Article Text

Abstract
Background: Evidence suggests that a raised level of cord serum IgE (CS-IgE) is a risk factor for allergic sensitisation. However, whether CS-IgE is a risk for asthma is controversial. A study was undertaken to investigate the association between CS-IgE levels and allergic sensitisation at 4 and 10 years of age and asthma at ages 1–2, 4 and 10.
Methods: CS-IgE was available for 1358 of 1456 children born between 1989 and 1990. The cohort was evaluated for allergic diseases at ages 1, 2, 4 and 10 years. Skin prick tests for six allergens were performed on 981 children at age 4 and 1036 at age 10. Asthma was defined based on a physician’s diagnosis. Using logistic regression analysis, the risk of asthma and allergic sensitisation for raised levels of CS-IgE (⩾0.5 kU/l) was estimated.
Results: At ages 4 and 10 years 20.2% and 27.0% of children, respectively, had allergic sensitisation. The risk of allergic sensitisation was significantly associated with raised CS-IgE levels at ages 4 (OR 2.29) and 10 years (OR 1.73). The prevalence of asthma was 10.3% at age 1–2, 15.2% at age 4, and 12.8% at age 10. CS-IgE was not associated with asthma at age 1–2 and 4 but showed an increased relative risk at age 10 (OR 1.66, 95% CI 1.05 to 2.62). The association was stronger in children who did not develop allergic sensitisation at age 4 or 10 (OR 3.35, 95% CI 1.41 to 7.93).
Conclusions: Raised cord serum IgE is a risk factor for allergic sensitisation at ages 4 and 10 years. This is the second study suggesting that CS-IgE is also a risk factor for asthma at age 10, probably related to the late onset of asthma. This association is not necessarily mediated by allergic sensitisation.
- CS-IgE, cord serum immunoglobulin E
- SPT, skin prick test
- asthma
- cord serum
- immunoglobulin E
- atopy
- neonates
- skin prick test
Statistics from Altmetric.com
There is evidence that factors early in life have major effects on the later development of allergy (atopy).1–8 A correlation between serum IgE levels during the first year of life and atopic diseases in the first 2 years of life was first reported in 1975 by Orgel et al, who proposed that serum IgE might be used as a predictor for allergic diseases.7 Subsequent studies examined the use of cord serum IgE (CS-IgE) as a biomarker for atopic diseases but the results were conflicting.1,8,9,10,11,12,13,14 One limitation of these studies is that only early childhood manifestations (up to 5 years) were investigated,6,7,10,15 with the exception of a Swedish study that followed newborns to the age of 11.8 In addition, almost all of the previous studies used total CS-IgE (Nambu et al1 investigated CS-IgE specific to a particular allergen). Comparisons of studies are further complicated by their use of different allergic outcomes.
The Isle of Wight cohort was established in 1989 to study the risk factors for atopy and its development during childhood. The first examination of CS-IgE in this cohort found it to be an insensitive predictor of asthma, eczema, and hay fever in the first year of life.16 A subsequent study of 4 year old children by Tariq et al17 showed that raised CS-IgE levels increased the risk of aeroallergen sensitisation without increasing respiratory allergic symptoms. The purpose of the current study is to investigate the association between CS-IgE levels and both allergic sensitisation and asthma in the Isle of Wight cohort up to the age of 10 years.
METHODS
Study population
After approval by the local research ethics committee, 1456 children born between January 1989 and February 1990 on the Isle of Wight, UK were recruited. Informed written parental consent was obtained for all participants. To measure cord serum IgE, samples were obtained from 1358 newborn infants.
Questionnaire and examination
In the first survey at the time of the child’s birth, parents were asked about their age, maternal smoking during pregnancy, and history of asthma, hay fever, and atopic eczema. At 1 and 2 years of age a questionnaire was administered seeking information on symptoms suggestive of allergic disease in children.
At 4 years of age all children and their parents were invited to attend the allergy clinic;18 981 (67% of the original cohort) attended and a questionnaire was completed and a physical examination conducted. A follow up questionnaire (postal or telephone) was used to gather information from an additional 237 children who had not attended the clinic, giving a total of 1218 children (84% of the original cohort). Some families did not participate in the study because they moved from the Isle of Wight, while others declined to have their child skin prick tested. Questionnaire information was collected on the presence of allergic diseases. Birth order data and details of environmental factors such as parental smoking, exposure to pets, and housing conditions were also recorded.
