Article Text

Statistics from Altmetric.com
Medical professionals in the UK need to engage more in smoking cessation services
Of the 120 000 people who die from smoking each year in the UK, more than half die from a respiratory disease. In 1997 deaths from lung cancer, chronic obstructive pulmonary disease (COPD), and pneumonia caused by smoking totalled over 63 000,1 all of which were potentially avoidable. These figures show that preventing smoking is more relevant to respiratory medicine than any other speciality. In this issue of Thorax Abdullah and Husten2 review the priorities for tobacco control in the developing world and summarise the difficulties of developing smoking cessation in countries already severely challenged by generally low levels of health service funding and infrastructure, by competing public health priorities such as HIV, by low levels of public awareness of smoking as a dangerous behaviour, and other issues. However, one of the problems they identify that is especially relevant in the UK is the need to engage medical professionals in smoking cessation.
The National Health Service (NHS) approach to smoking cessation in the UK has changed radically in the past 5 years. Although the effectiveness of behavioural support and nicotine replacement therapy (NRT) for smoking cessation had been recognised for many years, it is only since the publication of the government White Paper “Smoking Kills” in 19983 that these treatments, and subsequently bupropion therapy, have been made routinely available to smokers through the NHS. Before 1998, smoking cessation services were available to a tiny minority of smokers through sporadic local initiatives and the private sector, but this is no longer the case. All smokers should now be able to access effective cessation services providing evidence based and cost effective4 interventions, and many have already done so: in the year to April 2003 in England over 230 000 smokers attended NHS cessation services and set a quit date, and over 120 000 reported cessation for at least 