Article Text

Presented in part at the Annual Congress of the European Respiratory Society 1999 in Madrid and at the World Congress on Lung Health 2000 in Florence.
Abstract
BACKGROUND Pulmonary sarcoidosis is characterised by a mononuclear alveolitis with a predominance of CD4+ T cells and macrophages. We determined the intracellular expression of interferon (IFN)γ, interleukin (IL)-2, tumour necrosis factor (TNF)α, IL-4, IL-5 and IL-10 in CD4+ and CD8+, naive and memory lymphocytes from blood and bronchoalveolar lavage (BAL) fluid using three colour flow cytometry.
METHODS Eighteen untreated patients with pulmonary sarcoidosis were evaluated and stratified according to whether they had acute or chronic disease.
RESULTS Significantly more T cells expressed Th1 than Th2 type cytokines in both BAL fluid and peripheral blood samples, regardless of clinical presentation. Significantly greater proportions of T cells secreted Th1 type cytokines in BAL fluid than in peripheral blood. Th1 type cytokines were more frequently expressed by peripheral and alveolar T cells in acute disease than in chronic disease. There were no significant differences between CD4+ and CD8+ T cells. Concerning naive and memory lymphocytes, significantly higher CD45RO:CD45RA ratios were found in BAL fluid than in blood, and increased expression of Th2 type cytokines was found in peripheral compared with alveolar memory T cells.
CONCLUSIONS Our data support the immunopathogenetic concept of Th1/Th2 imbalance and compartmentalisation in pulmonary sarcoidosis and suggest that the cytokine patterns change during the course of disease. Expression of Th2 type cytokines in memory lymphocytes is decreased in the alveolar compartment compared with peripheral blood.
- sarcoidosis
- Th1/Th2 cytokines
- flow cytometry
Statistics from Altmetric.com
The hallmark of pulmonary sarcoidosis is a mononuclear alveolitis which is characterised by activated CD4+ lymphocytes, monocytes/macrophages, and non-caseating granulomas. An imbalance in the expression of Th1 and Th2 type cytokines by alveolar cells is thought to play an important role in the immunopathogenesis of sarcoidosis.1-5 It is well established that Th1 type cytokines are important mediators in pulmonary sarcoidosis and that there is a dependence of granulomatous inflammation on type 1 cytokines.1 ,2 Previous authors have shown a spontaneous release from alveolar cells of the Th1 type cytokines interferon (IFN)γ and interleukin (IL)-2 but not Th2 type cytokines.3 ,4 ,6-8 However, in a study using CD4+ T cell clones from bronchoalveolar lavage (BAL) fluid, Bäumeret al 9 found equal levels of Th1 and Th2 cytokine gene expression in patients with sarcoidosis. Thus, the conditions which favour a Th1 or Th2 pattern in the course of the disease remain to be clarified.
It has been shown that compartmentalisation of cytokine production occurs in pulmonary sarcoidosis2 ,10 with alveolar lymphocytes releasing more cytokines than peripheral cells. In this context the state of activation of peripheral and alveolar T cells is of interest as previous studies found high ratios of memory to naive alveolar cells in patients with sarcoidosis,11 and there is evidence that memory cells have a different pattern of cytokine release.12 In addition, the contribution of CD4– lymphocyte subpopulations to the release of Th1/Th2 cytokines in sarcoidosis has not been studied to date. Although the CD8+ T cells are in a minority among BAL cells from sarcoidosis patients, their relative proportion increases in later stages of the disease. They might therefore play a part in cytokine release of sarcoid alveolitis.
A central question is the relevance of Th1/Th2 type cytokines to the course of the disease, which may be important with respect to the fibrogenic potential of Th2 type cytokines such as IL-4 in cryptogenic fibrosing alveolitis.13 ,14 Since there are few data from longitudinal studies on the Th1/Th2 response in patients with pulmonary sarcoidosis, data on the Th1/Th2 cytokine pattern during different phases of the disease are needed. Some studies have divided patients into those with active and those with non-active sarcoidosis and found higher levels of Th1 type cytokine mRNA in the group with active disease.4 Since the clinical activity of sarcoidosis does not correlate clearly with the prognosis, we preferred to differentiate between sarcoidosis patients with acute and chronic disease to evaluate the cytokine production in different stages of the disease.
