Article Text

Statistics from Altmetric.com
This document is the result of a joint initiative by the British Thoracic Society (BTS) and the Society of Cardiothoracic Surgeons of Great Britain and Ireland (SCTS) to produce detailed recommendations for the selection and management of patients with potentially operable lung cancer. It should be read in conjunction with other work on the subject produced by the Standing Medical Advisory Committee (SMAC),1 the BTS,2 the Royal College of Radiologists' Clinical Oncology Information Network (COIN),3 The Scottish Intercollegiate Guidelines Network (SIGN),4 and the Cancer Guidance Group.5These existing guidelines make clear the general need for an assessment of fitness and operability. The purpose of the present work is to increase the precision of these and other recommendations where the evidence allows, and thus to give more detailed advice to physicians, surgeons, and oncologists who manage potentially operable patients.
In addition to improving the accuracy of the selection process, it is hoped that these guidelines will also encourage a more positive approach to the radical treatment of patients with early lung cancer in the UK. Surgery6 and survival7 rates appear to be higher in the USA and Europe than in the UK, and there are indications that better and more uniform assessment of patients in this country might improve the current situation.8
Methodology
A joint BTS/SCTS Working Party was established comprising a core Writing Group and taking advice from specialist advisors representing the Royal College of Radiologists and the Royal College of Pathologists.
The major areas for concern in terms offitness for surgery were considered to be: (1) age; (2) pulmonary function; (3) cardiovascular fitness; (4) nutrition and performance status; and in terms ofoperability to be: (5) diagnosis and staging; (6) adjuvant therapy; (7) the operations available; (8) locally advanced disease; and (9) small cell lungcancer.
The available literature on these topics was examined by obtaining references from MEDLINE, BIDS and EMBASE databases, together with manual reviews of the reference lists of individual papers. The evidence was considered in Writing Group drafts incorporating the references, and recommendations were made based on the evidence, graded according to the SIGN system,9 using the Agency for Health Care Policy and Research (AHCPR) model10 (table 1). The draft conclusions were considered on several occasions by the full Working Party, modified, and then circulated to all the members of the BTS and SCTS for consideration. Conclusions were then revised again by the core Writing Group to take account of comments. The final draft was sent to the Macmillan Fund, BACUP, and SIGN for further comment.
Levels of evidence and grading of recommendations based on the US Agency for Health Care Policy and Research (AHCPR)10
This document summarises the major evidence on the subjects considered and draws conclusions derived from it which are presented as recommendations.
It is suggested that these guidelines should be reviewed in five years.
Summary of recommendations
PART I: FITNESS FOR SURGERY
Age
- 1.
- Perioperative morbidity increases with advancing age. Elderly patients undergoing lung resection are more likely to require intensive perioperative support. Preoperatively, a careful assessment of co-morbidity needs to be made. [B]
- 2.
- Surgery for clinically stage I and II disease can be as effective in patients over 70 years as in younger patients. Such patients should be considered for surgical treatment regardless of age. [B]
- 3.
- Age over 80 alone is not a contraindication to lobectomy or wedge resection for clinically stage I disease. [B]
- 4.
- Pneumonectomy is associated with a higher mortality risk in the elderly. Age should be a factor in deciding suitability for pneumonectomy. [B]
Pulmonary function
- 1.
- There should be formal liaison in borderline cases between the referring chest physician and the thoracic surgical team. [C]
- 2.
- No further respiratory function tests are required for a lobectomy if the post-bronchodilator FEV1 is >1.5 litres and for a pneumonectomy if the post-bronchodilator FEV1 is >2.0 litres, provided that there is no evidence of interstitial lung disease [B] or unexpected disability due to shortness of breath.
step 1
- 3.
- All patients not clearly operable on the basis of spirometry should have: (a) full pulmonary function tests including estimation of transfer factor (Tlco); (b) measurement of oxygen saturation on air at rest; and (c) a quantitative isotope perfusion scan if a pneumonectomy is being considered. [B] [B] [B]
- 4.
- These data should be used to calculate estimated postoperative FEV1 expressed as % predicted and the estimated postoperative Tlco expressed as % predicted, using either the lung scan for pneumonectomy or an anatomical equation for lobectomy, taking account of whether the segments to be removed are ventilated or obstructed.
step 2
- 5.
- (a) Estimated postoperative FEV1 >40% predicted and estimated postoperative Tlco >40% predicted and oxygen saturation (Sao2) >90% on air: average risk. [B]
- (b)
- Estimated postoperative FEV1 <40% predicted and estimated postoperative Tlco <40% predicted: high risk. [B]
- (c)
- All other combinations: consider exercise testing. [B]
- 6.
- Patients for whom the risk of resection is still unclear after step 2 tests should be referred for exercise testing. [B]
step 3
- 7.
- (a) A best distance on two shuttle walk tests of <25 shuttles (250 m) or desaturation during the test of more than 4% Sao2 indicates a patient is a high risk for surgery. [C]
- (b)
- Other patients should be referred for a formal cardiopulmonary exercise test. [C] For cardiopulmonary exercise testing peak oxygen consumption (V˙o2peak) of more than 15 ml/kg/min indicates that a patient is an average risk for surgery. [C]
- (c)
- A V˙o2peak of <15 ml/kg/min indicates that a patient is a high risk for surgery.
high risk patients
- 8.
- The management of these patients should be considered at a formal multidisciplinary meeting between a chest physician, surgeon, and an oncologist. [C]
- 9.
- Such patients could be considered for a more limited resection; radiotherapy/chemotherapy. [C]
Cardiovascular fitness
- 1.
- All patients for lung resection should have a preoperative ECG. [B]
- 2.
- All patients with an audible cardiac murmur should have an echocardiogram. [C]
- 3.
- Patients who have had a myocardial infarction should normally not be operated on for lung resection within 6 weeks. [C]
- 4.
- Any patient who has had a myocardial infarction within 6 months and is being assessed for thoracic surgery should have a cardiology opinion. [C]
- 5.
- Patients who have had coronary artery bypass surgery should not be precluded from having lung resection. They should be assessed as for other patients with possible cardiac risk factors. [C]
- 6.
- The guidelines from the American College of Cardiology and the American Heart Association should be used as a basis for assessing the perioperative cardiovascular risk of patients undergoing lung resection (table 2). [C]
major risk
- (a)
- These patients should have a formal cardiological assessment and their management discussed at a multidisciplinary meeting. [C]
- (b)
- Patients found to have significant lesions on coronary angiography should be considered for coronary artery bypass surgery before lung resection. [C]
intermediate risk
- (a)
- Patients in this group with reasonable functional capacity (able comfortably to walk up one flight of stairs) should not normally be regarded as at greater than average risk for postoperative complications. They do not need further cardiac testing. [C]
- (b)
- Patients with poor functional capacity and those in whom there is doubt about the degree of severity of their angina pectoris or who report breathlessness which may be due to cardiac disease should have an ECG monitored exercise test and echocardiogram and the results should be discussed with a cardiologist. [C]
minor risk
- Patients in this group with one risk factor should not normally be considered to be at greater than average risk for postoperative complications. [C]
- 7.
- Particular care should be taken in patients presenting with more than one cardiovascular risk factor. [C]
- 8.
- All patients with a history of previous stroke, transient ischaemic attacks, or carotid bruits should be assessed by carotid Doppler studies. Patients with evidence of significant stenoses (for example, over 70%) should be assessed by a vascular surgeon or consultant in stroke medicine preoperatively and their management discussed with the thoracic surgeon. [C]
Weight loss, performance status and nutrition
- 1.
- Patients presenting with a preoperative weight loss of 10% or more and/or a performance status of WHO 2 or worse are highly likely to have advanced disease and to require particularly careful staging assessment, together with a search for evidence of co-morbidity. [C]
- 2.
