Article Text

Statistics from Altmetric.com
Recent reports from the Audit Commission1 and the House of Lords Select Committee2 on resistance to antibiotics have both been critical of general practitioner (GP) prescribing for the excessive use of antibiotics in respiratory illness, the increasing antibiotic resistance of respiratory pathogens, and excessive drug costs in the community. Such criticism of GPs is not new and appears to have little effect on prescribing habits. Why do all doctors prescribe antibiotics so often, is this behaviour amenable to change, and what does it have to do with hospital physicians?
If changes in prescribing in the community are to be achieved, there probably needs to be a better appreciation of the issues which drive it. This understanding is important, not only for those working in primary care, but also for those in hospital practice. Respiratory physicians and microbiologists teach and influence GPs, medical students, and junior doctors. Their advice and example is important but is less influential, especially in primary care, if it does not also reflect and address the difficulties experienced by doctors who have to treat patients whose attitudes and expectations may differ significantly from their own.
This review highlights some of the issues behind dependence on antibiotic prescribing, particularly for respiratory disease. It focuses on managing the commonest presentation of acute respiratory illness: a previously well adult consulting with a new episode of cough and other lower respiratory tract symptoms. This is often called “acute bronchitis”, an imperfect diagnostic label.3For most of these patients the doctor is uncertain whether antibiotics are indicated, but still prescribes them.
Lower respiratory tract illness
Acute lower respiratory tract illness results in many thousands of consultations in primary care and a significant number of acute medical admissions each year.4 ,5 The management of adults admitted to hospital with community acquired pneumonia receives much attention5 ,6 but, as illustrated by the pyramid in fig 1, such cases represent a small proportion of acute lower respiratory tract illness occurring in the community. Indeed, an iceberg may be a better analogy than a pyramid as this illness is hidden from hospital physicians below the surface. About a quarter of patients with symptoms seek medical attention7 and very few need to be admitted to hospital. About 5% of adults treated by their GP for a lower respiratory tract infection have pneumonia on the chest radiograph; of these, only 20% will be admitted to hospital and 5–10% of these may die and/or require intensive care management.8 In spite of this range of severity, diagnostic labels and typical management are strikingly uniform—namely, diagnosing infection and prescribing antibiotics.

The layers of the iceberg of lower respiratory tract illness (LRTi), infection (LRTI), and pneumonia seen in hospital and the community. The numbers in parentheses are estimates of the relative proportion of patients in each category. ITU = intensive care unit. Reproduced with permission from Macfarlane.8
The problems of disease and definitions
The sharpness of the divisions suggested in fig 1 is clearly unrealistic. As one descends from the top of the iceberg, frequency increases, classification blurs, and issues reflecting the patient and the circumstances of the consultation become increasingly important.9 It is in this area that most GPs work.
Infections which require antibiotics—caused by bacteria and atypical organisms—are found in a proportion of patients admitted to hospital with pneumonia and do occur in some adults in the community with pneumonia10 and lower respiratory tract infection.11 However, much lower respiratory tract illness may not be due to infection at all12 and many confirmed infections are viral rather than bacterial13 ,14 which, in most patients, are probably self-limiting. This view is supported by studies which show that antibiotics have little impact on the duration of symptoms of either acute bronchitis15-17 or many acute exacerbations of chronic obstructive pulmonary disease in the community.18 The majority of British GPs seem uninfluenced by this evidence for they prescribe antibiotics to about 75% of these patients,3 ,19-21 a practice shared by European physicians.22 ,23 It seems reasonable to suspect that strategies that rely on antibiotics to manage the more severe episodes at the top of the iceberg, and the labels that describe them as “infection”, may not be so appropriate for those at the bottom.
Problems of definitions have bedevilled both clinical practice and research, especially in primary care.8 ,19 British GPs rarely perform investigations when diagnosing and prescribing for lower respiratory tract illness. Even in hospital, where the diagnosis can be supported by laboratory and radiology findings, up to three quarters of patients initially diagnosed with a chest infection receive concurrent treatment for other conditions such as pulmonary infarction and heart failure until the diagnosis becomes clearer.24
GPs use a wide variety of diagnostic labels when patients present with acute lower respiratory tract symptoms.3 A term implying infection—for example, “bronchitis”, “chest infection”, or “lower respiratory tract infection”—may be chosen only after the doctor has decided to prescribe antibiotics perhaps to justify that decision.25 Indeed, describing the illness to patients in terms of “infection” makes not prescribing antibiotics more difficult.
