Article Text

Abstract
Background: Although breathlessness is common in chronic heart failure (CHF), the role of inspiratory muscle dysfunction remains unclear. We hypothesised that inspiratory muscle endurance, expressed as a function of endurance time (Tlim) adjusted for inspiratory muscle load and inspiratory muscle capacity, would be reduced in CHF.
Methods: Endurance was measured in 10 healthy controls and 10 patients with CHF using threshold loading at 40% maximal oesophageal pressure (Poesmax). Oesophageal pressure-time product (PTPoes per cycle) and Poesmax were used as indices of inspiratory muscle load and capacity, respectively.
Results: Although Poesmax was slightly less in the CHF group (−117.7 (23.6) v −100.0 (18.3) cm H2O; 95% CI −37.5 to 2.2 cm H2O, p = 0.1), Tlim was greatly reduced (1800 v 306 (190) s; 95% CI 1368 to 1620 s, p<0.0001) and the observed PTPoes per cycle/Poesmax was increased (0.13 (0.05) v 0.21 (0.04); 95% CI −0.11 to −0.03, p = 0.001). Most of this increased inspiratory muscle load was due to a maladaptive breathing pattern, with a reduction in expiratory time (3.0 (5.8) v 1.1 (0.3) s; 95% CI 0.3 to 3.5 s, p = 0.03) accompanied by an increased inspiratory time relative to total respiratory cycle (Ti/Ttot) (0.43 (0.14) v 0.62 (0.07); 95% CI −0.3 to −0.1, p = 0.001). However, log Tlim, which incorporates the higher inspiratory muscle load to capacity ratio caused by this altered breathing pattern, was ⩾85% predicted in seven of 10 patients.
Conclusions: Although a marked reduction in endurance time was observed in CHF, much of this reduction was explained by the increased inspiratory muscle load to capacity ratio, suggesting that the major contributor to task failure was a maladaptive breathing pattern rather than impaired inspiratory muscle endurance.
- inspiratory muscle endurance
- respiratory muscles
- chronic heart failure
- BMI, body mass index
- CHF, chronic heart failure
- Cldyn, dynamic lung compliance
- FEV1, forced expiratory volume in 1 second
- FRC, functional residual capacity
- FVC, forced vital capacity
- LVEDD, left ventricular end diastolic dimension
- LVEF, left ventricular ejection fraction
- NYHA, New York Heart Association functional class
- Poes, oesophageal pressure
- Poesexp, peak expiratory oesophageal pressure
- Poesmax, maximum negative oesophageal pressure during an inspiratory manoeuvre
- Poespeak/TTPoespeak, inspiratory muscle contraction rate
- PTPoes per cycle, inspiratory oesophageal pressure time product per breath
- PTPoes per cycle/Poesmax, inspiratory muscle load to capacity ratio
- RR, respiratory rate
- RV, residual volume
- TLC, total lung capacity
- Te, expiratory time
- Ti, inspiratory time
- Ti/Ttot, duty cycle
- Tlim, endurance time
- Ve, minute ventilation
- Vt, tidal volume
Statistics from Altmetric.com
- BMI, body mass index
- CHF, chronic heart failure
- Cldyn, dynamic lung compliance
- FEV1, forced expiratory volume in 1 second
- FRC, functional residual capacity
- FVC, forced vital capacity
- LVEDD, left ventricular end diastolic dimension
- LVEF, left ventricular ejection fraction
- NYHA, New York Heart Association functional class
- Poes, oesophageal pressure
- Poesexp, peak expiratory oesophageal pressure
- Poesmax, maximum negative oesophageal pressure during an inspiratory manoeuvre
- Poespeak/TTPoespeak, inspiratory muscle contraction rate
- PTPoes per cycle, inspiratory oesophageal pressure time product per breath
- PTPoes per cycle/Poesmax, inspiratory muscle load to capacity ratio
- RR, respiratory rate
- RV, residual volume
- TLC, total lung capacity
- Te, expiratory time
- Ti, inspiratory time
- Ti/Ttot, duty cycle
- Tlim, endurance time
- Ve, minute ventilation
- Vt, tidal volume
Breathlessness is a common symptom in chronic heart failure (CHF).1,2 Although an imbalance between the pressure generated by the inspiratory muscles and the maximal pressure achievable contributes to dyspnoea,3 the role of impaired inspiratory muscle endurance remains unclear. Early studies4–6 suggested that patients with heart failure have marked inspiratory muscle weakness but, using more detailed invasive techniques, later studies have shown that inspiratory muscle strength is only modestly reduced.7–9 Nevertheless, there is evidence of excessive loading of the inspiratory muscles during exhaustive exercise,7,10 but without overt diaphragm fatigue.7,11 These observations suggest that, in patients with CHF, an imbalance may exist between the capacity of the inspiratory muscle pump and its ability to sustain activity against inspiratory loads rather than straightforward weakness of the inspiratory muscles.
