Article Text

Statistics from Altmetric.com
Airway inflammation in asthma: basic and clinical science
S1 INCREASED TACHYKININ LEVELS IN THE AIRWAYS OF ASTHMATIC PATIENTS AND CHRONIC COUGH PATIENTS WITH COEXISTENT GASTRO-OESOPHAGEAL REFLUX DISEASE
R. N. Patterson1, B. T. Johnston1, L. G. Heaney1,2, L. P. A. McGarvey1. 1Department of Medicine, Queens University Belfast, Belfast, N Ireland; 2Regional Respiratory Centre, Belfast City Hospital, Belfast, N Ireland
Background: Gastro-oesophageal reflux disease (GORD) may aggravate airway diseases including asthma and chronic cough. One postulated mechanism is via a vagally mediated distal oesophageal-tracheobronchial reflex associated with airway sensory nerve activation and tachykinin release. In this study we tested the hypothesis that patients with airways disease and GORD have increased airway tachykinin levels compared to those without GORD.
Methods: The study population consisted of 32 patients (all non-smokers) attending the chest clinic at the Belfast City Hospital. Sixteen subjects with asthma (eight female, mean age 55.2 years, FEV1 61–112% predicted) and 16 with non-asthmatic chronic cough (11 female, mean age 61.8 years, FEV1 80–127%predicted) were recruited randomly and underwent 24 hour oesophageal pH monitoring. GORD was defined as increased total oesophageal acid exposure (% total time >4.9% at the distal probe). All subjects underwent sputum induction and differential cell count were obtained and concentrations of substance P (SP), Neurokinin A (NKA), albumin, and a2-macroglobulin were measured in sputum supernatants.
Results: Comparing all subjects, the mean SP and NKA levels were significantly higher in patients with GORD compared to those without GORD (SP; 1433.97 pg/ml versus 905.95 pg/ml, p = 0.026, NKA, 81.04 pg/ml v 49.13 pg/ml, p = 0.014). Significantly increased tachykinin levels were also measured when asthmatic patients with GORD were compared to those without GORD, (SP; 1508.37 pg/ml v 736.68 pg/ml, p = 0.035, NKA; 103.15 pg/ml v 56.77 pg/ml, p = 0.02). Although SP and NKA levels were also increased in the cough patients with GORD this did not reach statistical significance, (SP; 1534.71 pg/ml v 1088.75 pg/ml, p = 0.198, NKA, 55.99 pg/ml v 49.77 pg/ml, p = 0.709). There was a trend towards a significant increase in % neutrophils in the asthmatic patients with GORD compared to those without reflux (82.1% compared to 54.6%, p = 0.074) with no difference in inflammatory cell counts among cough patients. No difference in albumin or a-2 macroglobulin levels were noted in GORD patients compared with those without GORD in either the asthma or cough group.
Conclusion: Such observations have not previously been reported and suggest sensory nerve activation in the airways of respiratory patients with GORD. Inhibiting tachykinin release may provide an alternative therapeutic option for reflux associated respiratory disease.
S2 CLINICAL AND PATHOLOGICAL FEATURES OF NON-EOSINOPHILIC ASTHMA: A DISTINCT ASTHMA PHENOTYPE ASSOCIATED WITH INHALED CORTICOSTEROID RESISTANCE
M. A. Berry, A. Morgan, R. H. Green, C. E. Brightling, A. J. Wardlaw, I. D. Pavord. Department of Respiratory Medicine, Glenfield Hospital, Groby Road, Leicester, UK
Non-eosinophilic asthma has been identified as a potentially important clinical phenotype since there is some evidence that it is associated with a poor response to inhaled corticosteroid therapy. No studies have investigated the underlying airway immunopathology and there are no data from placebo controlled studies examining the effect of inhaled corticosteroids. We set out to address these issues. All patients with asthma were symptomatic and had one or more of the following markers of variable airflow obstruction: methacholine PC20<8 mg/ml, increase in FEV1 of 15% or greater following inhalation of 200 μg of salbutamol and/or peak flow amplitude as percent of mean over 14 days of >20%. Endobronchial biopsies were taken from 11 patients with non-eosinophilic asthma, 12 patients with eosinophilic asthma, and 10 normal control subjects. The patients with non-eosinophilic asthma and six patients with eosinophilic asthma entered a randomised, double blinded, placebo controlled cross over study of inhaled mometasone 400 μg once daily for eight weeks. Patients with eosinophilic asthma had a median 23 bronchial submucosal cells positive for major basic protein per mm2 which was higher than both normal controls (0 cells/mm2, p = 0.043) and patients with eosinophilic asthma (4.4 cells/mm2, p = 0.016). Submucosal mast cells numbers were not different between the groups. However airway smooth muscle mast cell numbers were higher in eosinophilic asthma (8 cells/mm2) and non eosinophilic asthma (9 cells/mm2) compared to normal controls (0 cells/mm2, p = 0.016). There were no significant differences in the number of submucosal cells positive for neutrophil elastase. The subepithelial layer thickness was 10.3 μm in patients with eosinophilic asthma compared to 5.8 μm in non eosinophilic asthma and 5.1 μm in normal controls (p = 0.002). Eight weeks’ treatment with inhaled mometasone led to a net 5.5 doubling dose improvement in methacholine PC20 in patients with eosinophilic asthma and a 0.5 doubling dose improvement in the non-eosinophilic asthma group (mean difference 5.1 doubling doses, 95% CI 1.1 to 9.1; p = 0.018). There was a net 1.0 point improvement in Juniper asthma quality of life following treatment with inhaled mometasone compared to placebo in the eosinophilic asthma group and a 0.2 improvement in the non-eosinophilic asthma group (mean difference 0.9, 95% CI 0.27 to 1.43; p = 0.008).
Non-eosinophilic asthma represents a pathologically and clinically distinct disease phenotype which is characterised by absence of eosinophilic airway inflammation in sputum and bronchial biopsies, normal subepithelial layer thickness, and resistance to the effect of short term treatment with inhaled corticosteroids.
S3 MAST CELL MIGRATION TO TH2 STIMULATED AIRWAY SMOOTH MUSCLE FROM ASTHMATICS
A. Sutcliffe1, D. Kaur1, A. J. Ammit2, L. Woodman1, J. L. Black2, A. J. Wardlaw1, P. Bradding1, J. M. Hughes2, C. E. Brightling1. 1Institute for Lung Health, Leicester, UK; 2Respiratory Research Group, Faculty of Pharmacy and Department of Pharmacology, University of Sydney, Australia
Background: Mast cell microlocalisation within the airway smooth muscle (ASM) bundle is an important determinant of the asthmatic phenotype. We have reported that activation of mast cell CXCR3 by ASM derived CXCL10 is an important mechanism mediating mast cell migration towards ASM in asthma. We hypothesised that mast cells may also migrate towards Th2 stimulated ASM from asthmatic donors.
Methods: Primary ASM from subjects with (n = 7) and without (n = 5) asthma were stimulated with IL-1β, 4, and 13 alone and in combination. We investigated: (1) mast cell migration towards the supernatants derived from these ASM cultures using chemotaxis assays with and without chemokine receptor blockers for CCR3, CXCR1, 3 and 4; genistein or pertussis toxin and (2) the concentration of CCL11, CXCL8, CXCL10, TGF-b, and SCF in these supernatants measured by ELISA.
Results: HMC-1 cells migrated towards stimulated ASM supernatant from the subjects with asthma, but not to non-asthmatics for all of the activation conditions (p<0.0001). Similarly ASM supernatant stimulated with IL-1β, 4, and 13 from asthmatics was chemotactic for human lung mast cells (HLMC) (2.4-fold compared with control media; p = 0.007), but not ASM supernatant from non-asthmatics (1.3-fold; p = 0.45). The HMC-1 and HLMC migration was mediated predominantly through the combined activation of CCR3 and CXCR1. The concentration of CCL11 and CXCL8, but not the other chemotaxins measured, was markedly increased after stimulation. However, the concentration of all of the chemotaxins was not increased in ASM cultures from asthmatics compared to non-asthmatic controls.
Conclusion: These results demonstrate that stimulated asthmatic ASM is chemotactic for mast cells, but suggest that either an additional mediator is released from the asthmatic ASM that facilitates CCR3 and CXCR1-mediated migration or alternatively an inhibitory mediator is released by non-asthmatic ASM that attenuates mast cell migration.
Supported by: Asthma UK & DoH Clinician Scientist Award.
S4 DELETERIOUS EFFECT OF DIESEL FINE PARTICULATE EXPOSURE IN OXFORD STREET ON ASTHMA
J. E. McCreanor1, J. Stewart-Evans1, J. Zhang2, M. J. Nieuwenhuijsen1, M. Svartengren3, P. Ohman-Strickland2, L. Jarup1, K. F. Chung1, P. Cullinan1. 1Imperial College, London, UK; 2University of Medicine and Dentistry of New Jersey, New Jersey, USA; 3Karolinska Institute, Stockholm, Sweden
Epidemiological evidence indicates a link between respiratory morbidity and urban fine particulates, many of which are produced by diesel powered vehicles. We studied the direct effects of urban levels of diesel exhaust in asthma patients using a “natural exposure chamber”.
On separate occasions 60 non-smoking adult asthmatics (31 mild, 29 moderate (FEV1 (mean % predicted) 93.4 and 84.1 respectively, age range 19–51 years (median 28)) walked at a normal pace, for two hours, in Oxford Street, London (where only pedestrians, diesel powered buses, and taxicabs are permitted) or Hyde Park, a large, nearby open park free of vehicles. Lung function and symptoms were monitored during exposures and for 24 hours after. Real time measurements of PM2.5, Ultrafine Particles (UFP), CO, temperature, and humidity were performed, as well as integrated elemental carbon (EC)/PM2.5 and NO2 levels. Exposures took place outside the pollen season (November to March).
There were significant differences in concentrations of particulate pollution between exposure sites (UFP concentration (mean) 66626 pt/cc (SD 13674) and 19459 (SD 6431); p<0.0001), furthermore EC (median) was significantly higher in Oxford Street (7.51 v 1.27; p<0.0001). Lung function (FEV1 and FVC) decreased from baseline at both exposure sites; this decrement was largest and more sustained following Oxford Street exposure (−5.76% v −1.88% (FEV1); p<0.0001; two hours from the start of exposure). Increased acidification of exhaled breath condensate occurred two and four hours after Oxford Street compared with Hyde Park (p<0.0025, p<0.0039). There was an increase in sputum neutrophils, interleukin-8 (IL-8) and myeloperoxidase (MPO) 24 hours after Oxford Street exposure as compared with Hyde Park exposure (neutrophils: 57 (SEM 3)% v 50 (SEM 3)%); IL-8: 82.1 ng/ml v 66.8 ng/ml, MPO: 5.34 ng/ml v 1.59 ng/ml). There were no significant changes in the concentration of plasma oxidative stress markers. Increased asthmatic symptoms were reported immediately following the Oxford Street exposure.
This real world study shows that exposure to urban levels of diesel exhaust on Oxford Street causes temporary worsening of respiratory function, airway inflammation and increased symptoms among asthmatic subjects. This emphasises the need for asthmatics to take regular preventative treatment.
S5 THE PATHOLOGY OF SEVERE PRESCHOOL WHEEZE
S. Saglani1,2, D. N. Payne1, A. G. Nicholson3, Z. Wang2, J. Zhu2, P. K. Jeffery2, A. Bush1. 1Respiratory Paediatrics, Royal Brompton Hospital, UK; 2Lung Pathology, Imperial College, UK; 3Histopathology, Royal Brompton Hospital, UK
Background: Eosinophilic airway inflammation and thickening of the bronchial epithelial reticular basement membrane (RBM) are two characteristic pathological features of asthma that are present in adults and school aged children,1 but are not present in infants with the symptoms and lung function characteristics of asthma.2 We have previously described RBM thickening in preschool children with recurrent, severe wheeze.3 The aim of this study was to examine the relationship between RBM thickness and mucosal airway inflammation in the preschool group.
Methods: The density of immunologically distinct inflammatory cells (eosinophils, neutrophils, CD45+, CD4+, and CD8+ cells) was determined in endobronchial biopsies (EB) from 27 preschool children (median age 24 (range 4–58) months) undergoing a clinically indicated bronchoscopy for recurrent, severe wheeze. Wheeze was confirmed using a video questionnaire. Confirmed wheezers (n = 13, median age 31 (range 7–57) months) and reported wheezers (n = 14, median age 16 (range 4–58) months) were compared to 11 non-asthma controls (median age 22 (range 5–42) months) undergoing bronchoscopy for investigation of stridor. RBM thickness was also measured in EB.
Results: The density of tissue eosinophils was higher in subjects with confirmed wheeze compared to controls (median density in confirmed wheeze 1.07 (range 0–3.51)% v reported wheeze 0.72 (0–2.04)% v controls 0 (0–1.05)%, p<0.05 confirmed wheeze v controls). No other differences in tissue inflammation were found between groups. The RBM was significantly thicker in the confirmed wheezers compared to controls, (p<0.05; median thickness in confirmed wheeze 4.6 (range 2.9–7.7) mm v reported wheeze 3.5 (2.4–5.4) mm v controls 3.4 (2.0–4.7) mm).
Conclusion: These data demonstrate that the characteristic pathological features of asthma in adults and school aged children are already present in a group of preschool children (median age 31 months) but only in those with severe, confirmed wheeze.
1
2
3
S6 AIRWAY INFLAMMATION FOLLOWING SMOKING CESSATION IN ASTHMA
R. Chaudhuri1, E. Livingston1, A. D. McMahon2, I. Fraser3, J. Lafferty1, C. McSharry3, M. Spears1, N. C. Thomson1. 1Departments of Respiratory Medicine & 3Immunology, 2Robertson Centre for Biostatistics, University of Glasgow, Glasgow, UK
Background: Over 25% of adults with asthma are active smokers. Compared to non-smokers with asthma, smokers have more severe symptoms and an impaired therapeutic response to corticosteroids. Sputum neutrophil counts are increased in heavy smokers with mild asthma. The effect of smoking cessation on airway inflammation in asthma is not known. The aim of the study was to prospectively assess airway inflammation and lung function in smokers with asthma who successfully quit smoking compared to asthmatic smokers who continue to smoke.
Methods: Smokers (⩾10 pack years) with asthma who demonstrated ⩾15% reversibility of FEV1 after salbutamol were recruited. After baseline measurements, they were offered the option to quit or continue smoking and spirometry was recorded after 1, 3, and 6 weeks. Induced sputum was performed at 3 and 6 weeks for cell counts and mediator measurements (IL-8, MPO, ECP). Data were analysed using ANCOVA.
Results: Thirty two subjects were recruited. Eleven chose to continue in the study as control smokers and 12/21 subjects who opted for the quit group achieved six weeks of smoking cessation. There were no significant baseline differences in age, spirometry, induced sputum cell counts and mediators between the control and quit groups. Comparing quitters with control smokers at six weeks’ cessation, there was a mean improvement of 427 ml in FEV1, 15.3% in FEV1% predicted and 96 l/m in PEF and a reduction in sputum neutrophil count but no change in sputum mediator concentrations (see table).
Abstract S6 Mean (95% CI) difference between quitters and continued smokers (controls)
Conclusion: Six weeks after stopping smoking asthmatic smokers show a considerable improvement in lung function and fall in sputum neutrophil count compared to asthmatic smokers who continue to smoke. This reinforces the importance of smoking cessation in asthma.
Pulmonary hypertension: basic mechanisms
S7 THE ROLE OF PI3K/AKT IN HYPOXIC PROLIFERATION OF PULMONARY ARTERY SMOOTH MUSCLE CELLS
L. S. G. E. Howard, A. Sobolewski, E. R. Chilvers, N. W. Morrell. Division of Respiratory Medicine, Addenbrooke’s Hospital, Cambridge, UK
Introduction: Pulmonary arterial hypertension in association with chronic hypoxia is characterised by remodeling of the small resistance pulmonary arterioles, including smooth muscle cell proliferation and neomuscularisation of intra-acinar vessels. In culture, the growth of distal pulmonary artery smooth muscle cells (PASMC) is inhibited by hypoxia (PO2∼3 kPa) (
). However, we have previously isolated a subpopulation of cells from human PASMC cultures from distal pulmonary arteries (<1 mm) through survival selection under hypoxic conditions which proliferate in response to hypoxia (PASMC Hyp+) (
). The phosphatidylinositol 3-kinase (PI3K)/Akt-regulated pathway is an important prosurvival pathway. We sought to determine its role in the hypoxic proliferation of PASMC Hyp+.
Methods:Hypoxia: Cell culture medium was pregassed with 95%N2/%%CO2 and plates wre kept in airtight Perspex chambers gassed with 95%N2/%%CO2. Cell culture: PASMCs were isolated by microdissection of human distal pulmonary arteries from patients undergoing cancer resection. PASMC Hyp+ were grown up from low density (∼10 cells/well) in 96-well plates in hypoxic conditions in 20% fetal calf serum/Dulbecco’s modified Eagle Medium, and smooth muscle cell supplements (Promocell). Cell proliferation: Cells were plated in 48-well plates at 104 cells/well and quiesced for 48 hours in 0.1% serum under normoxic conditions. Medium was replaced with pregassed hypoxic medium for 24 hours and 3H-thymidine was added 6 hours before lysis. Western blotting: Cells were plated at 250×103 cells/60 mm plate and quiesced for 48 hours in 0.1% serum when at 90% confluence. After treatment, cells were lysed at 4 hours and total cell protein was electrophoresed on 10%SDS-PAGE and transferred to nitrocellulose membranes. Membranes were probed with specific antibodies to Akt (Cell Signalling) and HIF-1α and HIF-1β (BD transduction labs).
Results: PASMC Hyp+ were confirmed to proliferate in response to hypoxia unlike unselected cells (PASMC Hyp-). This proliferation was inhibited by the PI3K inhibitor, LY294002 (10 mM). However, when HIF-1α was stabilised with 1 mM dimethyloxallyl glycine (DMOG) (Alexis), proliferation of both PASMC Hyp+ and Hyp- populations was inhibited. HIF-1α activation was markedly greater with DMOG than hypoxia. Hypoxia induced phosphorylation of Akt was increased in PASMC Hyp+ compared with PASMC Hyp-.
Conclusion: Hypoxia suppresses proliferation of PASMCs, possibly through a HIF dependent mechanism. However, a subgroup of PAMSCs proliferate at physiological levels of hypoxia and this appears to be partly dependent on the PI3K/Akt pathway.
This work is funded by the British Heart Foundation.
S8 A ROBUST GRADING SYSTEM FOR VASCULAR REMODELLING IN SEVERE CHRONIC OBSTRUCTIVE PULMONARY DISEASE LUNG RESECTIONS
P. Vaughan1,2, K. Pinnion1, D. A. Waller2, M. L. Foster1. 1AstraZeneca R&D (Charnwood), 2Department of Thoracic Surgery, Glenfield Hospital, Leicester, UK
Objective: Currently there is no robust, standardised grading system that encompasses the heterogeneity of pulmonary vascular remodelling seen in severe chronic obstructive pulmonary disease (COPD). We describe the development and validation of a histology based scoring system from lung volume reduction surgery (LVRS) samples. A number of features seen in arterioles of patients undergoing LVRS have not been previously described.
Methods: Samples of lung were obtained from five patients. The sections were stained with haematoxylin-eosin, and vessels identified as part of a bronchovascular pair, or the most severely remodelled vessel upon that slide. Only vessels with intact intima, media and adventitia were included. The algorithm incorporates features such as sclerosis, apoptosis, hypertrophy, loss of internal elastic lamina, and reorientation of smooth muscle cells. The features are documented as intimal or medial and a score of 0, 1, or 2 is assigned if the feature is absent, involving a portion of the wall or the vessel is circumferentially affected. The intima, media, and total vessel score can then be calculated. Intra and interobserver variation was determined.
Results: 257 vessels were identified (183 bronchovascular pairs). Median total score was 9 (range 4–19). There was no significant difference between intima, media and total scores when assessed repeatedly by one observer (p = 0.92, p = 0.79, and p = 0.65 respectively), with a good correlation between attempts (r = 0.74, p = 0.01). An independent observer, blinded to the initial scores, assessed 10 randomly assigned bronchovascular pairs. The interobserver coefficient of variation was 14%. Assessment of sclerosis was the single feature of inter observer bias. Intima, media, and total score were all significantly higher in the worst vessels than the bronchovascular pairs (p<0.0001 in all groups). In this data set medial pathology was the main discriminator of overall score. Overall intrapatient variation was consistently greater than interpatient variability.
Conclusions: A wide range of severity of pulmonary arteriolar remodelling is present, reflecting the heterogeneity of COPD, despite samples taken from the most severely affected areas of lung. This algorithm can be used as a research tool to quantify the severity of arteriolar remodeling. Further work is ongoing in an extended LVRS patient cohort.
S9 STATINS INHIBIT HYPOXIC PROLIFERATION OF PULMONARY ARTERY FIBROBLASTS: POTENTIAL FOR THE TREATMENT OF PULMONARY HYPERTENSION
C. M. Carlin, A. J. Peacock, D. J. Welsh. Scottish Pulmonary Vascular Unit, Western Infirmary, Glasgow, UK
Introduction: Pulmonary artery fibroblasts (PAFs) play an important role in pulmonary vascular remodelling, as seen in pulmonary arterial hypertension and chronic hypoxic lung disease. Statins (5-HMG CoA reductase inhibitors) have been shown to reduce pulmonary vascular remodelling in rats exposed to chronic hypoxia and monocrotaline and it has been suggested that statins may be useful in the treatment of pulmonary vascular disorders (
;
). In this study we sought to explore the effects of statin drugs on acute hypoxic PAF proliferation: we have previously shown that changes in proliferation and intracellular signalling in PAFs exposed to acute hypoxia mirror those seen in chronic hypoxia (
).
Methods: PAFs were harvested from lobar artery of Wistar rats (maintained in normoxic conditions) and used between passages 4–9. Cells were quiesced for 24 hours then stimulated with 1% serum +/− addition of simvastatin 1 μM (S), fluvastatin 1 μM (F), or mevalonic acid 1 mM (M). Cells were maintained in normoxic or hypoxic (PO2 = 35 mm Hg) conditions for 24 hours. Fibroblast replication was measured by [3H] thymidine uptake.
Results: [3H] thymidine incorporation was significantly increased in PAF cells exposed to hypoxia. Addition of simvastatin or fluvastatin blocked hypoxia associated proliferation. Addition of mevalonic acid (the immediate product of 5-HMG CoA reductase) negated the inhibitory effect of statins.

Conclusions: Hypoxic proliferation in PAFs is dependant on mevalonic acid or its downstream products. Further work is required to assess the potential of statins for the treatment of disorders in which there is chronic hypoxia and/or excessive PAF proliferation.
S10 CHARACTERISATION OF THE VASODILATORY ACTION OF TESTOSTERONE IN THE HUMAN PULMONARY CIRCULATION
A. M. Smith12, R. T. Bennett3, T. H. Jones1, 4, M. E. Cowen3, K. S. Channer2, 5, R. D. Jones1. 1Hormone & Vascular Biology Group, The University of Sheffield, Sheffield, UK; 2Royal Hallamshire Hospital, Sheffield, UK; 3Castle Hill Hospital, Cottingham, UK; 4Barnsley Hospital, Barnsley, UK; 5Faculty of Health and Wellbeing, Sheffield Hallam University, Sheffield, UK
Aim: This study was carried out to assess for the first time, the vasodilatory effect of testosterone in the human pulmonary circulation. The influence of gender, vessel size, endothelial function, and effect of past medical history upon the response to testosterone was studied in isolated human pulmonary arteries and veins and in isolated perfused whole lungs.
Methods: Isolated human pulmonary arteries and veins were studied by wire myography. Vessels were obtained from male (n = 7, age 65 (SD 3) years) and female (n = 6, age 56 (SD 7) years) patients. Vessels were preconstricted with U46619 (1 μM) and endothelial integrity was tested with acetylcholine (1 μM). Vessels were then washed before the addition of U46619 (1 μM) before exposing them to either testosterone or ethanol vehicle. Isolated lungs were studied in a ventilated and perfused model (methodology described in (Bennett, 2004 #435)). Lung samples (n = 12) were obtained from male (n = 6, age 62 (SD 7) years) and female (n = 6, age 66 (SD 4) years) patients. They were exposed to potassium chloride (KCl) (100 mM), prior to the addition of either testosterone (1nM-100 μM) or ethanol vehicle.
Results: In the isolated human pulmonary arteries, testosterone caused significant vasodilatation (fig 1A). Results from the isolated perfused human lung model showed greater responses to testosterone than the pulmonary arteries (1B). There was however no significant difference in the magnitude of the response to testosterone between the sexes.