The aim of the present study was to determine (1) whether there is an imbalance in Th1/Th2 cytokine expression and a difference in the intracellular cytokine profiles between blood and BAL fluid lymphocytes from sarcoidosis patients; (2) whether there is a difference in the cytokine profile between CD4+ and CD8+ T cells from sarcoidosis patients; (3) whether there is an association between the cytokine patterns of patients with sarcoidosis and an acute or chronic course of disease; and (4) whether differences in the cytokine patterns of naive and memory lymphocytes contribute to changes in cytokine profiles between the different patient groups.
Methods
SUBJECTS
We investigated 18 patients with histologically proven sarcoidosis who were not being treated with systemic steroids at the time of the investigation. The patients were divided into two groups according to duration of symptoms: acute disease with symptoms lasting <2 years and chronic disease with symptoms for >2 years.15 ,16 This division was identical with the radiographic appearance: all patients with acute disease had a type I chest radiograph (bilateral hilar lymphadenopathy) and all patients with chronic disease had a type II radiograph (hilar lymphadenopathy plus reticulonodular parenchymal infiltrates) or type III radiograph (parenchymal infiltration without hilar adenopathy). There were no significant differences in demographic data. Four patients with acute disease had Löfgren's syndrome (erythema nodosum, bilateral hilar lymphadenopathy, polyarthralgias) and there were similar frequencies of extrapulmonary involvement in both groups (table 1).
Clinical characteristics of sarcoidosis patients with acute onset of disease and chronic course of disease
BRONCHOALVEOLAR LAVAGE
After sedation with midazolam (3–10 mg) and topical anaesthesia with 2% lidocaine, bronchoalveolar lavage was performed with a fibreoptic bronchoscope (B71T20D; Olympus, Hamburg, Germany) under standard conditions for diagnostic purposes. In the patients with acute onset of disease this was done when they presented with acute symptoms. Informed written consent was obtained from all patients. Six to eight 20 ml aliquots of sterile saline were instilled and immediately re-aspirated. The mean recovery was 95 (7.5) ml (59.4% of the instilled volume). From the pellet differential cell counts of 500 cells were performed after two washes in sterile saline solution and staining with Wright-Giemsa. The viability of the cells was routinely assessed by trypan blue exclusion and was always >95%.
PREPARATION OF CELLS
Heparinised blood was obtained shortly before the BAL was performed during bronchoscopy. Peripheral blood mononuclear cells (PBMC) were isolated using density gradient centrifugation (Ficoll; Seromed, Berlin, Germany). Alveolar cells and PBMC were washed twice in Hank's balanced salt solution (HBSS; Sigma, Deisenhofen, Germany) and resuspended in RPMI 1640 with 2.0 g/l NaHCO3 (Seromed) containing 10% fetal calf serum (Seromed), 1% penicillin/streptomycin (Sigma), and 1% glutamine (ICN, Eschwege, Germany) at a concentration of 1 × 106 cells/ml.
INTRACELLULAR CYTOKINE STAINING
The cells were processed as described previously.17Briefly, PBMC and alveolar cells were stimulated with 10 ng/ml PMA (Sigma) and 1 μM ionomycin (Sigma) and transport of newly synthesised cytokines from the Golgi apparatus was blocked with 3 μM monensin (Sigma). They were then incubated for 5 hours at 37°C with 5% CO2. The cells were then harvested, washed with HBSS, fixed with HBSS containing 4% paraformaldehyde (Riedel-deHaen AG, Seelze, Germany), washed again twice with HBSS, and resuspended in saponin buffer (HBSS containing 0.1% saponin (Riedel-deHaen AG) and 0.01 M Hepes buffer (Seromed)) for permeabilisation. They were incubated for 20 minutes at 4°C in the dark with the following directly conjugated anti-cytokine and surface marker antibodies: (1) fluorescein conjugated: anti-CD45RO and anti-CD8 (both Pharmingen, San Diego, USA); (2) R-phycoerythrin conjugated: anti-IFNγ, anti-IL-2, anti-TNFα, anti-IL-4, anti-IL-10 and anti-IL-5 (all Pharmingen); (3) Cy-Chrome conjugated: anti-CD45RA and anti-CD3 (both Pharmingen). After washing the cells once they were finally resuspended in HBSS.
