Article Text

Abstract
Assessment of the current evidence for the use of leukotriene receptor antagonists as add-on therapy at steps 3 and 4 of the guidelines for adults with moderate to severe asthma.
- asthma
- add-on therapy
- leukotriene receptor antagonists
Statistics from Altmetric.com
CHALLENGES IN MODERATE AND SEVERE PERSISTENT ASTHMA
Of the 3.5 million adults with asthma in the UK, the majority have mild disease1 that can be controlled by inhaled short acting β2 agonists alone or in combination with low to moderate doses of an inhaled corticosteroid. Twenty per cent have more severe asthma and often, despite multiple drug treatments, these patients experience considerable morbidity including frequent exacerbations.2,3 The healthcare costs for moderate and severe persistent asthma are often high due to hospital admissions, absence from work, and drug usage.4,5 Guidelines on asthma management acknowledge the difficulties in achieving good asthma control in patients with moderate to severe disease defined by minimal symptoms, no exacerbations, no limitation of physical activity, and normal lung function, standards which can be achieved more easily in those with mild asthma.6,7 The challenge for academia, the pharmaceutical industry, and those involved in clinical care is to achieve good asthma control for adults with moderate to severe persistent disease by improving current management and by developing new improved treatments. The leukotriene modifying drugs, however, are the only new class of drugs that have been licensed for the treatment of asthma over the last 20 years. In this editorial we assess recent clinical trials of leukotriene receptor antagonists used as add-on treatment for adult patients with chronic asthma inadequately controlled on inhaled corticosteroids.
RECOMMENDATIONS FROM ASTHMA GUIDELINES
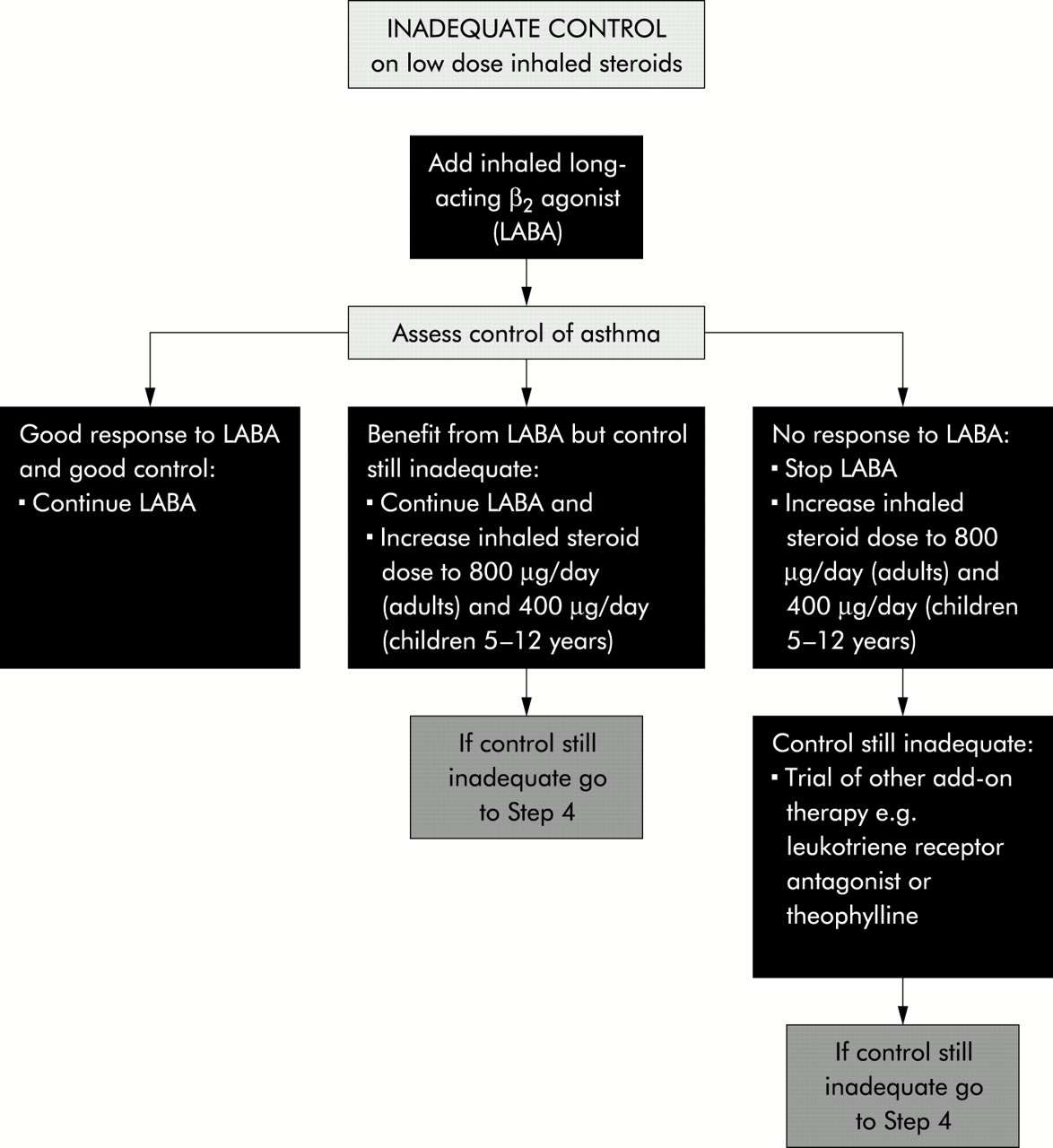
Recommendations from both national and international guidelines on the use of leukotriene receptor antagonists are broadly similar.7–9 The new British guideline on the management of asthma7 is evidence-based, using well defined methodology10 to evaluate all relevant published papers up to the end of September 2001. At step 3, inhaled long acting β2 agonists are the first choice add-on therapy to low or moderate dose inhaled corticosteroids (fig 1). Adding a leukotriene receptor antagonist represents a second line option. For patients at step 4 who remain inadequately controlled on these combinations of treatments, possible interventions include increasing the inhaled corticosteroid dose to 2000 μg daily or adding on a leukotriene receptor antagonist, a long acting oral β2 agonist, or a sustained release theophylline. Unfortunately no clinical trials of the benefits and safety of combinations of add-on therapies exist to guide management. Two papers published in this month‘s Thorax provide new information about several issues relating to the use of leukotriene receptor antagonists as add-on therapy to inhaled corticosteroids in adult asthma.11,12
{kind=link}
Step 3: Add-on therapy. Reproduced from BTS/SIGN.7
LEUKOTRIENE RECEPTOR ANTAGONISTS AND ASTHMA EXACERBATIONS
