Article Text

Abstract
Background:0 Primary antibody deficiency disorders are a heterogeneous group of disorders, which are treated by regular infusions of immunoglobulin. Despite replacement treatment, patients remain susceptible to infection. Effective management of infections is necessary to prevent the complications of chronic infection.
Aims: This retrospective survey of clinical practice examined the management of infections in patients who receive immunoglobulin replacement for immune deficiency.
Methods: Patients who received immunoglobulin replacement treatment in Newcastle during the year 2000 were identified. Medical records were reviewed. Basic clinical information and details of immunoglobulin replacement treatment were recorded. Episodes of infection were defined by documented symptoms, signs, or investigation results, and by the prescription of an antibiotic course. Details of episodes of infection and antimicrobial treatment were recorded.
Results: Thirty seven patients received immunoglobulin replacement during 2000. There were 101 episodes of infection. There was no correlation between the frequency of infection and the IgG trough value. Respiratory tract infections were most common (71 of 101). Where documented, 80% of infections were associated with clinical signs, 21% with pyrexia, and 64% with a raised C reactive protein value. Microbiological culture was performed in 30% of infections. Antimicrobial treatment was instituted along “best guess” lines in 99 of 101 episodes of infection.
Conclusions: Management of respiratory tract infections represents the largest problem in antibody deficient patients. Greater use of microbiological culture might allow more effective prescription of antimicrobial treatment. The generation of treatment guidelines and improved communication with general practitioners could improve the management of all episodes of infection.
- infection
- antibody deficiency
- hypogammaglobulinaemia
- CRP, C reactive protein
- CVID, common variable immune deficiency
- XLA, X linked agammaglobulinaemia
Statistics from Altmetric.com
Antibody deficiency may occur in a range of immunological disorders. The principle presentation is with recurrent infection, particularly of the respiratory tract.1 Immunoglobulin replacement treatment is central to the management of antibody deficiency. Intravenous or subcutaneous immunoglobulin preparations are administered at two to three weekly intervals, aiming to achieve trough IgG values within the normal range.2 Clinical trials have shown that immunoglobulin replacement treatment with an IgG trough value greater than 5 g/litre results in improved parameters of lung function and reduced infection rates.3
Despite immunoglobulin replacement treatment, patients with antibody deficiency remain at risk of developing acute “breakthrough” or chronic infections.4 Effective management of such infections with prompt and aggressive antimicrobial treatment is crucial to avoid associated morbidity and mortality. Additional therapeutic approaches, such as physiotherapy, prophylactic antibiotics, or surgery, should be considered in the management of recurrent or chronic infections.5
“Despite immunoglobulin replacement treatment, patients with antibody deficiency remain at risk of developing acute breakthrough or chronic infections”
There are few published data on the incidence and optimal management of breakthrough infections in patients receiving immunoglobulin replacement treatment. This survey of clinical practice aimed to quantify the clinical features and management of such infections.
MATERIALS AND METHODS
Adult patients with a current diagnosis of antibody deficiency who were treated with immunoglobulin replacement in Newcastle upon Tyne during the year 2000 were identified. All available medical records were reviewed. For each patient, basic clinical details for the year 2000 were recorded. These included age, sex, diagnosis, details of immunoglobulin replacement treatment, and trough IgG values.
For the purposes of our survey, an episode of infection was defined as a complex of symptoms, signs, and investigation results, which led to an antibiotic course being prescribed. Episodes included both acute infections and exacerbations of chronic infections. These episodes were treated by hospital clinicians, by general practitioners, and by patients themselves. Patients were not interviewed in the course of our study; only episodes of infection described in the notes were recorded. All episodes of infection that led to an antibiotic course being started between 1 January 2000 and 31 December 2000 were included.
Clinical details were recorded for each episode of infection. These details included physical signs, symptoms, temperature measurements, C reactive protein (CRP) concentration, details of microbial culture performed, recent trough IgG values, and antimicrobial treatment.
RESULTS
A total of 37 patients received immunoglobulin replacement treatment in Newcastle upon Tyne in 2000. The mean age of patients undergoing immunoglobulin replacement treatment was 40.4 years (range, 16–71). There were 23 female and 14 male patients. Diagnoses were common variable immune deficiency (CVID; 27), X linked agammaglobulinaemia (XLA; four), IgA deficiency (one), specific antibody deficiency (one), hyper-IgM syndrome (one), hyper-IgE syndrome (one), chronic lymphocytic leukaemia (one), and antiphospholipid syndrome with specific antibody deficiency (one).