- Routine preoperative assessment should include a simple measure of nutritional status such as the body mass index, together with a serum albumin measurement. Low values should be accepted as conveying an increased risk of postoperative complications. [C]
Multiple risk factors
- 1.
- Patients anatomically suitable for resection but with more than one adverse medical factor should have their management discussed formally at a multidisciplinary meeting between a chest physician, a surgeon and an oncologist. [C]
PART II: OPERABILITY
Diagnosis and staging
- 1.
- All patients being considered for surgery should have a plain chest radiograph and a computed tomographic (CT) scan of the thorax including the liver and adrenal glands. [B]
- 2.
- Confirmatory diagnostic percutaneous needle biopsy in patients presenting with peripheral lesions is not mandatory in patients who are otherwise fit, particularly if there are previous chest radiographs showing no evidence of a lesion. [B]
- 3.
- Patients with mediastinal nodes greater than 1 cm in short axis diameter on the CT scan should undergo biopsy by staging mediastinoscopy, anterior mediastinotomy, or needle biopsy as appropriate. [B]
Operability and adjuvant therapy
- 1.
- The proportion of patients found to be inoperable at operation should be 5–10%. [C]
- 2.
- Patients with stage I (cT1N0 and cT2N0) and stage II (cT1N1, cT2N1 and cT3N0) tumours should be considered operable. [B]
- 3.
- Patients with stage I tumours have a high chance and those with stage II tumours a reasonable chance of being cured by surgery alone. [B]
- 4.
- Patients known preoperatively to have stage IIIA (cT3N1 and cT1–3N2) tumours have a low chance of being cured by surgery alone [B] but might be considered operable in the context of a trial of surgery and adjuvant chemotherapy. [A]
- 5.
- Participation in prospective trials of multimodality treatment for locally advanced disease is strongly recommended. [C]
- 6.
- Some small individual studies indicate a place for surgery in T4N0 and T4N1 tumours within stage IIIB, few long term data are available. Generally, stage IIIB tumours with node involvement and stage IV tumours should be considered inoperable. [B]
- 7.
- There is no place for postoperative radiotherapy following complete primary tumour resection. [A]
Operations available
- 1.
- Sublobar resection is a useful option in patients with impaired pulmonary reserve, but there is a higher local recurrence rate than with lobectomy and long term survival is decreased by 5–10%. [A]
- 2.
- Mortality following resection should not be in excess of 4% for lobectomy and 8% for pneumonectomy. [B]
- 3.
- Bronchoplastic resection may be appropriate in patients with impaired pulmonary reserve and in selected patients with advanced endobronchial lesions. [B]
- 4.
- Carinal resection is a technically demanding procedure with significant potential for major postoperative problems and an increased risk of local recurrence. Consideration should be given to concentrating such surgery in a few centres. [C]
- 5.
- The use of video-assisted thoracic surgery (VATS) for the resection of bronchogenic carcinoma is rare and limited data are available. It causes less postoperative pain than open surgery and appears to give similar long term results. [B]
- 6.
- Systematic lymph node dissection at the time of lung resection is essential to achieve accurate staging. [B]
- 7.
- The therapeutic value of radical lymphadenectomy is uncertain. [A]
Locally advanced disease
- 1.
- The management of individual patients with locally advanced disease should be discussed at multidisciplinary meetings involving physicians, surgeons, and oncologists. [C]
- 2.
- The results of surgery for locally invasive non-small cell lung cancer (NSCLC) are good when the lateral chest wall is involved. [B]
- 3.
- Highly selected patients with vertebral column involvement or superior sulcus tumours may be suitable for radical surgery, possibly in combination with other treatments. [B]
- 4.
- There is no case for surgery in these groups when mediastinal lymph nodes are involved. [B]
Small cell lung cancer
- 1.
- Surgery is appropriate treatment for stage I small cell lung cancer (SCLC). [B]
- 2.
- The incidence of subclinical metastatic disease is much higher in SCLC than in NSCLC and all patients being considered for surgery should be staged by CT scanning and mediastinoscopy and screened by scanning of bones and brain and iliac crest bone marrow sampling. [B]
- 3.
- Patients with small peripheral nodules should not be denied consideration for surgery on the basis of a needle biopsy showing SCLC.
Clinical predicators of increased perioperative cardiovascular risk. Adapted from Eagle et al.71
PART I: FITNESS FOR SURGERY
Age and lung cancer surgery
All patients should have equal access to lung cancer services regardless of age.11 It has been estimated that by 2005 more than 40% of all patients with lung cancer presenting in the UK will be aged over 75 years.12 In order to assess the effect of age on perioperative mortality, morbidity, and survival, 173 papers were reviewed. With improvements in anaesthetic and surgical techniques and postoperative care during the last 40 years, the older studies may be less relevant to modern practice. Most of the studies were small, retrospective and descriptive, particularly with respect to outcome in patients over 80 years, and only 70 were suitable for detailed attention. For this work we have defined elderly as 70 years or over, and very elderly as 80 years or over.
PERIOPERATIVE MORTALITY AND MORBIDITY
Older studies quoted mortality rates after resection in elderly patients of up to 15–20%13 ,14 but more recent data suggest rates of 4–10%.15 ,16 The more recent data also suggest that, up to the age of 80, age has no significant effect on mortality.16 ,17 There is evidence that the potential association between advancing age and operative mortality is a reflection of increased co-morbidity rather than age per se.18 ,19 As for younger patients, studies in the elderly have shown that mortality is increased after pneumonectomy—especially right pneumonectomy—compared with lobectomy. In the elderly, mortality rates from reported series average 14% (range 6–36%) for pneumonectomy16 ,20 compared with 4–7% for lobectomy.16 ,17 This difference in mortality is greater than in younger patients. However, these differences diminish if patients are very carefully selected with attention to co-morbidity.20 There is evidence that morbidity, particularly cardiovascular, is increased with advancing age, especially in the context of extensive surgery.21 ,22
SURVIVAL AFTER SURGERY
Although evidence is contradictory, the majority of studies have shown that at 2 years survival after surgery for lung cancer is similar in elderly patients to that in other age groups.22-24Beyond stage II, survival is very poor.
SURGERY IN THE VERY ELDERLY (80 YEARS AND OVER)
Most studies in octogenarians are small and involve patients presenting with stage I disease treated by lobectomy or more limited resection. Earlier studies suggested a high perioperative mortality rate25 but more recent reports suggest this has fallen, reflecting a similar fall in operative mortality seen previously in less elderly patients.26 ,27 It is unclear whether operative morbidity increases with very advanced age.28There is no convincing evidence that patients of this age with stage I disease have a worse prognosis than younger patients.25 ,27 There are no reports relating specifically to stage II disease. In patients with stage III disease survival is poor.25 ,29
Recommendations
- 1. Perioperative morbidity increases with advancing age. Elderly patients undergoing lung resection are more likely to require intensive perioperative support. Preoperatively, a careful assessment of co-morbidity needs to be made. [B]
- 2. Surgery for clinically stage I and II disease can be as effective in patients over 70 years as in younger patients. Such patients should be considered for surgical treatment regardless of age. [B]
- 3. Age over 80 alone is not a contraindication to lobectomy or wedge resection for clinically stage I disease. [B]
- 4. Pneumonectomy is associated with a higher mortality risk in the elderly. Age should be a factor in deciding suitability for pneumonectomy. [B]
Pulmonary function
Poor respiratory function is a concern because of the risks of perioperative morbidity and mortality, and the possibility of postoperative long term disability and poor quality of life secondary to respiratory insufficiency. Risks are related to the pre-existing pulmonary function and to the extent of the planned surgery.
Pulmonary function should be assessed when patients are clinically stable and on maximal drug treatment.
