Article Text

Abstract
Introduction The Incremental Shuttle Walk Test (ISWT) assesses exercise capacity in patients with Chronic Obstructive Pulmonary Disease (COPD). Guidelines suggest 2 ISWTs should be performed. However, in patients who have been admitted with an acute exacerbation, it is unknown if 2 ISWTs are required.
Objective To investigate if a practice ISWT is needed for inpatients with an acute exacerbation of COPD.
Methods Patients admitted to hospital with an acute exacerbation completed 2 ISWTs, prior to discharge. Patients gave written informed consent (ISRCTN84599369) and were included if they used the same oxygen and mobility aid (if any) between tests.
Results 37 inpatients with COPD (19 male) were included: mean (SD) 67.89(8.02) years with BMI 24.66(6.60), FEV1 was 1.07(0.44)l[41.94(13.72)% predicted], FEV1/FVC 47.11(11.70)%, median (inter-quartile range) MRC dyspnoea grade 4(3–5), resting Borg breathlessness 2(0.5–3) and 11 had never exercised.
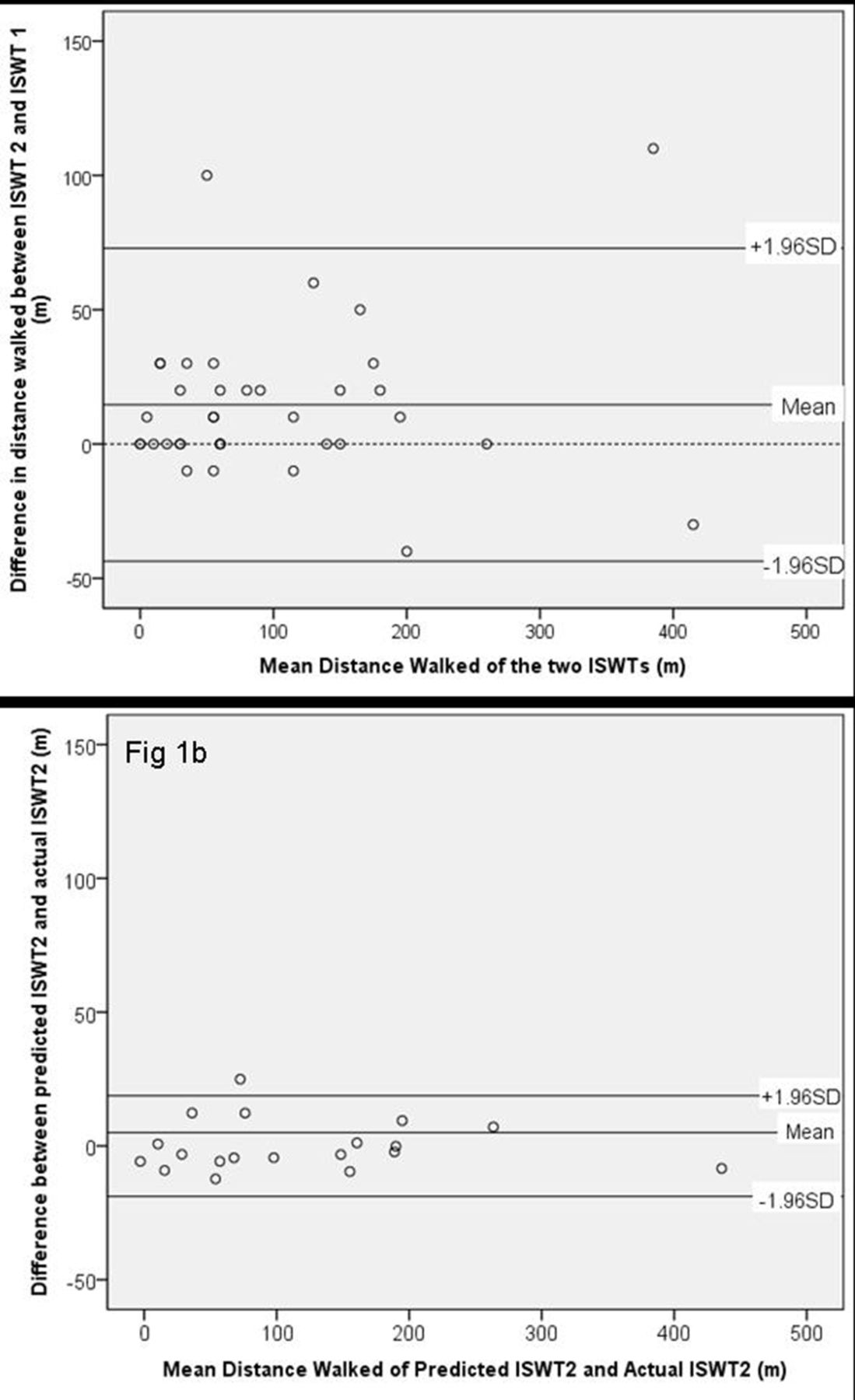
Participants achieved ISWT1 92.16(97.67)m, post-HR 108.64(14.33), post-SaO2 90.33(3.89), post-Borg breathlessness 4(3–5) and post-Rated Perceived Exertion (RPE) 13(13–15). There was a statistically significant increase of 14.59(29.12)m for ISWT2 (p < 0.05) but no significant differences in HR, SaO2, Borg or RPE. Bland Altman plot (Figure 1a) shows acceptable agreement between the ISWTs.
When calculating Endurance Shuttle Walk Test (ESWT) level at 85% VO2 peak as estimated from ISWT1 and ISWT2, there was a significant increase of one level (p < 0.05).
Multiple regression explained 92.1% of the variance (F (9–18)p < 0.001, R2 0.921) of the difference between ISWTs using FEV1%predicted, FEV1/FVC%, BMI, exercise history, resting SaO2, ISWT1 distance, ISWT1 post-SaO2, post-Borg and post-RPE (p < 0.05). Using the multiple regression equation to calculate predicted ISWT2, there was good agreement (Figure 1b) and no significance difference between this and actual ISWT2 (0.04 m, p > 0.05).
Conclusions There was a small but statistically significant increase between ISWTs, which was below the minimal clinically important difference. However, this difference changed the ESWT level for some patients which would have had consequences for exercise prescription.
This exploratory work has shown that we can predict the difference between ISWTs using a multiple regression equation which could substitute the need for a second ISWT; this needs to be confirmed prospectively. A practice ISWT is therefore not necessarily needed in this patient group.
{kind=link}
Bland Altman Plots showing agreement between ISWT1 and ISWT2 and 1b predicted ISWT2 and actual ISWT2