respiratory physician if a radiology report suggests the possible diagnosis of lung cancer (
). Some Units see such patients directly from the x ray department while others (including ours) rely on the patients GP to refer patients to the rapid access clinic.
An audit of 2369 reports from GP requested chest x ray, dating from 1st January to 28th February 2002 was conducted. In total, 63 reports were suspicious of malignancy. Of these, 40 advised referral to a chest physician, 16 advised computerised tomography (CT) scan, and seven did not give any advice. Of the 63 positive reports 48 were referred to a chest clinic (31 to the rapid access lung clinic and 16 to another chest clinic). Four patients were already under regular chest follow up and six were under the care of other physicians. Three patients had CT scan undertaken by the Consultant Radiologist and no further action deemed necessary. One patient was admitted via the Casualty Department because of symptoms and one elderly lady in a nursing home subsequently died without being seen. The time to being seen in a clinic ranged from zero to 49 days with a median of eight days.
We have found that only five patients were not referred to outpatients of whom three were investigated with CT directly by the x ray department. One of the remaining two patients presented with symptoms within two days to casualty and only one was missed (this was an elderly lady in a nursing home). Thus we have found that most patients with abnormal x rays are referred in a timely fashion but suggest that the x ray report should specifically suggest rapid access clinic referral. This system preserves both primary care and patient choice and prevents inappropriate referrals.
P61 EXPERIENCE FROM THE FIRST 24 MONTHS OF A FAST TRACK LUNG CANCER CLINIC
L. Dobson, D.M.G. Halpin, C.D. Sheldon, N.J.Withers. Royal Devon & Exeter Hospital, Exeter, Devon, UK
In May 2000 a dedicated Fast Track Lung Cancer Clinic was introduced at the Royal Devon & Exeter Hospital to facilitate referrals via the newly established two week wait (TWW) for suspected tumours. The clinic commenced as a weekly, Consultant provided service with the capability to see up to five urgent referrals weekly. General Pactitioners were informed about the new clinic by means of a letter, which also included local guidelines for referral via the “two week wait criteria”. Here we present an analysis of our experience over the first 24 months of this initiative.
A total of 378 new referrals were seen, with 180 (47.6%) of these being referred by the two week wait. Other referrals were via urgent GP letter (95), non-urgent GP letter (73), and Consultant referral (30). Of the TWW referrals seen, 169 (93.9%) were appropriate according to local guidelines and 100% of these referrals were seen within two weeks. Over the 24 month period the number of referrals via the TWW route has increased from 36 (1st six months of audit) to 64 (final six months).
Of the 378 patients seen in the FTLCC, 148 (39.1%) have been diagnosed with primary lung cancer or mesothelioma. A further 11 have been diagnosed with secondary cancer. Eighty eight (48.8%) of the TWW referrals had a diagnosis of primary lung cancer. Since the introduction of the TWW and the FTLCC there has been a sizeable decrease in the number of patients diagnosed as lung cancer following an emergency admission.
The establishment of a FTLCC has enabled us to fully achieve the TWW target. Referrals via the TWW are increasing and, in the main, are appropriate. The FTLCC may have reduced the number of patients admitted acutely with newly diagnosed lung cancer, but further follow up data will be required before this hypothesis can be confirmed.
P62 APPROPRIATENESS OF REFERRAL PATTERNS UNDER THE TWO WEEK RULE FOR LUNG CANCER
R.A. Heinink, H. Moudgil. Princess Royal Hospital NHS Trust, Apley Castle, Telford, UK
The Calman-Hine proposals for the management of lung cancer have forged the “two week rule” as the expected standard practice. Although many Trusts are able to meet these targets, less is known about the appropriateness of the actual General Practitioner (GP) referral patterns. This is particularly relevant against a background of direct or partial booking schemes for hospital appointments increasingly being made available to GPs. At this Trust, over a 12 month period to April 2001, there were 126 requests as possible lung cancer categorised under the two-week rule; 124 (98%) of these had been received centrally by the next working day and 121 (96%) had been offered outpatient appointments within the two weeks. At least 113 (90%) of these patients met at least one of the preset published criteria for respiratory referral. Four of the 13 inappropriate referrals were from one GP practice. Of the 126 referrals, for 92 the criteria were based on radiological abnormalities alone with similar numbers (both n=46) specifically prompted by the radiologists or on the GPs own initiative. Chest film changes accompanied 15 patients with haemoptysis and one had stridor. Haemoptysis alone was reported in six. Collectively, these two week rule referrals made up 48 (36%) of the 132 patients with diagnosed malignant disease presenting to the chest. A further 35 were diagnosed having been admitted acutely, 22 were detected at follow up clinics (including post admission), 15 were referred as routine whether by their GPs (n=9) or via other consultants (n=6), similarly nine others urgently outside two week rules by GPs (n=6) or via other consultants (n=3), and one patient remained with a non-respiratory physician throughout. Two others are undefined. Although we cannot presently comment on the patterns of referral of those outside the two week rule, this audit provides an insight into the appropriateness of two week referrals encountered here. It recognises the heterogeneous modes of presentation and referral but as expected singles out abnormal radiology as the main determinant. Importantly it also defines a large number (n=24) still electively referred outside the two week rule by both GPs and hospital teams. It concludes (1) that the majority (90%) referred under the scheme met the appropriate criteria for referral, (2) that only 48 (38 %) of these were then found to have malignant disease, and (3) that there are areas for improvement advising referral guidelines and timescales both within primary and secondary care.
P63 HAEMOPTYSIS IN PATIENTS WITH A NORMAL CHEST X RAY: CURRENT PRACTICE OF UK CHEST PHYSICIANS BASED ON A POSTAL SURVEY
N. McAndrew1, J. Woolley1, D.R. Baldwin2, A.L. Burton3. 1Wrexham Maelor Hospital, Wrexham, LL13 7TD; 2Nottingham City Hospital, Nottingham NG5 1PB; 3Royal Preston Hospital, Preston PR2 9HT, UK
Do patients who present with an isolated episode of haemoptysis and a normal chest x ray (CXR) need further investigation? If so, should this be with bronchoscopy (Br), computerised tomographic scan of the thorax (CT) or both? We sent a postal questionnaire to 610 UK chest physicians posing five clinical scenarios. The scenarios described patients with isolated haemoptysis and a normal CXR: a 35 year old never smoker (35NS); a 59 year old smoker with acute bronchitis (59S); a 70 year old smoker who had a violent coughing fit (70S); a 65 year old smoker with haemoptysis “out of the blue” (65S); a 70 year old never smoked (70NS). We received 291 replies (48%) (table).
Older patients and smokers are more likely to be investigated (p<0.0001, 35NS v 70NS; p<0.01, 70S v 70NS; χ2). A minority would not investigate minor haemoptysis occurring during acute bronchitis. CXR surveillance is more popular than CT alone (p<0.001;χ2). For smokers nearly 1/3 of respondents would rely on bronchoscopy alone. The most popular strategy employs both bronchoscopy and CT, (p<0.025, Br alone v CT & Br). The reliance on bronchoscopy alone is interesting as there is some evidence to suggest CT has greater sensitivity for picking up lesions not visible on CXR (
). CXR surveillance may have little benefit to the patient because it is less sensitive than either CT or bronchoscopy and because it will inevitably delay diagnosis. This survey has illustrated a lack of consensus in a difficult area of respiratory medicine.
P64 THE EFFECTIVENESS OF A LUNG CANCER MULTI DISCIPLINARY TEAM (MDT): A DISTRICT GENERAL HOSPITAL (DGH) EXPERIENCE
J.T. Samuel, S. Abubakar, A. David, K.J. Taylor, T.J. Charles. Glan Clwyd District General Hospital & The North Wales Cancer Center, Rhyl, Denbighshire LL18 5UJ, UK
Introduction: A number of strategies have been developed to combat lung cancer in the United Kingdom starting with the Calman Hine Report in 1995. The MDT approach incorporating various medical and paramedical specialities has been uniformly advocated to provide efficient and effective delivery of care. The effectiveness of the MDT approach has not been evaluated.
Aim: To assess the effectiveness of a lung cancer MDT in the management of lung cancer.
Methods: We audited the management of patients with lung cancer from Glan Clwyd DGH over a one year period before and after MDT was instituted at the North Wales Cancer Centre.
Results: See table.
Conclusions: In our audit, there were no significant differences in the diagnosis or treatment of patients after the formal MDT approach was adopted. More non-invasive investigations were performed and data collection was more extensive and structured. Further larger audits on the effectiveness of the MDT approach in lung cancer are required to determine if it indeed provides more effective delivery of care than previously practised.
P65 ANALYSIS OF HISTOLOGY RESULTS TO IMPROVE PROTOCOLS FOR THE DIAGNOSIS OF LUNG CANCER
S.M. Jones, P.P. Walker, I. Rylands, M. Babores, J.E. Earis, C.J. Warburton. Aintree Chest Centre, University Hospital Aintree, Liverpool, UK
There is still considerable variation in schematics for the management of pulmonary malignancies. This is particularly true for pleural disease where evidence is lacking. We looked at all 1012 cytological or histological assessments performed, in 654 patients referred between January 2000 and January 2001 with suspected pulmonary malignancy to produce local recommendations.
Pleural fluid cytology was analysed for diagnosis in 202 patients, of whom 48 had 2–4 samples taken. Twenty of 264 (9%) samples showed malignancy. In the 48 cases where a second sample was analysed only 3/48 were positive. In all three the initial result had been “suspicious or suggestive” of malignancy. Thirty eight sets of pleural biopsies were performed in 34 patients and 7/38(18%) showed malignancy. Twenty one patients with pleural effusions had a bronchoscopy. This was unhelpful in 18/21 irrespective of whether initial pleural cytology was reported as suspicious (7) or not (11). The 3/21 patients with diagnostic bronchoscopic abnormalities all had central abnormalities on CT.
At bronchoscopy where no lesion was visible 154 patients had a blind wash, brush biopsy or both. Eight of 154 (5%) had positive cytology and the addition of a brush biopsy increased the yield from 2% (2/92) to 11% (6/62). In 104 patients where a visible lesion was biopsied, an additional wash, brush biopsy or both increased the diagnostic yield by 6%—positive biopsy in 44 (42%), wash only in two (2%), brush only in three (3%), and wash and brush only in one (1%). Thirteen patients with a visible lesion and negative histology had a second bronchoscopy and 4/13 (31%) produced positive histology.
We recommend (1) Diagnostic rate for blind pleural procedures is small but significant. If initial pleural cytology is not “suspicious” further aspiration without biopsy is unhelpful. (2) Bronchoscopy should not be performed for undiagnosed effusions in the absence of central CT abnormalities. (3) If blind samples are taken at bronchoscopy then a wash and a brush should be performed. (4) Wash, brush biopsy, and bronchial biopsy should be performed for all visible endobronchial lesions. (5) Repeat bronchoscopy is a reasonable option in some patients although histology is obtained in <50%.
P66 RADICAL TREATMENT FOR NSCLC IN NORTHERN AND YORKSHIRE REGION
E.T. Peel, C. Bennett. North Tyneside General Hospital, Northern & Yorkshire Cancer Registry Information Service, UK
The casenotes of 400 consecutive patients with histologically confirmed non-small cell lung cancer (NSCLC) diagnosed in 1998 and registered with Northern and Yorkshire Cancer Registry Information Service (NYCRIS) database, were audited. The aim of the study was to determine the proportion of NSCLC patients receiving radical treatment (surgery or radical radiotherapy – dose ≥50Gy) and how they were assessed.
Data is presented on 368 patients (92%) in the table.
In patients not receiving radical treatment, the commonest reasons for those decisions were: advanced lung cancer (54%), died (18%), refused (13%), other disease (12%). The open and close rate was 8%.
We conclude that staging and performance status are not well documented, although the majority of patients have significant comorbid illness, the main determinant of suitability for radical treatment is the extent of the disease.
P67 LUNG CANCER IN WOMEN THROUGH THE 1990S
A. Bastin, D. Eraut, A. Davison, A.S. Haque, A. Hutchings, A. Lamont, C. Trask. Southend Associate University Teaching Hospital, Southend on Sea, Essex SSO ORY, UK
Lung cancer incidence is rising in females (F) and falling in males (M) in the UK. Smoking in young females increased in the early 90s. We have analysed the pattern of lung cancer in 2127 new cases (1421 M (67%) + 706 F (33%)) presenting over a 10 year period from 1990 to 1999 from the Southend Lung Cancer Study. This includes every case in a well defined population of 325 000. The mean age of F was 70.8 yrs (SD 10.3) and M 71.7 yrs (SD 9.7) (p<0.04)). There was a higher percentage of F never smokers (8.5%) compared with M (1.9%) (p<0.001). The proportion of never smokers was greater in elderly F compared to younger F (p=0.019). There was a higher percentage of M ex-smokers (60.2%) compared with F (51.1%) (p<0.001). There were 39.6% of F current smokers compared to 37.9% M (p=0.47). The proportion of current smokers falls with increasing age at diagnosis in both M and F (test for trend p<0.001).
We found a lack of evidence that the proportion of F to M had increased from 1990 to 1999 overall (test for trend p=0.3) nor in under 65s alone (p=0.151). In patients with confirmed squamous, adeno, or small cell histology (total 1342), there was an overall difference (p=0.001) in the proportion of histological types between M and F: squamous cell carcinoma 54% M v 41% F; adenocarcinoma 23% M v 28% F; small cell carcinoma 23% M v 31% F (χ2 p<0.001). Never smoking F were more likely to have adenocarcinoma than F who smoked (χ2 p<0.001). We found no evidence that the proportion of adenocarcinoma in smokers and never smokers changed over time in M and F (test for trend p=0.67). The proportion for M (10.5%) and F (8.9%) having either radical radiotherapy or surgery differed by 1.6% (95% CI −1.1% to 4.2%) (χ2 p= 0.26).
Conclusion: In comparing M and F with lung cancer through the 90s we have found: (I) F to be slightly younger than M; (ii) differences in histological types, with adenocarcinoma and small cell being more common in F and squamous cell carcinoma in M; (iii) more F never smokers; (iv) older F were more likely to be never smokers than younger F; (v) F never smokers were more likely to have adenocarcinoma than F smokers; (vi) no difference in the proportion of men and women presenting over time, and (vii) no evidence of a gender bias in those receiving “curative” treatment.
P68 LUNG CANCER IN OCTOGENARIANS, THE ROLE OF THE SURGEON
I.R. Ramnarine, S. Thomas, A.N.A. Jilaihawi, D. Prakash. The Department of Thoracic Surgery, Hairmyres Hospital, East Kilbride, Glasgow, G75 8RG, UK
Objective: To analyse the pattern of management of patients in their eighties referred to the surgeon with clinical evidence of lung cancer.
Methods: A retrospective series of 62 80 year old patients (42 males) with a clinical diagnosis of lung cancer referred to the surgeon over a 15 year period. The surgical management of these patients was reviewed.
Results: Pathological confirmation of tumour type was in 54 patients (87%) with 39 lung cancers (28 squamous cell, eight adenocarcinoma, one large cell, and one small cell carcinoma), seven diffuse malignant mesotheliomas, three metastases, and five other tumour types. Of the lung cancer patients, 10 had tumours that were unresectable (mean survival 8.4 months) and 29 had resectable lesions. Of the latter group, eleven patients had comorbid disease making them inoperable (mean survival 6.4 months). Eighteen patients had lung tumour resection. There were four pneumonectomies, 13 lobectomies, and one bilobectomy. Ten patients had stage 1, five had stage two, and three had stage 3a lung pathology. Operative mortality was 11% (two patients). One, two, and three year survivals were 72%, 64%, and 23% respectively. Four of the nine late deaths were from tumour spread and there are seven disease free survivors.
Conclusion: Age should not be a discriminating factor in determining operability in lung cancer patients. The surgeon plays an important role in the management of octogenarians with lung cancer offering a wide range of services from minor diagnostic procedures to definitive surgery.
P69 COPYING CORRESPONDENCE TO CHEST CLINIC PATIENTS: A SURVEY OF PATIENT VIEWS
S. Lohani, P.J. Sullivan, R. O’Driscoll, S.C.O. Taggart. Respiratory Department, Hope Hospital, Salford, M6 8HD, UK
Introduction: As part of the NHS plan to improve communication between health professionals and patients by 2004, it is expected that all future patients will receive copies of correspondence. It is likely that this directive will have important effects on the way in which providers deliver their service in addition to changing the way they relate to their patients.
Methods: From mid April to mid June 2002, we surveyed all patients attending our general respiratory clinics in addition to those visiting our dedicated Lung Cancer Clinic. Patients were asked to complete a self administered questionnaire with tick box format, designed to identify which patients wished to receive all or some copies of their correspondence and which patients preferred to receive no copies. The patient’s wishes were then recorded on their correspondence and letters were forwarded to the patients if required. Patients were requested to discuss any errors in their medications at their next clinic visit. Our medical secretaries recorded any incidents arising out of the introduction of this system. Patient preferences for receiving copies of correspondence at general respiratory and specialist lung cancer clinics (table).
Patient preferences for receiving copies of correspondence at general respiratory and specialist lung cancer clinics
A significantly greater proportion of patients attending our dedicated Lung Cancer Clinic preferred to receive no copies of correspondence than their general respiratory counterparts (27% v 14%, p=0.013 using Fisher’s exact test). Overall, 84% of our patients expressed a preference to receive copies of correspondence. Throughout the study period, no incidents were recorded bar one patient who wished to point out a medication error.
Conclusions: Based on our two month experience, we recommend caution for those planning to introduce copies of correspondence to all patients attending clinics as a small proportion would not wish to receive this. This proportion rises to almost a third for those patients attending Lung Cancer Clinics.
Lung injury, inflammation, and infection
P70 EPIDEMIOLOGY OF LUNG FUNCTION AND IMMUNOLOGY IN PIGEON BREEDERS: FIVE YEAR FOLLOW UP
T. Ismail, F. Boyd, C. McSharry, P. Lynch, C. Lynch, G. Boyd. Department of Respiratory Medicine and Immunology, North Glasgow University Hospitals NHS Trust, UK
Background: The immunopathogenesis of pigeon fanciers’ allergic alveolitis is unresolved. Most studies rely on subjects presenting at clinics and proper epidemiological evaluation is lacking. Changes in lung function, immunology, and associated symptoms among a cohort of pigeon fanciers were assessed.
Methods: Forty pigeon fanciers had serial lung function, serum antibody to inhaled avian antigens and symptoms monitored for five years.
Results: Between 1997 and 2002 there was a significant reduction in FEV1 (T = −2.87, p=0.007) and FEV1/FVC (T = −3.68, p=0.001). Twenty one subjects were seropositive in 1997 and a further four subjects showed evidence of new sensitisation in 2002 and there was no significant increase in the paired mean titre. The % predicted FEV1 correlated inversely with serum antibody titre (r = −0.380, p=0.019) and peripheral blood CD8 lymphocyte proportion (r = −0.319, p<0.05). The antibody titre also correlated inversely with the CD4:CD8 ratio (r = −0.325, p=0.014). Eleven subjects had symptoms of extrinsic allergic alveolitis in 2002 compared to 13 subjects in 1997.
Conclusion: Serial lung function in statistically determined cohort of pigeon fanciers seems to deteriorate significantly depending on the extent of the humoral antibody response to the inhaled antigens. These changes are associated with underlying immune dysfunction involving the imbalance of T-helper and T-cytotoxic lymphocytes. Subclinical inflammatory changes are common among pigeon fanciers and may be predictive of disease progression.
P71 SERIAL LUNG FUNCTION FOLLOWING PERIPHERAL BLOOD STEM CELL TRANSPLANTATION
L. Warren, L. Cormican, M. Gillion, D. Wilson, R. Freeman, S. Schey1, H. Milburn. Departments of Respiratory Medicine; 1Haematology, Guy’s Hospital, St. Thomas Street, London, SE1 7EH, UK
Background: Pulmonary function tests (PFTs) are an established tool in the prediction of respiratory complications following allogenic bone marrow transplantation (BMT) for haematological malignancy. Most of these patients are now managed with allogenic and autologous peripheral blood stem cell transplants (PBSCT), a procedure less toxic than BMT and thought to result in fewer pulmonary complications.
Methods: In this observational study we have followed serial pulmonary function tests in 70 patients up to 8½12 years following PBSCT for multiple myeloma (n= 35) and leukemia (n= 35, 43 % AML, 6 % ALL, 14 % CML, 37 % CLL) to determine whether there were any groups which were particularly susceptible to respiratory complications. The selection of CD34+ cells was performed in 22 cases during the harvesting of peripheral blood stem cells prior to transplantation.
Results: Over the duration of the study there was a notable decrease in TLCO (figure) and an increase in RV (non-significant) in those who received CD34 selected, in comparison to non-CD34 selected grafts.

Mean TLCO of CD34 and non-CD34 selected groups.
There was deterioration in lung function data (FEV1 and FVC) in the AML population in comparison to the combined PBSCT population.
Conclusion: Even though PBSCT is associated with fewer pulmonary complications, certain subgroups of patients are more prone to changes in lung function over time. This justifies the performance of serial lung function in these patients.
P72 LUNG REPAIR BY HAEMATOPOIETIC STEM CELLS (HSC) AFTER BONE MARROW TRANSPLANT (BMT)
S.M. Janes, T. Hunt, M. Brittan, R. Jeffery, S. Forbes, K. Hodivala-Dilke, M. Alison, N. Wright, R. Poulsom, M.J.D. Griffiths. Cancer Research UK, London WC2A 3PX, UK
Introduction: Recent data suggest that HSC contribute to repopulation of the pulmonary parenchyma after BMT (
;
). The aim of this study was to define in mice following BMT the phenotype and time course of the appearance of donor-derived cells in the pulmonary parenchyma.
Methods: Six week old female recipient mice were irradiated with 10 Gray as a split dose two hours apart to ablate their BM and then received male wild type whole BM by tail vein injection. Four mice were sacrificed at weekly intervals for six weeks and then at eight and 10 months. Lung sections were hybridised with FITC-labelled Y chromosome paint (Star-FISH, Cambio, Cambridge, UK) to detect cells of donor origin. For the mouse tissue we combined in situ hybridisation for the Y chromosome with immunohistochemistry for specific markers for macrophages, myofibroblasts, endothelial and epithelial cells.
Results: Y+ cells were widespread in the lung parenchyma a week after BMT, engraftment peaked between four and six weeks, and persisted for at least 43 weeks (figure). Y+ cells were absent from the airway epithelium and the endothelium of venules and arterioles. Y+ cells stained positively with epithelial cell markers T1α, Lectin lycopersicum esculentum, and CAM5.2.

Conclusions: Donor-derived HSC (Y+) cell’s morphology and staining suggests that they become part of the alveolar epithelium. The role of BM derived stem cells in lung repair is unknown but may be a novel target for manipulation or a means of delivering gene therapy to the distal lung.
SJ is supported by a training fellowship from the MRC UK.
P73 PERIPHERAL BLOOD CHANGES AND CRYPTOGENIC FIBROSING ALVEOLITIS. POSSIBLE MARKERS OF DISEASE?
V.A. Varney, D.T. Salisbury, H. Parnell. Department of Respiratory Medicine, St Helier Hospital, Wrythe Lane, Carshalton, Surrey SM5 1AA, UK
Background: Cryptogenic fibrosing alveolitis (CFA) is a disease associated with activated alveolar macrophages at broncho alveolar lavage. In the peripheral blood, autoantibodies and elevation of the ESR are common but not diagnostic. The prevalence of CFA has increased in the last decade providing more patients for studies.
We have observed a consistent feature (not yet described) of elevation in peripheral blood monocytes (MØ), mean red cell volume (MCV), and serum gamma glutamyl transferase (GGT). In all cases alcohol intake and drugs were excluded as a cause. Full liver function tests were otherwise normal along with vitamin B12 and folate levels. A bone marrow was examined in three cases confirmed a true macrocytosis without any other myelodysplastic features.
Methods: Ninety one patients (age 41–86 years) presenting with a new diagnosis of CFA had their baseline haematology and biochemistry studied. The results were compared with an age and gender matched reference range obtained from the same laboratory of non-CFA general population controls. The abnormalities at baseline were noted to be persistent throughout the patients treatments.
Results: See table.
Conclusion: Ninety one CFA patients showed a statistical increase in peripheral blood monocytes, MCV, and serum GGT. This observation requires further investigations and may represent a systemic disease with cytokine or other mediator effects on the bone marrow responsible for these changes.
P74 PULMONARY VASCULAR ENDOTHELIAL GROWTH FACTOR (VEGF) RECEPTOR EXPRESSION IN ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS)
A.R.L. Medford1, L. Armstrong1, N.B.N. Ibrahim2, K.M. Uppington1, A.B. Millar1. 1Lung Research Group, University of Bristol Division of Medicine, Southmead Hospital, Bristol, UK; 2Department of Pathology, Frenchay Hospital, Bristol, UK
Previous work in our laboratory suggested a role for VEGF (an angiogenic and permeability factor) in the pathogenesis of ARDS (
). VEGF receptors (VEGFR1, VEGFR2) are thought to be predominantly expressed in vascular endothelium and monocytes. Modulatory VEGF neuropilin co-receptors (NP1 and NP2) expression occurs in a variety of human tissues. The expression of these receptors in human normal and ARDS lung has not been extensively investigated. We hypothesised that there would be expression of these receptors on both sides of the alveolar-capillary membrane with significant upregulation in ARDS lung consistent with VEGF having a significant role. Immunohistochemistry was performed on post-mortem human lung sections from normal subjects and patients with late ARDS (n=4) using semiquantitative densitometric analysis via Histometrix software. RT-PCR was performed on cultured human type II alveolar cells (AE2), alveolar macrophages (AMs) and peripheral blood monocytes (PBMs) from normal subjects and ARDS patients. In normal lung, VEGF, VEGFR1 and VEGFR2 protein were expressed in vascular endothelium, alveolar epithelium, and AMs. NP1 and two were confined to the alveolar side. In late ARDS lung, there was significant upregulation of VEGF, VEGFR1, VEGFR2, NP1 but not NP2. NP1 and 2 expression was also evident on the vascular side of the alveolar-capillary membrane. RT-PCR confirmed VEGFR1, VEGFR2, and NP1 mRNA expression in AMs and AE2 cells. PBMs expressed only VEGFR1 mRNA. These data confirm the presence of VEGF receptors and co-receptors on the alveolar side of human lung in addition to the known vascular endothelial expression of VEGFR1 and 2. There is significant upregulation of these receptors in late ARDS consistent with VEGF having a significant role in ARDS on both sides of the alveolar-capillary membrane. The type 2 alveolar epithelial cell and alveolar macrophage appear to be additional targets for VEGF in human lung.
P75 VASCULAR ENDOTHELIAL GROWTH FACTOR ISOFORM (VEGF165b, VEGF165 AND VEGF189) EXPRESSION IN HUMAN AND MURINE INJURED LUNG
A.R.L. Medford1, L. Armstrong1, S. Godinho1, D.O. Bates2, S.J. Harper2, A.B. Millar1. 1Lung Research Group, University of Bristol Division of Medicine, Southmead Hospital, Bristol, UK; 2Microvascular Research Laboratory, Department of Physiology, University of Bristol, Southwell Street, Bristol, UK
Previous work in our laboratory suggested a role for VEGF in the pathogenesis of ARDS (Thickett DR, et al.
). However, VEGF is compartmentalised in normal human lung (Kaner RJ, et al.
). More recently, VEGF165b has been identified as an inhibitory splice variant found in a variety of human tissues including lung (Bates DO, et al.
