Article Text

Statistics from Altmetric.com
Past
The existence of a genetic disease caused by immotile cilia was reported in a short paper published in 1976.1 The prevalence was estimated to be one person in about 30 000. The following facts made it possible to draw these conclusions.
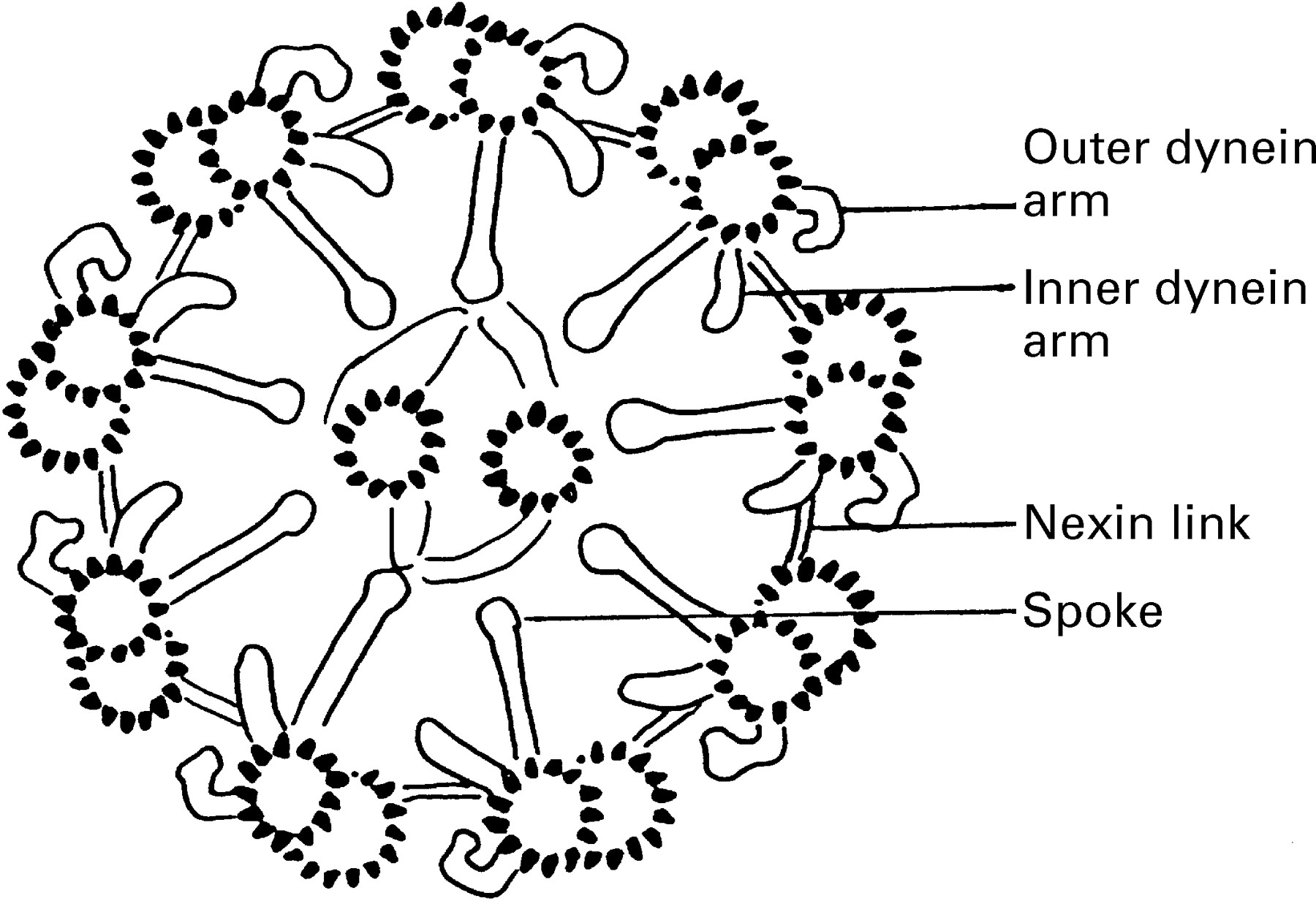
Cilia from the lung, nose, or elsewhere have a structure that is highly conservative and, moreover, resembles that of the sperm flagellum. The central part of the sperm tail, its axoneme, thus has the same well known 9 + 2 pattern as has a cilium, although it is about 50 μm long whereas the human cilium is only about 6 μm in length (fig1).
