Article Text

Abstract
Background: The effect of prophylactic nasal corticosteroids on wheezing episodes associated with colds was investigated in a 12 week parallel group, double blind, randomised controlled trial in preschool children.
Methods: Data were collected from 50 children aged 12–54 months with a history of at least three episodes of wheeze associated with colds over the previous winter, but few or no interval symptoms; 24 were given one dose of fluticasone aqueous nasal spray (50 μg) into each nostril twice daily and 26 received an indistinguishable placebo spray. Episodes of lower respiratory illness occurring within 2 days of the onset of a cold were identified from daily symptom diaries. The main outcome was nocturnal symptom score during the first 7 days of an episode.
Results: The groups were well balanced on entry except that the treatment group had a history of more prolonged episodes. During the trial there was no significant difference in the number of episodes in the treatment and control groups (27 and 37, respectively), in the severity of nocturnal symptoms (mean score 1.33 and 1.22, respectively, confidence interval of difference −0.24 to +0.47) or in daytime symptoms, activity or total scores during episodes. Compliance was estimated to be over 50% in 43 of the children.
Conclusions: Nasal corticosteroid treatment does not prevent acute wheezy episodes associated with upper respiratory infections (common colds) in preschool children.
- wheeze
- fluticasone nasal spray
- nasal corticosteroids
- children
Statistics from Altmetric.com
Seasonal episodes of wheeze and cough are common in preschool children, are disruptive to families, and costly to the National Health Service each winter in the UK. Clinical observation confirmed by virological evidence collected in school children has shown that a variety of viral upper respiratory tract (URT) infections (common colds) can initiate almost all of these lower respiratory tract (LRT) events.1 Most young children who experience these episodes, formerly known by the apt description “wheezy bronchitis”, do not progress to atopic asthma.2,3
Evidence for the extensive “cross talk” between the nose and lungs has recently been reviewed,4 but the precise mechanisms of the link between URT infection (common colds) and LRT symptoms have yet to be established. Although in experimental adult rhinovirus infections there is evidence of viral replication in the LRT,5 from what is known of rhinovirus biology it seems likely that the predominant site of viral activity is the nose. In an adult experimental model of viral wheeze due to human coronavirus6,7 there were marked differences in inflammation of the URT between wheezy and non-wheezy subjects, and very little evidence of viral replication in the LRT. If the LRT response to the common cold is at least partially mediated by indirect mechanisms rather than directly by infection of the LRT epithelium, it may be possible to ameliorate LRT symptoms in susceptible individuals by suppressing nasal inflammation. It is important to test this hypothesis, both because of potential advantages of direct URT treatment and because of the light it may shed on possible mechanisms in viral wheeze.
No experimental studies of this topic have been reported in adults or children. Certainly, prophylactic inhaled corticosteroids targeted at the lungs do not prevent acute episodes in children with pure viral episodic wheeze,8,9 although there is some evidence that high dose inhaled steroids at the onset of an episode may ameliorate some symptoms.10–12
Nasal corticosteroids reduce cytokine production and early symptoms in experimental rhinovirus infection in adults13 although, conversely, systemic steroids (the usual treatment for severe wheezy episodes) might potentiate viral replication.14 Another example of the possible benefits of nasal corticosteroids on the relationship between the URT and LRT is their effects on bronchial hyperresponsiveness (BHR) during seasonal rhinitis. Whereas nasal corticosteroids ameliorate both direct and indirect BHR in non-asthmatic subjects with rhinitis,15–18 orally inhaled corticosteroids have no effect18 which suggests an indirect (URT dependent) mechanism for BHR, potentially amenable to nasal therapy. The evidence is, however, inconsistent.19,20 Conversely, inhaled corticosteroids can ameliorate nasal symptoms in asthmatics with seasonal rhinitis.20
We set out to test the hypothesis that nasally administered fluticasone propionate in a dose shown previously to be safe and effective in children21–23 ameliorates the acute LRT symptoms associated with common colds in preschool children with a history of episodic viral wheeze in winter. We chose children without features of classical atopic asthma recruited from a primary care setting.
METHODS
Design of study
A 12 week double blind, randomised, parallel group design was used. Study numbers were assigned sequentially and drugs were prepacked in a block size of 4. Trial drugs were available in identical containers labelled only with the subject number. Decoding took place after all the data had been entered into the computer file.