Recent data from our laboratory have shown that the endurance of the inspiratory muscles, assessed using a technique of constant level negative pressure threshold loading, is a function of endurance time (Tlim) and the ratio of the inspiratory muscle load to inspiratory muscle capacity.12,13 Compared with previous methods,14,15 this technique directly assesses the inspiratory muscle load to capacity ratio and is novel because it allows for, and permits the evaluation of, patient initiated changes in breathing pattern that occur in response to high inspiratory loads.16 Thus, it has been shown previously that a reduction in Tlim does not necessarily imply significant impairment of inspiratory muscle endurance, but may indicate a particular breathing strategy response to loaded breathing.12,13 In the current study we hypothesised that there would be an overall reduction in inspiratory muscle endurance in patients with CHF. However, the main aim was to quantify the reduction in inspiratory muscle endurance and to examine the magnitude of the inspiratory muscle load to capacity ratio and assess its effects on Tlim.
METHODS
The protocol was approved by the local ethics committee. In line with the previous studies of inspiratory muscle endurance in patients with pulmonary disease,12,13 10 patients with CHF (nine men) recruited from our cardiology department and 10 healthy controls (nine men) were studied. The healthy volunteers were taken from hospital staff and their relatives. Patients with neuromuscular and pulmonary disease were excluded.
Cardiac and pulmonary function testing
CHF was defined as stable symptomatic left ventricular dysfunction with a left ventricular ejection fraction (LVEF) <45%.17 LVEF and left ventricular end diastolic dimensions (LVEDD) were measured by two dimensional and M mode echocardiography performed by a physician blinded to the results of the study. Pulmonary function tests were performed according to standard guidelines18 and expressed as a percentage of published values.19
Pressure measurements
An oesophageal balloon catheter (Ackrad Laboratories, NJ, USA) was positioned in the standard manner.20 Oesophageal pressure (Poes) was measured using a differential pressure transducer (±300 cm H2O; Validyne, CA, USA) and amplified by a carrier amplifier (Validyne). All signals were sampled at 100 Hz and passed via an analogue digital board to a computer (Apple Computers, CA, USA) running Labview 4.1 software (National Instruments, TX, USA). Dynamic lung compliance (Cldyn) was calculated during resting breathing by dividing tidal volume (Vt) by the oesophageal pressure difference at points of zero flow.
Maximum inspiratory pressure
Maximum inspiratory efforts were repeated from functional residual capacity (FRC) at least 10 times until three reproducible efforts were obtained. Each subject performed the manoeuvre using both a flange and tube mouthpiece in random order and the peak oesophageal pressure (Poesmax) with either mouthpiece was determined. Poesmax was defined as the inspiratory muscle capacity.
Inspiratory muscle endurance testing
Inspiratory muscle endurance was measured using a negative pressure threshold loading technique developed in our laboratory,12 in which subjects breathe against a constant level low resistance inspiratory threshold loading device.21 Patients with CHF and healthy controls were exposed to a similar negative pressure (40% Poesmax) and underwent 2–5 practice endurance runs, up to the target pressure, to become accustomed to the apparatus and the sensation of dyspnoea. During the first minute of the test the threshold pressure was progressively made more subatmospheric from −10 cm H2O to 40% Poesmax. No restrictions were placed on the pattern of breathing and no instructions were given regarding the breathing pattern to adopt. Tlim was the period from when the negative pressure imposed reached 40% Poesmax to task failure. All participants continued until the level of dyspnoea was intolerable and task failure was defined as the inability to generate the target pressure and open the valve.
We also used data obtained from 35 normal subjects performing the same protocol at a more negative threshold pressure (70% Poesmax). The data from 30 of these subjects have been presented previously12 and these data were combined with additional data from five extra subjects (mean age 61 years).