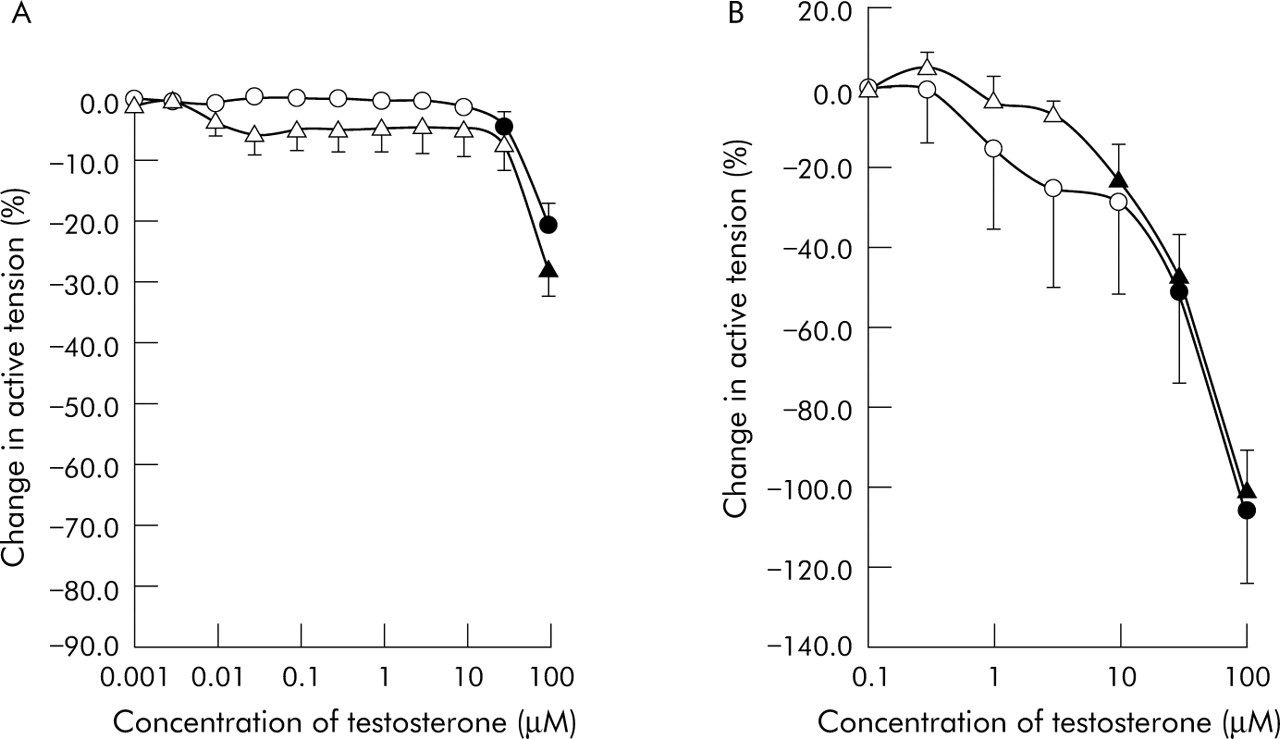
Conclusion: Testosterone acts as an efficacious vasodilator in the human pulmonary circulation, with no marked differences observed in the response dependant on sex. Testosterone may therefore be a potential novel agent in the treatment of pulmonary vascular disease, namely pulmonary hypertension.
S11 CHARACTERISATION OF REGULATORY ELEMENTS IN THE BMPR2 GENE PROMOTER
L. Long1, R. Machado2, R. C. Trembath2, N. W. Morrell1. 1Division of Respiratory Medicine, Department of Medicine, University of Cambridge School of Clinical Medicine, Addenbrooke’s and Papworth Hospitals, Cambridge, UK; 2Division of Medical Genetics, University of Leicester, UK
Mutations in the coding sequence of the bone morphogenetic protein type II receptor (BMPR-II) underlie many cases of familial, and some sporadic cases, of pulmonary arterial hypertension (PAH). However, about 30% of familial PAH do not harbour mutations in the BMPR2 coding sequence. In addition, we have reported that reduced lung vascular expression of BMPR-II is a feature of all PAH, whether or not a mutation exists in the BMPR2 coding region. These observations justify characterisation of the BMPR2 gene promoter for regulatory regions and a potential site of further mutations. We cloned a 5 kB human BMPR2 promoter into a luciferase reporter gene construct PGL-3 and transfected this into Hela cells. The presence of the 5 kB promoter resulted in a 15–30 fold increase in luciferase activity compared with vector alone. Using a series of deletion constructs we identified at least two cis-acting activating regions and one powerful repressor region. Analysis of the promoter sequence revealed putative NF-AT/PU-1 transcription factor binding sites in the repressor region. Mutation of this region (1.7 kB M1), or deletion of this region (1669 kB) restored promoter activity, implicating this region as the transcriptional repressor. EMSA assays demonstrated specific binding of nuclear protein to this region. In preliminary experiments, TNF-α markedly suppressed transcription of BMPR-II. Sequencing of the regulatory regions of the BMPR2 promoter in patients with PAH has revealed novel sequence variants. The functional significance of these variants is under investigation. Our findings suggest the presence of novel regulatory elements in the BMPR2 promoter that may be critical in the suppression of BMPR-II expression found in PAH.
Bronchoscopy in the diagnosis and treatment of lung tumours
S12 PROSPECTIVE STUDY OF THE VALUE OF BRONCHOSCOPY TO SCREEN FOR LUNG CANCER IN SMOKERS AND EX-SMOKERS AGED OVER 50 YEARS WITH PNEUMONIA
K. Houston, H. Singh, S. C. O. Taggart, P. M. Turkington, B. R. O’Driscoll. Department of Respiratory Medicine, Hope Hospital, Salford, Manchester M6 8WH, UK
Background: Previous reports have suggested that bronchoscopy in smokers over the age of 50 years presenting with pneumonia may have a high diagnositic yield for lung cancer.
.) found that 5/36 patients presenting with pneumonia without obvious underlying carcinoma on the chest x ray (CXR) had lung cancer at bronchoscopy. Furthermore, Wilson et al (BTS abstract, Thorax 2003 S3 p57) reported in a retrospective study that 20 out of 107 bronchoscopies over a 10 year period yielded a diagnosis of lung cancer when the only indication for bronchoscopy was pneumonia in a patient over the age of 50 years with a smoking history. However controversy remains as to whether this is an effective policy, especially as pneumonia is a common diagnosis. Previous audit of 603 admissions to this hospital with pneumonia as the main diagnosis showed that 70% of these patients were smokers or ex-smokers aged over 50 years.
Methods: Following the above publications, a policy was introduced at Salford Royal NHS Trust in January 2004 whereby smokers and ex-smoker over the age of 50 years admitted with pneumonia were offered flexible bronchoscopy. The clinical presentation and x rays were reviewed and the diagnostic yield of lung cancer detected at bronchoscopy was measured in this group of patients who did not have any other indication for bronchoscopy (for example, haemoptysis or other suspicious features on CXR).
Results: Between January 2004 and June 2005 there were approximately 900 patients admitted to this hospital with pneumonia. Out of these only 37 were referred for bronchoscopy who fulfilled the criteria of being over 50 and current or ex-smokers without another indication. Of these 37 only one was found to have cancer. However on review of this case by the Respiratory team, it was noted that a radiologist had already reported a left hilar mass prior to bronchoscopy.
Conclusion: Like other teams, our clinical experience is that we have seen many cases of lung cancer presenting with pneumonia, but most of these patients have had other suspicious features such as weight loss, prominent hilar shadows, volume loss, or haemoptysis. Our prospective 18 month study yielded no unexpected diagnosis of lung cancer in 37 smokers or ex-smokers aged over 50 who had bronchoscopy where pneumonia was the sole indication for this test. If this policy were applied strictly to all smokers and ex-smokers aged over 50 with pneumonia, we estimate that we would need to undertake approximately 400 additional bronchoscopy procedures per annum. In view of our negative findings, we have now discontinued this policy.
S13 THE VALUE OF TARGETED BRONCHIAL CYTOLOGY IN LUNG CANCER PATIENTS WITH A NORMAL BRONCHOSCOPY
S. Bari, D. A. Stock, C. M. Smyth, V. Kelly, M. J. Walshaw, M. J. Ledson. Liverpool Lung Cancer Unit, The Royal Liverpool Hospital and The Cardiothoracic Centre Liverpool, UK
Background: Some authors advocate that bronchoscopy is not indicated where there is no obvious central lesion, in the belief that the endobronchial appearance will be normal and tissue samples will need to be obtained by another route. However, such a philosophy ignores the possibility of a positive diagnosis through the use of bronchial washings and brushings, targeted to an area of interest. We have routinely used this approach in our lung cancer service, and were interested in assessing the diagnostic yield.
Method: We looked at all bronchoscopies carried out in our large lung cancer unit between April 2000 and February 2005 where a diagnosis of lung cancer was made when bronchoscopy showed no endobronchial lesion. We compared the results of bronchial washings and brushings taken from an area of interest (defined by chest x ray or CT scan) with the ultimate diagnosis and any histological findings when available.
Results: 607 samples were taken from 571 cases (mean age 70 years (range 45–96), 294 male) who fulfilled the criteria (out of 3124 bronchoscoped patients in total). Of these, 108 (19%) showed malignant cells (35 adenocarcinoma, 61 squamous cell carcinoma, 7 small cell, 2 metastatic, and 3 “cancer”). In 12 of these, histological samples were obtained (10 at thoracotomy) and all confirmed the cell type. A further 31 (5%) cases showed atypia (five of which had cancer diagnosed by a further procedure). The remaining 456 cases had no evidence for malignancy on cytological examination (reported as “normal” 52 cases, “no evidence of malignancy” 378 cases, and “inflammation” two cases). 140 of these had a clinical diagnosis of cancer and in 316 a diagnosis was obtained histologically by another route.
Conclusion: This study shows that in patients with peripheral lung lesions suspicious of cancer, targeted bronchial washings/brushings can achieve a positive cytological diagnosis of lung cancer in up to one fifth of cases. This technique allows a positive diagnosis of lung cancer in patients who are not fit enough for invasive procedures (in our study up to 96/571, 17%), aiding the selection of best oncological treatment. We remind clinicians charged with the care of lung cancer patients that this technique is a valuable tool in the diagnostic process.
S14 IMPACT OF A COORDINATED QUALITY IMPROVEMENT PROGRAMME UPON YIELD OF BRONCHOSCOPY IN SUSPECTED LUNG CANCER
M. Slade, G. Pengelly, H. MacMullen. Oxford Centre for Respiratory Medicine, Churchill Hospital, Oxford OX3 7LJ, UK
Introduction: Fibreoptic bronchoscopy (FOB) plays a central diagnostic role for patients with suspected lung cancer (LC). Careful patient selection, and a high diagnostic sensitivity for FOB will improve patient care by reducing the numbers of non-diagnostic procedures, which lead to unnecessary patient discomfort and repeated biopsies. During 2001, in a stepwise fashion, we introduced a series of measures aimed at improving patient selection and diagnostic yield of FOB: FOBs carried out to investigate LC were concentrated on the list of one chest physician specialising in LC, and performed or directly supervised by him (MS); one chest physician was made directly responsible for the bronchoscopy service; greater efforts were made to have a CT scan available before FOB; new bronchial brushes with a higher reported yield were used; there was careful and frequent liaison with the pathology department; and a continuous prospective audit of diagnostic yield begun. In 2002, transbronchial needle aspiration was introduced. Here we audit the results of this programme.
Methods: Audit of database entries since 2002, and retrospective note review for 2000 (before introduction of the quality programme). The principal outcome measures were the proportion of patients having FOB for suspected lung cancer in whom the procedure was diagnostic, and the sensitivity of FOB for detecting lung cancer, in each year of study. Secondary outcomes were the proportion of patients in whom a CT scan of the chest was available at bronchoscopy, and total numbers of FOB.
Results: (1) Patient selection: In 2000, 77/136 (56.6%) of FOBs for suspected LC were diagnostic. In 2002–05 the corresponding proportions were: 2002 79/91 (86.8%), 2003 110/132 (83.3%), 2004 48/68 (70.6%), 2005 (to July) 36/40 (90%) (p<10−7, χ2). (2) Sensitivity of FOB for LC: The overall sensitivity of FOB for detecting LC year by year was: 2000 77/110 (70.0%), 2002 79/89 (88.8%), 2003 110/125 (88.0%), 2004 48/55 (87.3%), and 2005 (to July) 36/38 (94.7%) (p<0.001, χ2). Since 2002, the sensitivity of FOB for LC where tumour is visible at FOB has never been less than 90% (BTS Guidelines on Diagnostic Flexible Bronchoscopy, minimum target 80%). (3) CT scanning: The proportion of patients having a CT before FOB rose from 21.6% before the programme to 55.3% in 2005 (p<0.0005, χ2). (4) FOB numbers: The total numbers of FOBs for LC have fallen.
Conclusion: The introduction of a coordinated programme of quality improvement in FOB has led to significant improvements in patient selection, sensitivity, and access to CT scanning before the procedure. Over the past five years the number of FOBs carried out for the investigation of LC has fallen. In part this is explained by better patient selection, with a greater proportion of patients investigated having LC, but alternative diagnostic approaches, and in particular the use of routine neck ultrasound, have also contributed to the fall in numbers of FOBs.
S15 ENDOBRONCHIAL PALLIATION OF MALIGNANT AIRWAY OBSTRUCTION: THE EARLIER THE BETTER?
M. Slade, G. Pengelly. Oxford Centre for Respiratory Medicine, Churchill Hospital, Oxford OX3 7LJ, UK
Introduction: Endobronchial treatments such as diathermy and stenting are believed to be effective at relieving breathlessness due to large airway obstruction, although the evidence rests upon large case series alone. These interventions may be employed either before or after other therapies such as radiotherapy or chemotherapy. It has been our practice increasingly to employ endobronchial treatment early in the patient pathway. This is because we believe that (1) this strategy may effect more rapid relief of symptoms in a disease for which most treatments are palliative, and (2) rapid palliation is better than slow palliation. In this audit we review the results of endobronchial intervention according to whether it was offered as the first treatment modality, or after other treatments had been completed.
Method: Retrospective review of prospectively collected data, July 2002 to July 2005.
Results: Airway stenting and endobronchial diathermy were the two treatment modalities employed. There were 18 procedures in 17 patients (M = 15, mean age 65 years) before any other therapy (“early treatment group”), and 25 procedures in 17 patients (M = 12, mean age 65 years) after prior treatment with radiotherapy, surgery or chemotherapy (“late treatment group”). Early treatment group: endobronchial treatment preceded surgical resection in two patients, and CHART radiotherapy in one. Two patients had no other active treatment, and 12 had palliative radiotherapy. One patient had WHO performance status (PS) = 3 prior to endobronchial treatment, which improved to PS = 1 after treatment, making definitive treatment by bi-lobectomy possible. The diagnosis was NSCLC in 13 patients, metastatic melanoma in two, and bronchial carcinoid in two. The mean FEV1 improved from 1.40 to 1.85 l (31.9% improvement, p = 0.01). PS improved by one point in nine patients, remained the same in six, and decreased by one in one patient (p = 0.008, Wilcoxon). One patient died of pneumonia four days after endobronchial diathermy. He had had obstructive pneumonitis, PS = 3 before the procedure, and had tumour completely occluding the right main bronchus. Eleven of the patients remain alive with a mean duration of follow up of 131 days. Late treatment group: the diagnosis was NSCLC in 12 patients, metastatic renal cell carcinoma in three, metastatic ependymoma in one, and oesophageal carcinoma in one. The mean FEV1 increased from 1.40 to 1.71 l (22.2% improvement, p = 0.00017) and there was an improvement in PS (p = 0.004, Wilcoxon). There were no procedure related deaths. Three patients remain alive, and the mean duration of follow up is 183 days.
Conclusions: In this retrospective comparison, early intervention with endobronchial treatment for large airway obstruction produced similar benefits in lung function and PS when compared with later intervention. Early endobronchial intervention may make possible subsequent radical treatment in patients for whom it was previously considered unsuitable on the grounds of poor PS.
S16 ENDOBRONCHIAL TREATMENT OF CARCINOID TUMOURS: A COMPLEMENTARY APPROACH TO SURGERY
M. Slade, G. Pengelly. Oxford Centre for Respiratory Medicine, Churchill Hospital, Oxford OX3 7LJ, UK
Introduction: The conventional management of typical bronchial carcinoid tumours is by surgical resection where lung function and performance status permit. We describe five patients in whom endobronchial tumour debulking (using diathermy, with or without cryotherapy) was employed as the first therapeutic intervention.
Method: Retrospective chart review.
Results: Five patients (two male, mean age 53, range 31–77) with typical bronchial carcinoid had endobronchial treatment as a first therapeutic intervention. This was used prior to surgery in two patients, and as the only treatment in three. Surgery was not offered to three patients because of poor lung function in one, patient choice in another, and multiple medical comorbidities in the third. Endobronchial diathermy was used in all patients, supplemented with cryotherapy in three. The principal objectives of endobronchial treatment in all patients were relief of obstructive pneumonitis, and improvements in lung function and performance status. The tumours produced partial (three patients) or total (one patient) occlusion of a main bronchus in four patients (80%), and total occlusion of a lobar bronchus in one patient. Mean (SD) FEV1 improved from 1.81 l (0.77 l) to 2.42 l (1.11 l) following treatment. There was radiographic and symptomatic improvement in obstructive pneumonitis in all patients. There was an improvement of 1 point in WHO performance status in three patients (60%). Two patients subsequently underwent definitive surgical resection, by right upper lobectomy in one and bilobectomy in the other. In both these cases performance status had improved from 2 to 1 prior to surgery following endobronchial treatment. Repeat endobronchial treatments were required in two of the three patients who were treated by this method alone. All patients remain alive after a median follow up of 18 months (544 days).
Conclusion: These preliminary results suggest that endobronchial treatment is an effective alternative to definitive surgery for typical bronchial carcinoid tumours in patients who are either unfit for or decline to undergo lung resection. Longer follow up is required to assess the safety of this approach. In addition, endobronchial treatment may be beneficially employed prior to definitive surgery, with a view to relieving bronchial obstruction and consequently improving both performance status and lung function.
Oxygen prescribing in lung disease
S17 THE NEW HOME OXYGEN SERVICE: ASSESSING THE IMPACT ON RESPIRATORY UNITS.
J. K. Quint, L. Ward, M. Monaghan, S. O. Ansari, K. Ganes Lingam, C. D. Eraut, A. G. Davison. Southend Associate University Hospital, UK
Introduction: The provision of the home oxygen therapy service in England and Wales will change significantly in 2006 and will include ambulatory oxygen for the first time. The implication for Respiratory units is unknown. A study was undertaken at Southend Hospital for the Eastern Region Oxygen Reference Group to attempt to predict the number of long term oxygen (LTOT) and ambulatory oxygen assessments that will be required each year. This was done using the British Thoracic Society clinical component guidelines on the assessment for provision of home oxygen services. Grade 1 patients are on LTOT and are housebound, Grade 2 on LTOT (active group) mobilise out of the house and should have assessments for ambulatory oxygen.
Results: 191 patients are on LTOT in the district currently (population 325 000). 89 patients completed assessment for LTOT from March 2004 to February 2005. 58 of these patients fulfilled the criteria for LTOT. 17 consecutive patients of those who fulfilled the criteria for LTOT were further studied. Lung function, smoking history, blood gases, oxygen requirement grade for ambulatory oxygen, and MRC breathlessness score were recorded. Nine patients met Grade 1 oxygen requirements, 8 Grade 2. Of those in Grade 1 the mean age was 72 (SD 8) and mean pack years 53.5 (SD 20). On assessment the mean pH was 7.42 (SD 0.03), pCO2 5.68 (SD 0.87), pO2 6.97 (SD 0.51), and HCO3− 27.3 (SD 3.7). None of the patients in this group was polycythaemic, only one had ankle oedema. The mean FEV1 was 0.75 (SD 0.44). Two patients had an MRC breathlessness score of ⩽4, 7 of 5. In the Grade 2 group the mean age was 65 (SD 7), mean pack years 40 (SD 26). The mean pH was 7.40 (SD 0.04), pCO2 5.61 (SD 1.34), pO2 6.7 (SD 0.77), and HCO3− 26.3 (SD 0.4). None of the patients in this group had ankle oedema or polycythaemia. The mean FEV1 was 1.12 (SD 0.48) and mean MRC score 4 (SD 1). Six patients had an MRC breathlessness score of at least 4, 2 of 5.
Conclusion: Approximately 50% of those eligible for LTOT will also require assessment for ambulatory oxygen. This could be greater for those already on LTOT (191 in our district) if the mortality of patients in Grade 1 is greater than in Grade 2. We estimate that each year in our district there will be 89 LTOT assessments, and 27 of these would require further assessment for ambulatory oxygen. It would appear from our results that using the MRC breathlessness score or clinical parameters to grade patients into 1 or 2 is of limited use. This study does not include the assessment for ambulatory oxygen in patients who desaturate on exercise in whom ambulatory oxygen is also recommended (Grade 3).
S18 EFFECT OF SHORT BURST OXYGEN THERAPY IN THE HOME ON RECOVERY FROM EXERCISE IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE: A DOUBLE BLIND CROSSOVER STUDY
S. J. Quantrill, R. White, A. Crawford, J. Barry, S. Batra, P. Whyte, C. M. Roberts. Whipps Cross University Hospital, UK
Background: £16 million per year is spent on oxygen cylinders in the UK. Although short burst oxygen therapy (SBOT) is widely used in chronic obstructive pulmonary disease (COPD), its benefit is unproven. Previous studies of SBOT have all been lab/hospital based, sometimes exercising subjects in a way that is not familiar to them—for example, bicycle ergometry. This study aimed for the first time to test patients in their own homes undertaking the daily activities of living for which they would normally use SBOT.
Methods: Thirty nine patients with COPD, identified from GP prescribing databases, were screened using a telephone questionnaire to ascertain suitability for the study. 22 patients (mean age 72 years, range 56–86 years, mean FEV1 0.87, 38% predicted) were deemed suitable and agreed to the study. Those with coexisting medical disorders which significantly contributed to reduced exercise tolerance, such as heart failure, angina, or arthritis, were excluded. Patients with an exacerbation in the past six weeks and those who could not confirm any definite benefit from their oxygen were also excluded. All patients stated that their oxygen cylinder helped them in some way. 11 (50%) also had long term oxygen therapy concentrators which were not used during the study. Patients were asked to identify two activities which they would normally use SBOT for and were told to use it in their usual way: all used SBOT post-exercise and via nasal prongs. None used oxygen before the activity. Each activity was then performed twice with either oxygen or air in a randomised fashion from identical disguised cylinders and 15 minutes rest period between activities. Pulse oximetry was measured throughout. End points were subjective and objective times to recovery after each activity. Objective recovery was defined as the point at which pulse rate had returned to within five beats of the initial level and oxygen saturation within 2%.
Results: Mean baseline oxygen saturation was 93.1% on air (SD 3.8). All patients desaturated on exercise and the mean level of desaturation was −6.9%. Mean overall subjective and objective times to recovery were 206 seconds and 112 seconds respectively. Mean subjective and objective times to recovery were 34 seconds (p = 0.03) and 38 seconds (p = 0.07) shorter respectively using oxygen compared to air. Of 17 patients questioned only five were correctly able to identify the oxygen on both occasions.
Conclusions: Objective recovery time was not significantly shorter when breathing oxygen compared to air. Although there was a statistically significant shorter time to subjective recovery with oxygen, the clinical significance of this must be debatable.
S19 A RANDOMISED CONTROLLED TRIAL TO ASSESS THE EFFECT OF HELIOX IN PATIENTS WITH EXACERBATIONS OF ASTHMA AND CHRONIC OBSTRUCTIVE PULMONARY DISEASE
S. K. Leaver, A. M. Higton, J. MacIntyre, R. K. Knight, T. B. Ho. Frimley Park Hospital, Frimley, Camberley, Surrey GU16 7UJ, UK
Heliox is a mixture of helium and oxygen. A number of studies have shown that it reduces work of breathing and there is evidence that it is useful in the treatment of asthma and chronic obstructive pulmonary disease (COPD). We hypothesised that heliox would improve outcomes in patients presenting with acute exacerbations of either asthma or COPD.
We carried out a randomised control trial of patients sequentially admitted to Frimley Park Hospital with exacerbations of asthma or COPD. An exacerbation of asthma was defined as two out of four of respiratory rate over 30, heart rate over 100, peak expiratory flow rate less than 200, and pCO2 over 4.5 kPa. Exacerbation of COPD was defined as two out of three of respiratory rate over 30, heart rate over 100, and pH less than 7.3. Patients were randomised to receive either standard treatment or standard treatment with heliox for six hours. Standard treatment included oxygen, salbutamol and ipatropium bromide nebulisers, steroids, antibiotics, aminophylline, magnesium, or terbutaline used at the discretion of the admitting physician.
We measured the following patient demographics: age, sex, smoking history, past medical history, home oxygen, home nebulisers, and severity of disease (using the SOFA score). The outcome measures were: change in observations, arterial blood gases, length of inpatient stay, need for non-invasive ventilation or intubation, and 28 day mortality. Ten patients were randomised to receive heliox and 10 patients to receive oxygen and air only.