At 10 years of age the information was updated and a physical examination was conducted during a visit to the research centre (n = 1043). Detailed interviewer administered questionnaires regarding asthma and allergy development were completed with a parent of each child. ISAAC written questionnaires were used to assess respiratory, nasal, and dermatological symptoms.19 When a visit was not possible, a telephone questionnaire was completed with a parent or a modified postal questionnaire was sent for the parent to complete and return (n = 330).
Extract of birth records
Data were obtained from hospital records on gestational age, birth weight, and neonatal complications (preterm delivery, fetal distress, newborn infection, jaundice, low blood sugar, hypothermia, congenital abnormalities, etc).
Cord serum IgE determination
Duplicate measurements of cord IgE were made on serum from umbilical vein blood samples using the Ultra EIA kit (Pharmacia Diagnostics AB, Uppsala, Sweden) which is designed to measure IgE levels between 0.2 and 50 kU/l in 0.1 ml serum or plasma. It is a solid phase enzyme immunoassay using monoclonal anti-human IgE, which has a high degree of correlation with the Phadebas IgE Prist method (r = 0.99).16 Cord IgA levels were measured in samples in which the level of IgE was higher than 0.3 kU/l. Any samples with IgA levels >10 mg/l were considered to be contaminated by maternal blood and were excluded. The method of cord IgE estimation has been described in greater detail elsewhere.16,20
Diagnostic criteria for asthma
The study physicians obtained information regarding the presence of allergic symptoms. For asthma, information included the presence and frequency of cough and wheezing, physician diagnosed asthma, and treatment given. At ages 1, 2 and 4 the minimum criteria for the diagnosis of asthma included three or more separate episodes of wheeze in the previous 12 months, each lasting at least 3 days. At age 10, asthma was defined as ever having a diagnosis of asthma, in addition to wheeze in the previous 12 months.
Skin prick tests
Skin prick tests (SPTs) were carried out on children at the age of 4 years (n = 981) and 10 years (n = 1036) using a standard battery of aeroallergens (house dust mite (Dermatophagoides pteronyssinus), grass pollen mix, cat and dog epithelia, Alternariaalternata, and Cladosporium herbarum). Histamine (0.1%) in phosphate buffered saline and physiological saline were used as positive and negative controls, respectively. The extracts were obtained from Biodiagnostics, Hamburg, Germany at age 4 and ALK-Abello, Denmark at age 10. Children were advised not to take antihistamines for 72 hours before the clinic appointment. Commercially available lancets (Medipoint Inc, Mineola, NY, USA) were used to prick the epidermis through the allergen extract drops. The tests were read after 15 minutes and a mean wheal diameter (sum of longest diameter + diameter diagonal to it divided by 2) of at least 3 mm more than the negative control was considered positive. Surrounding erythema was ignored. A child was regarded as sensitised when the reaction to at least one allergen was positive and non-sensitised when all recorded reactions were negative.
Statistical analysis
Likelihood ratios (sensitivity/(1−specificity)) were used to compare cut off points for CS-IgE. CS-IgE levels were then dichotomised into <0.5 kU/l and ⩾0.5 kU/l. Asthma at age 1–2 years was regarded as positive when at least one positive record was available at either age 1 or 2 years, and negative when there was at least one negative record and no positive record. SPTs and asthma at different ages were treated as dichotomous outcome variables and separate logistic regression models were run. Potential confounders were season of birth (spring: March–May; summer: June–August; autumn: September–November; winter: December–February); sex; birth weight (categorised as <1500 g, 1500–2500 g, 2500–4000 g, ⩾4000 g); neonatal complications (yes, no); maternal age (categorised as 16–23, 24–33, 34 years and older); history of maternal and paternal atopy (asthma, hay fever, atopic eczema); maternal smoking during pregnancy (yes, no); and having a pet at birth (yes, no).