). There is mounting evidence that the VEGF isoforms have different biological roles. We hypothesised that the VEGF165b would be significantly expressed in normal lung and that the distribution of the VEGF165b, VEGF165, and VEGF189 isoforms would be altered in acute respiratory distress syndrome (ARDS). Total RNA was extracted from cultured “normal” human type 2 alveolar epithelial cells (AE2, n = 4), as well as alveolar macrophages (AMs, n = 11) from normal subjects, at risk and ARDS patients. RNA was also extracted from C57BL/6 mice after lipopolysaccharide (LPS) induced lung injury (n = 9) and sham controls (n = 2). RT-PCR with VEGF isoform-specific primers was performed to assess VEGF165b, VEGF165, and VEGF189 mRNA expression. VEGF165b was expressed in all samples (n = 26). In injured murine lung, VEGF165 and VEGF189 were both expressed compared to only VEGF165 in normal murine lung. Seventy five per cent (n = 6) of samples expressing only VEGF165 were from normal lung. 75% (n = 12) of samples expressing both VEGF165 and VEGF189 were from injured lung. Expression of VEGF splice variants appears to be influenced by lung injury whereas the inhibitory splice variant is endogenously expressed in the lung. This may partially account for the high levels of compartmentalised VEGF in normal human lung. The relative expression of the inhibitory and the active isoforms may determine the functional role, in particular the pathogenic role of VEGF in ARDS. Further research is required to define the exact relative expression of these isoforms.
P76 AN AUDIT OF THE MANAGEMENT OF COMMUNITY ACQUIRED PNEUMONIA IN SOUTHAMPTON GENERAL HOSPITAL
S.K. West, S. King. Respiratory Department, Southampton General Hospital (SGH), UK
Introduction: The publication of the British Thoracic Society (BTS) guidelines into community acquired pneumonia (CAP) (
) prompted a review of clinical practices at Southampton General Hospital (SGH). The aim was to assess the present use of the core prognostic features outlined in the guidelines (confusion, urea, respiratory rate, and blood pressure) and their relation to management decisions.
Method: The patient group was all those admitted to SGH between September and November 2001 (inclusive) given the diagnosis of pneumonia on their discharge summary. Patients were then excluded according to the BTS exclusion criteria. The data was collected from the patients’ notes; specifically initial investigations, core prognostic features, severity of the pneumonia, antibiotic prescription, and patient outcome. The results were then compared with the guidelines and national statistics.
Results: Seventy three notes were obtained from 113 requested, of which 38 met the inclusion criteria. The main reason for exclusion was a recent hospital stay. The average age was 70 years and the length of stay nine days. Only seven patients had any documented assessment of severity, three of which were said to be severe. Subsequent use of information within the notes indicated that 45% could be classified as severe, 42% non-severe, and 13% mild. Measurement of core prognostic features varied, with blood pressure measured in 97% of cases, urea 82%, respiratory rate 74%, and mental test score 50%. Other problems with note keeping included minimal inclusion of radiographic results in the notes. The majority of antibiotic choices were appropriate in type but with 70% of first line antibiotics being given intravenously despite only 45% classifiable as severe. The overall death rate was 23.6% with three unrelated deaths. Two patients were subsequently changed to palliative management and four deaths were attributed directly to CAP. Thus the death rate from CAP was 10.5% with 89% of these initially graded as severe. 53% of all those graded as severe died.
Conclusions: There is presently minimal use of any formal severity assessment and a possible over reliance on intravenous antibiotics. This audit may provide a background on which to investigate the benefits of severity assessment forms in the care of all those admitted locally with possible CAP.
P77 STAPHYLOCOCCUS AUREUS CELL WALL DEFICIENT BACTERIA ARE HIGHLY RESISTANT TO CELL WALL ACTIVE ANTIBIOTICS AND HAVE AN ALTERED PROFILE TO OTHER CLASSES OF ANTIBIOTIC
C. Elmer , P. Cook , F. Nattress , P. Cheung2, T. Fawcett3. 1University Hospital of North Durham; 2Centre for Comparative Public Health, University of Durham; 3School Of Biological and Biomedical Sciences, University of Durham, UK
Background: Bacteria may lose all or part of their cell walls under certain environmental conditions, including the presence of cell wall-active antibiotics. Cell wall deficient bacteria (CWDB) are hard to detect by light microscopy or culture, but can proliferate in vivo and on specialised media. We investigated whether cell wall deficiency confers stable resistance to penicillin and its affect on the response to other antibiotics.
Method:Staphylococcus aureus cells were cultured in the presence of sublethal levels of penicillin G on various media, including one optimal for CWDB. Minimum inhibitory concentration (MIC) estimations were performed after three step increases in penicillin concentration and on cells that had been passaged in the absence of penicillin. Cells were examined by Gram staining and electron microscopy. Different strains of CWDB were subjected to disc diffusion tests for a range of other antibiotics.
Results: CWDB have a different colony morphology, stain Gram negative and have indistinct margins and altered cell morphology on electron microscopy. The MIC for penicillin increased following serial passages, particularly on CWDB optimal media (32 units/ml, compared with 1 unit/ml on DST medium, after 12 passages). After seven passages without penicillin the cell wall was regained, but penicillin resistance was maintained. CWDB were resistant to other cell wall active antibiotics. They also exhibited altered profiles in comparison to the wild type cells for erythromycin, trimethoprim, tetracycline, novobiocin, and nitrofurantoin.
Conclusion: In the presence of sublethal levels of antibiotics and media optimal for CWDB, S aureus rapidly develops a high degree of stable penicillin resistance. We propose that loss of the cell wall, though rarely demonstrated in clinical microbiology laboratories, is an important cause of antimicrobial resistance to cell wall active antibiotics. Surprisingly these cells show significant alterations in sensitivity to other classes of antibiotics too. This could have profound implications for antibiotic therapy.
P78 IgA1 PROTEASE FROM NON-TYPABLE HAEMOPHILUS INFLUENZAE CLEAVES TWO SITES IN HUMAN IgA1 HINGE REGION
D. Mistry, S. He, R.A. Stockley. Lung Investigation Unit, Queen Elizabeth Hospital, Birmingham, UK
Bacterial IgA1 proteases are thought to be important virulence factors in respiratory tract infections. This group of proteolytic enzymes specifically cleave one of several post-proline peptide bonds within the hinge region of human immunoglobulin A1.
We have partially purified an IgA1 protease with a different cleavage specificity, from a clinical isolate of non typable Haemophilus influenzae (NTHI), by anion exchange chromatography. Proteolytic assays were carried out with human IgA1, IgA2, and serum albumin. PCR of the NTHI genome was carried out with IgA1 protease sequence-specific primers to identify the gene(s) coding for the IgA1 protease(s) producing this cleavage pattern.
The protease specifically cleaved human IgA1 and did not cleave human IgA2 or serum albumin. However, the IgA1 protease cleaved more than one site within the hinge region of human IgA1. PCR amplification produced one IgA1 protease gene (iga) product. The PCR products contained homologous sequences to other iga genes of the serine-type IgA1 proteases and interspersed between these sequences were new deletions and insertions. The results indicate that the NTHI contains one iga gene sequence that encodes one IgA1 protease, which cleaves more than one peptide bond in the IgA1 heavy chain. The iga gene sequence may produce the unique cleavage specificity of the NTHI IgA1 protease and further work will require the identification of the residues essential for the IgA1 protease activity, to allow the design of specific inhibitors to this important class of proteolytic enzymes.
P79 ELEVATED NASAL NITRIC OXIDE CORRELATES WITH REDUCED NASAL MUCOCILIARY CLEARANCE IN BRONCHIECTASIS
A. Shoemark, S. Kharitonov, P. Barnes, R. Wilson. Host Defence Unit, Royal Brompton and Harefield NHS Trust and National Heart and Lung Institute, Imperial College of Science Technology and Medicine, London, UK
Effective mucociliary clearance (MCC) is an important first line host defence against infection. Nitric oxide (NO) is also thought to aid in host defence through its antibacterial properties and by increasing ciliary beat (Runer et al. 1998). NO is upregulated in the presence of infection and inflammation (Kharitonov et al. 1995). The aim of this study was to establish the relationship between nasal MCC and NO in patients with bronchiectasis, a disease associated with impaired host defence and inflammation.
Nasal MCC and NO were measured in 30 non-smoking subjects with stable bronchiectasis confirmed by CT scan, age 25–82 yrs mean 57, male (11), and eight control subjects with no respiratory problems. Eight patients regularly used nasal corticosteroids. Subjects with cystic fibrosis or primary ciliary dyskinesia were excluded as nasal NO is known to be low. NO was measured directly from the nostril during a breath hold using a chemiluminescence analyzer (LR2000 Logan research ltd. Rochester, UK). Three patients could not hold their breath for long enough for the test to be performed correctly. Nasal MCC time was measured by the saccharin test.
In bronchiectasis subjects without nasal corticosteroids, nasal NO was significantly (p<0.05) elevated in patients (n=6) with nasal MCC >60 minutes, mean 658ppb (SD 186), compared to patients (n=13) with nasal MCC =60 minutes, mean 402ppb (180), and controls, mean 418ppb (136). There was a correlation between nasal MCC and NO in patients with clearance = 60 minutes. r = 0.6, p<0.05. Although no significant difference in NO was found between subjects with no nasal corticosteroids and patients regularly taking nasal corticosteroids, in subjects regularly taking nasal corticosteroids there was no correlation between nasal MCC and NO.
In conclusion nasal NO is elevated in bronchiectasis patients with delayed nasal mucociliary clearance. This finding may be due to increased inflammation in the upper respiratory tract. Delayed clearance occurs despite any increase in ciliary beat that might occur with increased NO.
P80 STUDY OF EXHALED NITRIC OXIDE IN STABLE BRONCHIECTASIS
L.J. Ozerovitch, A. Shoemark, S. Kharitonov, P. Barnes, R. Wilson. Host Defence Unit, Royal Brompton and Harefield NHS Trust and National Heart and Lung Institute, Imperial College of Science Technology and Medicine, London, UK
We have previously shown that nitric oxide (NO) is elevated in some patients with stable bronchiectasis, but in others levels are normal. Exhaled NO levels are high along with systemic markers of inflammation (CRP and peripheral blood neutrophil count) during an exacerbation and fall after antibiotic therapy. These results suggest that NO is a marker of lung inflammation. The present study was conducted to compare those patients with elevated NO when stable to those with normal levels.
Twenty three patients with bronchiectasis shown on CT scan underwent a protocol of investigation which included full lung function tests, sputum examinations, blood investigations, ciliary studies, sweat test, shuttle walking test, and St George’s Respiratory Questionnaire (SGRQ).
There was no relationship between NO and walking distance nor any component of the SGRQ. There was also no relationship between NO and extent of bronchiectasis on CT scan, blood inflammatory markers, sputum bacteriology, sputum eosinophil count, nor any lung function parameter. There were correlations between gas transfer (% predicted) and walking distance (p<0.05); walking distance and CRP (p<0.05); gas transfer (% predicted) and Total SGRQ (p<0.05); walking distance and Total SGRQ and also the Activities component (p<0.004); and Total SGRQ and FEV1 (% predicted) (p<0.05).
In conclusion we do not know why some patients with stable bronchiectasis have elevated exhaled NO. We are continuing to study more patients using the same protocol, and also carrying out a more detailed analysis of the CT scans—for example, airway wall thickness—and a long term study to see if elevated NO influences the subsequent clinical course.
P81 CHILDHOOD ASTHMA IN THE HIGHLANDS OF SCOTLAND: MORBIDITY AND SCHOOL ABSENCE
J.B. Austin1, S. Selvaraj2, G. Russell3. 1Highland Primary Care NHS Trust; 2Highlands and Islands Health Research Institute; 3University of Aberdeen, UK
Background: The prevalence of childhood asthma in Scotland is one of the highest in the world. Allergic diseases may cause significant morbidity. The aims of this study were to describe the prevalence of asthma, eczema, and hay fever in the Highlands of Scotland and in the Shetland Isles and to examine factors in relation to quality of life and social deprivation.
Methods: A total population survey of 12 year old children using a parent completed questionnaire.
Results: 86.3% (2658/3080) returned questionnaires. Of the 2549 questionnaires analysed, 476 (18.7%) reported asthma, 362 (14.2%) wheeze in last 12 months, 508 (19.9%) hay fever, and 555 (21.8%) eczema. Of the children reporting asthma or wheeze, 35.4% (229/647) had missed school because of asthma or wheeze, 38.0% (246/647) had missed physical education. Of subjects with lifetime wheeze, 62.5% (354/566) reported sleep disturbance. Deprivation measured by DEPCAT scores was associated with maternal smoking and bronchitis in the child but not with allergic diseases.
Conclusion: Compared with previous studies, the prevalence of asthma is unchanged but eczema has increased in Highland adolescents. Allergic disease has a significant impact on school attendance and physical activity. Deprivation is associated with maternal smoking and bronchitis in the child but not with allergic diseases. The impact of allergic diseases in rural areas may be different from urban areas.
Acknowledgement: This study was funded by Chest, Heart and Stroke Scotland.
P82 CAN ASTHMA LIAISON NURSES REDUCE UNSCHEDULED CARE IN A DEPRIVED MULTIETHNIC POPULATION? ELECTRA: THE EAST LONDON CONTROLLED TRIAL FOR HIGH-RISK ASTHMA
C. Griffiths, G. Foster, G. Feder, H. Tate, S. Eldridge, N. Barnes1, A. Livingstone, T. Coats1, for The Electra Group. Dept General Practice and Primary Care, Barts and the Royal London Hospital, London, E1 4NS; 1The London Hospital, London E1, UK
Introduction: Evaluations of specialist nurses have focused on education in secondary care rather than liaison with primary care, and have not been set in multiethnic populations.
Design: Cluster randomised control trial comparing liaison nurse intervention versus best usual practice.
Setting: Forty four general practices in Tower Hamlets, east London Participants: 324 adults and children with asthma recruited after hospital admission or accident and emergency attendance.
Intervention: Intervention practices received two educational visits from liaison nurses to promote care of high risk patients. Participants from intervention practices received structured self management education from a liaison nurse. Control practices received one liaison nurse visit to discuss standard asthma guidelines. Participants from control practices received an inhaler technique check.
Main outcome measures: Participants free of unscheduled care; time to first unscheduled contact.
Results: Fifty per cent of participants were south Asian, 34% white, and 16% other ethnicities. Primary outcome data was available for 319/324 (98%) participants. Intervention by specialist nurse increased time to reattendance with an exacerbation (hazard ratio 1.17 (1.01–1.36) p<0.05) and percentage of participants not attending with exacerbations (p=0.056). Time to re-attendance was increased for white participants (1.33 (1.08–1.56) p=0.006) but not south Asians (1.18 (0.96–1.45) p=0.12).
Conclusions: Asthma liaison nurse intervention reduced unscheduled care in a deprived multiethnic population; white participants benefited but south Asians did not. Interventions are needed that improve asthma morbidity in non-white people with asthma.
Funded by the National Asthma Campaign.
P83 DEVELOPMENT OF CENTRALISED ASTHMA NURSE SPECIALIST FOLLOW UP SERVICE FOR PATIENTS WHO ATTEND OUT OF HOURS FOR ASTHMA
C. Calder, M. Reilly, L.M.Osman, A. Douglas, J.G. Douglas. Chest Clinic, Aberdeen Royal Infirmary, Aberdeen, AB25 2ZN, UK
Background: Local audit of patients attending out of hours (OOH) for asthma highlighted gaps in follow up in primary care. One possible solution was asthma nurse specialists (ANSPs) based in OOH centre, providing a centralised service for reviewing these patients.
Aim: Improvement in primary care management of patients attending OOHS for asthma.
Design: Twenty four practices in two Local Health Care Cooperatives matched by size and deprivation category were randomised to 12 practices whose patients would participate in ANSP service and 12 practices whose asthma care remained the same. Patients, aged 5–60, were recruited over 14 months.
Method: Two part time ANSPs with advanced asthma qualifications were employed. Patients were identified from OOH’s cooperative and Accident & Emergency daily. The Intervention group was sent a flyer followed by an asthma assessment telephone call by the nurses offering an appointment for a review at the Primary Resource Centre or at one rural practice between 09:00 to 18:00. A letter of invitation was sent if no telephone or if unable to contact. Prior to review and telephone call the nurses read primary care notes and repeat asthma prescriptions for each patient. The review, taking approximately 45–60 minutes, included asthma education, medication advice, and self management plans. Following review and or telephone call a summary liaison form was sent to the GP.
Results: Telephone assessment 177/237 (77%), contact time was median 9 (2–29) days. Attended review 62/237 (26%), contact time was median 18 (8–72) days. Refused review 81/237 (34%), 48 (20%) because had hospital/GP review already. Thirty eight out of 237 (16%) defaulted review appointment. Unable to contact 56 (24%) patients. Nurse management recommendations advised for 46/62 (74%) of those reviewed, of which 16 (35%) recommendations were acted on in the practice.
Conclusion: There was a poor response from patients to centralised review. This type of service may not be appropriate for OOH’s attenders
P84 WHAT TREATMENT FACTORS INFLUENCE READMISSION AFTER A HOSPITAL ADMISSION FOR ACUTE ASTHMA?
W. Rea, G. Perkins, A. Abhyankar, D.R. Thickett. Queen Elizabeth Hospital, Birmingham B15 2TH, UK
The most severe forms of asthma attack are the life threatening forms which result in hospitalisation. Once patients have been stabilised as an inpatient, the clinician is faced with the question of what to do with the inhaled therapy of patients admitted with acute exacerbations of asthma? The purpose of this study was to see if discharge medication influenced subsequent readmission rate.
Methods: All patients with a coding diagnosis of asthma were traced through hospital computer system. In 2000 there were 357 patients so labelled. Audit was carried out on 100 patients’ notes. Patients with a greater than 20 pack year smoking history or a diagnosis of COPD anywhere in the notes were excluded unless asthma had been diagnosed by a consultant chest physician. Subsequent to the case note audit, the patients were sent a short questionnaire at the end of 2001, inquiring about admissions to hospitals other than QEH. Steroid use and casualty attendance. Questionnaire letters have been received back from 54 out of 100.
Results: The BTS asthma step of the admitted patients correlated well with the risk of subsequent readmission (r2= 0.89, p=0.01). Patients with step 0 or step 1 asthma treatment had a low asthma readmission rate in the subsequent year (6%). Overall readmission rate was 41% in the year following discharge. Of those readmissions, 25% were to a different trust. Treatment by a respiratory specialist did not decrease the rate of readmission but did result in slightly longer hospital stays (1.2 days p=0.05 Mann Whitney U test).
Median dose of inhaled corticosteroid dose was 400 μg BDP upon admission and 800 μg equivalent upon discharge (p=0.009). There was no difference in the median steroid dose of patients admitted subsequently (805 μg) compared to those who were not admitted (800 μg, p=0.9). The time to first readmission after the index admission in 2000 was significantly longer in patients treated with long acting β agonists (105 days) compared to the group untreated with LAB (27.5 days, p=0.02 Mann Whitney U test). Of patients discharged from hospital, 38% have subsequently been prescribed a long acting β agonist.
Conclusions: The level of treatment received by patients seems to reflect their risk of hospitalisation in this cohort. Readmission rates are high and admission to more than one hospital is common in Birmingham. Specialist care has little effect upon crude readmission rates. The routine use of LAB following hospital discharge needs evaluating in a clinical trial.
P85 PSYCHIATRIC MORBIDITY IN DIFFICULT ASTHMA
E. Conway1, C. Kelly1, J. Gamble3, L. Heaney2 3. Departments of 1Mental Health; 2Medicine, Queen’s University Belfast; 3Regional Respiratory Centre, Belfast City Hospital Belfast BT9 7BL, UK
Introduction: Near fatal/fatal asthma are associated with psychiatric morbidity (PM). Studies have demonstrated PM in asthmatics of varying severity using questionnaire screening tools, but it is unclear how this relates to ICD10 psychiatric diagnosis (gold standard). The aim of this study was to: (1) examine psychiatrist diagnosed morbidity in a population of difficult asthmatics (persisting symptoms/frequent exacerbations despite high dose inhaled steroids/long acting β agonist, and (2) relate ICD10 diagnosis to response to the Hospital Anxiety Depression Questionnaire (HAD), a commonly used screening tool, with defined normal values.
Methods: Sequential new referrals to a difficult asthma clinic completed HAD questionnaire and were invited to attend for psychiatric interview as part of a systematic evaluation protocol. Psychiatric interview was performed, by an experienced medical liaison psychiatrist, blinded to all clinical information. After interview, an ICD10 diagnosis was recorded and treatment instituted as appropriate.
Results: Seventy eight patients were recruited (seven refused psychiatric assessment but were otherwise protocol compliant, five were non-compliant with the protocol). Of the remaining 66 subjects, 33 (50%) had an ICD10 psychiatric diagnosis; only seven (10%) were receiving current treatment. Depressive illness (F32) was common (20 (30%)) followed by generalised anxiety disorder (F41) (5 (8%)) plus a variety of other conditions. Anxiety (13.1 (0.82) v 8.5 (0.7)) and depression (10.1 (0.71) v 4.8 (0.47)) scores were significantly higher in subjects with an ICD10 diagnosis (p<0.001). The positive (PPV) and negative predictive value (NPV) for abnormal HADS scores for all psychiatric diagnoses were 60% and 86% respectively and for depressive illness, PPV 76%, NPV 96%.
Conclusion: There is a high prevalence of psychiatric morbidity, particularly depression, in difficult asthmatics, based on psychiatric interview, most undiagnosed at referral. HADS score has poor overall positive predictive value for psychiatric illness but normal depression score virtually excludes the commonest condition, depressive illness. We are currently examining the predictive role of undiagnosed psychiatric disorder in asthma outcome and optimal screening instruments in this population
P86 PSYCHOSOCIAL FACTORS IN ADULTS AT RISK OF ADVERSE ASTHMA OUTCOMES: RELATIONSHIPS WITH SYMPTOM CONTROL AND QUALITY OF LIFE
J.R. Smith1, M. Koutantji1, S. Mildenhall2, B.D.W. Harrison2, M. Noble3. 1University Of East Anglia; 2Norfolk & Norwich University Hospital; 3Acle Medical Centre, UK
Background: Despite effective treatments, a proportion of asthmatics suffer from poorly controlled disease and consequent reduced quality of life (QoL), hospital admissions, near fatal, and fatal asthma attacks. This study assesses psychosocial characteristics of adults at risk of such adverse asthma outcomes and examines relationships with symptom control and QoL.
Methods: Ninety two adults with severe asthma (on BTS Step 4/5 treatment and/or with previous admissions for asthma) who exhibited poor compliance (failure to attend clinics or comply with asthma management in other ways) were recruited via hospitals and GP practices in Norfolk and Suffolk. Cross-sectional socio-demographic/socio-economic data and self report measures of symptom control, QoL, psychiatric morbidity, perceived control over asthma, coping, and aspects of self management were collected via interviews in patients’ homes.
Results: In common with those experiencing fatal and near fatal asthma, these patients represent a socioeconomically disadvantaged group (for example, 60% not working, 63% receiving free prescriptions) with reduced QoL (mean 1.17 on a 0 (very good) to 2 (very poor) scale), high levels of psychiatric morbidity (for example, 36% experiencing moderate-severe anxiety, 33% reaching cut off for psychiatric caseness), and inadequate self management (for example, 82% not monitoring asthma, 39% smoking, 61% owning pets). High psychiatric morbidity, low perceived control over asthma and various indicators of low socioeconomic status were significantly correlated with poor symptom control and reduced QoL (all p<0.001). Being overweight, use of coping strategies which involve focussing on asthma (both p<0.05) or hiding asthma and, interestingly, high compliance (both p<0.001) were also associated with poorer asthma related QoL.
Conclusions: Various mechanisms may explain associations between psychosocial characteristics, symptom control, and QoL in at risk asthmatics and the direction of relationships is likely to be two way. Further psychological research to improve understanding in this area and an intervention study which attempts to address psychosocial issues in improving outcomes for at risk asthmatics are underway.
P87 RELATIONSHIP BETWEEN AIRWAY OBSTRUCTION AND SYMPTOM CONTROL IN PATIENTS WITH DIFFICULT ASTHMA
S. Aburuz1, J. McElnay 1, J. Millership1, J. Gamble 3, L. Heaney2.3. 1School of Pharmacy; 2Department of Medicine, Queen’s University Belfast; 3Regional Respiratory Centre, Belfast City Hospital, Belfast
Introduction: Several studies have demonstrated a poor relationship between symptom control and airways obstruction in patients with asthma. We examined this relationship in a population of difficult asthmatics (persisting asthma symptoms/frequent exacerbations requiring systemic steroids despite maintenance high dose inhaled corticosteroids (ICS) and a long acting β2 agonist) attending a hospital outpatient clinic.
Methods: FEV1% and asthma control scores (ACSs) (Juniper et al. 2001) were measured at the first clinic visit and at a follow up visit after a variable period of evaluation and treatment (9 (6.2) months).
Results: Fifty seven patients (37 females; median age 40 years; range 19–72 years; median ICS dose at presentation 2000 μg; range 1000–6400 μg BDP equivalent; median rescue steroid courses 12 months pre-referral = 5). Patients had poor control at the initial visit (mean ACS 4.1 (1.3); FEV1% 66.3 (22.7)). At the initial visit, FEV1% was correlated with limitation of activity (p=0.003), shortness of breath (p=0.018), wheezing (p=0.025) and ACS (p=0.018). FEV1% was significantly improved at the follow up visit (75.3 (22.6), p<0.0001) with an associated improvement in ACS (2.8 (1.3), p<0.0001). However, at the follow up, there was no correlation between FEV1% and any measured index of asthma control. At the initial visit, 25 patients had severe obstruction (FEV1% < 60%) and had significantly poorer ACSs (mean 4.6 v 3.7, p=0.003). At the follow up, 15 patients had FEV1% < 60% but no difference in ACSs (2.7 v 2.8, p=0.9). Best FEV1% was significantly less in this latter group (62 (21) v 96% (16%), p<0.0001) consistent with fixed airflow obstruction. When this group was excluded, FEV1% at follow up, was significantly correlated with night waking (p=0.02), wheezing (p=0.05), and ACS (p=0.036).
Conclusion: FEV1% correlates well with asthma symptoms in difficult asthma patients with poor control but not when control improves. This loss of relationship is due to subjects with fixed airflow obstruction where good subjective control does not exclude the presence of significant obstruction.
1. Juniper E, et al.
.
P88 UTILITY OF HISTORY IN THE DIAGNOSIS OF CHRONIC COUGH
J.C. Ojoo, S.A. Mulrennan, J.A. Kastelik, R. Thompson, A.E. Redington, A.H. Morice. Academic Department of Medicine, University of Hull, Castle Hill Hospital Cottingham, UK
Background: Patients referred to specialist cough clinics often have a history of prolonged period of cough, multiple investigations, and unsuccessful trials of therapy. It may be that symptoms in these patients are atypical making diagnosis of underlying condition difficult.
Aim: To determine presenting symptoms of patients with chronic cough in relation to their diagnosis.
Methods: In a prospective study based on a therapeutic rather than investigative protocol, consecutive patients with a history of cough for over eight weeks referred to the Hull Cough Clinic were enrolled. Assessment was by structured history, physical examination, chest radiograph, spirometry, and reversibility to nebulised salbutamol. From this information a diagnosis was made and patient had an eight week therapeutic trial. Further therapeutic trials were carried out depending on response to treatment and the likely diagnoses. Investigations were carried out in cases of failed therapeutic trials and to exclude specific pathology (in this study lung cancer, localised bronchiectasis and interstitial lung disease).