No significant difference was found with regards to patient demographics. There was a non statistically significant difference (p = 0.16) between each group in the length of stay (heliox mean of 12.1 days, air/oxygen mean of 4.2 days). There was no significant difference between the groups in need for non-invasive ventilation (heliox 1/11 patients, air/oxygen 0/10 patients), ventilation (no patients in either group), or 28 day mortality (heliox 2/11 patients, air/oxygen 1/11 patients).
For COPD and asthma patients treated with heliox compared to the control group there was a trend towards an improvement of paO2:FiO2 ratio at one hour (p = 0.10, two tailed t test).
Heliox is a safe and easily administered treatment with no adverse effects. We have not however demonstrated a significant advantage or disadvantage in its use in the exacerbations of asthma or COPD at this stage. Further trials are needed to further elucidate the role of heliox in these patient groups.
Acknowledgements: funded by an unrestricted educational grant from BOC.
S20 SUCCESS IN WARD OXYGEN PRESCRIPTION USING NOVEL APPROACH
S. Perrott, E. Reid, K. Goode, J. Tytherleigh, R. Mahadeva. Department of Respiratory Medicine, Addenbrookes NHS Trust, Hills Road, Cambridge CB2 2QQ, UK
Oxygen, used to treat hypoxaemia, may be lethal and should therefore be considered a drug and be prescribed. It is however widely recognised that oxygen prescription and administration is poor. To ensure safe and effective delivery of oxygen the prescription should include the flow, the concentration, the delivery device and the duration of use.
A multifaceted approach was applied to oxygen prescription and monthly audit of prescribing practice undertaken on the respiratory ward at Addenbrookes Hospital.
The outcome measures of the audit were whether oxygen was prescribed on the prescription chart, whether prescription matched patient use in relation to delivery device, flow and concentration, and whether administration was appropriately signed for on the prescription chart during nursing drug rounds. A multidisciplinary team including senior and junior doctors, specialist and ward nurses and physiotherapists met on a monthly basis to identify and address key issues which had resulted in a failure to achieve correct oxygen prescription and administration. A targeted plan was initiated and implemented as a result of the meetings.

During a seven month period there was a gradual improvement in oxygen prescription and administration, with 80% of all oxygen administration on the Respiratory ward meeting the goals of the audit, with 100% success for appropriate prescription and recording of administration for all of those patients who had oxygen prescribed.
These data are in contrast to other recent studies and indicate that a multidisciplinary problem solving approach can result in a high standard of oxygen prescription for at risk patients resulting in better care.
S21 LOW OXYGEN SATURATIONS, HIGH FLYING PATIENTS, BUT ARE THEY FIT TO FLY?
M. Rutter, D. Murray, P. K. Sreedharan, R. Mahadeva. Department of Respiratory Medicine, Lung Function Unit, Addenbrookes NHS Trust, Cambridge, UK
Air travel is rapidly increasing, with passenger numbers more than doubling through UK airports between 1987 and 2002. Current guidelines outline commercial flight cabin pressure should not exceed 8000 ft. Patients diagnosed with chronic lung disease (CLD) are susceptible to O2 desaturation at this pressure (565 mm Hg). The equivalent conditions can be simulated at sea level by reducing FiO2 to 15%.
We report on 24 patients with CLD who have undergone fitness to fly (FTF) assessments according to BTS guidelines. The patient breathed 15% O2 for 20 minutes through a demand valve with a dead space of 110 ml. Baseline levels of PaO2, PCO2, SpO2, and heart rate were measured. SpO2 and heart rate were recorded at two minute intervals during test. PaO2, PCO2, SpO2, and heart rate were measured at 20 minutes breathing FiO2 of 15%. Individuals with a PaO2 <6.6 kPa were recommended to have O2 during their flight. A questionnaire was completed by patients to ascertain what symptoms patients experienced when flying, and the cost and availability of O2. Differences between lung function parameters of those individuals who passed and those who failed the FTF test were assessed using appropriate statistical analysis using Sigmastat. 24 patients took the fitness to fly assessment, 15 of the patients had a diagnosis of COPD, nine patients were diagnosed with pulmonary fibrosis, CVID and asthma. 11 patients failed the test and were recommended to have O2 when flying. The cost of O2 varied from £0–£150. Most patients felt being charged for O2 was discrimination against the disabled. A few airlines allow patients to take their own cylinders at no extra cost. Patients found that if the flights quota of O2 had been used they would not be supplied O2. Furthermore if they were unable to have it on one flight they would also not be allowed to have it on the return flight even if the quota had not been fully reserved. In total our patients took 19 flights of which eight flights were recommended O2. Of these eight, six received O2. The patients who were not recommended to have O2 did not report any symptoms during the flight. Two of the patients that were recommended O2 experienced dizziness and shortness of breath when walking during the flight, despite receiving O2. Individuals who failed the FTF assessment had a trend towards a lower median (IQR) FEV1% 33.000 (29.5–68.25) versus 53.000 (31.5–85.0) for those who failed. There was no significant difference in mean KCO(c), TLCO(c), TLC, or RV between those who passed or failed the FTF assessment. Starting saturations and PaO2 were lower in those who failed; median (IQR) 94.0% (91–95) versus 95.5% (95–97) for those who passed; p = 0.003. Median (IQR) starting PaO2 was 9.2 kPa (8.5–9.9) for those who failed versus 10.4 (9.9–12.2) for those who passed; p = 0.003. There was no difference in the degree of desaturation induced by the test in those who passed and those who failed. In conclusion, although those who failed FTF assessments had lower baseline SP02 there was no reliable cut off and there was no robust physiological predictor of those who were to fail the FTF assessment.
S22 UPDATE ON BTS/BLF UK FLIGHT OUTCOMES STUDY
R. K. Coker, R. Shiner, M. R. Partridge. Respiratory Medicine, Hammersmith Hospitals NHS Trust, London W12 0HS, UK and Imperial College London NHLI Division, UK
Eighteen months into a national, prospective observational study of the outcomes of air travel for passengers with lung disease, 58 centres have agreed to recruit patients and 38 centres (65%) have to date submitted patients. Five hundred and twenty one physician questionnaires have been received, and 302 patient questionnaires have been returned following air travel.
Patients with a wide variety of respiratory conditions undertook air travel, the two largest single categories being airway disease (asthma and COPD), accounting for 48%, and diffuse parenchymal lung disease, accounting for 24%. Eleven patients have died, seven before flying, four after flying (two while on holiday), and none during flight.
A further 34 patients (7%) who had planned to take a flight did not do so. In 13 cases this was because of subsequent medical advice not to fly, in two cases because the airline was unwilling to carry them, in one case because the patient did not wish to use the recommended supplementary oxygen, and in 18 cases for circumstantial or personal reasons.
Flight assessments undertaken on the 521 patients included hypoxic challenge in 44%, a walk test in 8% and oximetry and spirometry in 94% and 97% respectively. With regard to those patients who undertook flight (261), comparison of the need for unscheduled medical care in the four weeks after returning home with the four weeks before travelling showed the numbers of patients consulting a doctor to be 31 before flying and and 70 after flying.
Acknowledgements: The authors wish to thank all those who have submitted patients to this study. They also thank Research Assistants Louise McNamara and Sajini Wijetilleka for their help in data collection and processing. The UK Flight Outcomes Study is jointly funded by the British Thoracic Society and the British Lung Foundation.
Radiological assessment of pulmonary modules: from CXR to SPECT
S23 ONE YEAR’S EXPERIENCE OF A CHEST RADIOGRAPH “SAFETY NET” PROTOCOL
H. Singh1, S. C. O. Taggart1, P. M. Turkington1, R. Chisholm2, K. Peplow1, B. R. O’Driscoll1. Departments of 1Respiratory Medicine and 2Radiology, Hope Hospital, Manchester M6 8HD, UK
Background: A significant number of abnormal chest radiographs (CXR) are not acted upon in a timely manner, potentially affecting outcomes and generating malpractice claims (
and
). Following a number of adverse events of this nature, a team of chest physicians, risk managers, radiologists, and lung cancer nurses at this hospital established a monitoring and intervention protocol for every abnormal CXR reported as suspicious of lung cancer. We now report the results of 12 months of monitoring.
Methods: All abnormal CXR reports, suspicious of lung cancer, in patients with no previous diagnosis of lung cancer were faxed to the lung cancer team office where the electronic record of each patient was checked for evidence of appropriate action within two weeks (for example, referral to a chest physician). If no action was evident, the lung cancer nurse (LCN) responded by contacting the relevant general practitioner (GP) or hospital consultant to ensure that appropriate action was taken.
Results: See table.
Abstract S23
Conclusions: Had the new system not been in place, 73 of 269 (27%) patients with suspicious CXR reports in a 12 month period would have had delayed action or no action by the clinician requesting the CXR. Of these 73 patients, 21 (29%) had a final diagnosis of lung cancer. The new system avoided two adverse events or legal claims due to delayed diagnosis per month at a cost of about £2,500 per annum.
S24 THE FREQUENCY OF CHEST X RAY ABNORMALITIES IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE SCREENING
G. M. F. Wallace1, J. E. Winter2, A. Taylor3, T. W. Taylor4, R. C. Cameron4, J. H. Winter1. 1Respiratory Unit, Ninewells Hospital, Dundee; 2Westgate Health Centre, Dundee; 3Clinical Technology Centre, Ninewells Hospital, Dundee; 4Radiology Department, Ninewells Hospital, Dundee, UK
Introduction: In Dundee patients aged 40 and over with either a known smoking history, or unknown history but receiving inhaled bronchodilators, are invited to their general practitioners for chronic obstructive pulmonary disease (COPD) assessment. If they have not had a chest x ray (CXR) in the past three years, they are offered one which is reported in a structured fashion. This adheres to a grade D NICE guideline which recommends CXR to exclude other pathologies. An audit of all COPD screening CXR reports, comprising seven questions, for a two year period of June ’03 to May ’05 was undertaken. 555 CXRs were performed.
Results: Question 1: Is the CXR technically satisfactory? 495 yes, 60 no; Question 2: Are the lungs a normal size? 299 normal, 244 large, 12 small probably due to technical reasons; Question 3: Is the heart a normal size? 503 normal, 50 large, 2 can’t say due to technical reasons; Question 4: Is there significant focal emphysema? 83 yes (72 upper zone, 10 lower zone, 3 unspecified); Question 5: Are there any features to suggest lung cancer? 14 yes, 541 no; Question 6: Any features of other disease likely to be causing dyspnoea? Yes 106, no 449; Question 7: Any features of other disease not causing dyspnoea? Yes 131. Of the 14 patients who had features to suggest lung cancer, nine had bronchogenic carcinoma (see table).
Abstract S24
Other dyspnoea causing diseases which were potentially treatable included cardiac failure 4, lower respiratory tract infection 40 (17 requiring follow up CXR), bronchiectasis 8, fibrosis 7, pleural effusion 4, ?new TB 3 (12% of all CXRs).
Conclusions: 61.7 screening CXRs need to be performed to detect one bronchogenic carcinoma. Four of the nine lung cancer patients had potentially curative treatment (44%). 33% had surgery comparing favourably with the local surgical referral rate of 8%. Given this and the other dyspnoea causing diseases detected, screening COPD CXRs have led to significant changes in management.
S25 FIVE YEAR EXPERIENCE OF AN X RAY CODING SYSTEM IN LUNG CANCER DIAGNOSIS
D. A. Stock, J. Hughes, C. McCann, M. J. Ledson, M. J. Walshaw. Liverpool Lung CancerUnit, The Royal Liverpool University Hospital and The Cardiothoracic Centre, Liverpool, UK
Background: There is a high incidence of lung cancer in Liverpool, and in order to cope with this in 2000 we undertook a major reorganisation of lung cancer services at our hospitals within the city. As part of this, we instituted a coded x ray system for all chest x rays (requested from both the primary and secondary care sectors) taken at our local DGH. This system was designed to be a failsafe mechanism to ensure that cancers were not missed and also to facilitate prompt investigation. We were keen to show that x rays were being coded appropriately, particularly in view of the fact that such coding systems have met with resistance in some radiology departments.
Methods: Using our large lung cancer database, we identified all cases in 2001 and 2004 where a coded chest x ray had prompted the referral. We determined the grade of the radiologist and correlated their report with the subsequent diagnosis (cancer/not cancer) in each case. During these years, 400 (2001) and 377 (2004) patients were diagnosed with lung cancer by our unit.
Results: There were 413 coded x rays in total: 166 in 2001 and 247 in 2004. Similar proportions of reports were issued by consultants and SpRs in each of the two years (2001: consultants 138 (83%), SpRs 28 (17%); 2004: 196 (79%) and 51 (21%) respectively, p = NS). In 2001, 106 coded x rays (64%) led to a subsequent diagnosis of lung cancer; the proportion was similar in 2004 (153 (62%)). Both consultants and SpRs attained similar diagnostic rates over these two years (2001: 63.8% and 64.3%; 2004: 64.3% and 52.9% respectively, p = NS). A total of 40 radiologists coded x rays during the years studied. 25 radiologists coded five x rays or fewer (56 x rays in total), of whom 21 were SpRs. This group had a collective accuracy of 66.1% versus 62.2% for the remaining 15 more frequent coders (range 44.4%–83.3%). The three radiologists who coded more than 50 x rays each (185, 44.8% of the total) had accuracy figures of 72.6%, 62.2%, and 52.5%.
Conclusions: This study shows that the changes introduced in 2000 are still being employed in 2004, where the diagnosis was prompted by this route in 40% of cases. Relative proportions being coded by consultant and SpR grades have not changed significantly, with an overall accuracy of approximately two thirds. Although there was a wide variation in accuracy between individual reporters, this was not related to the number of cases coded. These data allow us to provide performance feedback to our radiology colleagues and also act as a benchmark for future audit. It is of note that the NICE guidelines for the diagnosis and treatment of lung cancer were recently updated and now advocate the use of such coded chest x ray systems. We have found this system useful in aiding a timely diagnosis in patients with suspected lung cancer and recommend it to other lung cancer units.
S26 OUTCOME OF SMALL PULMONARY NODULES AT CHEST CT FROM A RAPID ACCESS LUNG CANCER CLINIC
K. Mohan, D. A. Stock, S. Bari, H. Fewins, M. J. Ledson, M. J. Walshaw. Liverpool Lung Cancer Unit, The Cardiothoracic Centre, Liverpool, UK
Introduction: Although most small pulmonary nodules (up to 1 cm) are benign, they may represent early lung cancer. Recognition and treatment of early stage lung cancer (stage I) is crucial to achieve a five year survival rate of 80%. Although the results of large population screening studies have suggested that <10% of these nodules are malignant, there have been few studies examining the outcome of such nodules in patients presenting with suspected lung cancer.
Methods: To investigate this further, we analysed the chest CT scan reports of 1163 patients presenting to our large lung cancer unit over a three year period. We identified 74 scans with small pulmonary nodules (⩽1 cm). 34 patients were excluded (21 ongoing follow up, 6 granuloma, 4 lost to follow up, and 3 died). The remaining 40 patients (mean age 66 years (48–84), 21 male) were eligible for the study. Twenty patients (50%) had underlying lung disease (16 emphysema, 2 bronchiectasis, and 2 asbestos related pleural plaques). The mean size of the nodules was 8 mm (2–10 mm) and the most common location of the nodules (23 patients, 56%) was the upper lobes. Data regarding the characterisation of the nodules were available in 24 patients (60%) (10 ill defined, 4 well defined, 4 spiculated, and 6 ground glass appearance).
Results: Patients underwent interval CT scans in accordance to our radiology protocol. Nodules were considered benign if they resolved, decreased in size or demonstrate no growth at two year follow up CT scans. Two patients underwent nodule resection (one malignant) and hence had no follow up CT for further evaluation. During the follow up eight patients demonstrated nodule growth, which occurred at a mean interval of 11 months (6–24) after the initial CT. Five patients had pathological confirmation of lung cancer and two were diagnosed on clinical grounds. One patient had a benign lesion at thoracotomy. Overall, 32 patients (80%) had benign nodules (based on resolution or stability at two years) and eight (20%) had malignant nodules (based on nodule growth and/or histological confirmation). Of these eight patients, one declined treatment, four underwent thoracotomy (for T1N1M0 NSCLC), and three patients were referred to oncology due to combination of poor lung function, performance status, and comorbidity.
Conclusions: Our results indicate a high incidence of lung cancer in patients with small pulmonary nodules referred to a lung cancer clinic. This indicates that in this selected population; surveillance screening for growth by interval CT scans is worthwhile. Further large prospective studies are required to determine the optimum methodology for the evaluation of such nodules.
S27 INITIAL EXPERIENCE WITH FDG-PET SCANS IN THE EVALUATION OF PATIENTS WITH LUNG CANCER
K. Mohan, A. McIver, H. Fewins, M. J. Ledson, M. J. Walshaw. Liverpool Lung Cancer Unit, The Royal Liverpool Hospital and The Cardiothoracic Centre, Liverpool, UK
Introduction: The recently published NICE guidelines recommend that every patient with lung cancer in whom curative surgery or radical oncological treatments are contemplated should undergo FDG-PET scanning, in order to assess the likelihood of mediastinal or distant deposits. The same scans should also be undertaken in the assessment of solitary pulmonary nodules. We were interested in assessing whether these guidelines improved the evaluation of patients attending our unit.
Methods: We report our initial experience over five months (February to June 2005) with FDG-PET scans, where a twice monthly mobile scanner service has been set up for the benefit of patients attending our large lung cancer unit. We compared the results of FDG-PET with CT scans and noted whether the extra information had changed management.
Results: Twenty eight consecutive scans were taken for this purpose over the audit period. In 14 the FDG-PET scan agreed with the findings of the CT scan.
With regard to the other 14 patients, in one case the CT scan suggested N2 disease whilst the FDG-PET scan did not: at subsequent thoracotomy no evidence of mediastinal disease was found. In two patients, the FDG-PET scan demonstrated evidence of N2 disease not apparent on the CT scan (upstaged): subsequent surgical investigations confirmed N2 disease. However, in a further patient where the FDG-PET was negative, the CT scan suggested N2 disease and this was confirmed at thoracotomy (false negative FDG-PET). The remaining 10 FDG-PET scans were performed in patients with solitary pulmonary nodules with no tissue diagnosis: in seven of these the FDG-PET was negative and these patients remain under surveillance (mean 75 days, range 65 to 114) with no evidence of nodule growth. In the other three cases where FDG-PET scanning was positive, all were discovered to have Stage 1 disease at thoracotomy.
The average time taken from booking to FDG-PET scan was 33 days (range 20 to 47), leading to treatment delays in 14 of the 17 patients who required active treatment (82%) beyond the recommended deadline of 62 days (mean time of 80 days (28 to 120)).
Conclusions: In these patients, we have shown that FDG-PET altered the management in 14 cases (46%), aiding the management in 13 (10 with solitary pulmonary nodules). FDG-PET is a valuable tool in the assessment of patients with lung cancer, but with the current resources can lead to a delay in treatment in the majority of patients.
S28 THE UTILITY OF NEOSPECT SCANNING IN THE DIAGNOSIS OF SOLITARY PULMONARY NODULES: A DISTRICT GENERAL HOSPITAL EXPERIENCE
O. Kankam1, M. Clee1, A. Dyson1, K. Foord2. Departments of 1Respiratory Medicine & 2Radiology, Conquest Hospital, East Sussex, UK
Solitary pulmonary nodules (SPNs) account for up to 30% of new cases of lung cancer.1 18F-deoxyglucose positron emission tomography (FDG- PET) is used in the diagnosis of malignant SPNs, but it is still not widely available. Depreotide scanning (Neospect) has been used in the assessment of SPNs.2
We evaluated the use of Neospect scanning in a district general hospital setting as an alternative to FDG-PET scanning in the diagnosis of SPNs.
Solitary pulmonary nodules (<3 cm) in 25 consecutive patients were evaluated by CT scan, Neospect scan, and histology. 11 patients had a histological diagnosis of cancer (adenocarcinoma 6, squamous cell carcinoma 5), 10 of whom had a positive Neospect scan. There were 10 false positives (inflammatory 9, sarcoid 1), one false negative (adenocarcinoma). The sensitivity, specificity, and negative predictive value of Neospect scanning in this cohort were 90.9%, 36.3%, and 80% respectively (see table).
Abstract S28
The value of a negative test is considerable if interpreted in the light of other clinical findings and should exclude malignancy in most cases. A positive test should prompt further diagnostic measures.
Until FDG-PET scanning becomes widely available, Neospect scanning is a cost effective alternative in the diagnosis of malignant SPNs; it is easy to set up in a district general hospital with nuclear medicine facilities.
1
2
Assessing airway inflammation in asthma
S29 A STUDY OF AIRWAY INFLAMMATION IN ACUTE SEVERE ASTHMA
A. V. Kamath1, W. R. Monteiro2, S. Mildenhall1, C. F. Ramsay1, O. P. Twentyman1, A. M. Wilson1, I. D. Pavord2, B. D. W. Harrison1. 1Norfolk and Norwich University Hospital, Norwich, UK; 2Institute of Lung Health, Glenfield Hospital, Leicester, UK
Background: Measurement of airway inflammation has been shown to predict treatment response in patients with asthma. Few studies have investigated airway inflammation in patients with acute severe asthma admitted to hospital.
Methods: The characteristics including history, spirometry, and previous physician documented poor adherence to treatment were recorded. Peripheral blood and sputum (spontaneous or induced) were analysed for differential leucocyte counts. Atopy was considered to be RAST test positive to one or more inhalant allergens. Patients were characterised according to sputum cell counts as eosinophilic (E) (⩾3% eosinophils), neutrophilic (N) (⩾65% neutrophilis), eosinophilic and neutrophilic (E&N) (⩾3% and ⩾65% respectively) and paucigranulocytic (PG) (⩽3% and ⩽65%). Blood eosinophilia was defined as >0.4′109/l. Associations between airway inflammation and blood cell counts were analysed using analysis of variance (ANOVA).
Results: Forty one patients were recruited into the study (F = 26). Mean age of patients was 47 years (range 18–77).
Abstract S29
Eight patients had blood and sputum eosinophilia, 21 had neither blood nor sputum eosinophilia, 12 patients had sputum but not blood eosinophilia, but no patients had blood eosinophilia without sputum eosinophilia.
Conclusions: (1) Only half the patients with acute severe asthma have eosinophilic (E) or eosinophilic and neutrophilic (E&N) airway inflammation. (2) Patients with peripheral blood eosinophilia almost certainly have eosinophilic airway inflammation.
S30 INDUCED SPUTUM GM-CSF CONCENTRATION IS INCREASED IN MODERATE AND SEVERE ASTHMA
S. K. Saha1, D. Parker1, P. D. Monk2, E. S. Cohen2, M. Berry1, W. Monteiro1, R. H. Green1, A. J. Wardlaw1, I. D. Pavord1, C. E. Brightling1. 1Institute for Lung Health, Leicester, UK, 2Cambridge Antibody Technology, Cambridge, UK
Background: Granulocyte-macrophage colony stimulatng factor (GM-CSF) has been implicated in the pathogenesis of asthma. GM-CSF expression in biopsies from steroid naïve asthmatics was related to severity of symptoms and GM-CSF has been measured in induced sputum from asthmatics. However, the measurement of GM-CSF in induced sputum has not been validated. We have now validated the measurement of GM-CSF in induced sputum by ELISA and we hypothesised that the GM-CSF concentration is increased with increasing asthma severity.
Method: The measurement of GM-CSF in induced sputum was validated in terms of: (1) the effect of the mucolytic DTT on the recovery of GM-CSF, (2) the recovery of exogenous spiked GM-CSF to selected sputum before processing, and (3) GM-CSF spiking to sputum supernatant. Sputum was induced in subjects with asthma (mild = inhaled beta agonist only, moderate = inhaled corticosteroid, and severe = oral prednisolone or intramuscular trimacinolone) and healthy controls and the induced sputum GM-CSF concentration measured by ELISA.
Results: The GM-CSF recovery was not affect by DTT. The coefficient of variation for the recovery of GM-CSF after spike of exogenous GM-CSF to selected sputum (n = 3) was 81% (9%). After the spike was added to the supernatant (n = 4) was 103% (15%). The induced sputum GM-CSF concentration was as shown in table 1. There was no relation between GM-CSF sputum concentration and either sputum eosinophil or neutrophil differential cell counts in the group as a whole, but there was a correlation between the sputum eosinophil count and GM-CSF concentration in subjects with moderate asthma (Spearman Rank correlation, r = 0.8, p<0.0001).
Conclusion: Induced sputum GM-CSF concentration is present in moderate and severe asthma, but not in mild asthma or normal controls. We cannot exclude the possibility that this increase in GM-CSF may be a consequence of corticosteroid therapy, but it is more likely that these findings support the view that GM-CSF may play an important role in the maintenance of airway inflammation in moderate to severe asthma.
Supported by: Cambridge Antibody Technology.