Immunoglobulin replacement treatment
Preparations used for immunoglobulin replacement treatment include Sandoglobulin, Octagam, Vigam Liquid, Alphaglobin, Flebogamma, Scottish National Blood Transfusion Service immunoglobulin, and Gammabulin. Immunoglobulin treatment was administered by the intravenous route in 36 of 37 patients and the subcutaneous route in one of 36 patients. Infusions of immunoglobulin took place in the hospital outpatient department in 16 of 37 patients and at home in 21 of 37 patients.
The mean trough IgG value for all patients was 9.15 g/litre (range, 5.67–12.5). Infusions were missed by three of 16 patients who attend the hospital outpatient department. One patient missed a single infusion. One patient missed nine successive infusions; no IgG trough values are available for this period. One patient attended intermittently and missed seven infusions; this was the single patient with IgG trough values below 6 g/litre.
Episodes of infection
In the year 2000, 101 episodes of infection were recorded among the 37 patients receiving immunoglobulin replacement treatment. Seven patients remained free of infection throughout the year. Linear regression analysis was performed to assess the relation between trough IgG values and the number of infections, and fig 1 shows the results. The correlation between trough IgG values and the frequency of infection was not significantly different from zero (r2 = 0.027, p = 0.35). Infection was documented and managed by the general practitioner in 36 of the 101 episodes and by hospital medical staff in 60 of the 101 episodes. In five of the 101 episodes of infection, the patient initiated antimicrobial treatment and subsequently informed medical staff.