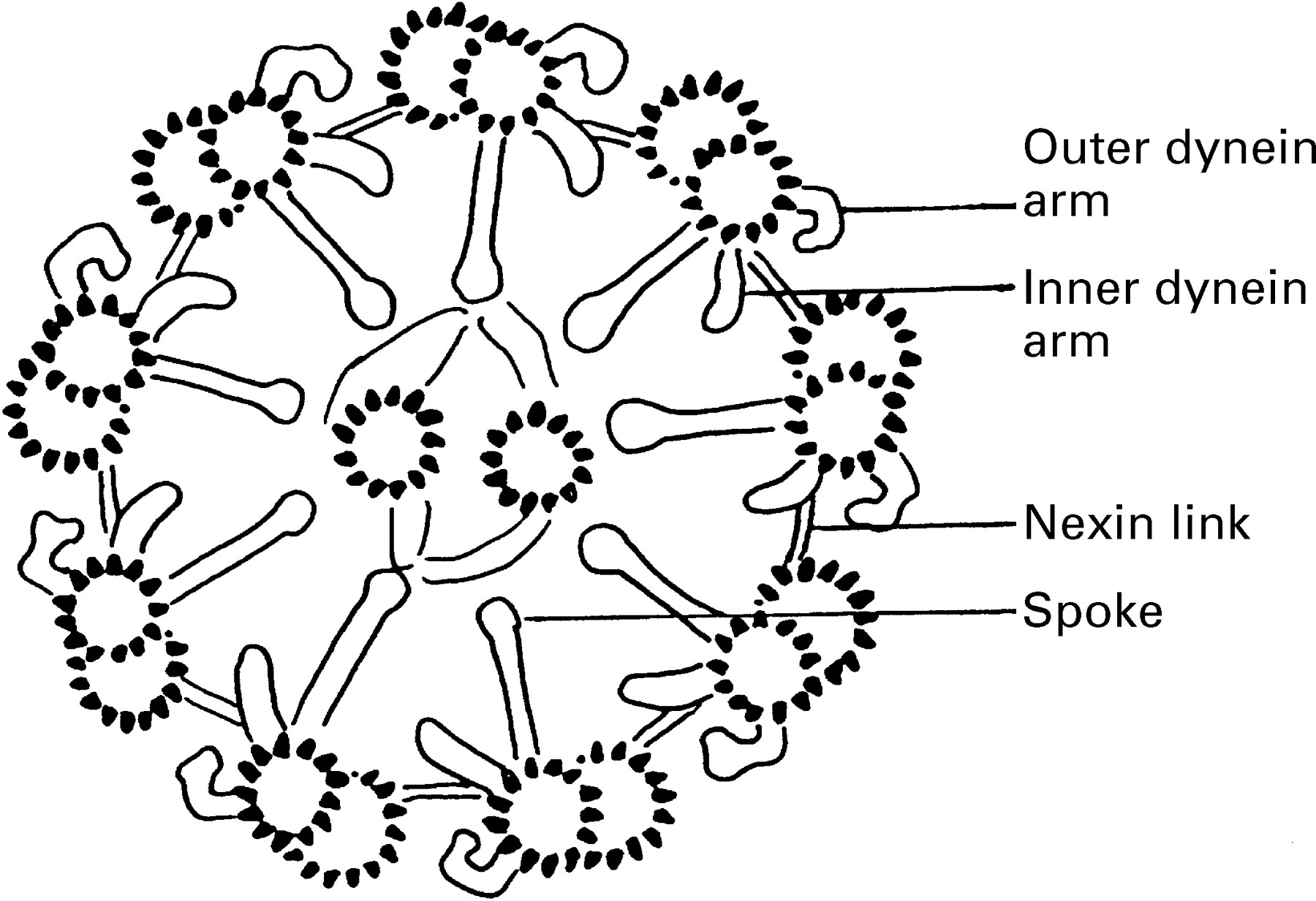
Schematic cross section of a ciliary axoneme. The central part of the spermatozoan flagellum has an identical ultrastructure. Nine microtubular doublets surround two central microtubules. The dynein arms are responsible for causing the nine microtubules to slide relative to each other. The nexin links restrict the sliding with the result that the cilium bends.
The ultrastructure of the sperm tail from three infertile men with immotile but otherwise normal spermatozoa had been described in two papers in 19752 ,3; they were found to lack the so-called dynein arms, the structures responsible for generating the movements of cilia or sperm tails.4 The absence of dynein arms had not been described in any other organism, although flagellar (or ciliary) mutants of other types had been described from a unicellular green alga.5 In one of these two papers the spermatozoa of two brothers were examined3 and it was suggested that “the two brothers have a genetic disorder in which the synthesis of the dynein proteins, or their assembly into dynein arms, is defective”.