Abstract S30 Median (IQR) concentration of GM-CSF in asthma
S31 ASSESSING ASTHMA CONTROL: THE RCP 3 QUESTIONS CORRELATED WITH CLINICAL PARAMETERS AND EXHALED NTRIC OXIDE LEVELS
M. Thomas1,2, K. Gruffydd-Jones2,3, C. Stonham1, S. Ward3. 1Minchinhampton Surgery, Gloucs; 2University of Aberdeen; 3Box Surgery, Wilts, UK
Background: Asthma symptoms may be under-recorded and underappreciated by healthcare professionals, and this may contribute to avoidable asthma morbidity. UK guidelines recommend the RCP “three questions” (asthma related day symptoms, night wakening and activity limitation) should be recorded at all asthma consultations, although the use of this tool has not been validated.
Objective: To assess the discriminative and predictive value of the RCP three questions in a community asthma clinic setting
Methods: Thirty seven patients (18 male, 15 under 16 years, age range 6–71 years, inhaled corticosteroid dose median (interquartile range): 400 (200–600) mcg/day BDP or equivalent median, % predicted FEV1 mean (SD) 85 (21) %), with confirmed asthma attending two primary care asthma clinics were enrolled. Assessments were made at two weekly over 12 weeks, including RCP 3 Questions score (positive response in last week for each question = 1, negative = 0), FEV1, Asthma Control Questionnaire (ACQ), Asthma Quality of Life Questionnaire (AQLQ) for adults, and Paediatric Asthma Quality of Life Questionnaire (PALQ) for children, and exhaled nitric oxide (eNO) level. Routine clinical care was allowed to continue.
Results: 234 RCP score readings were made; summated score was 0 in 53% of readings, one in 19%, two in 19% 3 in 9%. In cross sectional analysis of all study visits, the RCP score correlated very strongly to ACQ scores (Rank correlation (r) = 0.65, p>0.001), bronchodilator use over the previous two weeks (r = 0.59, p>0.01), AQLQ score in adults (r = 0.71, p>0.001), PALQ score in children (r = −0.50, p>0.001), weakly correlated to % predicted FEV1 (r = −0.14, p = 0.03), but not to eNO (r = 0.09, p = 0.18). Comparing occasions when the RCP score was 0 (n = 124) with those when it was 1 or more (n = 110), a score of 0 was associated with a better control assessed by the ACQ (mean ACQ score 0.4 v 1.5, p>0.001), AQLQ (6.6 v 5.2, p>0.001), PALQ (6.6 v 5.7, p>0.001), and eNO level (37.7 v 49.1 ppb, p = 0.03)
The change in RCP score between visits was assessed on 196 occasions; the change was −3 on 3% of occasions, −2 on 5%, −1 on 22%, 0 on 49%, 1 on 12%, 2 on 1%, and 3 on 1%. The change in RCP score correlated strongly with the change in ACQ score (r = 0.53, p>0.001), change in AQLQ score (r = −0.52, p>0.001), change on PALQ score (r = −0.68, p>0.001),) change in bronchodilator use over the previous two weeks (r = 0.44 p>0.001), change in % predicted FEV1 (r = −0.25, p>0.001 but not to change in eNO (r = −0.06, p = 0.2).
Conclusions: This study provides evidence of cross sectional and longitudinal validity of the RCP three questions in assessing asthma control against other clinical parameters. However, inflammatory biomarkers may measure different aspects of asthma.
S32 AIRWAY INFLAMMATION IN ASTHMA IS ASSOCIATED WITH AN INCREASE IN RESPIRATORY HEAT AND MOISTURE LOSS
D. D. Noble, J. M. McCafferty, A. P. Greening, J. A. Innes. Western General Hospital, Edinburgh, UK
Background: Increased mucosal vascularity is a hallmark of airway inflammation in asthma. We hypothesised that this would lead to a detectable increase in respiratory heat and moisture loss (RHML) that would reflect the degree of airway inflammation present.
Methods: Twenty one patients with stable asthma, 19 patients with acute asthma, and 18 healthy controls had RHML measured in a cross sectional study. The RHML measurements were made using a device that combines temperature and humidity measurement during inspiration and expiration and allows precise control over inspirate conditions and ventilatory pattern. The patients with stable asthma had parallel measurements of exhaled nitric oxide (NO), sputum eosinophilia, and exhaled breath condensate (EBC) pH. Eleven of the patients with acute asthma had serial measurements of RHML as their exacerbation resolved.
Results: RHML was increased in patients with stable asthma (97.7 (SD 7.6) J/l; p<0.05) compared with control subjects (91.9 (SD 4.5) J/l), but not in acute asthma (91.1 (SD 6.0) J/l). RHML measurement in stable asthma correlated with sputum eosinophilia (r = 0.73, p<0.001; see fig), but did not correlate with exhaled NO or EBC pH. In acute asthma, there was no elevation in RHML initially, however RHML decreased significantly from day 3–5 to day 7–9 following treatment (p<0.05).

Conclusion: RHML measurement may be a useful non-invasive marker of airway inflammation in asthma. However its utility is likely to be restricted to non-acute disease.
S33 EXHALED NITRIC OXIDE MONITORING IN COMMUNITY ASTHMA CLINICS: RELATION WITH ASTHMA CONTROL PARAMETERS
K. Gruffydd-Jones1,2, S. Ward1, C. Stonham3, M. Thomas2. 1Box Surgery, Wilts; 2University of Aberdeen; 3Minchinhampton Surgery, Gloucs, UK
Background: Asthma is defined as a chronic inflammatory disease of the airways yet clinical assessments are made on the basis of symptoms and airways caliber. Recent secondary care based studies have used exhaled nitric oxide (eNO) as a biomarker to guide anti-inflammatory treatment. Most asthma is managed in the community, but as yet the utility of eNO monitoring in community settings has been little investigated.
Objective: Prospective observational study assessing correlations between eNO and parameters of asthma control in a UK primary care setting.
Methods: Thirty seven patients (18 male, 15 under 16 years, age range 6–71 years, inhaled corticosteroid dose median (interquartile range): 400 (200–600) mcg/day BDP or equivalent, % predicted FEV1 mean (SD) 85 (21) %), with confirmed asthma attending primary care asthma clinics were enrolled; assessments were made by their asthma nurse at two weekly intervals over a 12 weeks. Assessments included eNO, FEV1, Asthma Control Questionnaire (ACQ), Asthma Quality of Life Questionnaire (AQLQ), and Paediatric (caregivers) Asthma Quality of Life Questionnaire (PALQ). Routine clinical care was allowed to continue.
Results: 232 eNO readings were performed; median (IQR) eNO 28 (14–55) ppb. eNO was similar in adults (25, 18–47, n = 128) to children (32, 13–76, n = 104), p = 0.5.
A weak negative correlation was seen between eNO and % predicted FEV1 (rank correlation (r) = −0.14 p = 0.039), stronger in adults (r = −0.23, p = 0.008), and not apparent in children (r = −0.06, p = 0.6). A weak correlation was seen between eNO and worse asthma control (more positive ACQ score in adults (r = 0.22 p = 0.014) and in children (r = 0.26 p = 0.007.) Low correlation was seen between eNO and worse asthma related QOL in adults (r = −0.13, p = 0.15) or children (r = −0.17, p = 0.09). Using a cut off point of 35 ppb as a marker of significant airways inflammation, those with a lower eNO score had had better asthma control (mean ACQ score 0.8 v 1.1, p = 0.009), a tendency to better lung function (% predicted FEV1 87% v 82%, p = 0.08) and disease-related health status that was significantly better in children (mean PALQ score 6.5 v 6.1, p = 0.008) and showed a similar but non-significant trend in adults (mean AQLQ 5.9 v 5.6, p = 0.12).
Conclusions: Although a wide scatter of eNO readings are found in patients treated in primary care asthma clinics, significant relationships were observed with parameters of clinical control. Further studies investigating the utility of this biomarker for inflammation in community asthma practice are warranted.
S34 REGIONAL VENTILATORY DEFECTS IN ASTHMA: REPRODUCIBLE IN STABLE ASTHMA
P. W. Ind1, N. A. Marks1, W. E. Svensson2, A. M. Al-Nahhas2. 1Respiratory Medicine, 2Nuclear Medicine, NHLI, Hammersmith Campus, Imperial College, London, UK
Regional ventilatory abnormalities demonstrated by 81m-Krypton scanning are well described in obstructive lung disease. We have compared 81mKrypton scans in asthma of various degrees of severity with those in eight normal subjects and examined reproducibility in stable asthma.
Thirteen asthmatic patients: five with mild asthma (FEV1>80% pred, inhaled corticosteroid (ICS) <500 μg/day), one with moderate asthma (FEV1 60–80% pred), five with severe asthma (FEV1<60% pred ICS 800–2000 μg/day), and two during an acute exacerbation (severe enough to require hospitalisation) were studied. Seven patients with stable asthma; three mild and four severe were studied on two occasions one month apart. Results were compared with those in eight normal controls (five female, FEV1 107 (SD 10)%) scanned after nebulised saline. In all subjects anterior and posterior Kr-81m scans were performed seated. We modified Barter’s classification (
) for grading regional defects in 81mKrypton scans of smokers. Scans, analysed blind by two observers, were graded normal (0) or abnormal: minor changes (1), moderate-diffuse (2), or severe (3). Discrepancies (all of 1 grade) were resolved by a third opinion (WES; Consultant in Nuclear Medicine).
Normal controls all had normal ventilation scans. All mild asthmatics had normal (or grade 1) scans. The patient with moderate asthma had an abnormal scan grade 1. The severe asthmatics all had abnormal scans grade 2 or 3. Patients scanned during acute exacerbations had abnormal scans; one grade 1 and one grade 3. In stable patients scan grade was identical on repeat scanning though in severe asthma individual defects were transient. There was good correlation between FEV1 % predicted and severity of scan grade (r2 = 0.86).
We conclude that abnormal 81mKrypton ventilation scans are common in all but mild asthmatics, and that they broadly correlate with asthma severity. Scan grade is reproducible in stable asthma though individual defects are transient in severe disease. This rapid, low cost, low radiation technique may be useful in assessment of asthma.
ARDS mechanisms and management
S35 CHEMOKINE PRODUCTION BY MOUSE LUNGS SUBJECTED TO INJURIOUS MECHANICAL VENTILATION REQUIRES EXTRACELLULAR REGULATED KINASE 1/2 PATHWAY ACTIVITY
L. Pinhu1, M. R. Wilson2, M. Takata2, M. J. D. Griffiths1. 1Unit of Critical Care, Imperial College London at the National Heart & Lung Institute; 2Department of Academic Anaesthesia, Imperial College London at Chelsea & Westminster Hospital, UK
Background: Over distension of the lung by mechanical ventilation (MV) contributes to the mortality of patients with acute lung injury. Mechanical forces enhance the release of mediators that exacerbate lung damage and contribute to systemic inflammation and death. The neutrophil chemokine IL-8 has been implicated in the pathogenesis of ALI clinically and in animal models. Stretching monolayers of A549 cells (a human lung epithelial cell line) induced IL-8 production that is dependent on the ERK1/2 pathway and nuclear factor kappa-B DNA binding (Griffiths & Pinhu. Proc ATS 2005:A834). The aim of these experiments was to investigate to effect of an inhibitor of this pathway (U0126) in a murine model of ventilator induced lung injury.
Methods: Following instrumentation, male C57BL6 mice received 32 mg/kg U0126 (i.p.; Tocris Cookson) in 200 μl PEG/DMSO or vehicle. Animals were ventilated (VT 7–8 ml/kg, PEEP 2.5 cmH2O) for one hour, and then randomly allocated to control (same settings) or injurious ventilation (VT 35 ml/kg, zero end-expiratory pressure, rate 90 min−1, using air supplemented with 5% CO2) for one hour. We have previously demonstrated that the latter promotes neutrophilic lung inflammation, cytokine production, and eventually, acute lung injury (
). At the end of this period, whole lung homogenates were analysed for phosphorylated ERK1/2 by western blotting and for the murine chemokine (KC and MIP2α) message by real time PCR.
Results: Injurious MV was associated with ERK1/2 phosphorylation and induction of mRNA for KC and MIP2α. U0126 abolished MV induced ERK 1/2 activation in whole lung (p<0.05, n = 6) and significantly decreased the induction of KC and MIP2α.
Conclusion: These data support the role of the ERK1/2 pathway in mechanotransduction leading to chemokine production in the lung parenchyma as suggested by our studies in vitro.
This project is supported by the British Lung Foundation, Wellcome Trust, and Medical Research Council UK.
S36 THE EXTRACELLULAR SIGNAL RELATED KINASE PATHWAY MEDIATES MECHANOTRANSDUCTION IN A549 CELLS
L. Pinhu, M. J. D. Griffiths. Unit of Critical Care, Imperial College London at the National Heart & Lung Institute, Sydney Street, London SW3 6NP, UK
Rationale: Over distension of the lung contributes to the mortality of patients with acute lung injury. Mechanical forces enhance the release of mediators that exacerbate lung damage and contribute to systemic inflammation and death. The neutrophil chemokine IL-8 has been implicated in the pathogenesis of ALI clinically and in animal models. Stretching monolayers of A549 cells (a human alveolar epithelial cell line) and primary cultures of human alveolar type 2 cells, models of alveolar epithelial over-distension, causes IL-8 production that is dependent on nuclear factor-kappa B (NFkB) activity (
). We aimed to elucidate further the signalling pathways underlying this process.
Results: In A549 cells comparing 0, 5 and 30% stretch (20 Hz for two hours: Flexercell 4000X), IL-8 message (Rotor-gene 3000) and protein (R&D Systems) was significantly increased by 30% stretch. Mechanical strain was associated with rapid phosphorylation of p38, ERK1/2, and JNK, but of the three mitogen activated protein kinase (MAPK) pathway inhibitors used only U0126 (MEK1/ERK, Tocris Cookson: 10 μM) abolished stretch-induced IL-8 production. After mechanical strain for 5 minutes, cRaf, MEK1/2, ERK1/2 and p90RSK were phosphorylated and by 10 minutes phosphorylated ERK1/2 and p90RSK were detectable in nuclear extracts. Stretch was associated with DNA binding (TransAM, Active Motif) of cJun that was antagonised by the JNK inhibitor (SP600125, Calbiochem: 10 μM) and with cFos that was blocked by U0126. U0126 did not affect p65/NFkB DNA binding.
Conclusion: Stretch induced IL-8 production by A549 cells is mediated by activation of the ERK1/2 pathway, possibly through cFos DNA binding.
Supported by the British Lung Foundation.
S37 STRETCH INDUCED PULMONARY OEDEMA IS MEDIATED BY TUMOUR NECROSIS FACTOR RECEPTOR I SIGNALLING IN MICE
M. R. Wilson, S. Choudhury, M. Takata. Department of Academic Anaesthetics & Intensive Care, Imperial College London, UK
High stretch/high tidal volume ventilation has been shown to induce injury and inflammation in healthy lungs, although the mechanisms involved are not well understood. We previously demonstrated in mice (
) that stretch induced pulmonary inflammation, as evaluated by neutrophil recruitment in response to a standardised lung injury, is mediated by tumour necrosis factor (TNF). However, it is unclear whether TNF is involved in the development of mechanically induced lung injury per se, which is predominantly determined by formation of high permeability pulmonary oedema. To investigate this, we compared the effects of high stretch ventilation in wildtype C57BL6 mice (WT), and mice lacking TNF receptor I (p55KO), TNF receptor II (p75KO), or both receptors (DKO). Anaesthetised mice were ventilated with high tidal volume (initial peak inspiratory pressure (PIP) 45–46 cmH2O) using 95%O2/5%CO2 for two hours, or until blood pressure fell <45 mm Hg.
High stretch ventilation led to lung injury in WT animals, shown by increased PIP, decreased pO2, increased protein levels in lung lavage fluid, and increased lung wet:dry ratio, with only 27% of animals surviving the two hour ventilation period. Similar findings were observed in DKO mice. However, p55KO mice were substantially protected from the development of injury (all animals survived with little sign of lung injury) while p75KO mice may have been more susceptible than WT. These data strongly implicate involvement of TNF receptor I signalling in the development of pulmonary oedema induced by high stretch ventilation.
Funded by MRC and Wellcome Trust.
Abstract S37
S38 VASCULAR ENDOTHELIAL GROWTH FACTOR: NOT JUST AN ENDOTHELIAL CELL GROWTH FACTOR?
J. R. Roberts, G. D. Perkins, D. R. Thickett. Department of Medicine, University of Birmingham, UK
Background: Vascular endothelial growth factor (VEGF) has been widely recognised as an endothelial cell mitogen that is anti-apoptotic in a variety of endothelial cell lines. VEGF bioactivity is reduced in the alveolar compartment of patients with acute respiratory distress (ARDS). Recovery from lung injury is associated with restoration of those levels. In fetal pulmonary epithelial cells, VEGF is a proliferative agent. This study intends to address the hypothesis that VEGF is mitogenic for primary adult distal lung epithelial cells (DLEC) and that it has anti-apoptotic actions.
Methods: DLEC were obtained from clonetics. DLEC are nonciliated primary lung epithelial cells. Cells were cultured and incubated with or without 10 ng VEGF 165 isoform for 24 hours. The MTT assay (Promega) was used to determine cell proliferation and viability. Cell monolayers were also “wounded” using a pipette tip and the rate of wound closure measured during the 24 hours using photomicroscopy. To determine the effects of VEGF on apoptosis, cells were first treated with 0.03% hydrogen peroxide (H202) for 30 minutes before VEGF was added and the percentage of apoptotic cells measured by flow cytometry using annexin V staining, and in a separate experiment cells were first treated with 10 ng sFasL before VEGF was added.
Results: Adding VEGF to DLEC resulted in increased proliferation (control 0.57 (0.04) OD units v VEGF treated 0.78 (0.04) OD units p = 0.01). This was associated with an increased rate of wound closure over 24 hours (control 9.8% (3) v VEGF treated 20.5% (3.3) p = 0.004). VEGF also appeared to have an anti-apoptotic function as it inhibited H202 induced apoptosis. H202 induced cell death compared to control cells (control live cells 81.6% (3) v H202 treated 34.3% (2.1) p = 0.001) and this was associated with an increase in annexin V positive cells (control 6.1% (1) v H202 44.5% (5) p = 0.0001). The number of live cells (H202 live cells 34.3% (2.1) v VEGF treated live cells 56.5% (1) p = 0.001) was increased and annexin V positive cells (H202 44.5% (5) v VEGF treated 28.5% (3.7) p = 0.02) were reduced in the presence of VEGF. VEGF also recovered the viability of cells treated with sFasL (sFasL 0.26 (0.001) OD units v sFasL + VEGF 0.46 (0.01) p = 0.001).
Conclusion: VEGF has a proliferative effect on primary lung epithelial cells. This effect has been shown to be associated with increased wound repair and reduced apoptosis in these cells. Further work is needed as VEGF may have an important role in the recovery of damaged epithelial cells in the ARDS lung.
S39 DO BETA AGONISTS PROMOTE EPITHELIAL REPAIR?
G. D. Perkins1,2, J. R. Roberts1, S. McMahon1, F. Gao2, D. R. Thickett1. 1University of Birmingham, Birmingham, UK; 2Birmingham Heartlands Hospital, Birmingham, UK
Background: Extensive damage to the alveolar capillary barrier, alveolar flooding, and impairment of gas exchange are the hallmarks of ARDS. We previously reported that IV salbutamol significantly reduced extravascular lung water (EVLW) in patients with ARDS. In parallel we found a reduction in alveolar-capillary permeability suggesting salbutamol may have promoted alveolar-capillary repair. The aim of this study was to investigate the effect of salbutamol in vitro on epithelial cell proliferation and wound repair.
Methods: A549 cells (ECACC, Sigma, UK) were grown to confluence. Using an in vitro wound repair model, cell monolayers were “wounded” using a pipette tip and the rate of wound closure measured during the 24 hours using photomicroscopy. In separate experiments, the effect of a physiological concentration of salbutamol (10−6 M) or bronchoalveolar lavage (BAL) fluid from patients in the treatment and placebo groups on wound closure was determined. To establish the effect on cell proliferation and viability, A549 cells were cultured in the presence of control media or 10−6 M salbutamol. The MTT assay (Promega) was used to determine cell proliferation and viability.
Results: Treatment of wounded monolayers with salbutamol significantly increased wound repair (salbutamol 75 (4.1)% v control 44.7 (7.1)%, p = 0.001). This effect was blocked by co-incubation with 10−5 M propranolol (55.5 (4.6)%, p = 0.008). Salbutamol had no effect on A549 cell proliferation (1.30 (0.3) OD v 1.33 (0.3) OD, p = 0.757). Compared to saline control, incubation of the wounded monolayer with BAL fluid from patients at the onset of ARDS significantly increased wound repair (BAL fluid 40.1 (4)% v saline control 20.2 (3)%, p = 0.001). The rate of wound closure following incubation of BAL fluid from patients after four days’ treatment with IV salbutamol was significantly greater than for placebo treated patients (salbutamol 52.7 (4.4)% v placebo 46.2 (4.3)% respectively, p = 0.008).
Conclusion: Physiological concentrations of salbutamol significantly increased wound repair in an in vitro model of mechanical alveolar epithelial damage. This occurred without increasing proliferation, suggesting the effect is through cell spreading. BAL fluid from patients treated in a randomised controlled trial with IV salbutamol stimulated significantly greater wound repair than BAL fluid from patients in the placebo arm. These data suggest that salbutamol may have an effect in vivo on repair of the alveolar capillary barrier.

The BPOLD registry
S40 ESTABLISHMENT OF A WEB BASED RESEARCH TOOL, INFORMATION RESOURCE, AND PATIENT LED SUPPORT FORUM FOR RARE PAEDIATRIC RESPIRATORY DISEASE IN THE UK (THE BPOLD REGISTRY)
A. Laverty1, P. Weller2. 1Portex Respiratory Unit, Great Ormond Street Hospital for Children, London; 2Centre for Measurement and Information in Medicine, City University, London, UK
Introduction: Research trials on rare paediatric respiratory diseases are hampered by a shortage of data due to scarcity of numbers and disparate geographical location of patients. Such rarity also leads to scant knowledge about these conditions and little opportunity for support within parents/patient groups.
Aims: (1) To establish a registry of rare lung diseases in British children, facilitating the collection of data on nine rare, or orphan, paediatric respiratory diseases across the UK. (2) To establish a website as an information resource for these diseases. (3) To provide a support network to sufferers of these diseases and their families.
Methods: A website was developed: a “back end” relational database (MySQL) is accessed via web pages developed using PHP scripting language. BPRS members were encouraged to register on site to allow them to securely submit incidence data via the website. Current knowledge on the conditions is available online and a forum allows patients and families to correspond.
Results: Since the site launch (20 January 2005), 82 clinicians have registered (table 1) with 20 (24%) submitting data on 44 occasions with results as shown in table 2.
Abstract S40, table 1
Abstract S40, Table 2
Conclusion: The British Paediatric Orphan Lung Disease (BPOLD) website (http://www.bpold.co.uk) provides a means by which registered UK paediatricians can submit data on nine rare lung diseases to a database. The site also acts as an information resource for clinicians and a support network for patients and families.
Sponsors: Cohen-Zimbler Family Trust and British Paediatric Respiratory Society.
Impact of the environment on paediatric lung disease
S41 HYGIENE HYPOTHESIS: A TEST WITHIN A UK BIRTH COHORT
J. M. Harris, P. Cullinan, P. Mills, C. White, S. Moffat, A. J. Newman Taylor. Department of Occupational and Environmental Medicine, Imperial College School of Medicine (NHLI), 1B Manresa Road, London, UK
We have previously reported, among the parents of a birth cohort in Ashford Kent, that neither serological nor documented burdens of early-life infection could adequately explain the “birth order” effect on atopy. We also reported that any associations between antibiotic prescriptions in early life and asthma were likely to be explained by a protopathic bias. Here we examine the same relations among the cohort children, a generation with far higher rates of antibiotic use and reported infections.
642 children were recruited before birth and seen annually until age 8 years. Information from GP medical records was available for 594 (93%), and atopic status (ascertained by skin prick test) at age 8 for 548 (85%), children. Details on current wheeze and seasonal rhinitis at age 8 were recorded for 593 (92%). 104 (19%) children were atopic and 79 (13%) were currently wheezy with 37 (6%) both atopic and wheezy; 123 (21%) had seasonal rhinitis of whom 36 (6%) had a positive skin test to grass pollen.
577 (97%) children had at least three infections recorded by age 5, a figure much higher than that of their parents (69%). Higher numbers of infections were recorded for boys and for high birth order children. After adjusting for parental allergy and birth order, there was no association between infection counts and atopy (odds ratio (OR) 1.01 (95% CI 0.99 to 1.03) per infection). Significant associations were found for wheeze and atopic wheeze, especially for lower respiratory (OR 1.15 (1.09 to 1.21) and 1.11 (1.06 to 1.17)) and gastrointestinal infections (OR 1.28 (1.06 to 1.50) and 1.29 (1.03 to 1.62)). Antibiotic prescriptions were also more frequent for the children than their parents; by the age of 5 only 11 (2%) children had never received a prescription for antibiotics; the corresponding figure for the parents was 24%. An increased risk of current wheeze was found for each antibiotic prescription (adjusted OR 1.06 (1.03 to 1.10)) but this was mostly explained by prescriptions for respiratory infections. No associations were found for atopy.