Recommendation
- 1. There should be formal liaison in borderline cases between the referring chest physician and the thoracic surgical team. [C]
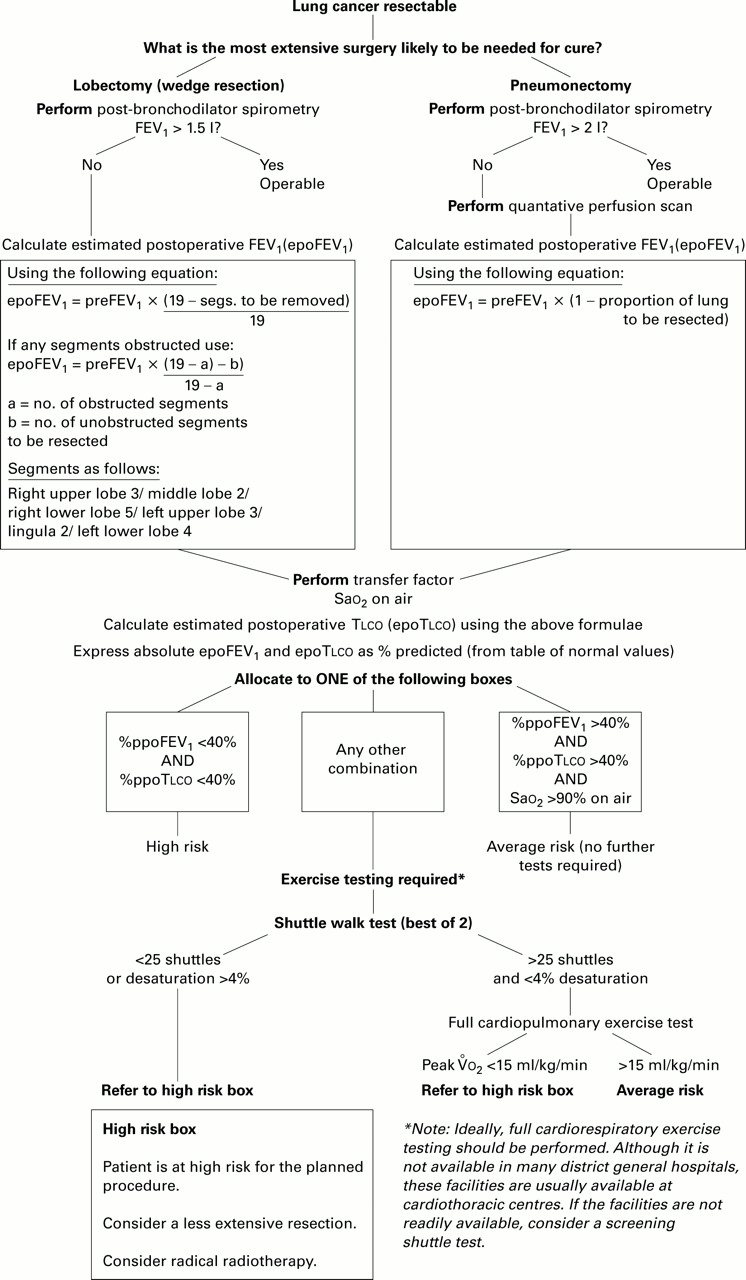
An approach to the selection of patients who are suitable for resection for lung cancer is set out in the algorithm in fig 1. Evidence for this is largely category B and category C. Few controlled data are available as patients deemed inoperable tend not to be operated upon.

Algorithm for selection of patients suitable for resection for lung cancer.
STEP 1
Spirometry
Data from more than 2000 patients in three large series in the 1970s have shown that a mortality rate of under 5% should be expected if the preoperative forced expiratory volume in one second (FEV1) is >1.5 litres for a lobectomy and >2 litres for a pneumonectomy.30-32 From these data the percentage estimated FEV1 as % predicted cannot be calculated and therefore this guideline cannot translate these absolute values to % predicted.
It is possible that some patients may have good spirometric values but a very low transfer factor (Tlco) because of diffuse interstitial lung disease or similar. These patients should be more fully assessed.
Recommendation
- 2. No further respiratory function tests are required for a lobectomy if the post-bronchodilator FEV1 is >1.5 litres and for a pneumonectomy if the post-bronchodilator FEV1 is >2.0 litres provided there is no evidence of interstitial lung disease [B] or unexpected disability due to shortness of breath.
- 3. All patients not clearly operable on the basis of spirometry should have: (a) full pulmonary function tests including estimation of transfer factor (Tlco); (b) measurement of oxygen saturation on air at rest; and (c) a quantitative isotope perfusion scan if a pneumonectomy is being considered. [B] [B] [B]
- 4. These data should be used to calculate estimated postoperative FEV1 expressed as % predicted and the estimated postoperative Tlco expressed as % predicted, using either the lung scan for pneumonectomy or an anatomical equation for lobectomy, taking account of whether the segments to be removed are ventilated or obstructed.
STEP 2
Calculation of postoperative lung function as % predicted
The calculation of postoperative lung function as % predicted for pneumonectomy and lobectomy is shown in boxes 1 and 2.
There is substantial evidence that the perioperative risks of resection are related to the absolute predicted postoperative FEV1 34-37 and the postoperative FEV1 expressed as % predicted.36-43 There is similar evidence for the independent measurement of the transfer factor.36 ,44-46
Although an absolute value of 800 ml for the predicted postoperative FEV1 may be adequate for resection,34 the two studies supporting this threshold30 ,34 mainly involved men. Using the % predicted FEV1 and Tlcoavoids women and the elderly being denied operations. For pneumonectomy there is a strong correlation between the postoperative FEV1 expressed as % predicted and calculated from the quantitative lung perfusion scans, and the actual values.31-34 ,38 ,47-51 For lobectomy there is a strong correlation between the postoperative FEV1 expressed as % predicted and the actual values when the calculation is made depending upon the number of segments to be removed at lobectomy.31 ,52 The calculation needs to be modified if any segments are obstructed.53
Whichever method is used, the calculated postoperative value tends to be an underestimate of actual postoperative values when patients have poor lung function—that is, estimates are conservative. Hence, those above the threshold are suitable for resection.
Thresholds for postoperative predicted values
A range of values for postoperative FEV1 between 34% and 45% predicted has been recommended as the lower limit of operability.40 ,41 For FEV1, the largest study38 recommended a figure of 40%. Similarly, for the Tlco 36 ,45 a figure of 40% has been recommended.38 The study by Pierce et al 36 supports the conclusion that both FEV1 and Tlco are independent prognostic factors.
Blood gas tensions and oxygen saturation at rest
Recent studies have shown that hypercapnia is not per se predictive of complications after resection, particularly if patients are able to exercise adequately.37 ,40 ,54 ,55 However, such patients are often precluded because of other adverse factors—for example, postoperative FEV1 and Tlco <40% predicted.
Ninan et al 56 found that there was a higher risk of postoperative complications among patients who either had oxygen saturation (Sao 2) on air at rest of <90% or desaturated by >4% from baseline during exercise.
Box 1: Calculation of postoperative lung function as % predicted for pneumonectomy
Pneumonectomy
Measurements:
- (1)
- Post-bronchodilator FEV1 (l) (pre FEV1)
- (2)
- Quantitative isotope lung scan (to obtain the fraction of the total lung perfusion present in the lung to be resected).
Calculation: Estimated postoperative FEV1 (l) (epo FEV1) = pre FEV1 × (1– fraction of total perfusion resected lung)
Expression: epo FEV1 (l) is expressed as % predicted
Transfer factor: This is measured and calculated as for FEV1. The calculated transfer factor will be an underestimate of the actual value.33
Box 2: Calculation of postoperative lung function as % predicted for lobectomy.
Lobectomy
Measurements:
- (1)
- Post-bronchodilator FEV1 (l) (pre FEV1)
- (2)
- Counting of lung segments to be removed: (a) number of obstructed segments to be resected (b) number of unobstructed segments to be resected
Calculation: Estimated postoperative FEV1 (l) (epo FEV1) = pre FEV1 × [(19 – a) – b]/ 19 – a Expression: epo FEV1 (l) is expressed as % predicted Transfer factor: this is treated in the same way as FEV1 Segments taken: right upper lobe 3; middle lobe 2; right lower lobe 5; left upper lobe 3; lingula 2; left lower lobe 4 (total = 19).