Subjects
Children aged 12–54 months were selected for study from six suburban, small town, or rural general practices (i.e. from primary care). The initial letter from their general practitioner to all children in the appropriate age group who had been prescribed bronchodilators (but not inhaled steroids) over the previous 12 months sought those with at least three reported episodes of wheeze during the previous winter period (October–March inclusive). Of 903 letters sent, 288 replies (32%) were received and 211 (23%) were not recruited (38 (4%) on inhaled steroids, 173 (19%) refused). Only 77 (8.5%) were recruited to the trial, of whom 27 later dropped out (see later) leaving 50 subjects for analysis.
The trial was approved by Leicestershire Health research ethics committee and signed informed parental consent was obtained from each family before randomisation.
Trial procedure
Children were recruited at a home visit by the research nurse (MW). Baseline information about the child and family was recorded on an interview based questionnaire. The trial medication was provided and its administration explained. Three 4-week symptom diaries were provided. The severity of night time symptoms, daytime symptoms, and disruption of daytime activity were recorded once daily on a scale of 0–4 (table 1). A record was made of any symptoms suggestive of an intercurrent infection (fever, cold, sore throat, or ear infection). All medication and contacts with the general practitioner were recorded. There was space for additional notes or comments. No invasive procedures (blood or skin prick tests) or lung function tests were performed.
Symptom categories
Telephone contact was made every 2 weeks. Completed diaries and used trial medication were returned by post or collected from children’s homes at the end of the trial. Additional home visits were made where support was required.
The active treatment was fluticasone propionate aqueous nasal spray at a dose of 50 μg (one dose) to each nostril twice daily for 12 weeks. The inactive (placebo) preparation was identical in appearance and composition, omitting only the active corticosteroid.
Outcome assessment
The major outcome of interest was the night time symptom score during LRT episodes. Secondary outcome measures were daytime scores, activity scores, aggregate symptom scores, and number of episodes reported.
Episodes were defined by inspection of the diaries as an obvious increase in symptoms above baseline within 2 days of the reported onset of a cold, febrile episode, or other URTI. For statistical analysis the duration of each episode was taken as 7 days. Episodes occurring within 7 days of the start of the trial were discounted. Following an episode a further episode could be defined only after a period of 7 days at baseline symptom levels had elapsed. Although the definition was subjective, the diary cards were all scrutinised and categorised blind by a single observer (MS) before the code was broken.
Compliance with treatment was estimated by weighing the medication returned at the end of the trial.
Analysis of data
Based on data collected in previous trials,8,10 to identify a 40% reduction in nocturnal symptoms during episodes with 80% power and 5% significance level, 30 children would be required in each treatment arm. Although 77 children were recruited to allow for dropouts, data for only 50 were analysed leaving the trial underpowered to show a 40% reduction in symptoms.
The Mann-Whitney test was used to compare the numbers of LRT episodes experienced by the children in the two treatment groups. As a summary measure, the mean symptom scores over the entire period of the diary were calculated for each child and, after logarithmic transformation to approximately normal distributions, these were compared using the two sample t test. The mean night time, daytime, and activity scores were then calculated for each episode; each was not significantly different from normality (by Kolmogorov-Smirnov test); they were compared using a multilevel analysis with the MLn statistical computer package24 since several children suffered more than one episode and it may reasonably be assumed that there is some within-child correlation of the characteristics of these episodes. Statistical tests were interpreted at the 5% level of significance.
RESULTS
Of 77 children recruited to the trial, 44 completed the 12-week protocol and a further six completed at least the first 6 weeks of the protocol. These 50 children were said to have complied and analysis of their data forms the basis of this report. The remaining 27 children dropped out or were excluded for the following reasons: child refused trial treatment (n=16), parents too busy or failed to complete or return diaries (n=5), child developed intercurrent illness (n=4), GP prescribed inhaled steroids (n=2).
The characteristics of the treatment and control groups were similar at entry in most respects (table 2). By chance, the severity and duration of winter wheezy episodes recalled by their parents was more severe for the treatment group. The difference was statistically significant for duration (p<0.05). Children had few symptoms between episodes because of the selection criteria.
