Article Text

Abstract
Background: There is conflicting information about the relationship between asthma and socioeconomic status, with different studies reporting no, positive, or inverse associations. Most of these studies have been cross sectional in design and have relied on subjective markers of asthma such as symptoms of wheeze. Many have been unable to control adequately for potential confounding factors.
Methods: We report a prospective cohort study of approximately 1000 individuals born in Dunedin, New Zealand in 1972–3. This sample has been assessed regularly throughout childhood and into adulthood, with detailed information collected on asthma symptoms, lung function, airway responsiveness, and atopy. The prevalence of these in relation to measures of socioeconomic status were analysed with and without controls for potential confounding influences including parental history of asthma, smoking, breast feeding, and birth order using cross sectional time series models.
Results: No consistent association was found between childhood or adult socioeconomic status and asthma prevalence, lung function, or airway responsiveness at any age. Having asthma made no difference to educational attainment or socioeconomic status by age 26. There were trends to increased atopy in children from higher socioeconomic status families consistent with previous reports.
Conclusions: Socioeconomic status in childhood had no significant impact on the prevalence of asthma in this New Zealand born cohort. Generalisation of these results to other societies should be done with caution, but our results suggest that the previously reported associations may be due to confounding.
- asthma
- socioeconomic status
- birth cohort
- childhood
Statistics from Altmetric.com
The prevalence of asthma in the developed world has increased over recent decades. At least part of this increase is real and not due to changes in diagnostic practices.1–7 This increase in genetically stable populations must be due to environmental or lifestyle factors. Since asthma is more common in westernised/wealthy nations, the increases in prevalence within these countries suggest that asthma may be a disease of affluence.8–10
Within countries there have been many attempts to relate the prevalence of asthma and atopy to socioeconomic status (SES). Unlike atopy, which is more common in higher SES groups,11 the evidence for socioeconomic patterning in asthma is conflicting.12,13 Studies have found both increased14–16 and decreased17–21 prevalence of asthma in higher SES groups, while other studies have found no relationship.22–24
There may be several explanations for these findings, including the methodology of the studies. The use of symptoms such as wheeze and cough to indicate asthma may be misleading. This may be because of the occurrence of non-asthmatic wheeze and cough (due to bronchitis, for example) or because of differences in reporting of these symptoms between socioeconomic groups.25–29 Alternatively, physician diagnosis and treatment of asthma may differ between economic groups leading to either an apparent increase in prevalence in those with better access to care or an apparent increase in asthma severity in those with inadequate treatment.12 Finally, it is probable that SES interacts with specific environmental factors to have different effects on asthma prevalence in different populations. For example, less affluent people in the USA have greater exposure to cockroaches and therefore may have more asthma symptoms due to cockroach allergy.30–32 House dust mites are more important in other populations and exposure may be greater in higher SES homes.31,33
Clouding the issue further, many studies of SES have been cross sectional and most have been restricted to children. We report a longitudinal cohort study from birth to age 26 that recorded both subjective and objective measures of asthma and atopy to examine the relationship between SES and asthma.
METHODS
Participants
The Dunedin Multidisciplinary Health and Development Study is a longitudinal investigation of health and behaviour in a birth cohort.34 Study members were born in Dunedin, New Zealand between April 1972 and March 1973. Of these, 1037 children (91% of eligible births; 52% male) participated in the first follow up assessment at age 3, constituting the base sample for the remainder of the study. Cohort families represent the full range of SES in the general population of New Zealand and are primarily white of European descent. Follow up assessments occurred at ages 5, 7, 9, 11, 13, 15, 18, 21, and at age 26 years when we assessed 980 (96%) of 1019 study members still alive. The study was approved by the Otago ethics committee and written informed consent was obtained at each assessment.
Measurements of socioeconomic status (SES)
The primary measures of SES used in this study were based on the scale of Elley and Irving.35 The scale places each occupation into one of six categories (6 = unskilled labourer, 1 = professional) based on the educational levels and income associated with that occupation in data from the latest New Zealand census.
