Article Text

Abstract
Background: High C-reactive protein (CRP) and homocysteine levels are risk factors for cardiovascular disease. Some, but not all, previous studies have reported increased levels of CRP and homocysteine in patients with obstructive sleep apnoea syndrome (OSAS). A study was undertaken to investigate the levels of these factors in carefully selected patients with OSAS and matched normal controls.
Methods: CRP and homocysteine levels were measured in 110 subjects following polysomnography (PSG). Non-OSAS patients (group 1) were compared with two patient groups (mild/moderate OSAS (group 2) and severe OSAS (group 3)) group-matched for body mass index (BMI), and a fourth group of patients with severe OSAS who were more obese (group 4). All were free of other disease and similar in age, smoking habits and cholesterol levels. 50 suitable patients were commenced on continuous positive airway pressure (CPAP) treatment after PSG and 49 were reassessed 6 weeks later.
Results: CRP levels were similar in groups 1, 2 and 3 (median (interquartile range (IQR)) 1.11 (0.76–2.11) mg/l vs 1.82 (1.20–3.71) mg/l vs 2.20 (1.16–3.59) mg/l; p = 0.727, Kruskal-Wallis test), but were significantly higher in group 4 than in the other groups (5.36 (2.42–9.17) mg/l, p<0.05 by individual group comparisons). In multivariate analysis of all subjects, BMI was an independent predictor for CRP levels (β = 0.221; p = 0.006) but apnoea-hypopnoea index and other measures of OSAS were not. There was no difference in homocysteine levels between all four groups (p = 0.1). CPAP did not alter CRP (2.29 (1.32–4.10) vs 2.84 (1.13–5.40) mg/l; p = 0.145) or homocysteine levels (8.49 (3.66) vs 9.90 (4.72) μmol/l; p = 0.381).
Conclusion: CRP and homocysteine levels are not associated with OSAS severity in men but CRP is independently associated with obesity.
- AHI, apnoea-hypopnoea index
- BMI, body mass index
- CPAP, continuous positive airway pressure
- CRP, C-reactive protein
- DI, desaturation index
- ESS, Epworth Sleepiness Scale
- OSAS, obstructive sleep apnoea syndrome
- PSG, polysomnography
- TNFα, tumour necrosis factor α
- TST, total sleep time
Statistics from Altmetric.com
- AHI, apnoea-hypopnoea index
- BMI, body mass index
- CPAP, continuous positive airway pressure
- CRP, C-reactive protein
- DI, desaturation index
- ESS, Epworth Sleepiness Scale
- OSAS, obstructive sleep apnoea syndrome
- PSG, polysomnography
- TNFα, tumour necrosis factor α
- TST, total sleep time
Obstructive sleep apnoea syndrome (OSAS) is a highly prevalent disorder affecting about 4% of adults,1 and is associated with repetitive episodes of transient oxygen desaturation during sleep. The predominant physical morbidity of the disorder is cardiovascular, and OSAS is an independent risk factor for a number of cardiovascular diseases, particularly systemic arterial hypertension2,3 but also coronary artery disease, congestive cardiac failure and cerebrovascular events.4 Treatment with nasal continuous positive airway pressure (nCPAP) decreases cardiovascular morbidity and mortality.5,6 However, the mechanisms underlying cardiovascular complications in OSAS remain unclear.