Despite very high rates of recorded early life infections and antibiotic prescriptions we have failed to find any plausibly causative relations with subsequent respiratory allergies.
Funded by the Colt Foundation, UK.
S42 CORONA IONS FROM HIGH VOLTAGE POWER LINES ARE NOT ASSOCIATED WITH ADVERSE EFFECTS ON LUNG HEALTH, ASTHMA, OR ATOPY IN YOUNG CHILDREN: A LONGITUDINAL BIRTH COHORT STUDY
A. Maitra1, L. Miller1, M. Wright3, H. Thomas4, A. Preece3, D. Henshaw2, J. Henderson1. 1Department of Community based Medicine, University of Bristol; 2Department of Physics, University of Bristol; 3Department of Nuclear Physics, Bristol Oncology Centre; 4Bristol Children’s Hospital, UK
Background: Corona ions emanating from high voltage overhead power lines may have an effect on the lung health and atopy by increasing respiratory tract deposition of particulate matter, including pollutants, and allergens (1, 2).
Objective: The aim of this study was to investigate the effects of corona ions associated with high voltage power lines on lung function, asthma, and allergy in children from a longitudinal birth cohort.
Methods: The Avon Longitudinal Study of Parents and Children (ALSPAC) recruited 14 000 pregnant women resident in Avon, and has followed their children’s health and other outcomes from birth. This study includes children who were resident at the same address from birth to 8.5 years, when relevant outcome assessments were made. This included spirometry, skin prick tests, reported symptoms of rhinitis and wheezing, and physician diagnosed asthma (PDA). Addresses of residence were mapped to high voltage power lines using distance along a downwind vector and categorized as ⩽400 m, 400 m–1 km, and >1 km.
Results: Complete data were available on 4197 children of whom 520 were resident within 1 km of a power line (150 were resident within 400 m). Data were available for the following number of subjects: lung function measurements (n = 2270); atopy by skin prick test (n = 2187); rhinitis (n = 1961); wheezing phenotypes (n = 2396); and PDA (n = 2543). Continued residence in an area downwind of and in close proximity to high voltage overhead power lines was not associated with any of the outcomes considered.
Conclusion: Estimated exposure to corona ions from overhead power lines was not associated with markers of lung health or atopy in this cohort of children.
S43 DOES THE FALL IN CHILDHOOD ASTHMA PREVALENCE REFLECT FEWER RESPIRATORY TRACT INFECTIONS?
D. S. Urquhart1, A-KAnderson1, S. A. McKenzie2. 1Portex Respiratory Medicine Unit, Institute of Child Health and Great Ormond Street Hospital for Children, London WC1N 3JH; 2Department of Paediatric Respiratory Medicine, Royal London Hospital, Whitechapel, London E1 1BB, UK
Background: Asthma prevalence has fallen over the last 10 years.1 Changes in atopic status, aeroallergen exposure, pollution, diet, and the protective effect of infections in early life are unlikely to account for this. An increase in inhaled corticosteroid prescribing in primary care could explain the fall,2 but adherence is poor, especially in preschool children.3 However, both acute respiratory tract infections (ARI) and RSV isolates have also fallen over the same period.4–6
Aims: To generate the hypothesis that the fall in childhood asthma prevalence may reflect a fall in ARI.
Methods: Review of UK statistical data on asthma exacerbations, hospital admissions and new diagnoses,7 numbers presenting to primary care with ARI,4 and primary source data for numbers of RSV, influenza A and B, and parainfluenza virus isolates (Health Protection Agency Centre for Infections (HPA) data 1990–2003).
Results: Asthma prevalence, acute respiratory infections in primary care, and RSV isolates over the last decade have all fallen by between 40 and 70% approximately (see fig).4,6,7 Influenza and parainfluenza isolates have not fallen.

Discussion: Asthma, atopic or not, is most commonly triggered by respiratory viruses8 and parents report infectious triggers are more likely than allergic ones.7 The relation between falling ARI and asthma is plausible. Of the three common viruses for which data exist, only RSV has fallen. Falling ARI may reflect improved living conditions from 1991–2003, when both overcrowding and child poverty decreased.7 By this rationale however, all viral infections, including rhinoviral would be expected to fall. These observations could inform further studies.
1
2
3
4
5
6
7
8
S44 ASSOCIATION OF ALVEOLAR MACROPHAGE CARBON LOADING AND ANNUAL MODELLED PM10 AT RESIDENCE IN HEALTHY CHILDREN
N. Kulkarni1, N. Pierse2, L. Rushton2, J. Grigg1. 1Department of Infection, Immunity and Inflammation, University of Leicester, Leicester UK; 2Institute of Environment and Health, University of Leicester, Leicester UK
Background: Epidemiological studies suggest that level of particulate matter (PM) at the home address is associated with an increased prevalence of respiratory symptoms in children. To date, these studies have used proxy markers of individual exposure. We sought to establish whether analysis of carbon loading of alveolar macrophages (AM) could be used to assess individual exposure to inhalable PM >10 μm (PM10).
Aim: To determine the association between AM carbon loading and modelled exposure of the home address to PM10.
Methods: Healthy children (8–15 years) from non-smoking families were studied. AM were sampled by sputum induction. Carbon loading of AM was measured using image analysis of 100 images of AM per child, and expressed as the median area of carbon (mm2)/AM/child. The mean annual modelled primary PM10 (that is, locally emitted PM10) was calculated for the home address using the AIRVIRO dispersion model. Linear regression was used to assess associations.
Results: Carbon loading was determined for 64/116 children. There was a weak, but positive, correlation between loading and modelled exposure (r2 = 0.081, p = 0.022). Thus for each unit increase in modelled primary PM10 at the home address, there was a 0.101 mm2 increase in the two dimensional surface area of carbon in AM.
Conclusions: Analysis of AM is a promising, non-invasive method of assessing individual PM exposure.
S45 COMPREHENSIVE ADOLESCENT ASTHMA SERVICE IMPROVES CLINICAL OUTCOMES
M. B. H. Smith, D. Addis, A. McCann, R. Convery. AIR centre, Departments of Respiratory Medicine and Paediatrics, Craigavon Area Hospital Group Trust, Craigavon, Co Armagh, N Ireland
Asthma is the most common chronic illness of adolescence. Recent evidence suggests that specialised care may improve outcomes.1
We have developed an interdisciplinary adolescent asthma service that includes nursing, pulmonary function technicians, pharmacy, allergy testing, audit personnel as well as paediatric and respiratory medicine consultants. The aim of this service is to provide intensive monitoring and self-management education to adolescents affected with moderate to severe asthma.
Of the patients available for analysis (n = 38, F: 34%, M: 65%) 76% were at BTS guidelines step 3. After a 6–12 month follow up of care there was a mean improvement in FEV1 of 7.13% and FVC of 4.9%. Of those patients with frequent symptoms there was reduction in daytime symptoms (mean –4.4 days: p<0.05), night time wakening (−3.4 nights per week: p<0.05) and rescue steroid (−2.33 courses per year: p<0.05) In patients who were skin prick positive for one or more allergens, there were significant improvements in number of symptom days per week (p<0.05), exertional symptoms (p<0.02), steroid rescue events (p<0.001), and number of admissions per year (p<0.05). The presence of allergic rhinitis or eczema did not predict similar benefits. Social isolation, delayed puberty/adrenal insufficiency, and osteoporosis were also confirmed in a small section of this group. Quality of life assessment from patients and families has been favourable.
Intensive, interdisciplinary care of adolescents with asthma results in important improvements in outcome. Concurrent allergy evaluation improves predictability of a therapeutic response.
1
Tuberculosis: clinical
S46 PHASE I/II CLINICAL TRIAL OF MVA85A IN INDIVIDUALS WITH LATENT TUBERCULOSIS: THE FIRST SUBUNIT TB VACCINE IN CLINICAL TRIAL
C. R. Sander, A. Pathan, F. Gleeson, R. J. O. Davies, G. Pasvol, J. VanWijgerden, A. V. S. Hill, H. McShane. Centre for Vaccinology and Tropical Medicine, Churchill Hospital, Old Road, Headington, OX3 7LJ, UK
There are 8–9 million new cases of tuberculosis (TB) per annum and one third of the world is infected with TB. BCG vaccination confers some protection against disseminated TB in children but has variable efficacy against adult pulmonary disease. Heterologous prime boost immunisation strategies induce high levels of cellular immunity. Antigen 85A is a highly conserved immunodominant protein expressed by all mycobacteria and is a leading candidate antigen for inclusion in a new TB vaccine. Several animal models have shown that boosting BCG (which secretes antigen 85A) with modified vaccinia Ankara expressing antigen 85A (MVA85A) induces greater protection against aerosol TB challenge than either vaccine alone.
There are concerns with new TB vaccines entering clinical trials about the induction of a Koch phenomenon (immunopathology), in individuals infected with TB or other mycobacteria. This is based on murine data where TB infected mice developed severe lung pathology following vaccination with an immunogenic vaccine, as well as on Koch’s original experiments in both guinea pigs and humans. Therefore, clinical trials for MVA85A began in individuals estimated to be as mycobacterially naive as possible and have progressed to BCG vaccinated individuals through to the current study of latently infected TB patients.
Several phase I trials of MVA85A have taken place in the UK and Africa in healthy uninfected volunteers. It induces high levels of antigen specific T cells in BCG naive subjects and significantly higher levels in BCG primed subjects. Responses are maintained for at least 12 months after vaccination.
We are recruiting latently infected individuals, defined by positive ESAT-6 and CFP-10 on ex vivo IFNγ elispots, from TB contact clinics. TB disease is excluded clinically and by chest x ray. Safety is the primary outcome of this trial and diary cards and regular clinical review with safety bloods including inflammatory markers are used to monitor side effects and adverse events. Thoracic CT scans are performed prior to vaccination and 10 weeks post vaccination to investigate the possible induction of Koch’s phenomenon. Six individuals have been vaccinated to date with no serious adverse events. Five out of six had normal thoracic CT scans at vaccination, one had mild mediastinal lymphadenopathy. The three follow up CT scans performed to date have remained normal. Ex vivo IFNγ and IL-2 elispots to antigen 85A, ESAT-6, and CFP-10 are being measured at 1, 2, 4, 8, 12, and 24 weeks post vaccination and are the primary immunological readout. We are seeing the induction of strong antigen specific T cellular responses. Up to date data will be presented.
Supported by: European Union AFTBVAC (C R Sander) and Wellcome Trust Fellowship (H McShane).
Abstract S46
S47 PROSPECTIVE STUDY OF PARADOXICAL REACTIONS IN TUBERCULOSIS PATIENTS
R. A. M. Breen, W. Holmes, F. Perrin, G. Bhatt, I. Cropley, M. A. Johnson, M. C. I. Lipman. Department of Thoracic and HIV Medicine, Royal Free Hospital, London NW3 2QG, UK
Background: Paradoxical reactions (PR), the transient worsening of tuberculosis (TB) during treatment have been widely reported since combination anti-retrovirals (HAART) became available for use in HIV infection. The development of PR can lead to extensive investigation and expense. However little is known about either the mechanisms or risk factors underlying this phenomenon; and no systematic study has been undertaken.
Methods: Since August 2003 we have been enrolling a cohort of TB patients with and without HIV and documenting the incidence of PR; and its clinical and laboratory features. PR is defined as a worsening of TB symptoms and signs with no evidence of treatment failure, drug reaction, or other intercurrent disease.
Results: 125 individuals have been enrolled to date of whom four have not HIV tested. Of the remaining 121, 39 are HIV positive (32%) and 82 (68%) HIV negative. These subjects are described in the table. HIV+ individuals with PR had a greater incidence of systemic symptoms (9 of 11 v 3 of 14) and more frequently required steroid treatment for severe reactions (8 of 11 v 3 of 14). HAART was discontinued during PR in one case. No-one had anti-TB therapy stopped. Inflammatory markers (CRP, ESR, and LDH) at baseline did not predict risk of PR; and also did not alter in a consistent manner with the onset of PR. Median blood CD4 count at TB diagnosis in the HIV+ patients with PR was 94 cells/μl (range: 11–803) and 260 cells/μl (13–844) in those with no PR. In HIV/TB patients who started HAART, the rise in blood CD4 count after 2 months was 72 cells/μl (0–123) in the PR group and 106 cells/μl (−42–334) in the no-PR group.
Conclusion: Our study demonstrates a high rate of PR in both HIV+ and HIV− subjects. This is typically at the original site of disease. It appears to be more severe in HIV+ patients; though in the majority of cases can be managed with symptomatic treatment or a watch and wait policy. Simple baseline blood tests do not predict risk of PR in our cohort.
S48 MIRU-VNTR FINGERPRINTING OF M TUBERCULOSIS ISOLATES FROM EAST LANCASHIRE: 2001–05
L. P. Ormerod1, P. Maynard2, I. Hafeez3, D. Sails, S. Barrett4. 1Chest Clinic and 2Department of Microbiology, Blackburn Royal Infirmary; 3Pendle Community Hospital, Nelson; 4Regional Mycobacteriology Unit, Newcastle Royal Victoria Infirmary, UK
Data on drug resistance in M tuberculosis isolates from the Blackburn part of East Lancashire from 1960–2000, suggests little transmission of tuberculosis between the Indian subcontinent (ISC) population with a consistent 7–10% isoniazid resistance rate, and the white population whose isoniazid resistance rate is virtually zero. MIRU-VNTR fingerprinting now allows local epidemiology to be enhanced.
All isolates of M tuberculosis from East Lancashire (Blackburn/Darwen; Hyndburn/Ribble Valley; Burnley Pendle, and Rossendale PCTs) are sent to the Regional Mycobacterium Centre in Newcastle. All isolates for the calendar years 2001–04, plus the first quarter of 2005, were retrieved and tested for the following MIRU loci: 2, 4, 10, 19, 16, 20, 23, 24, 26, 27, 31, 39, and 40. The repeat numbers of the 12 loci MIRU-VNTR were combined to give the 12 digit MIRU-VNTR profile. The exact tandem repeat loci (ETR) were also characterised for some isolates to provide additional discrimination within clusters.
187 isolates were recorded. 27 from white ethnic patients of which 12 (44%) were non-clustered, and 15 (56%) clustered; 160 from non-white patients of which 112 (70%) were non-clustered and 48 (30%) clustered. There were two white clusters with 4, and 5 cases respectively, where transmission via public houses was shown. One of these was known, but the larger cluster evolved over time and was only linked after fingerprinting. There were 13 non-white clusters; nine involved two cases, three involved three cases, one involved eight cases dividing into two subsets of six and two by ETR subtype. Five of the clusters could be definitely linked by contact tracing data. The remainder are undergoing more detailed retrospective analysis. There were six possible clusters with both white and non-white patients. Five of these had single white and non-white cases.
Retrospective analysis showed no epidemiological links, one “cluster” separated on drug resistance data, and clinical type of disease and timings did not support linkage of the other cases. Finally there was one large cluster of 15 cases, which split into four subsets on ETR. One subset of three cases included one white case, but retrospective analysis found no epidemiological or clinical link.
MIRU-VNTR testing of isolates complements conventional “shoe leather” epidemiology and can show a higher proportion of clustered cases than expected and possible transmission in settings not previously recognised. In this area of high prevalence, these data together with clinical and conventional epidemiological data, have shown not evidence of transmission between the white and non-white ethnic groups.
S49 TRENDS IN INCIDENCE AND MICROBIOLOGICAL CONFIRMATION OF EXTRA PULMONARY TUBERCULOSIS IN ENGLAND AND WALES 1999–2003
I. Abubakar, J. Crofts, P. Sonnenberg, J. M. Watson. Tuberculosis Section, CfI, Health Protection Agency, Colindale, London, UK
The number and proportion of extra pulmonary tuberculosis cases (EPTB) reported in England and Wales appears to be increasing. The diagnosis is often difficult due to the spectrum of disease and the limited specificity of the clinical manifestations. The diagnosis may be strengthened by histological findings or smear microscopy and only confirmed by microbiological culture. The Department of Health’s Tuberculosis (TB) National Action Plan has proposed a goal of 65% culture confirmation of pulmonary disease but no target for EPTB. We analysed national surveillance data to examine trends in EPTB and the proportion of cases confirmed by laboratory investigations. Data from Enhanced TB Surveillance for 1999 to 2003 for England and Wales were matched with national reference laboratory data to supplement microbiological information. Cases were categorised by diagnostic method including culture, microscopy, histology, and molecular amplification test. Trends in diagnosis and clinical and demographic factors associated with method of diagnosis were investigated. The number of patients with EPTB increased from 2310 in 1999 to 2885 in 2003 (see fig). The proportion of patients with evidence of any laboratory confirmation of EPTB increased from 54% in 1999 to 57% in 2003, (p for trend <0.01). A smaller increase was observed for culture confirmed disease (48% in 1999 and 49% in 2003, p for trend <0.05). The range for culture confirmed EPTB in Western European countries in 2002 was 5–70%. EPTB cases found to be associated with a lower chance of laboratory confirmation included those reported among children (0–14 years), females and those from the Indian subcontinent (p<0.01 for all). Patients with tuberculosis of the bone (69%), genitourinary tract (74%), or lymph nodes (68%) were more likely to have laboratory confirmation, while those with TB meningitis (36%), miliary (50%), or cryptic (21%) TB were less likely (p<0.01). These results indicate that an increasing proportion of cases of EPTB are microbiologically confirmed and that the increase in the proportion of all cases due to EPTB is likely to be real. While a substantial proportion of all cases remain unconfirmed, further study is needed of the reasons for failure to confirm to fully understand the observed trends.
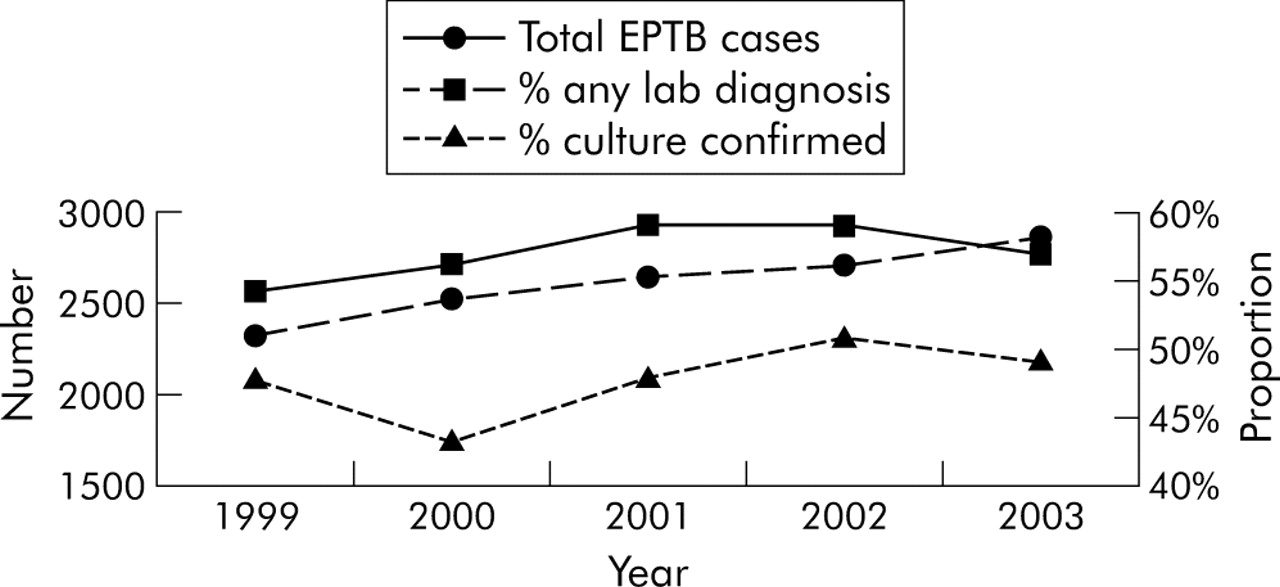
Total extra pulmonary tuberculosis cases and proportion of lab confirmed; E&W, 1999–2003.
S50 THE DIAGNOSIS OF ACTIVE TUBERCULOSIS AND THE ELISPOT TEST
A. E. Boyd, A. Ashcroft, G. H. Bothamley. Homerton University Hospital NHS Trust, London, UK
Introduction: Tuberculin (TST) is currently used in the diagnosis of tuberculosis (TB) but has a poor specificity. An elispot test based on secretion of interferon-γ by T cells in response to peptides of ESAT-6 and CFP-10 hold the promise of greater specificity. We have examined one of these (T SPOT-TB, Oxford Immunotec (OI)) in a clinical setting.
Methods: We conducted a single blind prospective case control study July 04–July 05 of 182 adult patients with suspected active TB. 24 were excluded because of failure of control (14), laboratory error (8) or insufficient white cells (2). The T SPOT-TB tests were provided free of charge by OI and were performed in addition to standard tests.
Results: See table.
Abstract S50
Conclusion: Excluding results in brackets, 27 of 28 (96.4%) patients with culture confirmed TB had a positive elispot (T SPOT-TB) test and one was borderline positive. In total, 37 of 46 (80.0%) patients treated for TB and four of 19 (21.0%) patients with a firm alternative diagnosis to TB had a positive elispot (T SPOT-TB) test.
S51 INCREASING TUBERCULOSIS IN ENGLAND AND WALES COMPARED WITH A DECREASING TREND IN THE USA: A MATTER OF MIGRATION
S. Duraira, P. D. O. Davies. Arrowe Park Hospital, Wirral and Tuberculosis Research and Resource Unit, Cardiothoracic Centre, Liverpool, UK
The Government action plan for tuberculosis (TB) published in October 2004 compares tuberculosis in the USA with the UK and suggests that the decline in tuberculosis achieved in the USA since 1993 can be copied in the UK if a “can do” attitude is adopted. The report states that a successful tuberculosis programme will be reflected in a decline in cases and case rates. We have analysed the latest data on tuberculosis available on the websites of the tuberculosis surveillance units of the two countries to determine why there is such a marked difference in the incidence and trends of TB (http://www.cdc.gov/nchstp/tb/pubs/slidesets/surv/surv2003/Slides/surv8.htm and http://www.hpa.org.uk/infections/topics_az/tb/epidemiology/figures/figure5.htm).
Data for England and Wales (E&W) were compared with data from the USA. In 2003 rates of disease in the white indigenous population of each country was virtually identical 2.9/100 000 per annum in the USA compared with 3.0 in E&W.
The number of cases in the USA had declined from approximately 28 000 per annum in 1992 to 16 000 by 2003 (43%) compared with an increase from 5921 to 6518 (10%) in E&W over the same period. Rates for all Foreign born in the USA declined steadily over this time. In the UK rates among the foreign born collectively increased form 73 in 1999 to 91 (25%) in 2002. Among the foreign born groups in the USA in 2003 expressing rates as a ratio to the white rate, the rate ratio for Asians was 10 and for the black group were 4. In E&W the rate ratios were 23 for Chinese, 65 for those of Indian subcontinent origin (India Pakistan Bangladesh and Sri Lanka), and 122 for black Africans. The aggregated case rate ratio for the foreign born in the USA for 2002 was 1.8 compared with 26.9 in E&W.
The cities of New York and London were compared in the government report, the former seeing an approximate halving of cases over the period covered compared with an approximate doubling in London.
The disparity in tuberculosis case rates between the two countries is largely explained by immigration patterns. This is likely to exceed any reduction in cases which can be made by a fully efficient tuberculosis control programme.
Non-invasive ventilation
S52 RANDOMISED CROSSOVER TRIAL OF MECHANICAL IN-EXSUFFLATION PLUS NON-INVASIVE VENTILATION (NIV) ASSISTED CHEST PHYSIOTHERAPY VERSUS NIV ASSISTED PHYSIOTHERAPY ALONE IN NEUROMUSCULAR PATIENTS WITH AN ACUTE RESPIRATORY TRACT INFECTION
M. Chatwin, A. K. Simonds. Clinical and Accademic Department of Sleep and Breathing, Royal Brompton Hospital, London, UK
Background: Respiratory tract infections (RTI) are a major cause of mortality and morbidity in individuals with neuromuscular disease (NMD), including those using non-invasive ventilation (NIV). The cough in-exsufflator, (CI-E) (JH Emerson, Co) is a device that increases peak cough flow (PCF) and should therefore improve sputum clearance. We hypothesised that treatment of an acute RTI will be more effective with CI-E in addition to current physiotherapy practice (CP+CI-E) (an increased non-invasive ventilator pressure, percussion, shaking, and manual assisted cough) compared to current physiotherapy practice alone in long term NIV users (an increased non-invasive ventilator pressure, percussion, shaking, and manual assisted cough) (CP).