Recommendations
- 5. (a) Estimated postoperative (epo) FEV1 >40% predicted and epo Tlco >40% predicted and oxygen saturation (Sao2) >90% on air: average risk. [B]
- (b) epo FEV1 <40% predicted and epo Tlco <40% predicted: high risk. [B]
- (c) All other combinations: consider exercise testing. [B]
- 6. Patients for whom the risk of resection is still unclear after step 2 tests should be referred for exercise testing. [B]
STEP 3
Exercise testing
An inverse relationship between exercise capacity and postoperative complications has been demonstrated in a number of studies using both simple exercise tests such as six minute walks, stair climbs, and formal cardiopulmonary exercise tests.37-39 56-60
Desaturation during exercise testing by more than 4% indicates an increased risk of postoperative complications.56 Formal cardiopulmonary exercise testing studies have shown that a preoperative peak oxygen consumption (V˙o 2peak) of >15 ml/kg/min is associated with no appreciable increase in perioperative mortality and complications.35 ,38 ,43 ,54 ,55 ,61-63 Of the screening exercise tests available, the shuttle walk test64 is more reproducible64-67 and has a higher correlation withV˙o 2peak estimated by formal exercise testing than the six minute walk test.64 ,68 Stair climbing tests have not been standardised or compared. The regression equation developed by Singh et al suggests that 25 shuttles on the shuttle walk test indicate aV˙o 2peak of 10 ml/kg/min.64Thus, allowing for the 95% confidence intervals from this study, 25 shuttles suggests a V˙o 2peak of <15 ml/kg/min, which means that >95% of patients unable to complete 25 shuttles will have a V˙o 2 of <15 ml/kg/min.
Recommendations
- 7. (a) A best distance on two shuttle walk tests of <25 shuttles (250 m) or desaturation during the test of more than 4% Sao2 indicates a patient is a high risk for surgery. [C]
- (b) Other patients should be referred for a formal cardiopulmonary exercise test. [C] For cardiopulmonary exercise testing peak oxygen consumption (V˙o2peak) of more than 15 ml/kg/min indicates that a patient is an average risk for surgery. [C]
- (c) A V˙o2peak of <15 ml/kg/min indicates that a patient is a high risk for surgery.
HIGH RISK PATIENTS
Patients whose exercise tolerance is severely impaired should be considered to be at high risk (fig 1, high risk box).
Recommendations
- 8. The management of these patients should be considered at a formal multidisciplinary meeting between a chest physician, surgeon, and an oncologist. [C]
- 9. Such patients could be considered for a more limited resection; radiotherapy/chemotherapy. [C]
Cardiovascular fitness
Pre-existing coronary artery disease increases the risk of non-fatal myocardial infarction or death within 30 days of non-cardiac surgery.69 There are very few data on the specific risks of patients who are facing lung resection. An assessment of the risks facing such patients depends almost entirely on data relating to patients undergoing general non-cardiac surgery. Likewise, there are no specific data allowing quantification of the risks specific to patients with lung cancer who have co-existent peripheral vascular or cerebrovascular disease.
PREVIOUS MYOCARDIAL INFARCTION
There are no clinical trials on which firm recommendations can be made as to how long patients should wait after a myocardial infarction before thoracic surgery. However, clinical opinion supports an interval of 6 weeks, and a cardiological assessment if there has been a myocardial infarction within 6 months of planned surgery.
PREVIOUS CORONARY ARTERY SURGERY
Patients who have coronary artery bypass surgery are not at increased risk from general surgical operations for at least 5 years after the procedure, providing they have not developed recent symptoms.
PREOPERATIVE ASSESSMENT OF CARDIOVASCULAR RISK
The American College of Cardiology and the American Heart Association have published comprehensive guidelines for the clinical prediction of perioperative risk.70 ,71 These are based on clinical predictors (table 2), the patient's exercise tolerance, and type of surgery involved. A recently published study72 ,73has emphasised the importance of multiple risk factors (table3).
Importance of multiple risk factors
Non-invasive methods of assessing cardiac risk
ECG monitored exercise test: A gradient of increasing ischaemic risk is seen in association with the degree of functional incapacity, symptoms of ischaemia, and severity of ischaemia as assessed by exercise ECG changes.70 However, the degree of functional incapacity due to cardiac disease may be difficult to assess in patients with poor respiratory function. In such patients more specialised techniques such as pharmacological thallium scanning may be appropriate.70 ,71
Echocardiography: Although there is a positive relationship between decreased ejection fraction and postoperative mortality or morbidity, left ventricular function is not a consistent predictor of perioperative ischaemic events. Echocardiography may be of value in patients with dyspnoea of uncertain cause.
CEREBROVASCULAR DISEASE
A previous stroke is a minor risk factor for perioperative cardiac complications,70 although it has been identified as increasing risk.72 ,73 There are no data on the risks of a postoperative stroke in patients with a previous stroke undergoing thoracic surgery, but this may be more likely if there is evidence of carotid artery stenosis.74 This is best detected by Doppler studies.
Recommendations
- 1. All patients for lung resection should have a preoperative ECG. [B]
- 2. All patients with an audible cardiac murmur should have an echocardiogram. [C]
- 3. Patients who have had a myocardial infarction should normally not be operated on for lung resection within 6 weeks. [C]
- 4. Any patient who has had a myocardial infarction within 6 months and is being assessed for thoracic surgery should have a cardiology opinion. [C]
- 5. Patients who have had coronary artery bypass surgery should not be precluded from having lung resection. They should be assessed as for other patients with possible cardiac risk factors. [C]
- 6. The guidelines from the American College of Cardiology and the American Heart Association should be used as a basis for assessing the perioperative cardiovascular risk of patients undergoing lung resection (table 2). [C]
major risk
- (a) These patients should have a formal cardiological assessment and their management discussed at a multidisciplinary meeting. [C]
- (b) Patients found to have significant lesions on coronary angiography should be considered for coronary artery bypass surgery before lung resection. [C]
INTERMEDIATE RISK
- (a) Patients in this group with reasonable functional capacity (able comfortably to walk up one flight of stairs) should not normally be regarded as at greater than average risk for postoperative complications. They do not need further cardiac testing. [C]
- (b) Patients with poor functional capacity and those in whom there is doubt about the degree of severity of their angina pectoris or who report breathlessness which may be due to cardiac disease should have an ECG monitored exercise test and echocardiogram and the results should be discussed with a cardiologist. [C]
minor risk
- Patients in this group with one risk factor should not normally be considered to be at greater than average risk for postoperative complications. [C]
- 7. Particular care should be taken in patients presenting with more than one cardiovascular risk factor. [C]
- 8. All patients with a history of previous stroke, transient ischaemic attacks, or carotid bruits should be assessed by carotid Doppler studies. Patients with evidence of significant stenoses (for example, over 70%) should be assessed by a vascular surgeon or consultant in stroke medicine preoperatively and their management discussed with the thoracic surgeon. [C]
Weight loss, performance status and nutrition
A history of recent loss of weight, poor nutritional status, and a poor performance status (World Health Organisation (WHO) or Eastern Cooperative Oncology Group (ECOG) scales) (table 4) have all been independently associated in lung cancer with advanced disease and a poor overall prognosis.76 ,77 Such patients are often inoperable because of locally extensive or metastatic disease. However, there are few data on these factors as independent predictors of perioperative morbidity and mortality. As for cardiovascular risks, much of the data in the literature derives from studies on non-thoracic general surgery patients.
Performance status
WEIGHT LOSS
This is usually measured as a percentage loss of body weight compared with the patient's usual stable weight. There is no uniformity about what figure is clinically significant, but a figure of >10% is often quoted as indicating clinically significant weight loss. We know of no study which has specifically evaluated the perioperative risks of such patients.