In recent years the identification of novel cardiovascular risk factors has significantly enhanced our understanding of the development of cardiovascular diseases in general and greatly improved risk stratification. These include factors of haemostasis and thrombosis such as homocysteine, fibrinogen and lipoprotein-a, and inflammatory markers such as selectins P and E, cellular adhesion molecules, tumour necrosis factor alpha (TNFα), interleukin 6 (IL6) and C-reactive protein (CRP).7 Of these, markers such as homocysteine and CRP have attracted specific attention as assays to measure their levels are widely available in general hospitals rather than specific research laboratories. In particular, CRP, an acute phase reactant, has been closely linked to cardiovascular diseases. It is the prototypic marker of inflammation and numerous prospective studies have shown that an increased level of CRP is a strong predictor of future cardiovascular risk.8,9,10 On the other hand, mildly raised levels of the amino acid homocysteine in the plasma have been shown to correlate with the incidence of premature coronary artery disease, peripheral vascular disease and stroke.11,12
Whether or not CRP and homocysteine levels are increased in patients with OSAS is still under debate. Some reports have identified increased levels of CRP in these patients13–18 while others have not.19,20 Also unclear is the impact of CPAP therapy on CRP levels, with one study reporting a favourable outcome14 and others finding no significant change in levels with effective CPAP therapy.19,21 A major pitfall of evaluating CRP levels is the fact that this marker is directly associated with obesity,22,23 and many previous reports have been influenced by small numbers, inadequately matched populations, particularly for body mass index (BMI), and inclusion of patients with established cardiovascular or metabolic diseases.
Similarly, the role of plasma homocysteine levels in OSAS is unclear, with some studies reporting higher levels only in OSAS patients suffering from pre-existing cardiac disease24,25 and other reports identifying homocysteine levels to be independently associated with OSAS.18,26 Only one study of 12 patients with OSAS has evaluated the effect of CPAP therapy after a variable time point and found a reduction in homocysteine levels.27 However, many of the reports on homocysteine in OSAS may have been influenced by similar methodological limitations as for CRP.
We performed a prospective controlled study in tightly selected groups of patients with OSAS and control subjects to evaluate the relationship of OSAS with CRP and homocysteine levels, with a specific focus on the impact of obesity as a possible confounder.
METHODS
Subjects
Consecutive men with suspected OSAS based on symptoms such as heavy and loud snoring, witnessed apnoeas and/or daytime sleepiness and no other medical disorder were considered for the study, which was approved by the St Vincent’s University Hospital ethics committee. Also recruited from the general population outside the hospital environment were normal men who were group-matched for age and BMI to the patient cohort. Based on our general sleep clinic population and the requirement to be free of all co-morbidity, we predicted that we needed healthy controls between 30 and 40 years and a BMI between 28 and 34 kg/m2. Over the course of the study, the demographic data of the patient population were carefully monitored to allow us to make slight adjustments in the criteria for the control population. These criteria were set purely on demographic variables, and analysis of data was made independently and in a blinded fashion.
All subjects gave written informed consent and no subject fitting the inclusion criteria refused participation. Each subject underwent clinical assessment, testing for full blood count, liver and kidney function, cardiac enzymes including troponin T and lipid profile. Furthermore, determination of vitamin B12 and folate were done in all subjects to ensure that low levels of these vitamins did not represent potential secondary causes for higher homocysteine concentrations. Each subject also completed the Epworth Sleepiness Scale (ESS) and supine blood pressure was measured while awake at least three times during the daytime. Overnight polysomnography (PSG) was performed as previously described.28 Apnoeas were defined as a complete cessation of airflow for at least 10 s and hypopnoeas as a reduction of respiratory signals for at least 10 s associated with oxygen desaturation of ⩾4% and/or arousal. Sleep studies were performed in the sleep laboratory and supervised throughout by an experienced sleep technician.
CPAP treatment
Fifty suitable subjects with moderate or severe OSAS who had agreed to possible CPAP therapy before the diagnostic sleep study initiated nasal CPAP therapy within 1 week after PSG. One patient dropped out due to intolerance of CPAP. The remaining 49 patients underwent repeat of their sleep study after 6 weeks of treatment. All were evaluated for symptoms and side effects, and objective compliance data were downloaded from the devices.
CRP and homocysteine measurements
Venous blood samples were obtained from all subjects while fasting at the same time (07:00 hours) following initial PSG and again from patients after 6 weeks of CPAP treatment and serum or plasma was stored at –80°C until further analysis. Serum for CRP levels was measured using a nephelometric technique which measures the light scattered onto complexes of samples containing CRP and monoclonal antibodies to CRP.