Childhood SES
Socioeconomic conditions may change during childhood, and rather than take the measurement from a single point at birth or early in life, we calculated childhood SES as the average of the higher SES level of either parent, assessed repeatedly from the study member’s birth through to age 15 (n = 1031). Although homemakers, unemployed, and students are not classified, only six study members could not be assigned an SES category between birth and age 15. The distribution of SES classifications was 1–1.9 = 14.3%; 2–2.9 = 19.9%; 3–3.9 = 34.8%; 4–4.9 = 23.2%; 5–6 = 7.2%.
Adult SES
To address the issues of whether adult SES has an impact on current asthma, and also whether the experience of asthma during childhood impacts on adult SES, the adult SES score was measured according to the study member’s own Elley-Irving category at age 26 (n = 934, the remaining cohort seen at 26 were homemakers, students, or unemployed and were omitted).35
Alternative measures of SES
Parental income taken as the total income of both parents recorded on two occasions (ages 13 and 15) and expressed as the mean of the totals at these ages (n = 955) was used as an alternative measure of childhood SES. The highest level of educational achievement by age 26 (1 = no qualifications; 2 = school certificate only (the most basic New Zealand qualification); 3 = higher level school qualification (e.g. sixth form certificate), or post-school qualification (e.g. trade certificate diploma); 4 = bachelors degree or higher) was used as an alternative measure of adult SES (n = 980).
Outcome measures
Asthma, wheeze and cough
At age 9 the accompanying adult (usually mother) answered questions on current wheezing and coughing symptoms and also provided a retrospective history of respiratory symptoms and illnesses since birth. The frequency, severity, trigger factors, and treatment of symptoms were recorded, including whether a diagnosis of asthma had been made.36 At age 11, 13, and 15 questions were asked regarding symptoms since the last assessment. At age 18, 21, and 26 a self-administered questionnaire,37 to which we added questions from the American Thoracic Society questionnaire,38 was completed by the study member before the interviewer administered questionnaire.
Current asthma was defined as diagnosed asthma with symptoms in the previous year. Current wheeze was defined as all reported wheezing, excluding those with only one or two episodes of wheezing each lasting for less than 1 hour in the previous year. Asthma treatment included any bronchodilator, corticosteroid, or cromoglycate medication.
Lung function and airway responsiveness
Spirometric tests were performed at each assessment from age 9, recording the best of three acceptable forced expiratory manoeuvres without prior bronchodilator (within 6 hours). At 18 and 26 bronchodilator responsiveness was measured by repeating the spirometric tests 10 minutes after nebulised or metered dose salbutamol (200 μg) via a large volume spacer. At ages 9, 11, 13, 15, and 21 a methacholine challenge was performed using a modified Chai protocol39 as previously described and validated.40 Five deep inhalations of methacholine 0.025 mg/ml were administered through a Hudson Updraft nebuliser and spirometric tests were repeated after 30 seconds and 2 minutes. Provided the forced expiratory volume in 1 second (FEV1) fell less than 20%, further methacholine was administered at concentrations of 0.25, 2.5 and 25 mg/ml. The procedure was stopped when FEV1 fell by 20%, if there were symptoms of concern, or after the final concentration. The provoking concentration causing a 20% fall in FEV1 (PC20) was determined by linear interpolation. A PC20 of 8 mg/ml or less was regarded as increased airway responsiveness. Study members showing airflow obstruction at baseline (FEV1/FVC <75% at 9 and 11 years or <70% at older ages) were not challenged but instead were retested after salbutamol. An increase in the FEV1 of 10% of baseline or more was regarded as indicating bronchodilator airway responsiveness.