It was assumed that a genetic defect involving the dynein arms in the sperm tail would affect those in the cilia as well. The mucociliary transport in the tracheobronchial tract of the two brothers was therefore also investigated. A radioactively tagged test aerosol was inhaled and the radioactivity in the lungs was measured for two hours.6 The mucociliary transport was found to be extremely slow or possibly absent. It was therefore presumed that all dynein arms were lacking or defective. The bronchial cilia of a fourth man with immotile spermatozoa were then examined and both the cilia and his spermatozoa were found to lack dynein arms.1
Two of the three men whose sperm ultrastructure had been examined at that time had (and still have) situs inversus; the third is one of the two brothers first examined. All three men have chronic sinusitis and bronchiectasis which, together with situs inversus, are the three cardinal signs of Kartagener’s triad or Kartagener syndrome. It was concluded that the aetiology of the disease is a genetic defect of the cilia and that “chance alone will determine whether viscera will take up the normal or the reversed position during embryogenesis, when normal dynein arms are missing”. This would result in a similar number of cases with and without situs inversus in the immotile cilia syndrome.
Kartagener syndrome could therefore be regarded as a subgroup of the immotile cilia syndrome. The clinical consequences are the same and include chronic cough and expectoration of mucoid, mucopurulent sputum, bronchiectasis, chronic rhinitis and nasal polyposis, recurrent maxillary rhinitis, often agenesis of the frontal sinuses, not rarely atelectasis, and often otitis before puberty. The clinical manifestations include chronic rhinitis, sinusitis and bronchitis dating from early childhood. Treatment is symptomatic and directed against complications in the respiratory tract. Early physiotherapy is recommended.
The prevalence of Kartagener syndrome has been estimated to be about one in 68 000; that of immotile cilia syndrome would hence be about one in 34 000. Situs inversus has a prevalence in Scandinavia of one person in 80007 and in the USA of one in 11 000.8 Roughly a fourth or a fifth of all persons with situs inversus also have bronchiectasis8 and these are very likely to have chronic sinusitis as well. This gives a prevalence of Kartagener syndrome of one in 50 000 and of immotile cilia syndrome of about one in 25 000. Familial studies of Kartagener syndrome have also shown that, among 104 siblings in a number of families, 30 subjects had either Kartagener syndrome or an “incomplete” syndrome (thus no situs inversus).9 These data are consistent with the opinion that the syndrome is inherited as an autosomal recessive mutant.
Present
Since the original publication on the immotile cilia syndrome several hundred papers have been published on cilia, spermatozoa, fertility or sterility, sensory organs, and brain function in this and related diseases and several reviews have also been published.10-13 As might have been expected, the situation is now more complex than it appeared to be 22 years ago.
It has been found that an ultrastructural abnormality of the ciliary axoneme is not always accompanied by a similar abnormality of the sperm axoneme. A man has thus been found to have a clear cut Kartagener syndrome including situs inversus, sinusitis, bronchitis and otitis media and yet to have motile spermatozoa and a healthy child.14 Whereas his cilia lack dynein arms and hence are immotile, his spermatozoa have normal dynein arms. The reverse situation has also been found—namely, a man with cilia of normal ultrastructure and presumably normal function (no lung problems) with immotile spermatozoa lacking dynein arms.15 There is even a case of a man with Kartagener syndrome and with immotile spermatozoa lacking dynein arms but with cilia with dynein arms that in vitro were found to be motile.16 It seems that cilia and spermatozoa are sufficiently different to have at least some proteins that are not shared.
In numerous people with clinical signs of immotile cilia syndrome the structure and function of their bronchial or nasal cilia have been examined. It appears that the immotile cilia syndrome is a highly heterogeneous disease. Several different genes may mutate and thereby give rise to non-functional cilia and hence to the clinical diagnosis of immotile cilia syndrome.
The ciliary axoneme is a construction containing at least 130 different polypeptide species.17 A differential diagnosis can only be made by electron microscopy which will indicate which components of the cilia are affected. In the first described cases the diagnosis was simple—namely, absence of dynein arms. This is still one of the largest subgroups of the disease. In other cases only the outer dynein arms are lacking or only the inner ones, or only the so-called spokes, or any of the many other components.10-13 Alternatively, the cilium appears to have a normal structure but does not function normally. In one of the many subgroups of the syndrome the epithelia that would normally be ciliated have cells with long and slender microvilli but no cilia can be found.18 The intriguing observation that about 50% of all subjects with immotile cilia syndrome have situs inversus is true for most subgroups, including those with a normal ciliary ultrastructure, but it is not true for the group who lack cilia, nor for a group whose main characteristic is a lack of the two central microtubules.