For homocysteine determinations, blood samples were collected into EDTA-containing specimen tubes and immediately placed on ice. Concentrations were determined by fluorescence polarisation immunoassay on an Abbott IMx analyser.
Statistical analysis
The expected difference in CRP and homocysteine levels between groups which might be clinically important and the pooled standard deviations were specified on the basis of previous published studies. The required sample size to detect a difference of 3.2 mg/l in CRP levels and 7.5 μmol/l in homocysteine levels between groups of different apnoea/hypopnoea index (AHI; which is the comparison of interest) with 90% power at the 5% significance level was 27 subjects in each group.
The baseline characteristics of the subjects and CRP and homocysteine levels are expressed as mean (SD) or median (interquartile range, IQR) depending on their distribution. The data were compared using one-way analysis of variance (ANOVA) or the Kruskal-Wallis test with post hoc pairwise comparison to assess for differences between groups for independent samples and the paired t test or Wilcoxon signed rank test for paired samples. Categorical variables were compared using the χ2 test. In addition, levels of cardiovascular risk factors among the groups were evaluated by ANOVA or the Kruskal-Wallis test. Pearson’s or Spearman’s correlation analysis was used to assess the correlation between CRP or homocysteine, respectively, with baseline and PSG variables. To identify potential independent predictors of CRP and homocysteine levels, a stepwise backward linear regression model was used with CRP or homocysteine as the dependent variables and age, BMI, smoking status, total cholesterol, triglyceride, LDL-cholesterol, HDL-cholesterol, ESS, AHI, desaturation index (DI), basal oxygen saturation (Sao2), min Sao2 and percentage total sleep time (TST) <90% as independent factors with group selection as covariates. To rule out a possible confounding effect of the non-BMI-matched group on the results of the CRP predictors, a separate general linear model to assess for analysis of covariance (ANCOVA) was employed with the different groups as factors and BMI as covariate. Statistical analysis was performed using a commercial software package (SPSS V.11, Chicago, Illinois, USA).
RESULTS
Subjects
The baseline characteristics of the study population are shown in table 1. The subjects were classified into three groups according to their apnoea/hypopnoea frequency as non-OSAS (AHI ⩽5; group 1), mild to moderate OSAS (AHI >5–⩽30; group 2) or severe OSAS (AHI >30; group 3). The non-OSAS group consisted of 22 normal control subjects recruited from the general population who did not complain of habitual snoring or excessive daytime sleepiness (ESS 5 (2)) and eight individuals with clinical features of OSAS including significant excessive daytime sleepiness (ESS 16 (3)) and snoring but who had no objective findings of sleep-disordered breathing on PSG studies. Also included was a fourth group of patients with severe OSAS (AHI >30) but who were significantly more obese (group 4). The four groups were similar with regard to age, smoking status, total cholesterol, LDL-cholesterol, HDL-cholesterol, folate and vitamin B12 levels. Non-OSAS subjects had a significantly lower triglyceride level than all other groups. The BMI and neck size of the subjects in group 4 were significantly higher than in all the other groups, but there was no difference in BMI between the remaining three groups. No subject had clinical evidence of any other medical disorder and the detailed biochemical profile—including liver and renal function, cardiac enzymes and resting electrocardiogram—were within normal limits in all subjects. No individual had increased troponin T levels.
Baseline characteristics of study population
No subject was taking any regular medication. AHI and oximetry data as well as ESS were significantly different between the groups. All subjects except one individual in the very obese group had daytime awake oxygen saturation >92%. Fifty suitable patients with moderate or severe OSAS who had agreed to possible CPAP treatment before the diagnostic sleep study initiated nasal CPAP therapy within 1 week after PSG. Their mean (SD) age was 40 (8) years and their BMI was 34 (6) kg/m2. One patient dropped out due to intolerance of CPAP. Following 6 weeks of CPAP therapy in the remaining 49 patients, AHI fell from a median (IQR) value of 37 (14–73) to 7 (4–11) (p<0.001 compared with pre-CPAP levels), DI fell from 38 (15–67) to 5 (2–8) and all had Sao2 levels above 90% during sleep (% total sleep time <90% 0 (0–0)%; min Sao2 93 (91–94)%). Mean (SD) ESS improved from 15 (5) to 7 (5) (p<0.001) and daytime blood pressure from 134/84 (17/11) to 127/80 (15/10) (p = 0.01). Objective recordings from CPAP machines revealed a mean (SD) nightly compliance of 4.6 (1.3) h.