Logistic regression was used to test the effect of CS-IgE levels on sensitisation and asthma, adjusting for the above mentioned potential confounding factors (logistic procedure). We estimated adjusted odds ratios of CS-IgE for SPT results and asthma at different ages. For asthma we also stratified data by SPT status. Adjusted odds ratios of SPT and asthma at different ages were estimated comparing the two levels of CS-IgE. All statistical analyses were performed using the SAS/Stat program (SAS Institute Inc, Cary, NC, USA).
RESULTS
CS-IgE was determined for 1358 children (93.3% of the original cohort). The proportion of newborn infants with increased CS-IgE levels (⩾0.5 kU/l) for various characteristics is shown in table 1. A maternal history of atopic disorders was a significant risk factor for increased CS-IgE. The number of children who had complete information on CS-IgE, SPTs, and all confounders was 862 at age 4 years and 900 at age 10 (63.5% and 66.3% of the sample with available CS-IgE; table 2). The number of children with complete information on the development of asthma as well as on CS-IgE and confounders was 1194 at age 1–2, 1068 at age 4, and 1191 at age 10 (78.6–87.9% of the sample of 1358; table 2). The proportion of children with raised CS-IgE levels (⩾0.5 kU/l) in the samples for different outcomes at different ages did not vary substantially (12.3–13.2%, table 2).
Characteristics of children with an available CS-IgE measurement
Number of children who had a measurement of cord serum IgE level at birth and at different ages by cord serum IgE levels