Inspiratory muscle load, inspiratory muscle contraction rate, and expiratory pressure
Inspiratory oesophageal pressure-time product per breath cycle (PTPoes per cycle) was averaged for the whole test. PTPoes per cycle was defined as the inspiratory muscle load.12 Peak inspiratory oesophageal pressure normalised for the time to peak oesophageal pressure (Poespeak/TTPoespeak) was used as an index of inspiratory muscle contraction rate, whereas peak expiratory oesophageal pressure (Poesexp) was used as a measure of intrapleural pressure change during expiration. As in previous studies,12,13 the inspiratory muscle load to capacity ratio was calculated as PTPoes per cycle/Poesmax.
Data analysis
Our first comparison was between patients with CHF and healthy controls exposed to the same inspiratory load (40% Poesmax). In line with our previous reports,12,13 Tlim values were logarithmically converted (log Tlim) and plotted against the corresponding inspiratory muscle load to capacity ratios (PTPoes per cycle/Poesmax), which allowed a second comparison to be made with control subjects studied at the higher threshold of 70% Poesmax. This approach was used because none of the normal subjects experienced task failure at 40% Poesmax and because values of PTPoes per cycle/Poesmax observed in patients with CHF at 40% Poesmax were comparable to those obtained in normal subjects at 70% Poesmax. To ensure that this comparison was appropriate and valid with respect to the age of the patients, modification of the previously published normal values12 was performed following additional studies in older subjects, as described above. Nevertheless, the additional normal data resulted in only a minor modification of the previously published values.12 The modified equation used in the current study to describe normal values was log Tlim = 3.5–3.6* PTPoes per cycle/Poesmax (r = 0.84, p<0.0001).
Data are expressed as mean (SD) unless stated otherwise. Differences between patients with CHF and healthy controls were assessed using unpaired t tests. Correlation between percentage predicted log Tlim and Poespeak/TTPoespeak was assessed using simple linear regression analysis. A value of p<0.05 was considered significant.
RESULTS
Cardiac and pulmonary function
All patients had severe left ventricular dysfunction (LVEF 22.5 (4.0)% and LVEDD 7.1 (0.5) cm; table 1). Five patients had a New York Heart Association (NYHA) classification score of III and five had a score of II. Forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), FEV1/FVC, total lung capacity (TLC), residual volume (RV), and FRC were similar in both groups (table 2).
Demographic and functional characteristics of patients with chronic heart failure
Mean (SD) differences in demographic data and lung function tests between healthy controls (HC) and patients with chronic heart failure (CHF)
Inspiratory muscle strength, breathing pattern, dynamic lung compliance, and inspiratory muscle load to capacity ratio
Poesmax tended to be lower in patients with CHF but this was not significantly reduced compared with the controls (table 3). Although patients with CHF and healthy controls were exposed to the same relative threshold load (40% Poesmax), all CHF patients discontinued the test within 30 minutes (mean Tlim 306 s) whereas all healthy controls sustained the target negative pressure for this time, at which time the test was terminated (p<0.0001).
Mean (SD) differences between healthy controls (HC) and patients with chronic heart failure (CHF) in inspiratory muscle strength, pulmonary mechanics, ventilatory breathing pattern, inspiratory muscle load, and endurance time during negative pressure threshold loading
In both patients with CHF and controls the pattern of breathing established at the start varied little throughout the test. Patients with CHF had higher minute ventilation (Ve, p = 0.05) and faster respiratory rate (RR, p = 0.05), with a shorter expiratory time (Te, p = 0.03) and longer duty cycle (Ti/Ttot, p = 0.001), but a similar inspiratory time (Ti, p = 0.95) compared with the healthy controls (table 3). Furthermore, there was a reduction in Cldyn in the CHF group (p = 0.006) accompanied by a slower Poespeak/TTPoespeak (p = 0.003) and higher Poesexp (p = 0.004).
The net effect of these changes in breathing pattern in patients with CHF was to increase the inspiratory muscle load to capacity ratio (PTPoes per cycle/Poesmax, p = 0.001). Although the reduction in Cldyn would have contributed to the increased PTPoes per cycle/Poesmax, we observed a positive correlation between PTPoes per cycle/Poesmax and Ti/Tot (r = 0.84, p = 0.002) but not Cldyn (p = 0.4). This, combined with the fact that the internal load as a percentage of the total load per breath calculated from Cldyn and mean Poes per cycle was approximately 18% in CHF patients and 11% in healthy controls, suggests that the major factor influencing the increase in PTPoes per cycle/Poesmax in patients with CHF was prolongation of the duty cycle.
