Article Text

Statistics from Altmetric.com
Ten years ago a joint working group of The British Thoracic Society and the Society for Thoracic Surgery in Great Britain in Ireland published its findings, concluding that there was ‘critical under-provision of Thoracic Surgery in the UK’.1 ,2 The situation has improved according to Lung Cancer Data (LUCADA),3 the National Lung Cancer Audit,4 and the English Cancer Repository Dataset reported in this number of Thorax.5 The English Cancer Repository Dataset study found that the proportion of patients with non-small cell lung cancer undergoing surgery has risen to 10.6% from 8.8% in 1998, the situation that prompted the formation of the working party. The data provide evidence that there is now better access to thoracic surgery in the management of lung cancer and that the drive by professional societies to achieve this has met with success. The critical question now is whether, on existing evidence, it is reasonable to believe that simply increasing lung cancer resection rates will result in overall better outcomes for future patients with lung cancer.
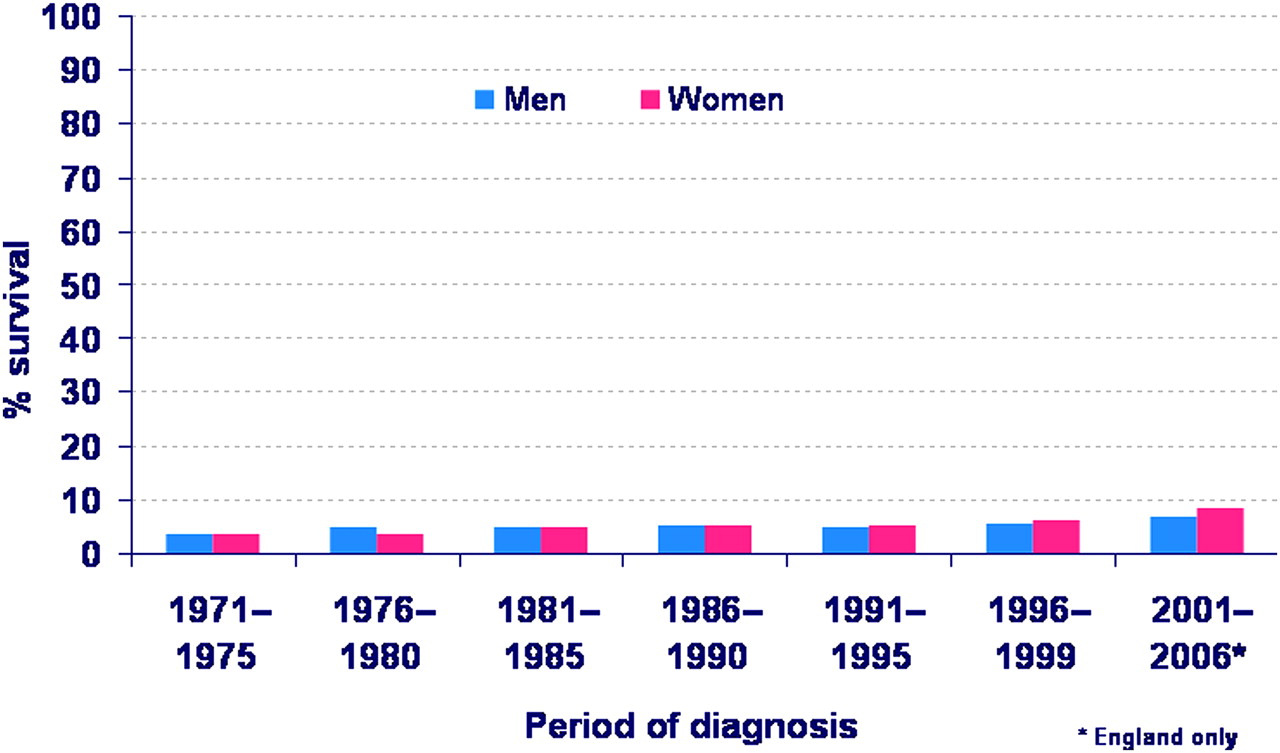
Overall survival for lung cancer remains extremely poor. In bowel cancer, 5-year survival has steadily increased from around 20% to 50% (figure 1) while that for lung cancer remains under 10% with negligible improvement over 40 years (figure 2). The lung cancer patients who have surgery are, by selection, the most favourable decile, yet fewer than one in four operated patients were alive 5 years later according to data in the National Lung Cancer Audit,4 the same as in patients operated on between 1949 and 1983.6 In the intervening 30 years, there have been fundamental changes in endoscopy, imaging, staging and the use of combination and adjuvant treatments, but in terms of crude, 5-year survival following surgery we have nothing to show for it. Cancer treatments are burdensome and disruptive for patients and their families near the end of life7 and so we should take stock of what is actually of benefit, rather than just do more of the same.