CRP levels
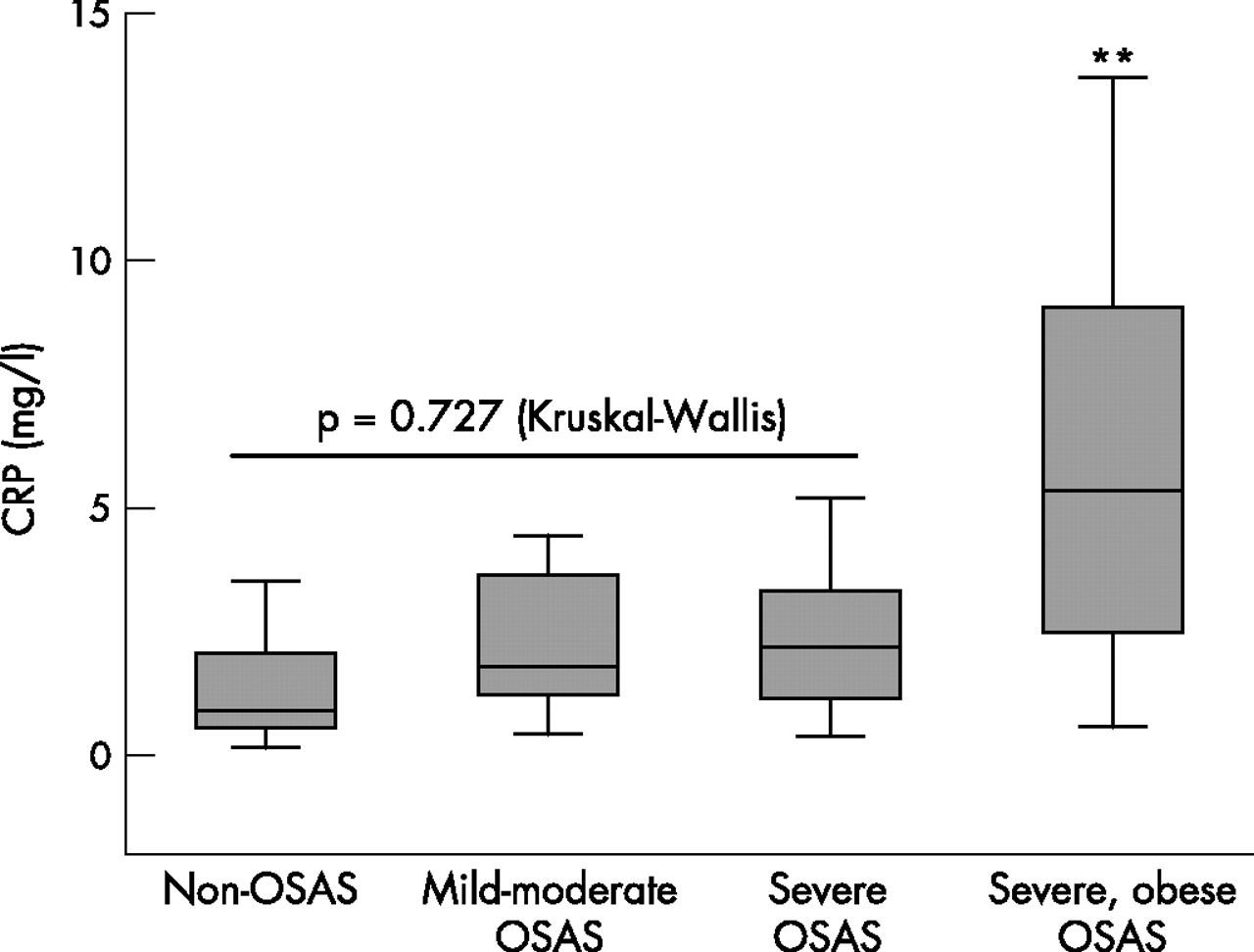
There were no significant differences between median (IQR) CRP levels in the non-OSAS group (group 1; 1.11 (0.76–2.11) mg/l), the group with mild to moderate OSAS (group 2; 1.82 (1.20–3.71) mg/l) and the severe OSAS/BMI-matched group (group 3; 2.20 (1.16–3.59) mg/l) (p = 0.727, Kruskal-Wallis test). Levels were higher in the severe OSAS/obese group (group 4; 5.36 (2.42–9.17) mg/l) than in all other groups (p<0.001 vs group 1, p = 0.006 vs group 2, p = 0.005 vs group 3) (fig 1).