Methods: Eight patients (6 male) with NMD (Duchenne muscular dystrophy, 4; spinal muscular atrophy II, 3; congenital muscular dystrophy, 1), median age 21.5 (range 4–44) years participated. All had difficulty clearing secretions and a symptomatic RTI with either a raised CRP median (range) 113 (13–321) or WCC 14 (7–25). Sputum culture was positive in three. Patients underwent a two day randomised treatment programme of CP for one session and CP+CI-E for second, with crossover order the next day (16 treatments in each arm). Total treatment time was recorded and treatment effect was assessed at 30 minutes or earlier if sputum clearance was complete. Mean heart rate (HR), mean oxygen saturation (SpO2), mean transcutaneous carbon dioxide (TcCO2) along with pre and post independently assessed auscultation score and amount of expectoration were recorded. Patients rated tolerance and effectiveness on a VAS.
Results: There was no difference for mean HR, SpO2 or TcCO2 recorded through either treatment. There was a significant improvement in auscultation scores for both groups (CP = 3.4 (SD 2.0) to 2.3 (SD 2.2); CP+CI-E 2.9 (SD 1.9) to 1.8 (SD 2.0)). All treatments lasted for at least 30 minutes apart from one CP+CI-E session. Treatment time after 30 minutes was significantly shorter in the CP+CI-E treatment group (CP = 17 (0–35) v CP+CI-E = 0 (0–26) minutes) (p = 0.03). Patients reported subjectively better VAS for amount of sputum cleared in the CP+CI-E group (CP 4.0 (SD 1.4) to 3.0 (SD 1.4) and CP+CI-E 4.0 (SD 2.2) to 2.4 (SD 1.7) (p<0.05) cm. Similar inspiratory and insufflation pressures were used (21 (SD 5.6) and 21 (SD 5.6) respectively).
Conclusion: Comparable results are seen for both methods of airway clearance CP (an increased non-invasive ventilator pressure, percussion, shaking, and manual assisted cough) and CP + mechanical insufflation exsufflation. CI-E in combination with NIV may facilitate a shorter and subjectively more effective physiotherapy session in neuromuscular patients with an acute RTI.
MC was supported by unrestricted research grants from: The Jennifer Trust for SMA (UK) and Breas Medical (Sweden).
S53 SPONTANEOUS BREATHING TRIAL TO PREDICT THE DEGREE OF VENTILATOR DEPENDENCE IN PATIENTS WITH NEUROMUSCULAR DISEASE
N. Hart1, A. Perez2, M. Lejaille2, M. Polkey3, F. Lofaso2. 1Lane Fox Unit, St Thomas’ Hospital, London, UK; 2Service de Physiologie, Hôpital Raymond Poincaré, Garches, France; 3Respiratory Muscle Laboratory, Royal Brompton Hospital, London, UK
Background: Patients with severe neuromuscular disease may require nocturnal (NVS) or even full ventilatory support (FVS). However, it is difficult to predict the daily requirement of ventilatory support. We hypothesised that inspiratory muscle strength and pattern of breathing adopted during a spontaneous breathing trial (SBT) would predict daily ventilator requirements.
Method: A prospective study of 19 patients with advanced neuromuscular disease was performed; 8 patients required NVS (<12 hours/day; mean 10 (SD 2) hours) and 11 patients required FVS (>12 hours/day; mean 20 (SD 3) hours). All patients were disconnected from their ventilator for up to 60 minutes following a night of ventilation. Prior to disconnection and at termination we measured inspiratory mouth pressure (PImax), arterial blood gases, tidal volume (VT), respiratory frequency (fR), and minute ventilation (VE) using a pneumotachograph. Subjective effort of breathing and headache scores were assessed using visual analogue scales.
Results: Groups were matched for age, body mass index, and duration of ventilatory support.
Abstract S53
Conclusion: There was no difference between the two groups prior to disconnection. However, at termination, although we observed similar inspiratory muscle strength and gas exchange, the FVS group had a rapid shallow breathing pattern. In addition, the FVS patients had greater perceived sensation of breathing difficulty and higher headache scores, despite a similar rise in PaCO2 as the NVS group. Therefore, measuring inspiratory muscle strength does not discriminate between patients on nocturnal and full ventilatory support, but assessment of breathing pattern combined with dyspnoea and headache scores during a SBT may facilitate decisions about level of ventilatory support.
Nicholas Hart was funded by Scadding-Morriston Davies Joint Fellowship in Respiratory Medicine and the Association Française Contre Les Myopathies.
S54 NON-INVASIVE VENTILATION AND CORTICOSPINAL PATHWAYS IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
N. S. Hopkinson1, T. Sharshar1,2, E. B. Swallow1, M. J. Dayer1, F. Lofaso2, J. Moxham3, M. I. Polkey1. 1Respiratory Muscle Laboratory, Royal Brompton Hospital, London; 2Hôpital Raymond Poincaré, Garches, France; 3Department of Respiratory Medicine, King’s College Hospital, London, UK
Background: The effect of chronic obstructive pulmonary disease (COPD) on the corticospinal pathways to the diaphragm is incompletely understood. We hypothesised that COPD might induce chronic changes which could be relevant to functional status and the need for home mechanical ventilation. We therefore compared the excitability of corticospinal pathways between ventilator users and non-users and in patients on and off ventilation and also studied the relation between cortical excitability and functional measures of disease severity and inspiratory muscle strength.
Methods: The diaphragm response to transcranial magnetic stimulation was compared between long term users and non-users of home ventilation and responses during spontaneous breathing compared to those during isocapnic non-invasive ventilation.
Results: The two patient groups did not differ in terms of motor evoked potential amplitude or latency, nor in the excitability of intracortical inhibitory or facilitatory circuits assessed using paired stimulation with short and long interstimulus intervals respectively. Intracortical facilitation was strongly correlated with inspiratory muscle strength (r2 0.72 p<0.001) whereas intracortical inhibition was correlated with PaCO2 (r2 0.51 p = 0.01). Acutely, ventilation reduced diaphragm motor evoked potential but had no effect on intracortical facilitation or inhibition implying an effect of neuromechanical feedback at brainstem or spinal level.
Conclusions: The excitability of intracortical circuits in COPD is related to measures of disease severity but not to chronic use of non-invasive ventilation. Acute ventilation does not produce the changes in intracortical excitability previously demonstrated in healthy subjects implying that there is long term reorganisation of the motor cortex in COPD.
Funded by The Wellcome Trust and The European Union ENIGMA project.
S55 NON-INVASIVE POSITIVE PRESSURE VENTILATION FOR ACUTE RESPIRATORY FAILURE: VALUE AS A CEILING THERAPY
S. Gareeboo, A. Petter, S. Singh. Chelsea & Westminster Hospital, Imperial College, London, UK
Background: Non-invasive positive pressure ventilation (NIV) is established in the management of acute hypercapnic respiratory failure (AHRF). It reduces the need for mechanical ventilation and improves survival compared to standard medical care in acute exacerbations of chronic obstructive airways disease (AECOPD). It is improves outcome in other causes of respiratory failure. However, whether it is of value in those with severe respiratory acidosis deemed unsuitable for mechanical ventilation remains unclear. A ward based NIV service, delivered by a consultant-led critical care outreach team was set up outside the intensive care unit at our hospital in 2003. We report the result of an audit of patients offered NIV in our unit.
Methods: A retrospective audit of patients offered NIV (excluding HDU/ITU) from June 2003 to March 2005 in a London Teaching Hospital. An Audit Record, modified from the BTS guidelines, was used.
Results: There were 96 episodes of NIV in 96 patients identified over a 20 month period. We reviewed 95 of those episodes; 65% of those being in patients with COPD. The overall success rate (improved on therapy and discharged) was 57%, with 20% of “failure” being due to intolerance of the treatment. The changes in pH and pCO2 are shown in table 1. Of the group who were given NIV as a ceiling of therapy, 33% survived to discharge. In contrast, the survival rate in those who did not tolerate the treatment and deemed unfit for intubation was 48%.
Conclusion: The audit confirms that NIV is effective in patients with AHRF. Moreover, it shows that NIV is beneficial as an active treatment irrespective of the decision to use it as a ceiling of therapy. It should hence need not considered as a palliative therapy.
S56 DOES LONG TERM DOMICILIARY NON-INVASIVE VENTILATION IMPROVE SURVIVAL IN SEVERE HYPERCAPNIC CHRONIC OBSTRUCTIVE PULMONARY DISEASE?
N. Oscroft, S. Pilsworth, T. Quinnell, J. Shneerson, I. Smith. Respiratory Support and Sleep Centre,Papworth Hospital, Cambridge, UK
Introduction: The survival of patients admitted with an acute exacerbation of chronic obstructive pulmonary disease (COPD) with acidosis is poor with studies reporting 1 year survival of 51% (
) and 62% (
). Prognostic indicators such as low forced expiratory volume in one second (FEV1), carbon dioxide (CO2) retention with oxygen (O2) therapy and older age have been shown to be markers of poor outcome. We review our experience of commencing long term domiciliary non-invasive ventilation (NIV) in patients with extremely poor prognostic markers and in whom consideration of long term NIV is recommended by NICE.
Methods: A retrospective case note analysis was performed on patients with a diagnosis of COPD who were transferred to our unit between 01/01/2000 and 31/12/2003 and commenced on long term domiciliary NIV. Before transfer patients received standard treatment for a COPD exacerbation including acute NIV but were not intubated. Patients were typically in hospital for over 48 hours before transfer. The following inclusion and exclusion criteria were used to define the population. Inclusion criteria: diagnosis of COPD: FEV1 <50% predicted, FEV1/forced vital capacity ratio <70%, total lung capacity> 80% predicted, smoking history >20 pack years. Prior to commencing NIV on referral to our unit daytime PaCO2>7.5 kPa with pH>7.35 or nocturnal transcutaneous pCO2>9 kPa. Exclusion criteria: age>80, other significant respiratory disease, left ventricular dysfunction, body mass index (BMI) >35. Referral predominantly for excessive daytime somnolence.
Results: Twenty eight patients were identified with these characteristics: mean (standard deviation): FEV1 0.58 l (0.25 l) 22.5%(10) predicted, age 65 (5.3), PaCO2 8.75 (1.3), PaO2 7.4 (1.9), pH 7.4 (0.05), BMI 27 (6.1). Blood gases at discharge following initiation of long term NIV were significantly improved (p<0.05) with PaO2 8.17 (0.9), PaCO2 7.3 (0.8). These improvements were maintained over subsequent follow up at 6–9 months PaCO2 6.75 (0.83), PaO2 8.1 (1.3). Median survival was 29 months (CI 0.37 to 4.4) with one year survival 64% and two year 53%.
Discussion: Randomised controlled trials of long term NIV have so far provided little evidence of survival benefit; however, poor compliance, patient selection, a lack of monitoring to confirm correction of nocturnal hypoventilation, and the use of relatively low ventilatory pressures may explain these findings. In comparison with other published series our cohort of patients with poor prognostic features have relatively good survival and sustained improvements in arterial blood gas measurements. Long term domiciliary NIV may have a role in the management of these severely hypercapnic patients in whom long term oxygen treatment alone worsens hypercapnia and survival is poor.
S57 EVALUATION OF THE TRANSER OF A CHRONIC VENTILATRY FAILURE SERVICE FROM A NATIONAL TO A LOCAL CENTRE
J. M. Palmer, P. D. Hughes. The Chest Clinic, Derriford Hospital, Derriford, Plymouth, UK
Introduction: Before April 2004 patients from both Plymouth Hospitals Trust (PHT) and South Devon Health Care NHS Trust (SDHCT) with chronic ventilatory failure (CVF) needed to undertake a 500 mile round trip to the Royal Brompton Hospital (RBH) in London to be set up on non-invasive ventilation (NIV). In April 2004 a CVF service was established by PHT to cater for and support the needs of patients requiring NIV from the two Trusts. A respiratory physician and a full time CVF specialist nurse lead the service which is able to provide cover from 8am until 6pm 7 days a week 365 days a year.
Methodology: The evaluation took place over a two month period to ascertain if the service was of benefit to the two acute NHS Trusts and to the patients it managed. The data were obtained using retrospective audit and a patient satisfaction questionnaire.
Results: Nineteen patients commenced NIV for CVF in the first year. Fourteen continue on NIV (1 with a diagnosis of COPD could not tolerate nasal ventilation long term, 2 with COPD died, and 2 with motor neuron disease died). Of those who continue 67% (n = 9) had an inpatient stay as part of the set up. For the Plymouth patients (n = 12) the average length of stay per set up was 4.7 days. As the service became established the average length of stay fell to 1.4 days as domiciliary set ups became the norm. Before 2004, the average wait for a bed at the RBH for a PHT inpatient on an acute medical ward was 10.8 days from referral with one patient “blocking” an acute medical bed for 32 days. Therefore transferring the service to Plymouth saved approximately 85 bed days (circa £11,000). The patient satisfaction survey showed that 68% (n = 15) of ex RBH patients either agreed or strongly agreed that they now feel better supported. No one said they felt less supported. In addition 73% (n = 16) of ex RBH patients either agreed or strongly agreed that they feel more confident that the service is now run from their local DGH. One respondent said she felt less confident with the service. This related to the perceived availability of tests, etc at the RBH. The 13 new patients who responded all either agreed or strongly agreed that they felt well supported by the local service. Furthermore while being set up 60% (n = 3) of patients set up solely at home including one in SDHCT stated that they strongly agreed that they were more than adequately supported through the setting up procedure.
Conclusion: The transfer of the CVF service from a national to a local centre has proven to be successful from both an organisational and patient perspective. The organisation has benefitted from reduced bed days and a cheaper service whilst patients feel better supported and more confident.
Novel molecular mechanisms of lung disease
S58 ADAM33 IN EMBRYONIC LUNGS
H. M. Haitchi1, F. Bucchieri1, R. M. Powell1, N. A. Hanley2, D. I. Wilson2, S. T. Holgate1, D. E. Davies1. 1The Roger Brooke Laboratories, Division of Infection Inflammation & Repair; 2Human Genetics, University of Southampton, Southampton, UK
Rationale: ADAM33 is an asthma susceptibility gene with polymorphic variation that is strongly associated with asthma and bronchial hyperresponsiveness (
). Single nucleotide polymorphisms (SNPs) in ADAM33 also predict impaired lung function in COPD (
) and in young children (
). To study the link between maternal atopy and development of asthma, we postulated that ADAM33 is expressed during embryonic lung development and is affected by Th2 cytokines.
Methods: Mouse lungs were harvested at embryonic day (ED) 11–19 and human embryonic lungs (HEL) (7–10 weeks) were collected following the Polkinghorne Committee guidelines after informed consent and ethical approval. Lung explants were cultured in vitro for 3–18 days±interleukin (IL)-13. Samples were processed for mRNA, protein, and image analysis.
Results: ADAM33 mRNA increased during embryonic development in mouse and human lungs. ADAM33 splice variants were detected in HELs but the β-isoform and the metalloprotease domain were rare. Western blotting confirmed the presence of multiple isoforms of ADAM33. Immunomicroscopy showed ADAM33 around alpha smooth muscle actin (αSMA) positive tubular structures within the undifferentiated mesenchyme. In vitro, ADAM33 and αSMA mRNA expression in ED12 lung explants cultured with IL-13 were increased after 48 hours (p = 0.015) and 72 hours (p = 0.026) compared with lungs cultured in medium alone. HELs cultured for 6, 12, and 18 days in the presence of IL-13 showed cystic phenotypic changes compared with medium alone.
Conclusion: The expression of ADAM33 in developing embryonic lungs and its interaction with IL-13 suggests a key role in airway modelling that may contribute to the pathogenesis of chronic lung disease.
Supported by: Asthma, Allergy and Inflammation Research Charity (AAIR), UK; The British Lung Foundation, UK.
S59 FUNCTIONAL ANALYSIS OF GSTP1 HAPLOTYPES ON CELL GROWTH AND APOPTOSIS IN NIH3T3 FIBROBLASTS
S. Holley, A. Fryer, W. Carroll, R. Strange, P. Hoban, W. Lenney. Institute of Science and Technology in Medicine, University of Keele, University Hospital of North Staffordshire, Stoke-on-Trent ST4 7QB, UK
Introduction: We have proposed that GSTP1 genotype is an important determinant of lung development and repair in childhood. Polymorphic variants of GSTP1 have been associated with susceptibility and outcome in asthma. GSTP1 variants are associated with lung function in children (Carroll et al. 2005) and with bronchial hyperresponsiveness in children and adults with atopic and occupational asthma (Fryer et al. 2000). Further, GSTP1 knockout mice have larger lungs and cells from these mice have significantly faster doubling times than those from wildtype mice (Ruscoe et al. 2001). The GSTP1 protein is important for the detoxification of the products of oxidative stress and in the regulation of cell proliferation and apoptosis. However, few data exist on the effects of GSTP1 polymorphism on these processes. We have used a cell culture based system to determine the effect of GSTP1 polymorphism on cellular growth and apoptosis under oxidative stress.
Methods: Using site directed mutagenesis on a human GSTP1 cDNA clone we constructed inducible GSTP1*A (Ile105-Ala114) and GSTP1*C (Val105-Val114) haplotypes in the LacSwitch expression system. NIH3T3 cells were stably transfected and inducible expression of GSTP1*A and GSTP1*C in isolated clones was confirmed by western blotting. The effect of GSTP1 alleles on cell growth and apoptosis, with and without the presence of oxidative stress (100 μM hydrogen peroxide, H202) was examined. Three clones of each haplotype were analysed.
Results: In the absence of H202, induction of GSTP1*A increased the cell doubling time by 3.85 (SD 0.43) hours and induction of GSTP1*C increased cell doubling times by 1.10 (SD 0.60) hours, compared to non-induced cells. In the presence of oxidative stress, cell doubling times were increased, in GSTP1*A clones by 2.80 (SD 1.08) hours but were decreased in GSTP1*C clones by 0.40 (SD 0.60) hours compared to non-induced cells. We also observed protection from apoptosis following exposure of the cells to oxidative stress. Upon induction of GSTP1 in these cells, apoptosis was significantly reduced in cells expressing GSTP1*A (13.44 (SD 1.17)%) and expressing GSTP1*C (12.82 (SD 2.37)%) compared to non-induced cells. Survival analysis with increasing concentrations of H202 also demonstrated that induction of GSTP1 expression led to an increase in the IC50 value by 49.97 μM and 40.77 μM in cells expressing GSTP1*A and GSTP1*C respectively compared to non-induced cells.
Discussion: Our data confirm that GSTP1 expression reduces cellular growth and protects against apoptosis. The differential effects on cellular growth and apoptosis observed with different GSTP1 variants demonstrate two mechanisms by which GSTP1 polymorphism might influence lung development during pre- and postnatal lung growth or may reduce the lung’s ability to repair itself during later life.
S60 ACTIVATION OF PAR1 BY FXA INDUCES FIBROBLAST TO MYOFIBROBLAST DIFFERENTIATION
M. A. Krupiczojc, C. J. Scotton, G. J. Laurent, R. C. Chambers. Centre for Respiratory Research, University College London, UK
Introduction: Differentiation of fibroblasts into highly synthetic and contractile, alpha smooth muscle actin (αSMA) positive myofibroblasts plays a central role in driving the fibrotic response to lung injury. Coagulation proteinases such as Factor Xa (FXa) induce a range of cellular effects via proteolytic activation of proteinase activated receptors (PARs). FXa is a potent fibroblast mitogen and can activate either PAR1 or PAR2 depending on cell type. The aim of this study was to examine the effect of FXa on fibroblast differentiation and to characterise the signalling receptor involved.
Methods: Primary human adult lung fibroblasts (pHALF), human fetal lung fibroblasts (HFL-1) and wild type murine lung fibroblasts (WT) were incubated with FXa, TFLLR-NH2, and FTLLR-NH2 (synthetic PAR1 agonist and corresponding control peptide respectively). αSMA expression was assessed by western blotting and results normalised relative to ERK expression for protein loading. αSMA fibre formation was visualised by standard immunocytochemistry protocol using chamber slides.
Results: At 36 hours, FXa and TFLLR-NH2 both significantly induced αSMA expression and fibre formation by approximately sevenfold in HFL-1 (p<0.01) and WT (p<0.01) fibroblasts relative to control media and FTLLR-NH2 treated cells. This effect of FXa on αSMA expression was much more pronounced in pHALF (15-fold, p<0.01) than obtained in HFL-1 and WT fibroblasts. The effect of FXa was mimicked by TFLLR-NH2 but the maximal response obtained was much reduced (2.5-fold, p<0.05). Assessment of the effect of antistasin, a synthetic peptide that mimics the core inhibitory region of leech antistasin, on αSMA expression revealed that FXa catalytic activity is necessary for the induction of αSMA expression. This effect occurred largely independent of thrombin activity as assessed by hirudin inhibition. Preincubation of pHALF with the selective PAR1 antagonist (RWJ-58259, PRD, JnJ) blocked FXa induced αSMA expression in a dose dependent manner with a complete inhibition obtained at a 4 μM concentration.
Conclusion: This study shows for the first time that FXa induces fibroblast to myofibroblast differentiation via the proteolytic activation of PAR1. PAR1 blockade may represent an attractive target for therapeutic intervention in a number of respiratory conditions associated with local FXa signalling and excessive matrix deposition.
S61 PAR1 SIGNALING IN LUNG EPITHELIAL CELLS INDUCES THE EXPRESSION OF CCL2/MCP-1 AND CTGF
R. H. Johns, C. J. Scotton, G. J. Laurent, R. C. Chambers. Centre for Respiratory Research, University College London, UK
Persistent local activation of the coagulation cascade is characteristic of fibroproliferative lung disorders such as the acute respiratory distress syndrome (ARDS) and idiopathic pulmonary fibrosis (IPF), and the bleomycin animal model of lung injury and fibrosis. Furthermore, strategies aimed at blocking coagulation attenuate experimentally induced lung fibrosis. Thrombin is able to activate its major cellular receptor, proteinase activated receptor-1 (PAR1) to induce the production of a number of potent proinflammatory and profibrotic mediators. Expression of PAR1 is increased in many fibrotic conditions, and we have recently reported that deficiency of PAR1 affords protection from bleomycin-induced lung inflammation and fibrosis in mice (Howell & Johns et al. Am J Pathol 2005). This protection is associated with significant reductions in lung levels of monocyte chemoattractant protein-1 (CCL2/MCP-1), connective tissue growth factor (CTGF), and transforming growth factor-beta-1 (TGF-β1). Given that bleomycin-induced lung fibrosis results from initial widespread epithelial injury, and that persistent “idiopathic” alveolar epithelial injury is considered to be integral to the pathogenesis of IPF, this study aimed to examine the potential relevance of PAR1 and its activation on lung epithelial cells.
Immunohistochemistry demonstrated a dramatic increase in parenchymal PAR1 immunostaining seven and 14 days following bleomycin injury in wildtype mice; and this was particularly evident on type-II alveolar and bronchial epithelial cells. In order to examine whether PAR1 activation could influence gene expression of proinflammatory and profibrotic mediators by epithelial cells, human alveolar epithelial A549 and human bronchial epithelial BEAS-2B cells were exposed to either thrombin, the specific PAR1 agonist peptide TFLLR, or FTLLR control peptide in vitro. Total RNA was isolated, reverse transcribed, and subjected to real-time RT-PCR analysis. Maximal CCL2/MCP-1 expression in response to thrombin and TFLLR was increased in A549 cells by 2.29 (SD 0.17) and 4.46 (SD 1.09) fold; and in BEAS-2B cells by 19.2 (SD 1.93) and 20.2 (SD 4.97) fold respectively (p<0.05). Maximal CTGF expression in response to thrombin and TFLLR was increased in A549 cells by 5.36 (SD 0.66) and 5.05 (SD 0.52) fold; and in BEAS-2B cells by 12.1 (SD 0.52) and 10.2 (SD 1.06) fold respectively (p<0.05). Maximal TGF-β1 expression in response to thrombin and TFLLR was increased in A549 cells by only 1.61 (SD 0.17) and 1.44 (SD 0.07) fold respectively (p<0.05); and was not increased in BEAS-2B cells. The FTLLR control peptide had no effect on expression. Taken together these data support the notion that following lung injury, epithelial cells may represent an important source of PAR1 inducible proinflammatory and profibrotic mediators. Strategies aimed at blocking epithelial PAR1 activation may thus represent an important new opportunity for the treatment of fibroproliferative lung disorders.