Factors reducing endurance time
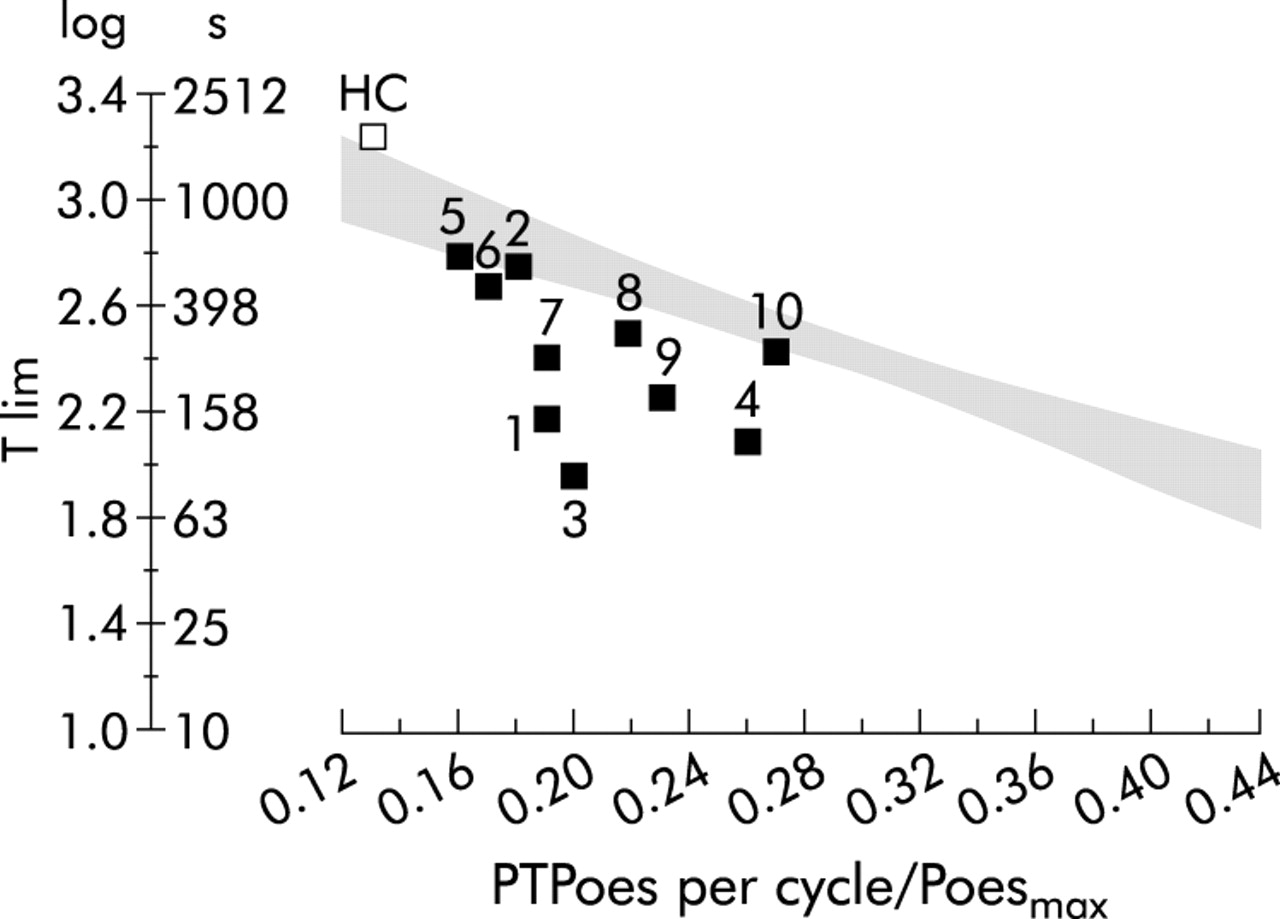
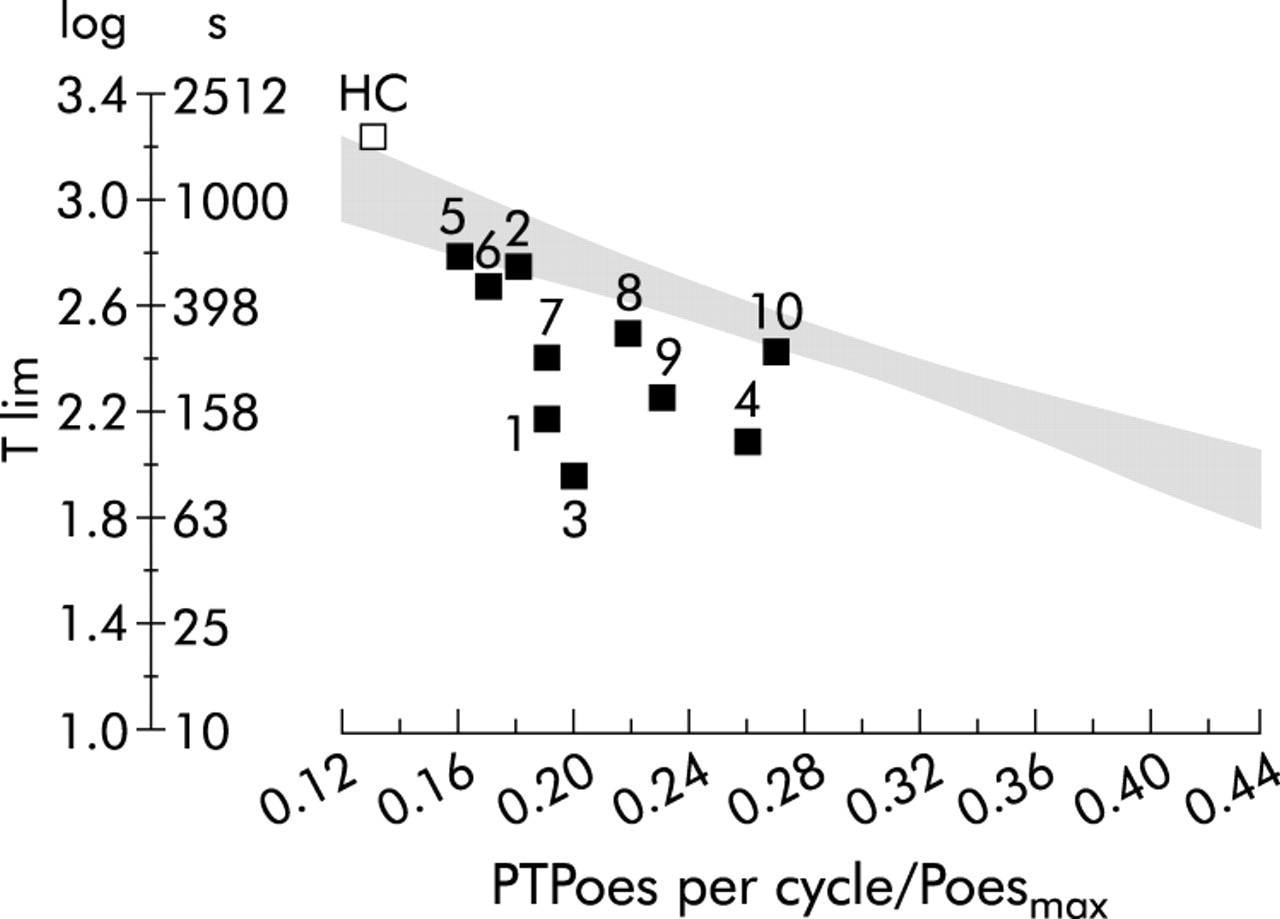
By plotting log Tlim against PTPoes per cycle/Poesmax, the inspiratory muscle endurance of patients with CHF was directly compared with the modified regression equation for normal controls (fig 1). The mean log Tlim for the patients with CHF was 86.7 (8.9)% predicted (range 69.8–96.0), with only three of the 10 patients having a value of less than 85% predicted (patients 1, 3 and 4; fig 1). Therefore, despite the fact that the CHF group had a substantial reduction in Tlim compared with controls set at a similar target negative pressure, Tlim was nearly appropriate when expressed as a function of the PTPoes per cycle/Poesmax. Finally, direct correlation was observed between percentage predicted log Tlim and Poespeak/TTPoespeak (r = 0.62, p = 0.05), which suggests that a slower inspiratory muscle contraction rate is observed during loaded breathing in patients with CHF.