Results: One hundred and eleven (73 female) patients mean (SD) age 56 yr (12.8) were recruited. Main initial diagnoses were gastro-oesophageal reflux disease (GER) 52 (46.9%), asthma 23 (20.7%), and rhinitis 19 (17.1%). Sixty three patients have had at least two clinic visits. Of those discharged so far, median (range) duration of cough was 8.2 yr (0.25 to 64) and mean duration of follow up was 14 weeks (2.4 clinic visits). Twenty four out of 63 (38%) patients were discharged at the second and 10/23 (43%) at their third visit. The main underlying diagnoses at discharge were GER (25.7%), asthma (22.9%), and rhinitis (11.4%). Twenty per cent required investigations to arrive at the diagnosis and exclude other pathology, the rest were managed successfully on the therapeutic protocol. Symptoms associated with diagnosis of asthma were dyspnoea (p=0.007), wheeze (p=0.04) and choking (p=0.03), GER were heartburn (p=0.01) and sour taste in the mouth (p=0.06) and for rhinitis were postnasal drip (p=0.05) and breathlessness (0.03).
Conclusion: In patients in whom we have made a diagnosis and are satisfied with treatment, the presenting complex of symptoms is indicative of the underlying cause of their cough. This finding highlights the importance of the history taking in the assessment of patients with chronic cough.
P89 FACTORS ASSOCIATED WITH POST BRONCHODILATOR FEV1 IN ADULTS WITH ASTHMA
M.A. Berry, R.H. Green, A.J. Wardlaw, I.D. Pavord. Glenfield Hospital, Groby Road, Leicester, LE3 9QP, UK
Fixed airflow obstruction occurs in a minority of asthmatic patients but is a predictor of overall mortality. Smoking has been identified as a factor associated with airflow limitation in asthma but evidence implicating other factors has been conflicting. In one study ten Brinke et al (
) identified elevated induced sputum eosinophil count as an independant risk factor for persistent airflow limitation in a homogeneous population of severe asthmatics. We have investigated factors associated with the post bronchodilator FEV1 in a heterogeneous population of 249 adults with a clinical diagnosis of asthma of variable severity and evidence of airflow variability and/or airway hyper-responsiveness. Patients had either never smoked or were ex-smokers with less than five pack years smoking history. Patients underwent methacholine challenge testing, pre and post bronchodilator spirometry, skin, and radioallergosorbent testing to commonly encountered aeroallergens and induced sputum analysis. Multiple independent linear regression analysis was used to identify any independent predictors of post bronchodilator FEV1% of predicted. Duration of symptoms, atopy, dose of methacholine required to cause a 20% fall in FEV1 (PC20), induced sputum eosinophil count and induced sputum neutrophil count were not significant independent predictors of post bronchodilator FEV1 (r2 = 0.060, p=0.162). Patients with post bronchodilator FEV1 of less than 80% predicted had significantly higher induced sputum eosinophil counts (geometric mean 3.95%) than those with FEV1 above 80% predicted (geometric mean 1.88%, mean fold difference 2.10, 95% confidence interval 1.19 to 3.72, p=0.011). Measures of current airway inflammation and responsiveness do not independently predict persistent airflow limitation, as measured by post bronchodilator FEV1% predicted in a heterogeneous population of non-smoking adult asthmatics. Although sputum eosinophil counts are higher in patients with persistent airflow limitation, sputum eosinophilia is not predictive of airflow limitation and cannot be implicated as causative.
P90 EMITS: IMPACT OF A CHANGE IN TRANSPORT POLICY ON RESPIRATORY HEALTH IN OXFORD
S.J. MacNeill1, M. Barnes1, R. Pitman2, P. Cullinan1. 1Occupational & Environmental Medicine, Faculty of Medicine, Imperial College of Science, Technology and Medicine, 1b Manresa Rd, London SW3 6LR, UK; 2Community Services, Oxford City Council, Ramsay House, 10 St Ebbe’s St, Oxford OX1 1PT, UK
EMITS (Environmental Monitoring of an Integrated Transport Strategy) was established to examine the effects of a change in transport policy on public health as well as on other aspects of life in Oxford. The Oxford Transport Strategy (OTS) was implemented in June 1999 and involved many changes, focused primarily on the city center where all traffic was barred from some streets and private vehicles from others.
Between 1998 and 2000, 1386 children aged 6 to 10 were recruited from seven Oxford schools. Schools were visited two to three times a year in different seasons for five day periods. On each day of each visit, research nurses measured the childrens’ peak expiratory flow and distributed questionnaires enquiring about respiratory symptoms on the previous day. Parents were also sent questionnaires enquiring about the medical history of the child and the presence of pollutants and irritants in the home. Regression analyses of daily peak flows among all children showed that lung function improved significantly by 5.87 units (std err= 0.71, p<0.001) post-OTS after controlling for potential confounders. Similarly, the odds of wheeze decreased post-OTS (OR=0.84, 95% CI 0.77 to 0.92).
While it is not clear at this stage that these improvements can be attributed solely to the transport strategy, they suggest that traffic management can result in valuable improvements in public health.
P91 HARIG: ASTHMA CARE IN THE HUNTINGDON PCT 2002
D. Lightfood, J. McAllister, for the HARIG Group. Hinchingbrooke NHS Trust, Huntingdon; Huntingdon PCT, UK
Introduction: Asthma has considerable impact in terms of morbidity and health care costs. The ACE(1) survey suggests that over 30% of patients who report feeling well to their health professional suffer daily asthma symptoms.The HARIG study set out to raise asthma awareness within the Huntingdon PCT and use the results to develop a strategy for asthma care.
Method: A shortened version of the “Impact of asthma” questionnaire was used for the study. This was freely distributed in all GP surgeries and given to patients who attended to request repeat scripts and for review. A freepost address was supplied for return of questionnaires.
Results: PCT population was estimated at 147 000 patients. 493 responses received, with asthma prevalence estimated at 5%, returns approximately 6.7% of asthma population. Female:male split was 60%:40%. Average duration of asthma was >5 years, with a predominance of sufferers in the 18–65 year age group. Thirty seven per cent of patients reported daily asthma symptoms, with this figure higher than 50% in some GP practices. More than 30% of patients experienced significant night time waking. There was considerable variance in use of reliever medication with 32% of patients reporting use at least once per day but this figure was as high as 67% in one practice. 45% of respondents reported that asthma has at least a moderate effect on their lives, but this did not always correlate with the reporting of other symptoms.
Conclusion and discussion: Amongst the HARIG questionnaire respondents there is considerable unmet need for asthma symptom control. The results broadly mirror those of the ACE survey with around one third of respondents suffering continued symptoms. There may however have been some selection bias in those who responded to the survey and the results may not be a representative sample of the whole PCT population. Within the Huntingdon PCT there may be further opportunity for standardisation of care and sharing of good practice between GP surgeries.
This project has been supported with a project grant from GlaxoSmithKline Pharmaceuticals PLC.
1. Jones KG et al.
.
P92 IMPULSE OSCILLOMETRY IN SUBJECTS WITH SEVERE ASTHMA
W. Anees, S. Manney, J. Mukhopadhyay, D. Petkova, J.G. Ayres. Severe and Brittle Asthma Unit, Birmingham Heartlands Hospital, Birmingham B9 5SS, UK
Introduction: Many subjects with severe asthma describe a worsening of symptoms on lying flat. This is felt to be due to an increase in vagal tone.
Aims: (1) To describe airway resistance and capacitative reactance measurements as assessed by impulse oscillometry (IOS) in subjects with severe asthma and to relate them to spirometric parameters. (2) To see whether IOS parameters are affected by posture. (3) To determine whether IOS could identify subjects who clinically had vocal cord dysfunction.
Methods: Forty one subjects with severe asthma attending a tertiary referral centre underwent spirometry and IOS whilst sitting using an MS-IOS digital instrument (Jaeger AG). IOS was repeated on lying flat. Subjects were clinically assessed (by JGA) as to whether they had a significant component of vocal cord dysfunction.
Results: Eighty per cent were female, mean age 43.6 years with an FEV1 69.5% predicted. Mean total airway resistance (R5) was increased at 203% predicted with 73% of subjects having abnormally high values (>150% predicted). Proximal airway resistance (R20) was a mean of 141% predicted being >150% predicted in 32%. An increase in R20 occurred on lying down (p=0.03) with a fall in distal capacitative reactance (X5) (p=0.05) for the group as a whole. Although total airway resistance (R5) did not increase significantly (p=0.18), increases in R5 on lying down did correlate with body mass index (r=0.47, p=0.003). R5 was inversely correlated with FEV1 and peak expiratory flow (r=−0.42) but R20 did not. X5 also correlated with FEV1 (r=0.52). IOS parameters or change in IOS parameters could not identify subjects who clinically had vocal cord dysfunction.
Conclusion: Increased airway resistance using IOS was demonstrated in some patients with severe asthma and increased significantly on lying down, possibly due to an increase in vagal tone. It was not helpful for identifying subjects thought to have vocal cord dysfunction.
Pulmonary vascular biology/pulmonary hypertension
P93 THE EFFECTS OF ACUTE HYPOXIA ON PROLIFERATION AND p38 MAP KINASE ACTIVITY IN HUMAN FIBROBLASTS FROM THE PULMONARY AND SYSTEMIC CIRCULATIONS
H. Mortimer, A. Peacock, P. Scott1, D. Welsh. Scottish Pulmonary Vascular Unit, Western Infirmary; 1Institute Biomedical and Life Sciences, University of Glasgow, UK
Introduction: We have previously shown that proliferation and p38 MAP kinase phosphorylation in pulmonary artery fibroblasts is increased by hypoxia in animal models (Welsh, et al. Am J Resp Crit Care Med 1998 and 2001). We now wish to know whether this is true in man. In this study, we have examined the effect of acute hypoxia on human pulmonary and mammary artery (systemic) fibroblast proliferation and p38 MAP kinase activity.
Methods: Fibroblasts were harvested from human pulmonary artery (HPAF) and mammary artery (HMF) obtained from cardiothoracic surgery and utilised between passages 3–10. Cells were quiesced for 24 hours then stimulated by acute hypoxia for 24 hours (PO2=20 mmHg) with or without 0, 0.1, 1, 3, 5, and 10% serum. Fibroblast proliferation was measured by [3H]thymidine uptake and p38 MAP kinase activity was measured by Western Blotting analysis.
Results: [3H]Thymidine incorporation was increased by acute hypoxia (p<0.01) in the HPAF cells, but not in the HMF cells. Acute hypoxia also gave rise to p38 MAP kinase activation in the HPAF cells and to a lesser extent in the HMF cells (results not shown).
Conclusion: Acute hypoxia stimulated the proliferation of HPAF cells but not HMF cells. The increase in p38 MAP kinase activity to hypoxia may suggest a role in the regulation of cell cycle associated events. These results are consistent with our animal findings showing that these effects transcend species and may be important in man.
Chest, Heart and Stroke (Scotland) and British Heart Foundation.
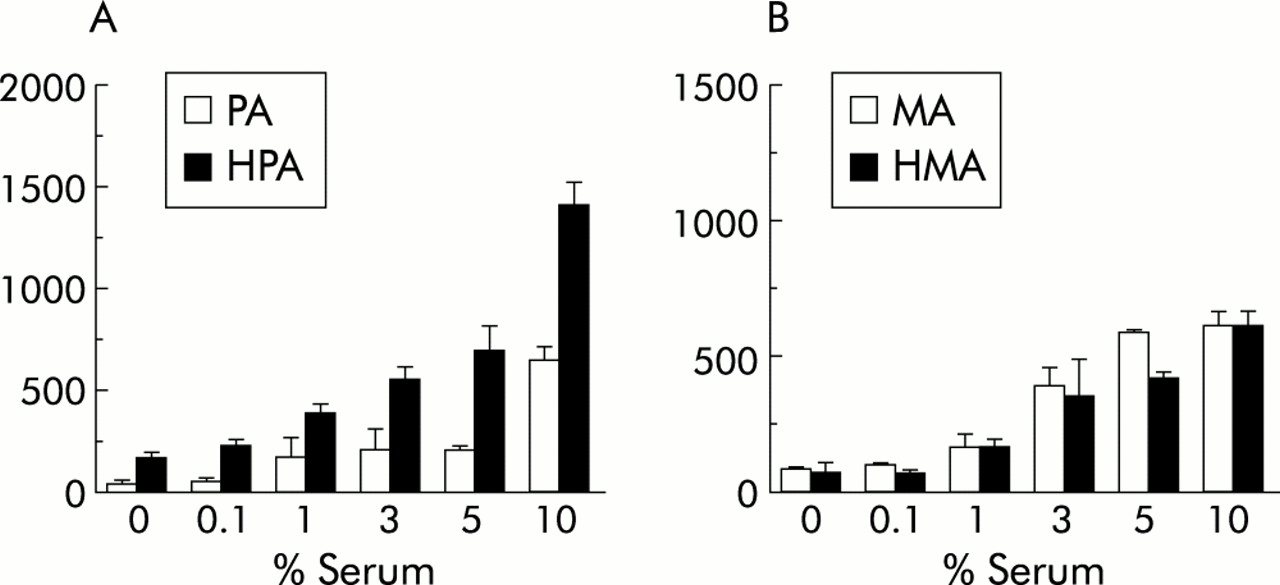
(A) HPAF. (B) HMF.
P94 ERYTHROCYTE SUPEROXIDE DISMUTASE ACTIVITY IN INFANTS WITH PERSISTENT PULMONARY HYPERTENSION AND CONGENITAL DIAPHRAGMATIC HERNIA
G.M. Walker, K.F. Kasem, C.F. Davis, M.R. Maclean. University of Glasgow, Glasgow, UK
Introduction: The antioxidant enzyme system is the primary intracellular defence system of the lung against oxygen toxicity. Endogenous SOD is the major mammalian antioxidant enzyme and catalyses the dismutation of superoxide anion to hydrogen peroxide. Reduced SOD activity has been demonstrated in animal models of Congenital Diaphragmatic Hernia (CDH)1 and in post mortem specimens from infants with persistent pulmonary hypertension of the newborn (PPHN).2 Erythrocyte SOD activity from live infants with these disorders has not been reported.
Methods: Blood was sampled from seven infants with PPHN and five with CDH. All were near term and mechanically ventilated. Following centrifugation and plasma removal, erythrocytes were stored at −20°C until analysis. SOD activity was calculated spectrophotometrically using the auto-oxidation of pyrogallol.3 Haemoglobin concentration was calculated using a standard Drabkin’s reagent. Differences in median values were calculated using the Mann-Whitney test.
Results: Median erythrocyte SOD activity of infants with PPHN was 1374.15 μ/g Hb (range 1114 to 1791). Erythrocyte SOD activity of infants with CDH was significantly lower (median = 1213.5, range 1016 to 1490.5, p=0.01).
Conclusion: Infants with CDH have lower erythrocyte SOD activity compared to similarly ventilated patients. This gives further evidence to explain the clinical fragility and poor response to inhaled nitric oxide seen in CDH.
1. Kapur P, et al.
.
2. Asikainen TM, et al.
.
3. Marklund S, et al.
.
P95 SUPEROXIDE AND SUPEROXIDE DISMUTASE IN PULMONARY HYPOXIC VASOCONSTRICTION
P.H. Milliken, R.M. Wadsworth. University of Strathclyde, UK
Superoxide is known to cause vascular damage and can consume protective NO that maintains a low pulmonary pressure. There is evidence suggesting that hypoxia upregulates NADH/NADPH oxidase and xanthine oxidase in the smooth muscle and endothelial cells of the pulmonary artery, increasing superoxide production. Superoxide dismutase (SOD) is widely distributed in the cells of the vasculature, destroying superoxide, however, the role of SOD in hypoxic vasoconstriction is unknown.1 Therefore, the effect of endogenous SOD inhibition and superoxide generation on hypoxic pulmonary vasoconstriction was investigated.
Male Sprague-Dawley rats were anaesthetised and the trachea and pulmonary artery cannulated. The lungs were ventilated with 20% O2 (normoxia), and perfused with 30 ml of modified Krebs solution. U46619 give preconstriction before a 10min hypoxic challenge (5%CO2, 95% N2). The lungs were then returned to normoxia for 10 mins before changing the perfusate to one containing either 1mM DETCA (high affinity Cu2+ chelator that inhibits endogenous SOD) or 10 μM LY83583 (superoxide generator). The lungs were allowed to equilibrate for 30 mins, before repeating the hypoxic and normoxic challenges. The NO donor SNAP (1.7x10-8 – 1.7x10-5 moles) was used after hypoxia in the LY83583 experiments.
Hypoxia induced a sustained monophasic increase in pulmonary pressure, that was reproducible (1.8 (0.2) mmHg 1st challenge and 1.7 (0.3) mmHg 2nd challenge, n=5). LY83583 augmented the hypoxic vasoconstriction (3.5 (1.0) mmHg, n=7), and attenuated the SNAP induced vasodilation. These results suggest that superoxide can support or enhance hypoxic vasoconstriction, perhaps by consuming endogenous NO. However, there was a significant reduction of hypoxic vasoconstriction in the presence of DETCA (1.0 (0.3) mmHg, n=7, p<0.05). Overall, these results suggest that hypoxic vasoconstriction can be modified by endogenous superoxide, however this interaction may be dependent upon the site of superoxide generation and the concentration of superoxide, as there is likely to be a greater amount of superoxide present in the experiments involving LY83583.
PH Milliken is funded by the British Heart Foundation (FS/2001056).
1.
.
P96 MICE OVER EXPRESSING THE 5-HT TRANSPORTER: A NEW MODEL FOR PULMONARY HYPERTENSION?
I. Morecroft, L. Loughlin, J. MacKenzie, A. Harmar1, M.R. Maclean. Institute of Biomedical and Life Sciences, University of Glasgow, Glasgow, G12 8QQ; 1Dept Neuroscience, Edinburgh University, Edinburgh, EH9 9JZ, UK
The 5-hydroxytryptamine transporter (5HTT) may play a key role in pulmonary vascular remodelling in primary pulmonary arterial hypertension (PAH) and secondary hypoxia-related PAH. Attenuated hypoxic pulmonary hypertension has been reported in mice lacking the 5HTT transporter gene and there is 5HTT over-expression in patients with PAH (
;
). Here we examine the development of PAH in mice over expressing the 5HTT gene (5HTT+ mice) and C57BL/6 × CBA wild type mice (WT) mice (female, 1 year old) exposed to two wks chronic hypoxia. Right ventricular (RV):total ventricular (TV) ratio was used as an index of pulmonary hypertension. In WT mice, RV/TV ratio was not altered after two wks hypoxia (0.205 (0.005) cf. 0.238 (0.012), n=6–7). In 5HTT+ mice, however, RV/TV ratio was increased (p<0.001, n=7) from 0.194 (0.009) to 0.297 (0.018). The number of remodelled small (<80 μm i.d.) vessels (assessed histologically) increased (p<0.001, n=6) from 2.61 (0.7%), (control hypoxic) to 7.8 (0.5%) (5HTT+ hypoxic). ET-1, NA, and 5HT induced contraction was measured using wire myography in small pulmonary arteries (∼200 μm i.d.) and were, in WT mice vessels (pEC50s: 9.8 (0.3) > 9.0 (0.2) > 6.9 (0.2) respectively). NA constriction was markedly reduced in the 5HTT+ mice and the potencies of ET-1 and 5HT were reduced (pEC50s: 8.4 (0.3) and 5.6 (0.3) respectively). In the 5HTT+ mice exposed to hypoxia however, there was a marked restoration of the contractile response to NA (pEC50: 8.6 (0.1)) and an increase in the response to ET-1 and 5HT (pEC50s: 8.6 (0.3) and 6.9 (0.4) respectively). The maximum response to ET-1 was increased by ∼40%. In WT mice lung membranes, the 5HTT ligand 3[H]-β-CIT bound with a Bmax of 1.068 (0.022) fmolmg-1 and a KD of 0.869 (0.054) nM (n=3). Non-specific binding was assessed using cold fluoxetine. Binding was markedly increased in the 5HTT+ mice, with a Bmax of 13.32 (0.25) fmolmg-1 and a KD value of 3.745 (0.033) nM (n=3). The results indicate that PAH is accelerated in 5HTT+ mice and this is associated with remodelling, increased lung 5HTT and increased contractile responses to 5HT, ET-1 and restoration of NA-induced contraction. 5HTT+ mice may provide a novel model of genetically susceptible PAH.
P97 HUMAN UROTENSIN-II ACTS AS A PULMONARY VASOCONSTRICTOR IN AN IN VIVO RABBIT MODEL OF PULMONARY HYPERTENSION SECONDARY TO LEFT VENTRICULAR DYSFUNCTION
G.A. Deuchar1, M.R. Maclean2, M.N. Hicks1. 1Department of Medical Cardiology, Glasgow Royal Infirmary; 2Institute of Biomedical and Life Sciences, University of Glasgow , Glasgow G12 8QQ, UK
The recently cloned peptide, human Urotensin-II (hU-II) has been shown to be the most potent vasoconstrictor identified to date, being an order of magnitude more potent than endothelin-1. In the pulmonary circulation, hU-II has been shown to result in a greater vasoconstrictor effect in isolated main pulmonary arteries from rats with pulmonary hypertension (PHT) secondary to chronic hypoxia. However, in isolated human pulmonary arteries, a vasoconstrictor response to hU-II was only uncovered following nitric oxide synthase (NOS) inhibition (
). Here we investigated the pulmonary and systemic effects of hU-II alone and in the presence of the NOS inhibitor L-NAME in a previously described in vivo rabbit model of PHT secondary to LVD (
). Briefly, eight weeks following coronary artery ligation or sham operation, ejection fraction (EF) was assessed using echocardiography and experiments were carried out in closed chest anaesthetised rabbits. Pulmonary arterial pressure (PAP) and systemic aortic pressure (AOP) were measured directly before and after cumulative administration of hU-II (0.001–5.0 nmoles.kg-1) either alone or following the infusion of L-NAME (30 μmoles.min-1). Coronary ligated rabbits had reduced EF (45.2 (1.0%) v 73.0 (0.9%), p<0.001), elevated basal PAP (16.8 (0.4) mmHg v 13.6 (0.2) mmHg, p<0.001) and evidence of right ventricular hypertrophy as measured by right ventricular/final body weight ratio (0.69 (0.03) g/kg v 0.48 (0.01) g/kg final body weight, p<0.001). A small significant pulmonary pressor effect was demonstrated to hU-II alone, with the maximum response being greater in rabbits with PHT (2.6 (0.5) mmHg, n=8, v 1.0 (0.3) mmHg in controls, n=8, p<0.05). Following NOS inhibition, there was a trend towards the maximum pulmonary pressor effect being increased in both groups (8.5 (2.6) mmHg, n=12, and 4.8 (1.5) mmHg, n=13, in rabbits with PHT and controls respectively). In contrast, it was shown that hU-II had no effect on systemic AOP in any of the experimental groups. In conclusion, hU-II appears to act as a selective pulmonary vasoconstrictor with no effect on AOP.
P98 THE PROSTACYCLIN ANALOGUE CICAPROST, INDUCES HETEROLOGOUS DESENSITISATION IN PULMONARY ARTERY SMOOTH MUSCLE CELLS VIA PROTEIN KINASE A DEPENDENT INHIBITION OF ADENYLYL CYCLASE
A. Sobolewski, K.B. Jourdan, P.D. Upton, N.W. Morrell. Department of Respiratory Medicine, University of Cambridge, Addenbrooke’s and Papworth Hospitals, Cambridge, CB2 2QQ, UK
Prostacyclin is the major arachidonic metabolite produced in vascular cells and is a powerful vasodilator of the pulmonary vasculature. Long term infusion of prostacyclin analogues is an effective treatment for primary and secondary pulmonary hypertension, but due to desensitisation of the agonist response, increased doses are required to maintain efficacy. The aim of this study was to investigate the mechanisms of prostacyclin desesnsitisation using the prostacyclin analogue cicaprost in rat pulmonary artery smooth muscle cells (PASMC). PASMC were isolated from precapillary pulmonary arteries of WKY. For timecourse studies confluent, serum-starved PASMC, were pre-incubated with cicaprost (63nM, for 15min to 12h), washed and stimulated with cicaprost (63nM, 15 min). In further studies other conventional Gsα-adenylyl cyclase coupled agonists (ISO, 1μM), adrenomedullin (ADM, 100nM), bradykinin (BRAD, 1μM) forskolin (FSK, 3μM) were added to PASMC pre-incubated with cicaprost (63nM, 6h). For resensitisation experiments cicaprost pre-incubated PASMC (63nM, 3h) were placed in serum-free media for 3 to 24 h prior to cicaprost addition (63nM, 15 min). For inhibitor studies a one hour pre-incubation with the PKA inhibitor, H89 (1μM) or the PKC inhibitor, bisindolylmaleimide (BIS, 100nM) was introduced prior to cicaprost pre-incubation (6h, 63nM). Experiments were terminated with 0.1M HCl and assayed for cAMP activity using an ELISA kit. Desensitisation of the cAMP response occurred after 6 hours pre-incubation with cicaprost (n=3, p<0.05). Desensitisation also occurred with ISO, BRAD, ADM in addition to FSK (n=3, p<0.05). The desensitisation effect was reversible, with cAMP returning to control levels 12 hours after removal of the agonist (n=3, p<0.05). PKA inhibition abrogated cicaprost desensitisation (80 (5%)), whereas the PKC inhibition reversed the effect to a lesser extent (59 (3%)). In conclusion, chronic treatment of PASMC with cicaprost, induced heterologous, reversible desensitisation by inhibition of adenylyl cyclase activity. Our data suggest that the desensitisation by cicaprost is mediated predominantly by PKA, and to a lesser extent, PKC inhibitable isoforms of adenylyl cyclase.
P99 BONE MORPHOGENETIC PROTEIN-4 INHIBITS HUMAN LUNG FIBROBLAST PROLIFERATION VIA EFFECTS ON CELL CYCLE REGULATORS
T.K. Jeffery, P.D. Upton, R.C. Trembath1, N.W. Morrell. Respiratory Medicine Unit, Department of Medicine, University of Cambridge, School of Clinical Medicine, Addenbrooke’s Hospital, Cambridge, UK; 1Division of Medical Genetics, University of Leicester, Leicester, UK
Introduction: Mutations in the bone morphogenetic protein type II receptor (BMPR2) have been identified in patients with primary pulmonary hypertension. Given that BMPR2 mutations may inhibit BMP-effects on cell proliferation we examined the effect of BMP-4 on the cell cycle and signal transduction via Smad-1 and p38MAPK pathways in human lung fibroblasts. Since this is the first time that pulmonary fibroblasts have been used to examine BMP-4 responses we also characterised BMPR2 receptor expression, ligand binding, and the effect of BMP-4 on fibroblast growth.
Methods: Human fetal lung fibroblasts (HFL-1) were used. BMPR2 expression was determined using RT-PCR. Ligand binding studies were carried out by constructing competition curves for 125I-BMP4 against BMPs 2, 4, and 7, and TGFβ1. To determine the effect of BMP-4 on the cell cycle, propidium iodide stained cells were analysed utilising a fluoresence activated cell sorter (FACS). Western analysis using antibodies directed towards phospho-p38MAPK, phospho-Smad-1 and the cell cycle proteins, p21, p27, cyclin D, and cyclin dependent kinase-2 (cdk2) was performed.