Likelihood ratios for different cut off points of CS-IgE indicated the level of risk for allergic sensitisation and asthma at ages 4 and 10 (table 3). The likelihood ratio (LR) is the likelihood that a specific level of a test result would be expected in a child with a disorder compared with the likelihood that that same result would be expected in a child without the disorder.21 CS-IgE levels above the detection limit increased the likelihood of the development of allergic sensitisation (LR >1) but not of asthma. CS-IgE levels of ⩾0.5 kU/l showed higher LRs in three of the four outcomes and thus provided more confidence in abnormal test results.
Likelihood ratios (LR) of allergic sensitisation (skin prick tests) and asthma for different levels of cord serum IgE
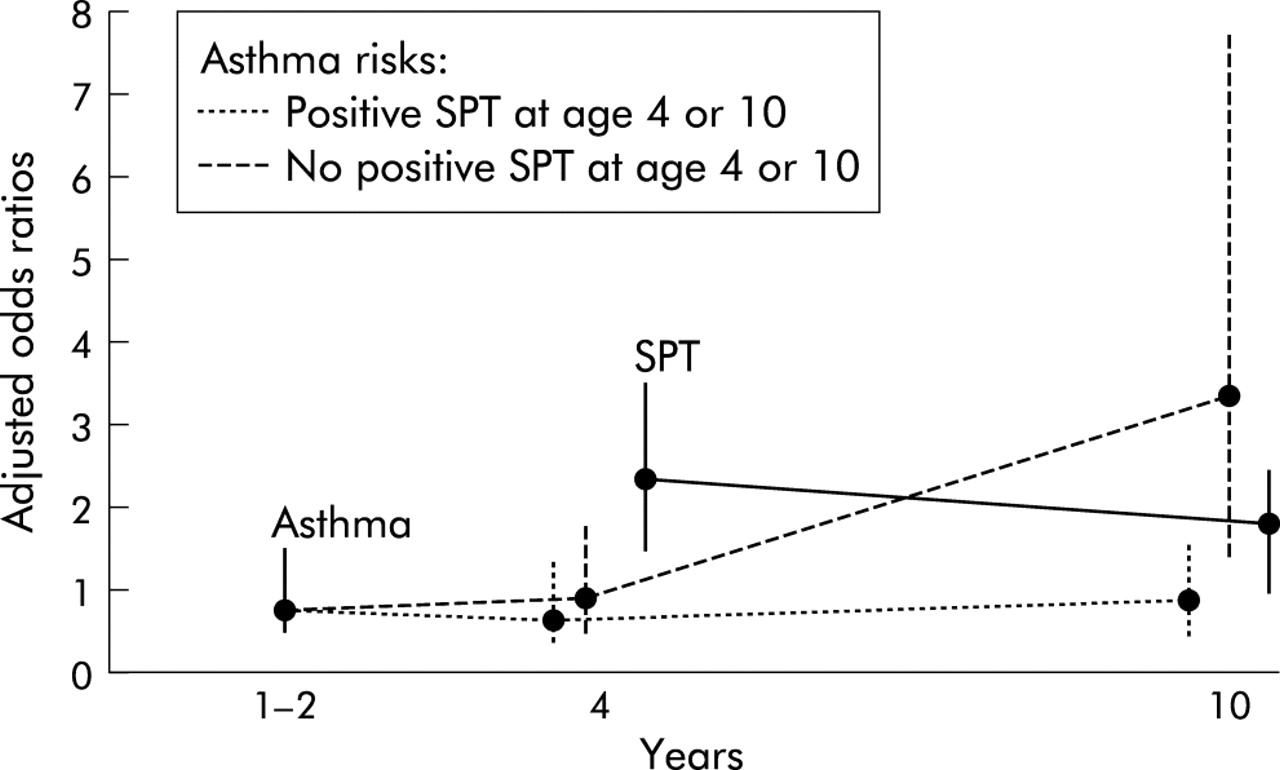
A positive SPT was evident in 20.2% (174/862) of the children at age 4 and in 27.0% (243/900) at age 10 (table 4). CS-IgE was a risk factor for a positive SPT both at age 4 and 10, but the association was stronger at 4 years of age (table 4, fig 1). With regard to specific SPTs, the prevalence increased for most allergens. However, the association (OR) between CS-IgE and allergic sensitisation decreased between 4 and 10 years (table 4).
Odds ratios (ORs) and confidence intervals (CI) for the risk of sensitisation with raised CS-IgE levels (logistic regression analysis)
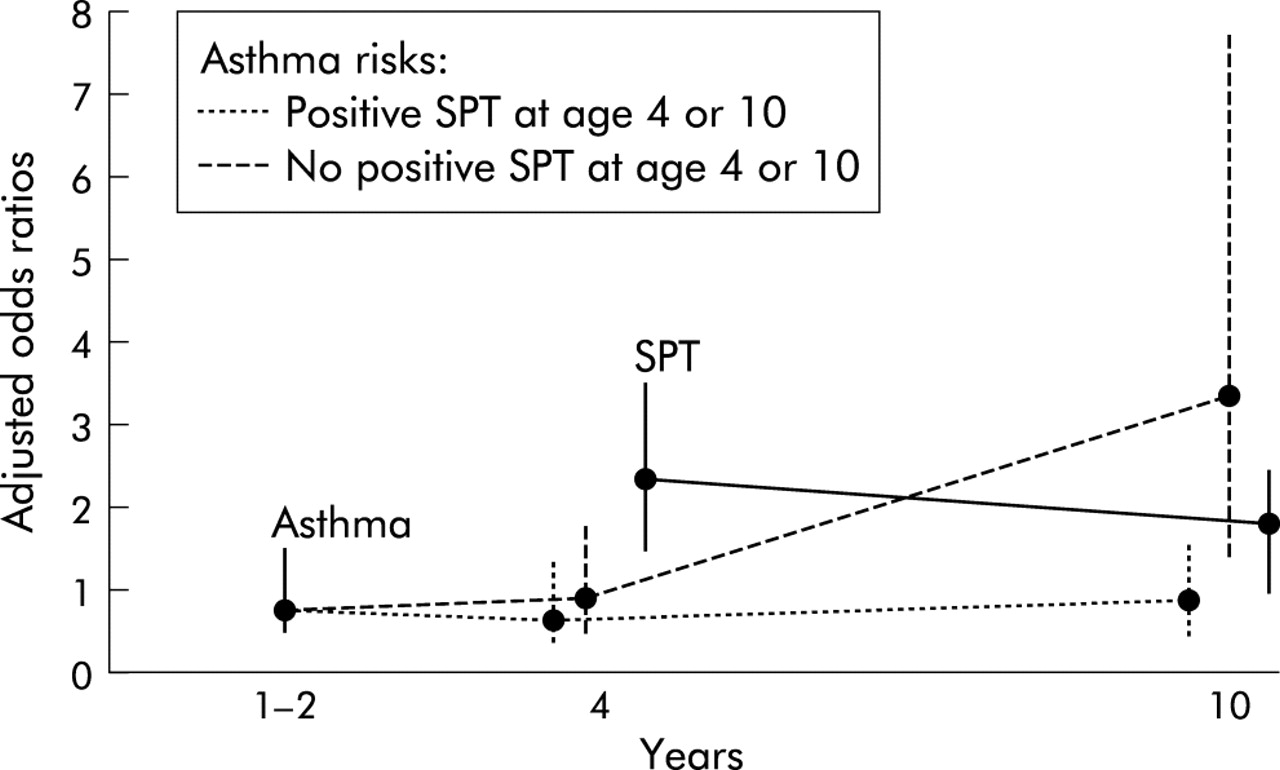
Adjusted odds ratios (OR) of skin prick tests (SPTs) and asthma at different ages for raised levels of cord serum IgE. The dots show the odds ratios and the vertical bars represent 95% confidence intervals.