PERFORMANCE STATUS
It is well known that the performance status (as measured by the WHO, Karnofsky or ECOG scales, table 4) is correlated with prognosis in inoperable lung cancer, both NSCLC and SCLC.77 ,78 In one surgical series of 331 patients the Karnofsky score was not an independent predictor of complications, but only a few patients with a poor performance status underwent surgery.79
Recommendation
- 1. Patients presenting with a preoperative weight loss of 10% or more and/or a performance status of WHO 2 or worse are highly likely to have advanced disease and to require particularly careful staging assessment, together with a search for evidence of co-morbidity. [C]
NUTRITION
In a recent UK series more than 40% of patients undergoing lung resection had a body mass index and skin fold thickness below the 25th centile.80 There is no agreement as to which of the various available measures of nutritional status are most appropriate for clinical work on patients with lung cancer but the possibilities include:
(a) an ideal body weight of <90%;
(b) a low body mass index, for example <18.5 (18.5 is IDEC grade I malnutrition);
(c) a triceps skin fold thickness of <25th centile compared with controls;
(d) a low albumin level.81 ,82
The consequences of poor nutrition are poor wound healing and, probably, a greater propensity to postoperative infection.83 ,84
Recommendation
- 2. Routine preoperative assessment should include a simple measure of nutritional status such as the body mass index, together with a serum albumin measurement. Low values should be accepted as conveying an increased risk of postoperative complications. [C]
Multiple risk factors
Patients often present with more than one abnormality of medical fitness for surgery. Individually these may not preclude surgery. However, there are no data on how these factors interact, and patients' suitability also depends on the extent of the proposed resection.
Recommendation
- 1. Patients anatomically suitable for resection but with more than one adverse medical factor should have their management discussed formally at a multidisciplinary meeting between a chest physician, a surgeon, and an oncologist. [C]
PART II: OPERABILITY
Diagnosis and staging
The subject of reporting resection specimens for lung cancer has recently been addressed in a minimum data set published by the Royal College of Pathologists85 and will not be considered further here.
A preoperative histological diagnosis is usually made following bronchoscopic examination or by percutaneous needle biopsy. However, only limited information may be available from bronchoscopic or needle biopsy specimens which, although reliable with regard to the diagnosis of malignancy, are less so in terms of tumour classification.86 Given that lung tumours show significant heterogeneity, small biopsy specimens should not be overinterpreted and a diagnosis of “invasive non-small cell carcinoma” is usually sufficient to distinguish the tumour from “small cell carcinoma” or “carcinoma in situ” at this point in patient management. Not infrequently no such evidence is available and investigations have to proceed on a presumptive basis. The presumption may be of diagnosis or of cell type. As fewer than 5% of patients with SCLC are operable, the following diagnostic and staging methods are predominantly for NSCLC. Stages and TNM classification in NSCLC are those described by Mountainet al 87 and are detailed in table 5.
TNM classification
A preoperative clinical assessment of tumour stage (cTNM) is made using a combination of imaging and surgical techniques.
IMAGING
Plain radiography
This should be done in postero-anterior and lateral projections using a high voltage (>125 kV) to ensure adequate penetration through the tumour and the mediastinum.
Computed tomographic (CT) scanning
CT scanning is recommended as a staging procedure for patients with NSCLC who are candidates for potentially curative surgery for the following reasons:
- (a) to identify enlarged mediastinal lymph nodes in order to determine the best approach for biopsy or aspiration cytology of the appropriate lymph node. The normal maximum short axis diameter is 14 mm, but nodes with a short axis diameter of more than 10 mm in normal subjects are rare and therefore 10 mm is widely regarded as the normal cut off point. The maximum short axis diameter is used in preference to the maximum long axis diameter because it does not depend on node orientation;
- (b) to determine the T stage to ensure resection is a realistic option;
- (c) to identify metastases in the chest or those portions of the abdomen included in the scanning volume, notably the liver and adrenal glands.
CT scanning may be performed with or without contrast enhancement, depending on local protocols and the ability to see the relevant mediastinal structures without the need for contrast. Contrast enhancement makes it easier for inexperienced observers to interpret the CT findings. Spiral CT scanning allows optimal contrast enhancement and should be used wherever practicable.
The accuracy of CT scanning for T and N staging is poor—for example, for N staging the sensitivity and specificity are approximately 60–65% and 60–70%, respectively.88 ,89 Overall, preoperative CT staging has been shown to overstage or understage when compared with operative findings in 40% of patients.90This means that patients should not be denied surgery on equivocal CT findings, and histological or cytological confirmation of intrathoracic lymph node involvement is required for patients in whom the only contraindication to potentially curative surgery is lymph node enlargement.
Magnetic resonance imaging (MRI)
MRI of the chest has not been shown to be a useful routine staging technique.88 The indications for MRI are restricted to clarifying the degree of invasion of the mediastinum, root of the neck, chest wall, or diaphragm where doubt exists regarding operability following CT scanning.
MRI has no advantage over CT scanning for the evaluation of enlarged lymph nodes
Positron emission tomography (PET)
PET is only available in a few centres. It has been shown to be the most accurate imaging investigation for the confirmation or exclusion of intrathoracic lymph node metastases from lung cancer (average sensitivity 88%, average specificity 93%).91 It is best used in conjunction with CT scanning for accurate localisation and interpretation and is advocated as a routine test in those centres where it is available. The use of routine PET scanning can indicate metastatic disease in mediastinal nodes which are of normal size on the chest CT scan, thereby leading to biopsy which can save formal thoracotomy for those patients in whom thoracotomy would not be beneficial.
Isotope scans and screening for distant metastases
In squamous cell cancer the yield from isotope bone scans or brain MRI or CT scans is less than 5%,92 although it may be higher in adenocarcinoma and it is definitely higher in SCLC (see later). If the patient has no symptoms suggestive of metastatic disease these investigations are generally not indicated, although one recent pilot study has suggested that high quality contrast enhanced MRI scans may reveal clinically occult metastases in a significant proportion of patients.93 Specialised sequences (chemical shift/opposed phase imaging) can distinguish incidentally discovered benign adenomas of the adrenal gland from adrenal metastases.94 It is convenient and easy to include the liver and adrenal glands in a CT scan of the thorax, however, and this is recommended.95
SURGICAL TECHNIQUES
Percutaneous needle biopsy
This technique96 has a high diagnostic success rate with acceptably low morbidity. In patients with peripheral lesions who are unfit for surgery needle biopsy may be invaluable, and it may also be necessary in patients being considered for a trial where preoperative diagnosis is an entry criterion. However, a negative biopsy does not necessarily rule out cancer in an at risk patient and a positive biopsy merely confirms that surgery should be considered.
SURGICAL STAGING
Bronchoscopy
Although primarily a diagnostic tool in lung cancer, indirect evidence of N stage and direct evidence of T stage can be gained in some cases (see table 5).87 Paralysis of a vocal cord (usually the left) implies extracapsular spread to mediastinal nodes, an indication of inoperability.97 The position of a visible tumour endobronchially dictates its bronchoscopic stage and indicates the type of resection which will be necessary for complete bronchial tumour clearance.
Mediastinoscopy and anterior mediastinotomy
Although the value of mediastinoscopy as a staging procedure is widely accepted,98 ,99 the precise indications are not universally agreed and the extent to which CT scanning can be used reliably to assess mediastinal (N2 and N3) nodes remains controversial. Mediastinoscopy gives access to nodes at stations 1–4 on the regional lymph node map (fig 2),100 the superior mediastinal or paratracheal nodes. It may also give access to station 7 (subcarinal) nodes and occasionally to station 5 (subaortic) nodes, but left anterior mediastinotomy101 is more reliable for this group and for station 6 (phrenic) nodes. Stations 8 and 9 are inaccessible from these approaches.