Results: BMPR2 mRNA was expressed in HFLs and binding experiments demonstrated that BMP-2 and BMP-4 competed equipotently for 125I-BMP-4 binding, BMP-7 was weakly competitive and TGFβ did not compete. BMP-4 dose-dependently (1–100 ng/ml) inhibited 3H-thymidine incorporation as well as proliferation of HFLs. FACS analysis demonstrated that BMP-4 (50 ng/ml) inhibited cells from exiting the G0/G1 phase of the cell cycle. BMP-4 up regulated the expression of inhibitors of the G0/G1 phase of the cell cycle, p21, and p27, with a corresponding down regulation in expression of the positive regulators, cyclin D and cdk2. Phospho-Smad-1 and phospho-p38MAPK were rapidly induced in response to BMP-4.
Conclusion: BMP-4 leads to cell cycle arrest in HFL-1 cells via induction of p21/p27 and inhibition of cyclin D/cdk2. The relative contribution of p38MAPK and Smad-1 on BMP-4 induced cell cycle arrest remains to be determined.
Funded by: British Heart Foundation and NHMRC of Australia (TK Jeffery).
P100 THE RESPONSE OF FIBROTIC AND NON-FIBROTIC PATIENTS WITH SCLERODERMA ASSOCIATED PULMONARY ARTEIAL HYPERTENSION (SScPAH) TO CONTINUOUS AMBULATORY ILOPROST THERAPY: IS A SIMILAR THERAPEUTIC APPROACH JUSTIFIED?
D. Mukerjee, B. Coleiro, C. Elliott, C. Knight, C.M. Black, J.G. Coghlan. Departments of Rheumatology and Cardiology, Royal Free Hospital, Pond Street, London NW3 2QG, UK
Background: It is now accepted that patients with non-fibrotic SScPAH respond to epoprostenol therapy in a similar fashion to Primary Pulmonary Hypertension (PPH). We have observed that PHT underlying SSc-associated fibrosis is not predominantly hypoxia-driven and postulated that the mechanisms underlying fibrosis/non-fibrosis-associated PAH in SSc may be similar and thus responsive to the same therapeutic strategy.
Methods: Forty seven patients were initiated on continuous ambulatory iloprost therapy between 1996–2001 as they met the funding criteria for this therapy. Functional impairment was quantified using the Six Minute Walk Test (SMWT).
Findings: Forty seven SSc patients (M:F = 7:40) with a mRAP=10 mmHg, mPAP=42 mmHg, mean SVO2=59 %, and mean CI=1.8 were started on ambulatory iloprost. There was no significant difference in haemodynamic parameters between fibrotics (n=20)/non-fibrotics (n=27). Initial mean SMWT=175m fibrotics/215m non-fibrotics, a mean improvement of 29% in the fibrotics (226m) and 36 % in non-fibrotics (291m) at 12 weeks. This change was clinically significant in both groups: gain of 52 m in fibrotics/ 78m non-fibrotics. At 24 weeks this benefit was maintained (272m in fibrotics/321m in non-fibrotics) with a mean gain of 28 metres in both groups. Six month survival was 81%, with 23 (49%) patients surviving >1 year of therapy (14 fibrotics/9 non-fibrotics).
Conclusion: In a SSc patient cohort similar in structure in terms of initial hemodynamic findings, treated with ambulatory iloprost, the response to therapy in terms of functional benefit is similar in fibrotic and non-fibrotic patients. This justifies inclusion of SSc patients with pulmonary fibrosis associated PHT in trials of newer therapies.
P101 ELEVATED PULMONARY: AORTIC RATIO IN PATIENTS WITH PULMONARY ARTERIAL HYPERTENSION ASSOCIATED WITH SYSTEMIC SCLEROSIS
F. Guarasci, D. Manuel, M. Akil, C. Davies, D. Fishwick, E.J.R. Van Beek, D.G. Kiely. Pulmonary Vascular Disease Unit, Dept of Radiology and Dept of Rheumatology, Royal Hallamshire Hospital, Glossop Road, Sheffield, UK
Pulmonary arterial hypertension (PAH) occurs in approximately 15% of patients with systemic sclerosis (SS) and is associated with a poor prognosis. A number of screening regimes using non-invasive techniques are currently used to identify patients for cardiac catheterisation. We have examined whether the pulmonary:aortic (P:A) ratio measured using CT may be a useful non-invasive predictor of PAH in these patients.
Twenty one patients (three male), mean age 60 yrs (range 45–70 yrs) with SS and suspected pulmonary hypertension were studied. Patients underwent HRCT and CTPA in addition to right heart catheterisation. CT scans were interpreted by investigators blinded to the results of the other investigations. The main pulmonary artery and aortic diameter were measured transversely at the same level and the ratio calculated.
Of the 21 patients studied, 19 had PAH at rest (MPAP at least 25mmHg). There was a significant correlation between MPAP measured at RHC and P:A ratio, r=0.50, p=0.02. All 16 patients with an elevated P:A ratio >1 had PAH. Patients with a P:A ratio >1 compared to patients with a P:A ratio <1 had a significantly greater MPAP: 43 (13) v 26 (14) mmHg (95% CI 2 to 31mmHg, p=0.02). Using a P:A ratio of >1 to identify patients with PAH at cardiac catheterisation had a PPV of 1.0 and a NPV of 0.4.
In conclusion, an elevated pulmonary to aortic ratio measured using CT scanning techniques predicts the presence of PAH in patients with systemic sclerosis. In these patients undergoing CT scanning of the thorax an elevated ratio should alert the physician to the possibility of pulmonary hypertension.
P102 THE HAEMODYNAMIC EFFECTS OF “PULSED” INHALED NITRIC OXIDE IN PATIENTS WITH PULMONARY HYPERTENSION
T. Siddons, T.W. Higenbottam, F. Guarasci, I. Armstrong, K. McCormack, D.G. Kiely. Pulmonary Vascular Disease Unit, Royal Hallamshire Hospital, Glossop Road, Sheffield, UK
We examined the acute haemodynamic effects of pulsed inhaled nitric oxide (iNO) in patients with pulmonary hypertension. Patients with pulmonary arterial hypertension (n=35), chronic thromboembolic pulmonary hypertension (n=17), and hypoxic lung disease (n=7) were challenged acutely with pulsed iNO at a dose of 1.6 x 10−7 moles per breath during right heart catheterisation. The iNO was delivered in pulses via nasal cannulae using a breath activated device for five minutes. Pulsed iNO significantly reduced mean pulmonary artery pressure (MPAP): 45.0 (14) v 47.2 (13) mm Hg, pulmonary vascular resistance (PVR): 785 (432) v 878 (456) dynes.s.cm-5, and increased CO: 4.4 (1.6) v 4.2 (1.5) l/min (p<0.001). There was no significant change in mean arterial pressure (MAP): 92 (16) v 91 (14) mmHg but a significant (p<0.05) fall in systemic vascular resistance (SVR): 1696 (560) v 1784 (568) dynes.s.cm-5. We identified four response types (1) Non responder = reduction in PVR <20%. (2) Pressure response type = reduction in mPAP and PVR > 20%. (3) Flow response type = reduction in PVR >20% with a reduction in mPAP <10 % and a clinically significant increase in CO. (4) Resistance response type = reduction in PVR >20% with reduction in mPAP between 10–20% and a non clinically significant increase in CO (see table).
Pulsed iNO appears to be an effective acute pulmonary vasodilator. Further work needs to be performed to examine whether these response types predict outcome from therapy or mortality.
P103 COMPASSIONATE TREATMENT OF PULMONARY HYPERTENSION WITH LONG TERM INHALED NITRIC OXIDE AND ORAL SILDENAFIL (VIAGRA™)
T. Siddons, T.W. Higenbottam, K. Amsha, I. Armstrong, K. McCormack, D.G. Kiely. Pulmonary Vascular Disease Unit, Royal Hallamshire Hospital, Glossop Road, Sheffield, UK
Despite recent encouraging reports of trials of analogues of prostacyclin and antagonists of the endothelin-1 receptors, many patients with pulmonary hypertension (PH), still receive no treatment as a result of the expense and/or difficulty in administering these therapies. We examined the effects of long term pulsed inhaled nitric oxide (iNO) or oral sildenafil (Viagra™) in eleven disabled patients with PH associated with other disease processes and in two patients with primary PH, who did not receive funding for prostaglandin therapy. Patients were offered compassionate treatment with either pulsed iNO or sildenafil, one patient receiving first pulsed iNO then sildenafil after a wash out period.
Sildenafil at doses of 25 to 50 mg three times per day resulted in a significant improvement in shuttle walking test 274 (189) m v 201 (116) m at baseline (p=0.045). Two patients discontinued therapy due to deterioration, but six patients continue on sildenafil with a mean duration of therapy of 16 months (range 4–22). In contrast, all patients given pulsed iNO for 12 hours overnight deteriorated, with no patient continuing on therapy for longer than 11 months (mean six months, range 2–11).
In conclusion, although long term nocturnal therapy with pulsed iNO appears to be an ineffective treatment for pulmonary hypertension, sildenafil appears to be an effective and well tolerated form of therapy in this heterogeneous patient population.
P104 FLOW VELOCITY PROFILES AND HAEMODYNAMICS IN PULMONARY HYPERTENSION: A PILOT STUDY
T. Saba, J. Foster1, M. Cockburn1, M. Cowan1, A. Peacock. Scottish Pulmonary Vascular Unit; 1Department of Radiology, Western Infirmary, Glasgow, Scotland
Standard assessment of the pulmonary circulation including mean pulmonary artery pressure (MPAP), cardiac output (CO), and pulmonary vascular resistance (PVR) predict prognosis in pulmonary hypertension (PHT) but do not always predict the severity of exercise intolerance. We wondered whether flow velocity profiles, which are likely to reflect the haemodynamic response to exercise, would help to explain the differences in symptoms between patients with similar resting haemodynamics.
Method: We used cardiac triggered cine MRI to measure mean velocity (MV) and peak velocity (PV) in the right pulmonary artery in three subjects with PHT and one normal subject (see table 1) within two days of cardiac catheterisation and six minute walk testing (6mwt). Studies were performed at rest (R) and after three minutes of straight leg raising exercise (EX).
Results: See figures 1 and 2.

Figure 1 Flow velocity profiles in subjects. Two and three showed flattening with exercise.

Figure 2 Flow velocity profiles in subjects one and four, showing peaking with exercise.
Conclusions: Resting pulmonary haemodynamics may not predict exercise tolerance in PHT. Exercise MRI is feasible in this group of patients and flow velocity profiles obtained in this way may help to explain the differences in symptoms between patients with similar pulmonary haemodynamics.
P105 HAEMODYNAMICS DURING EXERCISE ARE A BETTER MEASURE OF VASODILATOR RESPONSE IN HUMAN SUBJECTS WITH PULMONARY HYPERTENSION
R. Syyed, A.J. Peacock. Scottish Pulmonary Vascular Unit, Western Infirmary, Glasgow, UK
Patients with pulmonary hypertension (PHT) are deemed “non-responders” (NR) if they show no response to vasodilators at rest. We therefore decided to investigate the effects of vasodilators on pulmonary haemodynamics during exercise.
Methods: We investigated four patients, (two female, two male) with PHT to determine pressure and flow changes over a range of flows. Flow was changed by straight leg raising. A micromanometer tipped continuous pulmonary artery pressure (PAP) catheter was inserted. All four were non-responders to a vasodilator challenge (defined as a reduction of >20% in pulmonary vascular resistance). Resting pressure was measured and then three mins of supine alternate straight leg raising was performed, while the subjects inhaled air or nitric oxide (NO, 40–80 ppm) and oxygen (O2, 15L min). Cardiac Output (CO) was measured by non-invasive impedence cardiography. Subject data was pooled using the method described by Poon (
). The best-fit line for Pressure Flow (P-Q) plots was determined by linear regression. An adjusted two paired student t test was used to compare the line gradients.
Results: We found that although total pulmonary vascular resistance (as defined as mean PAP/ CO) showed no change at rest, the slope of the P-Q plots decreased with vasodilators during exercise (p<0.0005) (see figure).

Pressure flow changes during exercise.
Conclusion: In each of these four subjects, whilst there was no vasodilator response at rest, there was an improving relationship between pressure and flow during exercise whilst receiving the vasodilators NO and O2. In patients with PHT, the assessment of vasodilator response may be better performed during exercise than at rest.
P106 FUNCTIONAL AND HAEMODYNAMIC RESPONSE AFTER PULMONARY THROMOBENDARTERECTOMY FOR THROMBOEMBOLIC PULMONARY HYPERTENSION
F. Reichenberger, J. Parameshwar, D. Hodgkins, J. Dunning, J. Pepke-Zaba. Papworth Hospital, Papworth Everard, Cambridge, UK
Pulmonary Thrombo-Endarterectomy (PTE) is the treatment of choice in pulmonary hypertension due to proximal chronic thromboembolism. We evaluated the midterm functional and haemodynamic outcome until one year after PTE. The functional capacity was assessed using the six minute walking distance (6MWD). Haemodynamic parameters were obtained during right heart catheterisation with Swan Ganz catheter and cardiac output with thermodilution method. Until March 2002, 88 patients underwent PTE (44 male, 43 female, mean age 52 (18–81) years) at Papworth Hospital. Fifty eight patients completed a three months follow up, and 35 patients 12 months follow up. Two patients were followed up by other centres and two patients did not attend follow up visits. Preoperative functional and haemodynamic data show a severely reduced 6MWD and cardiac index with increased right atrial pressure (RAP) and mean pulmonary artery pressure (mPAP). Three months after surgery there was a significant increase in 6MWD and cardiac index, and a decrease in RAP and mPAP. These changes were statistically significant (t test p<0.0001). The functional and haemodynamic improvement sustained also 12 months postoperatively (see table). None of the patients died between three months and 12 months follow up.
Conclusion: Patients have a significant and sustained functional and haemodynamic improvement after PTE with normalisation of haemodynamic parameters in the majority of patients. The main improvement is achieved within three months after surgery.
Cystic fibrosis: Inflammatory consequences of chronic infection
P107 NEUTROPHIL APOPTOSIS AND BACTERIAL INFECTION IN CYSTIC FIBROSIS
A.P. Watt1, J. Courtney1, J. Moore 2, J.S. Elborn1, M. Ennis1. 1Respiratory Research Group, Centre for Infection, Inflammation and Repair, The Queen’s University of Belfast; 2Department of Bacteriology, Belfast City Hospital, Belfast, UK.
In cystic fibrosis (CF), impaired mucociliary clearance leads to chronic endobronchial bacterial infection and inflammation, mediated by neutrophils. Pseudomonas aeruginosa infection is associated with an exaggerated inflammatory response and colonisation with Burkholderia cepacia is often accompanied by progressive pulmonary deterioration. Apoptosis of inflammatory cells is considered an essential requirement for the resolution of an inflammatory response. It was hypothesised that the number of neutrophils undergoing apoptosis would alter with the agent of infection in CF lungs. The aim of this study was to assess the relationship between levels of neutrophil apoptosis and sputum microbiology in matched clinically stable CF patients. In this preliminary study 29 patients were recruited: six (4M) with no Gram negative infection, 10 (4M) colonised with P aeruginosa, 9 (4M) with B cepacia infection and 4 (3M) with other Gram negative infections such as Stenotrophomonas maltophilia. Sputum was induced as previously described (Kelly, et al. 2002). Cells were recovered from sputum plugs. Apoptosis was investigated by staining sputum cells with propidium iodide (PI) and annexin V (AV), and subsequent flow cytometric analysis. Non-parametric statistic analyses were used throughout. The % of necrotic granulocytes (AV−PI+) was significantly higher in the P aeruginosa group (17.1 (2.5%), p=0.008) and the B cepacia group (13.9 (1.3%), p=0.008) compared to those with no Gram negative infection (7.5 (1.6%)). B cepacia patients also had a significantly higher % of secondary necrotic cells (AV+PI+) than those with no Gram negative infection (13.6 (2.3%), 5.8 (1.9%), p=0.02) whilst those with no Gram negative infection had a significantly higher % of cells which were neither apoptotic nor necrotic (AV− PI−) than the B cepacia group (77.6 (5.2%), 58.3 (4.4%), p=0.02). These preliminary results indicate that neutrophil apoptosis is associated with the type of organism colonising the CF lung. The greater number of granulocytes in cell death pathways from patients infected with P aeruginosa or B cepacia suggests that this may be a mechanism of greater inflammation and subsequent lung injury in CF.
P108 A COMPARISON OF INFLAMMATORY MARKER LEVELS IN CLINICALLY STABLE CYSTIC FIBROSIS PATIENTS WITH CHRONIC INFECTION BY UNIQUE AND EPIDEMIC STRAINS OF PSEUDOMONAS AERUGINOSA
A.M. Jones1, L. Martin2, R. Bright-Thomas1, M.E. Dodd1, S. Elborn3, A.K. Webb1. 1Manchester Adult CF Centre; 2School of Pharmacy, Queen’s University, Belfast; 3Northern Ireland Adult CF Unit, Belfast
Introduction: There are an increasing number of reports of Pseudomonas aeruginosa cross infection outbreaks at cystic fibrosis (CF) centres. The clinical significance of acquisition of an epidemic strain for patients who already harbour P aeruginosa is unclear. If epidemic strains are more virulent they may be more likely to provoke an enhanced host inflammatory response. We compared levels of inflammatory markers in clinically stable CF patients who harbour epidemic and unique strains of P aeruginosa.
Methods: Patients at the Manchester Adult CF Centre were invited to participate if they were clinically stable and had received a course of intravenous antibiotics 4–6 weeks earlier. Patients were grouped upon the basis of bacterial fingerprinting results into those who harbour epidemic and unique P aeruginosa strains; patients co-infected with Burkholderia cepacia complex were excluded. The following were measured: total white cell (WCC) and neutrophil blood counts; sputum neutrophil elastase (NE), interleukin (IL)-8, tumour necrosis factor (TNF) α; plasma IL-6, NE/α1-antitrypsin complexes; serum C-reactive protein (CRP); and urine TNFr1. The groups were compared using t tests and Mann Whitney U tests.
Results: The two groups (unique v epidemic) (n=20 patients both groups) were well matched for mean age (28.5 v 28.0 years), percentage predicted (%) FEV1 (44.4 v 45.7), %FVC (60.1 v 67.0) and BMI (20.8 v 20.4). The two groups had similar mean (SD) WCC (10.3 (2.8) v 11.5 (3.3)) and neutrophil (7.4 (2.8) v 7.6 (3.1)) counts. There were no significant group differences in median (range) levels of sputum NE (22.0 (10.5 to 38.6) v 17.3 (7.1 to 173.5) μg/ml), IL-8 (13 449 (5521 to 56514) v 9989 (3782 to 155 500) pg/ml), and TNFα (11 (0 to 169) v 9 (0 to 278) pg/ml), plasma IL-6 (5.8 (1.3 to 25.7) v 6.4 (1.2 to 38.8) pg/ml) and NE/α1-antitrypsin complexes (246 (109 to 2115) v 229 (118 to 533) ng/ml), serum CRP (8 (1 to 29) v 8 (1 to 71) mg/L) and urine TNFr1 (1167 (286 to 3531) v 988 (286 to 5082) pg/ml).
Conclusions: There are no differences in levels of inflammatory markers between clinically stable adult CF patients who harbour epidemic and unique strains of P aeruginosa.
P109 A PSEUDOMONAS AERUGINOSA EXOTOXIN, PYOCYANIN, IMPAIRS PHAGOCYTOSIS AND CLEARANCE OF APOPTOTIC CELLS
S.M. Bianchi, L.R. Usher, D.H. Dockrell, G.W. Taylor, M.K.B. Whyte. Respiratory Medicine Unit, University of Sheffield, Sheffield, UKPseudomonas aeruginosa infection in patients with cystic fibrosis and bronchiectasis is characterised by a profound neutrophilic inflammation, with neutrophil products (for example, elastases) implicated in tissue injury. We have shown that pyocyanin, a pseudomonas exotoxin, accelerates neutrophil apoptosis (programmed cell death) potentially promoting bacterial persistence (
). We hypothesised that accelerated neutrophil death may result in further tissue injury if apoptotic cell clearance was impaired. We therefore studied the effects of pyocyanin on the ingestion of apoptotic neutrophils (APMN) by monocyte-derived macrophages (MDM). All data are expressed as controls versus 24 hour pyocyanin pretreatment. We have observed a time (100 (0%) v 22.7 (7.1%), p<0.001) and concentration dependent reduction in MDM ingestion of APMN in the presence of pyocyanin. We have shown that the reduced interaction is not due to loss of viability (23.2 (2.5) v 22.7 (1.2) cells/x400 field, p=0.440) or induction of MDM apoptosis by physiological concentrations of pyocyanin (0.6 (0.15%) v 0.93 (0.41%), p=0.108). Similarly we have demonstrated no loss in MDM function as assessed by basal and lipopolysaccharide induced MDM cytokine production. The impairment of phagocytosis has been shown to be specific to APMN as MDM phagocytosis of opsonised latex bead is not impaired (33.3 (4.2%) v 29.7 (2.3%), p=0.312). Also we have determined that the pyocyanin-induced defect is specific to the MDM—APMN killed by constitutive ageing or following exposure to pyocyanin are ingested similarly by healthy MDM. Using flow cytometry we have shown that pyocyanin is capable of inducing high levels of reactive oxygen species (ROS) within the MDM—however it does not appear that this mechanism is responsible for the defect as alternative sources of ROS (for example, hydrogen peroxide) do not result in similar impairment of phagocytosis, and antioxidants are unable to recover phagocytic capacity. We conclude that pyocyanin reduces MDM phagocytosis of APMN in vitro. This represents a novel mechanism by which microorganisms may contribute to immune evasion, bacterial persistence, ongoing inflammation, and lung injury.
P110 BURKHOLDERIA CEPACIA COMPLEX: A MULTILOCUS SEQUENCE TYPING (MLST) SCHEME BASED APPROACH
K.M. Thickett1 2, E. Mahenthiralingam3, D. Honeybourne1 2, C.G. Dowson2. 1Adult Cystic Fibrosis Unit, Department of Respiratory Medicine, Heartlands Hospital, Bordesley Green East, Birmingham, B9 5SS, UK; 2Department of Biological Sciences, University of Warwick, Coventry, CV7 4AL, UK; 3Cardiff School of Biosciences, Main Building, Museum Avenue, PO Box 915, Cardiff University, Cardiff, Wales, UK
The accurate identification of Burkholderia cepacia complex in cystic fibrosis (CF) is challenging. A polyphasic taxonomic approach is often employed in the study of B cepacia complex, including total protein electrophoresis, fatty acid analysis, biochemical tests, PCR amplification of rDNA, random PCR amplification (RAPD), pulse-field gel electrophoresis, and ribotype analysis. However, molecular diagnostic probes based upon the polymerase chain reaction (PCR) provide a rapid and frequently highly discriminatory means of identifying microbial infection. Recently recA sequence analysis has helped to unravel the phylogenetic relationships within the B cepacia complex and has formed the basis for a rapid PCR based identification of B.cepacia complex genomovars.1 Multi locus sequence typing (MLST) is a powerful, portable and rapid means of undertaking identification, typing and population genetic analysis and enables population based analyses not possible by pulse field gel electrophoresis (PFGE) or other macrorestriction profiling and allows the establishment of a world wide data base for the unambiguous identification of different strains. We have currently developed six loci for use in an MLST scheme for B cepacia complex including RecA, recA, beta subunit of ATP synthase atpd, poly-hydroxyalkoanoate polymerase phaC, glutamate synthetase (NADPH) large chain precursor, gltB, DNA gyrase β subunit, gyrB and GTP binding protein lepA. Southern blotting of whole chromosomes and restriction digests of total chromosomal DNA from B cepacia complex, (B cepacia genomovars I and III, Burkholderia multivorans, Burkholderia stabilis, and Burkholderia vietnamiensis) has been used to confirm the presence of loci as single copies. We describe preliminary phylogenetic relationships from these loci using isolates widely distributed across a recA phylogenetic tree.
1.
.
P111 STRAIN DEPENDENT SYSTEMIC INVASION AND INFLAMMATION IN A MURINE MODEL OF ACUTE PULMONARY Burkholderia cepacia infection
J.C. Davies1 2, R. Shaw1, T. Lloyd1, D.M. Geddes1, E.W.F.W. Alton1. 1Dept of Gene Therapy, Imperial College; 2Dept of Paediatric Respiratory Medicine, Royal Brompton Hospital, London, UKBurkholderia cepacia infection in CF may be asymptomatic, adversely affect lung function or invade systemically leading to the potentially fatal “cepacia syndrome”. Certain genomovars appear more detrimental than others, possibly related to invasiveness and pro-inflammatory activity: cepacia syndrome has been reported with GII and GIII organisms, and GIII infected lung transplant recipients have increased mortality. To explore this further, we tested a variety of B cepacia strains in a murine model of acute pulmonary infection. C57Bl/6 mice (6/group) were infected by nasal sniffing with 109 CF organisms including: 18822 & 13010 (GIIa&b), ET12 (GIII), and 18870 & 14294 (GIVa&b) (BCCM/LMG, Belgium). Forty eight hours later blood was obtained by abdominal venesection, the spleen was removed, and a BAL performed. Homogenised spleens were cultured in a semi-quantitative fashion on cepacia-specific medium. Growth was scored as 0 (negative), 1 (scanty colonies), 2 (multiple colonies), or 3 (confluent growth). Consistently high levels of systemic invasion were seen in animals infected with GIII and GII strains (scores of 3 in every animal). In contrast, the GIV strains produced less frequent and lower levels of invasion (mean (SEM) score GIVa 0.8 (0.4), GIVb 1.7 (0.2); p<0.05 compared with other infected groups). BAL neutrophil counts were higher in all infected groups than in PBS controls (p<0.05 or less), the highest levels being in groups GIII and GIIb. ET12 was significantly more pro-inflammatory than all the other strains, when the cytokines TNFα, IL-6, and IL-1β were measured both in BAL and serum. Although the GII strains were more invasive than the GIV, this was not reflected by differences in these ctyokines. This animal model confirms a differential host response to various B cepacia organisms, which appears to be related both to genomovar and strain. Strains from GII and GIII, those associated with cepacia syndrome in patients, were highly invasive. Further, the GIII organism elicited the greatest inflammatory response, both locally and systemically, suggesting a mechanism for the reported poor outcome after lung transplantation. Further studies, both in animal models and in the clinical setting are warranted, to improve attempts to identify patients most at risk of disease.
P112 VARIABILITY IN PRO-INFLAMMATORY ACTIVITY OF PURIFIED LIPOPOLYSACCHARIDE (LPS) FROM SELECTED Burkholderia cepacia genomovars; the role of LPS structural differences and chemotype
A. De Soyza1 2, R. Demarco De Hormaeche2, P. Corris1. 1Lung Biology and Transplantation group, University of Newcastle upon Tyne; 2Freeman Hospital and Department of Microbiology and Immunology, University of Newcastle upon Tyne, UK
Gram negative bacterial infections are a major cause of morbidity in adult cystic fibrosis patient. As compared to those infected with Ps aeruginosa alone the outcomes of Burkholderia cepacia infected patients are poorer. There also appears to be variability in outcomes within the B cepacia infected population (Frangolais, et al. Am J Respir Crit Care Med 1999). The most striking disease pattern is Cepacia Syndrome a fatal pneumonitis-sepsis syndrome. There are many host and pathogen factors which may contribute to this variability. The designation of closely related but distinct species, Genomovars I to VII, within the B cepacia complex may offer some insights into this variable pattern. Genomovars III, II, and V are the most prevalent in CF. We have shown poor outcomes in Genomovar III infected patients post-transplant (De Soyza, et al. Lancet 2001). As lipopolysaccharide (LPS) is a major mediator of sepsis we have investigated the pro-inflammatory potential of B cepacia LPS.