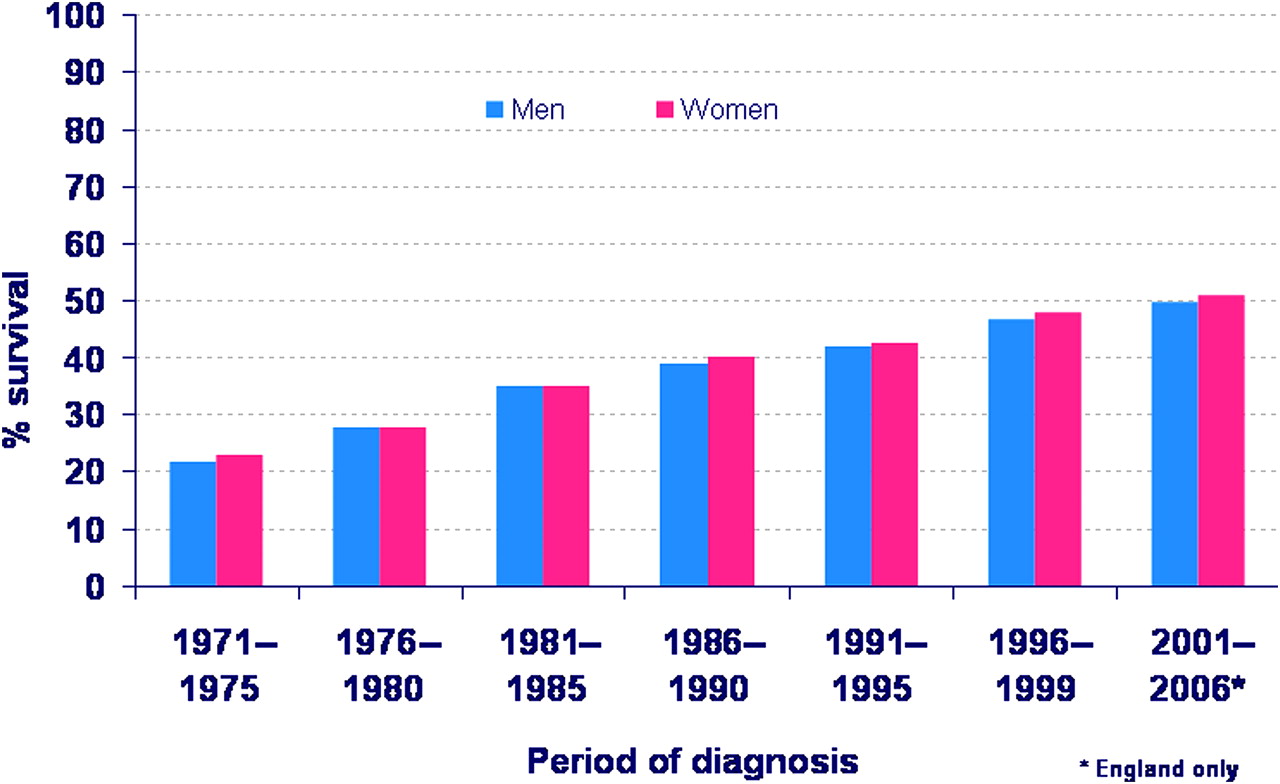
Age standardised 5-year relative survival rate, colon cancer, by sex; England and Wales, 1971-2006.
{kind=link}
{kind=link}
Age standardised 5-year relative survival rate, lung cancer, by sex; England and Wales, 1971-2006.
In 1970, Bernard Fisher in a 52-page treatise raised doubts about the benefit of radical surgery for breast cancer. He concluded that ‘progress in the treatment of breast cancer will result only when surgeons are willing to accept the concept of, and participate in, rigidly controlled cooperative clinical trials of promising findings. Such endeavours will make major contributions to medical progress in the remaining decades of this century’.8 Indeed they have—but not in lung cancer surgery; there have been vanishingly few trials and there are none open in the UK to test the efficacy of surgical resection in any group of patients. In order to devise a trial there has first to be uncertainty. During the 1970s following the writing of Fisher, an increasing number of surgeons moved away from radical mastectomy, and by 1978, writing in the BMJ under the title ‘If my wife had breast cancer’, Harold Ellis did not mention radical mastectomy as an option nor did any of the subsequent correspondents.9 It was the already changing climate that allowed the randomised trial of Veronesi and colleagues to be published in the New England Journal of Medicine in 1981.10 One could argue that by then the tide had turned, but it is the randomised controlled trial that is remembered as the clinching evidence.11 The widely accepted conclusion was that surgery for breast cancer offers control of the primary; if cancer is confined to that site, cure may well follow. Extending surgery did not increase cure rates.
