Article Text

Statistics from Altmetric.com
- ARDS, acute respiratory distress syndrome
- CAP, community acquired pneumonia
- CNS, central nervous system
- COPD, chronic obstructive pulmonary disease
- CSF, cerebrospinal fluid
- GP, general practitioner
- HDU, high dependency unit
- ICU, intensive care unit
- ILI, influenza-like illness
- NIV, non-invasive ventilation
- PCT, primary care trust
SYNOPSIS OF MAIN RECOMMENDATIONS
Scope and purpose
-
This document is intended for use in the UK in the event that the World Health Organization declares that an influenza pandemic has started,1 and the Department of Health in England (UK-wide lead agency on pandemic influenza, including the devolved administrations) has declared UK Pandemic Alert Level 2 (cases of pandemic influenza identified within the UK).
-
These guidelines are not relevant for the management of patients affected by seasonal/interpandemic influenza, lower respiratory tract infections, community acquired pneumonia or exacerbations of chronic obstructive pulmonary disease (COPD).
-
Once an influenza pandemic is under way, users are strongly urged to ensure that they refer to the most up-to-date version of these guidelines (from web-based access points).
SYNOPSIS 1 CLINICAL MANAGEMENT OF ADULTS REFERRED TO HOSPITALS
S1.1 Severity assessment in hospital
-
Patients with uncomplicated influenza infection would be expected to make a full recovery and do not require hospital care.
-
In uncomplicated infection, the illness usually resolves in seven days although cough, malaise and lassitude may persist for weeks.
-
Patients with worsening of pre-existing comorbid medical conditions should be managed according to best practice for that condition with reference to published disease-specific guidelines, if available, for example the National Institute for Health and Clinical Excellence’s COPD guidelines.
S1.2 Influenza-related pneumonia
-
In hospital, patients with influenza-related pneumonia and who have a CURB-65 score of 3, 4 or 5 (see Box A) are at high risk of death and should be managed as having severe pneumonia.
-
Patients with bilateral lung infiltrates on chest radiography consistent with primary viral pneumonia should be managed as having severe pneumonia regardless of CURB-65 score.
-
Patients who have a CURB-65 score of 2 are at increased risk of death. They should be considered for short stay inpatient treatment or hospital supervised outpatient treatment. This decision is a matter of clinical judgment.
-
Patients who have a CURB-65 score of 0 or 1 are at low risk of death. They can be treated as having non-severe pneumonia and may be suitable for home treatment.
Box A CURB-65 score
Score 1 point for each feature present:
-
Confusion (mental test score of ⩽8, or new disorientation in person, place or time)
-
Urea >7 mmol/l
-
Respiratory rate ⩾30/min
-
Blood pressure (SBP <90 mmHg or DBP ⩽60 mmHg)
-
Age ⩾65 years
S1.3 High dependency or intensive care unit transfer
-
Patients with primary viral pneumonia or a CURB-65 score of 4 or 5 should be considered for high dependency unit (HDU)/intensive care unit (ICU) transfer.
-
General indications for HDU/ICU transfer include:
persisting hypoxia with PaO2 <8 Kpa despite maximal oxygen administration
progressive hypercapnia
severe acidosis (pH<7.26)
septic shock
-
Patients with influenza admitted to intensive care units should be managed by specialists with appropriate training in intensive care, respiratory medicine and/or infectious diseases.
S1.4 General investigations
-
The investigations shown in table A are recommended in patients referred to hospital.
-
In those patients who are subsequently followed up in a hospital outpatient clinic or by a general practitioner (GP), a repeat chest x ray should be obtained at around six weeks if respiratory symptoms or signs persist or where there is a higher risk of underlying malignancy (especially smokers and those over 50 years of age).
-
Further investigations including a CT thoracic scan and bronchoscopy should be considered if the chest x ray remains abnormal at follow up.
S1.5 Microbiological investigations
S1.5.1 Early in a pandemic (UK alert levels 1, 2 and 3)
Virology—all patients
-
Nose and throat swabs in virus transport medium.
-
If presentation is more than seven days after onset of illness, an “acute” serum (5–10 ml clotted blood) should be collected and a “convalescent” sample (5–10 ml clotted blood) obtained after an interval of not less than seven days.
Bacteriology—patients with influenza-related pneumonia
-
Blood culture (preferably before antibiotic treatment is commenced)
-
Pneumococcal urine antigen (20 ml urine sample)
-
Legionella urine antigen (20 ml urine sample)
-
Sputum gram stain, culture and antimicrobial susceptibility tests on samples obtained from patients who:
are able to expectorate purulent samples, and
have not received prior antibiotic treatment.
-
Paired serological examination for influenza/other agents. Acute serum should be collected and a “convalescent” sample obtained after an interval not less than seven days (both 5–10 ml clotted blood).
S1.5.2 Once a pandemic is established (UK alert level 4)
Virology—not routinely recommended
Bacteriology—patients with influenza-related pneumonia in accordance to the severity of illness
-
Non-severe pneumonia (CURB-65 Score 0, 1 or 2)
No routine testing.
In patients who do not respond to empirical antibiotic therapy, sputum samples should be sent for Gram stain culture and antimicrobial susceptibility tests.
-
Severe pneumonia (CURB-65 Score 3, 4 or 5, or bilateral chest x ray changes)
Blood culture, preferably before antibiotic treatment is commenced
Pneumococcal urine antigen (20 ml urine)
Sputum gram stain, culture and antimicrobial susceptibility tests on samples obtained from patients who are able to expectorate purulent samples, and have not received prior antibiotic treatment.
Paired serological examination for influenza/other agents. “Acute” serum should be collected and a “convalescent” sample obtained after an interval not less than seven days (both 5–10 ml clotted blood).
Tracheal or endotracheal aspirate samples, if available, should be sent for Gram stain, culture and antimicrobial susceptibility testing.
S1.6 General management
S1.6.1 Initial management
-
Hypoxic patients should receive appropriate oxygen therapy with monitoring of oxygen saturations and inspired oxygen concentration with the aim to maintain PaO2 ⩾8 Kpa and SaO2 ⩾92%. High concentrations of oxygen can safely be given in uncomplicated pneumonia.
-
Oxygen therapy in patients with pre-existing COPD complicated by ventilatory failure should be guided by repeated arterial blood gas measurements. Non-invasive ventilation (NIV) may be helpful.
-
In patients without pre-existing COPD who develop respiratory failure, NIV may be of value as a bridge to invasive ventilation in specific circumstances when level 3 beds are in high demand. Respiratory and/or critical care units experienced in the use of NIV are best placed to ensure the appropriate infection control measures are adopted at all times.
-
Patients should be assessed for cardiac complications and also volume depletion and their need for additional intravenous fluids.
-
Nutritional support should be given in severe or prolonged illness.
S1.6.2 Monitoring in hospital
-
Temperature, respiratory rate, pulse, blood pressure, mental status, oxygen saturation and inspired oxygen concentration should be monitored and recorded initially at least twice daily and more frequently in those with severe illness or requiring regular oxygen therapy. An Early Warning Score system is a convenient way to perform this.
-
In patients who are not progressing satisfactorily a full clinical reassessment and a repeat chest radiograph are recommended.
S1.6.3 Discharge and follow up
-
Patients should be reviewed 24 hours prior to discharge. Those with two or more of the following unstable clinical factors should be considered for remaining in hospital:
temperature >37.8°C
heart rate >100/min
respiratory rate >24/min
systolic blood pressure <90 mmHg
oxygen saturation <90%
inability to maintain oral intake
abnormal mental status.
-
Follow up clinical review should be considered for all patients who suffered significant complications or who had significant worsening of their underlying disease, either with their GP or in a hospital clinic.
-
At discharge or at follow up, patients should be offered access to information about their illness, take home medication and any follow up arrangements.
-
It is the responsibility of the hospital team to arrange the follow up plan with the patient and the GP.
S1.7 Use of antivirals
-
Individuals should only be considered for treatment with antivirals (neuraminidase inhibitors) if they have all of the following:
an acute influenza-like illness (ILI)
fever (>38°C) and
been symptomatic for two days or less.
-
Treatment schedule: adults, oseltamivir 75 mg every 12 hours for five days (dose to be reduced by 50% if creatinine clearance is less than 30 ml/min—that is, 75 mg od)
-
Patients who are unable to mount an adequate febrile response—for example, the immunocompromised or very elderly—may still be eligible for antiviral treatment despite lack of documented fever.
-
Hospitalised patients who are severely ill, particularly if also immunocompromised, may benefit from antiviral treatment started more than 48 hours from disease onset, although there is no evidence to demonstrate benefit, or lack of, in such circumstances.
S1.8 Antibiotic management
S1.8.1 Influenza not complicated by influenza-related pneumonia
-
Previously well adults with acute bronchitis complicating influenza, in the absence of pneumonia, do not routinely require antibiotics.
-
Antibiotics should be considered in those previously well adults who develop worsening symptoms (recrudescent fever or increasing dyspnoea).
-
Patients at high risk of complications or secondary infection (Appendix 2) should be considered for antibiotics in the presence of lower respiratory features.
-
Most patients can be adequately treated with oral antibiotics.
-
The preferred choice includes co-amoxiclav or a tetracycline.
-
A macrolide such as clarithromycin (or erythromycin) or a fluoroquinolone active against Streptococcus pneumoniae (S pneumoniae) and Staphylococcus aureus (S aureus) is an alternative choice in certain circumstances.
S1.8.2 Non-severe influenza-related pneumonia
-
Most patients can be adequately treated with oral antibiotics.
-
Oral therapy with co-amoxiclav or a tetracycline is preferred.
-
When oral therapy is contraindicated, recommended parenteral choices include intravenous co-amoxiclav, or a second or third generation cephalosporin (cefuroxime or cefotaxime).
-
A macrolide (erythromycin or clarithromycin) or a fluoroquinolone active against S pneumoniae and S aureus is an alternative regimen where required—for example, for those intolerant of penicillins. Currently levofloxacin and moxifloxacin are the only recommended fluoroquinolones licensed in the UK.
-
Antibiotics should be administered within four hours of admission.
S1.8.3 Severe influenza-related pneumonia
-
Patients with severe pneumonia should be treated immediately after diagnosis with parenteral antibiotics.
-
An intravenous combination of a broad spectrum beta-lactamase stable antibiotic such as co-amoxiclav or a second (for example, cefuroxime) or third (for example, cefotaxime) generation cephalosporin together with a macrolide (for example, clarithromycin or erythromycin) is preferred.
-
An alternative regimen includes a fluoroquinolone with enhanced activity against pneumococci together with a broad spectrum β-lactamase stable antibiotic or a macrolide. Currently levofloxacin is the only fluoroquinolone with an intravenous formulation licensed in the UK.
S1.8.4 Route and duration of antibiotic
-
Patients treated initially with parenteral antibiotics should be transferred to an oral regimen as soon as clinical improvement occurs and the temperature has been normal for 24 hours, providing there is no contraindication to the oral route.
-
For most patients admitted to hospital with non-severe and uncomplicated pneumonia, seven days of appropriate antibiotics is recommended.
-
For those with severe, microbiologically undefined pneumonia, 10 days’ treatment is proposed. This should be extended to 14–21 days where S aureus or Gram negative enteric bacilli pneumonia is suspected or confirmed.
S1.8.5 Failure of empirical antibiotics
-
For those with non-severe pneumonia in hospital on combination therapy, changing to a fluoroquinolone with effective pneumococcal and staphylococcal cover is an option.
-
Adding further antibiotics effective against MRSA is an option for those with severe pneumonia not responding to combination antibiotic therapy.
SYNOPSIS 2 CLINICAL MANAGEMENT OF CHILDREN REFERRED TO HOSPITAL
S2.1 Severity assessment in children (see Appendix 5)
S2.1.1 In the community
-
Coughs and mild fevers. These children should be treated at home by parents with antipyretics and fluids (note: aspirin should not be used in children).
-
High fever (>38.5°C) and cough or influenza-likesymptoms. These children should seek advice from a community health professional. If there are no features that put them at high risk of complications they should be treated with oseltamivir, and given advice on antipyretics and fluids. Children aged <1 year and those at risk of complications (Appendix 2) should be seen by a genral practitioner.
-
High fever (>38.5°C) and cough or influenza-like symptoms, plus at risk group. These children should be seen by a GP or in A&E. Children may be considered at increased risk of complications if they have cough and fever (or ILI) and temperature >38.5°C, plus either chronic comorbid disease or one of following features:
breathing difficulties
severe earache
vomiting >24 hours
drowsiness.
These patients should be offered an antibiotic as well as oseltamivir (in those >1 year of age) and advice on antipyretics and fluids. Children aged <1 year with none of the above features should be treated with antipyretics and fluids with a low threshold for antibiotics if they become more unwell.
S2.1.2 Hospital admission
Indicators for hospital admission are:
-
Signs of respiratory distress
markedly raised respiratory rate
grunting
intercostal recession
breathlessness with chest signs
-
Cyanosis
-
Severe dehydration
-
Altered conscious level
-
Complicated or prolonged seizure
-
Signs of septicaemia—extreme pallor, hypotension, floppy infant
Most children admitted to hospital are likely to need oxygen therapy and/or intravenous support as well as antibiotics and oseltamivir.
Indications for transfer to high dependency or intensive care are:
-
failure to maintain a SaO2 of >92% in FiO2 of >60%
-
the child is shocked
-
severe respiratory distress and a raised PaCO2 (>6.5 Kpa)
-
rising respiratory rate and pulse rate with clinical evidence of severe respiratory distress with or without a raised PaCO2
-
recurrent apnoea or slow irregular breathing
-
evidence of encephalopathy
When there are no paediatric intensive care unit beds available, children will have to be triaged on the basis of the severity of their acute and coexisting disease, and the likelihood of their achieving full recovery.
S2.2 General investigations for children in hospital
-
A full blood count with differential, urea, creatinine and electrolytes, liver enzymes and a blood culture should be done in all severely ill children.
-
A chest x ray should be performed in children who are hypoxic, have severe illness or who are deteriorating despite treatment.
-
Pulse oximetry should be performed in every child being assessed for admission to hospital with pneumonia.
S2.3 Microbiological investigations in hospital
S2.3.1 Early in a pandemic (UK alert levels 1, 2 and 3)
Virology—all children
-
Nasopharyngeal aspirate or nose and throat swabs.
-
If presentation is more than 7 days after onset of illness, an “acute” serum (2–5 ml clotted blood) should be collected and a “convalescent” sample (2–5 ml clotted blood) obtained after an interval of not less than 7 days.
Bacteriology—children with influenza-related pneumonia
-
Blood culture (before antibiotic treatment is commenced).
-
Sputum samples obtained from older children.
-
Paired serological examination for influenza/other agents.
S2.3.2 Once a pandemic is established (UK alert level 4)
Virology—not routinely recommended
Bacteriology—children with influenza-related pneumonia
-
Blood culture (before antibiotic treatment is commenced).
-
Sputum samples obtained from older children.
-
Paired serological examination for influenza/other agents.
S2.4 General management of children admitted to hospital
-
Patients whose oxygen saturation is 92% or less while breathing air should be treated with oxygen given by nasal cannulae, head box, or face mask to maintain oxygen saturation above 92%.
-
When children are unable to maintain oral intake, supplementary fluids should, when possible, be given by the enteral route. Intravenous fluids in those with severe pneumonia should be given at 80% basal levels.
-
Children can be safely discharged from hospital when they
are clearly improving
are physiologically stable
can tolerate oral feeds
have a respiratory rate <40/min (<50/min in infants)
have an awake oxygen saturation of >92% in air.
S2.5 Antiviral therapy in children
-
In the setting of a pandemic, children should only be considered for treatment with antivirals if they have all of the following:
an acute ILI
fever (>38.5°C) and
been symptomatic for two days or less.
-
Oseltamivir is the antiviral agent of choice.
-
In children who are severely ill in hospital oseltamivir may be used if the child has been symptomatic for <6 days (but there is no evidence to demonstrate benefit or lack of it in such circumstances).
S2.6 Antibiotic therapy in children
-
Children (a) who are at risk of complications of influenza or (b) with disease severe enough to merit hospital admission during an influenza pandemic should be treated with an antibiotic that will provide cover against Spneumoniae, S aureus and Haemophilus influenzae (H influenzae).
-
For children under 12 years co-amoxiclav is the drug of choice. Clarithromycin or cefuroxime should be used in children allergic to penicillin. For children over 12 years doxycycline is an alternative.
-
Oral antibiotics should be given if oral fluids are tolerated.
-
Children who are severely ill with pneumonia complicating influenza should have a second agent added to the regime (for example, clarithromycin or cefuroxime) and the drugs should be given intravenously to ensure high serum and tissue antibiotic levels.
1 INTRODUCTION
1.1 Scope and purpose
This document contains guidance for health professionals regarding the treatment of pandemic influenza, agreed by experts from the British Infection Society, the British Thoracic Society and the Health Protection Agency. It is published as official UK guidance by the Department of Health in England and covers treatment in hospitals and the community, of both adults and children. It is intended for use in the UK in the event that the World Health Organization declares that an influenza pandemic has started,1 and the Department of Health in England (UK-wide lead agency on pandemic influenza, including the devolved administrations) has declared UK Pandemic Alert Level 2 (cases of pandemic influenza identified within the UK; see Appendix 1).2
This guidance should be read in conjunction with UK Infection Control Guidance for Pandemic Influenza,3 the Department of Health UK Pandemic Influenza Contingency Plan,2 Operational Guidance for Health Service Planners,4 and the Operational Framework for stockpiling, distributing and using antiviral drugs in the event of pandemic influenza5 and the Primary Care Operational Plan.
To facilitate preparedness planning, this document has been written in advance of the emergence of the next influenza pandemic, at a time when the identity of the causative virus remains unknown.
These guidelines are based on the best evidence available from previous pandemic and interpandemic influenza periods. The guidance may evolve as clinicopathological information on the eventual pandemic virus emerges. Once an influenza pandemic is under way, users are strongly urged to refer to the most up-to-date version of these guidelines (from web-based access points).
1.2 Context
Seasonal influenza is a familiar infection in the UK, especially during winter. Every year strains of influenza (type A or B) circulate, giving rise to clinical consultations in primary care (age-specific impact varies by season), episodes of hospital treatment (mainly in older persons and young children, but occasionally in working age adults), and deaths (mainly in the elderly). Treatment in primary care and hospital may be required due to the direct effects of influenza virus infection or its possible complications, most commonly secondary bacterial pneumonia. Increases in GP consultations for ILI and winter bed pressures are frequently associated with periods of known community influenza activity.6
Pandemic influenza occurs when a new influenza A virus subtype emerges which is markedly different from recently circulating subtypes and strains, and is able to:
-
infect humans;
-
spread efficiently from person to person;
-
cause significant clinical illness in a high proportion of those infected.
Because the virus is novel in humans, a high proportion of the population will have little or no immunity, producing a large pool of susceptible persons; accordingly the disease spreads widely and rapidly.