Methods: We selected three strains of B cepacia after pilot work suggested widely varying biological activity. These strains, GII (LMG 14273 and 13010) and GIII (LMG12614, an ET12 clone), were grown overnight and harvested. The bacteria were sonicated and treated with DNAse and proteinase K. LPS extraction using hot phenol was undertaken with final DNA/ protein contamination approx 5%. The purified LPS (1–100ng) were added to differentiated U937 macrophages and the tissue culture supernatants were collected at 0 and 24 hrs. Time course experiments were also undertaken up to 48 hrs. The supernatants were tested for septic shock related cytokines IL-1, IL-6 and TNF using ELISA. We silver stained 16% urea/SDS-PAGE gels to assess LPS structure.
Results: A dose-response was seen. The greatest difference was noted between the purified LPS at a dose of 100ng for TNF induction where LMG 12614 (ET12) was twice as effective at induction as compared to LMG 14273 (GII). LMG 13010 (GII) was as effective as the GIII, LMG12614. The gels confirmed that all were of rough LPS chemotype. The two high cytokine inducers LMG12614 and 13010 (GIII and GII) appeared to have the same LPS banding patterns; rough LPS with two distinct bands whilst LMG 14273 a distinct LPS pattern.
Conclusions: The observed differences between B cepacia complex strains LPS may in part explain the variable clinical outcomes. We identified differences between genomovars demonstrating that within the two most common genomovars there is a wide spectrum of activity. One GII strain appears to have the same LPS as the ET-12 GIII strain which may explain why some GII patients can develop Cepacia Syndrome. The chemotype of the LPS e.g. rough or smooth may be less important than the structural motifs within each LPS.
P113 LIPOPOLYSACCHARIDE STRUCTURAL PROFILES ARE NOT ALTERED IN GENOMOVAR III Burkholderia cepacia quorum sensing knockouts
A. De Soyza, R. Demarco De Hormaeche, P. Corris. Lung Biology and Transplantation group, University of Newcastle, Freeman Hospital and Department of Microbiology and Immunology, University of Newcastle upon Tyne, UK
Background: Attempts at creating vaccines using isolated bacterial antigens have been relatively unsuccessful for many important pathogens such as Pseudomonas. Gram negative bacteria form biofilms in cystic fibrosis lungs that appear to protect bacteria within the biofilm from antibiotics even at bactericidal levels. The maturation of biofilms is dependent on quorum sensing systems. Quorum sensing mutants produce greatly attenuated infections in animal models and may offer the possibility of an attenuated strain (perhaps with additional mutations in virulence genes) for use as a biological vaccine. Recent data has shown that quorum sensing also controls virulence related genes for proteases and iron binding siderophores. The effect of quorum sensing on a major bacterial pro-inflammatory moiety, lipopolysaccharide (LPS) is less clear. Work with Pseudomonas aeruginosa has demonstrated that migA a lipid A glycosyltransferase, has a quorum sensing box upstream. There is no data in the Cepacia field assessing the effect of quorum sensing knockouts on LPS structure. Two Burkholderia cepacia quorum sensing mutants, H111-I and H111-R have been created that are defective in the acylhomoserine lactone (AHL) synthase cepI and the AHL receptor cepR respectively. The effect of these mutations are to impair biofilm formation. These strains therefore may be potentially considered for investigation as starting points for biological vaccines. The effect of these mutations on LPS is however unclear.
Methods: The wild type parent genomovar III, strain H111 and the two mutants were kindly gifted (Dr B Huber, University Munich). These were grown in Luria Broth (LB) with appropriate selective antibiotics over 24 hours at 37°C. The organism were then centrifuged and resuspended to a standard optical density at 600nm of 0.2. SDS-PAGE was conducted with subsequent silver staining to assess any changes in LPS profiles.
Results: Silver stained SDS-PAGE gels revealed the LPS of all three strains were of smooth chemotype with multiple bands suggesting variable O side chain lengths. There were however no differences between the strains in terms of number or pattern of the bands seen on the gels suggesting the O chains of the LPS were not affected by the quorum sensing mutations. There appeared to be no differences in the LPS core. As opposed to data from Pseudomonas spp quorum sensing B cepacia mutants with smooth LPS do appear to have a change in LPS structure under the above growth conditions.
Conclusions: If quorum sensing mutants are to be considered as starting points for biological vaccines it may be important to create quorum sensing mutants in a wild type genomovar III strain with a LPS that has a low inflammatory potential.
Cystic fibrosis: Treatments and outcomes
P114 COMPARISON OF THE HALOLITE™ ADAPTIVE AEROSOL DELIVERY (AAD™) SYSTEM WITH A HIGH OUTPUT NEBULISER SYSTEM IN CYSTIC FIBROSIS PATIENTS
R.J. Marsden1, S.P. Conway2 , M.E. Dodd3 , F.P. Edenborough4, A.S. Rigby5, C.J. Taylor5, P.H. Weller6. 1Profile Therapeutics, UK; 2St. James’ Hospital, Leeds; 3Wythenshawe Hospital, Manchester; 4Northern General Hospital, Sheffield; 5Sheffield Children’s Hospital, Sheffield; 6The Birmingham Childrens’ Hospital, Birmingham, UK
The HaloLite AAD system (AAD) has been developed to improve inhaled medication delivery by giving feedback during and at the end of treatment. It will not deliver aerosol during nose breathing, talking, or if there is a poor mouthpiece lip seal. A multicentre randomised parallel study (MAL 25 –70) comparing AAD with conventional high efficiency nebulisers (NEB) was conducted at CF centres in Australia, Canada, USA, and Europe. Patients established on DNase and inhaled antibiotics were randomised to AAD or NEB within seven days following an exacerbation requiring oral or IV antibiotics. Patients used the study device to take their inhaled medications for 182 days. The primary outcome variable was change in FEV1 from day 0–182. Secondary outcome variables were days antibiotic use, exacerbation frequency, time to first exacerbation, safety, adherence to prescribed regimen, and compliance with device (by overt electronic monitoring in 20% of the sample). Patients completed a questionnaire to assess device acceptability.
259 patients were randomised (133 AAD, 126 NEB) median age 17 years, median FEV1 56% predicted. Preliminary analysis of mean change in % predicted FEV1 from baseline to day 182 was −3.5% for AAD and −2.4% for NEB. Difference in means = 1.1% confidence interval = −4.2% to 6.3%, p=0.7. There was no statistically significant difference between AAD and NEB for the secondary outcome variables except for a higher incidence of chest tightness per 1000 days (0.97 for AAD and 0.32 for NEB (p<0.05)). Completed questionnaires showed that compared to their previous nebuliser 69% of AAD patients felt that they received more dose compared to 30.4% for NEB; 56% of AAD patients felt better compared to 30% for NEB; 82% of AAD patients preferred the trial device compared to 37% for NEB. These differences were significantly different (p<0.0001). Fifty one per cent of prescribed doses were taken beyond 90% of the programmed dose for AAD compared with 26% of prescribed doses where the compressor was run for >6 minutes for NEB (p<0.006).
Conclusions: There were no differences in the efficacy outcome variables between the devices. A higher incidence of chest tightness for AAD may be indicative of more successful delivery of antibiotic to the lung. Patient acceptability of the device was better for AAD than for NEB. Patients take more doses to an acceptable level using AAD.
P115 COMPLIANCE IN CYSTIC FIBROSIS PATIENTS USING TWO DIFFERENT AEROSOL DELIVERY SYSTEMS
S.P. Conway1, M.E. Dodd2, R.J. Marsden3, P.H. Weller4. 1St. James’ Hospital, Leeds, UK; 2Wythenshawe Hospital, Manchester, UK; 3Profile Therapeutics, UK; 4The Birmingham Childrens’ Hospital, Birmingham, UK
CF patients may use conventional high output nebulisers (NEB) for up to an hour a day to aerosolise therapies aimed at preserving lung function. Poor techniques such as nose breathing, talking and inadequate lip seal compromise the time spent breathing correctly on the mouthpiece1 and hence the amount of drug delivered to the lungs. HaloLite (AAD) has been designed to generate aerosol only whilst patients breathe correctly through the mouthpiece. The system provides feedback to the patient during treatment and signals once the pre-programmed dose has been successfully delivered. The aim of this study was to compare compliance with AAD to compliance with NEB.
Patient Logging System (PLS) monitoring technology was used in a device study comparing AAD with NEB to overtly monitor 50 of 259 patients (from study MAL 25–70) over 182 days. “Adherence” (doses started/by the number of doses prescribed) and “compliance” (the % of doses taken correctly) were recorded. For AAD a correctly taken dose was defined as delivery of >90% of the pre-programmed dose, and for the NEB when the Porta-Neb™ PLS compressor was run for >6minutes. “True compliance” is adherence X compliance. FEV1 was recorded on day 0 and 28. The use of oral or IV antibiotics was recorded on day 0 and 28. The sample included 30 AAD and 20 NEB patients. Provisional data shows that adherence was 62% for AAD and 47% for NEB (p>0.05). Compliance was 84% for AAD and 43% for NEB. “True compliance” was significantly higher for AAD (51%) compared to NEB (27%) (p=0.006). For NEB there was no correlation between true compliance and % change in FEV1 after 28 days, neither was there a correlation between true compliance and % of change in FEV1 for the subgroup of patients who did not need oral or IV antibiotics for an exacerbation (n=14). For AAD there was no correlation between true compliance and FEV1 , however for the subgroup of patients who did not need oral or IV antibiotics for an exacerbation there was a correlation between % change in FEV1 and true compliance for AAD (n=17) (R=0.53) (p<0.03).
Conclusion: These data show that the AAD system increases true compliance and may contribute to the maintenance of FEV1.
1. Denyer J, et al. Does inhalation duty cycle in-vitro predict inhaled dose during domiciliary nebulizer use? Drug delivery to the lungs VIII 1997.
P116 PORTACATH COMPLICATIONS IN CYSTIC FIBROSIS PATIENTS
M. Suresh, W. Lenney, G. Hooper, C. Mayer, J. Forrest, A. Walsh. Academic Dept. of Child Health, North Staffs. Hospitals Trust, Staffs, UK
Introduction: Cystic fibrosis (CF) patients requiring repeated intravenous antibiotic courses eventually benefit from insertion of permanent vascular catheters such as a Portacath. There is little information on complications arising from such procedures, which need to be taken into consideration when discussing the relative merit with patients and parents.
Patients: Over a 12 year period out of a population of 78 patients 18 (six male, 12 female) have received 30 Portacaths. Ten patients were <18 years old, 11 have only needed one Portacath to date, three have required two, two have needed three, and two have received four Portacaths.
Results: Average length of use: 36.7 months. Longest surviving Portacath: 8 years 10 months. Reasons for failure: Catheter disconnection one, systemic/infective complications three, lung collapse one, leakage four, blockage with pain six. Short survival of the first Portacath is a marker for failure with subsequent Portacaths.
Discussion: Complications are relative frequent and unpredictable. Our findings are similar to others in CF and oncology patients. Needle-phobia is a common experience in CF Clinics but the use of Portacaths needs full discussion with families and should not be entered into lightly.
P117 ANTIBIOTIC RELATED RENAL IMPAIRMENT IN ADULT CF PATIENTS
M. Al-Aloul, B. Govin, P.A. Stockton, M.J. Ledson, M.J. Walshaw. Regional Adult CF Unit, The Cardiothoracic Centre, Liverpool, UK
Colonisation with multiresistant Pseudomonas aeruginosa (Pa) in CF results in repeated use of a limited number of antibiotics to which the organisms are sensitive, increasing the risk of toxic effects. In Liverpool, we have a multiresistant strain colonising many CF patients that is only sensitive to aminoglycosides and polymyxins, antibiotics that are known to cause renal damage that may be associated with excess levels and also cumulative lifetime dose. To assess the impact of repeated dosing with these antibiotics, we have compared renal function in those colonised with multiresistant Pa with a group of CF patients with similar clinical parameters but who are colonised by sensitive Pa strains. Overall, 52 patients (32 multiresistant) were studied (mean age (range): multiresistant 23.6 years (15 to 42) v sensitive 24.9 (18 to 37); FEV1 % predicted: 61.3 (16 to 95) v 61.8 (17 to 115); BMI: 21.6 (18 to 28) v 20.6 (14 to 27); CF related diabetes: 9 v 4 (all P=NS)). During exacerbations, all patients had aminoglycoside levels measured and adjusted after the 4th dose as per protocol and no episodes of acute toxicity were noted. Renal function was measured by estimation of serum urea and electrolytes and 24 hour urinary creatinine clearance when patients were in a stable clinical state. Patients produced satisfactory 24 hour urine collections, demonstrated by sufficient urine volume and total urinary creatinine excretion. All patients had serum creatinine and urea levels within the normal range, but those colonised with multiresistant strains had a lower creatinine clearance (mean 75 mls/min (range 11 to 115) v 101 mls/min (28 to 171)), (p<0.002), and had received more IV aminoglycoside courses (mean 23 per patient (range 0 to 100)) v (8 (0 to 30)), (p<0.007)), and more IV colomycin courses (22 (0 to 80) v 7.4 (0 to 50)), (p<0.006)). Also, the total number of IV courses correlated with worsening renal function (r=0.39, p<0.001). We conclude that repeated dosing with these potentially nephrotoxic drugs has damaged the renal function in those patients colonised by multiresistant Pa strains, and in some patients we can now no longer use these important antibiotics. This study illustrates the need to prevent colonisation by such strains if possible in CF patients. This is best achieved by measures designed to prevent cross infection, including suitable patient segregation.
P118 VARIATION IN REPORTED INTAKE OF PANCREATIC ENZYME REPLACEMENT THERAPY IN ADULTS WITH CYSTIC FIBROSIS
S. Thornton, S. Kelly, F. Edenborough. Adult Cystic Fibrosis Unit, Northern General Hospital, UK
Background: Pancreatic Enzyme Replacement Therapy (PERT), the number of enzymes taken with food, is assessed as part of the annual review. In this centre both the doctor and dietitian review independently, however it is the amount each patient reports to the doctor which is recorded on the UK National Cystic Fibrosis (CF) database.
Aim: To investigate whether reported intakes of PERT capsules differ when assessed by dietitian, doctor, or using a food diary.
Methodology: Patients attending their annual review at the CF Centre between July 2000 to May 2002 were asked the number of PERT capsules they consumed with meals, snacks, nutritional supplements, drinks etc each day. This is the recall method and is recorded by the dietitian (in conjunction with diet history) and the doctor on the same day. Patients are also requested to complete at least a three day food diary (two weekdays and one weekend day). They record the quantities and types of food, fluid and PERT consumed on those days. The numbers of PERT recorded by each method were compared.
Results: There was significantly less PERT intake reported using the recall method by dietitian, 3.6 ± 10.3 enzymes (p=0.04, t Test) compared to the database documented value (doctor).
The number of enzymes recorded on the food diaries was also lower than the database documented value (doctor), 3.8 ± 9.1 enzymes but was not significant (0.07, t Test).In addition, there is considerable variation in the number of PERT capsules reported using each method (table).
Conclusion: The actual over reporting of enzyme intake for the UK CF database is slight overall, however for an individual patient the report can vary by over 100% difference. It is also shown that 40% of patients are more than 25% inaccurate in their reporting. This may have implications for their individual enzyme assessment and monitoring. In light of this evidence we suggest that consideration is made to the method of assessment used.
P119 INTRAVENOUS ANTIBIOTICS INCREASE EXHALED NITRIC OXIDE IN CHILDREN WITH CYSTIC FIBROSIS
A. Jaffé, G. Slade, J. Rae, A. Laverty. Portex Respiratory Unit, Great Ormond Street Hospital for Children & Institute of Child Health, London, UK
Introduction: Data on the effect of intravenous (IV) antibiotics on exhaled nitric oxide (NO) in CF and on correlation of NO with lung function are conflicting because of lack of standardisation for the measurement of NO.
Aims: To assess the effect of IV antibiotics on exhaled NO in CF children and to correlate NO with lung function. Methods: Exhaled NO was measured on line during a slow exhalation according to ATS guidelines using an exhalation flow of 50 mL/s (NiOX, Aerocrine,) in CF patients admitted for IV antibiotics. Pulmonary function was measured according to ATS guidelines (Masterscreen, Jaeger). Measurements before and after treatment were compared by Wilcoxon Signed Ranks Test. Spearman correlation tests were used to assess correlation. A value of p<0.05 was considered significant.
Results: Fourteen CF subjects (10 female), median age (range) 12.1 years (5.9 to 16.0) were studied. Genotypes were as follows: ΔF508/ΔF508, n=10; ΔF508/N1303K, n=1; ΔF508/−, n=3. Reasons for admission were: infective exacerbation, n=4; routine quarterly antibiotics, n=10. Cough swab or sputum culture on admission: Pseudomonas aeruginosa, n=6; Staphylococcus aureus, n=6 (one had coliforms and one had Stenotrophomonas maltophilia in addition); no growth, n=2. Median (range) length of treatment was 8.5 (6–15) days. There was a significant improvement in mean (SEM) %FEV1 from 60.0 (6.3) to 68.0 (5.4) (p=0.02) and %FVC from 66.3 (5.5) to 75.1 (4.9) (p=0.003). There was a significant increase in NO following treatment (median (range): pre; 5.8 ppb (2.0 to 14.3), post; 9.2 ppb (0.8 to 25.1), p=0.02). There was no correlation between NO and %FEV1 or %FVC.
Discussion: NO is raised in lung diseases with an inflammatory component, however this is not true for CF, and is further supported by these results. Various hypotheses have been proposed to account for this. These include: entrapment in sputum; degradation by superoxide production from activated neutrophils; NO reductase in P aeruginosa; reduced inducible NO synthase expression in epithelial cells. Our results support these hypotheses as it is likely that antibiotic treatment results in a reduction in P aeruginosa colony forming units, neutrophil activation and airway sputum volume.
Conclusion: IV antibiotics increase exhaled NO in CF. However, NO does not correlate with lung function and is not a useful marker of lung disease in CF.
P120 FACTORS DETERMINING DIAPHRAGM STRENGTH IN CHILDREN AND YOUNG ADULTS WITH CYSTIC FIBROSIS
N. Hart1 3 5, P. Tounian2, M.I. Polkey3, A. Clement1, J. Moxham4, F. Lofaso5, B. Fauroux1. 1Paediatric Pulmonary Department; 2Gastroenterology Department, Armand Trousseau Hospital, Paris, France; Respiratory Muscle Laboratories, 3Royal Brompton Hospital; 4Kings College Hospital, London, UK; 5Department Of Clinical Physiology, Raymond Poincare Hospital, Garches, France
Respiratory failure is the major cause of death in patients with cystic fibrosis (CF). Although the diaphragm is the most important muscle of inspiration, it is unclear as to whether there are any alterations in diaphragm strength in patients with cystic fibrosis (CF). In the current study, we hypothesised that diaphragm strength would be determined by airflow obstruction and pulmonary hyperinflation, gas exchange impairment, inspiratory muscle load, and nutritional status of the patient. 20 patients with CF were studied (mean age 15.1 (2.8) years). We measured twitch transdiaphragmatic pressure (Tw Pdi) in response to bilateral anterior magnetic phrenic nerve stimulation to quantify diaphragm strength; forced expiratory volume in 1 sec (FEV1) and functional residual capacity (% Pred FRC) as estimations of airflow obstruction and hyperinflation; and diaphragm pressure time index (PTIdi) as an indicator of diaphragm load. Nutritional status was evaluated using body mass index adjusted for age and sex (BMI z-score), fat mass (FM), fat-free mass (FFM) and arm-muscle circumference (AMC). These were determined from measurements of height, body weight, mid-arm circumference (AC), and skinfold thickness (SK) at four different sites (biceps, triceps, subscapular, and suprailiac). FM and FFM were calculated from SK and weight. AMC was calculated from the formula AC − (0.134 * biceps SK/2 + triceps SK/2). FM, FFM, and AMC were expressed as percent predicted for statural age (% PredSA). Results are expressed as mean (SD). Tw Pdi was 24.3 (5.5) cmH2O; % Pred FEV1 was 44.5 (21.4); % Pred FRCpl was 159.8 (40.9); Pao2 was 9.5 (1.5) kPa; Paco2 was 5.5 (0.6) kPa; and PTIdi was 0.05 (0.03). Univariate regression analysis demonstrated Tw Pdi correlated with % Pred FEV1 (p=0.001; r = +0.68); % Pred FRCpl (p=0.005; r = -0.65); Pao2 (p=0.001; r = +0.68); Paco2 (p=0.03; r = −0.50); BMI z-score (p=0.003; r = +0.63); % PredSA AMC (r = +0.45; p=0.04); and % PredSA FFM (r = +0.47; p=0.04). There were no correlations between Tw Pdi and % PredSA FM (p=0.1) and PTIdi (p=0.2). In conclusion, in children and young adults with CF, diaphragm strength falls as airways obstruction and hyperinflation increases, gas exchange impairment worsens, and nutritional status declines. However, load does not have effect of diaphragm strength.
Dr N Hart was supported by the Scadding-Morriston Davies Joint Respiratory Medicine Fellowship, a European Respiratory Society Long Term Fellowship and a grant from the Association Française Contre Les Myopathies.
P121 INCREASED ENERGY EXPENDITURE DUE TO COUGHING IN ADULTS WITH CYSTIC FIBROSIS
A.A. Ionescu, R. Colasanti1, L.S. Nixon, C.E. Bolton, M. Williams1, D.J. Shale. Section of Respiratory Medicine University of Wales College of Medicine; 1School of Applied Sciences University of Glamorgan, Cardiff, UK
Patients with Cystic Fibrosis (CF) have increased resting energy expenditure (REE). We hypothesised that frequent coughing, occurring spontaneously and during physiotherapy in most patients, adds to the REE and overall energy expenditure (EE), which may contribute to weight loss.
We measured breath by breath REE (K4b, Cosmed) in 12 clinically stable patients and 10 healthy subjects. A steady state baseline was recorded and each subject coughed voluntarily three times after breathing in to TLC. A further 10 patients had REE measured on repeated occasions by the same method. During 45, 10minute recordings of REE 144 spontaneous coughs occurred. The REE before coughing occurred and after each coughing episode was recorded. The mean recovery time (VE, l/min back to baseline) after the three voluntary coughs (41 seconds) was used to calculate the EE after spontaneous coughing as the area under the curve after each cough by locally designed software. We also compared the REE after spontaneous coughs to the baseline REE, because the duration of the baseline record was variable (mean 106, maximum 371, minimum 8 seconds). There was no difference in EE after three coughs (ratio to baseline), between patients and healthy subjects (p>0.05). The FEV1 (patients) was inversely related to EE after three coughs, r =−0.0.58, p=0.04. Recovery time was similar to the healthy subjects. Spontaneous coughs in patients increased the EE by a mean (95% CI) 7.9 (2.7 to 13.3) % compared with baseline, mean (95% CI) 32.63 (30.51 to 34.75), and 30.66 (28.59 to 32.73) kcal/kg/min, p<0.01. The REE (area under curve over time) with spontaneous coughs was greater than REE recorded when spontaneous coughs were removed from the 10 minutes measurement; mean (95% CI) 28.0 (24.7 to 31.3) and 21.5 (18.6 to 24.3), respectively, p=0.016.
Cough increased the REE in adults with CF. For accuracy REE measurements in CF should include any spontaneous coughs that occur. Due to the frequency of coughing, the energy costs are likely to increase the negative energy balance in some patients.
Sponsored by the Cystic Fibrosis Trust UK.
P122 SEQUENTIAL SINGLE LUNG TRANSPLANTATION FOR SEPTIC LUNG DISEASE; A SINGLE CENTRE COMPARISON BETWEEN CF AND NON-CF BRONCHIECTASIS
A. De Soyza1, K. Gould 2, G. Parry3, J.H. Dark3, P.A. Corris1 3. 1Lung Biology and Transplantation Group; 2Department of Microbiology; 3Cardiothoracic Transplantation, Freeman Hospital, University of Newcastle, Newcastle upon Tyne, UK
Background: The outcomes for transplantation for septic lung conditions including Cystic Fibrosis (CF) and non-CF bronchiectasis have been comparable to those for non-septic lung conditions despite the additional risks associated with these conditions. Given the current organ donor shortage it is important to compare outcomes for each pre-transplant outcome within a single centre to allow appropriate allocation of organs. It is recognised that certain pre-transplant indications such as Pulmonary Fibrosis and Pulmonary Hypertension are associated with poor transplant outcomes. We have not previously compared the outcomes of Cystic Fibrosis and non-CF Bronchiectasis at this centre.
Methods: We identified all patients receiving lung transplants at this centre for septic lung diseases through our transplant database. A survival table was constructed and the two groups were compared using the log rank (Mantel-Cox) test for real survival. Pre-transplant recipient characteristics were also compared including pre-transplant body mass index, pre-transplant FEV1, need for non-invasive ventilation and median time post transplant.
Results: We have transplanted 96 CF patients and 26 non-CF Bronchiectatics (NCFBr) over 10 years. Median age at transplantation CF group 25.4 yrs (range 16 to 49.5) and NCFBr median 48 yrs (range 25 to 56) p<0.05. Survival was comparable between groups at one year CF 81%, NCFBr-76.5% p=0.46. At five years survival was 70% for CF and 72% for NCFBr p=NS. Pre-transplant FEV1% predicted was similar between groups median in the CF group =19.1% (range 8 to 35%) and NCFBr 18 (9 to 49%) p=NS. In each group early deaths were predominantly related to sepsis: The early deaths were due to sepsis in the CF group (9/96) and also in the NCFBr group 13% (4/29) Fishers exact test p=0.3. Median pre-transplant Body mass index (BMI - kg/m) was 17.8 (range 12 to 24) for CF and NCFBr =23 (range 16 to 32), Mann Whitney, p<0.01. No patient in the Bronchiectasis group required non-invasive ventilation pre-transplant whilst 11/96 CF patients had NIV pre-transplant Fisher exact test p=0.11. Similarly there were 12/96 CF patients infected with Burkholderia cepacia complex organisms whilst no NCFBr were infected with this organism p=0.11 pre-transplant Fisher exact test p=0.11.
Conclusions: Cystic Fibrosis patients had poorer pre-transplant nutrition and were more likely to be infected with B cepacia complex. There were however no statistical differences in post transplant survival noted. We conclude that despite these features CF patients are as likely to benefit from pulmonary transplantation than older non-CF bronchiectasis patients.