Entry characteristics of children who completed the trial
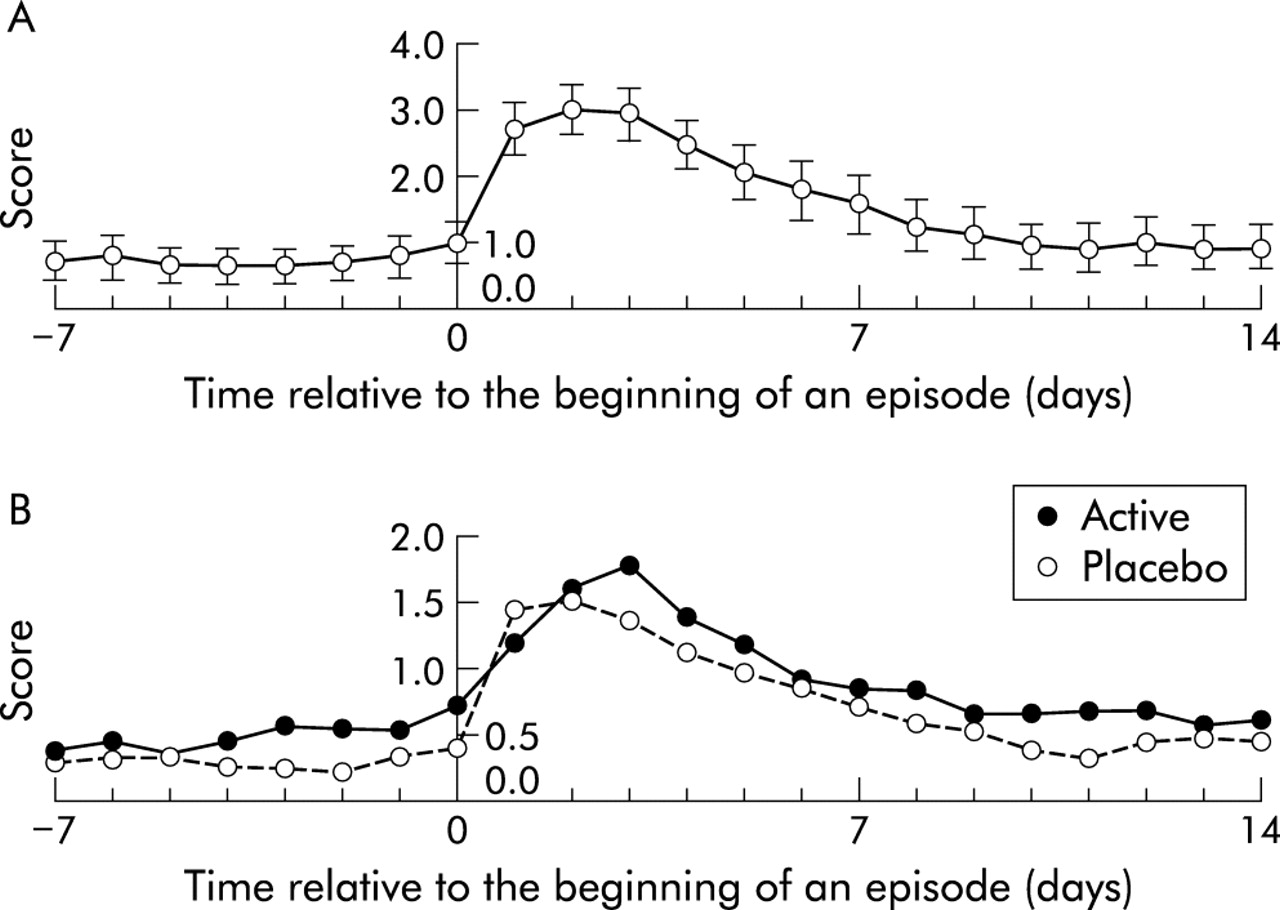
It is clear from a compilation of all the data for acute episodes (fig 1) that the onset was well defined, the level of symptomatology in the previous week was low, and the duration was about 1 week with a “tail” lasting for a further few days. There was considerable variability in the profile of individual episodes.
{kind=link}
Mean values and 95% confidence intervals for symptoms recorded from 7 days before until 14 days after the onset of episodes. (A) Daytime and night time symptoms for both groups combined. (B) Night time symptoms shown separately for active (solid symbols) and control (open symbols) groups.
Summary statistical analysis of the geometric means of night time, daytime, and activity scores for children showed no significant difference between active and placebo treatments The total number of episodes (placebo 37, active 27) and the number of children with episodes (placebo 23; active 19) did not differ between the groups (table 3). There was no evidence of a difference between groups in the number of episodes experienced by each child.
Analysis of episodes
The main outcome of interest was night time symptom score during episodes which, by definition, lasted for 7 days on each occasion. Using multilevel modelling, neither night time scores nor any other mean daily symptom scores during episodes differed between the active and placebo groups. A secondary analysis was carried out, adjusting for the total duration of wheezy episodes experienced by each child during the previous winter, and this produced no substantial changes in the result.