Influenza pandemics occur sporadically and unpredictably. In 1918, a devastating and unusual pandemic caused by influenza A/H1N1 (“Spanish flu”) killed between 20 and 40 million people worldwide. Other pandemics that followed had a less devastating impact but were nevertheless severe. Influenza A/H2N2 (“Asian flu”) emerged in 1957 and H3N2 (“Hong Kong flu”) in 1968; both caused roughly 1 million excess deaths worldwide.7
The circumstances still exist for a new influenza virus with pandemic potential to emerge and spread, and the longest interval so far recorded between pandemics is 39 years (1918–57). The unpredictability of the timing of the next pandemic is underlined by the occurrence of several large outbreaks of highly pathogenic avian influenza associated with epizootic transmission to humans.8 By far the most serious has been the massive and unprecedented outbreak of highly pathogenic influenza (A/H5N1) affecting poultry in East and South East Asia in late 2003, which is still continuing. This outbreak has so far been associated with a small number of human cases but a high proportion of deaths. Recently, epidemiological and virological changes have been reported from northern Viet Nam which may indicate that the virus is beginning to adapt to humans.9 Although the emergence of an A/H5N1 strain with capacity to spread efficiently between humans is neither inevitable nor imminent, international concern has increased regarding the possibility that avian influenza A/H5N1 may evolve to produce the next pandemic.
Other events and developments that inform the creation of this guidance are the development and licensing of a new class of drug (neuraminidase inhibitors) active against influenza, and UK government’s announcement of plans to procure 14.6 million treatment courses of oseltamivir (Tamiflu®)10 for use in the UK in the event of a pandemic.
1.3 Who are these guidelines aimed at?
These guidelines are offered for the guidance of all UK hospital doctors and primary care physicians. In the event of a pandemic, it is envisaged that all healthcare practitioners, regardless of individual specialisation, may be involved in the management of patients with influenza. It is intended that these guidelines also be of value to healthcare practitioners who do not usually manage patients with influenza but may be called upon to do so in a pandemic situation. Modification of some recommendations at a local level may be necessary in specific instances.
These guidelines are not relevant for the management of patients affected by seasonal influenza, sporadic acute exacerbations of COPD, lower respiratory tract infections or community acquired pneumonia (CAP).
1.4 Primary care
At the primary care level, a national Operational Plan including the following three broad areas is deemed important:
-
clinical management of patients with influenza
-
management of patient demand, including patients who do not have influenza
-
health service delivery plans.
These guidelines cover the first of these areas and will serve as the source document for the Primary Care Operational Plan. The Primary Care Operational Plan will incorporate all three areas within a single reference and is being developed by the Department of Health in collaboration with the Royal College of General Practitioners and the British Medical Association.
1.5 Healthcare delivery modes
Even though it is impossible to predict with certainty the impact of the next pandemic, based upon the available epidemiological and modelling information, it is clear that it will generate demands for health care which may saturate or overwhelm normal NHS acute services for a period of time, perhaps several weeks or months. Accordingly, it should be anticipated that the NHS (in common with all health systems around the world) will need to revert to emergency arrangements. These are laid out in further detail in Operational Guidance for Health Service Planners,4 the UK Operational Framework for stockpiling, distributing and using antiviral drugs in the event of pandemic influenza5 and in the Primary Care Operational Plan. With regard to the delivery of medical care for patients with influenza this is normally achieved through:
-
GP treatment of community patients “well” enough to be managed in the community
-
hospital care in acute medicine for persons considered too ill to be managed at home.
In the event of a pandemic, the following additional care settings may have to be considered as the threshold for hospital admission rises:
-
treatment of patients in the community (who would normally receive care from a GP) by other healthcare professionals (nurses, paramedics, pharmacists, etc) following treatment guidance laid out in this publication and using prescription-only medicines according to Patient Group Directives
-
treatment of patients in their own homes or in temporary intermediate care facilities by a GP, following treatment guidance laid out in this publication when, under normal circumstances, such patients would have been admitted for hospital care
-
treatment of severely ill patients in hospital by medical and nursing teams who do not normally manage patients with influenza or CAP, in areas of the hospital not normally used for providing medical care (for example, surgical teams and bed space diverted from routine elective work towards pandemic response).
1.6 Grading of recommendations
The recommendations offered in the current guidelines are based on a matrix of evidence centred mainly around seasonal influenza, expert opinion and group consensus. Grading of these recommendations based on the strength of the evidence base was deemed inappropriate.
2 EPIDEMIOLOGY AND HEALTH IMPACT PROJECTIONS
Summary
-
The scale and severity of illness (and hence consequences) caused by pandemic influenza generally exceed those of even the most severe winter epidemics.
-
Mortality in the UK is likely to exceed 50,000 deaths, possibly much higher.
-
Besides the elderly, excess mortality is also likely in younger adults and children.
-
Modelling studies suggest that after a case occurs in Hong Kong, because of international travel, it will take less than one month for the virus to reach the UK.
-
Once cases begin to occur in the UK it will take only 2–3 weeks before activity is widespread and roughly a further three weeks (six weeks after initial cases in UK) until activity peaks.
-
It is possible that there will be more than one epidemic wave (with an interval of several months) and, if a second wave occurs, it may be more severe than the first.
-
Cumulative clinical and serological attack rates across all waves together may be in the order of 25% and 50% respectively.
-
Increases in demand for healthcare services are likely to be very substantial in both primary care and hospital settings.
2.1 Introduction
When an influenza pandemic occurs, a substantial proportion (possibly all) of the population is likely to be non-immune, producing a large pool of susceptible persons. In past pandemics, the scale and severity of illness (and hence consequences) have been variable but broadly of a higher order than even the most severe winter epidemics. It is reasonable to expect this to be the case with the next pandemic as well.
2.2 Excess mortality
Excess mortality due to influenza occurs in most winter seasons but is especially marked during epidemics. The average annual excess mortality attributable to influenza in recent years is around 12,000 deaths per annum in England and Wales,11 although there is considerable yearly variation and some years are notably much higher than the average (estimated 26,000 in 1989/90 epidemic). Excess mortality in England and Wales associated with the three pandemics of the twentieth century has also varied widely; this was estimated at 198,000 civilians in 1918/19, and 37,500 in 1957/58. In 1968/69 and 1969/70 (both seasons considered to be associated with the influenza A/H3N2 pandemic), there were an estimated 31,000 and 47,000 deaths respectively.7 Therefore the extent of mortality associated with the next pandemic cannot be reliably predicted although it is reasonable to plan for a scenario worse than a severe winter epidemic of normal influenza.
2.3 Age distribution of morbidity and mortality
Typically, there are changes in the age distribution of cases compared with seasonal influenza. Mortality, which in typical seasonal influenza is usually confined to age groups over 65 years, tends to be increased in younger age groups. The size of any increase in morbidity and mortality and the extent to which a shift in age distribution occurs depend on a variety of factors including the nature of the pandemic virus and pre-existing immunity but appears to be a consistent phenomenon.12 Therefore, clinicians can expect to see relatively larger amounts of influenza-related illness in younger adults compared with normal winter activity. At least one third of all excess deaths may be expected in persons under 65 years of age.
2.4 Geographical and temporal spread
Virological and clinical surveillance of influenza have improved markedly since the last pandemic in 1968. However, the extent of international travel has also grown. Modelling studies using transmission characteristics based on the 1968/69 pandemic and international air-traffic data from 2002 indicate that the approximate delay between a first case in Hong Kong and first introduction to UK will be less than one month13 In terms of the spread within the UK, it will probably take only 2–3 weeks from the initial introduction(s) until activity is widespread and a further three weeks (six weeks from initial UK cases) until activity peaks.
The temporal and spatial spread of a pandemic strain is important, particularly in terms of the demand placed on healthcare services. Pandemic activity taking the form of a brief but severe peak in cases will be more difficult for all services to cope with, compared with an identical number of cases distributed over a longer time course. For example, during the A/H3N2 pandemic a long first wave occurred in the winter of 1968/69 with morbidity and mortality approximately at the same level as the previous seasonal influenza; but in the following winter of 1969/70 a short and more severe epidemic occurred with a threefold higher peak in general practice consultation rates and a fourfold higher peak in mortality attributed to influenza, bronchitis and pneumonia. The high peak in consultation rates is well illustrated in figure 2.1.
2.5 Pandemic waves
In 1918/19, the A/H1N1 pandemic occurred in three distinct epidemic waves: early spring 1918, autumn 1918 and late winter 1919. The second wave was by far the largest and case-fatality rates were also higher than in the first wave. The A/H3N2 pandemic caused an epidemic wave in the winter of 1968/69 but a more severe one in 1969/70. In contrast, the second wave of the 1957/58 pandemic in the UK was very small in comparison to the first.7 Thus it should be considered a possibility that more than one wave of influenza will occur within a few months of the emergence of a pandemic virus and a subsequent wave could be worse than the first.
2.6 Health impact projections
It is impossible to predict reliably with precision the level of excess mortality that will be experienced in the next pandemic. However, table 2.1 illustrates the broad range of excess mortality that it is reasonable to consider, based on various realistic combinations of case fatality rate and clinical attack rates derived from previous pandemics and epidemics.
A case fatality rate of 0.37% corresponds to the aggregate rate observed in recent epidemic seasons (1989/90, 1991/92, 1993/94, 1995/96, 1996/97, 1997/98 and 1998/99) and the 1957 pandemic, although the overall case-fatality rate observed in the 1918–19 pandemic was in the region of 1–2%. A clinical attack rate of around 25% corresponds to the approximate clinical attack rate seen in all three previous pandemics of the twentieth century. Thus, a figure of at least 50,000 excess deaths is likely.
Using mathematical projections, it is possible to illustrate the potential impact of the next pandemic, but these do not amount to accurate predictions. Table 2.2 summarises the number of events that might be expected by a GP with 1000 patients on his/her list and by a Primary Care Trust (PCT) serving a population of 100,000 persons.
Using the same assumptions, table 2.3 illustrates the number of events by week over an assumed 15 week (single wave) pandemic period in a typical PCT population of 100 000. Most major acute trusts receive patients from a catchment area spanning several PCTs and the figures below require pro-rata adjustment before applying to individual hospitals.
3 CLINICAL FEATURES IN ADULTS
Summary
-
Influenza is clinically defined as the presence of fever and new (or, in those with chronic lung disease, worsening) cough of acute onset in the context of influenza circulating in the community. This clinical definition may be modified once a pandemic occurs.
-
The spectrum of clinical disease associated with a pandemic strain cannot be forecast.
-
Pneumonia, either primary viral or secondary bacterial, is the commonest complication of influenza in adults.
-
Neurological complications are rare in adults.
3.1 How reliable is a clinical diagnosis of influenza infection during a pandemic?
The clinical manifestations of infection by influenza viruses are diverse, ranging from asymptomatic infection to fulminant respiratory distress leading to respiratory failure and death. Furthermore, the presence of an ILI comprising of a combination of fever, cough, sore throat, myalgia and headache is not specific for influenza infection. Other respiratory pathogens that may present with an ILI include viruses such as respiratory syncytial virus (RSV), adenovirus, rhinovirus and parainfluenza virus, as well as bacterial pathogens such as Chlamydia pneumoniae, Legionella sp, Mycoplasma pneumoniae and S pneumoniae.14–16
Studies that have examined the value of a clinical definition of ILI in the diagnosis of influenza infection have not always used the same clinical definition for an ILI and have included different study populations, making comparison between studies complicated. A systematic review of the literature in this area identified the threefold combination of the presence of fever, cough and acute onset to be the most predictive clinical features. The accuracy of this clinical definition was higher in persons aged 60 years and above compared to patient groups without age restrictions (positive likelihood ratio (95% CI) 5.4 (3.8 to 7.7) v 2.0 (1.8 to 2.1)).17 The probability of influenza infection also increases with increasing level of fever.18,19
Importantly, the predictive value of clinical definitions based on an ILI increases when influenza virus is known to be circulating in the community.15,17,20 In cohort studies, correlation of ILI with laboratory-confirmed influenza infection ranges from 25–45%, while in clinical trials rates of 70% have been consistently reported.15,21–23
Box 3.1 Clinical case definition of influenza (March 2006)
The presence of fever and new (or, in those with chronic lung disease, worsening) cough of acute onset in the context of influenza circulating in the community. (Important note: this definition may be modified once a pandemic occurs.)
These findings relate to influenza infections during interpandemic periods. During a global influenza pandemic, when a pandemic strain is known to be circulating locally in an immunologically susceptible population, the presence of an ILI would be expected to be highly predictive for influenza infection. (However, the extent to which a clinical diagnosis of ILI becomes predictive during a pandemic will also be determined by the behaviour of the public. If many, who would not normally present to a health professional, are prompted to present, then the predictive value of a clinical diagnosis of ILI will be reduced.)
3.2 What are the clinical features of uncomplicated influenza?
The following description will relate mainly to interpandemic influenza A infections. Influenza B and C are not considered pandemic threats. Different strains may be associated with different clinical presentations and disease severity. For instance, there is evidence to suggest that the H3N2 subtype causes more severe disease than H1N1 subtype.24 The spectrum of clinical disease associated with a new influenza A subtype (for example, a pandemic strain) cannot be determined currently and may differ from that described for interpandemic influenza.
The incubation period prior to the onset of symptoms is commonly 2–4 days (range 1–7 days). In adults, the illness typically presents as an abrupt onset of fever accompanied by a range of other symptoms as listed in Box 3.2.25–29
Box 3.2 Range of symptoms associated with uncomplicated influenza infection
-
Cough (∼85%)
-
Malaise (∼80%)
-
Chills (∼70%)
-
Headache (∼65%)
-
Anorexia (∼60%)
-
Coryzal symptoms (∼60%)
-
Myalgia (∼53%) and
-
Sore throat (∼50%).
Fever is the paramount symptom and may reach 41°C although more usually it ranges between 38–40°C. The peak occurs within 24 hours of onset and lasts typically for three days (range 1–5 days).25–29 The cough is generally dry although in up to 40% of cases it may be productive. A productive cough together with chest tightness and substernal soreness is more common in patients with underlying chronic lung disease. Myalgia affects mainly the back and limbs. Gastrointestinal symptoms such as vomiting and diarrhoea are uncommon (<10%) in adults. Abdominal pain is rare.
Clinical findings include a toxic appearance in the initial stages, hot and moist skin, a flushed face, injected eyes and hyperaemic mucous membranes around the nose and pharynx. Tender cervical lymphadenopathy is found in a minority (∼10%) of cases. Wheezing or lung crackles are recognised findings (∼10%) more commonly noted in patients with coexisting chronic lung disease.
Although the overall clinical picture of uncomplicated influenza in any specific age group is similar for different influenza A subtypes, the frequency of certain symptoms may vary. For instance, during the “Asian” pandemic of 1957 (H2N2), headache and sore throat were frequent initial symptoms.30
In uncomplicated infection, the illness usually resolves in seven days although cough, malaise and lassitude may persist for weeks.
3.3 What complications are associated with influenza infection?
Influenza virus infection has been associated with worsening in the clinical condition of patients with a range of existing medical conditions, such as heart failure, diabetes, coronary heart disease, asthma and COPD.
In addition, specific complications associated with influenza infection regardless of coexisting medical conditions are recognised (table 3.1). Based on data from interpandemic influenza, certain persons are identified as being at high risk from influenza-related complications. Such patients are similar to the group currently recommended for influenza vaccination by the Department of Health. These include those of all ages with chronic respiratory disease including asthma, chronic heart disease, chronic renal disease, chronic liver disease, immunosuppression due to disease or treatment, or diabetes mellitus, and all those aged 65 years or older, or those in long stay residential care (see Appendix 2).
In the course of a pandemic, it may emerge that the patient group at high risk of complications differs from the group currently identified. In such circumstance, details of the “high risk” patient group will be altered according to relevant clinico-epidemiological data.
3.3.1 Influenza-related pneumonia
The incidence of pneumonia (defined as a combination of respiratory symptoms and signs supported by chest radiographic changes consistent with infection) complicating influenza infection varies widely, from 2% to 38%, and is dependent on viral and host factors.25–27 Pneumonia generally occurs more frequently and with greater severity in patients with pre-existing chronic cardiac and respiratory conditions.
Patients who develop pneumonia may present with symptoms and signs indistinguishable from pneumonia related to other viral and bacterial pathogens. In the context of an influenza pandemic, the presence of an ILI and new or worsening dyspnoea should prompt a careful examination for the presence of complicating pneumonia. Two main types of influenza-related pneumonia are recognised: primary viral pneumonia and secondary bacterial pneumonia.25–28
Primary viral pneumonia
Patients with primary viral pneumonia typically become breathless within the first 48 hours of onset of fever. An initially dry cough may become productive of blood-stained sputum. Cyanosis, tachypnoea, bilateral crepitations and wheeze on chest examination and leucocytosis are usual. The commonest chest radiographic abnormality is of bilateral interstitial infiltrates predominantly in the mid-zones, although focal consolidation is also well recognised. Rapid clinical deterioration with respiratory failure may ensue.31 The mortality in hospitalised patients is high (>40%) despite maximum supportive treatment on intensive care.25–28 In the majority of fatal cases, death occurs within seven days of hospital admission.
Secondary bacterial pneumonia
Secondary bacterial pneumonia is more common (up to four times) than primary viral pneumonia. Typically, symptoms and signs of pneumonia develop during the early convalescent period (4–5 days from onset of initial symptoms). In others, symptoms of pneumonia blend in with the initial symptoms of influenza. Chest radiography usually demonstrates a lobar pattern of consolidation. Mortality rate ranges from 7% to 24%,25–29,32 although some small studies report higher mortality rates.
The spectrum of pathogens implicated is similar to that observed in CAP and includes S pneumoniae, S aureus, H influenzae and Groups A, C and G beta-haemolytic streptococci.27,28,33–35 Different pathogens have predominated at different times. For instance, in the 1918 pandemic, H influenzae, beta-haemolytic streptococci and S pneumoniae were the predominant pathogens isolated. In 1968, S pneumoniae was the predominant pathogen (48%) followed by S aureus (26%) and non-typeable H influenzae (11%).34 Notably, S aureus was identified two and a half times more frequently during the 1968 pandemic compared to pneumonia occurring in the interpandemic period.34,36
Secondary staphylococcal pneumonia is associated with a higher incidence of lung abscess formation (14% v 2%) and carries a poorer prognosis compared to non-staphylococcal pneumonias (mortality 47% v 16%).25,29,32,37 During the 1957 pandemic, S aureus was the predominant bacterial pathogen isolated in fatal cases of influenza-related pneumonia (up to 69% of cases in some series).25
Mixed viral-bacterial pneumonia
Bacterial and viral pneumonia can occur concurrently. In these instances, the chest radiograph may demonstrate lobar consolidation superimposed on bilateral diffuse lung infiltrates. The mortality rate in mixed viral-bacterial pneumonia is high (>40%), as for primary viral pneumonia.25–28
3.3.2 Cardiovascular
Minor abnormalities on ECG such as ST segment deviation, T wave changes and rhythm disturbances have been described in uncomplicated influenza illness. They have been reported in up to 81% of patients hospitalised with influenza.25 Most do not have cardiac symptoms. Myocarditis and pericarditis are occasionally encountered in severe illness.38,39 Postmortem evidence of necrotising myocarditis has been reported in patients without clinically significant myocarditis in the antemortem period.