P123 RECOMBINANT SENDAI VIRUS-MEDIATED CFTR cDNA TRANSFER
S. Ferrari1–4, R. Farley1–4, F. Munkonge1–4, U. Griesenbach1–4, S. Smith1–4, J. You2, A. Iida2, B. Wainwright3, D. Geddes1–4, M. Hasegawa2, E. Alton1–4. 1Department of Gene Therapy, NHLI, London, UK; 2DNAVEC Research Inc, Japan; 3University of Queensland, Brisbane, Australia; 4UK CF Gene Therapy Consortium, Edinburgh-London-Oxford, UK
To assess applicability for Cystic Fibrosis (CF), recombinant Sendai virus (SeV) carrying the CFTR gene was tested on different models of airway epithelial cells. In vitro CFTR activity was assessed at two days post-infection in murine mammary epithelial cells (C127 −/−) using a radioactive iodide efflux assay after challenge with forskolin/IBMX (F/I). Cells infected with a SeV vector carrying a mutated CFTR sequence (SeV-mCFTR) were used as controls whilst T84 were used as positive controls and results expressed as Δk .min-1 (s.e.m). T84 cells showed maximal efflux rate 2 min after F/I addition (0.24 (0.02), n=30) compared to C127 −/− values (0.004 (0.004), n=11), p<0.001. All three SeV-CFTR clones tested showed a characteristic delayed peak three minutes after F/I addition (SeV-CFTR 23–3 (0.34 (0.04), n=12); SeV-CFTR 23–4 (0.26 (0.03), n=6); SeV-CFTR 1–3 (0.16 (0.05), n=12). As for untreated C127 −/− cells, treatment with SeV-mCFTR did not lead to any change in efflux (−0.01 (0.02), n=12). In vivo experiments were carried out in G551D CF transgenic mice by administration of SeV-CFTR 23–3 and 23–4 (5 x 107 pfu, n=9) through nasal perfusion and CFTR activity analysed at day 2, 7, 14, and 28. SeV-mCFTR (n=9) was used as control. Two days post-infection, NPDlow Cl- values in animals treated with SeV-CFTR 23–3/23–4 (-0.11 (0.97) mV) were significantly (p<0.05) higher (that is, towards non-CF values) than those observed in animals treated with SeV-mCFTR (-3.25 (0.73) mV). NPDlow Cl- in animals treated with SeV-CFTR 23–3/23–4 remained significantly (p<0.05) higher at day 7 (0.20 (0.73) mV as opposed to −1.55 (1.23) mV in controls). Baseline values at day seven for animals treated with SeV-mCFTR (30.8 (3.6) mV) were not different to untreated CF mice, but in mice treated with SeV-CFTR 23–3/23–4 they were not different from those observed in wild type mice (12.1 (1.5) mV, p<0.01 compared to controls). By day 28, baseline and low chloride values had reversed to typical G551D CF mouse values. In conclusion we have shown that SeV can mediate CFTR gene transfer both in vitro and in vivo.
P124 GENE SILENCING THROUGH RNA INTERFERENCE AS PUTATIVE THERAPY FOR CF
U. Griesenbach1 4, S. Escudero-Garcia1 4, R. Farley1 4, S, Cheng2, D.M. Geddes1 4, N.J. Caplen3, E.W.F.W. Alton1 4. 1Department of Gene Therapy, National Heart and Lung Institute, Faculty of Medicine, Imperial College, London, UK; 2Genzyme Corporation, Framingham, USA; 3Medical Genetics Branch, NHGRI, National Institute of Health, Bethesda, USA; 4United Kingdom CF Gene Therapy Consortium, UK
Gene silencing through dsRNA-mediated RNA interference (RNAi) has been described in C elegans and Drosophila. We, and others, have recently described RNAi in mammalian cells mediated by small dsRNAs of 21–23 nucleotides (nts) termed short interfering RNAs (siRNAs) (Caplen NJ, PNAs 2002). Here, we provide preliminary proof of principle that gene silencing through RNAi can be achieved in lung in vivo. Balb/C mice (female 6–8 weeks) were simultaneously transfected with pcDNA3CAT (80μg/mouse ) and 22 nts siRNA corresponding to CAT (40μg/mouse ) or an irrelevant control siRNA, each complexed with the cationic lipid GL67 (n=12 in both groups). Forty eight hours after transfection the lungs were harvested and CAT activity assayed. CAT expression was reduced by 90% in animals treated with CAT siRNA, when compared to controls (control siRNA: 736.9 (437) pg CAT/mg protein, CAT siRNA: 80.1 (31.4) pg CAT/mg protein, p<0.001. A potential confounding factor is the co-transfection of the plasmid and siRNA, allowing for a non-posttranscriptional silencing mechanism of action. To address this, we compared the silencing of the green fluorescent protein (eGFP) using a siRNA against eGFP either in cells co-transfected with eGFP plasmid and siRNA or cells stably expressing a destabilised version of eGFP (eGFPd2) transfected with siRNA alone. The degree of silencing in both cases exceeded 90%. We have recently shown that, in contrast to the liver, uptake of DNA into the nucleus of airway epithelial cells is extremely inefficient in vivo. However, cytoplasmic transfection can be readily achieved. RNAi has been shown to primarily act within the cytoplasmic compartment and so may offer a major advantage over conventional antisense strategies that have been proposed for several disorders. Although the pathophysiology in CF is not completely understood, several proteins may provide good targets for gene silencing, including the epithelial sodium channel (EnaC), as well as several pro-inflammatory cytokines, such as IL-8 and chaperones, which retain delta F508 CFTR within the endoplasmic reticulum.
P125 INFECTION OF THE MURINE LUNG WITH NON-TRANSMISSIBLE RECOMBINANT SENDAI VIRUS EXPRESSING THE SECRETED PROTEIN INTERLEUKIN 10
U. Griesenbach1, T. Shiraki-Iida1 2, S. Ferrari1, H.L. Gautrey1, X. Hou2, A. Iida2, D.M. Geddes1, M. Hasegawa2, E.W.F.W. Alton1. 1Department of Gene Therapy, Faculty of Medicine, Imperial College London, London, UK; 2DNAVEC Research Inc., Tsukuba, Ibaraki, Japan
We have previously shown that a transmission-competent recombinant Sendai virus carrying mouse interleukin 10 cDNA (SeV-IL10) infects the airways efficiently. A second generation, and for human use potentially safer SeV has recently been generated, in which the gene for the membrane fusion protein (F protein) has been deleted from the viral genome (SeV/ΔF) (
). The F protein is essential for virus entry into the cell and is supplied in trans during vector production. However, following infection and virus replication of the vector genome in vivo the virus cannot re-infect neighbouring cells. Here, we assessed the efficiency of F-defective SeV (SeV-IL10/ΔF) in lungs of mice and in primate trachea. The lungs of C57Bl/6 mice were transfected by placing SeV-IL10/ΔF or a SeV-LacŽΔF control virus (7×104 and 7×107 CIU/mouse) as a single 100 μl bolus into the nasal cavity and the solution was sniffed into the lungs. Lung tissue and serum was harvested 2, 7, and 14 days after infection. IL10 production was measured in lung homogenate and serum using standard ELISA. In lung homogenate expression was highest two days after infection and was 2 and 4 logs above control levels for 7×104 and 7×107 CIU/mouse, respectively. At day seven expression in mice transfected with the higher dose had dropped to 1.3% of the day two levels, but only to 13% in the lower dose. At day 14 the lower dose still showed low but significant IL10 expression, whereas the higher dose was not longer different from control levels. High levels of serum IL10 were detected two days after infection with 7×107 CIU/mouse, but not in animals infected with 7×104 CIU/mouse, and were still significantly increased seven days after infection (SeV-IL10/ΔF: 3500 (492) and 75 (18) pg/ml at day two and seven respectively, SeV-LacŽΔF: 5.5 (5.4) and 0 pg/ml at day two and seven respectively, n=6, p<0.05). When compared to the previously used transmission-competent, first generation SeV virus (historical data), there was no difference in IL10 expression in lung homogenate or serum. We also transfected fresh and mucus depleted segments of primate trachea with SeV-IL10/ΔF or a SeV-LacŽΔF control virus (106 and 107 CIU) ex vivo (n=1) and preliminary results indicated efficient transfetion of fresh and mucus-depleted tissue (Fresh: SeV-IL10/ΔF = 405048 pg/mg, ΔFSeV-lacŽ: 3294 pg/mg, Mucus depleted: SeV-IL10/ΔF = 470874pg/mg, SeV-LacŽΔF: 20966 pg IL10/mg protein). In conclusion, the non-transmissible second generation SeV-IL10/ΔF infects airway epithelium as efficiently as the first generation virus. Preliminary results indicate that the virus titre at least in part determines the decline of transgene expression and that SeV-IL10/ΔF infects primate trachea efficiently.
Rehabilitation, symptoms, and smoking
P126 PILOT DATA: PULMONARY REHABILITATION IN RESTRICTIVE LUNG DISEASE
K. Dix, C. Daly, R. Garrod 1 , M. Howard, C. Rayner.
St George’s Hospital NHS Trust; 1School of Physiotherapy St George’s Hospital and Kingston University, UK
Introduction: Pulmonary rehabilitation is a proven therapy for patients with obstructive pulmonary disease , however little is known concerning the effects in patients with restrictive disease. This study reports on data from an seven week, ×2 weekly, “real life” programme of exercise and education in which patients with both restrictive and obstructive disease were admitted.
Methods: Outcome measures were baseline spirometry. Exercise tolerance using Shuttle Walk Test (SWT), health related quality of life using St George’s Hospital Respiratory Disease Questionnaire (SGRQ), mood state using Hospital Anxiety and Depression Scale (HAD).
Results: Sixty seven patients completed the course. Of these patients, 57 had baseline spirometry from which 48 were classified as obstructive; mean FEV1, 1.09 (0.4), FVC 2.5 (0.7) l and 9 restrictive, mean FEV1 1.42 (0.4), FVC 1.8 (0.5) l .
Both obstructive and restrictive patients showed a statistically significant effect of rehabilitation on SWT; mean difference (SD) 47.8 (86.9) (p=0.0005), 91.1 (64.1) m (p=0.002) respectively. However, the difference between the groups (43.3) m was not significant (p=0.16). There were statistically significant improvements in SGRQ (p=<0.001) and depression (p=<0.001) for the obstructive group and a trend in response for the restrictive group.
Conclusion: Low power means we cannot rule out the possibility of type II error for difference in SWT between the groups. Data from an uncontrolled “real life “ study indicates that patients with restrictive disease may show greater improvements in exercise tolerance than obstructive disease. This report highlights the need for baseline spirometry in the assessment and thorough evaluation of pulmonary rehabilitation in differing populations.
P127 OXYGEN COST SCORE FOLLOWING 4 STEP COPD PROGRAMME AND COMMUNITY BASED PULMONARY REHABILITATION
K. Holt, S. Dryden, I. Houghton, I. Eccleston. Wyre Primary Care Trust, Lancashire, UK
Since January 2000 Wyre PCT has been implementing a 4 step COPD Health Improvement Programme (HImP) to ensure correct diagnosis and optimal, guidelines led, therapy. The programme, developed in collaboration with Blackpool Victoria Hospital Chest Clinic, involves spirometry assessment by a mobile spirometry service visiting all General Practices with further assessment and patient management by COPD trained Practice Nurses. Following diagnosis (step 1), inhaled steroid trial (step2), anticholinergic trial (step 3), and long acting β 2 trial (step 4), community based pulmonary rehabilitation (PR) is now (since July 2001) offered to those patients motivated to attend. PR, led by a Physiotherapist and a Respiratory Nurse, is offered at two sites in the PCT; a Local Authority Sports Centre and a Village Community Centre. Patients attend for two hours twice a week for eight weeks and are then invited to attend one hour a week for ongoing supervised exercise. The Oxygen Cost Score (OCS) is used to assess breathlessness by functional ability at each stage of the HImP and PR programme.
Data from 55 COPD patients (10mild, 21moderate, and 30 severe using BTS criteria for severity) were used to examine dyspnoea, measured by OCS; before entering the 4 step programme (stage 1), on completion of the 4 step programme and before entering PR (stage 2), on completion of the eight week PR programme (stage 3).
The mean OCS and mean improvement (MI) after stage 2 and 3 is shown in the table.
The mean OCS and mean improvement (MI) after stage 2 and 3
Conclusions: These preliminary data suggest that COPD patients demonstrate an improvement in functional ability following a four-step community based HImP with further improvement gained by attending community PR. Patients with moderate and severe COPD appear to demonstrate greater improvement from PR than from the 4 step programme. The number of mild COPD patients referred for PR are too small to be meaningful.
P128 BREATHLESSNESS AND ANXIETY MANAGEMENT COURSE FOR PATIENTS WITH COPD UNSUITABLE FOR CONVENTIONAL PULMONARY REHABILITATION
K. Pye, J. Batten, L. Davies. Aintree Chest Centre, University Hospital Aintree, UK
Pulmonary rehabilitation is known to improve health status, symptoms, and exercise tolerance in patients with COPD. Particularly in secondary care, many COPD patients are unsuitable for conventional PR due to concomitant disease or extremely limited mobility. This breathlessness and anxiety management course, run by COPD nurse specialists, was designed specifically for these patients. All are receiving optimal medical therapy and are clinically stable at entry and have been deemed unsuitable for conventional PR. Patients attend once a week for 2 hrs over a six week period. Individual assessment is made and anxiety management, breathing control, relaxation techniques, partially supervised physical exercise, and support and practical advice tailored as appropriate. There were 41 patients referred to the course, but only 19 attended for initial assessment (12 not motivated, three transport problems, three repeated COPD exacerbations, four misc). Assessment at visit one and final visit consists of resting pulse and respiratory rate, 6MWD (with pre and post Borg scores), SGRQ, HAD, and MRC dyspnoea scale. Patients who exacerbated were allowed to continue if well enough, those patients who did not complete the course were not reassessed. Mean (SD) age 69 (7) years, 11 (58%) female, FEV1 1.03 (0.48) litres, % pred FEV1 36.9 (11.9), pH 7.39 (0.04), pO2 10.4 (2.3) kPa, pCO2 4.8 (0.7) kPa (on air).
Nine patients did not complete the course (six repeated COPD exacerbations, two worsening of pre-existing arthritis, one developed lung cancer).
There was no significant difference in age, sex, lung function, or exercise tolerance between those patients who completed the course and those who did not. There was a significant improvement in resting respiratory rate (18.4 to 15.6, p<0.05), change in Borg score after 6MWD (4 to3.1, p<0.05), HAD depression score (7.5 to 5.7, p<0.05) and the Activity (82.5 to 73.3, p< 0.01) and Impacts (60.9 to 51.06, p<0.05) score of the SGRQ. Although the 6MWD was not significantly improved in this small group there was a trend to improvement (202 to 280m).
Individually tailored programs are time consuming and drop out rate is high. However, those that do complete the course benefit in terms of health status and symptoms. Although numbers are small these results are encouraging and merit further study.
P129 DIFFERENT EXERCISE RESPONSES IN SUBJECTS WITH IDIOPATHIC HYPERVENTILATION
S. Jack, C.J. Warburton. Aintree Chest Centre, University Hospital Aintree, Liverpool L9 7AL, UK
Hyperventilation may occur as an acute and a chronic phenomenon. In addition, it may occur in isolation (idiopathic) or may co-exist with other disease processes. There are very little data on homogeneity within any of these subgroups.
We have studied 40 subjects referred through our chest clinics with symptoms suggestive of idiopathic hyperventilation (IH) and normal lung function. IH was confirmed by resting arterial hypocapnia and sustained hypocapnia during ramp-incremental exercise. Further analysis of the ventilatory response to exercise revealed that 11 of the 40 subjects demonstrated acute upon chronic hyperventilation at exercise onset (defined as RER >1.0), six of the 40 subjects demonstrated acute upon chronic hyperventilation at rest which continued during early exercise. Twenty three of the 40 subjects did not demonstrate acute hyperventilation in addition to their chronic hyperventilatory state.
There were no differences between the three groups in the Hospital Anxiety and Depression scores, Nijmegen Questionnaires, and St George’s Respiratory Questionnaires or in maximally achieved parameters during cycle ergometry and in breath—hold tolerance both on 21 and 100% O2. Resting respiratory rate was higher (mean (SD) 33.7 (6.7br/min) in the chronic group compared to the those demonstrating acute hyperventilation in addition to their chronic hyperventilation (mean (SD) 27.7 (8.3)) (p<0.02). There was a significant correlation between anxiety, resting Petco2 and BHTs and between Petco2 at rest and at maximal work rate achieved in the chronic group (p<0.05). Resting RR was significantly correlated with resting VE and resting Petco2 also in the chronic group. These relationships were not evident in the two groups which demonstrated acute and chronic hyperventilation. There was a significant correlation in these groups between anxiety and resting heart rate, which may be explained by anticipatory anxiety.
These data demonstrate that within this population of seemingly homogenous subjects with IH, there are different responses to exercise. This does not appear to alter the overall symptomatology of the groups or their other physiological indices. Whether the different responses to exercise relate to chronicity of symptoms needs further study.
P130 THE DAILY EXPERIENCES OF PATIENTS LIVING AND COPING WITH LONG TERM OXYGEN THERAPY (LTOT)
M. Logue, J.G. Daly, R. Sharkey. Altnagelvin Hospital Derry N Ireland
Aim: To describe experiences of patients who had been using oxygen at home for at least one year.
Patients: Five women and two men (mean age 58yrs) were identified from a hospital register of known oxygen dependant patients.
Inclusion criteria: diagnosis of chronic respiratory disease, using oxygen >16hrs daily and able to communicate verbally.
Design and methods: A phenomenological method was used to describe the daily problems encountered by patients living with LTOT and how they coped. Unstructured audio-taped interviews lasting approx 60 minutes were conducted in the patients’ home. Interviews were directed by the patients. Tapes were transcribed verbatim, checked for accuracy, and analysed using Colaizzi’s method.
Main Findings: Themes which emerged included that of feeling unprepared, living life on a lead, feeling stigmatised, and no longer your own person.
Feeling unprepared related uncertainty about the purpose of treatment, and impact on lifestyle. Descriptions ranged from nervousness to fear about the equipment and oxygen as well as a sense of being left to “get on with it” unsupported. All were unprepared for the timing of the introduction and felt disappointed that it had come “too soon in life”. Living life on a lead referred to restrictions caused by physical attachment to the equipment, lack of spontaneity, and pre-planning activities around oxygen. Feeling stigmatised related to a sense shame or embarrassment felt if seen in public with cumbersome cylinders and visible tubing. Coping descriptions referred to “camouflage” to conceal equipment outside, “brazening it out”, or “just going without”. No longer your own person related to descriptions of reduced autonomy, changes in status and role, and reliance on family or others. Coping descriptions related to social support and spiritual belief.
Conclusions: The patients in this small study would have benefited from the support of a respiratory nurse to provide counselling and support prior to the introduction of LTOT as well as follow up. Sense of stigma prevented some patients from using oxygen for outdoor activities. In the light of the ongoing review of domiciliary oxygen services, the experiences of these patients may have a bearing on the process of assessment and counselling prior to provision of LTOT and lightweight oxygen systems.
P131 A SURVEY OF THE PHARMACOLOGICAL MANAGEMENT OF THE SYMPTOM OF DYSPNOEA
L.J. Alloway1, C.L. Davis2, P. Hockey3. 1St Barnabas Hospice, Worthing; 2Countess Mountbatten House, Southampton;
3Southampton University Hospitals NHS Trust, Southampton, UK
Background: The symptom of dyspnoea is an increasing clinical problem, with rising incidence and longevity of patients with respiratory diseases. The current evidence base for treatment is sparse and often contradictory.
Aims: To determine current clinical practice in the symptomatic pharmacological management of dyspnoea, when disease related treatments are optimised, in patients with malignant and non-malignant diseases. To compare practice in two groups: respiratory and palliative medicine consultants.
Methods: Postal survey to consultant members of British Thoracic Society and Association of Palliative Medicine, with letter from the “Respiratory Centre” accompanying the anonymous survey. Data was analysed using nonparametric statistics to compare the results from the two groups.
Results: 896 surveys were sent. Of these 46% were returned: 37% useable (32% respiratory (R), 45% palliative medicine (PM)), 13% respondents did not specify which specialist register they are henceforth excluded from analysis.
Strong opioids are most frequently used first line for the symptomatic treatment of dyspnoea in both groups, followed by Benzodiazepines. χ2 Test was significant (p<0.0001) showing opioids used more frequently by PM and weak opioids were more frequently (p<0.003) prescribed by R physicians.
The majority of both groups (R 72%, PM 61%) agreed that there is not enough evidence available to support the use of their choice of drug.
PM physicians used significantly more: Lorazepam (p<0.0001), Cannabinoids (p<0.0001), Levomepromazine (p<0.0001), and nebulised saline (p<0.0001). Oxygen was used more frequently by R (p<0.002).
PM physicians were more likely (p<0.02) to prescribe the same drugs for non-malignant as for malignant diagnoses. R physicians were significantly (p<0.03) more concerned about respiratory depression with opioids in patients with non-malignant disease, compared to PM.
Conclusions: The data shows there are significant differences in the prescribing practices of PM and R physicians. It highlights concerns regarding lack of evidence base for practice and over 95% of the total sample felt more research was needed in this area.
Supported by an Educational Grant from Link Pharmaceuticals Ltd.
P132 USE OF THE PULMONARY FUNCTIONAL STATUS AND DYSPNOEA QUESTIONNAIRE AS AN OUTCOME MEASURE IN MULTIDISCIPLINARY PULMONARY REHABILITATION
W.D. Edwards, S.J. Miller, T.L. Griffiths. Cardiff and Vale NHS Trust and The Section of Respiratory Medicine, University of Wales College of Medicine, Llandough Hospital, Penarth Vale of Glamorgan, CF64 2XX, UK
Background: The Pulmonary Functional Status and Dyspnoea Questionnaire (PFSDQ) was developed as a self completed measure of changes in the ability to perform activities of daily living and the associated intensity of dyspnoea. It has been validated in patients with COPD. (
). A prime goal of pulmonary rehabilitation is to improve patients’ independence and quality of daily life. Hence, we sought to determine whether this questionnaire might be an appropriate outcome measure for use in multidisciplinary pulmonary rehabilitation programmes.
Method: Fifty one patients with chronic respiratory disease attending multidisciplinary pulmonary rehabilitation completed the PFSDQ at the start and end of their programme. In completing the PFSDQ, patients rated each of 78 commonly performed activities on a 0 (best) −10 (worst) scale to indicate the level of change from pre-morbid activity level and the dyspnoea associated with each activity. Patients also scored their overall experience of dyspnoea on “most days” in the last year, “today” and during “most day to day” activities.
Results: See table.
Conclusion: The PFSDQ is sensitive to the effects of multidisciplinary pulmonary rehabilitation with the majority of scores changing significantly. It may, therefore, represent a useful additional outcome measure, based as it is, on the activities of daily living.
P133 HIGH LEVELS OF CIGARETTE SMOKING IN AN HIV INFECTED POPULATION—TIME TO FORGET OPPORTUNISTIC INFECTIONS AND CONSIDER LIFESTYLE DISEASES?
I. Levy, C. Smith, E. Kaya, C.A. Sabin, M.A. Johnson, M.C.I. Lipman. Royal Free Hospital and School of Medicine, London NW3, UK
Antiretroviral (ARV) therapy has transformed the management of HIV disease. Improved immunity has led to reduced direct HIV-related morbidity and mortality; and a new focus on risk reduction for chronic conditions such as cardiovascular disease. This is especially important as many of the ARVs induce significant metabolic complications such as hyperlipidemia. We sought to characterise smoking habits within an HIV infected population, using a questionnaire-based evaluation linked to our prospective HIV database. Over a six week survey period, 394 ambulant subjects were enrolled (85% male, median age 34 - IQR 29–39, 30% previous clinical AIDS diagnosis, 73% using ARVS). Forty five per cent were current smokers and 24% ex-smokers. The current smokers were heavy users with a median pack year consumption of 15, IQR 6–25, and 75% reporting the first cigarette of the day within one hour of waking. They had a significant increased self reported incidence of chest infections compared to ex-smokers and non-smokers. Of the current smokers, 74% had tried to quit. Nicotine replacement and no cessation aids were the two most frequently used methods (44% each). The majority of ex-smokers stopped without specific cessation aids (69%). Cardiovascular risk factors were common, with elevated blood lipids reported in 20%. 30% of individuals had a family history of heart disease, and up to 10% drank more alcohol than the current recommended upper limits. Our study, the largest undertaken in Britain so far, reveals high levels of cigarette smoking within individuals who demonstrate considerable risk factors for smoking related disease. Smoking cessation work should target this at risk population.
P134 THE EFFECT OF SCHOOL TUTOR GROUP SMOKING PREVALENCE ON THE RISK OF INCIDENT SMOKING IN SECONDARY SCHOOL CHILDREN: A LONGITUDINAL STUDY
A.W.P. Molyneux1, S.A. Lewis1, M. Antoniak1, W. Browne3, A. McNeill4, R.J. Madeley2, C.A. Godfrey5, R. Britton1. 1City Hospital; 2University Hospital Nottingham; 3Institute of Education; 4St George’s Hospital, London; 5Centre for Health Economics, University of York, UK
Rationale: Peer smoking is associated with starting smoking in childhood, but this effect may be biased by smokers’ selection of smoking peers and their overestimation of smoking among their peers compared to non-smokers. We have prospectively investigated the effect of tutor group smoking prevalence (an objective, unbiased measure of peer smoking) on the uptake of smoking in Nottinghamshire school children.
Methods: A questionnaire survey of past and current smoking behaviour, parental, and sibling smoking histories was performed in pupils in Years 9 and 10 (aged 13 to 15) in 10 secondary schools in Nottinghamshire, UK in 2000, and repeated in 2001. Data were linked to identify all children who started smoking between the two surveys (incident smokers). We calculated the prevalence of current smokers in each pupils school tutor group in 2000. The independent determinants of incident smoking were analysed by multiple logistic regression and multilevel modelling.
Results: We obtained paired data on 2109 pupils in 2001 (73% follow up). Of the 1766 non-current smokers in 2000, 267 (15%) were incident smokers by 2001. Tutor group smoking prevalence was a significant risk factors for incident smoking after adjusting for female sex, parental and sibling smoking; the risk of incident smoking was independently greater for those in the highest quartile v lowest quartile of tutor group smoking (19% v 12% respectively, adjusted odds ratio 1.78, 95% Confidence Intervals 1.20 to 2.65). Multilevel modelling showed a negligible effect of schools.
Conclusions: Tutor group smoking prevalence is an important, independent, and unbiased determinant of incident smoking in teenagers.
Funded by the Wellcome Trust.
P135 A SURVEY OF SMOKING ATTITUDES AND BEHAVIOURS OF YOUNG PEOPLE ACCESSING A YOUTH PROJECT IN A DEPRIVED AREA OF NOTTINGHAM
E.L. Jones1, N, Romilly2, A. Challenger3, R. Burton2, E. Broadfield1, S.A. Lewis1, J.R. Britton1. 1Division of Respiratory Medicine, City Hospital, University of Nottingham; 2The Zone Youth Project, Aspley, Nottingham; 3New Leaf Smoking Cessation Service, Nottingham, UK
Rationale: Cigarette smoking is the single most important avoidable cause of mortality and morbidity in the developed world and although overall smoking prevalence is falling, young people in socioeconomically deprived areas in the UK continue to take up smoking at an alarming rate.
Methods: We conducted a questionnaire survey of 11 to 20 year olds The Zone Youth Project, a voluntary sector project in one of Nottingham’s most deprived areas, over a month period at all drop-in cafes, dance sessions, schools outreach, and sexual health sessions. A measurement of exhaled carbon monoxide (CO) was performed in consenting individuals.
Results: 264 valid questionnaires were returned and 75% of respondents consented to exhaled CO measurement. The median age of respondents was 14.0 (11–21) with 42% male. 49% were self reported current, regular smokers. Amongst the smokers the median CO reading was 8ppm (1–32) median Fagerstrom score 3.0 (0–7) and median number of cigarettes smoked per day 10. Most smokers obtained their cigarettes from newsagents, friends, or “faghouses” (contraband) and 94% came from households with at least one smoking adult. Of those who smoked, 65% would like to quit smoking and 85% had made previous unsuccessful attempts, giving up for an average of 0–3 weeks. 84% said that they would like the chance to use some kind of NRT with a preference for gum amongst the girls and patches amongst the boys. Family support and willpower rated highest amongst non-pharmacological aids with one to one support from a counsellor also scoring highly.
Conclusions: Our survey confirms the expected high prevalence of smoking in this group but the proportion of those young smokers who would like to quit and who have previously tried and failed was higher than expected. Views expressed will guide the design of specific smoking cessation services in this group.