In the 1970s Howie and colleagues, in a series of important studies, offered a new insight into the management of respiratory illness in primary care.19 ,25 They described an “urgent need . . . to define general practice illness in terms of its presenting signs and symptoms . . . so that objective respiratory symptoms may be recognised and studied with a view to deciding appropriate treatment”.19 Their challenge remains largely unanswered and is still timely: developing guidelines for the use of novel and expensive antiviral therapies for self-limiting acute lower respiratory tract illnesses will require a clear understanding of these issues.
Why do patients consult with acute lower respiratory tract symptoms?
Patients consult because their symptoms distress them and those around them. Cough is the cardinal feature of an acute lower respiratory tract illness. It demands attention from family, friends and work mates and it disturbs the sleep of patients and their household. Verheij et al found that 90% of patients with acute bronchitis consulted their general practitioner because they were annoyed by the cough, two thirds had disturbed sleep, and nearly half consulted because of pressure from family and friends.26 We found very similar results: common reasons for consultation for previously well adults with acute lower respiratory tract illness were the troublesome nature of the symptoms (92%), being prompted to consult by family and friends (46%), and for reassurance that it is not serious (39%).27 Cornford found that patients with a cough who consulted their GP were more worried about it and were more likely to feel that it was abnormally severe and was interfering with their social activities than patients with a cough who did not consult.28
There are parallels with other conditions. Littleet al found that between one third and two thirds of patients with a sore throat consulted only to legitimise their illness for family and friends or for work purposes.29 Thus, patients may not necessarily consult because of the features which doctors would consider “severe” but because their symptoms concern them or those around them. They also do not wish to be denied access to medication which they feel to be effective: there is a strongly held and widespread belief among patients that infection is the problem and antibiotics are the answer.21 This view, together with the doctor's willingness to prescribe them, provides fertile ground for a spiral of demand and supply.
In studies of over 2000 patients in primary care we noted that the decision to prescribe antibiotics for acute lower respiratory tract illness was influenced by non-clinical factors in nearly half of cases,3 ,21 common among which is the GP's desire to reduce re-attendance. Re-consultation during lower respiratory tract illness is very common with about one quarter of patients re-consulting once or more within a month of the index consultation.30 ,31 Over half will receive a further antibiotic even though evidence of active infection warranting an antibiotic is very unusual.30
GPs clearly recognise these influences, being willing to record that over three quarters of their own antibiotic prescriptions are not definitely clinically indicated (table 1). They acknowledge that patient pressure commonly influences their prescribing.3 ,21 Doctors may, however, overstate this pressure,32 perhaps to rationalise prescribing when they doubt the clinical indication but have neither time nor a strategy to react differently. GPs report that decisions about antibiotics and respiratory illness are the two commonest causes for prescribing discomfort.33 It is therefore clear that patients and doctors interact in a complex way in even apparently simple prescribing decisions.
The certainty of the decision to prescribe recorded by general practitioners for 1473 previously well adults treated with antibiotics for an acute lower respiratory tract illness.
Natural history of acute lower respiratory tract illness
Symptoms resolve slowly. Verheij et alfound that patients had coughed for an average of nearly two weeks before consultation for acute bronchitis and that over a quarter had persisting purulent sputum and had not returned to their normal activities two weeks later.26 A quarter of patients therefore had symptoms for over a month. Williamson reported that almost half of patients with acute bronchitis were still coughing three weeks after their GP consultation.34 We found that the cough had been present a mean of nine days before consultation and that two thirds of patients were still disturbed by cough 10 days later, at which time a quarter had still not returned to normal activities.33 Typically, cough persists for over two weeks in 90% of patients and for over three weeks in 80%. A third of patients were still taking cough mixtures at two weeks.36-38
We can therefore conclude that the average patient with an acute lower respiratory tract illness has been bothered by symptoms for a week or more before consulting their GP and that, in spite of antibiotics, a significant proportion will have continuing symptoms two or more weeks later.