{kind=link}
Plot of endurance time (log Tlim and Tlim) against the inspiratory muscle load to capacity ratio (PTPoes per cycle/Poesmax) in 10 patients with chronic heart failure. The shaded area represents the regression equation and 95% confidence bands, which has been modified from previous published data.12 Although the healthy controls (HC) exposed to 40% Poesmax do not fit the regression equation as these subjects did not reach task failure, the mean value for this group has been added for comparison. Patients 2, 5, 6, 7, 8, 9 and 10 had a log Tlim of ⩾85% predicted.
DISCUSSION
In patients with moderate symptomatic heart failure, endurance time was greatly reduced primarily as a consequence of the breathing strategy adopted, which caused an increase in the inspiratory muscle load relative to the inspiratory muscle capacity. However, given this ventilatory pattern, most of the patients with heart failure sustained an endurance time that was nearly appropriate for the inspiratory muscle load to capacity ratio, suggesting that task failure is not due to poor endurance characteristics of the inspiratory muscles.
Critique of method
Comparison with previous studies
Two separate methods have previously been used to assess inspiratory muscle endurance in CHF.14,15 Both studies showed an overall reduction in endurance, and both suggested that the likely cause was an increase in the inspiratory muscle load.15 Mancini et al15 used an incremental isocapnic voluntary ventilation test. Despite this volume loading method being well tolerated and demonstrating a lower maximal sustainable ventilatory capacity in patients with CHF, this technique is limited when applied to CHF patients with evidence of airflow obstruction. Indeed, although lower in heart failure, when maximal sustainable ventilatory capacity was normalised for FEV1 there was little difference between patients with CHF and controls. To overcome the influences of respiratory frequency and underlying airways disease inherent in the volume loading tests,22 Walsh et al14 used an incremental pressure loading technique.23 However, subsequent studies have questioned the usefulness of such incremental tests, as incremental loading tasks have a substantial learning effect24 and may reflect strength more than endurance.25 Incremental tests take no account of breathing strategy and therefore do not accurately reflect the load on the inspiratory muscles, a problem that is overcome if endurance time is expressed as a function of the inspiratory muscle load to capacity ratio.12
Why set the threshold pressure level at 40% of maximal?
In our previous studies a threshold pressure of 70% Poesmax was used.12,13 However, consistent with the study of Hammond et al,4 we observed that patients with CHF reached task failure prematurely at much lower target pressures. Accordingly, we determined from pilot studies that 40% Poesmax was the highest threshold pressure that was acceptable to the patients and allowed them to achieve an endurance time of a sufficient duration to assess inspiratory muscle endurance satisfactorily. Furthermore, as the PTPoes per cycle/Poesmax values observed in patients with CHF at the 40% Poesmax threshold level were numerically comparable to those observed in normal subjects exposed to a 70% Poesmax threshold level, additional comparisons could be made between CHF patients and normal subjects (fig 1).
Significance of findings
Factors influencing Tlim
A higher PTPoes per cycle/Poesmax has been shown to be associated with a reduced Tlim in normal subjects.12 In the current study a different breathing strategy was adopted in CHF patients, reflected as an increased RR, reduced Te, and therefore increased Ti/Ttot with little difference in Ti. Consistent with this trend, during exercise heart failure is characterised by an increase in Ve, RR,26–28 and Ti/Ttot.29 Although preservation of Ti in patients with heart failure allows an adequate Vt to be maintained and gas exchange to occur, this is at a cost since, to accommodate the increase in Ve, RR increases and Te falls resulting in increased Ti/Ttot. This adversely impacts on muscle energetics by reducing the time available for recovery before the onset of another inspiratory contraction.30 Thus, in the present study, Tlim was reduced in CHF patients as a consequence of the increased inspiratory muscle load to capacity ratio.
This increase in Ti/Ttot may be an indirect result of a reduction in Cldyn. Similar to previous studies,31,32 lung compliance was decreased in patients with CHF compared with controls, and although this degree of reduction in lung compliance only accounts for part of the higher inspiratory muscle load to capacity ratio observed in patients with heart failure, the increased respiratory system impedance associated with the reduction in lung compliance would increase the central inspiratory motor output and modify breathing strategy.33 In fact, the mechanical constraints imposed by lung stiffness in CHF may necessitate the preferential increase in RR rather than Vt. These data suggest that the high intrinsic load in CHF contributed, in part, directly to the increase in the inspiratory muscle load, but the indirect effects on breathing pattern had a greater influence on the magnitude of the inspiratory muscle load. Since this breathing pattern resulted in a reduction in Tlim in CHF patients compared with healthy controls exposed to the same relative load, it could be considered as a maladaptive ventilatory response to high inspiratory loads.