Atopic status
Skin prick testing was undertaken at age 13 in 714 study members using house dust mite (Dermatophagoides pteronyssinus, Bencard, UK), grass, cat, dog, horse, kapok, wool, Aspergillus fumigatus, Penicillium, and Cladosporum (Hollister-Stier, USA).41 These were repeated at age 21 in 885 study members with the addition of cockroach allergen (Hollister-Stier, USA). A positive response was defined as a weal diameter 2 mm greater than the negative control. Serum IgE was measured at ages 11 and 21 in 571 and 786 study members, respectively.42 IgE values were log-transformed before analysis to approximate a normal distribution.
Control variables
Parental asthma
The adult attending with the study member at age 7 was asked whether the natural mother and father had asthma, hay fever, or allergies.43 This information was obtained again from the study member at age 18. Preference was given to the information obtained at age 7 if available.
Cigarette smoking
Current smoking was defined as smoking daily for at least 1 month of the previous year. Parental smoking during the study member’s life was ascertained at ages 9, 11 and 13 from the accompanying parent and used as an indicator of likely exposure to environmental tobacco smoke. Whether the study member’s mother had smoked during pregnancy was asked at age 9.
Breast feeding
At the age 3 assessment parents were questioned about breast feeding and its duration. Study members were classified according to whether they had been breast fed for longer than 3 weeks.44 The accuracy of recall of the duration of breast feeding was validated by comparison of data recorded prospectively by infant healthcare workers.45
Birth order
Birth order was categorised according to whether the study member had no, one, two, or three or more older siblings.
Statistical analysis
Analyses of the effects of childhood SES were performed using the “xt” procedures of the Stata 8.0 software package (Stata Corporation, TX) for cross sectional, time series datasets (generalised estimating equations). Continuous variables were analysed using the xt regression model and binary outcomes by the xt logit model. Analyses were undertaken using asthma, atopy, FEV1/FVC ratio, and log IgE levels as dependent