Symptoms which prompt consultation: the “trigger line”
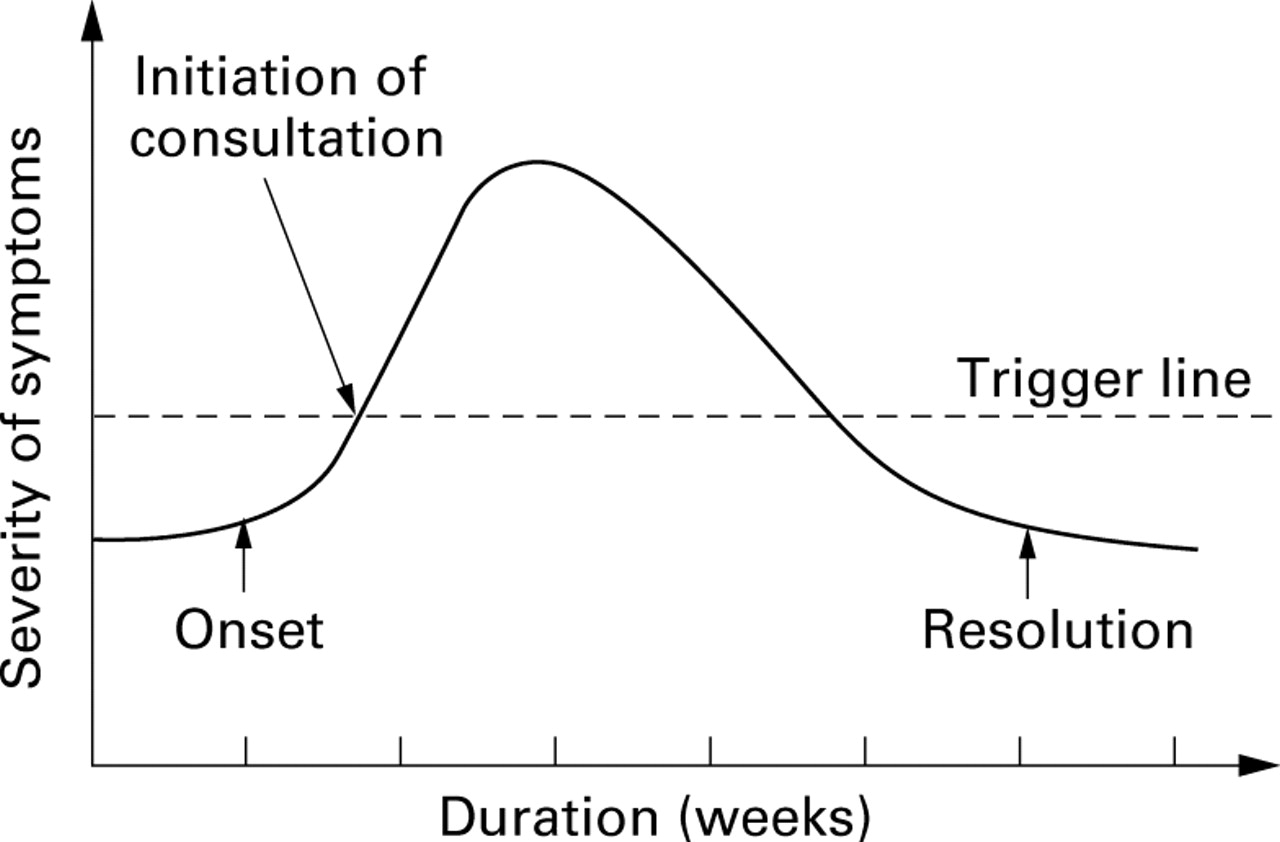
Teaching which is based solely on models of micro-organisms and the drugs which eliminate them is inappropriate. Let us consider instead lower respiratory tract illness in profile (fig 2) as a curve of symptoms from onset to resolution. Each patient has a horizontal “trigger line” which crosses the curve. Below it they tolerate their symptoms and above it they (or their family and friends) decide that “something must be done”. Where the trigger line crosses the symptom curve is the point at which patients seek medical attention or purchase medication over the counter. Those with a low trigger line tend to consult early in the natural history of their illness, well before the peak of their symptoms. The higher the individual's trigger line, the shorter is the duration of perceived troublesome symptoms.

{kind=link}
{kind=link}
Graphical representation of the natural history and duration of symptoms of lower respiratory tract illness. The “trigger line” represents the level of symptoms below which the individual patient tolerates the symptoms and above which the patient feels “something must be done”.
This concept of a symptom threshold is less familiar and less relevant to hospital practice, although the Accident and Emergency Department is one important exception. However, the actions which all doctors take influences subsequent patient behaviour29 and thoughtless, critical comments by a hospital doctor about prior antibiotic therapy, or the lack of it, is a powerful encouragement for future antibiotic dependence by both the patient and their GP.