FLOW CYTOMETRY
The cytokine expression was determined in CD3+CD8+, CD3+CD8–, CD3+CD45RO+, and CD3+CD45RA+ lymphocytes by three colour flow cytometry (FACScan, Becton Dickinson, Heidelberg, Germany). CD3+CD8– T cells were taken as CD3+CD4+ T cells after preliminary experiments had shown that these two populations are >95% congruent (data not shown).
Isotype specific antibodies (Pharmingen) belonging to the same Ig subclass as the monoclonal antibodies against the intracellular cytokines were used for setting thresholds for cytokine positivity.
For gating and calculation, Cell Quest software (Becton Dickinson) was used. Gating for lymphocytes using forward/sideward scatter was facilitated by CD3/CD8 staining; 20 000 cells were determined with at least 100 cells in every gate of lymphocyte subpopulations. The resulting numbers are percentages of cytokine expression of those subpopulations.
STATISTICAL ANALYSIS
Statistical comparison between the two study groups was performed using the Student's t test for independent samples. Results are given as means with 95% confidence intervals of mean differences unless otherwise stated. Differences between blood and BAL fluid from the same patient were tested by the Wilcoxon matched pairs test and the results are given as medians with 95% confidence intervals of median differences unless otherwise stated. Correlations were tested with the Spearman rank test. A p value of <0.05 was considered significant.
Results
BAL FLUID
As expected, patients with sarcoidosis had high total cell counts in the BAL fluid with a lymphocytic alveolitis as well as a raised CD4/CD8 ratio in patients with acute compared with chronic disease (table 2).
BAL fluid data of sarcoidosis patients with acute onset of disease and chronic course of disease
ACUTE V CHRONIC SARCOIDOSIS
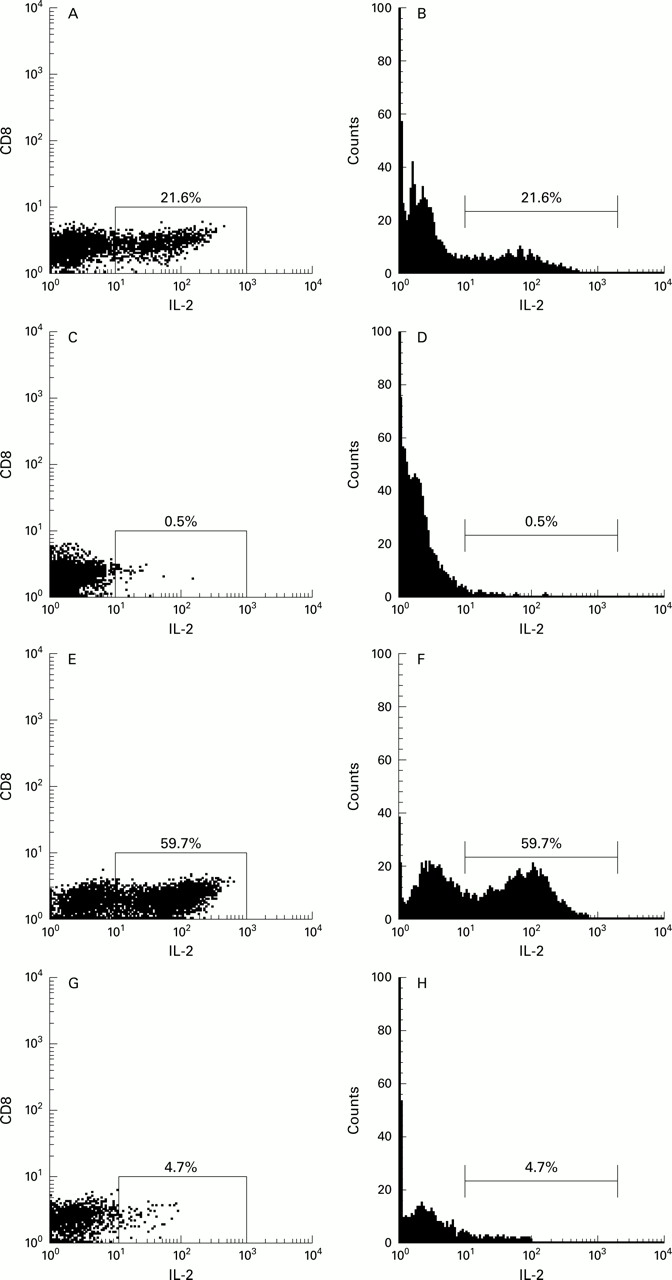
In patients with acute disease significantly higher proportions of peripheral and alveolar T lymphocytes (CD4+ as well as CD8+) expressed Th1 type cytokines than in those with chronic disease (representative examples of dot plots and histograms of IL-2 expression shown in fig1).