S62 HUMAN HERPES VIRUS-8 K5 PROTEIN REDUCES CELL SURFACE EXPRESSION OF BONE MORPHOGENETIC PROTEIN TYPE II RECEPTOR
T. K. Jeffery, P. D. Upton, H. J. Durrington, S. Hoer, P. J. Lehner, N. W. Morrell. Department of Medicine, University of Cambridge School of Clinical Medicine, Box 157, Addenbrookes Hospital, Hills Road, Cambridge CB2 2QQ, UK
Heterozygous germline mutations in the gene encoding the type II bone morphogenic protein receptor (BMPR2) have been found to underlie many cases of familial and sporadic pulmonary arterial hypertension (PAH). In familial cases low gene penetrance of mutant BMPR2 implies that an additional genetic or environmental event may be required to cause disease. In addition, reduced expression of pulmonary vascular BMPR-II protein is observed in the lungs of patients with idiopathic PAH, whether or not a mutation in the BMPR2 gene is identified. Since human herpes virus-8 (HHV-8) has been identified in the lungs of approximately 60% of cases of idiopathic PAH, we investigated the potential interaction between HHV-8 gene products and BMPR-II function. In common with all herpes viruses, HHV-8 expresses immunoevasion genes, which include K3 and K5. These two gene products are viral ubiquitin E3 ligases, which target a range of endogenous immunoreceptors for ubiquitination and degradation. To investigate the effect of the K5 protein on BMPR-II function we generated Hela cells expressing the K5 gene of HHV-8 and cells expressing a mutated dysfunctional form of K5. Stimulation of these cell lines with the BMPR-II ligand, BMP-4 and subsequent immunoblotting for phosphorylated Smad1/5 protein demonstrated reduced activation of Smad1/5 in K5 cells compared with control and K5 mutant cells. In addition, K5 cells showed reduced activation of a transiently transfected BMP response element reporter gene. To determine whether the K5 antigen affected BMPR-II receptor expression we compared radioligand binding of 125I-BMP4 on control and K5 cell lines as a measure of cell surface BMP receptors. 125I-BMP4 binding in K5 cells was reduced to 33.9 (SD 5.8)% of that in control cells.
Ongoing experiments are testing whether K5 reduces BMPR-II expression through ubiquitination and degradation. Our results demonstrate that the HHV-8 encoded K5 gene product interferes with cell surface BMPR-II expression and BMP signaling, providing a potential mechanism by which HHV-8 may play a role in the pathogenesis of PAH. We speculate that HHV-8 infection may contribute to a critical reduction in BMPR-II signaling, which predisposes to abnormal vascular cell proliferation in the pulmonary circulation and pulmonary hypertension.
Funded by the British Heart Foundation.
Bacterial infection: bench to bedside
S63 THE PULMONARY INNATE IMMUNE RESPONSE TO PSEUDOMONAS AERUGINOSA INFECTION IN HUMAN LUNG TRANSPLANT RECIPIENTS
R. Anderson1, P. S. Hiemstra1, I. Forrest2, D. Murphy2, C. Ward2, G. Johnson2, D. Proud3, J. Lordan2,4, K. Gould4, P. A. Corris2,4, A. J. Fisher2. 1Pulmonology Department, Leiden University Medical Centre, the Netherlands; 2Applied Immunobiology and Transplantation Research Group, University of Newcastle Upon Tyne; 3University of Calgary, Alberta, Canada; 4Cardiopulmonary Transplant Unit, Freeman Hospital, Newcastle Upon Tyne, UK
The antimicrobial peptides (AMPs) are a family of cationic peptides, characterised in humans by the cathelicidin hCAP-18/LL-37 and the alpha and beta defensins. These constitute part of the lungs’ first line of defence against microbial invasion. As well as their powerful antimicrobial properties, AMPs exert effects which control the extent of the immunological response to infection such as chemotaxis of inflammatory cells, activation of dendritic cells and orchestration of epithelial cell proliferation and repair.
Airway colonisation and infection with pseudomonas aeruginosa (PA) is associated with progressive airway damage in chronic lung disease. However, early after lung transplantation, PA infection is commonly seen in recipients with structurally normal lungs. The relation between early PA infection and the pulmonary innate response is poorly understood and in vivo data are lacking. We hypothesised that PA infection would activate the pulmonary innate immune response and in particular increase expression of AMPs in the airways.
Seventy lung transplant recipients were investigated with bronchoalveolar lavage (BAL) as part of post-transplant surveillance within one year of transplantation. BAL was sent for formal microbiological culture for bacteria, fungi, and viruses. Levels of hCAP-18/LL-37 and hBD-2 were measured in the acellular component of BAL using established ELISAs. 16 of the recipients had positive microbial cultures, 12 had PA isolated, four had other organisms Aspergillus fumigatus (2), Stenotrophomonas maltophilia (1), and Staph aureus (1), and in 54 there were no pathogens isolated. Levels of LL-37 were significantly higher in those with PA infection, median 9 (range 1–34) ng/ml compared to those with no pathogens 1 (0–38) ng/ml, p = 0.001. hBD-2 levels were similarly increased in recipients with PA isolated, median 1019 (0 to 3490) pg/ml compared to those with no pathogens isolated 201 (0 to 2500) pg/ml, p = 0.002. These differences persisted when patients with acute or chronic rejection were excluded from the analysis.
In conclusion, identification of PA in the airways of lung transplant recipients is associated with increased expression of key elements of the innate immune response. The increased AMP expression enhances local resistance to infection, but may also contribute to progressive airway injury in PA infected lung transplant recipients. Supported by a European Respiratory Society Fellowship to R Anderson.
S64 PROGNOSTIC FACTORS IN HIV ASSOCIATED PNEUMOCYSTIS JIROVECII PNEUMONIA
R. F. Miller1, E. Allen1, S. G. Edwards2. 1Centre for Sexual Health and HIV Research, RFUCMS, University College London, UK; 2Camden PCT, Mortimer Market Centre, London, UK
Background:Pneumocystis jirovecii is the cause of Pneumocystis pneumonia (PCP) in humans. The aim of this study was to identify prognostic factors associated with a poor outcome in HIV infected patients presenting with PCP.
Methods: Between 01 June 1985 and 31 May 2005 468 patients (444 men) presented to an inner London specialist HIV/AIDS treatment centre with 516 consecutive episodes of bronchoscopically confirmed PCP; data were incomplete/missing for six patients. In 409/462 patients (88.5%) PCP was their AIDS defining event. For each patient, by case note review, details of age, disease severity at presentation (Pa02, breathing room air), presence of intercurrent medical problems (alcoholism, psychosis, diabetes, ischaemic heart disease, etc), laboratory results (T-helper cell (CD4) count, haemoglobin, peripheral blood white blood count (WBC)), presence of co-pathology (either cytomegalovirus (CMV) or bacterial infection) in bronchoalveolar lavage (BAL) fluid), complications (pneumothorax, need for mechanical ventilation on the intensive care unit (ICU)) episode of PCP (first, second, or third) and outcome were recorded.
Results: Overall mortality was 13.6% and did not change with time; mortality 1985–95 = 14% (before the availability of highly active antiretroviral therapy [HAART], compared to 1996–2005 (the era of HAART), mortality = 12.5%; p = 0.4. In univariate analysis, factors associated with a poor outcome were; increasing patient’s age (p = 0.002), presence of comorbidity (p = 0.001), low haemoglobin (p<0.001), low CD4 count (p = 0.005), hypoxaemia (p<0.001), need for ICU (p<0.001), and development of pneumothorax (either secondary to bronchoscopy or to mechanical ventilation) (p<0.001). In multivariate analysis all these factors, except CD4 count, remained significant. Factors not associated with poor outcome were an elevated peripheral blood WBC, (p = 0.08), presence of co-pathology in BAL fluid (co-infection with CMV (p = 0.34) or bacteria (p = 0.38)) and episode of PCP (first, compared to subsequent episodes) (p = 0.33).
Conclusions: These data serve to inform clinicians about prognostic factors which are associated with a poor outcome from HIV associated PCP—namely older patients presenting with PCP who have comorbidity, who have anaemia and low CD4 counts (the latter two being surrogates of undiagnosed HIV infection), or who are hypoxaemic at presentation or develop a pneumothorax, either at bronchoscopy or while being ventilated on ICU.
S65 CASE MIX AND OUTCOME FOR ADULTS WITH COMMUNITY ACQUIRED PNEUMONIA ON THE INTENSIVE CARE UNIT: ANALYSIS OF THE ICNARC DATABASE
M. A. Woodhead1, C. Welch2, D. Harrison2, G. J. Bellingan3, J. G. Ayres4. 1Manchester Royal Infirmary; 2Intensive Care National Audit and Research Centre; 3University College, London; 4University of Aberdeen, UK
Background: Studies of CAP in the ICU are usually small and confined to single institutions. We used a large prospectively collected database to analyse case mix and outcome.
Methods: Data were extracted for 301 871 adult ICU admissions between 1995 and 2004 from the Case Mix Programme of this national comparative audit database covering 172 intensive care units. Cases were identified if pneumonia was the ultimate primary reason for ICU admission. CAP was identified by exclusion of potential nosocomial pneumonias (surgical admissions, those transferred from other ICUs only after two days) and those with a history of immune compromise. Admissions between 1995–99 and 2000–04 were compared.
Results: 17 869 cases of CAP, (5.9% of all ICU admissions), were identified. 59% of cases were admitted to the ICU less than 2 days, 21.5% between 2 and 7 days, and 19.5% only after 7 days after initial hospital admission. 57.5% of cases were male, with 16.5% being aged <45 and 24% >74. The number of CAP ICU admissions rose annually from 12.8/unit in 1996 to 29.2/unit in 2004 (p<0.001). The proportion of admissions from other hospitals (15%) did not change., but admission within the same hospital from HDU (6.9 to 11.9%) and A&E (14.8 to 16.8%) rose (p<0.001). Between the two periods there was a rise in those aged >74 (18.5 to 26.1%; p<0.001) and mean APACHE II score (6.83 to 6.91; p<0.001), and a fall in past history of severe respiratory problems (8.7 to 6.4%; p<0.001), renal replacement therapy (1.6 to 1.2%; p<0.01), steroid treatment (3.4 to 2.8%; p<0.05), those sedated and paralysed at admission (50.2 to 40.4%; p<0.001), CPR prior to admission (7.5 to 5.5%; p<0.001), and septic shock (7.3 to 6.6%; p<0.001).
ICU mortality was 34.9% and ultimate hospital mortality 49.4%. Death rates rose slightly between the two periods (ICU mortality 33 to 35.7%; p<0.001; hospital mortality 47.7 to 50.1%; p<0.005). Mortality was 46.3% in those admitted to the ICU <2 days after admission rising to 50.4% in those admitted at 2–7 days and 57.6 in those only admitted after 7 days in hospital (p<0.001). Median length of stay in the ICU was: survivors 6 (3–14) days, non-survivors 4 (1–10) days, and in hospital was: survivors 30 (17–53) days, non-survivors 12 (4–26) days. Only hospital stay in survivors changed between the two periods (28 (16–51) to 31 (17 to 55); p<0.001).
Conclusions: CAP makes up a small, but significant and rising, proportion of ICU admissions. Survival of over half of all cases vindicates the use of ICU in CAP but the mortality remains unacceptably high, especially in those admitted later in their hospital stay.
S66 LEGIONELLA URINARY ANTIGEN TESTING: WORTH ITS “WAIT” IN GOLD
J. E. Kirkcaldy1, T. C. Boswell2, J. T. Macfarlane1, S. Gill3. 1Clinical Respiratory Medicine; Microbiology; 2Clinical Audit; 3Department, Nottingham City Hospital, UK
Introduction: Legionella urine antigen (LdAg) testing has been widely adopted to aid diagnosis and management in patients with community acquired pneumonia (CAP). BTS national guidelines recommend testing all patients on admission with severe CAP, and those where the clinical or epidemiological features, or response to therapy may suggest legionella infection.
Aims: To determine: whether Legionella urinary antigen is requested according to guideline recommendation and which team members request testing; how promptly testing is carried out and results made available; the positive diagnostic yield and whether testing alters management; and the cost of inappropriate testing.
Method: Retrospective case note review of all adult medical patients who had LdAg testing requested over a six month period (4/9/03 to 4/3/04) at Nottingham City Hospital.
Results: Notes were available for 158 of the 162 patients who had a LdAg test performed and 80 (51%) of LdAg test requests were inappropriate, according to guidelines. The test was requested most commonly by SHOs (66), followed by consultant (35), SpR (20), and PRHO (10); (27 unknown). Inappropriate requests were made equally by clinicians of all grades 28/158 (18%) test requests were made electronically and the rest by hand written generic microbiology request forms. The median total delay between requesting the test and receiving the result was six days (range 1–17). Within this, the delay between request and the lab receiving the sample was one day (range 0–9); the rest was within the lab. The delay was greater for patients testing negative. Only 4/158 (3%) tests were positive for three patients (one duplicate test—all fell within guideline indication for testing) and no test results altered antibiotic management. Results were often available only near the end of, or after antibiotic course had completed. The annualised cost to our hospital of inappropriate testing for medical patients was around £2240 for reagents alone.
Conclusions: Cost of inappropriate requests could be reduced by better education of clinicians regarding indications for testing and by mandatory electronic requesting enabling restrictions to be placed on the ordering process. As current CAP guidelines recommend a regimen that covers legionella infection for all hospitalised patients, a faster turn round time would be needed for negative results to allow “step down” of initial antibiotic management.
S67 WHY ARE ANTIBIOTICS USED SO FREQUENTLY FOR ACUTE BRONCHITIS: CAN LESSONS BE LEARNT FROM THE PAST?
J. T. Macfarlane1, M. Worboys2. 1Clinical Respiratory Medicine, Nottingham City Hospital; 2CHSTM Wellcome Unit, Manchester University, UK
Antibiotics are prescribed for most adults with acute bronchitis (AB), even though evidence suggests they contribute little to recovery for the majority. Before antibiotics were freely available, AB was recognised as a common, usually self limiting condition and treated symptomatically. Yet by the late 1950s, over 80% patients were receiving antibiotics, which accounted for over a quarter of total community prescribing costs. Factors influencing this change have been examined. At that time, AB was the commonest cause of GP consultation especially in winter, with about 1 million sufferers annually. This placed a heavy demand on GPs who had seen a marked increased workload with the free NHS after 1948, with lists up to 5000 patients and up to 50 surgery and 30 home visits daily—higher, particularly for AB, during the large ‘flu epidemics which occurred every 2–3 years during the 1950s, and also the London smogs. In such circumstances, prescribing the new “wonder drugs” was quicker for the GP and welcomed by the patient, when compared with the traditional bed rest, cough mixtures, bronchitis tent, and steam kettle. Although the 1947 Penicillin Act had prohibited direct advertising, there was increasing public awareness of and demand for antibiotics. Expert opinion emphasised the importance of bacterial infection as a cause of AB and the need to prevent secondary infection (the importance of viral infections not being shown until the 1961–64 MRC studies). From 1949, Penicillin G became increasingly available but, being poorly absorbed, was largely given by inhalation or injection, which limited its community use to serious bedbound cases. However with the availability of newer, oral antibiotics (Chloramphenicol 1951, Aureomycin/Terramycin 1954, Tetracycline 1955, Penicillin V 1959), serial editions of popular medical textbooks and the National Formulary were increasingly recommending penicillin early even in milder cases and a second antibiotic if that “failed”, encouraged perhaps by the recognition of “atypical pathogens”. GPs were under increasing pressure from the expanding pharmaceutical industry, which spent 12% of sales income on promoting their proprietary drugs. In January 1962, the BMJ had 33 full page antibiotic adverts. In 1947, only 7% of scripts were for proprietary products compared with 48% by 1957; the 1958 Hinchcliffe Committee identified antibiotics as a major drug cost pressure. GP numbers had increased by about 20% but new GPs were ill equipped to manage common self limiting conditions such as AB, only having trained in hospital where antibiotics were used commonly, and they relied on drug representatives for education on new drugs—there being no vocational training.
Conclusion: Diverse social, political, medical, educational, pharmacological, commercial, and economic drivers in the 1950s contributed to the current overuse of antibiotics for AB.
Study supported by Wellcome Trust Award.
How can we improve patient education?
S68 ARE TELEPHONE CONSULTATIONS USEFUL IN RESPIRATORY OUTPATIENTS?
N. J. Roberts, M. R. Partridge. Imperial College London, NHLI Division at Charing Cross Hospital, St Dunstans Road, London W6 8RF, UK
Telephone consultations have been shown to be an effective tool in primary care. We have studied the usefulness and practicality of telephone consultations with patients with respiratory illnesses in secondary care.
448 sequential patients attending a follow up appointment in three different respiratory clinics in a central London teaching hospital were evaluated for suitability for a telephone consultation as an alternative to a face to face appointment. 157 of these patients were excluded because they were being discharged or referred elsewhere or they were not being seen again for 12 months. Of the remaining 291 patients, a total of 98 patients (33.7%), were thought to be suitable for alternating telephone and face to face consultations. Reasons for non-suitability: patient preferred to see the doctor (32/193, 16.5%); patient needs clinical investigations or examination (63.7% 123/193), language, hearing, or learning difficulties (15/193, 7.7%). Only one patient stated that they did not have a telephone. Those thought to be suitable included those with asthma, COPD, sarcoidosis, bronchiectasis, and unexplained cough.
60/98 patients (61.2%) were available at the time of the planned telephone consultations but 28/98 (28.6%) were not. 18 of these 28 patients also failed to attend a subsequent planned face to face consultation. (10 patients have still to receive their first telephone consultation). Of the 60 who have undergone a telephone consultation 63% were female with a mean age of 57 (SD 18.7) years. 25% of the telephone consultations were carried out with the patient at their workplace and 63% at home. The consultation started within a mean of 6 minutes of the stated appointment time and lasted for a mean of 8.8 (SD 3.5) minutes. In three cases (3/60, 5%) it was necessary to expedite face to face follow up as a result of the telephone consultation either because of the content of the call or because the consultant found it difficult to assess the patient over the telephone. Patient satisfaction with the telephone consultation and their subsequent face to face consultation has been assessed using a patient enablement instrument and the MISS-21 medical interview satisfaction scale adapted with the originators advice for telephone consultation.
A third of those attending respiratory outpatient clinics may be suitable for alternating face to face and telephone consultations. The latter are usually some what shorter than face to face consultations but the fail to be available rate is high.
We acknowledge with thanks the assistance of Drs M Sridhar, R Coker, and A Cummins in this study.
S69 HOW USEFUL DO PATIENTS FIND POST CONSULTATION LETTERS?
N. J. Roberts, M. R. Partridge. Imperial College London, NHLI Division at Charing Cross Hospital, St Dunstans Road, London W6 8RF, UK
As part of the NHS plan it was suggested that all patients should receive copies of the letters sent to their general practioner (GP) following outpatient consultations.1 The former Secretary of State for Health extended this proposal, suggesting that patients should have a specific letter written to themselves, after a hospital consultation.2 The aim of this study was to send patients attending five respiratory and cardiology consultants at Charing Cross Hospital, a copy of the letter sent to their GP plus a specific letter to themselves and to assess the usefulness and comprehensibility of each. Out of 105 patients, 84 consented (80%) and were sent both types of letter after their attendance. Patients completed a patient enablement instrument (PEI), returned both letters circling any misunderstood items, and stated a preference for either the GP letter, patient letter, or both (61 completed both PEI, questionnaire and returned the letters; two returned the letters only and one returned PEI and questionnaire only). The letters were analysed for dictation time, Flesch Reading Ease Score, Flesch-Kincaid Grade Level, and word count. GP letters took significantly longer to dictate compared to patient letters. (GP letter 3.28 minutes (SD 2.2), n = 81; patient letter 2.57 (SD 1.43), p = 0.019, n = 82). The Flesch Reading Ease Score was significantly higher in the patient letters (55.44 (SD 9.26), n = 84 (patient) v 49.76 (SD 9.1), n = 84 (GP), p<0.001). The GP letters were significantly longer than the patient letters and patients were significantly more likely to circle more items in the GP letters (p<0.001). 16/63 (25.4%) circled 1–5 items in the patient letters, whereas 31/63 (49.2%) circled 1–12 items on the GP letter. 36/62 patients (58%) would like to receive both letters, 13/62 (21.6%) would prefer the GP letter, and 13/62 (20%) wanted only the patient letter. The Flesh Reading Ease Score indicates that the patient letters were easier to read, and significantly shorter. 72 GPs were sent both letters for comparison and asked their views; 45 replied (62.5%). General themes were that there was not enough clinical information in the letters to patients for them to act as a replacement for GP letters and the GPs preferred the letters written to them. In conclusion, GPs still need their own letter and the majority of patients would like both letters but this would involve time and expense. A compromise might be to simplify the content of GP letters and to provide a speciality specific glossary for patients and to send occasional special letters to patients where the complexity of advice merits it.
We acknowledge with thanks the assistance of Drs Baker, Cummin, Fox, and Sridhar.
1
2
S70 ASSESSING RESPIRATORY PATIENTS KNOWLEDGE OF THEIR INHALED THERAPY
C. Chamberlain. RD&E (Wonford), Devon, UK
Aim: To explore respiratory patients knowledge of their inhaled therapy and to assess the contribution of regular medication review using a questionnaire.
Method: Data were collected from consenting patients using a questionnaire. The target group were patients presenting to respiratory nurse clinics within the medical outpatient setting. The data collection took place over a period of three months (September to November 2004). Questions included diagnosis, length of diagnosis, and knowledge of condition. Patients were asked to identify their inhalers, dosages, and any side effects. They were also asked if they had had a recent respiratory review and to identify the staff member who had undertaken this. Respiratory nurses were also asked to check inhaler techniques and patient knowledge of condition.
Results: 56 questionnaires were completed (100%). The mean age of patients was 65 years and the average number of inhalers was three. 56% had been diagnosed over five years, with only 7% being diagnosed within the last year. 74% had had a respiratory review within the last year and 73% of patients recalled medications being discussed. 98% of patients felt they had good/fair knowledge of their condition; however (after clinic consultation) respiratory nurses’ opinion was that only 59% of patients had good knowledge of their condition. 19% were also found to have poor inhaler techniques. Only 56% of inhalers were correctly identified by name, 59% were correctly identified by colour, and 11% were identified by type. The correct treatment regime was identified in 56% of cases but only 4% were aware of possible side effects. 30% of patients also admitted that they forgot their inhalers on occasions.
Conclusion: Despite having been diagnosed for several years and having had a recent respiratory review respiratory patients’ knowledge of their inhaled therapy remains poor when assessed by respiratory nurses but patients themselves believed it to be good/fair. The audit reinforces the fact that that “education is a process and not a single event” (British Thoracic Society/Scottish Intercollegiate Guidelines Network (BTS/SIGN), 2003, p58) and that education should be offered at every opportunity. The questionnaire was completed by a relatively small number of patients and questions were aimed at determining knowledge of inhaled therapy; other concurrent medications were not evaluated.
1
S71 PRIORITY INFORMATION NEEDS IN PARENTS OF CHILDREN WITH ASTHMA: RESULTS FROM A SURVEY USING A PAIRED COMPARISONS APPROACH
G. F. Kerry1, A. L. Caress2, K. Beaver2, A. Custovic1, A. Woodcock1, C. S. Murray1. 1North West Lung Centre, Wythenshawe Hospital, Manchester, UK; 2School of Nursing, Midwifery and Health Visiting, University of Manchester, UK
Background: Having appropriate information is important for parents of children with asthma, but evidence about the information parents would find most useful is lacking. Identifying the topics that are a priority for parents would help in tailoring asthma education.
Methods: A survey was undertaken of parents of children with established asthma attending an outpatient clinic at a district general hospital in the Northwest of England. Data were collected using a structured asthma specific information needs questionnaire, which employed a Thurstonian paired comparisons approach. This consisted of all possible pairings of nine “core information needs”, previously identified in adults with asthma (
), adapted for use with parents of children with asthma.
Results: Parents of 29 children (child’s median age 8.0 years, IQ range 5.1–12.3; median time since asthma diagnosis 3.7 years) completed the survey. Information needs were prioritised as shown in the table (information needs with Thurstone scale values).
Six (20%) respondents were satisfied/very satisfied with their level of information about their current top priority area, while six (20%) were dissatisfied/very dissatisfied. The majority of parents (25/29) were unable to identify additional information needs, while three parents highlighted the need for information on action to take when their child was unwell (that is, an asthma action plan). The majority of parents stated that they would most prefer to receive information from their child’s doctor (22/29) and/or asthma nurse (12/29). Main reasons for this choice were “confidence in their knowledge” and “familiarity with their child’s asthma”.
Conclusion: Further work is required to better understand why parents value specific items. Some parents identified the need for an asthma action plan. A larger study is now required to validate these findings, in particular to establish whether information about self management plans needs incorporating into the instrument.
Abstract S71
S72 LAY ASTHMA EDUCATORS KNOWLEDGE AND CONSULTATION STYLES
C. E. Brown1, E. M. Applegate2, A. L. Caress2, M. R. Partridge1. 1Imperial College London, NHLI Division at Charing Cross Hospital, London, UK; 2School of Nursing, Midwifery & Social Work, University of Manchester, UK
Several studies have shown that despite guidelines recommending self management education for those with asthma, few patients receive such education or written asthma action plans. One reason may be time pressures on healthcare professionals. We are therefore studying whether well trained lay educators can produce outcomes equivalent to that achieved by practice nurses.