{kind=link}
{kind=link}
Regional lymph node map. Reproduced with permission from Mountain and Dresler.100
In patients with no obvious mediastinal lymphadenopathy, particularly those with small peripheral tumours, mediastinoscopy may be omitted102 although a proportion of those with apparently early tumours will have microscopic lymph node metastases.103
Thoracoscopy
The presence of a pleural effusion containing malignant cells on simple aspiration indicates inoperability87 but an effusion resulting from consolidation distal to an obstructing lesion does not, and in case of doubt thoracoscopy is indicated. Greater experience with this technique may demonstrate its value for obtaining biopsy specimens of nodes at stations 8 and 9, but at present it is employed mainly to assess pleural disease.
ASSESSMENT OF OPERABILITY
Assuming satisfactory performance status, operability depends on the clinical assessment of tumour stage derived from the above investigations.
Preoperative clinical (cTNM) staging, as accurately as possible given the limitations of the investigations available, is therefore crucial.
Recommendations
- 1. All patients being considered for surgery should have a plain chest radiograph and a computed tomographic (CT) scan of the thorax including the liver and adrenal glands. [B]
- 2. Confirmatory diagnostic percutaneous needle biopsy in patients presenting with peripheral lesions is not mandatory in patients who are otherwise fit, particularly if there are previous chest radiographs showing no evidence of a lesion. [B]
- 3. Patients with mediastinal nodes greater than 1 cm in short axis diameter on the CT scan should undergo biopsy by staging mediastinoscopy, anterior mediastinotomy, or needle biopsy as appropriate. [B]
On the basis of these investigations, cTNM staging should be possible87 and appropriate surgery undertaken in the light of current knowledge of results (see later).
Operability and adjuvant therapy
“open and close” thoracotomy
Despite efforts to determine operability by careful staging, some patients will be found at operation to have disease which cannot be resected. There are few data to suggest what proportion of patients this should be. A figure of 5% has been suggested104 and reported,102 although in this study a similar number had what are reported as “incomplete resections”. According to the SCTS UK Thoracic Surgical Register105 the rate of “open and close” procedures has remained in the range 10–11.4% of the total number of thoracotomies for lung cancer for the last 5 years. As imaging techniques become more accurate this should fall to nearer the target rate of 5%.
Recommendation
- 1. The proportion of patients found to be inoperable at operation should be 5–10%. [C]
ADJUVANT THERAPY
Adjuvant therapy can be given pre or postoperatively and can consist of radiotherapy or chemotherapy, or both. Almost no possible permutation of the three treatment options has been left untried, but few firm conclusions can be drawn.
A recent meta-analysis of 14 trials of surgery versus surgery plus chemotherapy showed a long term survival benefit of 5% for those having both,106 but most patients entered in these trials had stage III disease. Little is known about the possible advantages of chemotherapy in stage I disease. Recent individual trials107 ,108 have shown most benefit from neoadjuvant or induction chemotherapy employing multidrug regimes containing cisplatin in patients with stage IIIA disease. Three multicentre randomised trials are currently in progress to assess the effects of adjuvant chemotherapy.
Adjuvant radiotherapy was thought to offer some benefit in patients with stages II and IIIA disease following presumed complete resection, but meta-analysis of available trial results suggests an adverse effect in stage I and II disease and no advantage in stage III disease.109 There are no controlled data on the common practice of giving postoperative radiotherapy to patients found to have “positive resection margins”—that is, unresected local disease—but there is some evidence that it is of value.110
The status of adjuvant therapy is changing as new treatments become available and dogmatic statements about the groups likely to benefit would be inappropriate as they might rapidly become out of date, but the following recommendations can be made.
Recommendations
- 2. Patients with stage I (cT1N0 and cT2N0) and stage II (cT1N1, cT2N1 and cT3N0) tumours should be considered operable. [B]
- 3. Patients with stage I tumours have a high chance and those with stage II tumours a reasonable chance of being cured by surgery alone. [B]
- 4. Patients known preoperatively to have stage IIIa (cT3N1 and cT1–3N2) tumours have a low chance of being cured by surgery alone [B] but might be considered operable in the context of a trial of surgery and adjuvant chemotherapy. [A]
- 5. Participation in prospective trials of multimodality treatment for locally advanced disease is strongly recommended. [C]
- 6. Some small individual studies indicate a place for surgery in T4N0 and T4N1 tumours within stage IIIB, few long term data are available. Generally, stage IIIB tumours with node involvement and stage IV tumours should be considered inoperable. [B]
- 7. There is no place for postoperative radiotherapy following complete primary tumour resection. [A]
Operations available
Surgical resection of lung cancer may be performed by a variety of operative procedures which exist within an escalating hierarchy of complexity and extent of pulmonary resection. These procedures may be classified as:
- (1)
- Sublobar resection:
- (a) wedge
- (b) segmental
- (2)
- Standard major pulmonary resection:
- (a) lobectomy
- (b) bilobectomy
- (c) pneumonectomy
- (3)
- Bronchoplastic resection:
- (a) sleeve resection
- (b) carinal resection
- (4)
- Video-assisted thoracic surgery (VATS).
In addition, the method of intraoperative management of mediastinal lymph nodes should be considered, with two broad options:
- (1)
- Sampling:
- (a) opportunistic
- (b) systematic
- (2)
- Clearance.
SUBLOBAR RESECTION
This may be performed for a peripheral carcinoma either by excising a non-anatomical wedge of lung tissue or by resection of the related bronchopulmonary segment. Both appear to offer a useful therapeutic option for surgical candidates with markedly reduced FEV1. Reported operative mortality rates are low, ranging from 1.4% to 3.5%,112-115 which is therefore similar to that of better risk patients undergoing conventional lobectomy. Patients are usually selected to be in clinical stage I, but assessment can be inaccurate with one study reporting 32% of cases in either stage II or III. Local recurrence rates are higher than those anticipated with lobectomy, ranging from 14%115 to 23%116 overall, and are considerably higher when stage III lesions are considered (59%).114 Long term survival rates appear to be between 5% and 10%, less favourable than with lobectomy,112 ,116 although a prospective Lung Cancer Study Group randomised trial117 reported survival to be equivalent to that with lobectomy. In this study, however, patients with local recurrence after wedge resection were then offered formal lobectomy. The literature is limited but consistent. Most reports are of retrospective series112-116 and the one randomised prospective trial was analysed on an intention to treat basis which understates the failure rate with sublobar resection.
Recommendation
- 1. Sublobar resection is a useful option in patients with impaired pulmonary reserve, but there is a higher local recurrence rate than with lobectomy and long term survival is decreased by 5–10%. [A]
STANDARD MAJOR PULMONARY RESECTION: PNEUMONECTOMY AND LOBECTOMY
Pneumonectomy and lobectomy are consistently described with mortality rates of 6–8% and 2–4%, respectively.118-122 The Lung Cancer Study Group118 reported a prospective analysis of 783 patients undergoing various degrees of resection and found no significant difference between morbidity rates between lobectomy (28.2%) and pneumonectomy (31.9%). They, with others119-121 reported that the operative risk and morbidity is increased by advancing age, ischaemic heart disease, right sided resection (pneumonectomy), preoperative chemoradiotherapy, poor performance status, and impaired respiratory function. In highly selected cases, however, excellent mortality figures can be achieved for elderly patients.122
Overall survival results have changed little in 30 years and largely reflect TNM stage.123 ,124 Comparing historical125 with contemporary series,126 ,127 however, an improving trend can be seen, presumably as a result of better patient selection. Some data would suggest that young patients (<40 years old) do particularly badly,128 reflecting advanced stage at presentation and aggressive tumour behaviour.