3.3.3 Myositis
In contrast with myalgia affecting the back and limbs, which is common on initial presentation, myositis generally develops after the subsidence of the acute upper respiratory tract symptoms. The gastrocnemius and soleus muscles are typically involved with pain and tenderness to palpation. Complete recovery usually occurs in three days. Elevation in serum creatine phophokinase is recognised.40,41 Rarely, this is associated with myoglobinuria and renal failure.42,43 Myositis is more commonly described in children than adults.
3.3.4 Central nervous system
Central nervous system (CNS) involvement in adults is uncommon. Most reports originate from Japan and occur in children.44,45 The main clinical syndrome is an encephalitis or encephalopathy manifesting in the form of decreased consciousness and seizures about three days (range 0–7 days) following the onset of upper respiratory tract symptoms. Focal neurological signs such as paresis, aphasia, choreoathetosis and cranial nerve palsies are less common. Cerebrospinal fluid (CSF) examination may be normal or reveal an elevation in protein or white cell count. Imaging by CT or MRI may be normal and if so, is indicative of a good prognosis and full recovery may be anticipated.46 Young age and abnormal CT/MRI findings are associated with a poor outcome including death or recovery with severe neurological sequelae (a fuller description is given in Section 4.2.6).
Acute necrotising encephalopathy is a rare fulminant syndrome associated with multifocal brain lesions that is described mainly in Japan.46 Other rare manifestations include transverse myelitis and Guillain-Barré syndrome.47,48
Reye’s syndrome, characterised by an encephalopathy, acute fatty liver, association with aspirin use and high mortality (∼40%), is a special situation that is almost exclusively seen in children and adolescents.46 Nevertheless, physicians managing adults are advised to be aware of this complication (a fuller description is given in Section 4.2.6.1.1).
3.3.5 Others
Other complications rarely encountered in adults with influenza A infection include toxic shock syndrome in conjunction with secondary S aureus infection49,50 and parotitis.51 Otitis media is more commonly encountered in children than adults.
3.4 Avian influenza A (H5N1) infection in humans
Human infections have been caused by different avian influenza A viruses in the past, including H9N2, H7N7, H7N3 and H7N2. In recent years, outbreaks of human infections by a novel strain of avian influenza A (H5N1) have raised particular concerns globally regarding the risk of a human pandemic.52 These concerns have been due in part to recognition that (a) avian influenza A (H5 N1) can pass directly from birds to humans and that (b) once in humans, avian influenza A (H5N1) causes severe disease with a high mortality.
The full spectrum of human illness associated with avian influenza A (H5N1) infection is not completely known. Descriptions of the clinical features of influenza A (H5N1) infection in humans are based largely on case series of hospitalised patients. Subclinical infections, mild illnesses and atypical presentations of influenza A (H5N1) infections in humans have been reported, but the frequency of such infections is difficult to determine.53–55
In hospitalised patients, an ILI similar to that associated with seasonal influenza A (H1N1 or H3N2) infection is recognised. Gastrointestinal symptoms are present in a relatively large proportion of both adult and paediatric cases, in contrast to the relatively low incidence of gastrointestinal symptoms in seasonal influenza. The majority of patients develop a severe primary viral pneumonia usually associated with lymphopenia, thrombocytopenia and deranged liver function tests. Renal failure and multi-organ failure may develop subsequently. Mortality is high. A more detailed description is given in Appendix 10.
Should influenza A (H5N1) acquire efficient human-to-human transmission capabilities, it may result in an influenza pandemic. In such an event, the clinical features of human H5N1 disease may alter.
4 CLINICAL FEATURES IN CHILDREN
Summary
-
The commonest presenting features of influenza during an epidemic are fever, cough and rhinorrhoea. In infants, fever with non-specific symptoms or diarrhoea and vomiting is common; in older children pharyngitis and headache are frequent.
-
The clinical features of influenza in children during a pandemic cannot be forecast.
-
Children with underlying respiratory or cardiac disease, immune compromise or who are non-ambulant are more likely to be severely affected.
-
The younger the child the more likely hospital admission will be needed.
-
The severe and life-threatening complications of influenza are likely to be
bacterial pneumonia
acute respiratory distress syndrome
encephalopathy or encephalitis presenting as seizures or altered mental status.
4.1 What are the clinical features of uncomplicated influenza in children?
The clinical features of influenza presenting in a pandemic cannot be predicted as they appear to be dependent on the strain of influenza and, in some respects, the host. A new strain of influenza A responsible for an epidemic or pandemic may result in a different spectrum of clinical features than previous strains.56,57
Common features during previous epidemics have been described and depend on the age of the child. The studies of clinical features are hospital based and are therefore likely to reflect more severe illness. These are nevertheless informative as one of the main issues in a pandemic is which patients require hospital admission. In young children presenting to primary care in a non-pandemic influenza season there are no specific clinical features that distinguish influenza from other winter viruses.58
Previously healthy infants and children
4.1.1 Neonates may present with non-specific signs of sepsis such as pallor, floppiness, (poor peripheral circulation, poor tone), lethargy, poor feeding, episodes of apnoea.59 Fever may be the only presenting feature. A North American study identified influenza as the most common reason for children aged 0–60 days being admitted to hospital during an epidemic with fever as the only clinical feature.60
4.1.2 Infants and very young children (under two years). Fever may be the only presenting feature in this age group too. They may also be irritable and toxic and are more likely than older children to present with gastrointestinal symptoms such as diarrhoea and vomiting. Febrile convulsions, particularly repeated convulsions, are positively associated with influenza A.61 Otitis media is also a common complication in children.62 Admission rates for under 2 year olds are 12 times higher than children aged 5–17 years.63
4.1.3 Older children. The presentation does not differ significantly from adults. Common features are sudden onset of high fever, chills (76–100%), cough, headache, sore throat, fatigue (51–75%), nasal stuffiness and conjunctivitis (26–50%). Fever tends to settle 2–4 days later though a dry cough and clear nasal discharge last for 1–2 weeks.59 A clinical prediction model from North America for influenza in children has shown that the triad of cough, headache and pharyngitis had a sensitivity of 80% and a specificity of 78% for a positive viral culture for influenza.64 The subjects, mean age 6 years, presented during an epidemic to a suburban emergency department with a febrile respiratory illness and one or more symptoms of influenza. A Finnish retrospective study of children referred to hospital from 1980–99 with influenza confirmed by antigen testing reported that the median age for those with influenza A was 2 years. The most common features were cough, fever and rhinorrhoea.62 These were also the commonest features reported in a Chinese study where the mean age of the subjects with influenza A was 4 years.65
Children with underlying medical conditions
4.1.4 Children with asthma and other chronic medical conditions66 (table 4.1) and those who are not ambulant67 experience substantial morbidity during influenza seasons with a disproportionate number requiring inpatient care and ventilatory support. Of the 22% of previously healthy children who were hospitalised with influenza in Texas during the winter of 1998–99, 75% were under 1 year old. Of the 60% hospitalised who had underlying conditions, only 27% were under 1 year.68
4.2 Complications and rarer clinical features (table 4.2)
4.2.1 Pneumonia
As in adults, influenza can present with either primary viral pneumonia or bacterial pneumonia most commonly caused by S pneumoniae or S aureus. There is much less published about pneumonia complicating influenza in children.
An outbreak of severe pneumococcal pneumonia in children occurred in Iowa in the winter of 1995–96. This was coincident with an epidemic of influenza (H1N1). Compared with controls, patients were 12 times more likely to have experienced a recent ILI. There were also more likely to have family members with the illness and to have positive serology in the convalescent period. Many of these patients required chest drainage.69
Another study in 2002 of 202 children with proven influenza reported that 78 who had chest radiographs had either radiographic evidence of viral pneumonia or normal radiographs. No child had lobar pneumonia reported.70
Evidence from recent outbreaks of avian influenza (H5N1) in Hong Kong and Vietnam suggests that while some children had mild disease,71 others appeared to have multi-organ disease including acute respiratory distress syndrome (ARDS).57 All children who developed progressive pneumonia with ARDS died. There were no reports of bacterial pneumonia.
There is no reason to believe that, apart from ARDS, pneumonia complicating influenza presents differently from CAP in children.72
The general clinical indicators for severity assessment of lower respiratory tract infection are summarised in the British Thoracic Society guidelines72 (Appendix 8). Failure to improve following 48 hours of antibiotics, or deterioration including a new, distinct spike of fever, should also be treated as severe and further complicating factors sought.
4.2.2 Croup
The clinical course of croup caused by influenza appears to be more severe than croup caused by the more common parainfluenza virus.73 It is more likely to be complicated by bacterial tracheitis.62
4.2.3 Otitis media
Influenza is a well recognised cause of otitis media.74 It is the commonest bacterial superinfection of influenza and is reported in approximately 25% patients aged <5 years.75
4.2.4 Bronchiolitis
Influenza ranks second only to respiratory syncytial virus as a cause of bronchiolitis.76 The clinical features are the same.77
4.2.5 Febrile convulsions
Children with influenza may present with febrile convulsions. In a community study in the Netherlands, recurrent febrile seizures were positively related to influenza A. It was recommended that children who have had a previous febrile convulsion should be immunised against influenza A.61
4.2.6 Encephalopathy and encephalitis
These complications are described in small case series.
4.2.6.1 Encephalopathy
This is defined as depressed or altered level of consciousness including lethargy and/or extreme irritability in younger children or significant change in personality or behaviour persisting beyond 24 hours, or confusion (older children). Encephalopathy usually presents as seizures within several days of the onset of fever.78 Seizures at this point are usually the first symptom of involvement of the CNS. Febrile convulsions, which are more likely to be repeated with influenza than with other causes of fever, generally occur with the onset of fever. Disturbances of behaviour and neurological deficit have been reported. A rapid and severe clinical course is usual with encephalopathy and is thought to be due to brain oedema mediated by cytokines rather than by direct invasion of the brain. Steroids are therefore considered. 202 children with encephalopathy were recognised in Japan between 1997 and 2001. Death occurred in 31%, residual neurological deficit in 26% and full recovery in 43%.79
4.2.6.1.1 Reye’s syndrome
This is a rare childhood acute encephalopathy associated with liver dysfunction. The cause is unknown but it typically follows viral illness and there is a clear association with aspirin therapy: thus an innate susceptibility coupled with aspirin taken for relief of viral symptoms. Influenza (particularly influenza B) is commonly implicated.80 There was a dramatic fall in incidence following warnings about aspirin use in children.81 It is possible that children on long term aspirin treatment for medical conditions may be at increased risk if they develop influenza infection.
Reye’s syndrome is characterised by protracted vomiting and encephalopathy in afebrile patients with minimal or absent jaundice, and hepatomegaly in 50% of patients. It comprises:
-
acute non-inflammatory encephalopathy with an altered level of consciousness
-
elevation of ammonia levels 24–48 hours after the onset of mental status changes (the most frequent laboratory abnormality)
-
hepatic dysfunction with a liver biopsy showing fatty metamorphosis or a more than threefold increase in alanine aminotransferase (ALT), aspartate aminotransferase (AST).
Neurological symptoms usually occur 24–48 hours after the onset of vomiting. Lethargy is usually the first neurological manifestation. Diarrhoea and hyperventilation may be the first signs in children younger than two years.
Other investigations. Head CT scanning may reveal cerebral oedema but results are usually normal. An electroencephalogram (EEG) may reveal slow wave activity in the early stages and flattened waves in advanced stages. Cerebrospinal fluid may or may not have increased opening pressure with white blood cells (WBCs) fewer than 9/ml3 (usually lymphocytes).
There is no specific treatment for Reye’s syndrome. Key aspects of management are correction of metabolic imbalance and reduction of intracranial pressure. Advice should be requested from a specialist in metabolic medicine. Many children have an underlying inborn error of metabolism. Mortality has fallen from 50% to less than 20% as a result of earlier diagnosis and more aggressive therapy.
4.2.6.1.2 Acute necrotising encephalopathy
Acute necrotising encephalopathy occurs mainly in Japan where it was first described in 1995. An estimated 100 deaths per annum are related to CNS complications of influenza in Japan.82 This suggests either a genetic predisposition for this complication or a variation in the strains of influenza circulating in Japan. Acute necrotising encephalopathy is characterised by high fever, convulsions and coma in children aged 1–5 years. The onset is 2–4 days after the respiratory symptoms and fewer than 10% of patients survive.83 There are no specific markers although some patients have raised liver transaminases. In many, the CSF is normal. Symmetrical multifocal brain lesions are seen and bilateral thalamic involvement is characteristic and may be demonstrated on MRI.83
4.2.6.2 Encephalitis
This is defined as encephalopathy plus two of the following: fever of 38°C or higher, seizures, focal neurological findings, WBC >5 cells/μl in CSF, electroencephalogram findings consistent with encephalitis, abnormal neuro-imaging.84
4.2.6.3 Differential diagnoses
These must be considered when a child presents with altered level of consciousness or irritability. There is good evidence of an increased risk of meningococcal disease following influenza infection.85 During a pandemic, the focus will be on diagnosing influenza-related illness. Other neurological conditions or drug toxicity, for example, may be missed.
4.2.7 Myositis
A literature review of 316 cases of myositis86 suggested that this was a complication mainly of schoolchildren. The calf muscles are predominantly affected. Rhabdomyolysis and renal failure are rare.
4.2.8 Myocarditis and pericarditis
These are also rare complications but have been described in children with underlying medical conditions.62
PART 1 Clinical management in primary care
5 GENERAL MANAGEMENT AND INVESTIGATIONS IN PRIMARY CARE
5.1 Triage
With widespread concern during a pandemic, a significantly increased demand for advice and consultation should be anticipated. There are likely to be significantly higher consultation rates for all types of respiratory tract infections including those which are normally managed well at home using over the counter remedies (for example, febrile colds, sore throat with temperatures). Consequently, demand management in both the practice and the Primary Care Trust (PCT) will be crucial to avoid the service’s capacity to triage care being overwhelmed.
Guidance on demand management and health service delivery is given in the Primary Care Operational Plan (see Section 1.4).87
Management decisions of patients with influenza should be based primarily on:
-
an assessment of illness severity
-
identification of whether the individual is in an “at risk” group
-
current advice from Department of Health/local public health officials based on the epidemiology of the pandemic.
Patients who are not considered to be at high risk and who have no features suggesting severe disease or complications may not need to be seen in face-to-face consultations by a primary care clinician.
5.2 General advice and symptomatic treatment in adults
All patients presenting in general practice with symptoms suggestive of influenza (except perhaps those in whom urgent admission is required) should be given both general advice and advice on symptomatic treatment. It is important that clinicians identify and address individual concerns and expectations, provide information about the illness, and provide information about what patients can do to help themselves and when they should seek further help. Some useful facts that can be provided to the patient are included in Box 5.1.
Box 5.1 Information about influenza to provide to patients
-
Influenza is caused by a number different types of “influenza” viruses.
-
The incubation period is typically 1–4 days and infected adults are usually contagious from the day of illness onset to five days after. Children are typically contagious for seven days, although sometimes for longer.
-
Fever usually declines after 2–3 days and normally disappears by the sixth day.
-
Cough, weakness and fatigue can persist for 1–2 weeks and up to six weeks.
-
Antibiotics do not benefit most people with influenza but are sometimes needed to treat secondary infections.
Important note: this information may be modified once a pandemic occurs.
There is little scientific evidence for most symptomatic and self-help treatment, but experience suggests that some of the following may help, and are unlikely to cause harm:
-
treatment of fever, myalgias and headache with paracetamol or ibuprofen
-
rest
-
drinking plenty of fluids
-
avoiding smoking
-
consider: short course of topical decongestants, throat lozenges, saline nose drops.
5.3 General management in children
Many infants and children will have coughs and mild fevers which may be due to other infections such as respiratory syncytial virus, especially over the winter months. These children should be managed in the usual way at home by parents with antipyretics and fluids.
Note: aspirin should not be used in children.
5.3.1 Children with high fever (>38.5°C) and cough or influenza-like symptoms
Management of these children is determined by disease severity (see Appendix 5). The principles of symptomatic management are similar to those for adults.
Recommendations
-
Children under one year of age year and those at high risk of complications (see Appendix 2) should be seen and assessed by a general practioner (GP) or at the A&E department.
-
Children age over 1 but under 7 years of age may be seen by a nurse or a GP and those aged 7 years and above may be seen by a member of the community health team (for example, community pharmacist).
-
All children (and parents) should be given advice on antipyretics and fluids.
-
Aspirin is contraindicated in children (aged under 16 years).
5.4 When should patients re-consult?
Examples of what should prompt a patient to re-consult are given in Box 5.2. Patients who are started on antiviral agents (see Section 7 for indications for antiviral use) would be expected to begin to improve within 48 hours of starting treatment. Failure to improve two days after starting an antiviral agent is an indication to re-consult. At the time of re-consultation, an alternative diagnosis should be considered as well as the occurrence of any influenza-related complications.
Box 5.2 Examples of what should prompt patients to re-consult
-
Shortness of breath at rest or while doing very little
-
Painful or difficult breathing
-
Coughing up bloody sputum
-
Drowsiness, disorientation or confusion
-
Fever for 4–5 days and not starting to get better (or getting worse)
-
Started to feel better then developing high fever and feeling unwell again
-
If taking antiviral drugs (for example, oseltamivir), symptoms should start to improve within two days. Lack of any improvement after two days from starting antiviral drugs is an indication to re-consult.
Important note: this information may be modified once a pandemic occurs.
Recommendations
-
Any rapid deterioration following first consultation should prompt a patient to re-consult.
-
Failure to improve two days after starting an antiviral agent is an indication to re-consult.
-
If the first consultation did not involve contact with a physician, re-consultation should preferably involve a physician, usually a GP.
5.5 What general investigations should be done in the community?
Recommendation
-
General investigations, including a chest x ray, are not necessary for the majority of patients managed in the community.
5.6 What microbiological investigations should be undertaken for patients in the community?
The aim of microbiological investigations early in a pandemic (UK alert levels 1, 2 and 3) will be to confirm that influenza A is circulating in the local community. Once a pandemic is established (UK alert level 4), microbiological investigations are not recommended routinely or likely to be available readily. Routine testing for bacterial pathogens is not recommended at any stage.
Recommendations
-
Where possible, early in a pandemic (UK alert levels 1, 2 and 3), nose and throat swabs, or nasopharyngeal swabs (in children), in virus transport medium should be submitted to the local laboratory.
-
Once a pandemic is established (UK alert level 4), microbiological investigations are not recommended.
6 CRITERIA FOR HOSPITAL REFERRAL
6.1 Which adults require hospital referral?
Adults with uncomplicated influenza infection usually do not require hospital referral. Patients who might require hospital admission fall into two main groups; those with worsening of a pre-existing medical condition and those with an influenza-related complication.