Inspiratory muscle endurance in CHF
Although the patients with CHF had a reduction in Tlim compared with healthy controls exposed to a similar inspiratory negative pressure, compared with healthy controls with similar PTPoes per cycle/Poesmax values the CHF patients had Tlim values that were largely appropriate for the inspiratory muscle load to capacity ratio, indicating preservation of the endurance properties of the inspiratory muscles. In addition, a slower inspiratory muscle contraction rate was observed in patients with CHF which may be a reflection of the fact that the diaphragm of patients with heart failure has increased numbers of slow type I endurance fibres and decreased fast type II strength fibres.34 The relevance of these findings in vivo is supported by data from our laboratory showing a shift to the left of the force-frequency curve in the diaphragm, an adaptation also consistent with a relative increase in endurance fibres.9
The effect on cardiac function of decreasing pleural pressures during inspiratory manoeuvres and of positive pleural pressures during ventilatory assistance is well documented.35–40 A more negative (subatmospheric) pressure during inspiration causes an increase in left ventricular afterload by increasing the transmural pressure across the left ventricular wall, and consequently results in a fall in the left ventricular output. Although we did not measure central haemodynamic responses, inspiratory threshold loading would be expected to cause a reduction in cardiac output and have a deleterious effect on inspiratory muscle function.41,42 However, in the current study CHF patients developed a breathing strategy that counterbalanced the adverse effect of large inspiratory negative pleural pressure on cardiac output by generating a more positive pleural pressure in expiration compared with the control subjects (Poesexp was subatmospheric in the controls), which would reduce afterload and increase cardiac output—an effect that would preserve inspiratory muscle function. Although a positive pressure in expiration can be a consequence of either increased abdominal muscle activity or an indicator of dynamic hyperinflation, the patients with CHF had an FEV1/FVC ratio similar to the healthy controls and we therefore presume that the Poesexp was a direct reflection of compensatory expiratory muscle activity. Nevertheless, this positive impact on cardiac output would be offset by the negative effect on muscle energetics due to the forced expiratory phase causing a reduction in Te and therefore a decrease in inspiratory muscle rest before the next inspiratory contraction.
Clinical significance
Previous data14,15 have shown that inspiratory muscle endurance is reduced in heart failure and is a possible cause of reduced exercise performance. Some studies have suggested an increase in inspiratory muscle load relative to inspiratory muscle capacity as a cause of dyspnoea and exercise intolerance,10 while other studies have reached contrasting conclusions.43 The findings of the current study indicate that, although endurance time is greatly reduced in heart failure, this is because patients with CHF adopt a maladaptive breathing strategy with a prolonged Ti/Ttot. These data support the clinical findings of Bernardi et al44 that respiratory pattern training techniques, which aim to modify the maladaptive breathing pattern and impose a more physiologically effective breathing strategy, alleviate dyspnoea and improve exercise tolerance in patients with CHF. Furthermore, this approach is consistent with our observation in normal subjects that changing breathing strategy can alter Tlim but without modifying inspiratory muscle endurance, when Tlim is expressed as a function of PTPoes per cycle/Poesmax.12
In conclusion, endurance time is significantly shorter in patients with CHF due to the breathing pattern adopted, which results in an increase in the inspiratory muscle load relative to the inspiratory muscle capacity. However, when inspiratory muscle endurance is expressed as a function of endurance time and the inspiratory muscle load to capacity ratio, the endurance properties of the inspiratory muscle are relatively well preserved in CHF. Maladaptive breathing strategies resulting in an increase in inspiratory muscle load are the principal contributors to task failure during loaded breathing in CHF rather than the strength or endurance of the inspiratory muscle pump.
REFERENCES
Footnotes
-
NH was funded by the Dorothy Osbourne Legacy (Royal Brompton Hospital Trust Fund). MIP’s research group receives support from the British Heart Foundation.
Linked Articles
- airwaves