Surgery for lung cancer is restricted to a ‘subgroup of patients with early stage disease’4 but ‘early’ conveys a temporal sense to the reader, that of catching the cancer while curable, whereas in practice what it actually means is that staging investigations show a limited extent of cancer. Lung cancers do not form an orderly queue and progress, stage by stage, from their first beginnings to eventual death of the patient at the same rate as each other. They vary greatly in their radiological doubling time and in their clinical rates of progression.12 The process of selecting patients for surgery includes repeated imaging, numerous investigations and the passage of some time. While the purpose is to identify the most appropriate patients for operation, an inevitable by-product of this process is identification of a cohort with inherently more favourable prognostic features. To prove that the operation was the cause of longer survival (as distinct from being associated with it), we must compare like with like.
The majority of evidence cited for surgical practice is in the form of follow-up studies of highly selected and therefore unrepresentative patients. The flaws in this much favoured method have been analysed in a case study of reports of the surgery for mesothelioma.13 If surgery is only one component of multimodal therapy, it is impossible to see the signal (the effect of surgery) from noise (variable outcomes and varying treatments). To what extent is the presumed additional survival time a result of the surgical component? When patients are offered more than one treatment, the observation of statistical association between more treatments and longer survival may be because only survivors thus far are available for further treatment.14 There is an inescapable truth which applies to all cancer treatment: they are all harmful to some degree, and unless the sum total of treatment benefit outweighs this, the net effect is harm.15
It is widely recognised that randomised trials of interventions are difficult to design and very difficult to carry out. As a result, when trials of cancer surgery are proposed, referees are prone to write critical reviews, listing many obstacles, but perhaps overlooking the possibility that they are themselves an obstacle. Many proposals are unfunded and even funded trials flounder; the challenge is to get through the obstacles and come out the other side with evidence. There has to be a ‘can do’ attitude and some degree of pragmatism may be required but the maxim of Lilford and coworkers that ‘some unbiased evidence is clearly better than none’ applies to lung cancer.16 More imagination, innovation and determination are required to design the trials that can be done.17 And once designed, it should be an imperative in clinical practice that patients are actively recruited to randomised controlled trials. There is now in Britain a growing movement from surgeons of all disciplines to drive recruitment in surgical trials.18 From NIHR, there was a recent, very welcome call for studies of surgical treatment. Future lung cancer patients should have the opportunity to benefit from these drives.
The role of surgery in lung cancer is limited to the minority but neither inclusions nor exclusions are based on controlled trials. We now know that the rigorous selection of carefully staged patients, operating only on those in whom there was a confidant expectation that they could be rendered cancer free, has provided cohorts of patients staged T1N0M0 with survival rates of up to 80%–90%. Among 1394 patients in trials of adjuvant chemotherapy, with less restrictive stage criteria, 5-year survival was over 50% (with or without chemotherapy)19 but among English registry patients4 it is about 25%, no better than 30 years ago.6 The concept that the application of successive treatments in modern oncology makes cancer a ‘chronic illness’i is not so far borne out by evidence as far as non-small cell lung cancer is concerned.4 ,12 This notion is prone to the confusion between surviving because of the treatment and surviving to be available for more treatment. It is certainly not a justification for unavailing surgery. Any extension of surgery to less rigorously selected patients should include a drive to test the policy in randomised trials. For any patient where the justification for surgery is ‘let's give her the benefit of the doubt’ it would be better for that doubt to be tested in a trial and then it can be ascertained where benefit lies, with surgery or with avoiding surgery.
Randomised trials may be the best way to prove conclusively what treatments are effective but meanwhile there is no shortage of data, thanks to those who have driven LUCADA and the Cancer Registries3–5 and it could (and should) be used. The use of existing data to get better estimates of likely effects has been used in thoracic malignant disease.14 ,19 ,20 In mesothelioma, a bounding study, using data from the biggest institutional report, allowed an estimation of the greatest margin of benefit that might be attributable to surgery.14 Pulmonary metastasectomy for disseminated colorectal cancer is one of the most frequent thoracic operations. Mathematical modelling with Thames Cancer Registry data applied to large follow-up studies of pulmonary metastasectomy was used to approach the question: what might survival have looked like if these patients had not had metastasectomy?20 The title of that study comes from a remark made at a cancer research meeting in justification of pulmonary metastasectomy: ‘better out than in’. Is not removing the cancer you can see self-evidently the right thing to do? As Dr Ben Goldacre says, ‘I think you'll find it's a bit more complicated than that …’.ii
References
Footnotes
Linked article 201768.
Correction notice This article has been corrected since it was published Online First. The following sentence has been amended to read: We now know that the rigorous selection of carefully staged patients, operating only on those in whom there was a confidant expectation that they could be rendered cancer free, has provided cohorts of patients staged T1N0M0 with survival rates of up to 80%–90%.
Competing interests None.
Provenance and peer review Commissioned; internally peer reviewed.
↵i http://www.cancer.org/Treatment/SurvivorshipDuringandAfterTreatment/UnderstandingRecurrence/WhenYourCancerComesBack/when-cancer-comes-back-treating-cancer-as-chronic-illness
↵ii http://www.badscience.net/2008/12/i-think-youll-find-its-a-bit-more-complicated-than-that-and-other-excellent-christmas-gifts/