At age 1–2 years physician diagnosed asthma occurred in 10.3% of the children (123/1194, table 5). The prevalence of asthma at age 4 was 15.2% (162/1068) and at age 10 was 12.8% (152/1191). Logistic regressions were used to test the associations of CS-IgE with asthma at ages 4 and 10. In addition, to assess whether these relationships were mediated by sensitisation, we stratified asthma at age 4 by SPT positivity at age 4 and asthma at age 10 by SPT positivity at age 4 or 10. Table 5 shows that cord serum IgE levels were not associated with asthma at age 4, irrespective of atopic status. The association of CS-IgE with asthma at age 10 had an OR of 1.66 (95% CI 1.05 to 2.62) which is statistically significant. When stratifying by SPT results, the association lost its significance in children who had a positive SPT at age 4 or 10 (OR 0.83). However, the majority of children had a negative SPT at both ages. In these children the association between CS-IgE and asthma at age 10 became stronger (OR 3.35, 95% CI 1.41 to 7.93). Figure 1 shows that the relative risk (OR) of CS-IgE for asthma increases with increasing age of diagnosis.
Odds ratios (ORs) and confidence intervals (CI) for the risk of asthma with raised CS-IgE levels (logistic regression analysis)
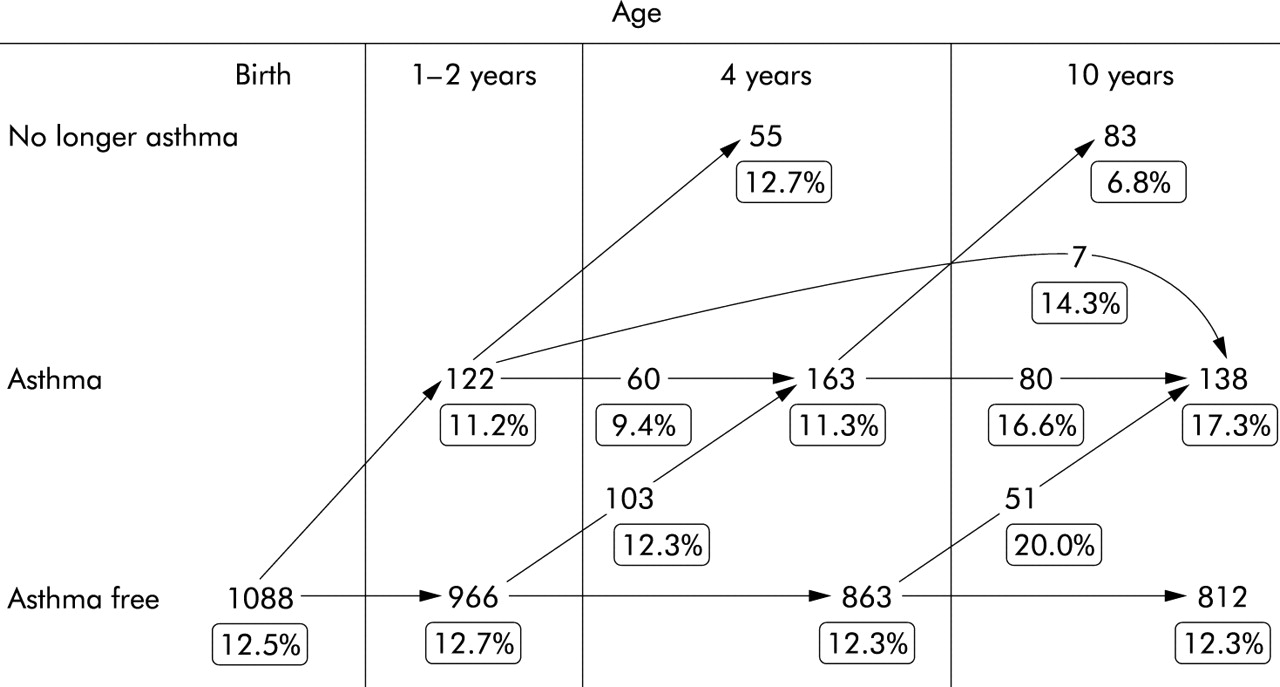
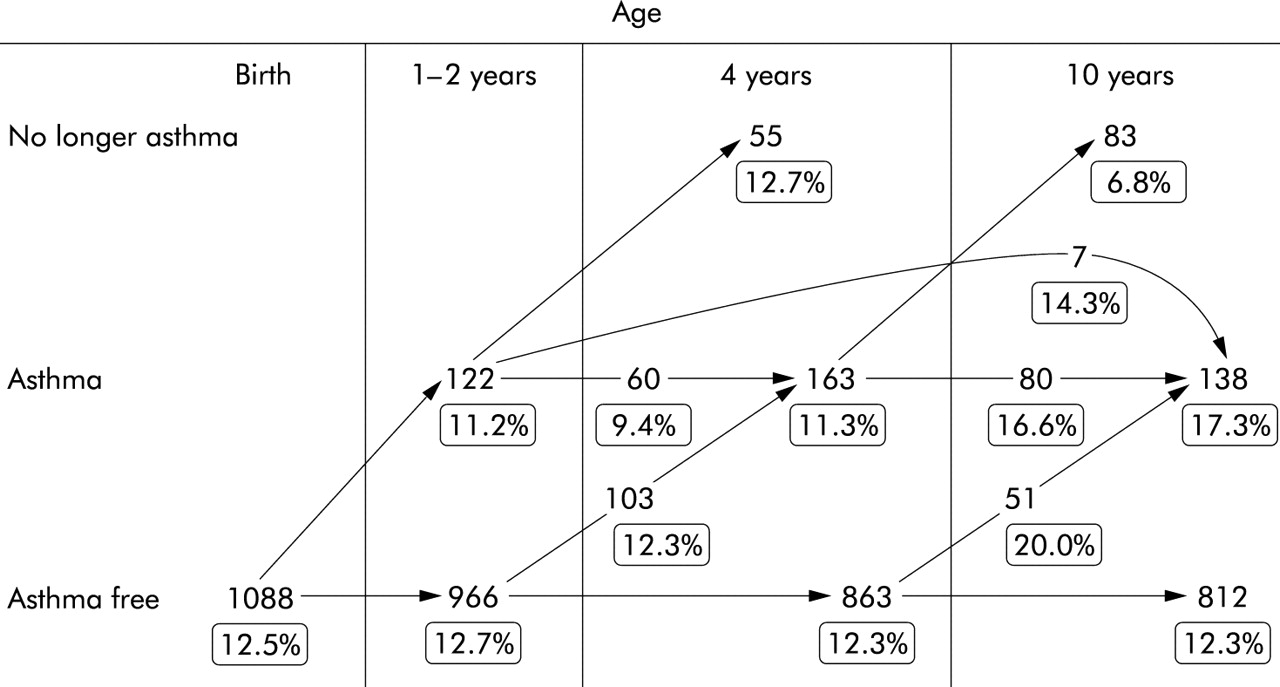
The dynamics of the development of asthma are shown in fig 2. Of the 138 children who were diagnosed with asthma at age 10, only 44 had asthma at age 1–2. Fifty one children were first observed to have asthma at age 10 (37% of the children with asthma at age 10). For each subgroup in fig 2, the percentage of children with raised cord serum IgE is shown. In children with late onset asthma (developing after 4 and before 10 years), the proportion is substantially higher (20%) than, for instance, the subgroup with early onset asthma at age 1–2 years (11.2%, fig 2).
{kind=link}
{kind=link}
Dynamic for groups of asthmatics diagnosed in different ages and percentages of raised cord serum IgE.