4 weeks.5 This number was nearly double that of the previous year, and further ambitious targets have been set for throughput in the next 3 years.5 Therefore, while many countries lack the infrastructure, funding and political will to provide smoking cessation services, the UK does not. So, are these services actually being used to their full potential?
“.. . if we don’t use smoking cessation services we will lose them”
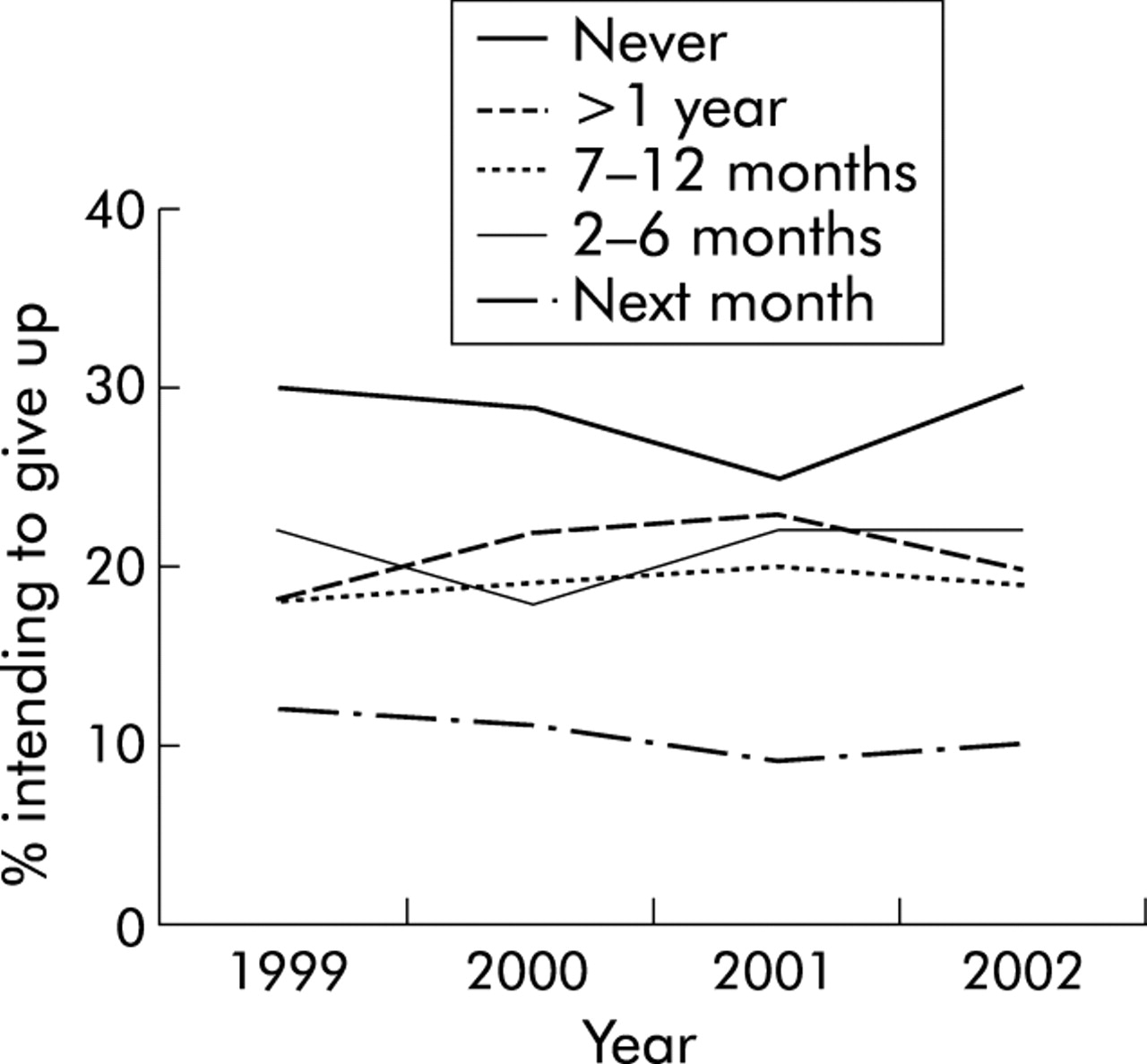
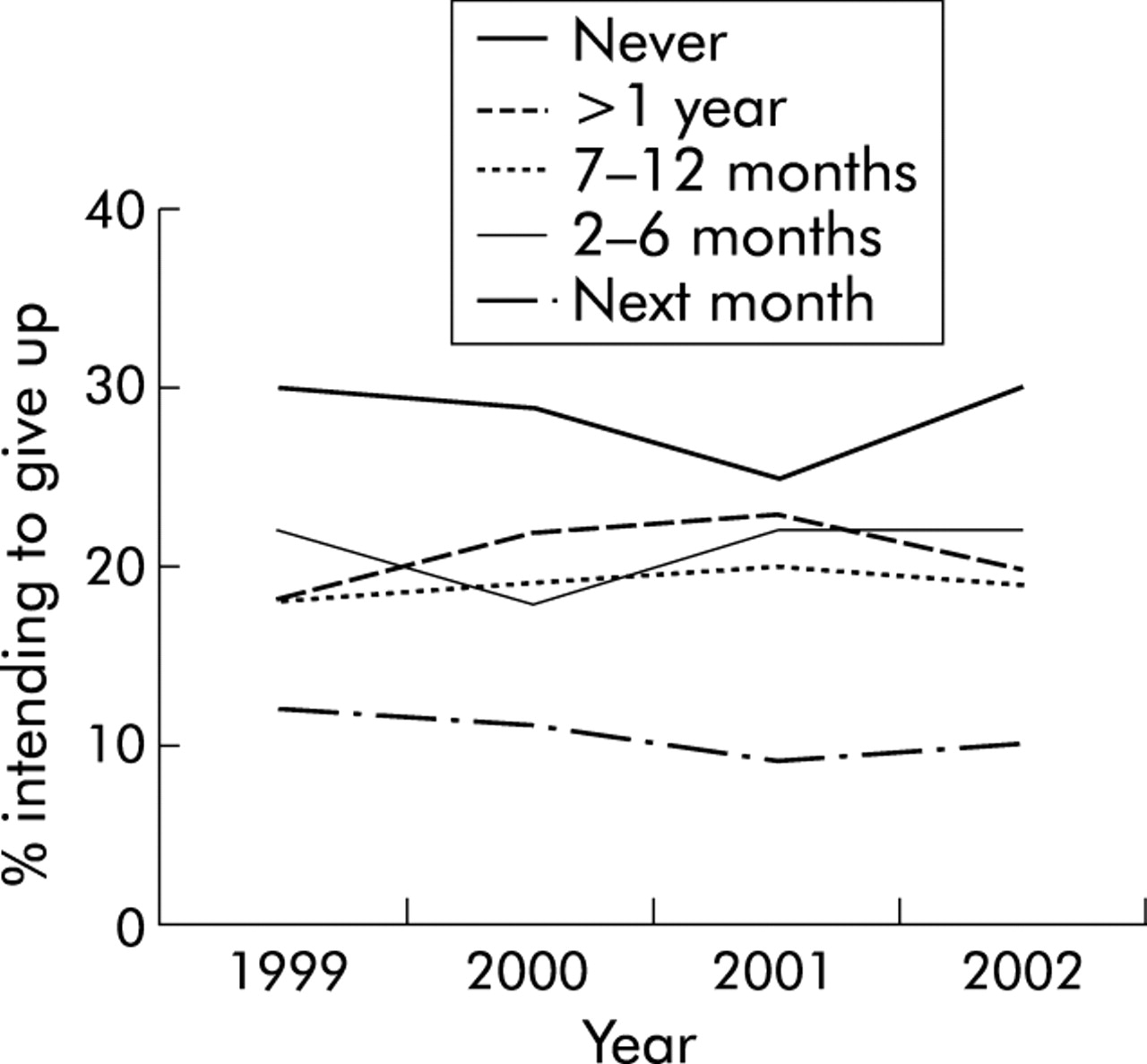
Surveys of attitudes to smoking by smokers in the UK have shown consistently that most smokers—typically about 70%—intend to give up smoking.6 The figures also show that in many cases this is not an expression of a vague and distant aspiration, since consistently about 50% state that they intend to give up within the next year, 30% within 6 months, and 10% in the next month (fig 1⇓).6 In absolute terms, these percentages translate into around 6 million smokers wanting to give up within the next year and 1.2 million in the next month. Against these totals, the 230 000 or so who set a quit date through NHS cessation services in the 12 months to April 2003 represent a very small proportion and, indeed, reflect a failure to capitalise on a major preventive opportunity. At least some of the responsibility for this lies with the medical profession.
{kind=link}
Intention to give up smoking, and when, in smokers aged 16 and over in Great Britain. Data from Lader and Meltzer.6
It has been argued for some time now that smoking status should be considered a vital sign—as routine a component of any medical consultation as measuring the pulse or blood pressure.7 This has been emphasised repeatedly in clinical practice guidelines for smoking cessation in the UK8,9 and USA,10–,12 which stress the importance of asking about smoking status at all consultations, advising all smokers to stop smoking, and arranging appropriate smoking cessation support for all smokers who are motivated to try. In practice, however, it is clear that, at least until