In some of the many subgroups the cilia or the sperm tails or both have some motility. This has inspired many investigators to invent a new designation for one or all of the subgroups—primary ciliary dyskinesia is the most common alternative term,19 or acilia syndrome or ciliary aplasia for the subgroup in which cilia are lacking.
An early diagnosis of the disease is important in order to start proper treatment of the child and to avoid other unnecessary medical examinations. If an electron microscopic examination has shown the cilia to have a normal structure, no diagnosis can be made. A functional test of the cilia is preferable. A simple method is the saccharin test in which small grains of saccharin are placed on the nasal mucosa and the time for them to be transported to the pharynx is measured.20 This technique is not completely reliable, however, and cannot be used for children under the age of about five years.
The most reliable test is one elaborated by Jorissen and Bertrand21 in which a biopsy specimen from the nasal epithelium is cultivated in a culture solution to which pronase has been added to dissociate the cells from the epithelium, as well as antibacterial drugs. After a few days the cilia are shed and after a further period of about six weeks a population of new cilia have emerged. The test records whether these fresh cilia beat with coordinated beatings which will result in a rotation of the isolated cells or cell aggregates. If there is no rotation after regrowth of the cilia the patient is diagnosed as having immotile cilia syndrome. In cases where cell aggregates from the original biopsy specimen show no rotation but the cells with regrown cilia rotate, the condition is classified as a secondary ciliary dyskinesia, perhaps caused by bacterial toxins.
Prospects for the future
A major aim in the study of immotile cilia syndrome is to find the gene (or genes) responsible for the disease. This will not be an easy task as several hundred different genes are involved in building a cilium and each of them might be the defective one that makes the cilium immotile, dysmotile, or absent. Some candidate genes are those that code for the dynein heavy chains with their phosphorylating sites, those coding for tubulins which make up the microtubules, and those that code for the proteins that bind dynein heavy chains to the tubulins.
More than 10 genes have been shown to encode different dynein heavy chains.22 When these genes and those for the tubulins etc have all been isolated and characterised it will be possible to screen the genome of a patient with suspected immotile cilia syndrome in a search for defective or lacking dynein genes. Such a diagnosis will not be more helpful to the patient than the functional test of Jorissenet al 21 but it will inform us which particular gene is responsible in each affected person and pedigree. Are only a few genes responsible for most of the cases? If so, why are these genes so fragile? Or is the defective gene any one of several hundreds? Do we all carry at least one gene that in double dose would have given us non-functioning immotile cilia?
Isolation of a responsible gene has another value—namely, that of finding out what gene transcripts it will produce. In several cases the gene product will be well known: the 17 proteins of the spoke,23 the dynein heavy chain of the outer dynein arm or those of the inner arm,24 etc. A more knotty problem is to establish how body asymmetry is determined, and thus to find out how a particular gene will cause the heart to go to the left side while its allele will let chance alone decide its position, and then also of the viscera.
