Article Text

Statistics from Altmetric.com
A 60-year-old Caucasian man was admitted to our emergency department with progressive dyspnoea, chronic cough and general asthenia. Physical examination revealed lack of left chest wall motion and absent breath sounds over the left hemithorax.
Vital signs were stable with a heart rate of 90 bpm, blood pressure of 120/70 mm Hg, respiratory rate of 20 breaths per minute and oxygen saturation by pulse oximetry of 95% while breathing room air.
The patient reported being an active smoker with a 40 pack-year smoking history. He also had a history of type IV osteogenesis imperfecta, a connective tissue pathology that could be associated with lung abnormalities.1 ,2
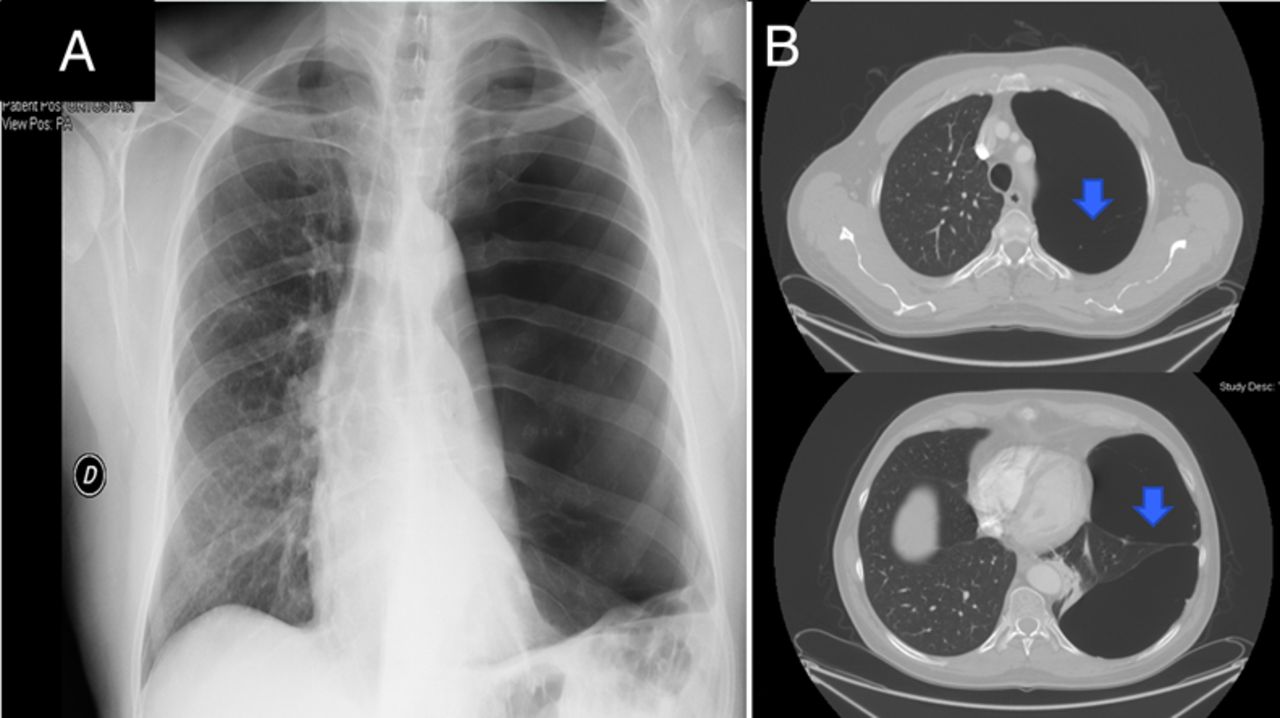
A chest radiograph (figure 1A) was suggestive of a left massive pneumothorax that may require emergency insertion of a chest tube thoracostomy. However, a distinct pleural line could not be identified on the chest radiograph and bronchovascular pattern was visible in the left base of the lung.

Chest radiograph suggestive of a left massive pneumothorax (A) and CT scan revealing two giant bullae with internal division and septae separated by a small area of lung parenchyma (B).
Therefore, the patient underwent a CT scan, which revealed two giant bullae of the left upper and lower lobes with multiple intrabullae septae (figure 1B). Though chest ultrasonography could not be performed due to lack of equipment in the emergency department, it could have proved useful to identify pleural sliding. However, given that the patient was haemodynamically stable and not in significant respiratory distress, we opted to obtain the definitive diagnostic test, which is a chest CT scan.3
The patient underwent left thoracotomy for the resection of the two giant bullae (figure 2A, B). This led to a complete re-expansion of the left lung after surgery (figure 2C). The patient was discharged after 5 days without any postoperative complications. Of note, the α1-antitripsin level was normal.

{kind=link}
{kind=link}
View of the giant bullae during surgery when it is inflated (A) and when air flow is interrupted before resection with the whole lung re-expanded (B). The postoperative chest radiograph shows left lung expansion (C).
In conclusion, we report an interesting and previously unreported case of osteogenesis imperfecta and giant bullae successfully treated by bullae resection.
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.