very recently, this has not occurred. Recent clinical audit data from primary care13 and from my own14 and at least one other hospital15 in the UK show that inquiring about smoking status and advising cessation are still far from routine activities. At a national level, even in 2002, less than half of all smokers recall receiving advice to quit from a health professional at any time in the last 5 years,6 while the proportion of smokers who have used specialist services and/or pharmacotherapy in the past year has remained below 20% for the last 4 years.6,16 Undergraduate medical training in the UK still does not typically deliver adequate clinical training in smoking cessation methods, leaving most junior doctors feeling unprepared to deal with smoking in their patients.17 Hospital managers have also been slow to respond to the opportunities available to fund cessation support, since half the hospitals in the UK still do not provide a cessation counselling service for inpatients.18 Data from the USA are similar and indicate that medical schools are not delivering appropriate training,19 that many practising physicians feel underprepared to deal with smoking in their clinical work,20 that cessation advice is provided during consultations only to a minority of smokers21 and that, as in the UK,22 this advice tends to be limited to those with a smoking related disease.21
In the developing world many of the obstacles to implementing effective smoking cessation services arise from political and economic influences that are beyond the immediate control of individual clinicians. In the UK the situation is now very different—the services are or should be available but are not being used. As a result we are not only missing a major opportunity to improve the individual health of our patients and the collective public health, but also running the risk that the political will to continue to provide the services will stall. The danger is that, if we don’t use smoking cessation services, we will lose them.
REFERENCES
Linked Articles
- airwaves