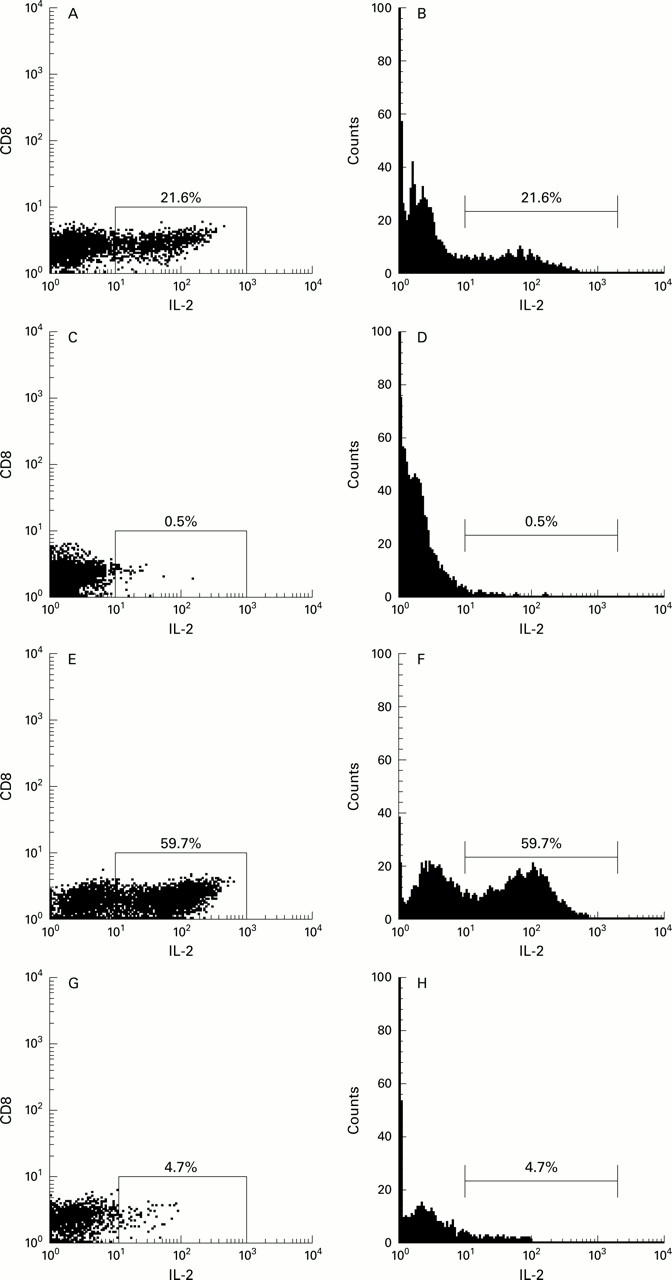
FACS dot plots and histograms. Representative examples of IL-2 expression in peripheral and alveolar CD4+ T cells from sarcoidosis patients with acute and chronic disease. CD4+ cells were gated as CD3+/CD8– lymphocytes. (A) and (B), peripheral CD4+ T cells in acute disease; (C) and (D), peripheral CD4+ T cells in chronic disease; (E) and (F), alveolar CD4+ T cells in acute disease; (G) and (H), alveolar CD4+ T cells in chronic disease.