{kind=link}
Serum level of high sensitivity C-reactive protein (CRP) in subjects without obstructive sleep apnoea syndrome (OSAS), with mild to moderate OSAS, severe OSAS/BMI-matched group and severe OSAS/obese group. Boxes represent values within the interquartile range, whiskers represent the data range, and lines across the boxes represent the median values. Kruskal-Wallis represents the comparison of non-OSAS, mild to moderate OSAS and severe BMI-matched groups (groups 1–3). **Statistically significant difference between the more obese severe OSAS group (group 4) when compared with groups 1–3 by individual group comparison (p<0.05 for all comparisons).
As the patients with severe OSAS and a higher BMI had significantly worse PSG variables than the severe OSAS BMI-matched group, we adjusted both groups for AHI and oximetry variables by excluding nine subjects in the BMI-matched group who had an AHI between 30 and 40/h. These two groups were then similar in demographic and also PSG parameters. BMI was significantly different (33.7 (2.5) vs 42.5 (4.8) kg/m2; p<0.001) and CRP levels remained higher in the very obese group (3.01 (1.71) vs 5.66 (3.89) mg/l, p = 0.027).
Spearman’s correlation analysis showed that CRP levels correlated positively with BMI (r = 0.484, p<0.001), neck size (0.413, p<0.001), ESS (r = 0.295, p = 0.002), total cholesterol (r = 0.194, p = 0.048) AHI (r = 0.423, p<0.001), DI (r = 0.456, p<0.001) and %TST <90% (r = 0.421, p<0.001) and negatively with the basal Sao2 (r = –0.312, p<0.001) and minimal Sao2 (r = –0.414, p = 0.001). The CRP level did not show any significant correlation with age, smoking status, HDL-cholesterol, LDL-cholesterol and triglyceride level.
Stepwise backward linear regression analysis including all subjects identified the BMI as the strongest and the total cholesterol as a further independent predictor of CRP level (table 2).
Stepwise multiple regression analysis of the relationship between C-reactive protein (CRP) levels and various independent variables
To assess the potential impact of neck size rather than general obesity, we substituted the BMI for neck size in the multivariate analysis. There was a strong correlation between these two variables (r = 0.781, p<0.001). In this second multivariate analysis, neck size was the strongest (β = 0.405, p = 0.003) and cholesterol a further independent predictor (β = 0.235, p = 0.020), which was similar to the model described in table 2.
As group 4 represented patients with a significantly higher BMI which could have potentially influenced the results, we performed an ANCOVA to assess for a possible confounding effect. As shown in table 3, the different groups did not show a significant relationship with CRP levels.
Analysis of covariance to assess the effect of the different groups and body mass index (BMI) on C-reactive protein (CRP) levels
Homocysteine levels
Homocysteine levels in all the patient and control groups were within the normal laboratory reference range of 5–15 μmol/l. No significant difference in homocysteine levels was detected between non-OSAS subjects (8.30 (2.12) μmol/l), those with mild to moderate OSAS (7.16 (1.58) μmol/l), BMI-matched subjects with severe OSAS (8.40 (2.98) μmol/l) and obese subjects with severe OSAS (9.16 (4.87) μmol/l; p = 0.1, ANOVA).