DISCUSSION
Our results show that raised CS-IgE (⩾0.5 kU/l) is a risk factor for allergic sensitisation at ages 4 and 10 years, and for asthma at age 10 years but not at age 1–2 or 4 years. To our knowledge, this is the second study to examine the association between CS-IgE and asthma at a later age in childhood.22 Studies over the past three decades conducted on the association between CS-IgE and asthma in childhood are not in agreement.2,6,17,22–27 Most involved only a small number of children and did not follow them beyond 5 years.23–27 In addition, some studies were based only on a clinical assessment of atopy, not on a determination of allergic sensitisation.7,22,23 Our results corroborate previous studies which found that CS-IgE is a risk factor for allergic sensitisation in early childhood and extend this observation for the first time to the age of 10 years. Our findings also support the report by Croner et al22 that raised CS-IgE increases the incidence of asthma cumulated during childhood up to the age of 11 years (four investigations at 1.5, 3, 7, and 11 years).4,8,22
The analyses are based on samples of children with complete information on the outcome (sensitisation or asthma), exposure (CS-IgE), and potential confounders. Comparisons of the initial subjects who had CS-IgE measurements (n = 1358) with those used in the analyses indicate that selection bias is unlikely (table 2).
Contamination of cord blood with maternal blood was assessed using IgA as a biomarker. This led to the exclusion of 86 infants from further analysis.17,27 Hence, a potential misclassification of cord blood IgE is unlikely. To dichotomise CS-IgE levels, cut off points of 0.5–1.3 kU/l have been used in previous studies.2,4,8,22–27 We chose to use the cut off point of 0.5 kU/l CS-IgE for two reasons. Firstly, it has been shown to be the optimal level in previous analyses of this birth cohort17 and, secondly, likelihood ratios indicated that the certainty of atopic development is increased for CS-IgE levels of ⩾0.5 kU/l (LR >1.58 for three of four outcomes). Higher levels of CS-IgE were less reliable because of the small number of children (for example, ⩾1.0 kU/l and asthma at age 10: n = 9). To assess allergic sensitisation we used skin prick tests which are accepted as an objective marker for evaluating allergic sensitisation.28,29 The use of both negative and positive controls reduced the possibility of false results.
IgE production is downstream in a pathway that starts with the presentation of antigens (allergens) to the immune system. This may result in the preferential activation of Th2 cells which are programmed to secrete interleukin (IL)-4 and IL-13 and to induce IgE production.30–32 An important question is whether the association of cord IgE levels with asthma is due to its relation with early sensitisation. Our results indicate that the direct effect of CS-IgE disappears in children who developed sensitisation (positive SPT at age 4 or 10 years, table 5). Since CS-IgE is also a significant predictor of a positive SPT (table 4), it is likely to have an indirect effect on asthma: CS-IgE→SPT positivity→asthma. However, sensitisation is not a necessary link in the chain of reactions because, in children who did not develop sensitisation (representing the majority), a strong direct effect between CS-IgE and asthma became obvious (OR 3.35, table 5). We also investigated whether only early sensitisation (at age 4) changed the direct and indirect effect of CS-IgE on asthma and found that the results did not differ substantially from those when SPTs at age 4 and 10 were combined.
Exposure to pets at birth was not associated with CS-IgE levels (table 1) and did not explain the occurrence of allergic sensitisation and asthma. The additional control of pet exposure at age 4 and for the number of children in the home, separately and in combination, also had no effect on the results.
It is widely accepted that dramatic changes in immune responses occur during pregnancy and fetal markers of immune response are detected as early as 10–22 weeks gestation.33 To prevent the termination of pregnancy the fetomaternal immune system is shifted in a Th2 direction.34,35 This Th2 shift begins with the secretion of human chorionic gonadotropin which, in turn, stimulates progesterone production. Progesterone then promotes the secretion of Th2 cytokines over the secretion of Th1 cytokines.33 Although cytokine production may be variable in the early stage of development, the Th1 and Th2 subsets become stable after repeated stimulation.30–32 There are two theories as to the time when sensitisation and T cell stability occurs: the prenatal priming hypothesis which considers that fetal life immunological events are more important in the development of allergy in childhood, and the hygiene hypothesis which considers that the insults happen after birth. Given that CS-IgE is a biomarker of prenatal immunological conditions, our findings favour the prenatal priming hypothesis. CS-IgE was associated with overall SPT positivity at ages 4 and 10 (table 4). The presence of a significant adjusted OR for the overall SPT and specific SPTs—both at age 4 and 6 years later—supports this idea. There was a non-significant reduction in the OR of CS-IgE despite the increased percentage of children with a positive SPT at age 10, which may reflect a weakening of the effect of prenatal conditions compared with postnatal events (table 4, fig 1).