Mean IFNγ expression in patients with acute disease was significantly increased in alveolar CD4+ T cells (54.2% v20.5% (95% CI of mean difference 7.6 to 60.0)) and in alveolar and peripheral CD8+ T cells (58.7% v 20.9% (95% CI 6.4 to 69.1) and 30.4% v 5.9% (95% CI 8.6 to 40.4), respectively). In peripheral CD4+ T cells IFNγ was only slightly increased (11.5% v 4.2% (95% CI –0.8 to 15.4), NS; fig 2).
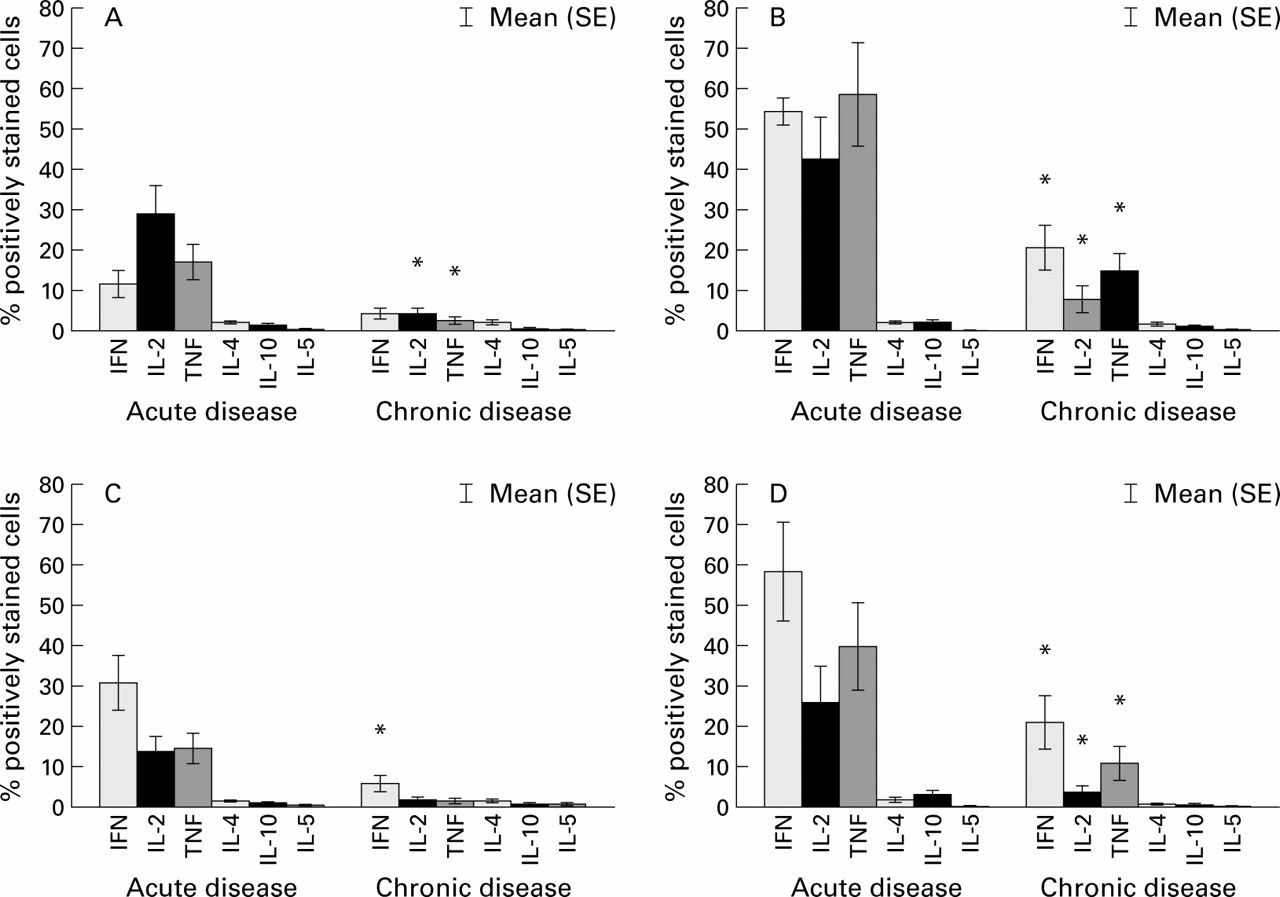
Intracellular cytokine expression in T cells from sarcoidosis patients with acute onset of disease (n=9) compared with patients with chronic disease (n=9). (A) Expression in peripheral CD4+ T cells; (B) expression in alveolar CD4+ T cells; (C) expression in peripheral CD8+ T cells; (D) expression in alveolar CD8+ T cells. *p<0.05 compared with acute onset of disease.