Typical 5 year western survival rates129 ,130 for post-resectional staged (p) NSCLC are: T1–2N0 50–70%, T1–2N1 35–50%, and T1–2N2 20–30%. Survival may be better in some series with squamous cell carcinoma but others do not confirm this effect, particularly for small peripheral lesions. Tumours identified on preoperative mediastinoscopy to have N2 disease have very poor 5 year survival.131 ,132
T3 tumours, on the other hand, do have useful 5 year survival when nodal spread is limited and resection complete: pT3N0 45%, pT3N1 37%, pT3N2 0%.133
Bilobectomy134 ,135 may be associated with increased postoperative morbidity and may present problems due to the residual pleural space. Operative mortality is intermediate between lobectomy and pneumonectomy.136 Long term survival is similar to that generally obtained with lobectomy or pneumonectomy, but local recurrence may be more common than with conventional lobectomy.134
Although almost all available data regarding immediate and late outcomes after the standard major pulmonary resection procedures are derived from retrospective case series, the information is consistent and allows an accurate definition of expected mortality, morbidity, and survival rates.
Recommendation
- 2. Mortality following resection should not be in excess of 4% for lobectomy and 8% for pneumonectomy. [B]
BRONCHOPLASTIC RESECTION
Bronchoplastic and tracheoplastic resections, otherwise referred to as “sleeve” resections, allow the extension of lobectomy and pneumonectomy procedures to situations where tumour would normally lie at the resection margin. They are therefore of use in two circumstances; a parenchyma preserving lobectomy can be performed in patients with impaired pulmonary reserve where a pneumonectomy would otherwise have been required, and a pneumonectomy may be performed where tumour involves the very proximal bronchus or main carina and which would otherwise be deemed irresectable. These procedures are often more applicable to carcinoid and other intermediate grade bronchial lesions, but can be appropriate in highly selected, very localised bronchogenic carcinomas which are predominantly endobronchial or carinal in location.
These procedures are technically demanding. Bronchoplastic procedures are generally reported to have similar operative mortality to standard resections of 2.5–6.2%.136-140 Main carinal resection, however, carries an appreciable mortality of nearly 12%,141 ,142 even in experienced hands. This is usually performed as part of an extended right pneumonectomy,143 ,144 at which time an interval of up to 4 cm may be reconstructed between the trachea and left bronchus.144 Rarely, small lesions involving the carina only may be excised without pulmonary resection.144 Long term survival largely reflects the underlying disease stage,136-142 but local recurrence may be more likely with an incidence of 17% even with apparently complete resection.139 Relatively high morbidity is associated with the procedure, including damage to the recurrent laryngeal nerves.
These are rare procedures, especially main carinal resection. The available results come from a few units with significant series which may therefore overstate the results obtained when this procedure is performed on an occasional basis. It may be appropriate to question whether these resections should be restricted to centres with large and well established thoracic surgery programmes so that a few individuals can build up a significant level of experience.
Recommendations
- 3. Bronchoplastic resection may be appropriate in patients with impaired pulmonary reserve and in selected patients with advanced endobronchial lesions. [B]
- 4. Carinal resection is a technically demanding procedure with significant potential for major postoperative problems and an increased risk of local recurrence. Consideration should be given to concentrating such surgery in a few centres. [C]
VIDEO-ASSISTED APPROACHES
Video-assisted thoracic surgery (VATS) is a minimal access approach to the management of intrathoracic disease. No data are available regarding the long term outcome of wedge resection of peripheral bronchogenic carcinomas using a VATS approach, but there is no reason to suppose that it will not mirror the experience outlined above with open wedge resection.
VATS lobectomy is a rarely utilised approach to lobectomy (<2% of UK practice).145 The limited available data suggest that the perioperative morbidity and mortality are similar to open resection146 ,147 while perioperative pain is reduced.148 Long term survival, as judged by 3 year results following resection of bronchogenic carcinoma, is showing a similar trend to that of open lobectomy.147 ,148
One specific advantage of this minimally invasive approach is that it can be used immediately before proceeding with a standard resection in order to detect unsuspected causes of irresectability and thereby reduce the open and close thoracotomy rate.149
This surgical strategy is too early in its development to allow firm conclusions to be drawn regarding effectiveness. Further evaluation should ideally take place within the context of a randomised prospective study.
Recommendation
- 5. The use of video-assisted thoracic surgery for the resection of bronchogenic carcinoma is rare and limited data are available. It causes less postoperative pain than open surgery and appears to give similar long term results. [B]
LYMPH NODE MANAGEMENT
Management of mediastinal lymph nodes during major pulmonary resection follows surgical preference and ranges over a spectrum which extends from random sampling of suspicious nodes, through systematic dissection of each mediastinal node station, to radical block dissection of all mediastinal lymphatic vessels. The optimal approach remains the subject of debate. While there is little doubt that extensive harvesting of mediastinal nodes leads to accurate staging, there is uncertainty over the contribution that this process can make to survival. Exponents of block dissection point to excellent long term survival results with early stage lung cancer and attribute this to the removal of lymph nodes. Others argue that mediastinal lymph node status is, in fact, a relatively low level predictor of survival and that the apparently enhanced survival associated with dissection results from a “staging effect” whereby patients have simply been more accurately allocated to the relevant groups. Only one study150 has addressed this issue within the context of a prospective randomised trial. It compared block dissection with systematic dissection and found no survival benefit with block dissection. While the method of achieving detailed mediastinal assessment is less important, the value of accurately determining node status cannot be overemphasised. Without reliable staging there can be no basis for comparison of results and, ultimately, no ability to compare treatment strategies.
Recommendations
- 6. Systematic lymph node dissection at the time of lung resection is essential to achieve accurate staging. [B]
- 7. The therapeutic value of radical lymphadenectomy is uncertain. [A]
Locally advanced disease
When considering prognostic benefits, the decision to offer patients surgical resection of NSCLC is usually based on whether or not there are distant metastases and/or the extent of mediastinal lymphadenopathy. However, there is a small group of patients in whom there is a notable absence of these features, despite advanced local disease, associated with well preserved performance status. In these cases aggressive surgical treatment of the tumour may achieve a cure and should be considered, preferably by a team comprising physician, surgeon, and oncologist.
Recommendation
- 1. The management of individual patients with locally advanced disease should be discussed at multidisciplinary meetings involving physicians, surgeons, and oncologists. [C]
CHEST WALL RESECTION
About 5% of lung tumours extend locally across the parietal pleura to involve the chest wall. Historically, this was considered a sign of inoperability until Coleman described two patients who survived eight and 13 years after en bloc resection of lung and chest wall.151 Since then surgeons have increasingly extended resection to include the chest wall in appropriate cases.152-155
Invasion of at least the parietal pleura is consistent with stage T3. However, some peripheral tumours may be densely adherent to the parietal pleura at thoracotomy but, on pathological examination, show invasion only up to the visceral pleura. Staging in these cases is T2.
The presence of constant, localised, and increasingly severe chest wall pain at a site adjacent to a lung tumour abutting the adjacent internal aspect of the chest wall is a good predictor of significant chest wall invasion. The depth of this invasion may be predicted by the thoracic CT scan with an accuracy of up to 90%.156 Rib destruction or extension of the tumour into the muscles overlying the rib cage may be in evidence and can help in deciding the extent of chest wall resection necessary. MRI scanning of these structures gives more definition than CT scanning157 and may be a useful adjunct, especially when the tumour encroaches on the thoracic spine.
When chest wall adherence is encountered at thoracotomy, it is reasonable to attempt to dissect the tumour from the chest wall in the extrapleural plane. However, if any resistance is encountered, an en bloc chest wall resection should be considered as it may be that this is the only way to achieve complete resection. Failing to achieve the latter is a predictor of poor long term prognosis.153 ,154 ,158 In addition, lymph node metastasis, tumour stage and patient age all impact adversely on survival.
For all patients who have a complete en bloc resection for lung cancer with chest wall invasion, overall survival figures are 30–40%.152-154 ,158 In the absence of lymph node metastasis, however, in patients under 60 years of age a 5 year survival of up to 85% has been described.152 ,155
The value of adjuvant radiotherapy either before or after combined chest wall and lung resection is controversial.159However, if there is any doubt as to the completeness of the resection, then postoperative radiotherapy is logical to try to prevent local recurrence.