Pearson’s correlation analysis only identified a significant relationship between homocysteine levels and HDL-cholesterol (r = –0.212, p = 0.028) which remained independently associated in stepwise multiple linear regression analysis (table 4). There was no correlation between homocysteine and age, smoking status, BMI, total cholesterol, triglyceride, LDL-cholesterol, ESS and all PSG variables.
Stepwise multiple regression analysis of the relationship between homocysteine levels and various independent variables
Effect of CPAP therapy on CRP and homocysteine levels
Patients with OSAS who were commenced on nasal CPAP therapy after their diagnostic PSG were re-evaluated 6 weeks later. There was no change in BMI, no other diseases were diagnosed or medications introduced. Treatment with nasal CPAP did not alter CRP levels (2.29 (1.32–4.10) mg/l vs 2.84 (1.13–5.40) mg/l; p = 0.145) or homocysteine levels (8.49 (3.66) μmol/l vs 9.90 (4.72) μmol/l; p = 0.381).
DISCUSSION
In this study we have identified an independent relationship between CRP levels and BMI, but not with the severity of sleep disordered breathing in male subjects who were free of cardiovascular disease. Homocysteine levels were not determined by OSAS severity or demographic variables. Effective CPAP therapy of 6 weeks duration had no effect on either CRP or homocysteine levels.
OSAS is associated with the development of cardiovascular diseases, particularly systemic arterial hypertension2,3 but also coronary artery disease, congestive cardiac failure and stroke.4 CPAP therapy significantly reduces cardiovascular morbidity and mortality.5,6 The pathophysiology underlying cardiovascular complications in OSAS remains unclear. The pathogenesis is probably multifactorial, and potential mechanisms include sympathetic excitation, inflammation, vascular endothelial dysfunction and metabolic dysregulation. CRP levels are widely recognised as potent independent predictors of future cardiovascular events in apparently healthy subjects,8 as well as in subjects with known cardiovascular disease.9,10 Moreover, recent data suggest a direct active role in the pathogenesis of atherosclerosis.29 CRP is mainly produced in the liver in response to interleukin-6 (IL6). Adipose tissue is a potent source of IL6 production which leads to increased CRP levels in obese subjects.22,23
It is still uncertain whether CRP levels are raised in patients with OSAS. Since the index report in 2002 of a pilot trial suggesting that CRP levels might be related to the severity of OSAS,13 a number of other studies have addressed this issue and have come to different conclusions.14–20 The reasons for the different findings may have included a number of methodological factors such as small subject numbers, inadequately matched study populations (particularly in terms of BMI) and inclusion of patients with pre-existing cardiovascular or metabolic diseases. In a cohort including 30 patients with OSAS and 14 controls, Yokoe et al14 observed increased CRP levels in the patient group, but the patients had significantly higher BMI and the populations also included subjects with hypertension, coronary artery disease, stroke and diabetes mellitus. Further studies suggested an association between CRP levels and OSAS but with similar methodological limitations.15–17 However, recent studies have suggested that obesity rather than OSAS per se is the best predictor of CRP.19,20 A recent study by Can et al18 found higher CRP levels in patients with OSAS than in matched controls, but only patients with mild to moderate disease were included and no direct correlation to PSG parameters was observed. Furthermore, the effect of CPAP therapy on CRP levels is still unclear. Although Yokoe et al14 found an improvement in CRP levels after 1 month of CPAP therapy, two subsequent studies failed to confirm these results.19,21 In particular, Akashiba and co-workers21 followed 96 patients with OSAS receiving CPAP treatment for 9 months and found no significant change in CRP levels.