6.1.1 Worsening of pre-existing medical condition
Patients who experience a worsening or clinical deterioration of pre-existing medical problems due to influenza infection should be managed according to recommended best practice for the medical condition in question. For instance, a patient with an acute exacerbation of chronic obstructive pulmonary disease (COPD) triggered by influenza infection should be managed according to current NICE Guidelines for COPD.88
Those with worsening of a pre-existing condition are likely to be in a group at “high risk” of influenza-related respiratory complications and consequently at risk of hospitalisation or death (Appendix 2). This group should be promptly reassessed if the illness is getting worse and considered for hospital referral.
6.1.2 Influenza-related pneumonia
Pneumonia is the commonest influenza-related complication requiring hospital admission. Patients complaining of new or worsening dyspnoea should be carefully assessed for signs of pneumonia. If pneumonia is diagnosed, disease severity assessment is recommended and hospital referral made accordingly.
There is no validated severity assessment tool developed specifically for influenza-related pneumonia. The CRB-65 score (table 6.1) is a well validated severity assessment tool developed for patients with community acquired pneumonia (CAP)89,90 and recommended in the British Thoracic Society (BTS) CAP Guidelines 2004 for use in the community setting.72 It is offered as an example of an assessment tool for influenza-related pneumonia.
The use of any severity assessment tool does not replace clinical judgement. A patient’s social circumstances should also always be taken into account.
In view of the rapid and fulminant course of primary viral pneumonia, patients with pneumonia who have bilateral chest signs (crackles) should be considered for hospital referral.
6.1.3 Other complications
Other influenza-related complications are uncommon. There are no specific recommendations relating to criteria for hospital admission or disease severity assessment in these cases.
Recommendations
-
Patients with clinically defined uncomplicated influenza infection would be expected to make a full recovery. They require good symptomatic management, access to antiviral treatment, information about the natural history, and advice as to when to re-consult.
-
Patients with new or worsening symptoms—particularly shortness or breath or recrudescent fever not responding to treatment—should be examined to assess the presence and severity of influenza-related pneumonia.
-
Patients with worsening of pre-existing comorbid medical conditions should be managed according to best practice for that condition with reference to published disease-specific guidelines, if available.
-
In patients with influenza-related pneumonia clinically, hospital referral and assessment should be considered for patients with a CRB-65 score of 1 or 2 (particularly score 2) and urgent admission for those with CRB-65 score of 3 or more.
-
Patients with bilateral chest signs of pneumonia should be referred to hospital for further assessment regardless of CRB-65 score.
-
The CRB-65 score does not replace clinical judgment.
6.2 Which children require hospital referral? (see Appendix 5)
Recommendation
-
Children who are severely ill should be referred for assessment for admission. Indicators of severe disease are:
cyanosis
severe dehydration
altered conscious level
complicated or prolonged seizures
signs of sepsis such as extreme pallor, hypotension, a floppy infant
signs of respiratory distress such as markedly raised respiratory rate, grunting, intercostal recession or breathlessness with chest signs (a useful severity assessment tool for respiratory distress taken from the BTS pneumonia guidelines is given in Appendix 8).
7 ANTIVIRAL USE IN PRIMARY CARE
7.1 Introduction
The guidance given in this Section summarises the key recommendations relevant to primary care. Full details relating to the principles and practice of antiviral use in adults and children are provided in Sections 13 and 19 respectively. Guidance relating to the delivery of antivirals is laid out in detail in the UK Operational Framework for stockpiling, distributing and using of antiviral drugs in the event of pandemic influenza5 and in the Primary Care Operational Plan.
7.2 What drugs should be used for antiviral treatment during a pandemic?
Recommendations (see Appendix 9)
-
The antiviral treatment of choice is oseltamivir (Tamiflu®). This is given as a five-day course of oral tablets; 75 mg twice daily for adults. Liquid suspension is available for children from the age of 1 year upwards (see table 7.1).
7.3 What are the anticipated benefits of antiviral treatment?
From clinical trial data accrued to date and based on seasonal, interpandemic influenza, the anticipated positive effect of antivirals in a pandemic will be:
-
reduction of illness duration by 24 hours, and therefore more rapid mobilisation of affected individuals including essential workers
-
a possible reduction in hospitalisation of infected individuals
-
a reduction of subsequent antibiotic use by infected individuals.
The evidence accrued to date does not suggest there will be a reduction of overall mortality, nor does it rule it out.
7.4 Who should receive antiviral drugs?
Recommendations
-
Ideally, antiviral treatment should be offered to every patient who is over one year of age who
has an acute influenza-like illness
fever (⩾38°C in adults, or ⩾38.5°C in children) and
presents within 48 hours of the onset of symptoms.
-
Exceptions:
Patients who are unable to mount an adequate febrile response—for example, the immunocompromised or very elderly—may still be eligible for antiviral treatment despite the lack of documented fever.
Immunosuppressed patients, including those on long term corticosteroid therapy, may suffer more prolonged viraemia, and could possibly benefit from antiviral therapy commenced later than 48 hours after the onset of influenza-like illness (ILI).
Patients who are severely ill, but who have not been hospitalised due to non-clinical reasons, may benefit from antiviral therapy commenced later than 48 hours after the onset of ILI. There is no strong evidence to support antiviral use in these exceptional situations.
7.5 What are the adverse effects of oseltamivir?
The commonest adverse effect of oseltamivir is nausea in about 10% of patients. This can be managed with mild anti-emetic medication. Other side effects are listed in Appendix 9.
7.6 Delivery of antivirals in primary care
National distribution arrangements are laid out in the UK Operational Framework for stockpiling, distributing and using antiviral drugs in the event of pandemic influenza5 and the Primary Care Operational Plan. The drug will be made available through these arrangements to pharmacies, PCTs and/or GP surgeries.
Recommendations
-
PCTs are encouraged to plan for the delivery of antivirals to the large numbers of previously healthy persons with an ILI via community health professionals, including community pharmacists.
-
GPs should focus their efforts on assessment and management of those persons at high risk of complications (see Appendix 2) and patients developing complications.
8 ANTIBIOTIC USE IN PRIMARY CARE
8.1 Adults with influenza not complicated by pneumonia
The use of antibiotics in adults with influenza not complicated by pneumonia is determined by (a) the presence of any comorbid illnesses and (b) the timing of first consultation with respect to the onset of symptoms.
8.1.1 Patients without severe pre-existing illnesses
Features of an acute bronchitis, with cough, retrosternal discomfort, wheeze and sputum production are an integral part of the influenzal illness. In previously well individuals who do not have pneumonia or new focal chest signs, antibiotics are not indicated. If the patient is seen later in the course of the illness and the illness is worsening, for instance with recrudescent fever or increasing breathlessness, a worsening bacterial bronchitis or developing pneumonia is possible and the use of antibiotics should be considered.
In selected patients, a delayed antibiotic prescription may be offered at first consultation. The antibiotic prescription should come with clear instructions that the antibiotics should be used if the illness is not starting to settle after two days or if there is worsening of symptoms. The potential advantage of this approach of delayed antibiotic prescription is to minimise rates of reconsultation.91 There are no robust data regarding the effect of such an approach on the incidence of influenza-related complications.
8.1.2 Patients with COPD and/or other severe pre-existing illnesses
Those at high risk of influenza-related complications because of (a) COPD and/or b) other severe comorbid diseases should be strongly considered for antibiotics at first consultation.
If, having started antibiotics, patients do not begin to improve over the next 48 hours of antibiotic treatment (or if they get worse) they should be advised to re-contact their GP for assessment of pneumonia and its severity (see Sections 3 and 6).
Antibiotics should cover the likely bacterial pathogens including Streptococcus pneumoniae (S pneumoniae), Haemophilus influenzae (H influenzae), Moraxella catarrhalis (M catarrhalis) and Staphylococcus aureus (S aureus).
The preferred first choice of antibiotic for non-pneumonic bronchial infections, including those patients with COPD, should include an effective oral β-lactamase stable agent such as a tetracycline (for example, doxycycline) or co-amoxiclav. A macrolide (for example, erythromycin or clarithromycin) is an alternative for those intolerant of the preferred first choices, while remembering the possibility of antimicrobial resistance. Clarithromycin has better activity against H influenzae than azithromycin.
Further details regarding the principles of antibiotic use including antibiotic resistance patterns are given in Section 14.
Recommendations (see table 8.2)
-
Patients without severe pre-existing illnesses and who have uncomplicated influenza, or simple bronchitis, do not routinely require antibiotics.
-
Patients without severe pre-existing illnesses who are seen later in the course of illness and who have developed significant worsening of symptoms (particularly recrudescent fever or increasing breathlessness) should be considered for antibiotics.
-
Patients with COPD and/or other severe pre-existing illnesses, and who are therefore at high risk of influenza-related complications, should be strongly considered for antibiotics at first consultation.
-
Most patients can be adequately treated with a week’s course of oral antibiotics.
-
The preferred choice of antibiotic needs also to cover infection with S aureus—for example either doxycycline or co-amoxiclav (see table 8.1).
-
A macrolide (for example, erythromycin or clarithromycin) is an alternative choice in certain circumstances.
8.2 Adults with influenza-related pneumonia
The principles of antibiotic selection for patients with influenza-related pneumonia who can be managed in the community are similar to those for the management of sporadic CAP in general except that adequate cover for S aureus, in addition to cover for S pneumoniae, should be included in any empirical regimen.
For this reason a tetracycline, such as doxycycline or oral co-amoxiclav is the preferred regimen (table 8.2).
A macrolide (for example, erythromycin or clarithromycin) is an alternative for those intolerant of the preferred first choices.
Recommendations (see table 8.2)
-
A tetracycline (for example, doxycycline) or co-amoxiclav is preferred.
-
A macrolide (for example, erythromycin or clarithromycin) is offered as an alternative choice for those intolerant of penicillins.
-
Those with features of severe infection (that is, bilateral chest signs or CRB-65 score of 3 or more) should be urgently referred to hospital (see Section 6).
-
For those referred to hospital, GPs may consider administering antibiotics immediately where the illness is considered life threatening or where delays (more than two hours) in admission are likely.
8.3 Children with influenza
Secondary bacterial infections particularly pneumonia and otitis media are common in children with influenza. S pneumoniae, S aureus and H influenzae are the most common pathogens encountered during influenza outbreaks.
Recommendations
Children in any one of the following groups should be treated with an antibiotic that will provide cover against S pneumoniae, S aureus and H influenzae:
-
those at risk of complications of influenza (see Appendix 2)
-
those with one or more of the following adverse features:
breathing difficulties
severe earache
vomiting for more than 24 hours
drowsiness, or
-
those with disease severe enough to merit hospital admission during an influenza pandemic.
For children under 12 years co-amoxiclav is the drug of choice.
Clarithromycin or cefuroxime should be used in children allergic to penicillin. For children over 12 years doxycycline is an alternative (see Appendix 7 for paediatric antibiotic doses).
PART 2 Clinical management of adults referred to hospital
9 SEVERITY ASSESSMENT OF ADULTS REFERRED TO HOSPITAL
9.1 What severity assessment strategy is recommended for patients referred to hospital with influenza-related pneumonia?
There is no validated severity assessment tool developed specifically for influenza-related pneumonia. The CURB-65 severity assessment tool as described in the British Thoracic Society Community Acquired Pneumonia (BTS CAP) Guidelines 2004 is recommended for the stratification of hospitalised patients with influenza-related pneumonia into disease severity groups72 (table 9.1). In addition, the presence of diffuse bilateral lung infiltrates on chest radiography consistent with primary viral pneumonia is an adverse prognostic feature. Such patients should be treated as for severe pneumonia. In all instances, clinical judgement is essential when assessing disease severity.
Recommendations
-
Patients with bilateral lung infiltrates on chest radiography consistent with primary viral pneumonia should be managed as having severe pneumonia regardless of CURB-65 score.
-
In hospital, patients with influenza-related pneumonia who have a CURB-65 score of 3 or more are at high risk of death and should be managed as having severe pneumonia.
-
Patients who have a CURB-65 score of 2 are at increased risk of death. They should be considered for short stay inpatient treatment or hospital supervised outpatient treatment. This decision is a matter of clinical judgement.
-
Patients who have a CURB-65 score of 0 or 1 are at low risk of death. They can be treated as having non-severe pneumonia and may be suitable for home treatment.
9.2 When should transfer to a high dependency unit or intensive care unit be considered?
The indications for transfer to high dependency unit (HDU) or intensive care unit (ICU) are no different in patients with influenza infection compared with other patients. Most patients who might require HDU/ICU care will have influenza-related pneumonia or a severe exacerbation of underlying comorbid illness, for example, exacerbation of chronic obstructive pulmonary disease (COPD). In a pandemic situation when HDU/ICU beds may not be readily available, prioritisation of patients on an individual basis matched against available resources will be expected.
Recommendations
-
Patients with primary viral pneumonia or a CURB-65 score of 4 or 5 should be considered for HDU/ICU transfer.
-
General indications for HDU/ICU transfer include:
persisting hypoxia with PaO2 <8 Kpa despite maximal oxygen administration
progressive hypercapnia
severe acidosis (pH<7.26)
septic shock.
-
Patients with influenza admitted to an ICU should be managed by specialists with appropriate training in intensive care, respiratory medicine and/or infectious diseases.
10 GENERAL INVESTIGATIONS FOR ADULTS IN HOSPITAL
10.1 What general investigations should be done on all adults referred to hospital?
10.1.1 Radiology
In acute uncomplicated influenza the chest x ray is usually normal. When primary viral pneumonia occurs as a complication, particularly in elderly adults, the chest x ray often shows multiple infiltrates or consolidation. Cavitations or pleural changes suggest bacterial superinfection. In combined viral-bacterial pneumonia, the clinical features typically appear later than primary viral pneumonia and the chest x ray often shows cavitation or pleural effusions. Secondary bacterial pneumonia usually occurs after apparent improvement from the viral infection; the chest x ray may show consolidation.
Recommendations
-
A chest x ray should be obtained during assessment of a suspected case of influenza seen in the hospital setting (accident and emergency department or acute admissions ward).
-
In those patients who are subsequently followed up in a hospital outpatient clinic or by a general practitioner (GP) a repeat chest x ray should be obtained at around six weeks if respiratory symptoms or signs persist or where there is a higher risk of underlying malignancy (especially smokers and those over 50 years of age).
-
Further investigations including a CT thoracic scan and bronchoscopy should be considered if the chest x ray remains abnormal at follow up.72
10.1.2 Blood tests
In those patients with illness severe enough to present to secondary care then the following tests may be useful:
-
Full blood count: a leucocytosis with left shift may occur in those with primary viral pneumonia, mixed viral-bacterial pneumonia or secondary bacterial pneumonia. (Lymphopenia has been noted in human cases of severe avian H5N1 influenza.)
-
Urea and electrolytes may reveal evidence of hypo- or hypernatraemia or renal impairment.
-
Liver function tests are usually normal.
-
Creatine kinase may be elevated in those with severe myalgia.
C-reactive protein is unlikely to be helpful except where superimposed bacterial infection is suspected.72 However, the diagnostic value of C-reactive protein (CRP) in lower respiratory tract infections remains controversial.92
Recommendations
-
The following blood tests should be obtained in patients admitted to hospital:
Full blood count
Urea, creatinine and electrolytes
Liver function tests
Creatine kinase (if myositis is suspected)
-
In patients with suspected secondary bacterial infection, the CRP level may aid diagnosis.
10.1.3 Other tests
Recommendations
-
Pulse oximetry should be carried out in all patients presenting to secondary care.
-
If the oxygen saturation is below 92% then arterial blood gases should be obtained.
-
An electrocardiogram (ECG) should be obtained in all patients with cardiac or respiratory complications.
10.1.4 Lung function tests
In acute uncomplicated influenza larger airway function remains normal. However, there is often an increase in bronchial reactivity which may persist for many weeks after resolution of the infection.93 Lung function tests are unnecessary in most patients.
11 MICROBIOLOGICAL INVESTIGATIONS FOR ADULTS IN HOSPITAL
11.1 Introduction
The guidelines provided below are based on the assumption that when cases are first occurring in the UK as part of a global pandemic, it will be possible to perform full microbiological investigations in all new cases of influenza-like illness (ILI) and influenza-related pneumonia. As case numbers rise, possibly to pandemic levels, full or indeed any microbiological investigation will become increasingly difficult. Thus, data on the relative frequency of different bacterial causes of influenza-related pneumonia and their antimicrobial susceptibilities among investigated cases gathered earlier in the pandemic should be available to guide and refine empirical antimicrobial therapy choices for cases occurring later in the pandemic.
The most likely pathogens implicated in influenza-related pneumonia are Streptococcus pneumoniae (S pneumoniae), Staphylococcus aureus (S aureus), Haemophilus influenzae (H influenzae)and to a lesser extent beta-haemolytic streptococci (see Section 3.3). In the early phases (UK alert levels 1, 2 and 3; see Appendix 1) of a pandemic microbiological diagnostic approaches should focus on confirming influenza as the primary illness, defining bacterial causes of influenza-related pneumonia and optimising both specific (for individual patients) and general (for populations) antimicrobial treatment recommendations. In later pandemic phases (UK alert level 4) with the much higher caseloads anticipated, microbiological investigation should be focused on patients with severe influenza-related pneumonia unresponsive to empirical antimicrobial therapy. Actual and practical local level transition to less intense microbiological investigation may occur at UK alert level 3 in some regions as the number of local cases is likely to vary between regions.
11.2 Early in a pandemic (UK alert levels 1, 2 and 3), what microbiological investigations should be undertaken for hospitalised patients?
It will be necessary to perform full microbiological investigations on all hospitalised cases, including patients with severe and non-severe influenza-related pneumonia, in order to:
-
confirm influenza as the primary infection,
-
optimise treatment options for the patients investigated and
-
define the most common bacterial causes of influenza-related pneumonia and their antimicrobial susceptibility patterns.
The latter data will help to inform empirical antimicrobial therapy of subsequent cases for which microbiological investigation may not be undertaken fully, or at all.
11.2.1 Virology
In influenza, rapid virological tests, viral culture and polymerase chain reaction (PCR) of respiratory samples will yield positive results 1–7 days after illness onset. However, if presentation is more than seven days after the onset of ILI then such sampling and testing is unhelpful. Instead, serum samples for serological testing for evidence of recent influenza infection is recommended.
Specific detailed microbiological guidance for taking and handling specimens from individuals at risk of avian influenza prepared by Professor Maria Zambon of the Health Protection Agency (HPA) Centre for Infections is available at http://www.hpa.org.uk/infections/topics_az/influenza/avian/microbiological_guidance.htm.
11.2.2 Bacteriology
Bacteriological investigations are only recommended in patients with influenza-related pneumonia. Legionella pneumophila infection is not normally associated with influenza-related pneumonia. Despite this, Legionella urine antigen tests should be performed on severe CAP cases in the early stages of an outbreak/incident in order to confirm Legionella infection is not the reason for a local increase in pneumonia admissions. These recommendations are modified from those contained in the BTS CAP Guidelines 2001, Thorax 2001:56(Suppl IV); see Sections 5.7, 5.8 and 5.9 (pages iv23–28) and the 2004 Update (see page 4–page 5), both available at http://www.brit-thoracic.org.uk/iqs/bts_guidelines_pneumonia_html.