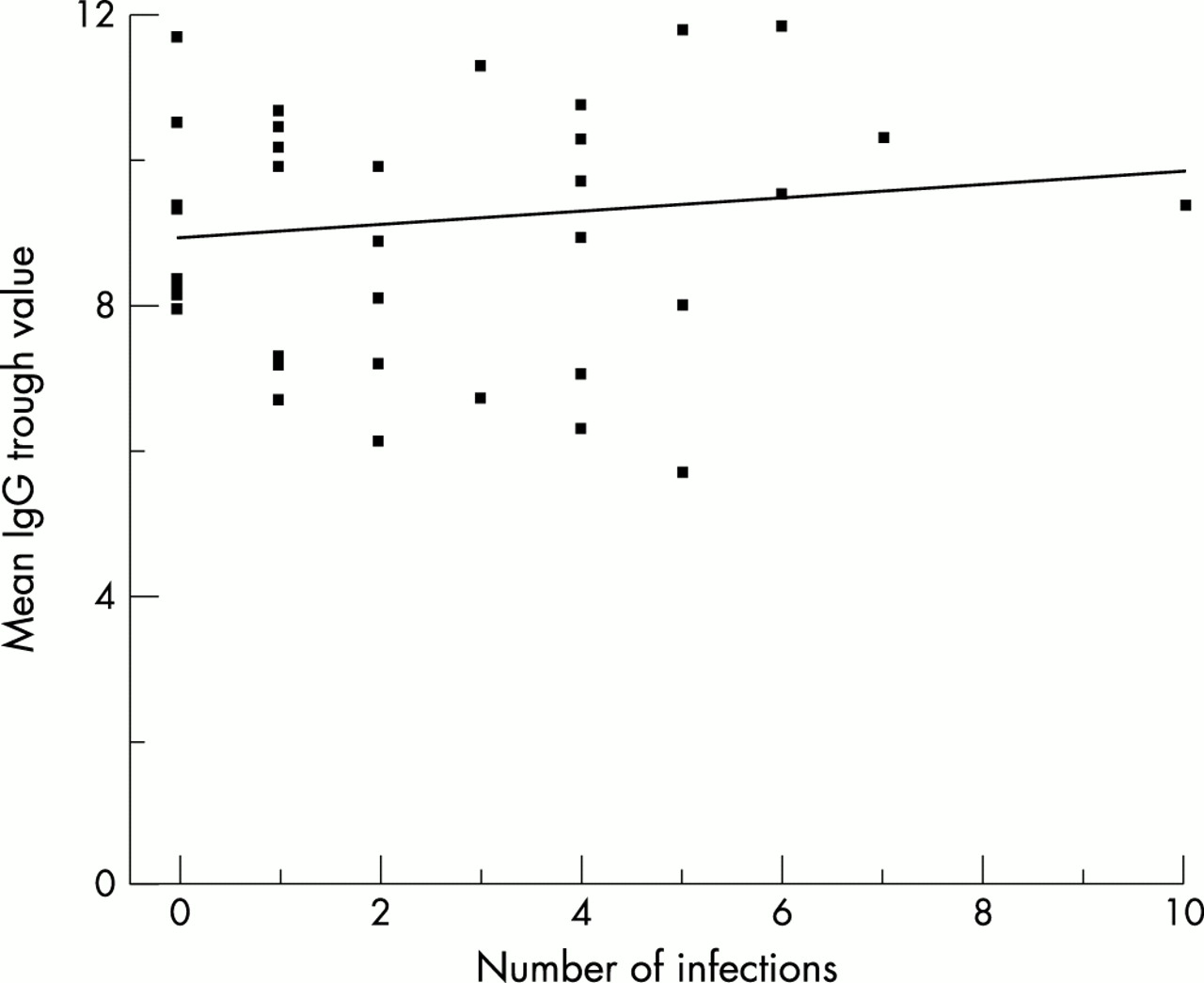
Linear regression analysis of number of infections versus mean trough IgG values in 37 patients receiving immunoglobulin replacement treatment.
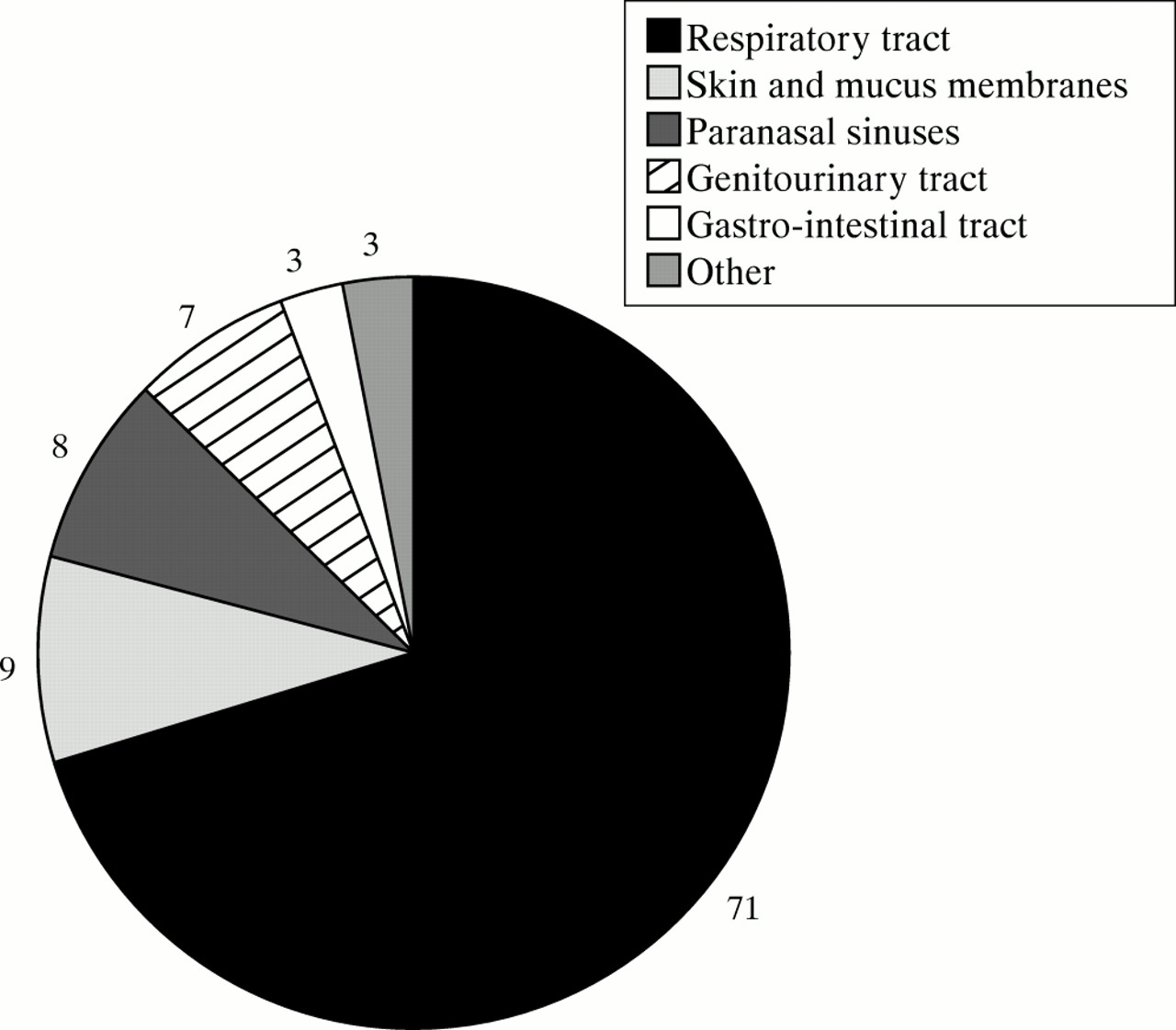
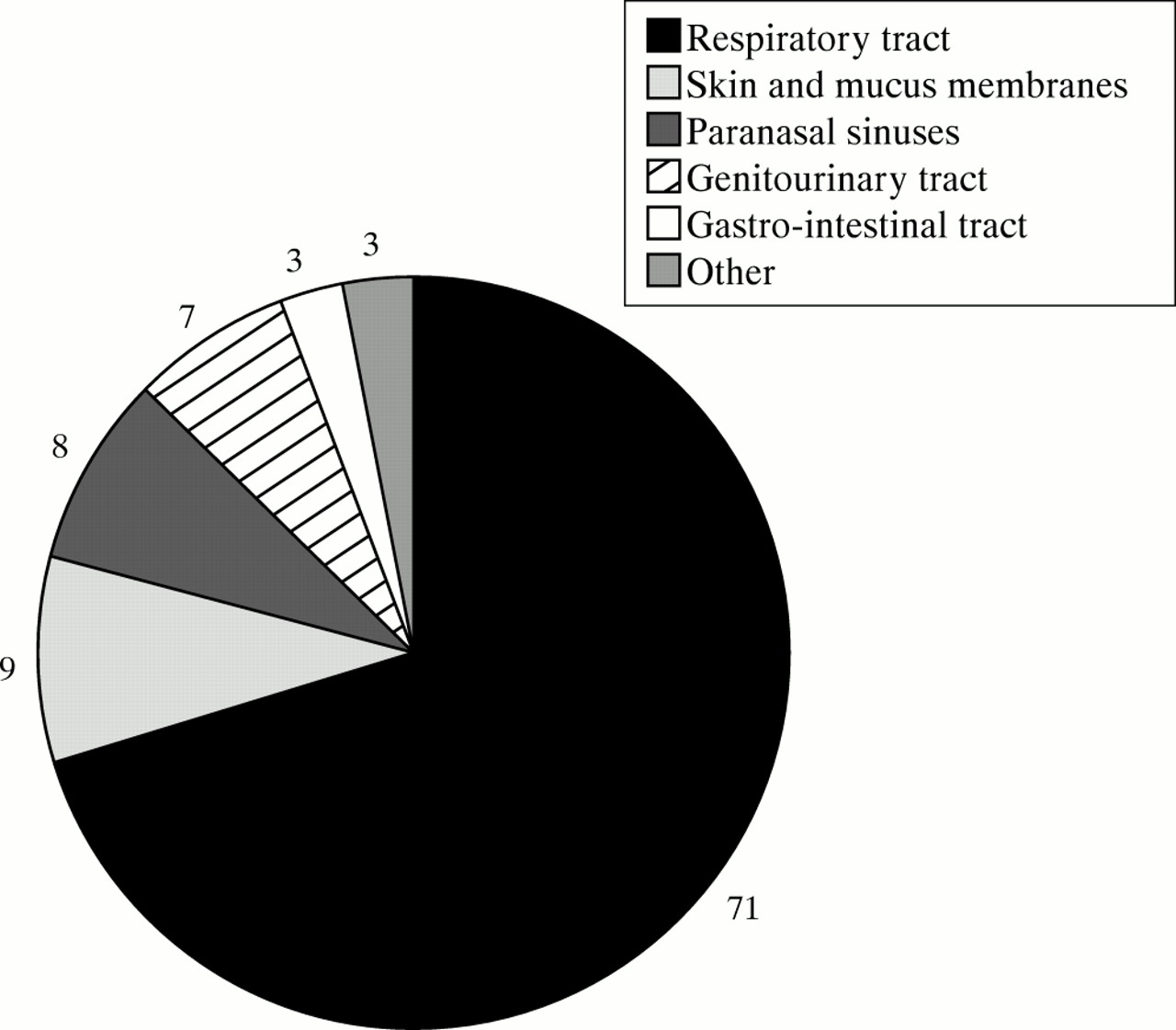
Figure 2 summarises the total numbers of each type of infection. The most common site of infection was the respiratory tract, accounting for 70% of all infections. Examination findings were documented in 51 of the 101 episodes of infection, and were positive in 80% of these cases. In contrast, temperature was documented in only 14 of the 101 episodes of infection. When temperature was documented, only 21% episodes of infection were associated with a temperature > 38°C. Interestingly, all patients with fever were admitted to hospital for treatment of their infection.