The present study has a number of strengths in comparison with some previous reports. First, we took great care in patient selection to exclude any with a cardiovascular or other medical disorder and none were taking any regular medication. Groups were matched for all demographic parameters and, in order to study specifically the effect of BMI on CRP levels, we included a further group of patients with severe OSAS but significantly higher BMI. This group had higher CRP levels than all other groups with or without OSAS, even after adjustment for AHI. Furthermore, 6 weeks of effective CPAP therapy had no effect on CRP levels and no PSG variable showed a significant independent relation to CRP. BMI was an independent predictor of CRP levels in multivariate analysis and even after separate analysis, allowing for the potential confounding effect by selecting a non-BMI-matched group, this relationship was still present. We therefore conclude that CRP levels are not increased in patients with OSAS, independent of obesity.
These findings underline the complexity of the process leading to cardiovascular complications in OSAS. There is growing evidence that inflammation plays a role in this process and, as one possible explanation, we have identified a selective activation of inflammatory over adaptive pathways by intermittent hypoxia in a cell culture model.28 As a consequence, we (and others) have found increased circulating levels of TNFα in patients with OSAS which fall with short-term CPAP treatment.30–32 Other inflammatory factors have been found to be increased in OSAS including IL8 and intercellular adhesion molecule-1.33 Differences in the relation of inflammatory markers to obesity might be explained by findings from studies suggesting that adipose tissue is a potent source of IL6, the precursor of CRP, but less so of TNFα.34 Various studies have shown a direct relationship between BMI and CRP levels,22,23 and these interactions seem to dominate this stage of inflammation whereby OSAS itself might potentially influence the production of other inflammatory cytokines, particularly TNFα.
A further finding of the present study is that patients with OSAS had similar homocysteine levels to control subjects, and multivariate analysis revealed no association of these levels with OSAS severity. Homocysteine is an intermediate amino acid formed during the metabolism of methionine. The proposed mechanisms of development of atherosclerosis in subjects with higher homocysteine levels are oxidative stress and depletion of nitric oxide leading to endothelial dysfunction.35 Prospective studies have shown a correlation between mildly increased homocysteine concentrations and premature coronary artery disease, peripheral vascular disease and stroke.11,12 Previous studies assessing homocysteine levels in patients with OSAS have reported different findings18,24–26 but, similar to previous studies of CRP levels in OSAS, these reports may have been influenced by small numbers and potential limitations in study design. Lavie et al24 conducted a large study and only detected increased homocysteine levels in OSAS patients with co-existing cardiovascular disease. Only one report to date has studied the effect of CPAP therapy on homocysteine levels.27 However, only 12 subjects were included in this study, the patients were suffering from various cardiovascular diseases and the time of re-evaluation varied.
One potential limitation of our study is the inclusion only of men. We designed the study specifically in this way to avoid gender differences which could influence the analysis. However, as a consequence, our data cannot automatically be extrapolated to female patients with OSAS. Furthermore, the non-OSAS group of 30 subjects included 8 subjects with suspected OSAS but who failed to demonstrate objective abnormalities on their PSG. None of these subjects described symptoms of narcolepsy, periodic limb movements or any other sleep disorder associated with excessive daytime sleepiness, so upper airway resistance syndrome may be the underlying diagnosis. This group is therefore strictly not a normal control population. However, we do not believe this to have influenced the results as CRP and homocysteine levels did not differ between true controls and sleepy non-OSAS patients and also between sleepy non-OSAS and BMI-matched patients with OSAS (data not shown).
In conclusion, the present data provide evidence that OSAS is not related to CRP or homocysteine levels. However, CRP levels are strongly linked to obesity. Other cardiovascular risk markers such as TNFα might therefore be better targets for predicting cardiovascular risk in subjects with OSAS.
Acknowledgments
The authors thank all staff members of the Sleep Laboratory at St Vincent’s University Hospital for their help and support and all patients and controls for participating in this study; and Dr C Gormley, Department of Statistics, School of Mathematical Science at University College Dublin for her expert statistical help in preparation of the manuscript.
REFERENCES
Footnotes
-
Published Online First 24 January 2007
-
WMcN is funded by the Health Research Board, Ireland.
-
Competing interests: None declared.
Linked Articles
- Airwaves