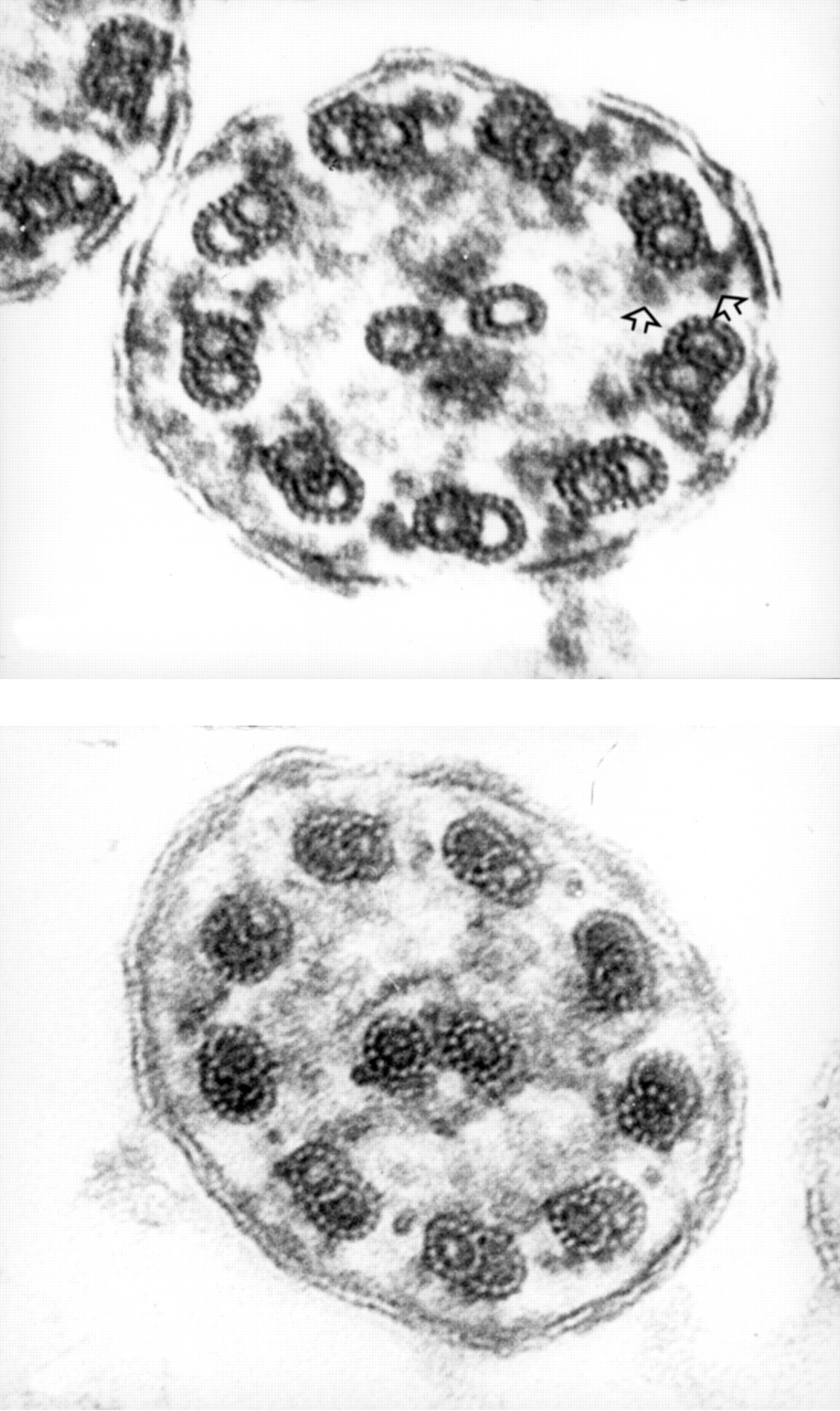
Electron microscopy has played an important part in the exploration of the immotile cilia syndrome in spite of the fact that the standard techniques in use today are far from ideal for making the dynein arms visible. In particular, the inner dynein arms have a very inconspicuous appearance in cilia, somewhat less so in sperm tails. For this or for other reasons a ciliary cross section from a healthy person will normally show only about three diffuse inner dynein arms where nine would be expected. When fixed with the tannic acid-containing fixative by Mizuhira and Futaesaku,25 particularly the modified variety with no osmium after fixation, all dynein arms are seen.26 Micrographs in which this fixative has been used may therefore give new information about the structure of cilia in different subgroups of the immotile cilia syndrome (fig 2).
{kind=link}
{kind=link}
Cross section of a cilium from a subject with normal motile cilia (top) and a subject with immotile cilia (bottom). Outer and inner dynein arms (see fig 1) appear to be lacking in the subject with immotile cilia. If generalised, such a deficiency is likely to cause its carrier to suffer from rhinitis, sinusitis, polyposis, otitis, and bronchitis and in 50% of cases also to have situs inversus.
A new method has recently been suggested that might be useful in the diagnosis of the disease.27 It is also suitable for the examination of children as it is extremely rapid and totally painless. The nitric oxide level in the air, sampled directly from the nose or from normally exhaled air, is measured. Practically no nitric oxide was found in the air sampled from four children with Kartagener syndrome whereas large amounts of nitric oxide were found in healthy children and in those with asthma, cystic fibrosis, and other respiratory problems. Whether these low values are due to an agenesis of frontal sinuses which are an important source of nitric oxide or whether ciliary defects are connected functionally to nitric oxide synthesis is as yet unknown. The latter possibility as a histochemical marker exists for the nitric oxide synthase. In a study by Xue et al 28 nitric oxide synthase was found to be localised in the basal bodies of the cilia in the lung. A connection between non-functioning cilia and a non-functioning nitric oxide synthesis would be a puzzling feature, but so are many other features of the immotile cilia syndrome.