There was a significantly higher expression of IL-2 in alveolar and peripheral CD4+ T cells from patients with acute onset of disease (42.3% v 8.0% (95% CI 10.9 to 57.8) and 28.7% v 4.2% (95% CI 7.8 to 41.2), respectively), and in alveolar and peripheral CD8+ T cells (25.7%v 3.8% (95% CI 1.4 to 42.5) and 13.5%v 1.8% (95% CI 3.2 to 20.1), respectively). TNFα expression was also significantly increased in patients with acute disease (alveolar and peripheral CD4+ T cells: 58.5% v 14.8% (95% CI 15.2 to 72.4) and 16.8% v 2.5% (95% CI 4.2 to 24.3), respectively; alveolar and peripheral CD8+ T cells: 39.7%v 10.8% (95% CI 2.4 to 55.4) and 14.3%v 1.7% (95% CI 4.1 to 21.2), respectively). The proportion of cells expressing the Th2 type cytokines IL-4, IL-5 and IL-10 was generally low (0.2–3.2%) and there were no significant differences between patients with acute and chronic disease except for a significant increase in IL-10 expression in alveolar CD8+ T cells (3.2% v 0.7% (95% CI 0.4 to 4.6)) from patients with acute compared with chronic disease. This finding may be explained by a strong correlation between TNFα and IL-10 expression in alveolar CD8+ T cells (r=0.69; p<0.01).
PERIPHERAL V ALVEOLAR CELLS
Alveolar T cells (CD4+ as well as CD8+) showed a significantly higher expression of Th1 type cytokines than peripheral cells. Median IFNγ expression was significantly increased in alveolar CD4+ and CD8+ T cells compared with peripheral cells (20.2%v 3.6% (95% CI of median difference 12.1 to 44.0) and 16.7% v 8.5% (95% CI 8.7 to 34.8), respectively) and similar differences were observed in the expression of IL-2 and TNFα.
CD4+ V CD8+ T CELLS
No significant differences in cytokine expression between alveolar or peripheral CD4+ and CD8+ T cells were observed, regardless of disease progression. In general, CD8+ T cells showed a slightly lower rate of Th1 type cytokine expression; however, mean IFNγ expression was significantly higher in peripheral CD8+ T cells than in CD4+ T cells from patients with acute disease (30.4%v 11.5% (95% CI of mean difference 0.9 to 37.0), p<0.05). Again, the expression of Th2 type cytokines was very low in both subpopulations of T cells.
CYTOKINE EXPRESSION OF NAIVE AND MEMORY LYMPHOCYTES
The cytokine pattern of naive and memory lymphocytes was investigated to assess the influence of T cell activation on cytokine expression in patients with acute and chronic disease.
As expected, the CD45RO+:CD45RA+ ratio was significantly higher (21.9v 0.6 (95% CI 18.2 to 44.6)) in BAL fluid than in blood from all patients in the study group. Increased proportions of memory lymphocytes were found in the blood of patients with chronic disease compared with those with acute disease, but there was no difference in the BAL fluid between the patient groups (fig3).