What effect do antibiotics have on trigger lines?
PATIENTS WHO HAVE AN INFECTION LIKELY TO RESPOND TO ANTIBIOTICS
In this small group symptoms reflect bacterial or atypical respiratory infection. Antibiotics may modify either the severity or duration of the symptoms. In our analogy this will flatten and/or lower the curve in fig 2, reducing the area above the trigger line. But this is relatively uncommon, as randomised controlled trials suggest there is little or no benefit from antibiotics for most patients.15-17 This group probably includes some of the small proportion of patients with acute lower respiratory tract illness for whom their GP is confident that antibiotics are definitely clinically indicated (table 1).3 ,21
PATIENTS IN WHOM THE NATURAL HISTORY OF THE SYMPTOMS ARE NOT MODIFIED BY ANTIBIOTIC THERAPY BUT THE GP FEELS PRESCRIBING IS THE ONLY PRACTICAL OPTION
This is the much larger group of patients where the GP is uncertain whether antibiotics are indicated but still prescribes them—about 80% of cases in our studies. An antibiotic probably does not modify the natural history of the disease but it does influence the patient's belief in the need to see a doctor and to receive antibiotics for subsequent episodes, thus developing a cycle of re-consultation.
This further prescription reinforces dependence on this strategy for future episodes, lowering their trigger line. We found that the most powerful predictor of re-consultation was prior consulting habit.39 Little et al have shown that patients prescribed an antibiotic for sore throat are more likely to re-consult for future episodes due to “medicalisation” of the condition.40
GPs most commonly prescribe antibiotics for acute lower respiratory tract illness for five or seven days,3 by which time symptoms have rarely subsided. In a quantitative systematic review of randomised placebo controlled trials of antibiotics for acute bronchitis, Fahey et al calculated that only 9% of patients treated with antibiotics reported improvement after 11 days.15 Patients usually re-consult around eight or nine days after their initial consultation—that is, about two days after finishing their antibiotics.37 ,38 Having been told they have an “infection” and given antibiotics to cure it, patients not unreasonably assume that their failure to respond results from too short a course and/or the wrong antibiotic.
The way forward
UNHELPFUL STRATEGIES
We feel confident that the way forward is not by searching for new or more effective antibiotics, or by providing GPs with expert advice from secondary care or government that “you should not prescribe antibiotics”.13 ,41 Lower respiratory illness is often managed in less than ideal circumstances—empirical treatment, busy clinics, out of hours consultations—and when patients often have unrealistic expectations.
A MORE HELPFUL STRATEGY: ADJUSTING THE TRIGGER LINE
A better way forward may be to seek to alter patient behaviour and expectations—in our analogy, to raise the trigger line. This means not providing a prescription and a convenient clinicopathological label but to assess the likelihood of antibiotics modifying the illness and, where they will not, to identify the real reason for consultation. Reaching common ground between doctor and patient without the patient feeling “fobbed off” or rejected is far from easy, but works to the benefit of the practice and the patient.31
PATIENT AND COMMUNITY STRATEGIES
Education and information reduces dependence on and belief in the value of antibiotics in the community for minor illness. The Department of Health's National Advice to the Public campaign (NAP) will be ineffective without support.41 Information given to patients should address four issues: the long natural history of lower respiratory tract symptoms; the clear evidence for the lack of effectiveness of antibiotics; the increasing problem with antibiotic resistance of common respiratory pathogens; and side effects due to indiscriminate antibiotic use. Symptom curves may aid understanding without discouraging patients whose symptoms may point to significant infection.
DOCTOR STRATEGIES
The second arm of the Department of Health's initiative in primary care, the National Campaign on Antibiotic Treatment (CAT), recommends “no prescribing of antibiotics for simple coughs and colds” as the first of four objectives for GPs.41Doctors need to be aware of and have confidence in evidence based recommendations that antibiotics have little benefit in the management of most consultations for lower respiratory tract illness.15 Educating doctors in this way can reduce inappropriate use of antibiotics.42 Reassurance and education at the initial consultation takes longer than prescribing but results in more satisfied patients43 and is an investment which reduces consultations for minor symptoms and drug costs.44 ,45 Leaflets are an effective way of informing patients and modifying behaviour in primary care.29 ,38 ,40 ,46 If medication is needed, use of symptomatic remedies rather than antibiotics should be reconsidered as better and safer ways to raise the trigger line.
