Article Text

Abstract
Background: One postulated cause of the sudden infant death syndrome (SIDS) is upper airway obstruction during sleep. Several studies have suggested that SIDS may be more common in families with obstructive sleep apnoea/hypopnoea syndrome (OSAHS), but were limited by uncertainty as to whether the deaths were due to SIDS. We have tested the hypothesis that parents of true SIDS cases have an increased frequency of apnoeas and hypopnoeas during sleep.
Methods: The parents of 269 rigorously determined SIDS cases were invited for single night polysomnography and daytime ventilatory control measurement.
Results: Parents of 198 cases were identified but 152 did not respond or declined. Fifty five parents of 34 cases were studied and matched for age, height, and weight to 55 subjects from general practice registers. There was no difference in breathing during sleep between the parents of SIDS cases (median (IQR) 5.9 (3.2, 10.7) apnoeas+hypopnoeas/h) and controls (6.7 (4.0, 12.2) apnoeas+hypopnoeas/h; p = 0.47), but the SIDS parents had lower minimum nocturnal oxygen saturation (median (IQR) 92 (89, 93)%) than controls (92 (90, 94)%; p = 0.048). There were no major differences in control of breathing when awake between SIDS parents and controls.
Conclusions: These results provide no evidence to support an association between SIDS and OSAHS. However, the minor impairment of oxygenation during sleep in SIDS parents requires further study.
- obstructive sleep apnoea/hypopnoea syndrome
- sudden infant death syndrome
- genetics
- AHI, apnoea/hypopnoea index
- fR, respiratory frequency
- OSA, obstructive sleep apnoea
- OSAHS, obstructive sleep apnoea/hypopnoea syndrome, Sao2, oxygen saturation
- SIDS, sudden infant death syndrome
- Te, expiratory time
- Ti, inspiratory time
- Ve, minute volume
- Vt, tidal volume
Statistics from Altmetric.com
- AHI, apnoea/hypopnoea index
- fR, respiratory frequency
- OSA, obstructive sleep apnoea
- OSAHS, obstructive sleep apnoea/hypopnoea syndrome, Sao2, oxygen saturation
- SIDS, sudden infant death syndrome
- Te, expiratory time
- Ti, inspiratory time
- Ve, minute volume
- Vt, tidal volume
The sudden infant death syndrome (SIDS) is a condition of unknown aetiology and is the most common cause of death in babies under the age of 1 year.1 There have been many theories about the cause of SIDS,1 including disorders of cardiac, respiratory and thermal control, but most are based on anecdote or association and none have been proved to cause many of these tragic deaths.
One theory is that SIDS may be caused by obstructive apnoeas in infants who die because they fail to arouse. There is some evidence in favour of this hypothesis including:
-
a small increase in obstructive apnoeas in infants who subsequently die of SIDS;2
-
upper airway narrowing in SIDS cases3 and in cases of “near miss SIDS”;4
-
similar facial characteristics in SIDS cases and in non-obese patients with sleep apnoea/hypopnoea syndrome (OSAHS), with back setting of the maxilla;3
-
the subsequent development of obstructive sleep apnoea in cases of “near miss SIDS”;5
-
an increased frequency of reported SIDS in family members of patients with OSAHS.6,7
However, these data are suggestive rather than conclusive. The studies suggesting an increased frequency of SIDS in the family members of patients with OSAHS6,7 may be affected by recall bias, with OSAHS patients being more likely than normal subjects to have asked relatives about unexplained deaths during sleep. In addition, these studies are retrospective and the possibilities of other causes of death in SIDS cases cannot be excluded, despite attempts to do so.6,7
We therefore tested the hypothesis that, if SIDS is caused by obstructive sleep apnoea (OSA) in children and is familially related to OSAHS, then the parents of true SIDS cases would have an increased frequency of apnoeas and hypopnoeas during sleep.
