Article Text

Abstract
A 73 year old man developed chest pains 5 minutes after fibreoptic bronchoscopy. The procedure had been performed without sedation following an intratracheal injection of 5 ml 2.5% cocaine solution and xylocaine spray to the pharynx for topical anaesthesia. A 12-lead electrocardiogram showed an evolving anterior myocardial infarction. Cardiac catheterisation revealed coronary artery spasm in the proximal left anterior descending artery at the site of non-significant plaque disease. The risk factors, mechanisms, and treatment of cocaine induced myocardial infarction following intratracheal injections are discussed.
- fibreoptic bronchoscopy
- cocaine
- myocardial infarction
Statistics from Altmetric.com
Cardiovascular complications of fibreoptic bronchoscopy, although infrequent, are more common in the elderly.1 A number of methods are available for the induction of topical anaesthesia in fibreoptic bronchoscopy, including the use of transtracheal 2.5% cocaine solution and xylocaine spray to the pharynx.2 Coronary artery spasm secondary to cocaine use for other reasons is well documented as a cause of myocardial infarction in the presence of normal coronary arteries.3,4 We report a case of an acute myocardial infarction in a patient with “normal” coronary arteries following fibreoptic bronchoscopy using intratracheal cocaine.
CASE REPORT
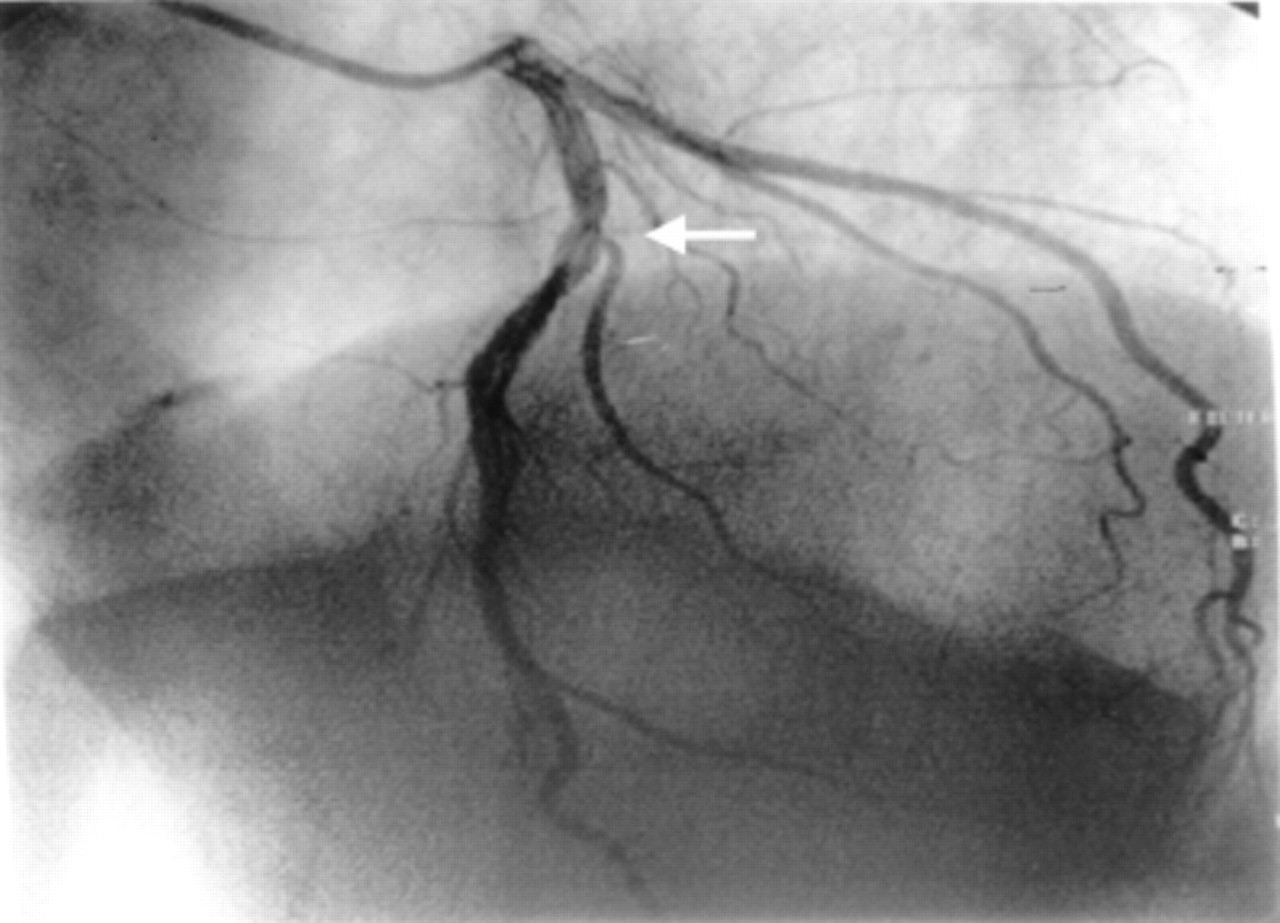
A 73 year old man with mild asthma was referred to the rapid access chest clinic with a history of breathlessness, cough, and weight loss. He had no risk factors for ischaemic heart disease apart from smoking cigarettes over a period of 2 years in his forties. Physical examination was unremarkable. The pre-bronchoscopy electrocardiogram (ECG), urea, and electrolytes were normal. Spirometric tests showed an obstructive airways pattern (forced vital capacity (FVC) 2.57 l, forced expiratory volume in 1 second (FEV1) 1.24 l, FEV1/FVC ratio 48). His chest radiograph showed some ill defined peripheral shadowing in the upper zones. Fibreoptic bronchoscopy was performed with an intratracheal injection of 5 ml 2.5% cocaine solution and several puffs of xylocaine