{kind=link}
{kind=link}
Types of infection in the 37 patients receiving immunoglobulin replacement treatment. The numbers of each type of infection are listed by each chart section.
The CRP value was measured and documented in 39 of the 101 episodes of infection. When CRP was documented, 25 episodes of infection were associated with a raised CRP concentration. The reference range for CRP in our laboratory is 0–5 mg/litre. The mean CRP value seen in episodes of infection was 37.9 mg/litre (range, 6–194). Outside defined episodes of infection, the mean CRP value was 6.85 mg/litre (range, 0–76). Ten patients had a mean CRP value of > 10 mg/litre. In four of the 10 patients, this mean CRP was skewed by a single high CRP concentration. In six of the 10 patients, this mean CRP value represented consistently raised CRP concentrations.
Table 1 details the range of clinical samples sent for culture and the pathogens isolated. Sputum samples were most often sent for microbiological culture; these were collected in 23 of 71 episodes of respiratory tract infection. Microbiological culture was performed equally for all types of infection, with the exception of sinusitis. A nasal swab was cultured in only one of eight episodes of sinusitis. The sensitivity of organisms to “best guess” blind antibiotic treatment was only assessed in seven samples. Fortunately, all these organisms were sensitive to the antibiotic being used and best guess treatment did not need to be altered.
Range of clinical samples sent for microbiological culture and range of pathogens cultured from each type of sample
In total, 111 courses of antimicrobial drugs were prescribed during the survey period. Twenty three different antimicrobial drugs were prescribed. Intravenous antibiotics were required in only two of the 101 episodes of infection. The duration of antibiotic treatment was documented in 56 of 111 courses. The mean duration of antibiotic treatment was 12 days (range, 3–28). Antimicrobial treatment was started without performing microbiological culture or before culture results were available in 99 of 101 episodes of infection. Where details of antibiotics were recorded, best guess treatment was generally appropriate to clinical findings in 98 of 99 of these episodes of infection. The most variable best guess treatment was for respiratory tract infections, for which azithromycin (19 courses), co-amoxiclav (16 courses), amoxycillin (12 courses), and ciprofloxacin (eight courses) were the most commonly used antibiotics.
DISCUSSION
The most common diagnosis was CVID, accounting for almost three quarters of all patients. The adequacy of immunoglobulin replacement treatment was assessed by serial measurement of IgG trough values. In our survey, all compliant patients receiving immunoglobulin replacement treatment had a preinfusion IgG > 6g/litre.
There were 101 infective episodes. The distribution was skewed—two individuals had more than seven episodes of infection in 2000. Analysis by simple linear regression showed no correlation between the number of infective episodes and IgG trough values. The two patients with IgA deficiency and selective antibody deficiency were excluded from this analysis because they had normal IgG values before immunoglobulin replacement treatment. Most clinical immunologists aim to achieve IgG trough values within the normal range. There is evidence that a higher trough value (> 8 g/litre) results in a lower infection rate in patients with XLA.6 No equivalent data exist for patients with CVID. Data from this limited cohort do not suggest that IgG trough values above 6 g/litre offer additional protection from infection. However, patients who have previously suffered more infections may receive larger doses of immunoglobulin replacement treatment.