Sputum investigative efforts must be focused on quality samples (that is, those from patients who are able to expectorate purulent samples, and have not received prior antibiotic treatment) and not dissipated on large numbers of poor quality samples. It is important to acknowledge that the criteria for quality samples may only be met for a minority of admissions. Laboratories should offer a reliable sputum Gram stain for appropriate samples, as on occasions this can give immediate indication of likely pathogens. The most likely influenza-related pneumonia pathogens are S pneumoniae, S aureus and H influenzae, all of which may present a characteristic appearance on Gram stain of purulent sputum. Laboratories performing sputum Gram stains should adhere to strict and locally agreed criteria for interpretation and reporting of results.
Recommendations (early in a pandemic: UK alert levels 1, 2 and 3)
A. Virology—all patients
-
Nose and throat swabs in virus transport medium should be collected from all patients and submitted to the local laboratory. The relevant laboratory should be notified of the suspected diagnosis and there should be close liaison over sample collection, handling and transport.
-
Rapid testing by direct immunofluorescence or rapid enzyme immunoassay test, virus culture and/or PCR should be undertaken according to local availability and/or referred to an appropriate laboratory
-
During UK alert level 1, when the UK is on high alert for the first cases of pandemic influenza, suspected cases are likely to be investigated by local Health Protection Teams from the HPA and its partner organisations in the devolved administrations.
-
During UK alert levels 1 and 2, clinicians dealing with suspected cases of pandemic influenza should ensure that the local Health Protection Team is informed and involved from the outset.
-
The HPA and its partner organisations in the devolved administrations have established a network of more than 20 laboratories across the UK which have been proficiency tested in molecular diagnosis of influenza A/H5N1. Access to this service should be via local Health Protection Teams.
-
If presentation is more than seven days after onset of illness, an “acute” serum (5–10 ml clotted blood) should be collected and a “convalescent” sample (5–10 ml clotted blood) obtained after an interval of not less than seven days. The two sera should be examined serologically for evidence of recent influenza infection.
B. Bacteriology—patients with influenza-related pneumonia
The following bacteriological tests should be performed:
-
Blood culture (preferably before antibiotic treatment is commenced)
-
Pneumococcal urine antigen (20 ml urine sample)
-
Legionella urine antigen (20 ml urine sample)
-
Sputum Gram stain, culture and antimicrobial susceptibility tests on samples obtained from patients who:
are able to expectorate purulent samples, and
have not received prior antibiotic treatment.
Sputum samples should be transported rapidly to the laboratory.
-
Paired serological examination for influenza/other agents. Acute serum should be collected and a “convalescent” sample obtained after an interval not less than seven days (both 5–10 ml clotted blood) and the two sera stored for subsequent testing.
11.3 Once a pandemic is established (UK alert level 4), what microbiological investigations should be undertaken for hospitalised patients?
Once a pandemic is established, virological investigations are not recommended routinely and in a pandemic situation may not be readily available. The diagnosis of influenza will be based on clinical findings. If influenza-related pneumonia is present, the degree of microbiological investigation will be directed by disease severity and the presence of comorbidities.
In influenza-related pneumonia, examination of sputum should be considered for patients who do not respond to empirical antibiotic therapy. This will be particularly relevant if S aureus is identified as a common influenza-related pneumonia pathogen during the early phase of the pandemic as, in contrast to S pneumoniae and H influenzae, antimicrobial susceptibilities of this organism are less predictable and empirical choices more speculative.
Recommendations (once a pandemic is established: UK alert level 4)
A. Virology—not routinely recommended
B. Bacteriology—patients with influenza-related pneumonia
(I) Non-severe pneumonia (CURB-65 Score 0, 1 or 2)
Sputum samples should be sent for Gram stain culture and antimicrobial susceptibility tests in patients who do not respond to empirical antibiotic therapy.
(II) Severe pneumonia (CURB-65 Score 3, 4 or 5)
Specific investigations should include:
-
Blood culture, preferably before antibiotic treatment is commenced
-
Pneumococcal urine antigen (20 ml urine)
-
Sputum Gram stain, culture and antimicrobial susceptibility tests on samples obtained from patients who:
are able to expectorate purulent samples, and
have not received prior antibiotic treatment.
Sputum specimens should be transported rapidly to the laboratory.
-
Paired serological examination for influenza/other agents. “Acute” serum should be collected and a “convalescent” sample obtained after an interval not less than seven days (both 5–10 ml clotted blood) and the two sera stored for subsequent testing.
-
Tracheal or endotracheal aspirate samples, if available, should be sent for Gram stain, culture and antimicrobial susceptibility testing.
12 GENERAL MANAGEMENT OF ADULTS ADMITTED TO HOSPITAL
12.1 Introduction
Initial management will depend on the assessment of the reason for admission, the presence of complications, and the impact of the influenza on any pre-existing disease, or psychosocial factors. For instance, some elderly patients may require admission for social reasons.
In broad terms, the most likely clinical reasons for admission will be (in order of frequency):
Lower respiratory tract complications
-
Non-pneumonic bacterial exacerbation of chronic lung disease such as COPD (possibly with a mixed viral infection)
-
Secondary bacterial pneumonia
-
Mixed bacterial and viral pneumonia
-
Primary viral pneumonia
Cardiac complications
-
Exacerbation of pre-existing cardiac disease with cardiac failure and/or arrhythmia
-
Primary myocarditis
Other complications
-
Exacerbation of other pre-existing disease, such as diabetes mellitus
-
Neurological complications
-
Rhabdomyolysis
-
Severe sinusitis
The initial management is likely to most usually involve that of respiratory and cardiac complications, especially pneumonia, and these are discussed below. Management of other less common primary influenzal complications (such as rhabdomyolysis, encephalopathy) is not covered.
12.2 What initial management strategy should be offered to patients with respiratory and cardiac complications?
All influenza patients admitted to hospital with abnormal cardiorespiratory symptoms and signs, including influenza-related pneumonia should have a chest radiograph, and electrocardiogram and should have oxygenation assessed by pulse oximetry, preferably while breathing air (see Section 10). Those with SaO2 <92% should have arterial blood gas measurements, as should all patients with features of severe illness. Knowledge of the inspired oxygen concentration is essential to the interpretation of blood gas measurements and should be clearly recorded with the blood gas result.
Continuous oxygen therapy is indicated for those patients with PaO2 <8 Kpa, hypotension with systolic blood pressure <100 mmHg, metabolic acidosis with bicarbonate <18 mmol/l or respiratory distress with respiratory rate >30/min.94 The aim of oxygen therapy should be to maintain PaO2 at >8 Kpa or SaO2 >92%. Unless complicated by severe COPD with ventilatory failure, high concentrations of oxygen of 35% or greater are indicated and can be safely used.
High concentration oxygen therapy given to patients with pre-existing COPD who may have CO2 retention can reduce hypoxic drive and increase ventilation-perfusion mismatching. In such patients initial treatment with low oxygen concentrations (24–28%) should be progressively increased on the basis of repeated arterial blood gas measurements, the aim being to keep SaO2 >90% without causing a fall in arterial pH below 7.35, in line with the management strategy recommended in the NICE COPD Guidelines.95 Non-invasive ventilation (NIV) may be of value in patients with COPD who are in acute hypercapnic respiratory failure.72,96
12.2.1 Non-invasive ventilation
The use of NIV in patients with respiratory failure due to severe pneumonia but without coexisting COPD has not been shown to influence mortality.72,96 Nevertheless, during an influenza pandemic when Critical Care Level 3 beds97 are in high demand, NIV may be of value as a bridge to invasive ventilation in specific circumstances. In all instances, the risks of infection due to the dissemination of respiratory droplets related to the use of NIV must be taken into account when deciding on management strategies. Respiratory and/or critical care units experienced in the use of NIV are best placed to ensure the appropriate infection control measures are adopted and observed at all times, including the use of Personal Protection Equipment (see UK Infection Control Guidance for Pandemic Influenza).3
All patients should be assessed for volume depletion and may require IV fluids. The potential for influenza to cause cardiac decompensation, either through exacerbation of pre-existing cardiac disease or from a primary myocarditis, should be borne in mind, with any complicating heart failure and arrhythmias being managed in the usual way.
Physiotherapy may be of benefit in selected patients with excess bronchial secretions, particularly those with concurrent COPD. In cases of severe illness requiring prolonged hospital admission increased nutritional support, whether enteral, parenteral or via naso-gastric feeding, should be arranged.
Recommendations
-
Hypoxic patients should receive appropriate oxygen therapy with monitoring of oxygen saturations and inspired oxygen concentration with the aim to maintain PaO2 >8 Kpa and SaO2 >92%. High concentrations of oxygen can safely be given in uncomplicated pneumonia.
-
Oxygen therapy in patients with pre-existing COPD complicated by ventilatory failure should be guided by repeated arterial blood gas measurements. NIV may be helpful.
-
In patients without pre-existing COPD who develop respiratory failure, NIV may be of value as a bridge to invasive ventilation in specific circumstances when Critical Care Level 3 beds are in high demand. Respiratory and/or critical care units experienced in the use of NIV are best placed to ensure the appropriate infection control measures are adopted at all times.
-
Patients should be assessed for cardiac complications and also volume depletion and their need for additional intravenous fluids.
-
Nutritional support should be given in severe or prolonged illness.
12.3 What monitoring should be conducted during a hospital stay?
Pulse, blood pressure, respiratory rate, temperature, oxygen saturation (with a recording of the inspired oxygen concentration at the same time) and mental status should be measured initially at least twice daily. This is most conveniently performed using an Early Warning Score (EWS) chart, which all ward staff should be familiar with. Those with severe illness, requiring continuous oxygen or cardiovascular support, should be monitored more frequently.
Failure to improve clinically within 48 hours should result in a full clinical reassessment and failure to improve over four days is an indication to repeat the chest radiograph.
Recommendations
-
Temperature, respiratory rate, pulse, blood pressure, mental status, oxygen saturation and inspired oxygen concentration should be monitored and recorded initially at least twice daily and more frequently in those with severe illness or requiring regular oxygen therapy.
-
An EWS system is a convenient way to perform this.
-
In addition to a full clinical reassessment, a chest radiograph should be repeated in patients who are not progressing satisfactorily.
12.4 When can patients be safely discharged from hospital?
There will be considerable pressure to discharge patients early during a pandemic. The type and availability of out-of-hospital facilities will dictate hospital discharge decisions. Some guidance regarding simple parameters to review when considering hospital discharge can be obtained from a recent US prospective, multicentre, observational cohort study of 680 patients admitted to hospital with CAP98 and is offered as advice for all patients admitted with influenza-related respiratory complications.
Recommendations
-
Patients should be reviewed before 24 hours of discharge home. Those with two or more of the following unstable clinical factors should be considered for continued hospital management:
temperature >37.8°C
heart rate >100/min
respiratory rate >24/min
systolic blood pressure <90 mmHg
oxygen saturation <90%
inability to maintain oral intake
abnormal mental status.
12.5 What arrangements should be made for follow up after hospital discharge for influenza and by whom?
It is usual practice to arrange “routine” hospital clinic follow up and repeat the chest radiograph at around six weeks after discharge for acute respiratory illness such as pneumonia. However, there is no evidence on which to base a recommendation regarding the value of this practice in patients who have otherwise recovered satisfactorily. It is also not known whether there is any value in arranging clinical follow up in a hospital clinic rather than with the patient’s GP. During an influenza pandemic situation, it is likely that only patients who developed complications or who had significant worsening of their underlying disease will be offered clinical review at one or other venue.
At discharge, patients should be offered access to information about their take home medication, smoking and lifestyle advice as appropriate, potential future complications and action to take in the event of a relapse of symptoms.
Recommendations
-
Follow up clinical review should be considered for all patients who suffered significant complications or who had significant worsening of their underlying disease, either with their GP or in a hospital clinic.
-
At discharge or at follow up, patients should be offered access to information about their illness, take home medication and any follow up arrangements.
-
It is the responsibility of the hospital team to arrange the follow up plan with the patient and the GP.
13 USE OF ANTIVIRALS IN HOSPITALISED ADULTS
13.1 What drugs should be used for antiviral treatment during a pandemic?
Oseltamivir (neuraminidase inhibitor) will be the mainstay for therapy in the pandemic. The M2 inhibitors, amantadine and rimantadine, are unsuitable for use for treatment due to the rapid emergence of resistance together with side effects.
From clinical trial data accrued to date and based on seasonal, interpandemic influenza, the anticipated positive effect of antivirals in a pandemic will be:
-
reduction of illness duration by 24 hours, and therefore more rapid mobilisation of affected individuals including essential workers
-
a possible reduction in hospitalisation of infected individuals
-
a reduction of subsequent antibiotic use by infected individuals.
There is insufficient evidence accrued to date to determine the effect of antivirals, if any, on overall mortality. Therefore the major utility of antivirals will be to maintain the essential workforce, and reduce hospitalisation and antibiotic treatment of complications.
13.2 Who should be treated with antivirals (neuraminidase inhibitors) during a pandemic?
Recommendations
-
Individuals should only be considered for treatment with neuraminidase inhibitors if they have all of the following:
an acute ILI
fever (>38°C) and
been symptomatic for two days or less.
-
Treatment schedule: adults: oseltamivir 75 mg every 12 hours for 5 days. Dose to be reduced by 50% if creatinine clearance is less than 30 ml/minute.
-
Exceptions:
Patients who are unable to mount an adequate febrile response—for example, the immunocompromised or very elderly—may still be eligible despite lack of documented fever.
Hospitalised patients who are severely ill, particularly if also immunocompromised, may benefit from antiviral treatment started more than 48 hours from disease onset.
This advice reflects the lack of robust evidence to guide the use of antivirals in these exceptional circumstances and places a high value on the potential benefits of antiviral therapy.
13.3 How do antivirals work?
Drugs available for treatment and prevention of infection by influenza are summarised in table 13.1. There are four drugs available, the older agents (amantadine and rimantadine) and the neuraminidase inhibitors (oseltamivir and zanamivir).
Older agents. Amantadine and rimantadine (rimantadine is not currently licensed in the UK), are related substances that act by blocking the ion-channel function of the influenza virus M2 protein. This protein, although a minor surface constituent of the influenza virus particles, is essential for virus replication. They are only active against influenza Type A. Amantadine is not recommended by NICE for treatment and/or prophylaxis of interpandemic influenza, so in the absence of national stockpiling, supplies of amantadine can be expected to be very low. H5 viruses in South East Asia are resistant to amantadine, so this agent may play no role at all depending on the nature of the pandemic strain.
Neuraminidase inhibitors. Neuraminidase inhibitors have been developed that have a potent anti-influenza activity in vitro and also have clinical efficacy. They are active against both Type A and Type B influenza viruses. The neuraminidase (NA) surface protein of the virus is essential for the de-aggregation and release of newly synthesised virions from infected cells. Inhibition of this enzyme interrupts propagation of the influenza virus within the human respiratory tract.
Two neuraminidase inhibitors so far have been developed to the level of entry into the formulary:
-
Zanamivir is a modification of Neu5Ac2en, a dehydrated neuraminic acid derivative.
-
Oseltamivir is a similar molecule except it has a cyclohexene ring and replaces a polyglycerol moiety with lipophilic sidechains.
Oseltamivir can be taken by mouth, whereas zanamivir must be inhaled, using a diskhaler device. An intravenous formulation of zanamivir has been developed but its efficacy has not been established. This may be relevant for the management of ventilator cases. Both drugs are active against both the influenza Type A and influenza Type B viruses.
13.4 What effect do antivirals have on the natural history of influenza?
Older agents: Both amantadine and rimantadine are effective for the treatment of Type A influenza virus infection if treatment is begun within 48 hours of the onset of illness.99 Historical data show that they can shorten the illness by approximately one day but their efficacy in preventing complications, hospitalisations, or deaths has never been established. Although these drugs are effective, their use in clinical influenza treatment has been limited as a result of their proclivity to induce viral resistance, and their side effect profile.
Neuraminidase inhibitors
13.4.1 Effect on symptoms
Several large clinical trials have demonstrated the utility of zanamivir and oseltamivir in treatment of adults with influenza in the community (table 13.2). The evidence yielded by these studies has recently been reviewed by the Cochrane Collaboration.100 Overall, neuraminidase inhibitors have been shown to shorten the duration of symptoms by one day. Across all studies, the time gained in returning to normal activities is half a day for laboratory-confirmed cases of influenza. The beneficial effect appears to be confined to patients in whom there is fever, (38°C in the study reported by Nicholson et al, 2000,101 and 37.8°C in the study reported by the MIST group 1998102) and who are treated within 48 hours of the onset of symptoms. Oseltamivir has also been shown to have efficacy in children aged 1–12 years. In one study involving 452 children with proven influenza, the median duration of illness was reduced by 36 hours (26%) in oseltamivir compared with placebo recipients (101 hours; 95% CI, 89 to 118 v 137 hours; 95% CI, 125 to 150; p<0.0001). Oseltamivir treatment also reduced cough, coryza and duration of fever.103 The neuraminidase inhibitors may have the additional benefit of reducing transmission between hosts; in studies of experimental human influenza, zanamivir greatly reduced titres of virus cultured from the nasopharynx as well as the mean duration of viral shedding.104
13.4.2 Effect on outcomes
Virtually all studies on the efficacy of neuraminidase inhibitors to reduce complications have been conducted with oseltamivir, and this drug has been shown to have some effect on outcomes other than time to recovery. In a metanalysis of adults and adolescents with a virologically proven influenza illness, oseltamivir treatment reduced overall antibiotic use for any reason by 26.7% (14.0% v 19.1% with placebo; p<0.001) and the incidence of influenza-related chest infections such as bronchitis resulting in antibiotic therapy by 55% (4.6% v 10.3% with placebo; p<0.001). In those subjects considered at increased risk of complications, 74 (18.5%) of 401 placebo recipients developed a chest infection leading to antibiotic use compared with 45 (12.2%) of 368 oseltamivir recipients (34.0% reduction; p = 0.02). Hospitalisation for any cause occurred in 18 (1.7%) of 1063 placebo recipients compared with 9 (0.7%) of 1350 oseltamivir-treated patients (59% reduction; p = 0.02). In contrast, among subjects with an ILI but without a confirmed influenza infection, the incidence of complicating chest infections (6.7% v 5.3%), overall antibiotic use (19.7% v 19.3%), or hospitalisations (1.7% v 1.9%) was similar between placebo and oseltamivir recipients, respectively.105 So far, the neuraminidase inhibitors have not been extensively investigated in patients who are at the highest risk of serious complications of influenza. Such patients include the elderly and those with serious cardiopulmonary illness, such as COPD. The neuraminidase inhibitors have not been associated with a reduction in mortality, but the clinical trials conducted so far have not been appropriate to measure this.