Passing the prescribing decision back to the patient is another pragmatic, if clinically uncomfortable, approach. In the management of sore throat, allowing patients to decide when and if to use a prescription for antibiotics reduces antibiotic usage by two thirds.29 Post-dated prescriptions when the need for an antibiotic is doubtful is another suggested strategy.41
The use of “open option” descriptions such as “chesty cough” and “chest cold”, which do not imply the presence of infection and the need for antibiotics, should be encouraged where appropriate.
RESEARCH STRATEGIES
More research is certainly needed. We have yet to develop ways of confidently identifying at presentation those patients in whom antibiotics will prove effective and those in whom they will not. For example, although a fifth of patients with the common cold may have a secondary nasopharyngeal bacterial infection and derive some minor benefit from antibiotics, they cannot be identified at presentation.47 However, it is clearly difficult; thoughtless pursuit of this benefit—which means giving antibiotics to everyone with a common cold “to be sure”—is a policy likely to fuel expectation and demand.
Our term “lower respiratory tract illness” describes briefly a simple and intuitive symptom complex which GPs can identify and record easily within a routine consultation. Encouraging the development of a common nomenclature for use in research would produce studies whose results could be more easily compared and applied in clinical practice.
Patients are not a homogeneous group; it is unlikely that any one educational intervention will prove universally effective. However, a simple information leaflet explaining the natural history of lower respiratory tract illness did significantly reduce re-consultation38 and is one of very few studies demonstrating benefit from a non-pharmacological intervention. We need to research other novel approaches.
Conclusions
Learning to use antibiotics wisely for acute respiratory symptoms is not easy and is not just a task for doctors in primary care. The teaching which undergraduates and trainees receive about respiratory infection from hospital based physicians has a powerful effect upon their future practice, whatever speciality they choose. Teaching should not just follow traditional approaches such as the treatment of “pneumonia” and “bronchitis”, but reflect the spectrum of acute respiratory illness, the often difficult pressures on prescribers, and the importance of learning the skills to cope with them. Developing joint teaching with departments of primary care may be particularly helpful for undergraduates, and the supervision of what trainees in medicine do and say demonstrates to GPs that hospital doctors appreciate these issues and support their efforts.
Concerns about overuse and over-reliance on antibiotics for respiratory illness are not new, yet these conditions continue to be poorly managed because of doctors' dependence on prescribed medication. Recommended management strategies should change to focus on techniques which raise the trigger line of individual patients and also the community. In this way we may reduce the distress caused to patients, their families, and to the community by this range of common, incompletely understood, and currently poorly managed symptom complexes.
How might we improve the management of lower respiratory tract illness in primary care?
- (1)
- Use a consistent nomenclature.
- (2)
- Discourage the use of labels such as “chest infection” and “bronchitis” which imply disease, the presence of infection, and the need for antibiotics.
- (3)
- Use open labels such as “chesty cough” which describe the symptom complex but do not drive the prescribing decision for antibiotics.
- (4)
- Recognise the long natural history.
- (5)
- Develop educational materials which explain this natural history and the lack of benefit for antibiotics to both individual patients and the community in most situations.
- (6)
- Encourage a better understanding of the issues by secondary care specialists.
- (7)
- Direct prescribing to answering questions such as: (a) which patients benefit from antibiotics, and how to identify them in routine consultations? (b) what is the spectrum of pathogens in lower respiratory tract illness? (c) which education strategies reduce antibiotic prescribing?
The following three questions merit further study:
When there is uncertainty in the doctors' decision to prescribe antibiotics, is sharing that uncertainty and involving the patient in the prescribing decision a useful strategy?
Do psychological markers of health seeking behaviour offer an insight into why some patients consult for lower respiratory tract illness?
Do episodes of lower respiratory tract illness have predictive value as a marker of the subsequent development of airways disease?
Acknowledgments
The authors thank Professor David Metcalfe, Professor Theo Verheij, and Dr William Jeffcoate for their valuable guidance and comments and gratefully acknowledge the many general practitioners who have contributed to the community studies.
References
Footnotes
Some of the community studies were funded by the British Lung Foundation, the Cooperative Society of Manchester, and by Rhone Poulenc Rorer.
Conflict of interest: none.