{kind=link}
{kind=link}
{kind=link}
CD45RO:CD45RA ratio in blood and BAL fluid from patients with sarcoidosis: (A) in blood compared with BAL fluid from all sarcoidosis patients (*p<0.05 compared with blood; box = median ± interquartile difference; whiskers = 5–95%); (B) in blood from patients with acute onset of disease compared with chronic disease (*p<0.05 compared with acute onset of disease); (C) in BAL fluid from patients with acute onset of disease compared with chronic disease.
Increased Th1 cytokine expression occurred in memory lymphocytes compared with naive lymphocytes in both blood and BAL fluid. In addition, we observed greater expression of Th2 type cytokines in peripheral memory lymphocytes than in naive lymphocytes (table 3). However, CD45RA positive lymphocytes were also able to express effector cytokines such as IFNγ in smaller proportions. This pattern of cytokine expression does not explain differences in the cytokine profiles between acute and chronic sarcoidosis, since greater Th1 cytokine expression in patients with acute disease than in those with chronic disease was found in both memory and naive lymphocytes (data not shown), and the increased Th2 cytokine expression of peripheral memory lymphocytes was equally observed in both patient groups: IL-4 expression in CD45RO+ v CD45RA+ lymphocytes in acute disease 5.9% v 1.3% (95% CI 1.4 to 7.9), in chronic disease 4.4% v 0.5% (95% CI 0.7 to 7.1).
Mean (SE) cytokine expression in peripheral and alveolar memory and naive lymphocytes from all sarcoidosis patients
Discussion
In this study we have shown that Th1 type cytokines are the predominant lymphokines in pulmonary sarcoidosis. As described previously,18-20 a marked increase in the expression of IFNγ, IL-2, and TNFα was observed. By using three colour flow cytometry we were able to differentiate between the two subgroups of T cells (CD4+ and CD8+) and their activation state (CD45RA+ (naive) and CD45RO+ (memory)), as this method allowed simultaneous staining of surface markers and intracellular cytokines at the single cell level.
In contrast to the high rate of Th1 cytokine expression, the expression of Th2 type cytokines (IL-4, IL-10, and IL-5) was generally low. These data are in accordance with data from other studies.3 ,4 ,6-8 Alveolar T cells may either be biased to Th1 type by the surrounding milieu, which is characterised by high levels of IL-12 and low levels of IL-10 in sarcoidosis patients,7 or they may have lost their potential to produce and release Th2 type cytokines before selective transmigration from the circulation to the pulmonary compartment. However, in a previous study using T cell clones from different compartments, the main distinction between peripheral and bronchoalveolar clones was a shift to both ends of the spectrum (Th1 and Th2) in CD4+ T cell clones generated from BAL fluid.9 This difference might be explained by the methods used as T cell clones have to be stimulated in vitro so that the results represent the overall capacity of T cells to produce Th1 and Th2 cytokines and not their expression in vivo. One limitation to our approach of comparing proportions of cytokine expressing cell populations is the fact that cytokine expression does not necessarily correlate with the biological activity which may be different at the molecular level. Moreover, the concept of Th1/Th2 dichotomy, which is derived from experimental models of intracellular infection, may be an oversimplification of the immunological process21 and a broad pattern of cytokine profiles between the extremes of pure Th1 and Th2 types may be found in clinical disease.
As there is a lack of longitudinal studies on Th1/Th2 response in patients with pulmonary sarcoidosis, we decided to study the Th1/Th2 patterns in both the acute and chronic phases of the disease as we were interested in the change in cytokine pattern with the duration of the disease. Accordingly, we chose a definition which is based on comprehensive clinical data15 ,16 and may differentiate between patients with a high probability of spontaneous remission and those with a more protracted course of disease. In our study this stratification corresponded to the radiological type of disease. We found that significantly higher proportions of T cells from patients with acute onset of disease expressed Th1 type cytokines than T cells from patients with chronic disease. Expression of Th2 type cytokines was low and there were no differences between the two groups in this respect. One might predict higher expression of Th2 type cytokines in T cells from patients with chronic disease following the hypothesis that Th2 type cytokines are important mediators of fibrosis in interstitial lung disease.2 ,14 ,22 Our failure to demonstrate such a pattern may be explained by the fact that all but one of our patients with chronic disease had a type II chest radiograph and consequently no evidence of end stage lung fibrosis. Nevertheless, our finding of higher proportions of Th1 type cytokines in patients with acute disease supports the hypothesis that cytokines play an important role in the course of pulmonary sarcoidosis and may influence the development into a chronic disease. In this regard, Prior and Haslam23 have shown that patients with high serum levels of IFNγ have a better chance of achieving a complete resolution after treatment with oral corticosteroids, which corresponds to the lower IFNγ expression we found in our patients with chronic sarcoidosis. Unfortunately, we were not able to evaluate the impact of treatment in our population as our patients had not received corticosteroids for a longer period before the investigation.