variables and childhood SES as the independent variable. All analyses included a term for the age of measurement and were adjusted for sex. Analyses were repeated with adjustment for potential covariates including family history of asthma, smoking, breast feeding, birth order, maternal smoking during pregnancy, and the presence of a smoker in the household. Analyses of the effect of childhood asthma (up to the age of 15) on adult (age 26) SES and of adult SES on adult asthma outcomes were performed using linear or logistic regression. p values of <0.05 were regarded as statistically significant.
RESULTS
Childhood SES
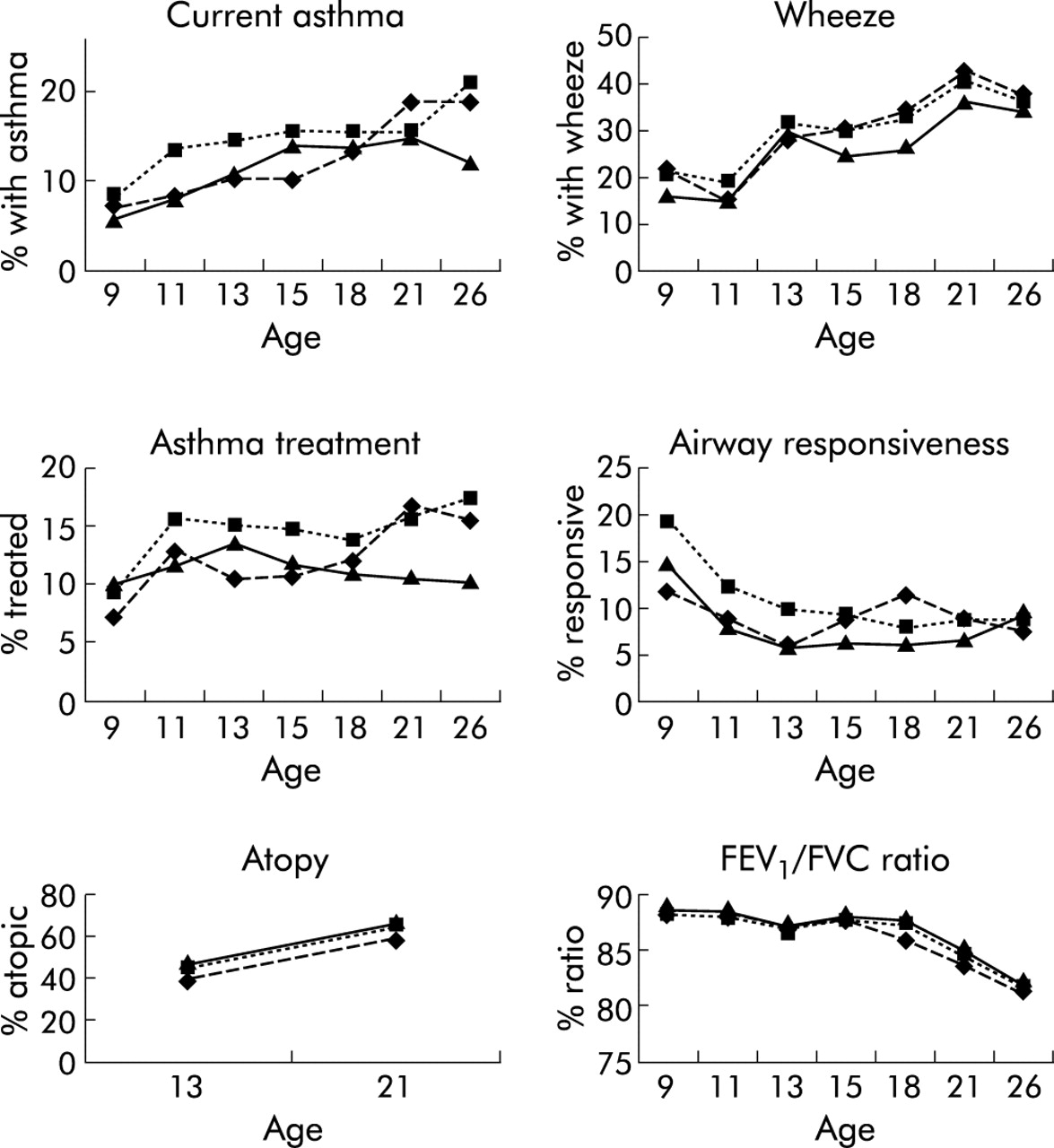
The prevalence of asthma, wheeze, asthma treatment, airway responsiveness, atopy, and the mean FEV1/FVC ratio at each age for high, medium, and low Elley-Irving childhood SES groups are shown in fig 1. These indicate no consistent pattern of association between SES and the asthma outcomes measured. Cross sectional time series analyses also indicate no significant associations between mean childhood SES and a diagnosis of asthma, wheeze, asthma treatment, time off school or work for asthma, lung function, or airway responsiveness to methacholine or salbutamol in either the analyses adjusting for sex alone, or the analyses adjusting for other covariates (table 1).
Odds ratios, coefficients and 95% confidence intervals from cross sectional time series analyses of asthma, wheeze, asthma treatment, time off school/work due to asthma, bronchial responsiveness, atopy, FEV1/FVC ratio, and log serum IgE on childhood socioeconomic status (SES; 1 = professional, 6 = manual labourer)

{kind=link}
Prevalence of asthma, wheeze, asthma treatment, airway responsiveness, atopy, and spirometric values in high (mean Elley Irving score ⩽2, ▴), medium (mean score 2–4, ▪) and low (mean score ⩾4–6, ♦) childhood socioeconomic status (SES) groups.
There was a trend towards increased atopy on skin prick testing (any skin prick test positive) with increasing childhood SES (p = 0.044), but this was no longer significant after controlling for birth order, family smoking, smoking during pregnancy, and breast feeding (p = 0.084). There were no significant associations between SES and log serum IgE.