Funded by Cancer Research UK.
P136 SMOKING CESSATION SERVICES FOR TEENAGE SMOKERS: QUALITATIVE AND PILOT INTERVENTION STUDIES
A.W.P. Molyneux1, S.A. Lewis1, T.J. Coleman2, A. McNeill3, R.J. Madeley2, C.A. Godfrey4, J.R. Britton1. 1City Hospital; 2University Hospital Nottingham; 3St George’s Hospital, London; 4Centre for Health Economics, University of York, UK
Rationale: Most adult smokers started smoking as adolescents. Half of adolescent smokers would like to stop smoking and 70% have tried unsuccessfully to give up. There is little provision of smoking cessation services for teenagers. We carried out a study in secondary schools to investigate teenage smokers’ views of how smoking cessation help should be provided to them, and developed and piloted a prototype school-based smoking cessation intervention based upon these findings.
Qualitative study Methods: We invited teenage smokers (aged 13 to 16, previously identified by a questionnaire survey), from six secondary schools in Nottinghamshire, UK, to attend focus groups to discuss smoking behaviours, knowledge, and attitudes to smoking cessation, delivery of smoking cessation services to teenage smokers, and barriers and motivators to use of such services. Group discussions were recorded and transcribed. Transcripts were coded, sorted and indexed using a framework analysis by three researchers. Emergent themes are presented.
Results: 135 smokers participated in 25 groups. Teenage smokers would prefer help with cessation that is non-judgmental, confidential, and delivered by trained counsellors to individuals or small friendship groups, at school in school time, with the opportunity to use Nicotine Replacement Therapy.
Pilot study Methods: We conducted an uncontrolled pilot study of a prototype cessation intervention in three schools. We invited smokers (aged 14 to 16, identified by a survey) to attend the intervention alone or in small friendship groups, receiving six weekly smoking cessation counselling sessions delivered by a trained counsellor, with a six week course of Nicotine Replacement Therapy (NRT) given as appropriate under medical supervision. Self reported abstinence was validated by an exhaled carbon monoxide of ≤5 ppm. Results 158 smokers were screened and 155 enrolled, 91 (59%) female, mean age 15, smoking mean 10 cigarettes per day. One hundred and forty nine (96.1%) participants set a quit date, 138 (89%) used some NRT, of whom 47 used a six week course. At the final visit 21 (14%) were abstinent and 82 participants (53%) attended.
Conclusions: This study suggests that this school based smoking cessation intervention is acceptable to teenage smokers, that it is feasible and associated with reasonable cessation rates.
Funded by the Wellcome Trust.
P137 AN ASSESSMENT OF SMOKING IN ACUTE MEDICAL INPATIENTS
E. Poon, C.W. Lau, L.Y.C. Yam, C.W. Lam1. Pamela Youde Nethersole Eastern Hospital; 1Ruttonjee Hospital, HK
Aim: To investigate the epidemiology and smoking habits of hospital inpatients and to assess the willingness of smokers to quit.
Study population: Inpatients of acute medical wards of the Pamela Youde Nethersole Eastern Hospital, Hong Kong.
Method: A questionnaire survey was prospectively administered by nursing staff on admission of all patients to the acute medical wards between 15th April and 22nd April 2002. Data collected included age, gender, smoking status/history, and an assessment of willingness to quit. Patients who could not provide such information were excluded.
Results: There were 446 admissions to six acute medical wards over the one week period. Out of the 418 (93.7%) questionnaires returned, there were 208 males (49.8%). Mean ages were 66.2 (17.5) years (males) and 69.7 (18.0) years (females). 171 (41.1%) patients had ever smoked (135 males). Males smoked more than females (29.8 (22.7) v 15.9 (14.2) pack years (p<0.0001)) and started smoking at a younger age (35.8 (17.4) v 45.5 (16.3) years (p=0.008)). 57 (13.6%) current smokers (47 males) had smoked 25.4 (22.4) pack years. Of these, 35 (61.4%) had ever thought of quitting, 33 (57.9%) acknowledged a willingness to quit, and 26 (45.6%) accepted help towards quitting. Neither current age, age at which smoking commenced, or overall consumption in pack years was related to attitude towards smoking cessation, although those who had smoked less tended to be more willing to quit. Males had thought more about and were significantly more willing to quit than females however, an equal proportion of both sexes accepted help with cessation. 114 (27.3%) ex-smokers (89 males) had quit for 12.5 (11.4) years, having smoked 28.5 (21.7) pack years.
Conclusions: 41.1% of medical inpatients surveyed had ever smoked. 13.6% were current active smokers and of these 45.6% agreed to intervention with help in smoking cessation. The hospital inpatient setting provides a good opportunity to assess smoking status with a view to assisting smokers to quit.
The therapy of asthma
P138 BODIPY-TMR-CGP 12177: AN IRREVERSIBLE FLUORESCENT PROBE FOR THE HUMAN β2-ADRENOCEPTOR WITH AGONIST PROPERTIES
J.G. Baker, I.P. Hall, S.J. Hill. Institute of Cell Signalling, Medical School, Queen’s Medical Centre, Nottingham NG7 2UH, UK
Current methods to study native receptors in cells from patients are thwarted by the need for large numbers of cells. Fluorescent techniques offer an opportunity to work at the single cell level. BODIPY-TMR-CGP12177 (BOD-CGP) is a fluorescent analogue of the hydrophilic β-adrenoceptor (β2-AR) antagonist CGP 12177. It can stimulate cAMP accumulation (EC50 = 28.2 (4.0) nM, n=3) and gene transcription (EC50 =25.3 (3.6) nM; EMAX=47% of the maximum isoprenaline response) in CHO-K1 cells expressing the human β2-AR and a cyclic AMP response element reporter gene (CHO-β2 cells). Studies using 3H-CGP-12177 indicated that BOD-CGP was able to displace the specific binding of this radioligand to the human β2-AR with an apparent KD of 15.8 (3.0) nM, n=4. Pretreatment with BOD-CGP (100nM) reduced the maximal specific binding of 3H-CGP 12177 by 50%, even after the fluorescent ligand had been washed out two hour previously. This provides strong evidence that BOD-CGP is effectively irreversible over this time period. Visualisation of the binding of the fluorescent BOD-CGP to single living cells (CHO-β2) using confocal microscopy demonstrated clear membrane labelling at concentratons of 30nM BOD-CGP and above. Analysis of the total pixel intensities of each image enabled an estimate of the KD for BOD-CGP to be determined from saturation analysis (27.6 (6.4) nM; n=4). The binding of 50nM BOD-CGP to living cells was also inhibited by increasing concentrations of the β2-antagonist ICI 118551 (IC50 = 4.30 (0.86) nM; n=4) and CGP 12177 (0.76 (0.40) nM; n=3). Simultaneous imaging of the binding of this red fluorescent ligand (BOD-CGP) to a β2-AR-Green Fluorescent Protein fusion protein in CHO-K1 cells indicated that BOD-CGP did not induce receptor internalisation. A similar observation was made with the low efficacy agonist salbutamol, whereas the full agonist isoprenaline caused substantial receptor internalisation. In conclusion, we have fully characterised a novel fluorescent ligand for the human β2-AR and shown that it can be used to visualise receptors in single living cells. The irreversible nature of this ligand should make it readily applicable to the study of β2-ARs in acutely isolated native human cells in health and disease.
JGB is a Wellcome Trust Clinical Training Fellow.
P139 DO SELECTIVE TOPICAL β ANTAGONISTS FOR GLAUCOMA HAVE LESS RESPIRATORY SIDE EFFECTS?
J.A. Nightingale1, J.F. Kirwan2. 1Royal Brompton and Harefield NHS Trust; 2Institute of Ophthalmology
Topical β antagonists are prescribed for glaucoma in approximately 500 000 people in the UK. We have previously shown that prescription of these drugs is associated with an excess incidence of airways obstruction.(1) Selective topical β antagonists are marketed as being less likely to induce airways obstruction than non-selective topical β antagonists.The aim of our study was to determine whether selective topical β antagonists are associated with a smaller risk of developing airways obstruction than non-selective topical β antagonists.
Data obtained from the Mediplus™ UK primary care database were used to perform a historical cohort study to determine one year incidence of airways obstruction in subjects following treatment with topical β antagonists for glaucoma for the period 1993–1998. Cases were defined as having received a first prescription of a drug specifically used in the management of airways obstruction. Only subjects with no history of airways obstruction were included. Analysis was performed using proportional hazard modeling to minimise potential confounding.
For selective topical β antagonists 12 of 324 treated subjects developed airways obstruction, compared with 112 of 9094 controls (adjusted hazard rate 3.0 (95% confidence interval 1.6 to 5.4)). For non-selective topical β antagonists the corresponding figures were 69 of 2321 subjects compared with the same control group (adjusted hazard rate 2.2 (95% confidence interval 1.6 to 3.0)). There was no significant difference between groups (p=0.5), both being associated with a significantly increased risk of airways obstruction.
We conclude that selective topical beta antagonists do not appear to have less respiratory side effects than non-selective topical β antagonists in the treatment of glaucoma.
1. JF Kirwan, et al. BMJ 2002:(in press).
P140 SMALL AIRWAY RETICULAR BASEMENT MEMBRANE (RBM) THICKENING IN CLINICALLY STABLE LUNG TRANSPLANT RECIPIENTS (SLTR) IS NOT AFFECTED BY THREE MONTHS TREATMENT WITH INHALED CORTICOSTEROIDS (ICS)
C. Ward1, A. De Soyza, A. Fisher, G. Pritchard, P. Corris. Lung biology and transplantation group, university of Newcastle Upon Tyne; 1The Freeman Hospital, NE7 7DN, UK
Introduction: Recent publications have demonstrated potentially pathological changes in clinically stable lung transplant recipients (SLTR), with frank airway remodelling demonstrated in allograft recipients with established BOS. In asthma Rbm thickening has been demonstrated at an early stage and it is suggested that ICS treatment reduces this. There is no such data regarding Rbm thickening in small airways sampled at transbronchial biopsy (TBB) of lung allografts.
Hypotheses: Rbm thickening exists in small airways of lung allograft recipients. ICS treatment may decrease small airway Rbm thickening.
Methods: Thirty one SLTR >3 months post transplantation, randomised to three months 400μg CFC BDP bd or a formulation designed to yield at least an equivalent small airway dose (200μg HFS BDP bd Autohaler). Bronchoscopy BAL and TBB pre and post ICS. TBB were fixed in 10% buffered formalin, embedded in paraffin and H+E stained. Assessment of airway Rbm thickness was carried out at Image analysis from serial stepwise sections by a blind experienced observer, exceeding ERS criteria (>1mm Rbm always scored). Ethical considerations required the use of a normal range for RBM thickness in large airway biopsies (
). Rbm is thought to be systematically thicker in large airways. See figure.

*Normal large airway Rbm (
Conclusion: Small airway Rbm thickening exists even in SLTR, but its significance with regard to the subsequent profound remodelling in BOS (1) is not known. three months of moderate ICS did not affect Rbm thickening. Further longitudinal studies, including the effect of anti-remodelling strategies are possible.
P141 RAPID EFFECTS OF SINGLE DOSE FLUTICASONE PROPIONATE ON ALLERGEN-INDUCED EARLY ASTHMATIC RESPONSES IN MAN
R.I. Ketchell, M.I. Allenby, M.W. Jensen, G.W. Clarke, B.J. O’Connor. Department of Respiratory Medicine and Allergy, GKT School of Medicine, King’s College, Bessemer Road, London, SE5 9PJ, UK
Background: There is no evidence to date to suggest that inhaled glucocorticosteroids (GCS) affect the early asthmatic response (EAR) following allergen inhalation in sensitised asthmatic subjects. This is perhaps surprising as we have previously demonstrated that single dose inhaled fluticasone propionate (FP) attenuates airway responsiveness to the mast cell stimulus adenosine 5’-monophosphate (AMP) within two hours (Ketchell, et al. J Allergy Clin Immunol 2002:(in press)).
Objective: The aim of this study was to assess the effect of inhaled FP on allergen-induced airway narrowing.
Methods: In a randomised, double-blind placebo controlled, crossover study in mild steroid-naïve asthmatics, 12 subjects with a known EAR to inhaled allergen, underwent two constant-dose allergen challenges separated by 3–4 weeks. Each challenge was preceded two hrs earlier by a single dose of inhaled FP 1000μg or matched placebo via an accuhaler™. The EAR was measured as the % change in FEV1 from baseline at 5, 10, 15, 20, 30, 45, 60, 90, and 120 minutes following allergen challenge and the area under the curve during the first two hours (AUC0–2hr).
Results: FP 1000μg significantly attenuated the EAR compared to placebo with a 45.1 (12.2) % reduction in AUC0–2hr (p=0.04). A reduction in FEV1 was observed at each time interval, although differences were not significant until the 90 minute time point (p=0.01). The mean maximal % fall in FEV1 was observed at the 15 min time interval and was 18.9% following a single dose of FP 1000μg and 21.6% following placebo (ns)
Conclusions: This study confirms rapid anti-inflammatory effects of inhaled FP in man. The time interval of protection suggests an effect on mast cell mediator responses such as increased microvascular permeability and/or mucosal blood flow rather than on mast cell degranulation and immediate smooth muscle responses. Inhaled GCS may provide additional beneficial topical effects in the management of acute allergic asthma.
P142 FOUR MONTH ADJUSTABLE OR FIXED BD DOSING WITH BUDESONIDE/FORMOTEROL IN A SINGLE INHALER REDUCES SYMPTOM SEVERITY
P. Ind1, J. Haughney2, D. Price2, J-P. Rosen3, J. Kennelly3. 1Hammersmith Hospital, UK; 2University of Aberdeen, UK; 3AstraZeneca UK, Luton, UK
Aim(s): To evaluate the efficacy of budesonide/formoterol combination (B/F; Symbicort Turbuhaler) administered as either adjustable or fixed bd dosing.
Methods: Patients (mean age 48 years) were randomised to adjustable maintenance (n=782; B/F two inhalations bd for four weeks, thereafter 1–4 inhalations bd depending on asthma symptoms for 12 weeks) or fixed B/F dosing (n=771; two inhalations bd for 16 weeks). Primary efficacy variables were reduction in symptom severity (according to GINA definitions) and total exacerbations.
Results: Changes in symptom severity are shown in the table. Ninety four per cent of patients (both groups) reported no exacerbations. The average number of daily inhalations was 15% lower in the adjustable dosing group.
Conclusions: Patients treated with both adjustable and fixed-dose B/F demonstrated a reduction in symptom severity as shown by the marked shift from moderate to mild intermittent. Overall there was a 46% reduction in patients graded as moderate persistent and a doubling of patients categorised as mild intermittent. A reduced overall daily dose was observed in the adjustable arm.
P143 SYMBICORT USED IN A GUIDED SELF MANAGEMENT PLAN PROVIDES ADDITIONAL ENABLEMENT TO ASTHMA PATIENTS COMPARED WITH FIXED DOSING
J. Haughney1, D. Price1, J-P. Rosen2, K. Morrison2. 1University of Aberdeen, UK; 2AstraZeneca UK, Luton, UK
Aims: To assess the effect on patient enablement of a guided self management plan compared with fixed dosing in asthma patients prescribed Symbicort.
Methods: After a four week run-in on budesonide/formoterol two inhalations bid, patients received adjustable dosing (n=124) or fixed dosing (n=104) for 12 weeks. Patients completed a validated Patient Enablement Instrument1 (PEI) within eight weeks of the last clinic visit. The PEI has six questions (“As a result of your treatment do you feel you are: Q1: able to cope with life; Q2: able to understand your illness; Q3: able to cope with your illness; Q4: able to keep yourself healthy; Q5: confident about your health; Q6: able to help yourself”). Patients’ responses are scored 0 (“same or less” or “not applicable”) to two (“much better”). A mean difference in total score of ≥0.82 between groups, or an individual’s total score of =6 is considered to reflect a relevant treatment benefit.3
Results: The baseline and demographic characteristics of the two groups were well matched. The total PEI scores were (mean (SD)) 6.24 (3.73) and 5.44 (3.84) in the adjustable and fixed dosing groups, respectively (difference 0.8 (95% CI −0.2 to 1.8), p=0.12). A statistically significantly greater proportion of patients receiving adjustable dosing had a score of ≥6 compared with fixed dosing (57% v 43%, p=0.04). There were no significant differences between responses to Q1, Q3, Q5, and Q6.
Conclusions: Guided self management with Symbicort provides a greater level of patient enablement than fixed dosing.
1. Howie JG, et al.
.
2. Dowell J, et al.
.
3. Howie JG, et al.
.
P144 AIRWAY DRUG DELIVERY: SIZE MATTERS—BIGGER IS INDEED BETTER
O.S. Usmani, M.F. Biddiscombe, P.J. Barnes. Department of Thoracic Medicine, National Heart and Lung Institute, Imperial College School of Medicine, London, UK
Current inhaler devices are inefficient as the dose delivered is a polydisperse distribution of drug particle sizes, and only 20% reaches the lungs. Aerosol particle size influences drug deposition and in vitro models conclude 2–6μm as optimal. Monodisperse aerosols are the appropriate research tools to investigate particle size effects, as the dose is within a narrow size distribution. We hypothesised that engineering such aerosols of salbutamol would identify the ideal bronchodilator particle size and improve inhaled therapeutic drug delivery.
We previously described our use of a spinning top aerosol generator to produce such aerosols, and reported larger particles were significantly more potent bronchodilators in asthmatics—6μm∼3μm >1.5μm, at 1/10th standard MDI doses. The 6μm particles achieved equivalence with 200μg MDI salbutamol. No adverse effects were observed. We then hypothesised the differences were a result of the deposition characteristics of each particle size, in that larger particles were better matched to their target site of action.
We therefore undertook to assess lung and extrathoracic deposition patterns using 2D planar imaging and 99mTc-labelled monodisperse salbutamol (30μg dose) aerosols, in 12 asthmatic subjects with simultaneous measures of clinical efficacy. The smaller particles achieved greater total lung deposition; 1.5μm (56%), 3μm (50%), 6μm (46%), however the larger particles were more efficacious 6μm∼3μm >1.5μm (FEV1, p<0.05). We quantified regional deposition in the lungs and found more of the larger particles in the central+intermediate zone; 6μm (75%), 3μm (66%), 1.5μm (56%). The penetration index confirmed greater peripheral lung penetration of the smaller particles; 1.5μm (0.79), 3μm (0.60), 6μm (0.36); (p<0.05).
The data support our hypothesis that for β2-agonists, regional airway targeting to the conducting airways is more important than alveolar deposition. Particles in the higher part of the respirable range achieve the greatest clinical response and we advocate small doses, when correctly delivered, may improve the therapeutic index. We now aim to investigate the effects of inspiratory flow and respiratory disease severity on aerosol deposition. With resurgence of interest in inhalation drug delivery as a means of systemic therapy, we must take the opportunity to research basic aerosol science to enhance the efficiency of clinical airway drug delivery.
P145 THE MEASUREMENT OF THE SUBMICROMETER SIZE DISTRIBUTION OF METERED DOSE INHALERS (MDI)
M. Crampton1, R.P. Kinnersley1, J.G. Ayres2. 1Divison of Environmental Health & Risk Management, University of Birmingham, Birmingham, B15 2TT; 2Department of Respiratory Medicine, Birmingham Heartlands Hospital, Birmingham, B9 5SS, UK
Recent studies indicate that toxicity of materials in ultrafine aerosol form is greater than that of the same material in coarser aerosol form. At the same time it has been observed that the HFA formulation of beclomethasone (Qvar) is more potent compared to the CFC product. A pertinent difference between the two is that the former yields smaller particles.
The size distribution by number of a range of pMDIs (including Qvar [3M], Salbutamol [GSK], HFA-Fluticasone [GSK], Beclomethasone [GSK], Budesonide [AstraZeneca]) was measured to determine the proportion of particles in the sub-micrometer range. Measurements were made by Electrical Low Pressure Impactor (size range 30nm–10μm) and a Scanning Mobility Particle Sizer (size range 10–100nm). All devices tested yielded high numbers of fine and ultrafine particles, the number being greater for HFA than for CFC propelled MDIs (% < 100 nm, HFA-Qvar:76%, HFA-Salbutamol:75%, HFA-Fluticasone:76%, CFC-Belcomethasone:65%, CFC-Budesonide:57%). We suggest that the number of fine and ultrafine particles, the concentration of drug per particle, the molecular properties and the hydroscopic properties of the drug, may all influence MDI potencies. See figure.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
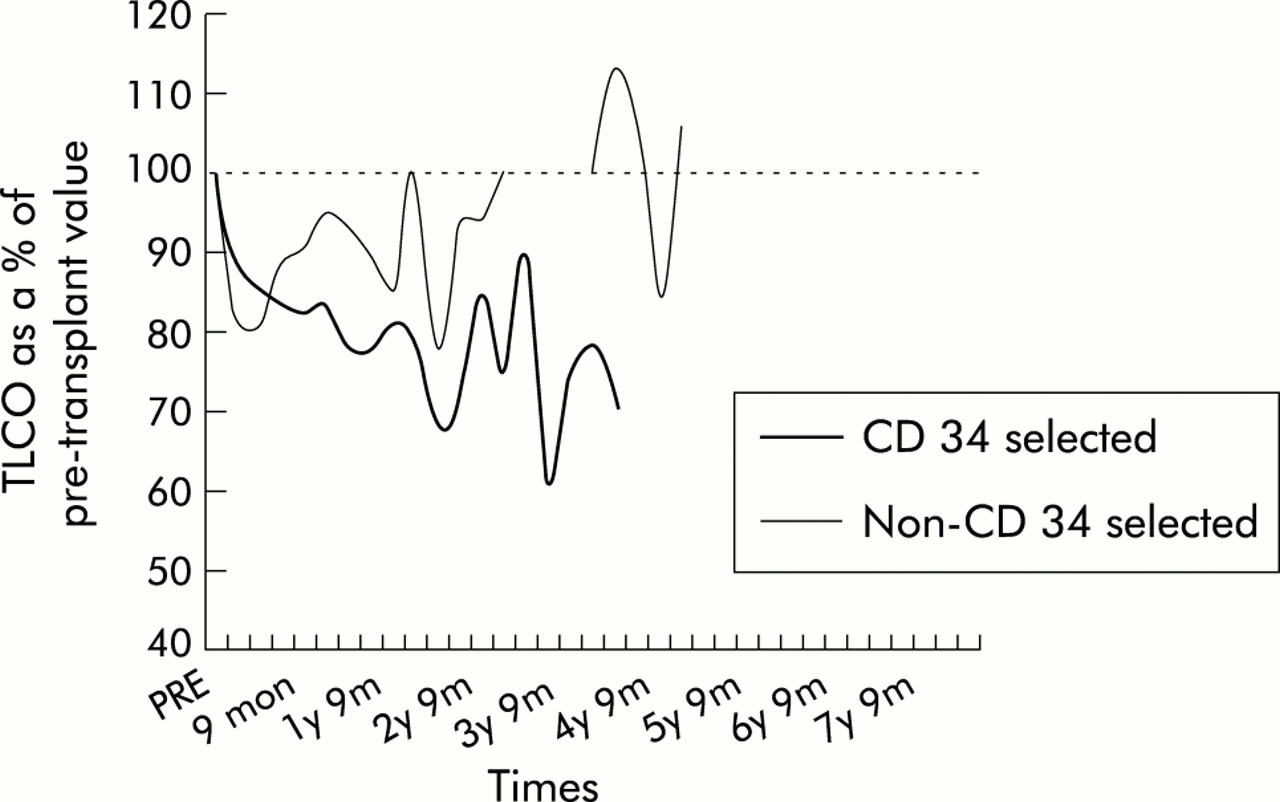{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Size distribution of pMDIs (number weighted).
This work was supported by an academic grant from 3M Pharmaceuticals.
P146 PD20 TO METHACHOLINE IS PREDICTED BY AIRWAY INFLAMMATION AND REMODELLING: A SYSTEMATIC, LONGITUDINAL, STEROID INTERVENTION STUDY OF AIRWAY BIOPSY (Ebb) AND BAL PARAMETERS
C. Ward1, D. Reid2, M. Pais2, B. Orsida2, B. Feltis2, R. Bish2, D. Johns2 , E. Haydn Walters2. 1Lung Biology and Transplantation Group, University of Newcastle upon Tyne and The Freeman Hospital, UK; 2University of Tasmania and Monash University, Australia
Introduction: We have recently shown that PD20 may be predicted from a model including terms measuring airways remodelling; (Reticular basement membrane (Rbm) thickening) and inflammation quantified at BAL.1 In this study we have refined our paradigm, including information on large airway biopsy (ebb) inflammation and the effect of inhaled corticosteroid treatment.
Hypothesis: Ebb provides complimentary inflammatory indices to BAL, which supports a link between inflammation, airway remodelling and PD20.
Methods: A double blind, randomised, placebo-controlled, parallel group study of inhaled fluticasone propionate (up to 12 months FP 750μg bd) in 35 symptomatic, mild to moderate atopic asthmatics with previously described BAL inflammation, Rbm thickening and PD20.1 Quantification of ebb inflammation by immunohistochemistry/image analysis.1 Matrix analysis of individual univariate correlations, with subsequent “best subsets” multiple regression.
Results: Cross sectional, multiple regression analysis explained 56% of the variability in BHR, 23% related to log EG2 (eosinophil) counts, 19% to log Rbm thickness, and 14% to BAL epithelial cells improving our previous model (overall 40%; 1). Following three months FP ebb inflammatory cell counts fell significantly, with no further FP effect, for example, baseline median ebb EG2 count 8/mm basement membrane (bm), (range 0–32), three month; 2/mm bm (0–22; p<0.01 v baseline), 12 month median 2/mm bm (0–72, NS v 3 months). Changes in ebb inflammation preceded an effect on Rbm thickness and the maximal effect on BHR (@12 months FP, 1).
Conclusion: Ebb and BAL are complimentary, and further support the view that PD20 to methacholine reflects airway remodelling and inflammation in asthmatic subjects. A lack of specificity for any one part of asthma pathophysiology may represent a strength of BHR testing.
Chris Ward is an ERS research fellow.
1. Ward, et al.
.
P147 RELATIONSHIP BETWEEN ADHERENCE TO PRESCRIBED REGIMENS AND ASTHMA CONTROL IN PATIENTS WITH DIFFICULT ASTHMA
S. Aburuz1, J. McElnay 1, J. Millership 1, J. Gamble 3, L. Heaney2 3. 1School of Pharmacy; 2Department of Medicine, Queen’s University Belfast; 3Regional Respiratory Centre, Belfast City Hospital, Belfast
Introduction: Non-adherence with prescribed therapy is a major problem in the management of chronic illness. The aim of the present study was to examine the relationship between asthma control and adherence to oral therapy (prednisolone (P) and theophylline (T)) and high dose inhaled steroids (HDIS) in a population of difficult asthmatics (persisting asthma symptoms/frequent exacerbations requiring systemic steroids despite maintenance high dose inhaled corticosteroids plus a long acting β2 agonist).