The clinical efficacy of pharmacological drugs for asthma depends on their ability to decrease symptoms, improve lung function, and reduce asthma exacerbations.7 The leukotriene receptor antagonist montelukast has been shown to improve symptoms and lung function13 and several short to medium term studies have reported modest inhaled corticosteroid sparing effects.14,15 The ability of montelukast to influence exacerbation rates in adults has not previously been assessed. The leukotriene receptor antagonist zafirlukast administered at an unlicensed dose of 80 mg twice daily to patients with severe persistent asthma receiving high dose inhaled corticosteroids at a dose of ≥1200 μg daily for 6 weeks reduced exacerbations, improved symptoms, lung function and reduced β2 agonist usage.16 A Cochrane systematic review of published and unpublished randomised controlled trials identified up to 2001 concluded that there was insufficient evidence, using the rate of exacerbations of asthma requiring rescue systemic corticosteroids as the primary outcome measure, to support the use of leukotriene receptor antagonists as add-on therapy to inhaled corticosteroids compared with doubling the dose of inhaled corticosteroid.17
In this issue of Thorax Vaquerizo and colleagues11 report the results of a 16-week randomised controlled trial in 639 adults with asthma inadequately controlled on inhaled budesonide at doses ranging from 400 μg to 1600 μg daily. Patients were randomised to receive either montelukast 10 mg or placebo and to continue on a constant dose of inhaled budesonide. The group receiving montelukast showed improvements in the primary end point (mild asthma exacerbation days) and in various secondary end points including symptom score, β2 agonist use, and morning PEF. The results were independent of budesonide dose. This large well conducted study provides good evidence that the addition of a leukotriene receptor antagonist to low, moderate, and high doses of an inhaled corticosteroid reduces mild asthma exacerbations and improves other indices of asthma control. The efficacy of montelukast in reducing the rate of severe exacerbations was not addressed in this study.
Previous studies have found that the efficacy of leukotriene receptor antagonists is less than that of inhaled long acting β2 agonists as an add-on treatment to inhaled corticosteroids when assessed by changes in symptoms and lung function.18,19 A randomised trial of inhaled salmeterol in a dose of 50 μg twice daily compared with zafirlukast in a dose of 20 mg twice daily found that the long acting inhaled β2 agonist was more effective in improving symptoms and lung function in adult patients with persistent asthma, the majority of whom were receiving inhaled corticosteroids.18 A 12-week comparison of fluticasone 200 μg plus salmeterol 100 μg daily with fluticasone 200 μg plus montelukast 10 mg daily19 found that the former combination produced greater improvement in asthma control. A long term trial is indicated comparing the effectiveness of leukotriene receptor antagonists and inhaled long acting β2 agonists alone and in combination as add-on therapy to low to moderate doses of inhaled corticosteroids, with asthma exacerbation rates as the primary outcome measure.