Total parental income at ages 13 and 15 was not associated with current asthma, significant wheeze, asthma treatment, lung function, atopy, serum IgE, or airway responsiveness in either the analyses adjusting for sex alone or the analyses adjusting for other covariates.
Adult SES
The study member’s own SES and educational achievement by age 26 were not significantly associated with current asthma, doctor diagnosed asthma, current wheeze, time off work due to asthma, or bronchodilator response at age 26. Significant associations between being woken by a cough at 26 and both adult SES and educational status in unadjusted analyses were not significant after adjustment for current smoking (data not shown). The FEV1/FVC ratio tended to be lower in those with lower educational achievement (p = 0.026) and lower SES (p = 0.071), but these were not significant in the fully adjusted analyses (p = 0.13 and 0.16, respectively).
Impact of asthma on adult SES and educational achievement
There were no significant associations between a diagnosis of asthma in childhood and the educational achievement or adult SES of the study member at age 26, even after adjusting for childhood SES.
DISCUSSION
This study found no convincing evidence of an association between childhood SES and asthma at any age from childhood to early adulthood. The findings were consistent whether we used parental occupation or parental income as the measure of childhood SES. Furthermore, adult SES had no influence on adult asthma, and a diagnosis of asthma in childhood had no impact on educational achievement or adult SES. Our findings with regard to asthma contrast with those for other health problems in this cohort in which significantly worse adult health occurred in those who grew up in a low SES background.46
There was a significant trend to increased atopy with higher childhood SES. This was not statistically significant after adjusting for potential confounding factors, but is consistent with the findings of other studies.11 We did not find any significant association between serum IgE and SES.
This study addresses some of the problems which limit the interpretation of previous studies. Firstly, we have prospectively collected data throughout childhood into early adulthood, allowing a search for consistent associations between SES and asthma at different ages. Secondly, objective measures of lung function and airway responsiveness were performed as well as subjective measures of asthma such as symptoms, doctor diagnosis, and treatment. We can therefore discount apparent differences in the prevalence of asthma due to selective reporting of symptoms, differences in diagnostic practice, or access to care. Thirdly, detailed information was available on known and potential confounders such as smoking during pregnancy, parental asthma, parental smoking (indicating likely exposure to environmental tobacco smoke), birth order, and breast feeding.
Although we have identified no relationship between SES and asthma from childhood to early adulthood, this does not preclude an association during later life. There was a trend to a reduced prevalence of asthma and less asthma treatment in those from advantaged socioeconomic backgrounds by age 26 (fig 1). However, this trend was not apparent for wheeze, airway responsiveness, or lung function and was in the opposite direction to the trend observed for atopy.
The generalisability of our findings to other populations is unclear. In common with any study of social conditions and health, the findings may not apply to societies in which social conditions differ markedly. Although the Dunedin cohort represents the entire socioeconomic spectrum of New Zealand, the range and nature of the socioeconomic disparities may be less or greater in other countries. In addition, issues relating asthma to SES may differ across countries. For example, poor housing in the USA may expose children to high levels of cockroach allergen. In this cohort cockroach allergy was less common than allergy to house dust mite (unpublished). Exposure to house dust mite is likely to be universal in a city such as Dunedin.47 Nevertheless, we believe that this study is the most comprehensive examination of the relationship between asthma and socioeconomic conditions to date. Data from surveys in other countries should be interpreted in the light of the methodological issues that we have raised.
Acknowledgments
We are grateful to the study members and their parents for their continued support. We also thank Air New Zealand and Dr Phil A Silva, the study founder.
REFERENCES
Footnotes
-
The Dunedin Multidisciplinary Health and Development Research Unit is funded by the Health Research Council of New Zealand. The respiratory section of the study was funded by the Health Research Council, the Otago Medical Research Foundation, the New Zealand Lottery Grants Board, and the Asthma Foundation of New Zealand.
Linked Articles
- airwaves