Respiratory tract infections, including sinusitis, bronchitis, and pneumonia, were the most common type of infection. These constituted 78% of all episodes of infection identified during our study. Previous studies have shown that the respiratory tract is the most common site of infection in CVID, XLA, and chronic lymphocytic leukaemia.7–9 Respiratory tract infections in antibody deficient patients are commonly caused by encapsulated bacteria such as Streptococcus pneumoniae and Haemophilus influenzae, and less commonly caused by staphylococci and Pseudomonas aeruginosa.7 Sputum cultured during the period of study yielded a similar range of organisms from 17 of 23 samples; these included H influenzae, S pneumoniae, and P aeruginosa.
The associated features of the infections were documented to a variable extent. This largely represented a lack of communication between general practitioners and hospital clinicians when episodes of infection were managed in the community. Temperature was measured and documented in only 14% of episodes of infection. However, the two patients with a temperature > 38°C required hospital admission for intravenous antibiotic treatment. CRP concentrations were measured in 39% of episodes of infection. The mean CRP value was 37.9 mg/litre during episodes of infection, compared with 6.85 mg/litre outside episodes of infection. However, there was considerable overlap in the range of CRP concentrations that were observed in the presence or absence of infection. This overlap has important implications for the use of regular CRP values to assess chronic or recurrent infection.
Take home messages
-
Respiratory tract infections are the largest problem in antibody deficient patients
-
There was no correlation between the frequency of infection and the IgG trough value
-
Greater use of microbiological culture might allow more effective prescription of antimicrobial treatment
-
The generation of treatment guidelines and improved communication with general practitioners might improve the management of all episodes of infection
There is considerable concern about chronic/recurrent respiratory tract infections and the development of bronchiectasis. A national audit, performed between 1993 and 1996, identified bronchiectasis in 20% of patients with CVID and 12% of patients with XLA. The routine use of adequate immunoglobulin replacement after diagnosis has reduced the subsequent development of bronchiectasis from 77% of patients to 42% of patients.10 However, bronchiectasis may progress despite adequate immunoglobulin replacement. A prospective three year study using high resolution computerised tomography demonstrated silent progression of bronchiectasis in five of the 14 patients, all of whom were receiving intravenous immunoglobulin replacement treatment and had trough serum IgG concentrations of > 5 g/litre.11
“This survey of clinical practice allows local targets to be set for management of episodes of infection in antibody deficiency”
Chronic or recurrent infections may be monitored by means of symptom diaries and by the regular measurement of CRP concentrations. No formal symptom diaries were submitted for the period of survey. However, all patients had CRP values measured regularly. Raised CRP concentrations were seen in 10 patients outside episodes of infection. This was suggestive of unnoticed acute infection in four patients (an isolated raised CRP value on a background of normal CRP concentration), and chronic infection in six patients (continuously raised CRP values). Patients with unnoticed acute infection should be promptly assessed and antibiotic treatment instituted if required. Indicators of chronic infection allow changes to basic management, including physiotherapy, regular antibiotics, and the possibility of surgical resection of badly affected areas of the bronchial tree.12
Only five courses of antibiotic treatment were initiated by patients themselves. Little information is available about these episodes of infection. Because our survey depends on clinical records, it probably underestimated the number of patient managed episodes of infection. General practitioners and hospital clinicians differed in their management of infections. Lack of documented examination findings, temperature measurements, CRP values, and culture results may result largely from poor communication between these two groups. The consensus document suggested that patient held records would aid this communication.2 No such patient held records were available from the period of survey. Syndromes of antibody deficiency are very rare and unlikely to be encountered by most general practitioners.13 Protocols for the management of common infections might be helpful for these general practitioners.
This survey of clinical practice allows local targets to be set for management of episodes of infection in antibody deficiency. Several areas for improvement exist. Greater use of microbiological culture should be made. This will require more sputum samples and nasal swabs to be collected. Where best guess treatment is started, antibiotic sensitivity should be routinely assessed and antibiotics changed if required. Basic guidelines for the treatment of common infections should be agreed and circulated to general practitioners. Patients should be encouraged to record details of prescriptions from general practitioners. Additional therapeutic interventions should be sought in patients who suffered chronic/recurrent infections in 2000. The final target should be to reduce the number of infections for each patient in subsequent years.