METHODS
Sleep histories and overnight polysomnography were obtained for parents of SIDS cases and age, sex, height and weight matched controls. The study was approved by the local medical ethical advisory committees and all subjects gave written informed consent.
Case selection
SIDS cases were identified by the specialist pathologist in SIDS in the departments of paediatric pathology at the Royal Hospital for Sick Children, Edinburgh and Yorkhill Hospital, Glasgow during the period 1987–98. In all SIDS cases known causes of sudden infant death which are identifiable after death had been excluded by expert medical examination and the Procurator Fiscal led confidential enquiries including detailed post mortem examination with cultures, pathological evaluation, neuropathology, appropriate electromicroscopy, enzyme, toxicological investigations, and whole body radiology. The parents of 269 consecutive SIDS cases were invited to participate (fig 1), all approaches being made through the family practitioner of the SIDS victim at the time of death. The parents of 57 of the SIDS cases could not be traced by the family practitioner and the family practitioners indicated that the parents of 14 cases should not be contacted for emotional reasons. The parent(s) of the remaining 198 SIDS cases were still registered with their family practitioner but 125 parent pairs did not respond to our two letters of invitation, 25 parent pairs were identified by the postal service as having moved away, the parents of two cases declined to participate, and 12 pairs agreed to take part but did not attend for their sleep studies. Fifty five parents of 34 SIDS cases therefore participated in the study.

Subject recruitment to the study.
Controls were obtained from family practice registers and matched with the parents studied on a one to one basis for sex, age within 5 years, height to within 5 cm, and weight to within 5 kg. Each was approached by an independent research guardian and asked to participate in an unspecified medical research study. One hundred and thirty three possible subjects were approached before 55 suitable controls agreed.
Protocol
All SIDS parents and control subjects and their partners underwent overnight polysomnography using Compumedics S system (Compumedics, Australia) and our normal techniques.8 All had their height and weight measured. SIDS parents and controls were invited to have lateral cephalometry to determine upper airway dimensions and facial bone structure.9
The subjects were asked to return for a further half day when the ventilatory responses to hypoxia and hypercapnia were measured by dynamic end tidal forcing using our standard techniques.10 Isocapnic hypoxia (saturation 85%) was maintained for 7 minutes. The isoxic hypercapnic response was measured using step changes of 0.5 and 1.5 kPa in end tidal Pco2. Finally, the response to an added inspiratory/expiratory resistive load (14 cm H2O/l/s) was measured.
Analysis techniques
Sleep,11 breathing,12,13 and cephalograms9 were scored manually using the referenced standard definitions, all by observers blinded to case/control status. Respiratory variables were averaged over 2 minute periods before both the hypoxic and hypercapnic responses and also before and at the end of resistive loading. The hypoxic ventilatory response was expressed as the Ve/saturation (Ve/Spo2: l/min/%) relationship10 and the hypercapnic response was expressed as the Ve/Petco2 (l/min/kPa) relationship and intercept B (kPa).14
Analysis of data
Data were analysed using the two tailed paired t test or Wilcoxon rank sign test with Bonferroni correction for multiple comparisons, as appropriate. Results are expressed as mean (SD) or median and interquartile range (IQR), as appropriate.
RESULTS
Sleep studies
Fifty five SIDS parents and 55 control subjects had overnight polysomnography. There were no significant differences between the parents and controls for age (37 (6) years v 37 (6) years; p = 0.26), sex (parents 26M, controls 26M), height (1.69 (0.09) m v 1.69 (0.08) m; p = 0.15), or weight (75.9 (16.8) kg v 76.8 (16.2) kg; p = 0.19).
There was no significant difference in the apnoea/hypopnoea index (AHI) between parents and controls (median 5.9 (IQR 3.2, 10.7) apnoeas+hypopnoeas/h slept for SIDS parents v 6.7 (4, 12.2) apnoeas+hypopnoeas/h slept for controls; p = 0.48; table 1). SIDS parents had statistically significantly lower minimum nocturnal oxygenation (median 92% (IQR 89, 93) for parents v 92% (90, 94) for controls; p = 0.048). There was a trend towards more episodes of 4% O2 desaturation during sleep in the SIDS parents (p = 0.068). There was no difference between the groups in the time with oxygen saturation below 90%, in awake oxygen saturation, nor in arousals from sleep.