Little is known about the CD8+ T cells in pulmonary sarcoidosis because studies in the past have focused on CD4+ T cells as they are the major T cell population in the lung of patients with sarcoidosis. However, Agostini et al 24 observed a CD8 alveolitis in 3.8% of patients with sarcoidosis, and the proportion of CD8+ T cells has been shown to increase in chronic disease in relation to CD4+ T cells.25 Accordingly, in our study the CD4/CD8 ratio in this subgroup decreased to 30% of the value in acute disease despite comparable total cell counts in the BAL fluid. Moreover, we observed that CD8+ T cells from patients with sarcoidosis did not differ from CD4+ T cells in their cytokine expression in blood and BAL fluid. In general, their rate of cytokine expression was only slightly lower than that of CD4+ T cells and, in blood from patients with acute disease, they even expressed more IFNγ. This indicates that CD8+ T cells are not passive bystanders of the immune response but exhibit a similar pattern of activation and mediator release as the CD4+ T cells. Thus, the role of CD8+ T cells in sarcoidosis may have been underestimated in the past.
Supporting the concept of compartmentalisation of the immunopathogenesis of pulmonary sarcoidosis,2 ,10 we found a higher expression of Th1 type cytokines in alveolar cells than in peripheral T cells. Moreover, we observed higher CD45RO:CD45RA ratios in BAL fluid than in blood, as shown previously.11 In this regard, similar results were obtained from the epithelial surface of the normal lower respiratory tract, a tissue constantly exposed to environmental antigens.26 The most likely explanation is that memory T cells accumulate in inflamed tissues by selective margination, migration, and/or proliferation in response to antigen contact.27 Since differences in cytokine release between memory and naive lymphocytes have been described predominantly in healthy subjects,12 we compared their intracellular cytokine expression to assess the influence of T cell activation on the cytokine profiles in the different patient groups. Overall, the differences in the CD45RO:CD45RA ratios between acute and chronic sarcoidosis did not correspond to the observed cytokine patterns as Th1 type cytokines were increased in acute disease, but the proportion of memory lymphocytes was the same in both groups (BAL fluid) or even decreased in patients with acute disease (blood). Interestingly, when comparing alveolar and peripheral memory lymphocytes we found lower proportions of Th2 type cytokine producing cells in the alveolar compartment and consequently a surplus of Th1 type cytokines. This finding may be explained by a reduced potential of alveolar memory lymphocytes to produce Th2 type cytokines due to a chronic upregulation of IL-12 and a relative absence of IL-10, as mentioned above,7 ,28 or to selective migration and enrichment of Th1 cells in the lung.
In conclusion, our data support the immunopathogenetic concept of compartmentalisation and the predominance of CD4+ T cells producing mainly Th1 type cytokines in acute pulmonary sarcoidosis, which becomes less prominent during the course of the disease. CD8+ T cells seem to react in the same way as CD4+ T cells showing comparable cytokine patterns. Little is known about their function in pulmonary sarcoidosis so this has to be elucidated in future studies. In addition, longitudinal studies are needed to evaluate the effect of different cytokine patterns on the course of the disease.
Acknowledgments
The authors would like to thank Joachim Müller-Quernheim and Gernot Zissel for helpful discussion, Thomas Kohlmann for statistical advice, and Ute Wegener and Barbara Fischer for excellent technical assistance.