The main complaint related to children’s intransigence with nasal therapy. Treatment was withdrawn in one child because of nausea (fluticasone group). Trial medication was returned by the parents of 40 children at the end of the trial. Mean (SD) compliance estimated by weighing the bottles was 99.9 (44.6)%. One child was given no medication and six others received less than half of the intended number of doses. There was no difference in compliance between active and placebo groups.
DISCUSSION
This trial has shown no effect of prophylactic intranasal corticosteroids (fluticasone propionate 50 μg per nostril twice daily) on LRT symptoms associated with URT infections in preschool children. Although underpowered for its original objective of detecting a 40% reduction in nocturnal symptoms, the chance of missing an effect of this size was negligible (table 3).
It seems unlikely that any oversights or deficiencies in the conduct of the trial could have led to a falsely negative result, although compliance is always an issue. Our crude estimate of overall mean compliance based on weighing medication returned at the end of the trial was about 100%, with a wide scatter. In other circumstances once daily administration is adequate,21 so there should be a good margin of effective dosing.
The subjective technique used for recognition of episodes might be criticised. It is certainly difficult to be sure about the onset of an episode in the presence of variable day to day symptoms. However, since episodes were identified blind before decoding, there should have been no bias. We have explored the development of a computer based algorithm for discerning acute episodes automatically. Preliminary analysis using a moving time average (window length 7 days, start of episode when weekly average total symptom score increased by 2, end of episode when score back to baseline) picked up 44 of 64 episodes (and one additional episode which had not been identified by subjective scrutiny). The severity of computer generated episodes was greater in the treatment group, and this translated into a significant odds ratio (OR) of 15.4 (CI 1.2 to 198) for a more severe daytime outcome for the treatment group, and a similar trend (OR 3.5; CI 0.5 to 25) for night time scores. An automated scoring algorithm for this type of research could be valuable but has yet to be perfected.
From a clinical viewpoint, the treatment was ineffective in this group of preschool children with mainly episodic wheeze and relatively few interval symptoms. Because we did not record URT symptom severity (only its presence or absence), we cannot judge whether nasal corticosteroids had an effect on nasal inflammation as has previously been (transiently) demonstrated in adults.13 There were no fewer colds in the treatment group. It seems likely that corticosteroids in the dose given here had little effect on inflammation in viral URT infections, in comparison with their major role in nasal allergic inflammation. Thus, we have not adequately tested the hypothesis that LRT symptoms in children with viral episodic wheeze are mediated to a significant degree by indirect mechanisms emanating from the URT. This could only be achieved with a drug which reduces the URT inflammatory effects of the common cold.
Similar groups of preschool and older children with mainly episodic symptoms given lung targeted preventer inhaled corticosteroids during the winter months do not respond8,9—although high doses of inhaled steroids given at the time of an episode may alleviate symptoms.10–13 This approach may be worth exploring using high dose nasal corticosteroids during episodes. In contrast, several studies of preventer inhaled steroids in mixed pattern wheeze (equivalent to classical atopic asthma) have shown effects both on interval symptoms and episodes.25,26 It seems likely from the present data that any effect on LRT symptoms in these studies was achieved by direct anti-inflammatory effects on chronic asthmatic airway inflammation rather than by an indirect nasal anti-inflammatory effect.
Episodic viral wheeze appears to be a condition independent of extrinsic allergy and not associated with chronic airway inflammation or baseline BHR.27 This may partly explain the difference between the beneficial effects of nasal corticosteroids in allergic airway diseases15–18 and the negative results in our study.
Because the many viruses which are commonly implicated in viral wheeze operate through a variety of different adherence mechanisms and induce different cytopathic effects in different target zones of the respiratory tract, it may be rewarding to seek a final common pathway leading to wheeze rather than to explore virus specific mechanisms in detail. In this regard, the possibility that inflammation in the URT may be the vital common trigger factor leading to wheeze in individuals with susceptible airways still needs to be ruled out. Given the ethical constraints on research in young children, an adult model of viral episodic wheeze may promote better opportunities to explore this hypothesis.6,7
Acknowledgments
We thank Dr David Richards for facilitating a grant-in-aid from Glaxo Smith Kline and for the coded trial preparations. Glaxo Smith Kline played no part in the conduct or analysis of the trial or the preparation of the manuscript. We thank the general practitioners and practice managers of six Leicestershire practices (Melton Mowbray, Long Clawson, Uppingham, Highgate (Sileby), Winstanley Road and Evington) for their assistance. Mr Andrew Leary obtained the compliance data by painstakingly weighing the medication.
REFERENCES
Footnotes
-
Conflict of interest: Professor Silverman has previously received research and travel grants from several pharmaceutical companies including GSK.
Linked Articles
- Airwaves