13.5 Will antivirals have activity against the pandemic strain of influenza virus?
It is not known for certain whether the neuraminidase inhibitors will be effective in pandemic influenza because their use has only been assessed in interpandemic influenza, where the virulence is moderate and there is some degree of host immunity. The antiviral activity is likely to be adequate; in vitro, all neuraminidase inhibitors have been demonstrated to have a broad spectrum of activity against multiple avian influenza viruses.106 The older agents, rimantadine and amantadine, were studied in both the 1968 Hong Kong pandemic and again when H1N1 influenza appeared in a pandemic in 1977. Their efficacy has been reviewed by Hayden.99 When the older agents were given for 4–8 week periods as prophylaxis in a community setting, their protective efficacy against influenza illness averaged 70% compared with placebo. This compares with 80–90% efficacy observed with the same agents in studies during the interpandemic period.
13.6 Can influenza virus develop resistance to the antivirals?
When amantadine or rimantadine are used to treat patients, resistant viruses emerge rapidly and approximately 30% of treated children or adults will shed resistant variants starting 2–5 days after the onset of treatment.104 The resistant viruses shed from these patients retain full virulence, infectivity and transmission potential. When contacts of cases treated with amantadine or rimantadine are given post-exposure prophylaxis with these older agents, the reduction in secondary cases is minimal.107
In contrast, the frequency of emergence of resistance during treatment with the neuraminidase inhibitors is reported to be low. However, during studies of experimentally-induced influenza A/H1N1 infection in healthy adults, 4% of participants shed viruses with a histidine to tyrosine substitution at position 274 within the binding site of oseltamivir.108 In these cases the volunteers had increased influenza viral load within the nasopharynx but there was no deterioration of symptoms. So far, there have been no proven instances of transmission of oseltamivir or zanamivir-resistant variants in field clinical trials, but the experience is relatively small currently. Sequence analysis of H5N1 human isolates from North Vietnam have revealed virus with a 274-Y (resistant) sequence. Although the isolate was not fully resistant, its IC50 for oseltamivir was shifted upwards and it is therefore less susceptible to oseltamivir than other H5N1 isolates that had been tested from the region. The patient from whom the virus was isolated was concurrently being treated with oseltamivir.
13.7 What side effects occur during use of antivirals?
Both amantadine and rimantadine can cause nausea and vomiting in a small percentage of individuals receiving them (table 13.1). Unfortunately amantadine is also associated with very unpleasant central nervous system side effects including anxiety, depression, insomnia and hallucinations. The side effects are dose related and do resolve with discontinuation of the drug.
In the case of the neuraminidase inhibitors, both drugs appear relatively safe. Zanamivir has very few side effects, but can result in bronchospasm which might be potentially serious in patients with asthma. Oseltamivir requires dose reduction in patients with low creatinine clearance (<30 ml/min). Nausea occurs in 5–15% of oseltamivir recipients but is seldom severe enough to lead to drug discontinuation (table 13.3).
14 USE OF ANTIBIOTICS IN HOSPITALISED ADULTS
14.1 Introduction
Antimicrobial chemotherapy will be indicated primarily for respiratory complications due to secondary bacterial infections, principally influenza-related pneumonia. The majority of patients with exacerbations of COPD and other chronic lung conditions, such as bronchiectasis, due to secondary bacterial infections will also require antimicrobial chemotherapy, as will some patients with severe sinusitis.
Few pneumonias and lower respiratory tract infections are defined microbiologically at initial assessment and hence most prescribing is empirical. In broad terms the antimicrobial management of these patients should follow the guidance offered in relevant national guidelines for the management of community acquired pneumonia and COPD, but modified in the light of the different range of pathogenic bacteria that may be implicated, specifically S aureus infection.
In the minority of cases, the aetiology may be determined after hospital admission, thereby permitting modification of the initial empirical regimen.
Although the pathogens responsible for community acquired pneumonia are diverse, in the case of bacterial pneumonia complicating influenza the principal pathogens which should be covered by any initial empirical antimicrobial therapy include: S pneumoniae, H influenzae and S aureus. The latter is said to be more common with combined viral-bacterial pneumonia, as some strains of staphylococci have synergistic effect with the virus. Gram negative enteric bacillary infection is also sometimes seen. Exacerbations of COPD will be largely associated with S pneumoniae, H influenzae, and Moraxella catarrhalis (M catarrhalis). Severity assessment and the association of pre-existing comorbid disease is essential in predicting prognosis and in turn determines management, choice of antibiotic therapy and its method of administration (see Section 9).
14.2 Antibiotic resistance of respiratory pathogens
During an influenza pandemic this will be principally related to concerns about the local pattern of antimicrobial resistance of S aureus, and assessing the possibility of methicillin resistant S aureus (MRSA) being present locally. Clinicians should be kept closely informed of any local shift in antimicrobial resistance patterns, both at the start and during a pandemic. S aureus is widely resistant to penicillin109 and an increasing number are now methicillin resistant (MRSA); when occurring in the community this generally reflects hospitalisation within the recent past or residence within a nursing home.110 Hence, β-lactamase unstable penicillins (penicillin G, aminopenicillins) and, in the case of MRSA, isoxazolyl penicillins (flucloxacillin, cloxacillin) and cephalosporins, are inappropriate for such infections. The true incidence of resistance among pathogens in the community is difficult to estimate because most laboratory samples come from selected populations. With this limitation in mind, the presence of β-lactamase production among H influenzae varies geographically but ranges from 2–17%111,112 in various parts of the UK. M catarrhalis has a high rate of β-lactamase production.
Antibiotic resistance among S pneumoniae is of concern worldwide, owing to the dominance of this organism as a cause of community acquired pneumonia and because penicillin and macrolide resistance are frequently linked.112,113 However, to date it is not a common enough problem in the UK to influence initial antimicrobial management decisions.
Recent data provided by the HPA of antimicrobial sensitivities of respiratory pathogens isolated from blood and respiratory samples during the last 3–4 years (Robert George, personal communication) found macrolide resistance among about 10–14% methicillin sensitive S aureus (MSSA) isolates and 12–19% of S pneumoniae. Macrolides, apart from clarithromycin, have poor in vivo activity against H influenzae. By contrast, tetracycline resistance was around 5–8% for S pneumoniae, 3% for H influenzae and 2–8% for MSSA.
Fluoroquinolones have activity against methicillin sensitive S aureus (MSSA): with MIC 90 figures of 1.0 mg/l for ciprofloxacin, 0.5 mg/l for levofloxacin and 0.12 for moxifloxacin.114 Modern fluoroquinolones (oral moxifloxacin and oral and IV levofloxacin currently licensed in the UK) are therefore a possible choice for secondary bacterial infections following influenza where MSSA is a likely pathogen. A recent pharmacokinetic and pharmacodynamic in vitro study indicated that moxifloxacin 400 mg od had advantages over ciprofloxacin 500 mg bd or levofloxacin 500 mg od in antimicrobial effects against S aureus.115 The quinolones, levofloxacin or moxifloxacin, also provide cover against S pneumoniae and H influenzae. MRSA is an unlikely pathogen in the UK in the context of community acquired respiratory bacterial infection following influenza and fluoroquinolones are not sufficiently active against MRSA.
14.3 Formulation of these recommendations
There are no robust research studies available to provide evidence based guidance on the best empirical choice of antimicrobial therapy for bacterial complications of influenza. For these reasons the recommendations for treatment have been made on the basis of assessing a matrix of laboratory, clinical, pharmacokinetic and safety data, interpreted in an informed manner and taking account of other published guidelines.116
Empirical therapy
14.4 Adults with influenza not complicated by pneumonia
In those with chronic lung disease, particularly COPD, bacterial exacerbation will be the commonest cause of admission. It is likely that all such patients sufficiently ill to require hospital admission with an exacerbation will require antibiotics. Management of their underlying condition, such as COPD, should follow standard guidelines, including the use of corticosteroids if indicated.
Antibiotics should cover the likely bacterial pathogens including: S pneumoniae, H influenzae, M catarrhalis and S aureus. Oral therapy should be sufficient for those without adverse severity features and who are able to take oral medication.
The preferred first choice of antibiotic for non-pneumonic bronchial infections should include an effective oral β-lactamase stable agent such as co-amoxiclav, or a tetracycline, such as doxycycline. A macrolide is an alternative for those intolerant of the preferred first choices, while remembering the possibility of antimicrobial resistance. Clarithromycin has better activity against H influenzae than azithromycin. A newer generation fluroquinolone (for example, levofloxacin or moxifloxacin) with enhanced activity against S pneumoniae is an alternative choice if there is increased likelihood of resistance or local issues that dictate such a choice.
Recommendations (see table 14.1)
-
Previously well adults with acute bronchitis complicating influenza, in the absence of pneumonia, do not routinely require antibiotics.
-
Antibiotics should be considered in those previously well adults who develop worsening symptoms (recrudescent fever or increasing dyspnoea).
-
Patients at high risk of complications or secondary infection (Appendix 2) should be considered for antibiotics in the presence of lower respiratory features.
-
Most patients can be adequately treated with oral antibiotics.
-
The preferred choice includes co-amoxiclav or a tetracycline.
-
A macrolide such as clarithromycin (or erythromycin) or a fluoroquinolone active against S pneumoniae and S aureus is an alternative choice in certain circumstances.
14.5 Adults with non-severe influenza-related pneumonia
Patients will be suffering from primary viral pneumonia, or combined viral-bacterial pneumonia, or secondary bacterial pneumonia. The features of each of these are covered in Section 3.
All patients with pneumonic involvement should receive antibiotics. The principles of antibiotic selection for non-severe influenza-related pneumonia are similar to those for the management of sporadic community acquired pneumonia in general,72 except that adequate cover for S aureus should be included in any empirical regimen. It is also not felt necessary to routinely provide cover for atypical pathogens (Mycoplasma pneumoniae, Chlamydia sp, Coxiella burnetti, Legionella sp) during a pandemic as the large majority of patients will be hospitalised as a direct result of influenza and its complications caused by bacterial infection.
For these reasons oral co-amoxiclav or a tetracycline, such as doxycycline, is the preferred regimen (table 14.1). When oral therapy is inappropriate, parenteral co-amoxiclav or a second or third generation cephalosporin is offered as an alternative. Based on in vitro data, the activity of selected cephalosporins against MSSA in the UK in descending rank order is cefuroxime (MIC90 1–2 mg/l) > cefotaxime (MIC90 2 mg/l) > ceftriaxone (MIC90 16 mg/l) (Robert George, personal communication). Only cefuroxime and cefotaxime are recommended as cephalosporins offering adequate MSSA cover within an empirical regimen.
A macrolide or one or the new fluoroquinolones are identified as an alternative in hospitalised patients, in specific circumstances. These include those intolerant of penicillins or where local microbiological surveillance suggests they are better choices. At the time of completing these guidelines, only levofloxacin and moxifloxacin are licensed and available in the UK for pneumonia.
Flucloxacillin is not recommended as part of an empirical regimen because its activity against a narrow spectrum of pathogens (predominantly S aureus) would require it to be used in combination with more than one other antibiotic. It is offered as the antibiotic of choice in confirmed methicillin sensitive S aureus (MSSA) infection.
Regardless of the regimen selected it is critical that the antibiotics be administered promptly (within four hours of admission), and in the case of the patient with severe pneumonia without delay, by the admitting doctor in the admissions ward or by the GP if delays are expected in the hospital admission process. Delays in administration of antibiotics are related adversely to mortality in some studies, particularly when managing elderly patients.117,118
Following initial assessment and empirical therapy, progress should be monitored carefully. The route and choice of antibiotic treatment will require adjustment, either by stepping up and broadening the spectrum of microbiological activity in the light of clinical deterioration or as a result of positive microbiological information, or stepping down with improvement as discussed below.
Recommendations (see table 14.1)
-
Most patients can be adequately treated with oral antibiotics.
-
Oral therapy with co-amoxiclav or a tetracycline is preferred.
-
When oral therapy is contraindicated, recommended parenteral choices include intravenous co-amoxiclav, or a second or third generation cephalosporin (cefuroxime or cefotaxime respectively).
-
A macrolide (erythromycin or clarithromycin) or a fluoroquinolone active against S pneumoniae and S aureus is an alternative regimen for those intolerant of penicillins. Currently levofloxacin and moxifloxacin are the only recommended fluoroquinolones licensed in the UK.
-
Antibiotics should be administered within four hours of admission.
14.6 Adults with severe influenza-related pneumonia
Mortality is greatly increased in those with severe pneumonia (Section 9). The illness may progress before microbiological information is available.
Preferred and alternative initial treatment regimens are summarised in table 14.1. The recommendation of broad spectrum β-lactam regimens plus a macrolide in those with severe influenza-related pneumonia is based on the following rationale:
-
While S pneumoniae and Saureus remain the predominant pathogens, Gram negative enteric bacilli, although uncommon, carry a high mortality.119
-
The recommended empirical regimen will offer double cover for the likely pathogens implicated in influenza-related pneumonia and there is some evidence to indicate that combination therapy is associated with better outcomes in severe pneumonia.120
-
Although there is no evidence of an increased incidence of infection by atypical pathogens in influenza-related pneumonia, in severe pneumonia, it is felt necessary to include cover for atypical pathogens, particularly Legionella sp, as it may not be possible at the outset to distinguish between patients with sporadic severe community acquired pneumonia in whom Legionella infection is important, and influenza-related pneumonia.
Parenteral administration of antibiotic is recommended in those with severe community acquired pneumonia regardless of the patient’s ability or otherwise to take oral medication. This is to ensure prompt, high blood and lung concentrations of antibiotic.
A fluoroquinolone is offered as an alternative, despite limited data on their use in severe pneumonia.121 At the time of writing, levofloxacin is the only licensed and available agent in the UK for severe pneumonia. It is marketed in parenteral and oral formulations. However, until more clinical experience is available we recommend combining it with another agent active against S pneumoniae and S aureus such as a broad spectrum β-lactam or macrolide when managing severe influenza-related pneumonia.
Recommendations (see table 14.1)
-
Patients with severe pneumonia should be treated immediately after diagnosis with parenteral antibiotics.
-
An intravenous combination of a broad spectrum beta-lactamase stable antibiotic such as co-amoxiclav or a second (for example, cefuroxime) or third (for example, cefotaxime) generation cephalosporin together with a macrolide (clarithromycin or erythromycin) is preferred.
-
An alternative regimen includes a fluoroquinolone with enhanced activity against pneumococci together with a broad spectrum β-lactamase stable antibiotic or a macrolide. Currently levofloxacin is the only such fluoroquinolone licenced in the UK.
-
Patients who have been in hospital within the last few months have a higher chance of carrying MRSA as opposed to patients who have not been hospitalised recently. Therefore due consideration should be given to the possibility of MRSA if they are known or suspected to have a staphylococcal pneumonia and/or are not responding to empirical therapy.
14.7 When should the IV route be changed to oral?
There can be no rigid recommendation concerning the timing of transfer to oral therapy and further studies of this area are needed.122 Any decision must be individualised on the basis of assessing all factors, including the absence of any contraindications to oral administration, the availability of any microbiological information regarding aetiology of the infection and clear evidence that the patient is responding to initial therapy. The recommended guideline is that oral therapy be considered in a patient who has shown clear evidence of improvement and whose temperature has resolved for a period of 24 hours.
Recommendations
-
Patients treated initially with parenteral antibiotics should be transferred to an oral regimen as soon as clinical improvement occurs and the temperature has been normal for 24 hours, providing there is no contraindication to the oral route.
14.8 For how long should antibiotics be given?
Until there are more precise methods to reliably identify microbiological and clinical end-points, the duration of therapy will remain subject to clinical judgement and custom. For these reasons the duration of therapy will vary by individual patient, disease severity and speed of resolution.
Recommendations
-
For most patients admitted to hospital with non-severe and uncomplicated pneumonia, seven days of appropriate antibiotics is recommended.
-
For those with severe, microbiologically undefined pneumonia, 10 days’ treatment is proposed. This should be extended to 14–21 days where S aureus or Gram negative enteric bacilli pneumonia is suspected or confirmed.
14.9 Failure of initial empirical therapy
In those patients who fail to respond to initial empirical therapy, several possibilities need to be considered, the first of which is whether the correct diagnosis been made. Radiographic review is recommended for the community and hospital-managed patient. This may also indicate complications of pneumonia such as pleural effusion/empyema, lung abscess or worsening pneumonic shadowing, which will be more common in the presence of staphylococcal infection.
The initial empirical antibiotic regimen may need to be reassessed. However, compliance with, and adequate absorption of an oral regimen should first be considered.
Microbiological data should be reviewed and further specimens examined, with a view to excluding S aureus and Gram negative bacillary infection.
In the hospital-managed, non-severely ill patient, changing to a new fluoroquinolone such as levofloxacin provides a second alternative.
In the severely ill patient already receiving a β-lactam/clarithromycin regimen, it is recommended that further staphylococcal cover is added to include cover for MRSA.123 In addition, urgent referral to a respiratory physician should be made for clinical assessment including the possible need for bronchoscopic sampling. Other rapid MRSA diagnostic techniques are in the evaluation stage.
Recommendations
-
For those with non-severe pneumonia in hospital on combination therapy, changing to a fluoroquinolone with effective pneumococcal and staphylococcal cover is an option.
-
Adding further antibiotics effective against MRSA is an option for those with severe pneumonia not responding to combination antibiotic therapy.
Specific pathogen-directed antibiotic therapy
14.10 What are the optimum antibiotic choices when specific pathogens have been identified?
When a pathogen has been identified specific therapy as summarised in table 14.2 is proposed. In transferring patients from empirical to pathogen-targeted therapy, the regimen and route of administration will be determined by the continued need for parenteral therapy and known drug intolerance. These recommendations are again based on a synthesis of information, which includes in vitro activity of the drugs, appropriate pharmacokinetics and clinical evidence of efficacy gleaned from a variety of studies. The choice of agent may be modified following the availability of sensitivity testing or following consultation with a specialist in microbiology, infectious disease or respiratory medicine. Close liaison with the local microbiology service will be essential during a pandemic.
Currently S pneumoniae highly resistant to penicillin (MIC ⩾4 mg/l) is uncommon in the UK. However, it is important that the situation is monitored and in future higher doses of penicillins or alternative regimens may need to be considered.
S aureus is an uncommon cause of sporadic community acquired pneumonia in the UK, but will assume much greater potential importance during a pandemic. Most community isolates are methicillin sensitive, although the recent increase in MRSA in hospitalised patients may result in subsequent readmission with an MRSA infection, secondary to influenza. Options for methicillin sensitive and resistant infections are based on parenteral administration in view of the serious nature of staphylococcal pneumonia.
Recommendations
-
If a specific pathogen has been identified, the antibiotic recommendations are summarised in table 14.2.
PART 3 Clinical management of children referred to hospital
15 SEVERITY ASSESSMENT IN CHILDREN REFERRED TO HOSPITAL
15.1 Initial management (see Appendix 5)
(a) Coughs and mild fevers. Treat at home
An influenza pandemic is likely to occur during the winter season when other winter viruses such as respiratory syncytial virus (RSV) are also circulating. Many children will have coughs and mild fevers and should be managed in the usual way at home by parents with antipyretics and fluids. (Note: aspirin should not be used in children under 16 years of age.)
(b) High fever (>38.5°C) and cough or influenza-like symptoms. Advised by community health professional
Children with high fever (>38.5°C) and cough or influenza-like symptoms will be seen by a community health professional (a nurse or doctor if under 7 years of age). If there are no features that put them at high risk of complications they should be treated with oseltamivir, and given advice on antipyretics and fluids. Children under 1 year of age and those at risk of complications (Appendix 2) should be seen by a general practitioner (GP).