Results of sleep studies in parents of SIDS cases and controls
Cephalometry
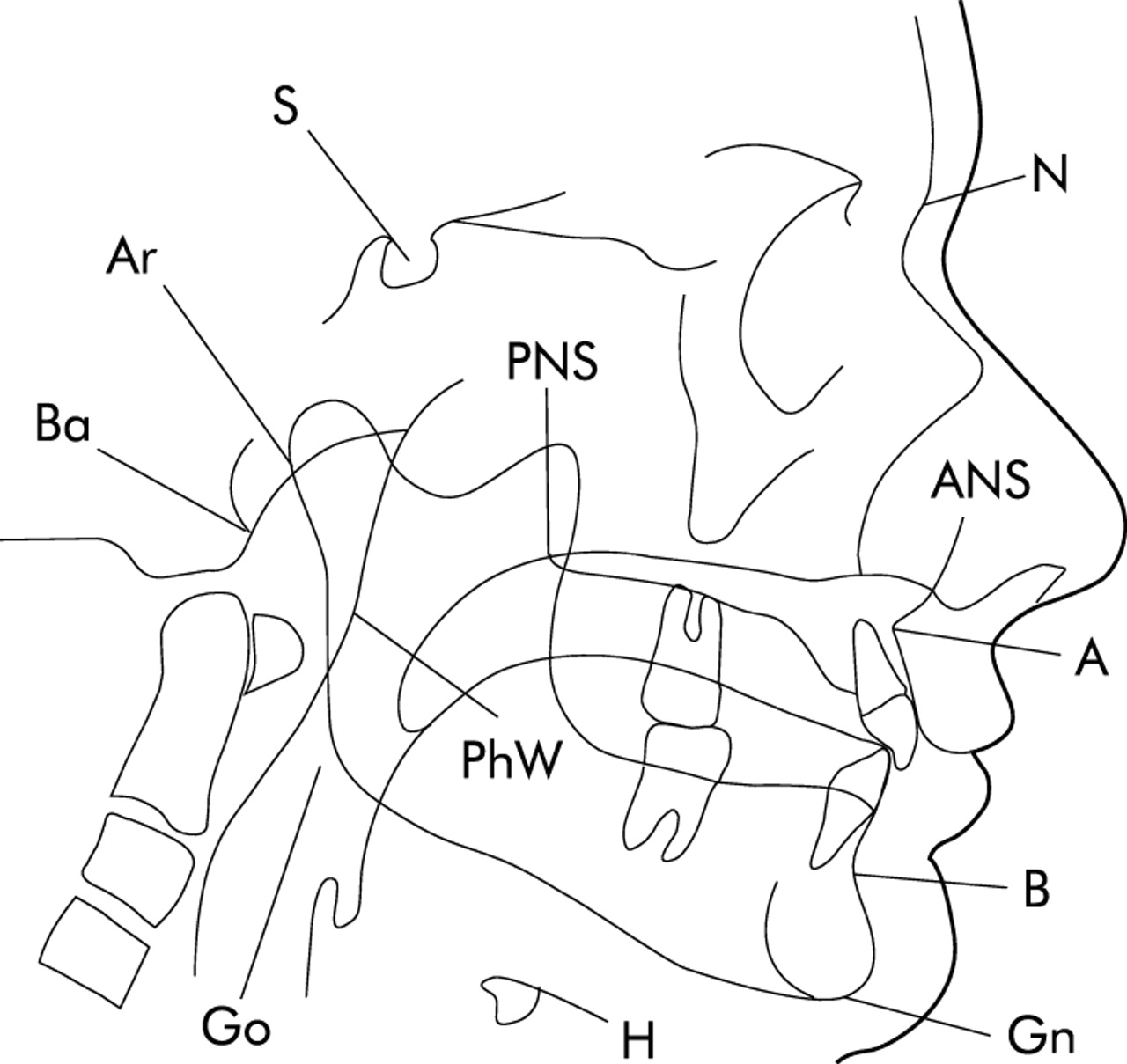
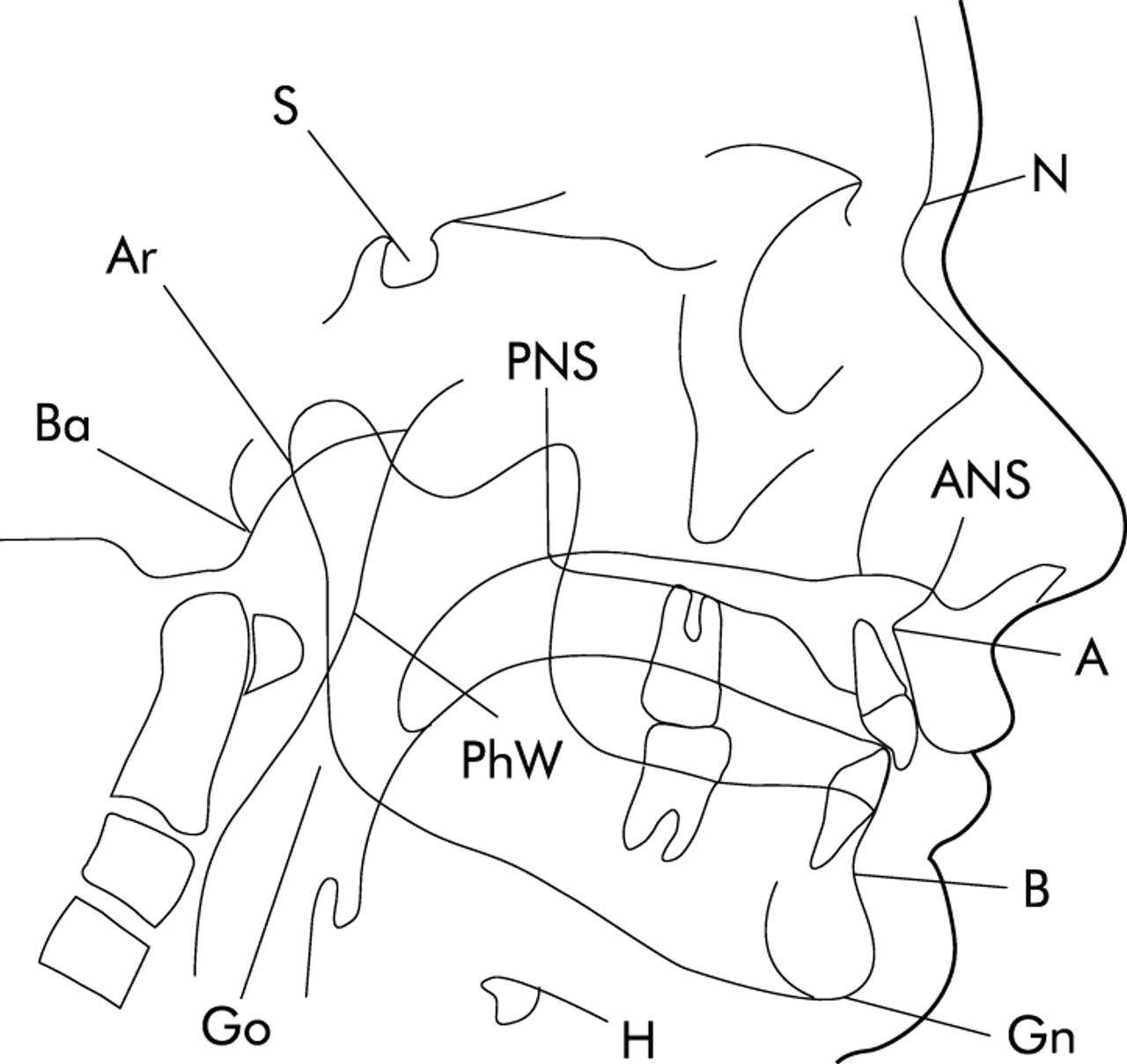
Cephalometry was performed in 44 of the 55 matched pairs; at least one member of the other 11 pairs declined the radiographic exposure. There was no significant difference in any skeletal length or angle between the two groups (table 2, fig 2), nor was there any evidence of cephalometric predispostion to upper airway narrowing in either sex of SIDS parents when comparisons were performed within the sex.