We observed a stronger association between raised CS-IgE levels and a maternal history of atopy than with a paternal history of atopy (table 1). This is in agreement with previous findings and other evidence that maternal immune responses may influence allergic responses in offspring.36–39
CS-IgE had a prognostic value (OR 1.66) for asthma at age 10 years. In the one previous investigation with a comparable follow up time after birth, Croner et al found a fivefold increase in the cumulative incidence of asthma in children at 11 years with CS-IgE levels of 0.9 kU/l and higher.22
At ages 1–2 and 4 years the minimum criteria for the diagnosis of asthma included three or more separate episodes of wheeze in the previous 12 months, each lasting at least 3 days. At age 10 the definition of asthma was at least one episode of wheezing in the previous 12 months in addition to being diagnosed with asthma by a physician at least once. Different criteria for a diagnosis of asthma at ages 4 and 10 may have led to misclassification. This misclassification, should it exist, would be non-differential. A previous diagnosis of asthma was less likely to have biased an asthma diagnosis at age 10 because fewer children were diagnosed as asthmatics at this age (12.8%) than at age 4 (15.2%, table 5). It is unlikely that the level of CS-IgE affected the asthma diagnosis at age 10 but not at age 4, as this information was not available to the field workers who collected information on the presence of wheeze and asthma diagnosis.
As already mentioned, there is evidence that early life events may influence atopy and asthma later in life. But how could CS-IgE levels predict asthma at age 10 years and not at an earlier age? One possible explanation is that the diagnosis of asthma in early childhood is based on transient symptoms that tend to disappear later in life. Kurukulaaratchy et al40 showed that, in approximately two thirds of children who had wheezing in the first 4 years of life, it had disappeared by the age of 10. In addition, it has been reported that most infants who wheeze are not necessarily atopic and that the wheezing disappears in many as they grow older.41 Assuming this kind of “sorting process”, the diagnosis of asthma becomes more reliable for children with persistent wheezing. However, our data do not support this explanation as the percentage of those with asthma at ages 1–2, 4 and 10 years (12.5%) who had raised levels of CS-IgE was not different from those who never had asthma (12.3%, fig 2).
Another possible explanation is that the late onset of asthma is related to CS-IgE. In this case, we would expect a higher proportion of children with raised CS-IgE levels in the late onset group. In our study, 51 children (fig 2) had asthma at age 10 but not earlier, but only a few of them had wheezing before the age of 10 (6% at age 1–2 and 10% at age 4). However, 20% of these children had raised CS-IgE levels which is the highest proportion of any of the groups studied (fig 2). The next highest proportion of raised CS-IgE levels (16.6%) was in children who had asthma at age 4 and again at age 10 years. Our results therefore support the late onset theory rather than the “sorting process” explanation.
As shown in fig 1, the trend for ORs for asthma increased until it reached significance at age 10. In addition, the percentage of asthmatics with raised CS-IgE levels was 8.7% at age 1–2, 15.0% at age 4, and 18.5% at age 10 years (table 5). This could be seen as a gradual development of asthma in those with raised CS-IgE levels and hence supports the importance of CS-IgE as a biomarker of fetal life events in the development of asthma later in life.
In conclusion, raised cord serum IgE levels measured at birth increase sensitisation to aeroallergens by the ages of 4 and 10 years and the development of asthma at 10 years but not at younger ages. These findings support the importance of prenatal conditioning in the development of allergy later in life. The lack of significance of CS-IgE as a risk factor for asthma early in life may be due to the gradual development of asthma as the cohort aged and the existence of a late onset variety of asthma. Further investigations are needed to increase our understanding of the immunological mechanisms responsible for the effect of fetal life events on childhood allergy. Long term assessments are also needed because of the possibility of late onset childhood allergy.
REFERENCES
Linked Articles
- airwaves