(c) High fever (>38.5°C) and cough or influenza-like symptoms plus at risk group. Assessed by GP or at A&E department
Children may be considered at increased risk of complications if they have cough and fever (or influenza-like illness) and temperature >38.5°C and either (i) chronic comorbid disease (see Appendix 2) or (ii) one of the following features:
-
breathing difficulties
-
severe earache
-
vomiting >24 hours
-
drowsiness.
These patients should be offered an antibiotic as well as oseltamivir (in those over 1 year of age) and advice on antipyretics and fluids. Children under 1 year of age with none of the above features should be treated with antipyretics and fluids with a low threshold for antibiotics if they become more unwell.
15.2 When to refer for admission?
The most severely ill children should be referred for assessment for admission. Indicators are:
-
Signs of respiratory distress
markedly raised respiratory rate
grunting
intercostal recession
breathlessness with chest signs
(A useful severity assessment for respiratory distress is taken from the British Thoracic Society pneumonia guidelines72; see Appendix 8.)
-
Cyanosis
-
Severe dehydration
-
Altered conscious level
-
Complicated or prolonged seizure
-
Signs of septicaemia—extreme pallor, hypotension, floppy infant.
15.3 Assessment in hospital
Children will be triaged for admission to wards, high dependency unit (HDU) or paediatric intensive care unit (PICU). Most children admitted to hospital are likely to need oxygen therapy and/or intravenous support as well as antibiotics and oseltamivir (see General Management Section 18).
15.4 Indications for transfer to high dependency or intensive care unit
-
The child is failing to maintain a SaO2 of >92% in FiO2 of >60%.
-
The child is shocked.
-
There is severe respiratory distress and a raised PaCO2 (>6.5 KPa).
-
There is a rising respiratory rate and pulse rate with clinical evidence of severe respiratory distress with or without a raised PaCO2.
-
There is recurrent apnoea or slow irregular breathing.
-
There is evidence of encephalopathy.
15.5 What to do when there are no PICU beds available?
In a pandemic situation, paediatric high dependency and intensive care beds are likely to fill quickly and will be insufficient to meet demand. Children will have to be triaged by the senior paediatrician on duty in consultation with tertiary specialists in respiratory medicine, paediatric intensive care or paediatric infectious diseases. Triage will be on the basis of the severity of the child’s (a) acute and (b) coexisting disease and the likelihood of the child achieving full recovery. Where admission is not possible the tertiary specialists will provide advice and support on management to the general paediatrician.
16 GENERAL INVESTIGATIONS FOR CHILDREN IN HOSPITAL
16.1 Are blood tests useful?
A low white blood count (WBC) is common in influenza A in children (WBC <4 in 8–27%,62,71 WBC <5 in 24%84) with a lymphopenia (<1.5 in 41%124;<1.0 in 40%71). In contrast, a raised WBC (>15) is found in only 8–12% of cases.62,71
In the H5N1 cases reported from Vietnam125 all seven children had WBC <4.0 (mean 2.44) and 6/7 had a lymphopenia <1.0 (mean 0.66). Six of the seven children died. In contrast, only two of the seven children reported from Hong Kong died but they were both leukopenic and lymphopenic. The survivors had a mean WBC of 12.44 and lymphocyte count of 3.11.126 Four of five cases reported from Thailand were lymphopenic.127
In influenza A thrombocytopenia (<100) is found in 5–7%.71,84 Thrombocytopenia was found in four out of seven cases of H5N1 infection in Vietnamese children.125
Liver transaminases are raised in 27% of influenza A patients125 and were raised in six out of six of those measured in the Hong Kong H5N1 outbreak126 and five out of six in those measured in Vietnam.125
C-reactive protein (CRP) is unhelpful in influenza with values <10 in 55%84; <20 in 72% and >80 in only 5%.62
The CD4/CD8 ratio was inverted in the two children and three adults in whom it was measured in the Vietnam outbreak (mean 0.7, range 0.59–1.08) Two of these patients survived.125
Recommendation
-
A full blood count with differential, urea, creatinine and electrolytes and liver enzymes and a blood culture should be done in all severely ill children.
16.2 When to do a chest radiograph?
One of the largest studies of the value of chest radiography was undertaken in children aged between 2 months and 5 years with community acquired pneumonia managed as outpatients with time to recovery as the main outcome.128 Chest radiography did not affect the clinical outcome in these children with acute lower respiratory infection. This lack of effect was independent of clinicians’ experience. There are no clinically identifiable subgroups of children within the World Health Organization case definition of pneumonia who are likely to benefit from a chest radiograph. The authors concluded that routine use of chest radiography was not beneficial in ambulatory children aged over two months with acute lower respiratory tract infection.
16.2.1 Observer agreement on radiographic signs of pneumonia
Clinicians basing the diagnosis of lower respiratory infections in young infants on radiographic diagnosis should be aware that there is variation in intraobserver and interobserver agreement among radiologists on the radiographic features used for diagnosis. There is also variation in how specific radiological features are used in interpreting the radiograph. A recent study on standardisation of chest x ray interpretation in paediatric pneumonia illustrates the importance of standardised training.129 The cardinal finding of consolidation for the diagnosis of pneumonia appears to be highly reliable130 and reasonably specific for bacterial pneumonia (74% of 27 patients with alveolar shadowing had bacterial proven pneumonia)131 but overall chest radiography is too insensitive to be useful in differentiating between patients with bacterial pneumonia and those whose pneumonia is non-bacterial.132,133
In the context of an influenza pandemic, a chest x ray will not distinguish viral pneumonia from viral illness with bacterial superinfection and all children with signs of pneumonia should be treated with antibiotics.
Recommendation
-
A chest x ray should be performed in children who are hypoxic, have severe illness or who are deteriorating despite treatment.
16.3 Who should have pulse oximetry?
Oxygen saturation (SaO2) measurements provide a non-invasive estimate of arterial oxygenation. Pulse oximetry will be a key tool in assessment and management and it is essential that it is used correctly and that users are aware of the possibility of artefactually low readings. The oximeter appears easy to use and requires no calibration. However, it requires a pulsatile signal from the patient. It is also highly subject to motion artefacts. To obtain a reliable reading:
-
The child should be still and quiet
-
When using paediatric wrap around probes, the emitting and receiving diodes need to be carefully opposed
-
A good pulse signal (plethysmograph) should be obtained
-
Once a signal is obtained, the saturation reading should be watched over at least 30 seconds and a value recorded once an adequate stable trace is obtained.
Recommendation
-
Pulse oximetry should be performed in every child being assessed for admission to hospital with pneumonia.
17 MICROBIOLOGICAL INVESTIGATIONS FOR CHILDREN IN HOSPITAL
To be read in conjunction with the corresponding section for adults (Section 11 in Part 2).
17.1 Introduction
As with adults, the extent of virological and microbiological investigations undertaken in children should vary according to the stage of the pandemic and additionally according to the severity of an individual case. It should be noted however, that the clinical features of influenza in children are less characteristic than in adults (see Section 4) and the need for special diagnostic tests is therefore greater.62,134,135 A respiratory panel including influenza A and B, RSV, adenovirus, rhinovirus and parainfluenza 1,2,3 should be standard. The clinical features of human metapneumovirus infection may also be similar but current laboratory tests are limited.124 Which tests are performed will vary according to the local laboratory but might include rapid antigen tests, immunofluorescence, culture, RT-PCR and serology. See Health Protection Agency (HPA) guidance for further details.
17.2 Rapid influenza tests
The utility of such tests has been demonstrated in studies where rapid knowledge of a diagnosis of influenza (within 10 minutes) has been shown to have an impact on clinicians’ behaviour with respect to antibiotic use, performance of other tests and admission to hospital.136,137 It may be imagined that in a pandemic situation such a test could result in earlier use of antiviral therapy and a more rational approach to hospital admission and to prophylaxis of contacts. However, using a molecular reference standard, one test was shown to have low sensitivity (44%) but high specificity (97%), suggesting that its role might better be to “rule in” influenza rather than “ruling it out”.138 Similar conclusions have been made with other commercial rapid tests.139,140 As a reflection of this, rapid antigen tests were positive in only two of six patients with avian influenza A (H5N1).125
17.3 Bacteriology
The need for bacteriological tests in cases of influenza with pneumonia is also logical and the range of pathogens similar to adults36,69,141–145 except that Legionella infection is extremely unlikely to occur in a previously healthy child and Legionella-specific antigen testing is therefore unnecessary. The urinary pneumococcal antigen tests in children may lack both sensitivity and specificity and should be interpreted with care.146,147 Sputum collection in children is also unreliable although in older children (for example, over 12 years of age) it may be possible and should be handled as indicated for adults.
(I) Recommendations: early pandemic (UK alert levels 1–3)
A. Virology—all children
-
Nasopharyngeal aspirate or nose and throat swabs in virus transport medium should be collected from all patients and submitted to the local laboratory. The relevant laboratory should be notified of the suspected diagnosis and there should be close liaison over sample collection, handling and transport.
-
Rapid testing by direct immunofluorescence or rapid enzyme immunoassay test, virus culture and/or polymerase chain reaction should be undertaken according to local availability and/or referred to an appropriate laboratory. Testing for influenza A and B, RSV, adenovirus, rhinovirus and para-influenza 1,2,3 should be standard.
-
During UK alert level 1, when the UK is on high alert for the first cases of pandemic influenza, suspected cases are likely to be investigated by local Health Protection Teams from the HPA and its partner organisations in the devolved administrations.
-
During UK alert levels 1 and 2, clinicians dealing with suspected cases of pandemic influenza should ensure that the local Health Protection Team is informed and involved from the outset.
-
The HPA and its partner organisations in the devolved administrations have established a network of more than 20 laboratories across the UK which have been proficiency tested in molecular diagnosis of influenza A/H5N1. Access to this service should be via local health protection teams.
-
If presentation is more than seven days after onset of illness, an “acute” serum (2–5 ml clotted blood) should be collected and a “convalescent” sample (2–5 ml clotted blood) obtained after an interval of not less than seven days. The two sera should be examined serologically for evidence of recent influenza infection.
B. Bacteriology—children with influenza-related pneumonia
The following bacteriological tests should be performed:
-
Blood culture (before antibiotic treatment is commenced)
-
Sputum Gram stain, culture and antimicrobial susceptibility tests on samples obtained from older children who:
are able to expectorate purulent samples, and
have not received prior antibiotic treatment.
Sputum samples should be transported rapidly to the laboratory.
-
Paired serological examination for influenza/other agents. “Acute” serum should be collected and a “convalescent” sample obtained after an interval not less than seven days (both 2–5 ml clotted blood) and the two sera stored for subsequent testing.
(II) Recommendations:established pandemic (UK alert level 4)
A. Virology—not routinely recommended
B. Bacteriology—children with influenza-related pneumonia
Specific investigations should include:
-
Blood culture, before antibiotic treatment is commenced
-
Sputum Gram stain, culture and antimicrobial susceptibility tests on samples obtained from older children who:
are able to expectorate purulent samples, and
have not received prior antibiotic treatment.
Sputum samples should be transported rapidly to the laboratory.
-
Paired serological examination for influenza/other agents. “Acute” serum should be collected and a “convalescent” sample obtained after an interval not less than seven days (both 2–5 ml clotted blood) and the two sera stored for subsequent testing.
-
In an intubated patient tracheal or endotracheal aspirate samples should be sent for Gram stain, culture and antimicrobial susceptibility testing as well as viral testing (listed above).
18 GENERAL MANAGEMENT OF CHILDREN ADMITTED TO HOSPITAL
18.1 Introduction
During an influenza pandemic children are likely to be admitted to hospital because of the severity of their disease and its complications or because of the impact of influenza on pre-existing disorders such as cardiac, respiratory or neurological disease. Management of pre-existing disorders is outside this guideline. The most common reason for admission is likely to be:
-
Lower respiratory tract disease with either a viral or bacterial or mixed pneumonia.
Other reasons for admission include:
-
Severe gastroenteritis
-
Cardiac disease—viral myocarditis
-
Encephalitis.
18.2 Triage
Children should be triaged to ward or HDU/PICU after severity assessment (Section 15).
18.3 Cohorting
An influenza pandemic is likely to occur in the winter months when other winter viruses responsible for paediatric morbidity and hospital admission are circulating (such as RSV and adenovirus). Particularly in the early stages of a pandemic (UK alert levels 1–3) it will be important to use rapid virological tests in an attempt to cohort influenza positive and RSV positive infants separately and to separate from other patients (see UK Infection Control Guidance for Pandemic Influenza).3
18.4 Who needs oxygen?
Hypoxic infants and children may not appear cyanosed. Agitation may be an indication of hypoxia. Patients whose oxygen saturation is less than 92% while breathing air should be treated with oxygen given by nasal cannulae, head box, or face mask to maintain oxygen saturation above 92%. Nasal cannulae do not deliver a FiO2 more than around 40% even at flow rates of 2 l/min in infants and 4 l/min in older children. Alternative methods of delivering higher concentrations of humidified oxygen such as a head box or a Venturi face mask may be necessary. If SaO2 >92% cannot be maintained with FiO2 of 60% then additional support such as CPAP, BiPAP or intubation and ventilation should be considered.
Recommendations
-
Patients whose oxygen saturation is 92% or less while breathing air should be treated with oxygen given by nasal cannulae, head box, or face mask to maintain oxygen saturation above 92%.
18.5 Who needs fluids?
Children who are unable to maintain their fluid intake due to breathlessness, fatigue or gastroenteritis need fluid therapy. Where possible additional fluid should be by the enteral route and where nasogastric tube feeds are used, the smallest tube should be passed down the smallest nostril to minimise effects on respiratory status. Severely ill children may need intravenous fluids and if the child is in oxygen therapy intravenous fluids should be given at 80% basal levels (to avoid complications of inappropriate ADH secretion) and serum electrolytes should be monitored.
18.6 What monitoring is necessary?
The monitoring will depend on the child’s condition. Severely ill children will need continuous monitoring of heart rate, respiratory rate, oxygen saturation and neurological status. All children on oxygen therapy should have four-hourly monitoring including oxygen saturation.
18.7 Who needs physiotherapy?
Chest physiotherapy is not beneficial in previously healthy children with pneumonia. Children with underlying conditions such as cystic fibrosis or neuromuscular weakness will benefit from intensive physiotherapy
18.8 Management of fever and pain
Children with influenza are generally pyrexial and may have some pain, including headache, chest pain, arthralgia, abdominal pain, and earache from associated otitis media. Pleural pain may interfere with depth of breathing and may impair the ability to cough. Antipyretics and analgesics can be used to keep the child comfortable and to help coughing.
18.9 When can children be safely discharged from hospital?
In a pandemic situation there will be great pressure on availability of hospital beds. All children should be assessed for discharge at least twice daily. Children should not remain in hospital if they are receiving therapy that could be given in the community. In previously healthy children suitable discharge criteria would be:
-
child is clearly improving
-
is physiologically stable
-
can tolerate oral feeds
-
respiratory rate is <40/min (<50/min in infants)
-
awake oxygen saturation is >92% on air.
18.10 Who needs follow up?
Most children will make an uneventful recovery and not require follow up. Those with a prolonged illness may be followed up by their GP. Only children with severe disease and/or at high risk of sequelae need hospital follow up. Children with lobar collapse should have a follow up chest x ray. Follow up chest x rays after acute uncomplicated pneumonia are of no value where the patient is asymptomatic.148,149
19 USE OF ANTIVIRALS IN HOSPITALISED CHILDREN
To be read in conjunction with the corresponding section for adults (Section 13 in Part 2).
19.1 Introduction
Five antiviral agents are theoretically available for the therapy of influenza in children: the M2 ion channel inhibitors amantadine and rimantadine (both administered orally and for influenza A only), the neuraminidase inhibitors oseltamivir (administered orally) and zanamavir (administered through an inhaler), and ribavirin (aerosolised).
19.2 Amantadine/rimantadine
The limitations of amantadine and rimantadine are detailed in Section 13, particularly in the context of a pandemic where resistance may already be present.150 Both have been shown to be effective in the treatment of influenza A in children.151 Concerns exist about the development of resistance during therapy for both agents.151,152 A household study showed that treatment and prophylaxis with rimantadine resulted in rapid selection and transmission of drug resistant virus.153
19.3 Neuraminidase inhibitors
In a double blind, randomised, placebo controlled study, 217 children (1–12 years of age) received oseltamivir with a resultant reduction in the median duration of illness, incidence of otitis media as a complication of influenza (12% v 21%) and the need for antibiotic prescriptions in those with influenza (68 of 217, 31% v 97 of 235, 41%; p = 0.03) compared to placebo.103 The most common side effect was vomiting (5.8%).
A systematic review and meta-analyses published in 2003 which included studies up to December 2001, included only two studies of zanamivir and one study of oseltamivir103 in which these drugs were administered for treatment of influenza A or B in children under 12 years of age.154 The reduction in the median time to alleviation of symptoms for influenza positive children when compared with placebo was 1.0 day (95% CI 0.4 to 1.6) for zanamivir and 1.5 days (95% CI 0.8 to 2.2) for oseltamivir. Across all ages a 29% (95% CI 10 to 44) relative reduction in complications requiring antibiotics was observed for zanamivir and for children specifically a 35% relative reduction was observed for oseltamivir. This was updated through to December 2002 in a Cochrane review.155
Using its search criteria it identified two trials of oseltamivir (one in healthy children103 and one in children with asthma which was later published156) and only one with zanamivir. Its conclusions were therefore the same with respect to median illness duration in healthy children. A significant reduction in complications (otitis media) was noted for oseltamivir while a trend to benefit was seen for zanamivir.155 Vomiting was significantly more common among oseltamivir recipients than placebo recipients (15% v 9%).
The review noted that there may be a difference in efficacy according to serotype with oseltamivir showing a significant reduction in time to resolution for influenza A (34%) but not B (8.5%).155 With respect to children with asthma there was a trend to reduction in time to freedom from illness for oseltamivir recipients but this did not reach statistical significance. Oseltamivir appeared to result in a more rapid improvement in pulmonary function, and was well tolerated in children with asthma.155,156 The Cochrane review concluded that oseltamivir was the preferred drug as it has shown a benefit with regard to secondary complications. It also concluded that there was no evidence of benefit in at-risk children (that is, those with asthma). From the perspective of pandemic use however, it should be noted that there was no evidence of harm in this group.
With regard to dosing of oseltamivir, pharmacokinetic studies have suggested that young children clear the drug faster than older children, adolescents and adults and therefore need higher doses.157,158 The major practical issue with regard to zanamivir is its mode of administration limiting its use to children over the age of 5 years (FDA guidance: over 7 years of age).155
The development of resistance to oseltamivir in children may be more common than appreciated and more common than seen in adults. In one study resistance mutations were documented in 18% of 50 children.158 This has implications for widespread use in a pandemic situation.