spray to the pharynx for topical anaesthesia. The bronchoscopic examination was uneventful and revealed a normal endobronchial tree. However, 5 minutes after the procedure the patient became distressed with dyspnoea, tachycardia, and chest pain. He was given intravenous hydrocortisone and aminophylline for signs of bronchospasm. A 12-lead ECG showed an evolving anterior myocardial infarction (fig 1). He was taken to the cardiac catheterisation laboratory with a view to primary angioplasty. Coronary angiography revealed a non-significant stenosis (<25%) in the proximal left anterior descending artery with coronary artery spasm (fig 2). Cardiac troponin T was raised at 1.19 μg/l (normal range <0.01) indicating some myocardial damage. He was treated with aspirin and intravenous heparin and made an uneventful recovery. Bronchial lavage fluid grew Haemophilus influenza and Staphylococcus aureus for which he was treated with oral clarithromycin. There was no evidence of any underlying malignancy.
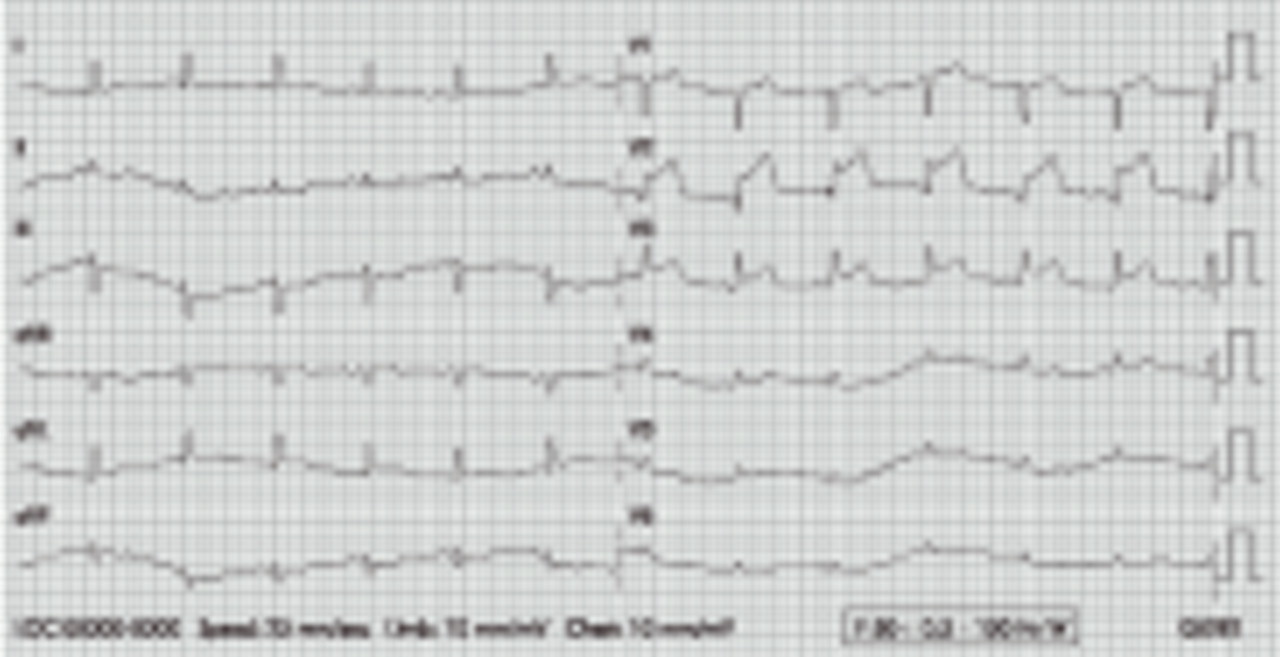
ECG showing evolving anterior myocardial infarction.

{kind=link}
{kind=link}
Coronary angiogram showing coronary artery spasm in the proximal left anterior descending artery.
DISCUSSION
Day case fibreoptic bronchoscopy is routinely performed in many centres using intratracheal 2.5% cocaine solution and xylocaine spray to the pharynx. It has recently been shown that toxic systemic levels of cocaine (>0.9 mg/l) are attained following intratracheal injection of 5 ml 2.5% cocaine solution. The peak median cocaine concentration was 1.42 mg/l 1 hour after intratracheal injection and toxic levels of 1.34 mg/l were maintained at the time of discharge 2 hours after the procedure.5 However, a study by Graham et al comparing this method of local anaesthesia with either bronchoscopic injections of cocaine or nebulised lidocaine (lignocaine) has shown it to be better tolerated and the preferred method of local anaesthesia by both patients and bronchoscopists.2 Cardiovascular sequelae of this procedure include a rise in blood pressure and heart rate which can be associated with ST segment depression or transient bundle branch block, especially in the elderly smoker.1 These changes can be attributed to cocaine.
Cocaine is cardiotoxic and its use has been linked to coronary artery spasm, angina, myocardial infarction, arrhythmias, sudden cardiac death, and myocardial contraction bands, which might act as a substrate for arrhythmias.3,6 Its principal cardiac effects are mediated via four main pathways7,8:
-
Increased myocardial oxygen demand due to an acute rise in systemic blood pressure and heart rate.
-
Coronary vasoconstriction caused by its α1 adrenergic properties and calcium dependent direct vasoconstriction.
-
Endothelial dysfunction which predisposes to vasoconstriction and thrombosis.
-
Promotion of arteriosclerosis.
It is important to avoid beta-blockers in treating cocaine induced chest pains or acute myocardial infarctions as this may result in unopposed α1 adrenergic action with worsening coronary spasm. Calcium channel antagonists or nitrates should be administered as early as possible. Cardiac catheterisation is an important first step to determine if vasospasm is the dominant pathology which can potentially be reversed by intracoronary injection of vasodilators, or if it is occurring at a point where pre-existing plaques are present when percutaneous transluminal angioplasty (PCTA) and intracoronary stenting may be useful. The presence of thrombus is best treated with IIB/IIIA receptor blocking drugs.
This case illustrates a potentially severe complication of a routine and common investigation, the effects of which may be minimised if recognised and treated early. Furthermore, these risks remain present at the time of discharge in day case procedures, and are greater in those patients with pre-existing atherosclerosis, the elderly, and smokers due to underlying endothelial dysfunction. For the same reason, hypertensive and diabetic patients must be considered at high risk. Patients at high risk should be observed for longer periods or told to return to the unit should they develop chest pains soon after discharge. Bronchoscopists might wish to consider using lidocaine in these high risk groups which, although less efficacious, has a lower risk of cardiac complications.9