Mean (SD) cephalometric measurements in parents of SIDS cases and controls
{kind=link}
{kind=link}
Diagrammatic representation of cephalometry measurements. Go = gonion; Gn = gnathion; Ar = articulare; ANS = anterior nasal spine; PNS = posterior nasal spine; Ba = basion; H = hyoid; MP = mandibular plane; PhW = pharyngeal wall; S = sella; N = nasion; A = subspinale; B = supramentale.
Ventilatory responses
Nine pairs of subjects successfully completed ventilatory response testing. There were no significant differences in baseline end tidal gas tensions or ventilatory pattern at any time during the study between the two groups when breathing air, nor in hypoxic or hypercapnic responses (hypoxic response: median (IQR) −0.19 (−0.41, −0.10) l/min/% in parents, −0.13 (−0.67, −0.08) l/min/% in controls, p = 0.9; hypercapnic response: median (IQR) Ve/Petco2 7.69 (5.88, 19.70) l/min/kPa in parents, 7.70 (4.65, 15.1) l/min/kPa in controls, p = 0.3; intercept B: median (IQR) 4.06 (3.75, 4.57) kPa in parents of SIDS cases, 4.34 (3.65, 4.81) kPa in controls, p = 0.9). Following addition of the resistive load there was a significant reduction in inspiratory time (Ti), expiratory time (Te), and respiratory frequency (fR) and an increase in tidal volume (Vt) in both groups (table 3). There were significant differences between the controls and the patients in the resistive loading induced changes in Ti, Te, and minute volume (Ve) (table 3).
Effect of resistive loading
DISCUSSION
This study found no difference in the breathing pattern during sleep between parents of SIDS cases and control subjects. This finding is contrary to our original hypothesis and thus does not provide any evidence of a familial association between abnormal breathing during sleep in adults and SIDS in their children. Some of the previous evidence in favour of a possible association6,7 is circumstantial and possibly influenced by recall bias and uncertainty about the accuracy of the diagnosis of SIDS. The current study avoids these problems by being based on thoroughly investigated index cases of SIDS and on objective measurements of breathing during sleep. It also included scrupulous matching of the parents with community controls. Recent studies have given conflicting results with no evidence of a kinship relationship between OSAHS and SIDS in an Icelandic population study.15 An Australian study showed a much higher rate of OSAHS (19 out of 20) in infants from families where there were multiple histories of SIDS, apparent life threatening events, or OSA.16 However, they found a much lower frequency of OSA (31 of 105) in infants in whose family there had been only one case of SIDS or an apparent life threatening event. Furthermore, the follow up studies showed improvement in overnight sleep pattern in these infants with a resolution by 12 months of age. Our study in the parents of SIDS cases also showed no persisting abnormality in terms of irregular breathing in adult life in relatives of SIDS cases.
The significance of the marginally lower oxygen saturations during sleep in the SIDS parents is difficult to evaluate. However, it is of interest that reduced arousability from sleep has recently been reported in infants with apparent life threatening events.17 It is possible that the greater hypoxaemia permitted during sleep in the parents of SIDS cases reflects a decreased arousability to hypoxaemia. However, that was not the a priori hypothesis of this study and independent confirmation is required.