One particular issue with regard to paediatric use of oseltamivir is the apparent age limitation on its license (that is, not for children under 1 year of age). This is particularly important because during epidemic years, of all children with influenza, it is children under 6 months of age who are most likely to be hospitalised.159 The basis for this exclusion appears to be that rat data have shown high mortality in infant rats at 7 days of age when given a dose of 1000 mg/kg together with high brain levels of oseltamivir, assumed to reflect the immature blood-brain barrier at this age. This is reflected in product literature and an FDA alert, although there are no published data. As a result, there are few human data in this age group as it was felt that it would be difficult to monitor central nervous system toxicity in this age group. However, because of a fear of encephalopathy due to influenza in young children, Japanese paediatricians have been using it in infants and data on 102 consecutive infants from Japan revealed no encephalopathy or mortality in recipients.160 A second Japanese report where 47 children under 1 year were treated (4 mg/kg/day) showed similar efficacy for fever to a group of older children and no serious adverse effects.161
There are no data on the effectiveness of oseltamivir if given more than two days from onset of illness. It is likely to be less effective and in particular to have little or no effect after 5–6 days of illness unless the child is immunosuppressed. Giving oseltamivir to sick hospitalised patients is theoretically likely to decrease their infectivity and so may be useful but there are no data to support this.
19.4 Ribavirin
In a double blind, placebo controlled study children hospitalised with influenza who had been ill for 48 hours or less and who had a temperature of 37.8°C or more were randomised to receive either ribavirin or placebo. Sixty two patients (35 in the placebo group, 27 in the ribavirin group) had a confirmed diagnosis of influenza. The time to reduction of temperature to 38.3°C or less for the ribavirin group was 8.9 hours compared with 22.6 hours for the placebo group (p = 0.04). There were no other differences detected between groups.162 There have been no further published studies in the 11 years since this report thus ribavirin cannot be recommended at this time.
Recommendations
-
In the setting of a pandemic, children in the community should only be considered for treatment with antivirals if they have all of the following:
an acute influenza-like illness
fever (>38.5°C) and
been symptomatic for two days or less.
-
Oseltamivir is the antiviral agent of choice.
-
Treatment schedule for children over one year:
body weight 15 kg or under, ie <3 years: 30 mg every 12 hours
body weight >15–23 kg, ie <7 years: 45 mg every 12 hours
body weight 24 kg and over, ie >7 years: 75 mg every 12 hours.
-
In children who are severely ill in hospital oseltamivir may be used if the child has been symptomatic for less than six days.
-
Oseltamivir may be considered for the treatment of infants under 1 year of age, especially those with severe influenza. This would need to be done following appropriate discussion with the parents highlighting the concerns from the animal data and the relative paucity of human data in this age group.
20 USE OF ANTIBIOTICS IN HOSPITALISED CHILDREN
20.1 Who should receive antibiotics?
Secondary bacterial infections particularly pneumonia and otitis media are common in children with influenza. A case-control study during an outbreak of severe pneumococcal pneumonia demonstrated that patients with severe pneumonia were 12 times more likely to have had an influenza-like illness and four times more likely to have positive influenza serology than controls.69 Infections with Staphylococcus aureus (S aureus) and Haemophilus influenzae (H influenzae) are also more common during influenza outbreaks.
A randomised controlled trial of antibiotics in 85 children aged four months to 11 years presenting with influenza-like symptoms during an influenza epidemic showed a decreased incidence of pneumonia in the antibiotic treated group (2.4% v 16.3% p = 0.031).163 There was no change in duration of fever or incidence of acute otitis media. Interestingly only one out of seven of the cases of pneumonia in the placebo group was thought to be bacterial. The authors postulated that as bacterial proteases facilitate propogation and pathogenesis of influenza in a mouse model, decreasing bacterial numbers and hence protease levels in the lung may decrease viral pneumonia.
Another randomised trial of cephalosporins versus macrolides in 365 Japanese children with influenza-like symptoms showed faster alleviation of fever (3.8 (SD 1.4) v 4.3 (SD 1.4) days p = 0.006) in the macrolide group and a decrease in number with chest x ray evidence of pneumonia (2 v 13 cases p = 0.002; 14/15 had interstitial changes).164 The authors postulate that anti-inflammatory effects of macrolides may be responsible.
Recommendation
-
Children who (a) are at risk of complications of influenza or (b) with disease severe enough to merit hospital admission during an influenza pandemic should be treated with an antibiotic that will provide cover against S pneumoniae, S aureus and H influenzae.
20.2 Which antibiotic?
The antibiotics of choice must cover the likely pathogens as above. Data from HPA 2004 indicate that in the UK <2.5% of S pneumoniae strains are penicillin resistant and 14.1% are erythromycin (macrolide) resistant. Similarly 14% of methicillin susceptible S aureus were erythromycin resistant. Only 76% of H influenzae are susceptible to amoxicillin but >94% are susceptible to co-amoxiclav. There may be local variations to this data and clinicians should consult with their local microbiology department.
Recommendations
-
For children under 12 years co-amoxiclav is the drug of choice.
-
Clarithromycin or cefuroxime should be used in children allergic to penicillin. For children over 12 years doxycycline is an alternative.
20.3 What if the pathogen is known?
Rarely a blood culture or pleural tap will provide the pathogen. The antibiotics should then be specifically tailored—for example, benzyl penicillin IV or oral amoxicillin for S pneumoniae and flucloxacillin or clindamycin for S aureus.
20.4 Oral or intravenous?
A recent randomised controlled trial of the equivalence of oral amoxicillin versus IV benzylpenicillin in 252 children admitted to hospital with community acquired pneumonia showed no difference in duration of illness or complications.165 Oral antibiotics should be given provided oral fluids are tolerated.
20.5 Antibiotic choice for severe or complicated pneumonia?
Children who are severely ill with pneumonia complicating influenza should have a second agent which provides good cover for Gram positive organisms added to the regime (for example, clarithromycin or cefuroxime) and the drugs should be given intravenously to ensure high serum and tissue antibiotic levels.
21 ACKNOWLEDGEMENTS
Many people have helped with the preparation of these guidelines and our thanks go to them. In particular we would like to thank Dr Kevin Mortimer for expertly coordinating the reference database; Dr David Boldy, former Chairman, and Dr Norman Johnson, current Chairman of the British Thoracic Society Standards of Care Committee; Mrs Sheila Edwards, Chief Executive of the British Thoracic Society for support and advice; Dr Claire Holt, Dr Minghzi Zhang and Dr Eri Papanikou for their help; Sir Alan Croft, Dr Clive Graham and Dr Anita Simonds for their comments.
Declaration of interests: The committee members fulfilled the requirements of the British Thoracic Society regarding personal declaration of interests. Declaration of Interest forms were updated annually by committee members and the contents submitted to the British Thoracic Society Standards of Care Committee. These are available for inspection on request from the Chairman of this Committee.
Affiliations and addresses of committee members:
British Thoracic Society. Dr Wei Shen Lim, (Chairman and Editor), Consultant Physician, Nottingham University Hospitals; Dr Graham Douglas, Consultant Physician in Respiratory Medicine and Infection, Aberdeen Royal Infirmary; Dr David Honeybourne, Consultant Physician, Heartlands Hospital, Birmingham; Professor John Macfarlane, Consultant Physician, Nottingham University Hospitals; Dr Mark Woodhead, Consultant Physician, Manchester Royal Infirmary.
British Infection Society. Professor Robert Read (Lead), Professor of Infectious Diseases, Sheffield University; Dr Nick Beeching, Royal Liverpool University Hospital; Professor Karl Nicholson, Professor of Infectious Diseases, University of Leicester.
Department of Health. Dr Barbara Bannister, Consultant in Infectious Diseases and Director of the High-Security Infectious Diseases Service, Royal Free Hospital; Dr Jane Leese, Senior Medical Officer, Department of Health.
Health Protection Agency. Dr Robert C George, Director, Respiratory and Systemic Infection Laboratory, Health Protection Agency Centre for Infections; Dr Jonathan S Nguyen-Van-Tam, Consultant Epidemiologist, Respiratory Disease Department, Health Protection Agency Centre for Infections.
Paediatric Group. Dr Anne Thomson (Lead), Consultant in Paediatric Respiratory Medicine, John Radcliffe Hospital, Oxford; Dr Ekundayo Ajayi-Obe, Consultant Paediatrician, Hammersmith Paediatric Ambulatory Unit, Hammersmith Hospital; Dr Nicola Coote, Consultant Paediatrician, Hammersmith Paediatric Ambulatory Unit, Hammersmith Hospital; Dr Anthony Harnden, General Practitioner and University Lecturer, Department of Primary Care, University of Oxford; Dr Paul Heath, Senior lecturer in Paediatric Infectious Diseases and Hon Consultant, St George’s Hospital Medical School; Dr Sheila Mckenzie, Consultant Paediatrician, Queen Elizabeth Children’s Services, Royal London Hospital.
Primary Care Group. Professor Paul Little (Lead), Professor of Primary Care Research, University of Southampton; Professor Chris Butler, Professor of Primary Care Medicine, Cardiff University; Professor Tom Fahey, Head Tayside Centre for General Practice; Dr Douglas Fleming, Director Birmingham Research Unit of the Royal College of Practitioners; Dr Nick Francis, Medical Research Council Health Services Fellow, Department of General Practice, Cardiff University.
Societies and colleges approached directly for comments: British Geriatrics Society, British Society of Antimicrobial Chemotherapy, Faculty of Accident and Emergency, Intensive Care Society, Royal College of General Practitioners, Royal College of Nursing, Royal College of Paediatrics and Child Health, Royal College of Physicians.
APPENDICES
Appendix 10 Clinical features of avian influenza A (H5N1) infection in humans
The first recorded instance of human infection by avian influenza H5N1 occurred in May 1997 in Hong Kong. The first patient was a 3 year old child who presented initially with symptoms of fever, sore throat and abdominal pain. He later developed Reye’s syndrome, acute respiratory distress syndrome, multi-organ failure and eventually died.166 A total of 18 persons were subsequently infected before the outbreak ended in December 1997.126,167 Half the patients were aged 18 years and below and only two were aged over 50 years. Abdominal symptoms, such as diarrhoea, vomiting and abdominal pain, were described in 10 (56%) patients. Eleven (61%) had a severe illness characterised by pneumonia occurring within 14 days of symptom onset, lymphopenia, deranged liver function tests and a high mortality (six (55%) of 11 patients with pneumonia). Secondary bacterial infections were not identified as the cause of the pneumonias.
The most recent human outbreak of influenza A (H5N1) infection began in December 2003. The clinical features of hospitalised patients infected by the re-emergent avian influenza A (H5N1) in 2004 were similar to those described in patients in 1997 (table A10.1) Children and young adults were the main groups affected. Gastrointestinal symptoms were common. The presence of lymphopenia and deranged liver function tests was again associated with a poorer prognosis.125
Since December 2003, over 150 cases had been reported to the World Health Organization.168 The mortality rate among hospitalised patients has been generally high (>40%). Death has occurred an average of 10 days after the onset of illness and most patients have died of progressive respiratory failure.
There has been a review of avian influenza A (H5N1) infection in humans up until September 2005.55 Updated information can be found at http://www.who.int/csr/disease/avian_influenza/en/.

Pandemic influenza: initial management of adults referred to hospital.

Pandemic influenza: initial investigations for adults referred to hospital.
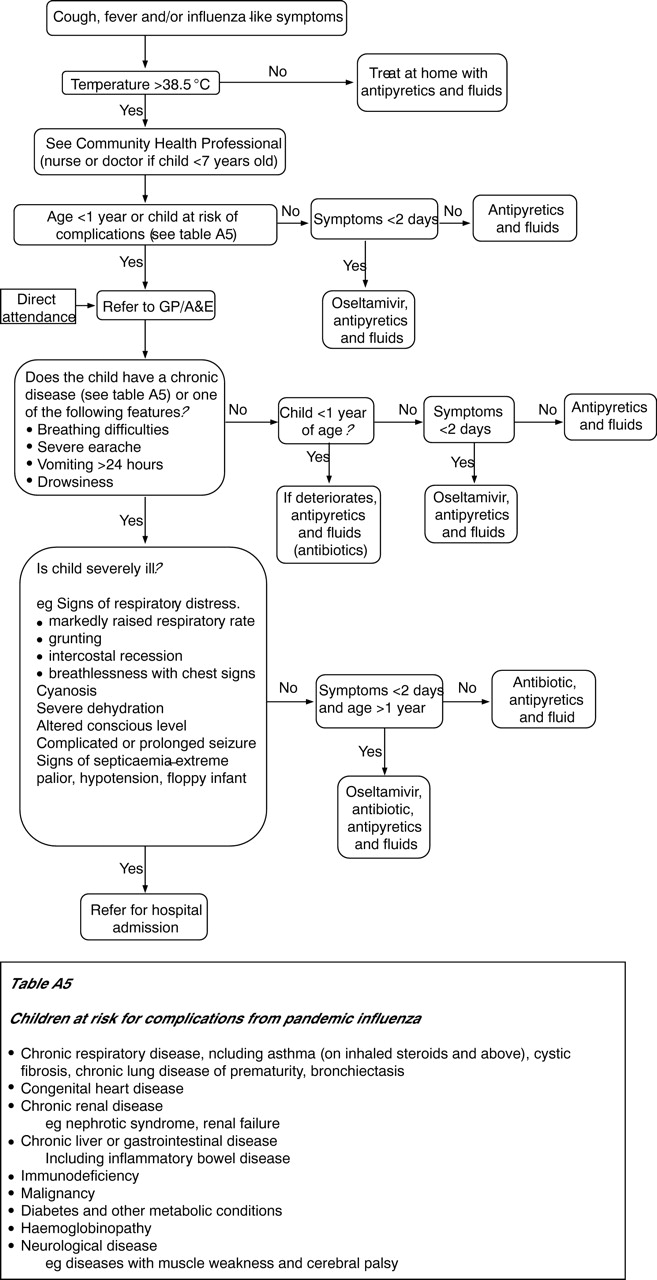
Pandemic influenza: initial assessment and management of children.

Pandemic influenza: management of children referred to hospital.
International phases and their significance for the UK
Patients at high risk of influenza-related complications*
Pandemic influenza: antibiotic doses for children
Paediatric respiratory distress severity assessment
Antiviral treatment: indications, doses and side effects

{kind=link}
{kind=link}
{kind=link}
{kind=link}
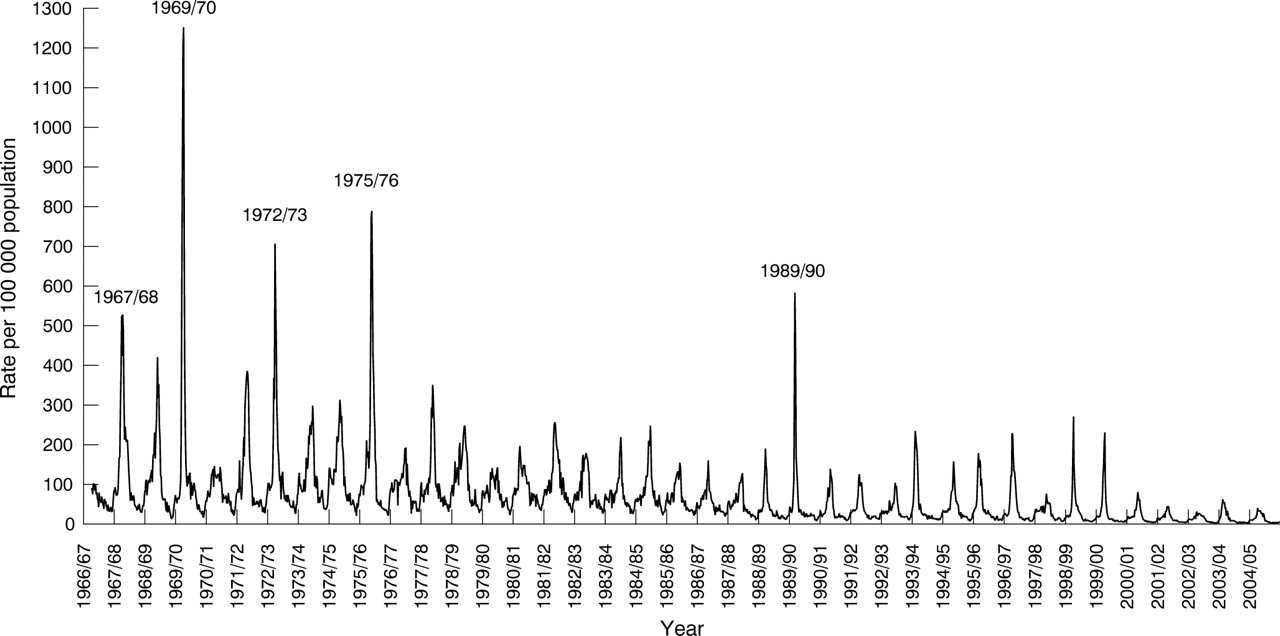{kind=link}
Royal College of General Practitioners’ index for influenza and influenza-like illness, 1966 and 2005 (year marked at start of season, that is, week 40 (October)).
Table A General investigations
(A) Range of possible excess deaths based on various permutations of case-fatality rates and clinical attack rates for England and Wales
(B) Range of possible excess deaths based on various permutations of case-fatality rates and clinical attack rates for the UK
Estimated burden of illness attributable to pandemic influenza over the entire pandemic based on a 25% clinical attack rate and illustrative case hopitalisation and case-fatality rates of 0.55% and 0.37% respectively
Demand for Health Care Contacts by primary care unit: weekly totals for the number of new clinical cases, and thus potential demand for Heath Care Contacts, per 100 000 population, and per Primary Care Trust (PCT), community pharmacy, GP practice or GP list of various sizes (see footnote for definition of “small”, “medium” and “large” as they are used in the table)
Complications associated with influenza infection in adults
The most common underlying conditions in children admitted to hospital, Texas 1998–99.68
Complications of influenza in children
Severity assessment used to determine the management of influenza-related pneumonia in patients in the community (CRB-65 score)
Adult and child dosages of oseltamivir
Antibiotic management in adults with influenza managed in the community
Empirical antibiotic treatment regimens for adults with pneumonic and non-pneumonic lower respiratory tract infections (including exacerbations of COPD and acute bronchitis) complicating influenza managed in the community
Severity assessment used to determine the management of influenza-related pneumonia in patients admitted to hospital (CURB-65 score)
Antiviral agents for influenza
Neuraminidase inhibitors in the treatment of adults with community acquired influenza: summary of trial data
Side effects of oseltamivir
Preferred and alternative initial empirical antibiotic treatment regimens and parenteral to oral switch regimens for pneumonic and non-pneumonic lower respiratory tract infections complicating influenza managed in hospital
Recommended therapy of most likely microbiologically defined causes of pneumonia complicating influenza (local specialist advice should always be sought)
REFERENCES
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Supplementary materials
IMPORTANT ERROR: Appendix 3, page i37. After the question "Does the patient have pneumonia?", the flow chart incorrectly directs the reader down the left side for the management if the answer is yes, and down the right side if the answer is no. These should be the opposite way around. A corrected pdf of this flow chart is posted here.
Files in this Data Supplement: