Article Text

Abstract
Background: There is increasing recognition that questionnaires of health status and lung density measurements are more sensitive tools for assessing progression of emphysema than forced expiratory volume in 1 second (FEV1) and transfer coefficient (Kco). A study was undertaken to investigate prospectively the correlation between annual change in health status and computer tomography (CT) derived lung density in subjects with α1-antitrypsin deficiency.
Methods: Twenty two patients of mean (SD) age 40.7 (9.2) years with ZZ type α1-antitrypsin deficiency were investigated at baseline and 30 months later by FEV1 and Kco, St George Respiratory Questionnaire (SGRQ), and by a spiral CT scan of the chest. CT data of chest images were analysed using software designed for automated lung contour detection and lung density measurements. The density data were corrected for changes in inspiration levels.
Results: Changes in lung density, expressed as 15th percentile point or relative area below –950 HU, correlated well with changes in health status (SGRQ total score): R = −0.56, p = 0.007 or R = 0.6, p = 0.003. Neither changes in health status nor changes in lung density correlated significantly with changes in FEV1 or changes in Kco.
Conclusions: The SGRQ total score (which is a global measure in COPD) and lung density (a specific measure of emphysema) are sensitive to deterioration in patients with α1-antitrypsin deficiency. This finding may facilitate future studies with new drugs specific for emphysema, a frequently occurring component of COPD.
- lung densitometry
- α1-antitrypsin deficiency
- emphysema
- computed tomography
- outcome measures
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) in individuals with α1-antitrypsin deficiency of the Z phenotype is frequently regarded as a classic example of a condition where genetic predisposition and environmental exposure interact.1 Emphysema is the most prevalent clinical phenotype of COPD in α1-antitrypsin deficiency and its progression is expressed in the literature as annual decline in forced expiratory volume in 1 second (FEV1).2 Compared with non-deficient individuals, individuals with α1-antitrypsin deficiency who have never smoked have a relatively rapid annual decline in FEV1, with mean slopes reported between 47 and 86 ml/year.3
In some countries treatment by weekly infusions of human plasma derived α1-antitrypsin is available but, to date, no effect of α1-antitrypsin on annual decline in FEV1 has been proved in randomised trials. Power calculations, however, have shown that a large number of patients (550) for a long period of time (3 years) would be needed to show a statistically significant reduction of 50% in the annual decline in FEV1.4 Such studies are almost impossible to organise and therefore more sensitive outcome parameters for trials with new drugs for patients with α1-antitrypsin deficiency need to be studied.
As an alternative to pulmonary function tests, measurement of health status is increasingly recognised as a tool for assessing treatment effects in clinical trials, both for asthma and COPD.5 The St George’s Respiratory Questionnaire (SGRQ) was used in a 3 month study of salmeterol in COPD for assessment of treatment efficacy.6 Patients who scored the treatment as being effective and who had completed three questionnaires during the study had a mean improvement in SGRQ total score of 4.3 units (95% CI 1.8 to 6.9). In the ISOLDE trial of fluticasone in patients with moderate to severe COPD the rate of decline in the SGRQ score was reduced by fluticasone by nearly 40%.7 Moreover, the difference between steroid and placebo treated groups widened progressively with time. This difference supported the registration of fluticasone propionate for COPD in the UK.
Lung densitometry measured by computed tomographic (CT) scanning is another new method for assessing treatment efficacy.8 In this technique emphysema can be quantified by two measures—relative area below –950 HU (RA-950) and 15th percentile point (Perc15). Both are derived from the frequency distribution (histogram) of the densities of all lung voxels. RA-950 is defined as the relative area (RA) under the curve of the histogram below a threshold of −950 Hounsfield Units (HU), and Perc15 is defined as the cut off density value in HU for which 15% of all voxels has a lower value.
In a landmark cross sectional clinical study, lung densitometry expressed as the 5th percentile point (Perc5) showed a high correlation with both quantitative pathology scores of emphysema (R = 0.77, p<0.001).9 In addition, cross sectional studies by Gevenois et al10 on the correlation between lung density (RA-950) and quantitative pathology showed a Pearson correlation of 0.70 (p<0.001).
CT lung densitometry has recently been used in longitudinal studies, demonstrating that lung densitometry is more sensitive than FEV1 in detecting the progression of emphysema.4,11 However, the annual decline in FEV1 did not correlate with the annual decline in density.
The positive results of SGRQ as an outcome parameter in studies such as the ISOLDE trial prompted us to assess the correlation between annual change in SGRQ total score and the annual decline in lung density in subjects with α1-antitrypsin deficiency of ZZ phenotype.
METHODS
Twenty two subjects with newly detected α1-antitrypsin deficiency of ZZ phenotype volunteered to participate in the study. The characteristics of the patients are shown in table 1. None of them received α1-antitrypsin replacement therapy. Each patient was examined at baseline and after 30 months. If patients were free of exacerbations during the previous month, pulmonary function testing, spiral CT scanning of the chest, and a SGRQ were performed. The ethical board of LUMC approved the study and all patients gave informed consent.
Baseline characteristics of study patients
Pre-bronchodilator spirometric tests were performed according to ERS guidelines with a rolling seal spirometer followed by post-bronchodilator spirometric tests after inhalation of 400 μg salbutamol.12 Carbon monoxide transfer coefficient (Kco) was measured by single breath helium dilution on a Jaeger Masterscreen (Viasys, de Bilt, Netherlands).13
The SGRQ was applied as recommended14 with questions referring to the 3 months preceding the study visit.
Spiral CT scanning was performed as previously described using a Philips SR 7000 or Philips AVE scanner.4 Subjects inhaled 400 μg salbutamol during the hour before the scan. All patients were scanned with instructions to inhale to full inspiration. At baseline and follow up, each patient was scanned on the same scanner. Reconstruction algorithms were kept the same over the study period.
Lung density was measured using software developed by us in cooperation with MEDIS Medical Imaging Systems BV, Leiden, the Netherlands.15 After automatic lung contour detection, the lung volume during breath holding was calculated followed by analysis of the density histogram of all lung voxels. The CT data were independently analysed by two observers (WH, EB) and the resulting measurements of lung volume and density were averaged. There was good agreement between the observers (mean (SD) difference in volume, Perc15, and RA-950 was −0.15 (2.1) ml, 0.27 (1.5) HU, and 0.43 (0.58)%, respectively).
Statistical analysis
The density data were corrected for changes in inspiration levels between baseline and follow up using a linear mixed effects model fit by maximum likelihood, with log-transformed lung volume as random effect and log-transformed Perc15 or RA-950 as fixed effect. The derived slope between log volume and log Perc15 (−1.49 log(HU)/log(ml)) or RA-950 (20.15%/log(ml)) was used for correction of the data for each individual patient.
The correlation between changes in FEV1, Kco, Perc15, and RA-950 and changes in SGRQ were assessed by the Spearman correlation coefficient as the changes were not normally distributed. In order to compare our baseline measurements with those in the literature, the correlation between all baseline measurements was also calculated.
RESULTS
Patient demographic data
At study entry six of the 22 patients had a pre-bronchodilator FEV1 and Kco above 80% predicted. The remaining 16 patients had a mean post-bronchodilator FEV1 of 38% predicted (range 25–54% predicted). Of these 16 patients, two could not perform a single breath helium dilution measurement for Kco; the remaining 14 had a mean Kco of 49% predicted (range 25–95% predicted).
Correlation between baseline outcome parameters
The baseline Perc15 correlated well with baseline Kco (R = 0.66, p = 0.001) and with FEV1 (R = 0.68, p = 0.0001), which are comparable to values reported by Gould et al.9 Similar results were obtained with RA-950 (table 2). Baseline SGRQ total score correlated significantly with lung function and lung density measurements (table 3).
Correlation between baseline lung function and baseline lung density
Correlation between St George Respiratory Questionnaire (SGRQ) and both lung function and lung density
Changes in health status and lung density
The mean (SD) baseline SGRQ total score (32.4 (20.1)) correlated significantly with its annual change (R = 0.44, p = 0.041, fig 1). The mean (95% CI) change in SGRQ score during the study period was 6.5 units (–2.9 to 17.5). Baseline density measurements (Perc15 −928 (44.2) HU and RA-950 12.2 (11.6)%) did not significantly correlate with their annual change (Perc15: R = −0.03, p = 0.89; RA-950: R = 0.28, p = 0.21). The mean (95% CI) change in Perc15 and RA-950 during the 30 month period was –4.0 HU (–26.0 to 18.0) and 3.4% (−6.6 to 13.3), respectively.

Relation between baseline SGRQ total score and its change over a mean period of 30 months in 22 patients with Pi Z α1-antitrypsin deficiency (Spearman correlation coefficient = 0.44, p = 0.04).
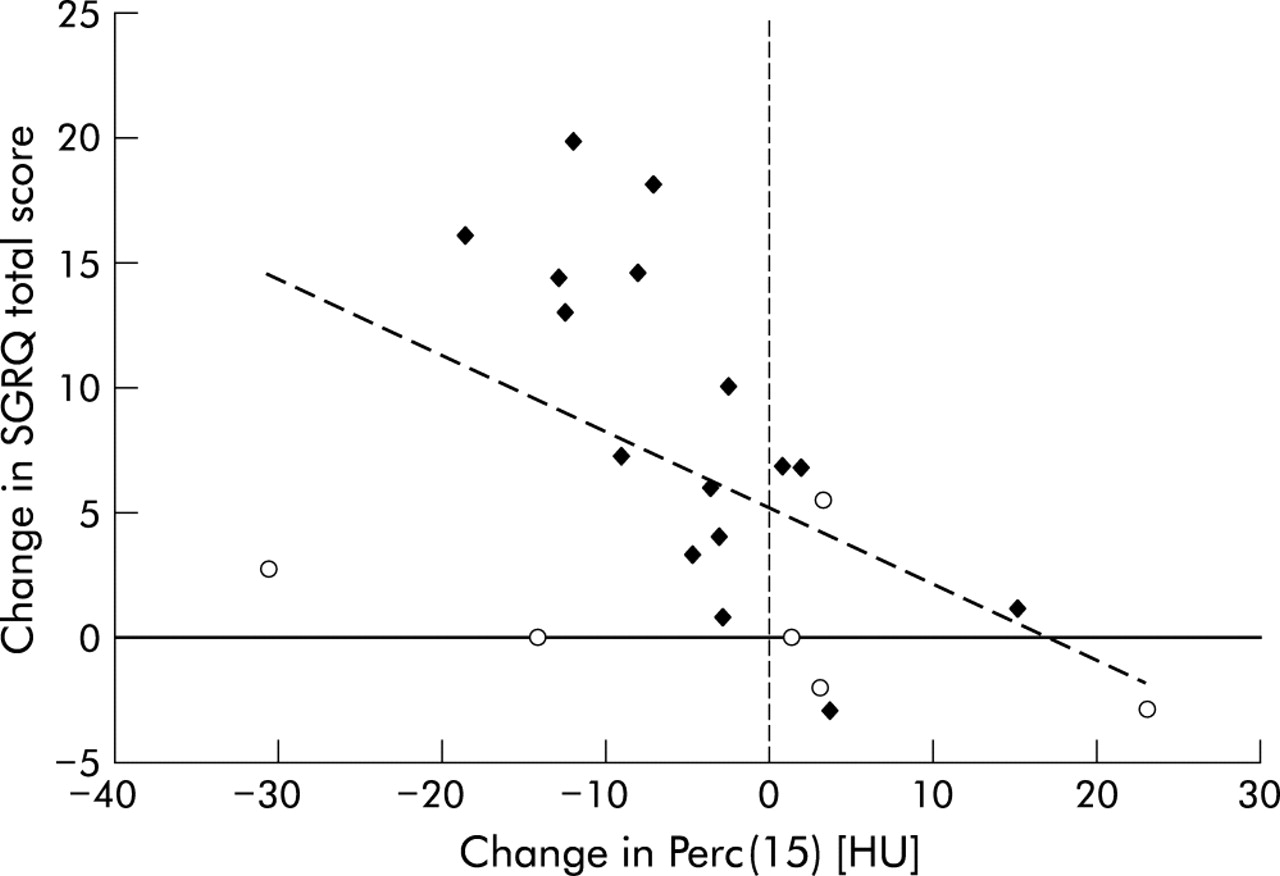
Changes in Perc15 correlated well with changes in health status as shown by the SGRQ total score (R = −0.56, p = 0.007, fig 2). Likewise, changes in RA-950 correlated with changes in the SGRQ total score (R = 0.604, p = 0.003, fig 3). Changes in absolute values of FEV1 and Kco did not significantly correlate with changes in SGRQ or with changes in lung density (table 3).

Relation between change in Perc15 and change in SGRQ total score over a mean period of 30 months in 22 patients with Pi Z α1-antitrypsin deficiency (Spearman correlation coefficient = −0.56, p = 0.007). Open circles are patients with normal lung function.

{kind=link}
{kind=link}
{kind=link}
Relation between change in RA-950 and change in SGRQ total score over a mean period of 30 months in 22 patients with Pi Z α1-antitrypsin deficiency (Spearman correlation coefficient = 0.60, p = 0.003). Open circles are patients with normal lung function.
DISCUSSION
We have found evidence that change in lung health status significantly correlates with change in lung density in patients with severe α1-antitrypsin deficiency. This analysis shows a relatively high correlation between the two measurements compared with a previously reported twofold lower correlation between decline in both SGRQ score and FEV1.16 Our results suggest that a change in health status score caused by emphysema coincides with a change in a measure of lung pathology obtained by CT scanning. This suggests that lung density measurements may be a useful parameter for the evaluation of new drugs specifically designed for the treatment of emphysema.
To our knowledge, this is the first report to show that changes in health status and lung density are significantly correlated. Dowson et al were unable to find a correlation between SGRQ total score and HRCT derived lung density in a similar study population.11 As the SGRQ total score did not decline over 24 months in their study, only a weak correlation between annual decline in the activity domain of the SGRQ and FEV1 was observed in 47 Pi Z subjects over this time.11 The difference between the results of their study and ours can be explained by the longer period of observation, the more sensitive measurement of lung density (due to the correction for changes in inspiration level and the fact that the entire lung volume was scanned), and the wider range in baseline characteristics of the patients in our study.
The mean change in SGRQ total score in our patients with lung function values below 80% predicted was high (8.7 units (range –2.9 to 19.8)), underscoring the rapid decline in patients with α1-antitrypsin deficiency. The mean change in those with normal lung function was 0.6 units (range –2.9 to 5.5) which is comparable to previous findings.5 On average, COPD patients without α1-antitrypsin deficiency reach a significant level of deterioration of 4 units every 15 months, while age related worsening in the SGRQ score of 0.12 units per year is observed in healthy subjects without COPD.5 A change in total score of 4 units over any given period of time is therefore seen as a clinically important reduction in health status, leaving a change of less than 4 units difficult to interpret.
Figure 1 shows that in our study population baseline SGRQ total score had a linear correlation with its change over time, indicating that healthy subjects will only have a small change in total score whereas patients with COPD will deteriorate more rapidly if their baseline health status was poor. We are not aware of any studies in which the SGRQ total score was in the range of 85–100. In contrast, when FEV1 values are below 30% predicted, a small change over time is usually seen.17
Selection bias may have occurred in our study. However, recruitment of patients was based on consecutive referral with a diagnosis of α1-antitrypsin deficiency rather than reduced pulmonary function. Of the 22 patients, six were identified by family screening, five of which had a normal FEV1 and Kco. As can be seen in fig 2, the variation around the regression line was highest at low values of change in SGRQ score. All patients with normal lung function (n = 6) are clustered in this part of the graph (open circles). On the other hand, the change in their lung density was high in both a positive and a negative direction. No cross sectional or longitudinal data are available to enable interpretation of the change in lung density in a normal population.
We wish to emphasise the effect on the correlation between change in SGRQ total score and change in Perc15 of omitting the six patients with normal lung function (fig 2). This results in a significant improvement in correlation from 0.56 to 0.74 (p = 0.001, table 3). No such improvement was found for change in RA-950 (R changed from 0.60 to 0.67). The different behaviour of Perc15 and RA-950 suggests that the percentile method is able to detect changes in mild emphysema, whereas the relative method is not. We therefore recommend reporting change in lung density by the percentile method. The authors are partners in the Spread study which aims to study this aspect in more detail in a longitudinal multicentre study.
Although baseline values of FEV1 and Kco correlated well with baseline lung density and baseline SGRQ total score, no such correlation was found when the change in each of these parameters was calculated. This probably reflects either the low number of patients studied or the relatively short period of time.
While pulmonary function tests have been used for many years for monitoring the progression of emphysema, measuring lung density is a novel concept. This concept originates from cross sectional work which showed acceptable correlations between quantitative microscopic emphysema scores and both CT lung density values and Kco.9,10 In addition, previous studies have shown that air trapping is of no concern as scans are taken during inspiration.9,10 However, since the level of inspiration by patients during follow up scans will never be precisely the same, corrections for inspiration level must be computed as indicated in our methods of analysis.
We conclude that the SGRQ total score, a global measure in COPD clinical assessment, and lung density, a specific measure of emphysema, are sensitive to deterioration in patients with α1-antitrypsin deficiency. It is hoped that this finding will encourage the development of trials for new drugs targeted at the treatment of emphysema, a frequently occurring component of COPD.
Acknowledgments
The authors thank their colleagues at the Alpha 1 International Registry (AIR, www.aatregistry.org) for valuable discussions. The Spread Project is described at www.lumc.nl/lkeb/spread.
REFERENCES
Supplementary materials
. Publisher Correction
Please note that there is an error in the affiliation and correspondence information for J Stolk, WH Ng and KF Rabe.
The correct information is shown here:Department of Pulmonology, Leiden University Medical Center, Leiden, The Netherlands
The error is much regretted.
Linked Articles
- airwaves
- Correction