Method: A range of parameters was used to assess adherence and asthma control in patients, with difficult to control asthma, attending a hospital outpatient clinic. Plasma P was measured by HPLC. Plasma T was measured by fluorescence polarization immunoassay. Urinary Cortisol (C) was measured by HPLC and corrected for creatinine (UCC ratio). Non-adherence was recorded if (a) Prednisolone: no plasma P detectable; (b) Theophylline: no plasma T detectable. Adherence to HDIS was recorded if morning UCC ratio was suppressed below 8.0 nmol C/mmol creatinine. Asthma symptom control scores (ASCSs) were recorded using the Juniper Asthma Control Questionnaire.(1)
Results: Eleven (25%) patients of 44 patients taking T and 14 (56%) of 25 patients taking P were non-adherent. Of 43 patients taking HDIS (median 2000μg; range 1000–4000μg BDP equivalent), 31 (72%) had suppressed UCC ratio. ASCS, wheezing a morning symptoms were significantly lower (p<0.05) in patients with UCC suppression. There was no relationship between FEV1% and suppression of urinary cortisol. Asthma control did not vary with adherence with theophylline or prednisolone.
Discussion: There was a high prevalence of non-adherence with prescribed oral therapy in patients with difficult asthma. Asthma control was related to the presence of urinary cortisol suppression in patients receiving HDIS, which may reflect non-adherence with inhaled therapy. Failure to suppress urinary cortisol can be used as a marker of possible non-adherence to HDIS in this population.
1. Juniper E, et al.
.
P148 EARLY ANTIBIOTIC PRESCRIPTION AND ALLERGIC DISEASE IN UK ADULTS
P. Cullinan, J.M. Harris, P. Mills, S. Moffat, C. White, F. Figg, A. Moon, A.J. Newman Taylor. Occupational & Environmental Medicine, Faculty of Medicine, Imperial College of Science, Technology and Medicine, London, UK
To investigate any association between treatment with antibiotics in early life and subsequent atopic or allergic disease, we studied a population of adults in southeast England. 1063 men and women (93% of those eligible), parents of a birth cohort based in Ashford, Kent, agreed to participate. Allergic diseases were defined by responses to a questionnaire; atopy was measured by responses to skin prick tests with common aerollergens. Prescription information for the first five years of life was successfully obtained from the general practice records of 746 (70%) subjects. There were no important differences in the rates of atopy or allergic disease between those whose records were or were not available for examination.
Thirty six percent of adults were atopic; 14% reported a history of asthma and 29% hay fever. 564 (76%) had at least one antibiotic prescription, with a median of three. The median age at first prescription was 1.5 years. Older subjects were more likely not to have a prescription record, indicating a temporal increase in prescription patterns. There was a clear association with family size, whereby adults with fewer siblings were significantly more likely to receive at least five prescriptions by the age of five years (p<0.001). There was no evidence of any association between atopy and total antibiotic prescriptions in total (adjusted OR 1.01, 95% confidence interval (0.97 to 1.05) per prescription), a pattern which did not alter at any age or by antibiotic class. Asthmatics—with or without atopy—were more likely to have received an antibiotic prescription by the age of five years (adjusted OR 1.08 (1.03 to 1.13) per prescription). This relationship increased with age at prescription (adjusted OR 1.02 per prescription by age 1; 1.18 age 1–2; 1.14 age 2–3; 1.23 age 3–4; 1.32 age 4–5). A similar but less marked pattern was observed for hay fever, again with or without evidence of pollen sensitisation. These findings do not rule out a positive association between antibiotic use and subsequent allergic disease; but are more probably explained by a protopathic bias.
P149 IS A TWO WEEK TRIAL OF ORAL PREDNISOLONE PREDICTIVE OF TARGET LUNG FUNCTION IN PAEDIATRIC ASTHMA?
C. Lex, D.N.R. Payne, N.M. Wilson, A.M. Li, A. Zacharasiewicz, A. Bush. Department of Paediatric Respiratory Medicine, Royal Brompton Hospital, London, UK
The optimum length of a steroid reversibility trial in children is not known. We have used a two week trial of oral prednisolone to determine target lung function for subsequent asthma therapy. The aim of this study was to determine whether in fact on subsequent visits some children actually exceeded this “target lung function”.
Methods: Twenty five severe asthmatic children (median age 13 (range 6–16) years were studied. Severe asthma was defined as persistent symptoms despite treatment with ≥1600μg/d of inhaled budesonide or equivalent, long-acting β2-agonist ± regular steroids. FEV1 was measured following high-dose systemic steroids (oral prednisolone 40 mg/day for 14 days) and compared with the highest FEV1 obtained in subsequent visits during the following year. Results: The mean (SD) FEV1 as a percentage of the predicted value following the formal steroid trial was 74,28 ± 19,66 (range 38–103). A total of 8 (32%) children actually obtained an increase of >10% above their “target” FEV1 during the following year at routine clinic spirometry. There were no important changes in prescribed asthma medications (for example, cyclosporine, methotrexate, s.c. terbutaline), which might have accounted for this in these eight children. In 17/25 (68%) children FEV1 measured in subsequent visits remained stable or declined. The mean age of both patient groups was equal, and it was not possible to predict which children would exceed “target lung function” from baseline characteristics or post-steroid FEV1.
Conclusions: A two weeks course of prednisolone is not necessarily predictive of target lung function. Further studies are needed to find out whether a higher dose or longer duration of the steroid trial is more predictive, or whether adding an acute inhalation of β2-agonist at the end of the trial may increase predictive power.
Tuberculosis
P150 TUBERCULOSIS INCIDENT AND OUTBREAK SURVEILLANCE IN ENGLAND AND WALES: REPORTS FROM JANUARY 1999 TO JUNE 2002
A. Story, J. Watson. Communicable Disease Surveillance Centre, Respiratory Division, Tuberculosis Section, 61 Colindale Avenue, London, NW9 5EQ, UK
We are currently developing a central information resource on tuberculosis incidents and outbreaks that can be used to inform future management. The aims of this surveillance initiative are to gain insight into the occurrence and distribution of tuberculosis incidents and outbreaks; monitor and evaluate the effectiveness of control measures and inform policy; network relevant parties as an accessible information resource for one another; and provide a means of recording examples of best practice and lessons learned.
In order to more fully understand the terms and specification required for this new aspect of tuberculosis surveillance we have retrospectively collated tuberculosis related incidents and outbreaks reported to CDSC from January 1999 to June 2002.
A total of 47 reports associated with actual and potential tuberculosis transmission involving health workers and institutions have been received, 33 of which relate to health and allied professionals posing an infection risk. Similarly, 29 reports relating to education workers and institutions, including one outbreak, which involved extensive contact investigation have been received. There are four reported instances of tuberculosis among prisoners and one incident involving a prison guard. A total of 22 instances of tuberculosis presenting a potential public health threat to airline passengers have been reported, 18 involving passengers and four airline employees.
Incidents and outbreaks reported to CDSC to date represent only a sample of the total episodes. It is planned that the development of a more formal system to capture, collate, and report on tuberculosis incidents and outbreaks will enable a more accurate assessment of their frequency, distribution and public health impact to be made.
P151 TRENDS IN TUBERCULOSIS CASE FATALITY IN ENGLAND AND WALES 1988–2000
A.R. Martineau1, P.D.O. Davies2. 1Department of Respiratory Medicine, Newham General Hospital, London E13 8SL, UK; 2Aintree Chest Centre, University Hospital Aintree, Liverpool L9 7AL, UK
To determine trends in tuberculosis (TB) case fatality in England and Wales according to age and disease site we analysed published notification and mortality data for TB from 1988–2000 (see table overleaf). In contrast to 1974–1987,(1) case fatality for TB of all sites and age groups combined fell over this period despite increasing incidence of disease. Declining case fatality is likely to be due to changes in TB epidemiology: younger patients with higher rates of extra-pulmonary disease and lower case fatality rates accounted for an increasing proportion of TB cases over the study period. Improvements in TB notification rate, under diagnosis of TB at post mortem and improved case management may also have contributed to the decreasing case fatality rates observed.
1. Nisar M, et al.
.
P152 ERRORS IN THE NOTIFICATION OF TUBERCULOSIS
C. Seehra1, F.A. Drobniewski2, P.G. More 2, D.C.S. Hutchison3. 1Lambeth, Southwark & Lewisham Health Authority (LSLHA); 2PHLS Mycobacterium Reference Unit, Dulwich; 3Respiratory Medicine, King’s College Hospital, London, UK
Introduction: In the UK, clinical disease with Mycobacterium tuberculosis (MTB) is notifiable by law, whether cases are MTB culture positive or culture negative treated as MTB. Notification initiates contact tracing and provides epidemiological data. Two main sources of error exist: (1) Under notification (failure to notify cases of MTB infection). (2) Over notification (notification of cases not due to MTB infection). Both errors can occur and we have examined local procedures, with emphasis on over notification.
Methods: We have studied notified patients treated at King’s College Hospital (KCH) and resident in LSLHA. Over notification in 1996 to 2000 inclusive was defined for this audit by comparison of notified cases with microbiologically confirmed cases. Under notification (limited to 1999) was detected by search of KCH Pharmacy data base for patients prescribed anti-tuberculosis chemotherapy, but not notified as TB.
Results: In 1996 to 2000, 279 cases were notified as tuberculosis, 229 (82%) being MTB culture positive. Forty one culture negative cases were notified, 32 being clinically probable MTB and nine probably not. Nine cases were culture positive with non-MTB mycobacteria. Thus 18 notified patients definitely or probably did not have MTB infection, an over notification rate of 18/279 or 6.5% (CI 4 to 10). 18/50 or 36% (CI 23 to 51) of all notified cases who were not MTB culture positive were erroneously notified as MTB.
In 1999, 45 cases were notified. The Pharmacy data base identified 11 unnotified MTB cases, giving an under notification rate of 11/45 or 24.4% (CI 13 to 40). Four notified patients did not have MTB infection, giving an over-notification rate of 4/45 or 8.8% (CI 2 to 21).
Conclusion: Combining over and under notification rates for 1999 yields a net under notification rate of 7/45 or 15.6% (CI 7 to 29). The microbiological data base should lead to notification of all MTB positive cases. Culture negative cases contribute an important error and must be verified by other means, the Pharmacy data base proving to be the most successful. Denotification procedures must be more vigorously pursued.
P153 UPDATE ON AN OUTBREAK OF ISONIAZID MONO-RESISTANT TUBERCULOSIS IN NORTH LONDON
M. Ruddy1, A.P. Davies2, M.D. Yates1, S. Yates2, S. Balasegaram3, B. Patel2, S. Lozewicz2, S. Sen4, M. Bahl5, E. James6, M. Lipman7, Y. Drabu2, J. Watson3, M. Piper8, F. Dronniewski1, H Maguire3, on behalf of a Londonwide Incident Committee. 1PHLS Mycobacterium Reference Unit, King’s College Hospital (Dulwich); 2North Middlesex University Hospital Trust; 3PHLS Communicable Disease Surveillance Centre; 4Barnet, Enfield & Haringey Health Authority; 5Camden & Islington Health Authority; 6Barnet & Chase Farm Hospital Trust; 7Royal Free Hospital Trust; 8Department of Health Prison Policy Unit
Since January 2000 an outbreak of isoniazid mono-resistant Mycobacterium tuberculosis has been investigated. Typing of suspected isolates has been performed at the PHLS Mycobacterial Reference Unit using a new rapid PCR-based method (RAPET), with confirmation by RFLP IS6110 typing showing a distinctive 15 band pattern. Case finding has been performed by initial retrospective and continuing prospective analysis of isoniazid mono-resistant isolates from the source and neighbouring hospitals, and all isoniazid mono-resistant isolates in London from January 1999 onwards, along with comparison of the fingerprint to RFLP IS6110 databases. The earliest case detected was a Nigerian student resident in London in 1995. Epidemiological links were established by questionnaire in face to face interviews. Outbreak control is coordinated by an Incident Control Committee at the PHLS Communicable Disease Surveillance Centre. To date 97 patients’ isolates have demonstrated the RAPET pattern. Eighty eight microbiologically confirmed cases have been identified in London, with 14 clinically proven cases in their contacts and nine epidemiologically linked cases outside London. Contact tracing so far has suggested a higher than predicted transmission rate (11%). Thirty contacts have been placed on chemoprophylaxis. The epidemic curve suggests that the peak of the outbreak may not yet have been reached. A wide range of racial and social groups have been involved in the outbreak with 17 of the cases associated with prisons including one prison staff member. The investigation has revealed the first documented case of transmission in a UK prison. Nosocomial transmission has occurred involving staff and patients. The involvement of IVDUs and sex workers along with documented compliance problems in 38% of cases has made control of the outbreak difficult.
P154 MISSED DIAGNOSIS OF TUBERCULOSIS IN THE ACCIDENT AND EMERGENCY DEPARTMENT
M. Bhattacharyya, A. Choudhury, G.E. Packe. Newham Chest Clinic, Shrewsbury Road, Forest Gate, London E7 8QP, UK
In our district many patients present with illness first to the accident & emergency department (A&E) at our hospital rather than to primary care. This is a result of several factors such as poor understanding of the primary care system in the UK, and poor access to primary care. The aim of this study was to ascertain how many patients with tuberculosis in our district present to the A&E department, and how well they are diagnosed at presentation.
Of the 243 notified cases of tuberculosis (TB) in Newham during 1999, 121 (50%) patients were seen at A&E prior to notification. Of these 121 patients, 62 had pulmonary disease; their median age was 32 years (range 1 to 88 years). Fifty one patients attended the A&E department more than once (total 211 visits). The number of attendances: number of patients, was as follows: 1 attendance: 70 patients, 2:30, 3:9, 4:8, 5:3, 6:1. Of the 171 visits for which A&E patient information cards were traced: 143 (84%) were for TB related episodes, 12 (7%) were episodes unrelated to TB, and 16 (9%) did not wait after being triaged.
Records for the TB related episodes (143 visits) were divided into those in whom TB was suspected when seen in the A&E department (37 visits), and those in whom TB was not suspected (106 visits). All patients where TB was suspected had one or more symptoms suggestive of the diagnosis (cough, haemoptysis, night sweats, breathlessness, lymphadenopathy, and fever). However, in the 106 A&E visits where TB was not suspected, 61 (58%) cases had one or more symptoms suggestive of TB.
Of the 37 visits at which TB was suspected, the number of cases and the department of the clinician who raised the suspicion were: 29 A&E clinician, five general medicine, two surgical, one gynaecology. Of the cases that were unsuspected, the majority of cases were seen only by A&E clinicians. In all cases where presenting symptoms may have suggested TB (98 visits), 19 (19%) patients had a chest x ray performed and nine (9%) had sputum taken for acid-fast bacilli. Those patients that were not followed up later presented to A&E or another hospital department where the correct diagnosis was eventually made.
Many TB patients attended A&E where the diagnosis was unsuspected. In our district, with a high incidence of TB, A&E staff need better education about the diagnosis of TB.
P155 LONDON ACCIDENT AND EMERGENCY (A&E) DEPARTMENTS: AN OPPORTUNITY TO DIAGNOSE TUBERCULOSIS (TB) EARLY?
A. Smith, A. Goodburn, A. Story, R. Miller, G. Scott, H. Booth. TB Clinic, Middlesex Hospital, University College London Hospitals (UCLH), UK
TB is a major health problem in London, accounting for more than 40% of the national total. North Central London Sector has seen the highest rate of increase in TB since 1998 (155%), and is also the epicentre of an ongoing outbreak of isoniazid resistant TB. Early case finding remains an essential part of TB control.
Aims: (1) To identify the rate of usage of A&E to access healthcare in our TB patient population. (2) To identify whether A&E attendances present an opportunity to diagnose TB early.
Methods: TB notifications between the period from January 2001 to March 2002 (15 months), were cross referenced against A&E and microbiology records for the six month period prior to each notification.
Results: There were 171 TB notifications during this time. Of these, 48 (28%) patients were seen in A&E a total of 69 times prior to their diagnosis. Thirty two patients had pulmonary TB (19 smear positive) and 10 were HIV positive (one previously undiagnosed). Thirty five patients were admitted from A&E of which 27 were diagnosed as a direct result of their admission. Four patients were discharged from A&E with TB clinic follow up. Seventeen (eight admitted) of the 48 patients did not have TB diagnosed or considered at the time of their A&E attendance(s).
Conclusions: A third of our patients with subsequent TB diagnoses had attended A&E within the six month period preceding notification. This may reflect the difficulties that this patient population has in accessing healthcare by other means. It also serves to emphasise the key role A&E staff have to play in TB case finding among this population.
Thirty five out of 48 patients with TB were admitted, suggesting that these patients were systemically unwell on presentation, and emphasising the importance of liaison between acute general medical and TB services. In 17 out of 48 cases the diagnosis of TB was either not made or considered, representing a potential missed opportunity to diagnose TB early.
P156 PERFORMANCE STATUS ON ADMISSION TO HOSPITAL: A SIMPLE PREDICTOR OF DEATH IN PATIENTS WITH PULMONARY TUBERCULOSIS IN SOUTH AFRICA
S. De Valliere1, M. Nthangheni2, R.D. Barker3. 1Department of Medicine, Medical University of Southern Africa—Polokwane Campus, Pietersburg, South Africa; 2Statistics and Operations Research, University of the North, Private Bag X1106, Sovenga 0727, South Africa; 3King’s College Hospital, Bessemer Road, Camberwell, London, UK
Background: Simple measures are required to identify patients most at risk of dying from tuberculosis. Performance status has been used in studies of cancer patients but we are not aware that it has been tested as a predictor of mortality among patients with tuberculosis.
Methods: During a period of three months all adults (age ≥15years) admitted to one of six South African hospitals and put on anti-tuberculous treatment for suspected or confirmed pulmonary tuberculosis were eligible. At the time treatment was initiated performance status was recorded by the doctor or the nurse in charge. The vital status of the patient (alive or dead) was determined two months after initiation of treatment (table).
Results: 347 patients were admitted to hospital and started on TB treatment during the study period. For nine patients performance status was not obtained and so analysis has been restricted to the remaining 338 patients.
Discussion: Performance status at the time of diagnosis appears to be a powerful predictor of mortality in this population.
Supported by TB Alert.
P157 TUBERCULOSIS AND HIV SEROPREVALENCE IN LAMBETH, SOUTHWARK AND LEWISHAM, AN AREA OF SOUTH LONDON
M. Melzer1, A. Warley2, H. Milburn2, D. O’Sullivan3, R.D. Barker4, D. Shelton5, F. Drobniewski5, G.L. French2. 1Department of Infection and Tropical Medicine, Northwick Park Hospital, Watford Rd, Harrow, Middlesex HA1 3UJ; 2Department of Infection and Respiratory Medicine, Guy’s and St Thomas’ Hospital, Lambeth Palace Rd, London SE1 7GD; 3Lambeth, Southwark and Lewisham Health authority, 1 Lower Marsh St., Lambeth, London SE1 7NT; 4Department of Respiratory Medicine, King’s College Hospital, Denmark Hill, London SE5 9RS; 5Mycobacterium Reference Unit, Dulwich Hospital, East Dulwich Grove, London SE22 8QF, UK
Since the mid 1980s the number of cases of TB notified within the UK has continued to rise although the contribution of HIV to this rise remains unclear. A 12 month prospective cohort study was conducted at chest and HIV clinics in four hospitals in Lambeth, Southwark, and Lewisham (LSL), an area of South London, to determine the proportion of patients with culture-proven TB infected with HIV. Secondary aims were to determine the proportion of patients with TB and undiagnosed HIV at first presentation to chest clinics, to determine the proportion of patients presenting with TB as an AIDS defining illness (ADI) and to identify risk factors for co-infection with TB and HIV. In chest clinics, demographic data and left over blood from patients aged 16 or over with culture-proven TB was collected, anonymised, and HIV tested. In HIV clinics, demographic data on patients with TB already known to be HIV seropositive was also obtained. Twenty one patients (13%, 95% CI 8% to 19%) of 159 with culture-proven TB were infected with HIV. Four (3%) of 133 patients at first presentation to chest clinics had undiagnosed HIV; two were subsequently diagnosed. Of the 21 patients with TB and HIV, nine (43%) presented with TB as an ADI. Patients with TB and HIV were significantly more likely to be aged between 35–55 years compared to HIV seronegative patients (12/21 (57%) v 38/138 (28%), p=0.006). None of the patients from the Indian Subcontinent were HIV seropositive (0/21 v 25/138 (18%), p=0.047). At the present time, universal HIV testing of patients with culture-proven TB in chest clinics within the UK is unlikely to significantly reduce the number of patients with undiagnosed HIV.
P158 OUTCOME OF HIV ASSOCIATED TUBERCULOSIS IN THE ERA OF HIGHLY ACTIVE ANTIRETROVIRAL THERAPY (HAART)
K. Dheda, F. Lampe, M. Lipman, M. Johnson. Department of HIV and Thoracic Medicine, Royal Free Hospital, & School of Medicine, London, UK
Background: The benefit of HAART on outcome in TB/HIV co-infected patients is unclear due to concerns about drug adherence, absorption, overlapping toxicities, drug interactions, and paradoxical reactions. We therefore investigated the effect of HAART on survival in co-infected patients.
Methods: Ninety two HIV/TB co-infected patients treated at a London HIV clinic were retrospectively identified. Patients starting TB treatment prior to 1 January 1996 (n=36) were compared to those starting TB treatment after 1 January 1996 (n=56), when HAART was introduced. HAART was included as a time-updated covariate in a Cox regression model with adjustment for other prognostic factors.
Results: Compared to patients treated for TB prior to 1996, those treated during or after 1996 were older (median age 35 v 30), and were more likely to be women (43% v 17%), Black African (63% v 44%), and in the heterosexual risk group (68% v 47%). Baseline CD4 count tended to be lower for patients in the post-1996 compared to the pre-1996 group (73% versus 61% <200 /mm3). TB treatment with Rifabutin was much more common in the post-1996 group (34% v 6%). During a median of 2.6 years of follow up there were 29 deaths. Three years after initiation of TB treatment, survival was 63% in the pre-1996 group compared to 79% in the post-1996 group (p=0.19, log rank test over whole follow up period). This difference in survival was significant after adjustment for baseline CD4 count (HR for post-1996 versus pre-1996: 0.42; 95% CI 0.18 to 0.96, p=0.039). In a Cox model that included HAART use as time-updated variable, and adjusted for baseline CD4 count, extrapulmonary TB, previous AIDS and calendar period (pre or post 1996), the use of HAART resulted in a marked reduction in risk of death (HR: 0.26; 95% CI 0.10 to 0.72, p=0.009) and explained the effect of calendar period. Initial CD4 count < 200 /mm3 (HR: 3.4; 95% CI 1.3 to 9.3, p=0.015) and a prior history of AIDS (HR: 2.3; 95% CI 1.1 to 5.1, p=0.032) were also independently associated with risk of death.
Conclusion: Use of HAART in patients with TB/HIV co-infection results in a substantial reduction in risk of death.
P159 TUBERCULOSIS: A CHEAP DISEASE?
S. Berkovitz, R. Hurd, M. Mandani, D. Adler, N. Johnson. Whittington Hospital, London; Camden and Islington Community NHS Trust, UK
Tuberculosis is an increasing problem in some parts of London. Despite a lack of evidence, it is often regarded as a cheap disease to treat. To test this hypothesis, we describe the first comprehensive cost analysis of a dedicated adult tuberculosis service in a busy district general hospital.
All relevant care data was obtained for patients notified with tuberculosis or given chemoprophylaxis in the year 2000, up to their discharge from hospital care. Computerised information was obtained from hospital and tuberculosis office databases in addition to paper based tuberculosis record cards and medical notes. Mean costs for inpatient (£170 per bed night) and outpatient (£67 per appointment) episodes were provided by the Trust finance department and specific drug costs the hospital pharmacy.
Ninety seven patients were notified with tuberculosis and 23 patients given chemoprophylaxis. Mean age at notification was 37 years (median 29, range 13–91). Of the notified patients, 46 were admitted to hospital at some stage, 11 on two occasions. Mean length of stay was eight days (median one day, range 1–83). Two patients died in hospital. Completion rates for therapy were 89%. A summary of the cost analysis is shown in the table.
A summary of the cost analysis
Tuberculosis is not a cheap disease to treat. If control of tuberculosis is not taken seriously, it poses a considerable health economic problem.
P160 TUBERCULOSIS AND HEALTH BELIEFS IN THE BANGLADESHI COMMUNITY OF EAST LONDON
V. White1, S. Hillier2, J. Moore-Gillon1. 1Depts of Respiratory Medicine; 2Human Science and Medical Ethics, Bart’s and the London School of Medicine & Dentistry, EC1A 7BE, UK
We investigated the understanding and recognition of symptoms of TB, any associated stigma, use of alternative practitioners and attitudes to medication amongst Bangladeshi patients with TB in Tower Hamlets, east London. Forty three newly diagnosed subjects were approached and 41 took part. Twenty six were male and 15 female, aged 20–85 (median 36). 19 had pulmonary and 22 extra pulmonary TB. Each underwent two interviews, of c.1 h duration, the first within a few days of diagnosis, the second after 1–3 m treatment. Interviews were semi-structured, for analysis with NVivo software after transcription.
Strikingly, only two subjects admitted to knowing that TB could infect organs other than the lungs. Twenty four of the 41 associated cough, haemoptysis, and weight loss with TB, but the significance of fevers and night sweats was largely unrecognised. Most were afraid to discuss their diagnosis outside their close family, with 31 subjects believing there was significant stigma associated with TB and five stating that TB affected a sufferer’s prospects of marriage. While most (27) expressed no concerns about medication, the others were unhappy with size and/or number of tablets and duration of treatment. Only six admitted to pluralistic health practices: while adhering to standard therapy, they consulted religious leaders and took herbal remedies.
Seven subjects admitted to being not literate in any language. Adherence, assessed semi-objectively (including tablet counts and urine checks) was not related to literacy, proficiency in English, nor educational attainment, and the least compliant patient was UK university educated. Fear of TB, the desire for cure and respect for medical staff were the most commonly expressed reasons for adherence.
Our findings of lack of awareness of TB symptoms and of substantial stigma must give rise to concerns both about delays in presentation for medical care and regarding contact tracing. Culturally appropriate health education initiatives may help address these problems. We keep in mind, however, that our findings might not necessarily have been significantly different had we studied UK born white TB patients.
VLCW is supported by Bart’s Special Trustees and Spitalfields Community Trust.
P161 NO BOOSTER EFFECT IN BCG IMMUNISED TUBERCULOSIS CONTACTS UNDERGOING REPEAT HEAF TESTING
A.R. Martineau, M. Chaudery, J. Jeyanathan, G.E. Packe. Newham Chest Clinic, Shrewsbury Road, Forest Gate, London E7 8QP, UK
Individuals who undergo repeat tuberculin testing may exhibit increasing reaction size in the absence of new infection. This phenomenon is known as boosting. Boosting is thought to be commoner in BCG vaccinated individuals compared to non-vaccinated individuals.1 BTS guidelines only advise repeat tuberculin testing in non-BCG vaccinated TB contacts whose initial tuberculin (Heaf) test is negative.2
We performed a retrospective analysis of TB contacts to establish if there was an excess of increased Heaf reaction on repeat Heaf testing in BCG vaccinated individuals. One hundred and forty one TB contacts, with an initially negative Heaf test (grade 0–1), had repeat tuberculin testing at our clinic (74 female; age range 18 days to 60 years). Sixteen had neither history of BCG nor BCG scar; 119 had either (n=19) or both (n=100); six had no recorded details of BCGstatus and were excluded from the analysis. In 34 cases, the grade of the 2nd Heaf test was unequivocally higher than the grade of the 1st Heaf test. In the remainder (101 cases) it was not. 27/119 (22.7%) of those with previous BCG demonstrated an increase in Heaf grade, compared with 7/16 (43.8%) of those with no evidence of previous BCG (table).
These results do not support the contention that boosting is more common in BCG vaccinated subjects.
1.
.
2. Joint Tuberculosis Committee of the British Thoracic Society.
.