Despite previously reporting that babies who died of SIDS had back set maxillae3 and that families with OSAHS who reported possible cases of SIDS in their families had back set maxillae and mandibles,6 we did not find any difference in the facial structure between parents of SIDS cases and population controls. The sample sizes in this study (44 matched pairs for cephalometry) were much larger than in previous studies and ascertainment of the SIDS cases was much better than in the previous study in OSAHS families where SIDS was based on family members’ reports without inquiry or necroscopic confirmation. It therefore seems unlikely that there is any familial facial structure abnormality which predisposes to SIDS.
However, this study has significant limitations, including recruitment rates and power. Only 55 of a potential total of 542 SIDS parents were studied. Many of those not studied (n = 198) could not be traced or were considered by their family practitioners to be emotionally unsuitable for this study. Only 55 of the 332 parents contacted agreed to participate. This rate reflects a combination of the emotional sensitivity of the subject to many parents, the high number of young single parent families, the high number with social problems1 with resulting difficulties in participating, and the frequency with which young often single parents change addresses. We made very strenuous efforts within the limits of the sensitivity of the problem to maximise recruitment. We believe that the recruitment rate we obtained, while disappointing, was as high as could be ethically obtained among SIDS parents. We have no reason to believe the parents studied were different from those who did not participate, but have inadequate demographic information about these individuals (because of the sensitivity of the topic) to analyse this. The power of the study was adequate to determine significant differences in breathing during sleep or facial structure, but the number of subjects agreeing to participate in the ventilatory control studies limited the power of these observations as discussed below.
Another limitation is the number of statistical comparisons made (n = 35). This in no way detracts from the certainty of the negative observation on our a priori hypothesis that parents of SIDS cases would have more apnoeas and hypopnoeas than controls. It does, however, cast some doubt on the certainty of the six “statistically significant” differences observed as, by chance alone, two of the comparisons would have been expected to be significant (5% of 35). These results therefore need independent verification.
We found no difference between the two groups in either chemosensitivity (Ve/Petco2) or the threshold (B) for the ventilatory response to hypercapnia, or the chemosensitivity to hypoxia. Previous studies of chemosensitivity in parents of SIDS cases have produced conflicting evidence. Some groups have reported blunting of the hypoxic7 or hypercapnic18 drives whereas others, like ourselves, have found no evidence of reduced chemosensitivity in parents of SIDS cases compared with age matched controls.19 Failure to detect a difference between the two groups in our study could be due to a type 2 statistical error as we were only able to obtain measurements of ventilatory responses in nine subjects in each group. However, we observed no trend towards the substantially lower drives in the SIDS parents reported in other studies.7,18 Instead, both the hypoxic and hypercapnic responses were almost identical in the two groups. One possible cause of the conflicting findings might be the incidence of OSA in the SIDS parents since OSA itself may be associated with a reduced hypoxic ventilatory drive.20–22 OSA was a selection criterion for the parents studied by Tishler et al,7 whereas only one of our SIDS parents had more than 15 apnoeas+hypopnoeas/h slept.
Our studies confirm previous observations that there is no significant difference in resting breathing pattern between parents of SIDS cases and controls.19,23 The differences in the response to inspiratory/expiratory resistive loading, with SIDS parents showing a lesser response in terms of Ti, Te, and Ve, are difficult to assess as they were the only three significant changes found in 18 comparisons of breathing pattern between groups and were not a priori postulates. We studied only nine pairs of subjects in this component of the study and individuals vary in how they adapt to resistive loading.24 The results suggest possible differences in non-chemical ventilatory control in families of SIDS cases and merit further investigation.
REFERENCES
Footnotes
-
The study was supported by a grant from the Scottish Cot Death Trust and Dr P E Brander was supported by the Finnish Anti-Tuberculosis Association Foundation.
Linked Articles
- airwaves