TUMOURS ADHERENT TO THE VERTEBRAL COLUMN
Involvement of a vertebra by a tumour can be anticipated when the patient complains of persistent pain overlying the appropriate part of the spine. Erosion of the vertebral body by an adjacent tumour may be visible on plain radiographs and CT scans, supplemented by MRI. Resection in these patients is generally not appropriate because of the dismal prognosis. In the absence of radiological evidence of bony erosion, however, thoracotomy can be contemplated in individual cases. It may be appropriate to collaborate with a neurosurgeon so that the vertebral resection can be accomplished, as this may be achieved more efficiently using a posterior approach.
There are a number of reports of pathologically complete tumour resection following removal of part160 or even the whole of a thoracic vertebra.161 Despite this, histological involvement of even the periosteum of the vertebrae is associated with a poor prognosis, even in the absence of lymph node metastases and tumour free margins after resection. These tumours have therefore been designated T4 on staging.
SUPERIOR SULCUS (PANCOAST) TUMOURS
Bronchogenic carcinomas arising at the apex of the lung often invade the lower portion of the brachial plexus, the upper ribs and thoracic vertebral bodies, the stellate ganglion, and the subclavian vessels. They produce a characteristic syndrome of pain and neurological deficit affecting the arm along with a Horner's syndrome. Respiratory symptoms are often completely absent because of the peripheral location of the tumour within the lung. Without specific treatment patients are usually dead within 10 months of diagnosis, with most experiencing severe unrelenting arm pain which makes this one of the most distressing forms of lung cancer.162 The standard view is therefore that patients with tumours at the lung apex who have any of these symptoms (other than mild to moderate shoulder or arm pain) should not undergo surgery.
Surgical management of these tumours was developed by Paulson and colleagues.162-165 Following these reports the standard approach in many parts of the world has been radiotherapy followed by resection via a posterolateral thoracotomy. Paulson recognised that the presence of a Horner's syndrome, invasion of the brachial plexus and subclavian vessels or vertebrae all implied a poor prognosis even with aggressive treatment. The standard view is therefore that patients who present with any of these features should not undergo surgery.
The value of preoperative radiotherapy has never been examined in a randomised trial or even in a non-randomised controlled fashion. The most useful data are provided in a retrospective report which suggested that preoperative radiotherapy did provide a significant survival benefit on multivariate analysis.166 Postoperative radiotherapy is less consistently used but is generally given when completeness of resection is in doubt. Data available show no survival benefit. If anything, there is a trend towards poorer survival in patients treated, implying a selection bias for patients with more advanced disease.167
More recently Darteville and colleagues have described an innovative approach in which the tumour is first explored via a supraclavicular anterior cervical incision.168 ,169 Following division and removal of the medial half of the clavicle, the relationship of the tumour to the subclavian vessels and their branches, the brachial plexus, and bony structures is demonstrated. This may allow for a safer and more complete dissection of the tumour from these structures than through a standard thoracotomy. The latter is employed following the cervical dissection, should it be necessary to extend the dissection into the thorax. Complete resection of the tumour, with vascular reconstruction if necessary, has led to an impressive 5 year survival rate in 31% of the 29 patients reported. Of note, the majority of patients received postoperative radiotherapy and chemotherapy and none had involvement of mediastinal lymph nodes by tumour.
Recommendations
- 2. The results of surgery for locally invasive non-small cell lung cancer (NSCLC) are good when the lateral chest wall is involved. [B]
- 3. Highly selected patients with vertebral column involvement or superior sulcus tumours may be suitable for radical surgery, possibly in combination with other treatments. [B]
- 4. There is no case for surgery in these groups when mediastinal lymph nodes are involved. [B]
Small cell lung cancer (SCLC)
Because of the more aggressive nature of this type of lung cancer, a much higher proportion of patients present with widespread metastatic disease than patients with NSCLC. The long term results following surgery were studied as part of an MRC trial published in 1973 which showed such a poor cure rate that many surgeons stopped resecting SCLC regardless of stage.170 The introduction of effective chemotherapy has since made a non-surgical approach widely accepted.
Unfortunately, when patients with limited disease are treated with primary chemotherapy, the majority experience an early relapse in the ipsilateral lung or mediastinal lymph nodes.171 This observation has led to a resurgence in resection as part of primary treatment of the disease. A number of reports, albeit with relatively small patient numbers, have shown that, with limited disease, long term cures are possible in a significant proportion.172-175Preoperative staging has been more rigorous, involving routine brain and bone scanning along with mediastinoscopy. These investigations show subclinical disease more frequently than in patients with NSCLC.
In appropriately selected patients the results of resection of early tumours are acceptable. In the Veterans Administration Surgical Oncology Group study of 132 patients the 5 year survival rates were: T1N0 59.5%, T1N1 31.3%, T2N0 27.9%, T2N1 9%, and any T3 or N2 3.6%.174 This study also made the important observation that the TNM staging system of NSCLC could be used to identify the subgroup of patients with limited SCLC who could benefit from surgery.
Scientific analysis of the place of surgery and/or chemotherapy in SCLC has been attempted in randomised studies176 but has yielded equivocal data. However, all patients undergoing resection of SCLC should be considered for postoperative chemotherapy to treat suspected micrometastases. In some centres preoperative chemotherapy and/or radiotherapy is routine.177 There is then debate as to the benefits of restaging patients prior to resection.178 ,179 Also of importance are the effects of preoperative treatments on the postoperative pathological stage of the tumour, which confounds attempts at comparative analysis of the various treatment modalities. Shepherd180 found no differences in survival between groups of patients who had surgery followed by chemotherapy or vice versa. Many early peripheral lung cancers can only be diagnosed histologically following a needle biopsy. In these patients a diagnosis of SCLC should be viewed with caution as a significant number prove to be NSCLC on examination of the resected specimen. Should these patients not undergo surgery because of the needle biopsy diagnosis, the opportunity for curing a patient with NSCLC will have been missed.177 Indeed, some tumours have both small cell and non-small cell components, making an accurate diagnosis based on a small biopsy specimen difficult.181
Pathologically, SCLC represents the aggressive end of a spectrum of neuroendocrine tumours of the bronchus which include atypical carcinoids.182 As such, SCLC comprises a heterogeneous group of variable clinical severity. It may be that the subgroup of patients who are cured by treatment are those with less aggressive SCLC than the majority of patients who will die early from the disease, regardless of treatment.
Recommendations
- 1. Surgery is appropriate treatment for stage I small cell lung cancer (SCLC). [B]
- 2. The incidence of subclinical metastatic disease is much higher in SCLC than in NSCLC and all patients being considered for surgery should be staged by CT scanning and mediastinoscopy and screened by scanning of bones and brain and iliac crest bone marrow sampling. [B]
- 3. Patients with small peripheral nodules should not be denied consideration for surgery on the basis of a needle biopsy showing SCLC. [B]
Acknowledgments
The authors are grateful to Mrs Pippa Bowie, research assistant, Clinical Effectiveness Unit, Kettering General Hospital and to the many secretaries and others who contributed to the production of the document.
References
Footnotes
Writing Group: Professor P Armstrong (Imaging), Dr J Congleton,* Mr S W Fountain (Chairman),* Dr T Jagoe, Dr D F McAuley,* Dr J MacMahon,* Dr M F Muers,* Mr R D Page,* Dr P K Plant,* Dr M Roland, Dr R M Rudd, Mr W S Walker,* Dr T J Williams*. Specialist advisors: Professor M I Saunders (Royal College of Radiologists), Dr A G Nicholson (Royal College of Pathologists).
* Members of the core Writing Group.
No sponsorship was sought or received in the production of the document and all authors made a declaration that they had no conflicts of interest in accordance with British Thoracic Society policy.