LEUKOTRIENE RECEPTOR ANTAGONIST COMPARED WITH DOUBLING THE DOSE OF INHALED CORTICOSTEROID AS ADD-ON TO MODERATE DOSES OF INHALED CORTICOSTEROID
For most patients with asthma a plateau in the therapeutic response to inhaled corticosteroids exists at doses below 1000 μg inhaled beclomethasone or equivalent.20–23 Although some patients may obtain additional benefit from higher doses, the risk of systemic adverse effects starts to rise. In this issue of Thorax Price and colleagues12 report the results of a 16-week randomised controlled trial in 889 adults with asthma inadequately controlled on inhaled budesonide 800 μg daily. Patients received either montelukast 10 mg plus inhaled budesonide 800 μg daily or inhaled budesonide 1600 μg daily. Both groups had similar improvements in the primary end point (morning PEF) and in secondary end points including symptoms, exacerbations, and asthma specific quality of life. Adding montelukast led to a slightly faster onset of action and both drug regimes were well tolerated. This large study provides good evidence that the efficacy of adding a leukotriene receptor antagonist is similar to doubling the dose of inhaled corticosteroid. Potential criticisms are that the trial may not have been long enough to detect differences in exacerbation rates and the lack of a placebo group prevented an assessment of the magnitude of response to the active treatments. Many patients at step 4 who have asthma that is not adequately controlled on an inhaled corticosteroid at a dose of 800 μg daily are receiving an inhaled long acting β2 agonist, and it remains unclear whether the addition of a leukotriene receptor antagonist is of clinical benefit in this circumstance. In a group of 72 patients with symptomatic chronic persistent asthma already taking high dose inhaled corticosteroids and other add-on therapies such as a long acting inhaled β2 agonist, the addition of montelukast for 2 weeks did not improve symptoms or PEF recordings,24 although the effect of long term treatment on exacerbation rate has not been examined. Leukotriene receptor antagonists might be less effective or ineffective in patients with moderate or severe asthma already receiving multiple drug therapies.
SAFETY OF LEUKOTRIENE RECEPTOR ANTAGONISTS
In clinical trials, including those reported in this issue of Thorax,11,12 the leukotriene receptor antagonists montelukast and zafirlukast have been well tolerated. The main side effects reported were headache and gastrointestinal disturbance. Administration of the leukotriene receptor antagonists has been associated with the development of the Churg-Strauss syndrome but it seems unlikely that this is a causal relationship.25,26
PLACE OF LEUKOTRIENE RECEPTOR ANTAGONISTS AS ADD-ON THERAPY
The most effective use of leukotriene receptor antagonists can be established only through clinical trials that recruit patients from the full spectrum of asthma severity. The studies on the use of leukotriene receptor antagonists as add-on therapies reported in this issue of Thorax may not be representative of the full range of adult asthmatics in the general population. For the purposes of regulatory submissions, pharmaceutical products are usually evaluated using randomised controlled clinical trials which inevitably are conducted in relatively small highly selected patient populations. These studies are efficient in that they provide an excellent context within which to evaluate the potential efficacy of the new product using a minimal number of patients, but do not provide adequate data on the implications of the introduction of the product into normal clinical practice, involving the treatment of the much more diverse patient population that exists in real life. Additional diversity comes from extremes of age, non-white populations, non-asthma drug treatment, and diseases in addition to asthma. Asthmatic patients may be smokers, and smoking has been associated with impaired efficacy of inhaled corticosteroids.27 In addition, non-pragmatic studies are ineffective for determining long term safety.28
Based on current published evidence, leukotriene receptor antagonists are second line alternatives to inhaled long acting β2 agonists as add-on therapy at step 3 of the asthma guidelines.7 This recommendation might need to be reviewed following the outcome of long term studies comparing the two classes of drugs using a range of end point measurements including asthma exacerbation rate. For patients at steps 3 or 4 of the guidelines who are receiving an inhaled corticosteroid at a dose of at least 800 μg daily but who are not taking an inhaled long acting β2 agonist, the addition of a leukotriene receptor antagonist has been shown to be as beneficial as doubling the dose of inhaled corticosteroid, at least over the medium term. Future pragmatic clinical studies should examine the long term benefits and safety of different add-on therapies including leukotriene receptor antagonists to help guide the management of moderate to severe asthma.
REFERENCES
Linked Articles
- Airwaves