15 lay educators were recruited from a diverse background for this multisite project. After an initial two day residential course at the National Respiratory Training Centre (NRTC) they received three follow up NRTC sessions at monthly intervals followed by three monthly troubleshooting sessions with local health professionals. 140 patients have been seen so far by these lay educators and 117 by practice nurses. As part of the mentoring of the advice being given to the patients, all notes and treatment recommendations made by the lay trainers still taking part are monitored, occasional consultations witnessed, and the Asthma Knowledge Questionnaire (AKQ) used at a point 12 months after initial training to assess retention of factual knowledge. The practice nurses seeing patients in the nurse arm of the study underwent identical assessment.
Results for the AKQ for eight nurses and seven lay trainers showed no significant difference. Consultations were observed and monitored according to a semi structured check list looking at length of consultations, use of open ended questions, summarising, checking of understanding, use of jargon, eliciting of fears and concerns, and outside interruptions. Nurse led consultations were shorter than those conducted by lay trainer, and interrupted more by other practice staff, but general style of consultations was almost identical between nurses and lay educators. Patients attending either a lay trainer or nurse also completed the Medical Interview Satisfaction Scale (MISS 21) after the first consultation. Initial analysis of 191questionnaires, from 92 lay and 99 nurse consultations, have shown equivalent results. Mean total score is 99.13 (SD 9.4) for nurses and 101.00 (SD 11.8) for lay educators.
Using lay people to deliver healthcare in one carefully defined subject area is possible and with good training achieves equivalent knowledge transfer, similarity of consultations styles, and equivalent patient satisfaction. Whether patient outcomes are equivalent will only be apparent on completion of the trial.
This study was supported by The BUPA Foundation.
S73 OBSTACLES TO SELF MANAGEMENT IN BRONCHIECTASIS: THE PATIENTS’ PERSPECTIVE
K. Lavery1, B. O’Neill2, J. S. Elborn1,3, J. M. Bradley1. 1Department Respiratory Medicine, Belfast City Hospital, N Ireland; 2Institute of Health and Rehabilitation Sciences, University of Ulster, N Ireland; 3Department of Respiratory Medicine, Queen’s University Belfast, N Ireland
Introduction: The new twenty year regional strategy for health and social care in Northern Ireland, A Healthier Future, reaffirms a commitment to promoting self- management in chronic respiratory disease such as bronchiectasis. The content and method of delivery of self management should give due consideration to the specific requirements of the disease population.
Aims: To identify from a patients’ perspective if they use self management, to identify any perceived obstacles to self management and to determine what support is needed to promote self management.
Methods: A total of thirty two patients with a clinical diagnosis of bronchiectasis attended focus groups. The patients were recruited using purposive sampling from physiotherapy records held at the Belfast City Hospital. Four focus groups were assembled according to gender and age (males and females, aged 18–64 years and males and females aged over 65 years). A follow up questionnaire was used to quantify the findings from the focus groups.
Data analysis: Each of the focus groups were videotaped and subjected to qualitative analysis using the Grounded Theory approach.
Results: Patients perceived they were engaging in some methods of self management relating to self regulation of inhaled therapies, antibiotics, physiotherapy, exercise, and complementary medicine. Perceived obstacles to effective self management included lack of information, disease severity and stability, side effects, health service policies, lack of motivation, and confidence. Patients suggested self management could be promoted through disease specific information and guidance, appropriate policies, and accessibility to healthcare and rehabilitation facilities.
Conclusion: Patients with bronchiectasis are receptive to self management but perceive a number of obstacles to effective self management. Health and social care professionals need to provide information, education, and training for patients and carers to overcome these obstacles to enhance self management of this disease.
Growing old with cystic fibrosis
S74 OSTEOCLAST FORMATION POTENTIAL FROM HAEMATOPOIETIC PRECURSORS IS ALTERED DURING INFECTIVE EXACERBATION IN ADULT CYSTIC FIBROSIS PATIENTS
E. Shead1, C. Haworth2, E. Gunn2, D. Bilton2, M. Scott1, G. Wakley3, J. Compston4. 1Addenbrooke’s NHS Trust, Cambridge, UK; 2Papworth NHS Trust, Cambridge, UK; 3University of Bristol, UK; 4University of Cambridge, UK
Osteoporosis is a disease characterised by low bone mass, bone fragility and an increased fracture risk. Approximately 25% of CF adults have low bone mineral density with CF disease severity the most consistent correlate. Aris et al (AJRCCM 2000) have shown a temporal relation between inflammatory markers and biochemical markers of bone resorption during exacerbations. More recently, Haworth et al have shown interleukin-6 to be an independent predictor of change in bone mineral content over one year in CF adults (Haworth et al. Thorax 2004). Osteoclasts are bone resorbing cells, formed from haematopoietic mononuclear cells and colony forming units (CFU-GM). Formation is controlled by factors which are involved in the inflammatory process. Therefore, increased proliferation and/or differentiation of osteoclasts at times of inflammation (infective exacerbations) may induce a burst of resorptive activity. The aim of this study was to investigate the relation between pulmonary infection and osteoclastogenesis in CF adults by measuring CFU-GM growth and proliferation before (baseline), during (day 1 and 14) and after (day 42) an infective exacerbation treated with intravenous (IV) antibiotics. CFU-GM colonies were cultured in Methocult H4534 (Stem Cell Technologies, France) for 14 days and enumerated visually. Proliferation within colonies was measured using a propidium iodide DNA preparation identifying the dividing cell population by flow cytometry. Thirteen patients (6 male, mean (SD) age 22.8 years (4.0), FEV1 49.1% of predicted, BMI 20.6 kg/m2) were recruited. Patients were in a stable condition (defined as no respiratory exacerbations requiring oral or IV antibiotic therapy for four or more weeks) at baseline. None of the patients had been prescribed oral corticosteroids for at least three months and all patients were colonised with Pseudomonas aeruginosa. Mean colony numbers at each timepoint were: baseline - 12.5, day 1–16.2, day 14–15.5, and day 42–16.6. A one way analysis of variance showed no significant difference between mean colony numbers at each timepoint (p = 0.8045). However, within-patient multiple comparison analysis (Tukey’s) showed significant differences in colony numbers between timepoints (p<0.05) in 10 patients, with the greatest colony growth seen at day 1, decreasing to a level close to baseline by day 42. Proliferation increased significantly at day 1 (p<0.01) and decreased by day 14 (p<0.001) (Tukey’s). Colony number and proliferation were not correlated at any timepoint (p = 0.81) when patients were considered individually or as a group. The increase in CFU-GM formation in CF patients suggests the presence of stimulatory factors and/or lack of inhibitory factors in serum during infective exacerbations. This may lead to proliferation of cells formed from CFU-GMs, including osteoclasts, resulting in increased bone resorption and bone loss during periods of pulmonary infection.
S75 LONG TERM EFFECTS OF DIABETES AND INSULIN TREATMENT ON CLINICAL STATUS AND LUNG FUNCTION IN CYSTIC FIBROSIS
K. Mohan, K. Israel, H. Miller, P. Dyce, M. J. Ledson, M. J. Walshaw. Adult CF Unit, The Cardiothoracic Centre, Liverpool UK
Introduction: Cystic fibrosis related diabetes (CFRD) is associated with worsening clinical status and increased mortality in CF patients, and deterioration in pulmonary function and body mass index (BMI) has been shown to occur up to five years prior to its onset. Although treatment with insulin confers short term clinical advantage, few studies have compared its long term effect on clinical outcome.
Methods: To investigate this further, we looked at spirometry (% predicted), nutritional state and number of hospital admissions for a period of up to five years before and three years after the diagnosis of CFRD and the institution of insulin therapy in 38 patients (mean age 21.5 years (range 11–39), 13 male) in our large CF unit, where 53 of 172 patients (30.8%) have CFRD.
Results: In the cohort, prior to CFRD diagnosis the mean rate of deterioration in FEV1 was –2.27% per year (range – 0.07 to –9.11), FVC –1.97% per year (range –0.02 to –10.51), and BMI – 0.02% per year (range –0.04 to –1.74). At diagnosis, the mean FEV1 was 55.45 (range 24–112), mean FVC 70.35 (range 29–112), and mean BMI was 19.42 (range 15.32–24.51). At three months following CFRD diagnosis and institution of insulin therapy, there was a significant improvement in FEV1 (mean 61.00, p<0.0001), FVC (mean 77.31, p<0.0001), and BMI (mean 20.33, p<0.001). This improvement in FEV1 and FVC was not maintained at one year (means 57.03, p = 0.24 and 74.01, p = 0.08 respectively). Thereafter, FEV1 declined at a rate similar to that pre insulin treatment (–3.72% per year, p = 0.29), but there was a trend for the rate of deterioration in FVC to slow post treatment (–0.95 per year, p = 0.49). The mean post treatment FEV1 returned to pretreatment baseline 18 months later. The improvement in BMI was maintained at one year post diagnosis (mean 20.39, p<0.001), and furthermore there was a trend for improvement in BMI for up to three years following treatment of CFRD compared to pre-treatment (mean BMI change 0.06 per year, p = 0.83). There were no significant changes in the number of hospital admissions before (1.62 per patient per year) and after (1.63 per patient per year) the onset of diabetes.
Conclusions: Thus, we have shown that insulin treatment reverses and slows the rate of decline in BMI at three years after the onset of diabetes. Although a significant improvement in lung function was noted at three months, this effect was not sustained in the longer term, but insulin treatment did appear to “stabilise” FEV1 for an average of 18 months. This study reinforces the importance of encouraging patients with CFRD to take their insulin therapy.
S76 RIGHT VENTRICULAR DIASTOLIC FUNCTION AND C-REACTIVE PROTEIN CIRCULATING LEVELS CORRELATE TO SURVIVAL IN ADULTS WITH CYSTIC FIBROSIS
R. Sabit1, A. Ionescu2, A. A. Ionescu1, C. E. Bolton1, L. S. Nixon1, D. J. Shale1. 1Respiratory Medicine, Cardiff University, Llandough Hospital, Cardiff, Wales; 2Morriston Cardiac Centre, Morriston, Wales
Background: We have previously reported the correlation of subclinical systolic right ventricular (RV) impairment in patients with cystic fibrosis (CF) studied with tissue Doppler imaging (TDE) with increased inflammatory indices. We hypothesise that tissue doppler indices (TDI) and inflammatory parameters might identify CF patients with reduced survival.
Methods: We correlated survival status in our patients to clinical, TDI, and inflammatory indices at inclusion in the study. TDI systolic and diastolic velocities and time intervals were recorded at the lateral and medial mitral annulus, at the lateral tricuspid annulus (TVA), and at the RV free wall in the apical four chamber view. Patients were studied during clinical stability (no change in symptoms, medication, FEV1 of more than 10%, for the month previous to the inclusion in the study).
Results: We had information on 22 patients (13 M; mean age (SD) 24.4 (4.1) years) at a mean follow up of 2144 (580) days (range 348–2465 days); three patients were lost to follow up. There were seven CF related deaths (3 M), at an average of 1456 (605) days after inclusion in the study (range 348–2073 days). The isovolumic relaxation time (IVRT) at TVA was shorter in survivors (41.9 (20.3) v 63.2 (12.3) ms, p = 0.04); C-reactive protein (CRP) (7108 (6914) v 17838 (15239), p = 0.06) and clinical severity score (85 (8) v 75 (5), p = 0.08) trended towards significance. Area under the ROC curve was 0.84 (p = 0.03) for IVRTTVA versus survival status.
Conclusion: Prolonged isovolumic relaxation by tissue Doppler of the tricuspid valve annulus, a subtle index of diastolic right ventricular dysfunction, and increased CRP identified cystic fibrosis patients with reduced survival.
S77 OUTCOMES OF CYSTIC FIBROSIS PATIENTS UNDERGOING INVASIVE VENTILATION ON THE INTENSIVE CARE UNIT
C. H. Ward2, C. Bloom1, M. J. D. Griffiths3, S. R. Thomas1. 1Chest Clinic, St George’s Hospital, London, UK; 2Department of Respiratory Medicine, Queen Elizabeth the Queen Mother Hospital, Margate, UK; 3Adult Intensive Care Unit, Royal Brompton Hospital, London, UK
Background: Survival to adulthood is increasingly common in patients with cystic fibrosis (CF). Despite improved medical management of CF and widespread use of non-invasive ventilation on respiratory wards, some patients suffering from acute respiratory failure (ARF) are admitted to intensive care units (ICU). Furthermore, patients with CF now more commonly undergo surgical procedures requiring postoperative ICU admission. Data regarding clinical outcomes are scarce. We have carried out a retrospective study of adult CF patients who underwent endotracheal (ET) intubation and invasive mechanical ventilation (IMV) on the ICU of a UK CF referral centre. The study follows on from one presented to the British Thoracic Society in 1999 by Thomas et al.
Results: Over 159 months, (1991 to 2004), there were 44 episodes of IMV in 39 CF patients; 21 for medical causes of respiratory failure (infective exacerbation, pulmonary haemorrhage or anaphylaxis); and 23 for post-op care. 23 episodes were in male patients. Body mass index was universally low with a mean of 17.9 kg/m2, (range 14.9–22.5) and mean FEV1 was 28% of predicted. For the medical group, patient ages ranged from 17 to 42 years. In nine out of 21 (43%) episodes the patient survived to ICU discharge and in seven episodes (33%) the patient survived to hospital discharge. In four out of 21 (19%) episodes the patient was still alive at six months. In the surgical group, the patients were aged between 18 and 42 years. In 20 of 23 episodes the patient underwent a surgical procedure for pneumothorax. This group did well; in 17/20 episodes (85%) the patient survived ICU and 75% of the patients were discharged from hospital. Overall, the patient survived ICU in 29 out of 44 (65%) episodes and survived hospital in 23/44 (52%).
Discussion: The survival rate of our patients is similar to that recently reported from Australia, (
) where 9/20 patients (45%) survived hospital. In both groups, all patients requiring ICU care for haemoptysis died within six months.
) previously described ICU survival in 20/32 (63%) episodes of IMV for IE of CF; eight had lung transplants from the ventilator. The equivalent figures for our study were 7/16 (44%); none were transplanted. In Vedam’s study, the patient survived 6/10 episodes of IE; one was transplanted during the same admission. Mortality of CF patients on the ICU remains high; these data add to the scarce information that can guide decision making when CF patients are critically ill.
S78 PALLIATIVE CARE NEEDS OF PATIENTS WITH ADVANCED CYSTIC FIBROSIS
S. J. Bourke, A. D. Gascoigne, K. Heslop, A. Anderson, C. Jennings, M. Field1, K. Mannix1. Adult Cystic Fibrosis Centre and Palliative Care Team; 1Royal Victoria Infirmary, Newcastle upon Tyne, UK
Introduction: Although the prognosis of patients with cystic fibrosis (CF) has greatly improved, many die in early adulthood and have complex palliative care needs, which need to be defined and addressed.
Results: Of 208 patients who attended our CF centre from 1997 onwards, 36 have died at a mean age of 26.75 (range 17.1–51.6) years; five died 18 to 51 months post lung transplantation of obliterative bronchiolitis or sepsis; 31 died of CF lung disease (24 had Pseudomonas and 7 Burkholderia cepacia infection); 10 were on an active transplantation waiting list, eight had been assessed, eight had declined transplantation, and four had not yet been considered for transplantation. Most had gradually progressive CF lung disease but five suffered an acute crisis (haemoptysis, cepacia syndrome, acute exacerbation); 13 (42%) were in long term planned palliative care, 12 (39%) were switched to palliative care late, within one week of death, and six (19%) were in full active care till death. Four patients died at home and 27 (87%) died in hospital; one patient had spent time in a hospice. Many had undergone invasive procedures (gastrostomy or nasogastric feeding, portacath insertion, dental extractions) during the previous year in preparation for potential lung transplantation, whereas such procedures were avoided in those receiving longterm planned palliative care.
Prominent symptoms were dyspnoea (100%), difficulty expectorating sputum (71%), chest pain (71%), severe malaise (58%), headache (45%), severe anxiety/fear (42%), abdominal pain (9%), haemoptysis (6%). All patients received palliative antibiotics, 84% opiates, 55% benzodiazepines, 13% hyoscine, 13% cognitive behavioural therapy, 29% non-invasive ventilation. Seven patients (22%) had specific CF complications (3 distal intestinal obstruction, 2 pneumothorax and 2 portacath erosion of skin). Autopsy was performed in only one patient. Many had siblings with CF, young children, spouses, and parents present during the final illness.
Conclusions: “Quality of death” is important for the patient and the family. Many patients have specific anticipated fears, such as “choking to death” which can be allayed. Transition from active to palliative care is particularly complex in the context of transplantation. Most patients wanted to be on the CF ward during their terminal illness and many still needed the specialist skills of the CF team. Specialist palliative care team input was particularly helpful in discussing advanced directives and end-of-life issues and in managing severe anxiety.
Outcomes of lung cancer diagnosis and treatment
S79 CHANGE IN PRACTICE IN THE DIAGNOSIS OF LUNG CANCER IN GREENWICH 1998–2004
E. E. Strawson, A. Patterson, T. C. Stokes, J. R. Webb. Queen Elizabeth Hospital, Woolwich, London SE18 4QH, UK
Background: The benefits of a CT scan prior to bronchoscopy in patients with lung cancer has already been demonstrated in a small group of 171 patients treated in a specialist referral unit (
). We report our experience in 1031 patients over seven years in a district general hospital population.
Aim: To demonstrate a change in the order of and number of investigations; CT (computed tomographic) scans, fibreoptic bronchoscopy (FOB), and percutaneous CT guided biopsy (PCTB) and what effects this has had on service delivery.
Method: Data were collected at the weekly lung cancer MDT (multidisciplinary team meeting) from January 1998 to December 2004 initially by the Consultant Chest Physicians and from 2003 by the MDT coordinater.
Results: See table.
The median time to diagnosis over the seven year period was 10, 9.5, 13, 14, 15, 17, 17 showing a significant increase of 1.4 days per year on average (p<0.0005).
Conclusion: From 1998 to 2004 there has been a significant increase in the total number of CT scans, number of patients having a CT scan as the first investigation, a decrease in FOBs, and an increase in the number of PCTBs. The median time to diagnosis has increased on average by 10 days over the seven year period. The introduction of early (prebooked) CT scans has improved the selection of the most appropriate invasive investigation (FOB or PCTB), however this has resulted in an increase in the time to diagnosis. These findings have important implications regarding new government targets for time to diagnosis (31 days) and treatment (62 days), for resource use in radiology, and training in bronchoscopy.
S80 LUNG CANCER CARE IN LIVERPOOL: REAUDIT EIGHT YEARS ON
S. Bari, J. Hughes, D. A. Stock, C. M. Smyth, M. J. Walshaw, M. J. Ledson. Liverpool Lung Cancer Unit, The Royal Liverpool University Hospital and The Cardiothoracic Centre, Liverpool, UK
Background: Liverpool has the highest incidence of lung cancer in England and Wales, with up to 400 cases occurring each year within the catchment area of two central teaching hospitals. A city wide audit in 1996/97 demonstrated that services were fragmented and inadequate, and following publication of this we organised a joint lung cancer unit between the two hospitals. This included the formation of a one stop rapid access clinic where patients are offered a consultation, CT scan, and bronchoscopy (where appropriate) on the same day, and the working of clinicians across both hospital Trust boundaries. We were interested to assess whether this reorganisation had improved the care of lung cancer patients in Liverpool.
Method: We reaudited patients presenting with lung cancer to the two hospitals over the same six month calendar period in 2004/05 and compared patient demographics, route of presentation, clinician input, duration of the patient journey, and treatments offered between the two time periods eight years apart. There were similar patient numbers in 1996/97 (186, group A) and 2004/05 (168, group B).
Results: There was no difference in age between the two groups (mean 69.9 years v 69.1). In Group A only 69 (37%) presented as outpatients, (29 (16%) as GP referrals) whereas in Group B this was 94 (56%, 79 (47%) via the GP). Furthermore, in group B 49 patients (29%) presenting as acute admissions were discharged speedily to be investigated in the outpatient service: this facility was not available for group A. Only 96 (51%) were investigated by chest physicians in group A: this was 100% for group B. Whereas only 98 patients (53%) in group A had a staging CT scan, this had improved to 167 (99%) in group B. More group B patients underwent bronchoscopy (130 (76%) v 127 (68%)) and the time to bronchoscopy also improved (mean wait 2.9 days v 11.4). Histological diagnosis rates were better in group B (124 cases (74%) v 119 (64%)), although cell types were similar.
Although surgical resection rates did not improve, reflecting the high comorbidity in these patients, all patients in group B received an oncological opinion and more benefited from radio- and/or chemotherapy (group B 73 (43%) v group A 18 (10%)).
Conclusion: This reaudit has shown that reorganising lung cancer services in Liverpool has improved the care offered to patients. The implementation of a one stop lung cancer clinic allows most patients to be seen as outpatients, reducing the burden on A&E and inpatient facilities. Breaking down the barriers between hospital Trusts through cross site working and shared personnel has allowed more timely investigation of and improved treatment for these unfortunate patients, thereby enhancing the quality of care offered by the health care providers.
Abstract S80
S81 LUNG CANCER OUTCOMES AT A UK CANCER CENTRE: CAN WE DO BETTER?
C. M. Free, M. Ellis, D. R. Baldwin. Nottingham City Hospital, Hucknall Road, Nottingham NG5 1PB, UK
Introduction: There have been few data published on survival from lung cancer in the UK. Most population survival estimates by stage are based on data from the USA.1 An accurate denominator, though difficult to achieve, is essential to ensure accurate survival figures. We describe survival rates by stage for our lung cancer population at Nottingham City Hospital and the treatment offered.
Methods: Prospective data from the lung cancer multidisciplinary team (MDT) meetings between 1998–2001 were cross referenced with information supplied by Trent Cancer Registry for registrations of lung cancer during the same period. Where information was missing notes were reviewed retrospectively and a comprehensive dataset was created. Notes were retrospectively reviewed for patients with stage I–IIIA who did not undergo treatment with curative intent.
Results: There were 842 new lung cancers diagnosed between 1998–2001. Non-small cell lung cancer (NSCLC) 614 (73%), small cell (SCLC) 137 (16%), clinical diagnosis 91 (11%). The MDT did not discuss 20% of cases (n = 169), despite a policy of discussing all patients. Mean age at diagnosis was 69.7 years. Information on stage at diagnosis was available in 69% of NSCLC (78% of those discussed by MDT). Stage at diagnosis: I (118/489; 24%), II (45/489; 9%), III (151/489; 31%), IV (175/489; 36%). Patients without SCLC were treated as follows: surgery (81/705; 12%), radical radiotherapy (RT) (32/705; 5%), palliative RT (222/705; 31%), chemotherapy (59/705; 8%), best supportive care (BSC) (255/705; 36%), Missing data (58/705; 8%). The table shows cumulative survival by stage (excluding SCLC). The overall five year survival was 7.5%.
Of patients with stage I–IIIA disease only 94/203 (46%) received treatment with curative intent. Patients were declined surgery for the many reasons: Patient choice (10%), lung function (30%; mean FEV1 0.88), performance status or comorbidities (23%), progression prior to surgery (11%). The reasons were unclear in 8%.
Abstract S81
Conclusions: These data show survival by stage at a cancer unit with thoracic surgery on site. The data are comprehensive and reflect the true picture. Survival figures are lower than those for the USA published by Mountain except for stage 3 at 36 months. 54% of patients with stage 1 to 3A disease did not receive potentially curative treatment, usually for appropriate reasons. More comprehensive UK data for comparison are needed.
1
S82 CANCER WAITING TIME TARGETS AND TUMOUR STAGE AT SURGERY FOR LUNG CANCER
V. Kelly, J. Maguire, M. Ledson, C. Smyth, M. Jackson, M. Walshaw. Liverpool Lung Cancer Unit, Cardiothoracic Centre, Thomas Drive, Liverpool L14 3PE, UK
The Department of Health now places particular emphasis on the 31 and 62 day targets between GP referral, diagnosis, and treatment for patients with cancer. Surgery is the potentially curative treatment for patients with lung cancer; tumour stage at operation correlates strongly with survival at five years. There is little evidence that surgery within any specific time frame affects tumour stage or outcomes for patients with lung cancer.
We have reviewed the case notes of 200 consecutive patients who underwent surgery for lung cancer in the Liverpool Cardiothoracic Centre from July 2004 to May 2005. 157 of these patients were from England where the 62 day target applies. 84/157 (53%) had been referred from primary care as urgent - suspected cancer. Of these, 47/84 (56%) underwent surgery within 62 days, and 37/84 (44%) missed the 62 day target. These breaches were due to delays in diagnosis and staff and patient holidays rather than surgical complexity of individual cases. There was no significant difference in tumour stage between patients who underwent surgery before and after the 62 day target (Stage I 57.4% v 61.1%, Stage II 19.1% v 24.3%). However, 16/17 (94.1%) of the patients who underwent surgery within 42 days (6 weeks) of urgent GP referral had either stage I (70.6%) or stage II (23.5%) tumours. These patients were found to have undergone surgical assessment sooner than patients who waited more than six weeks for surgery.
We conclude that a 62 day target time between urgent referral and surgery for patients with suspected lung cancer does not result in an advantage in terms of tumour stage in patients who undergo surgery within the target time. Our data suggest that a target time of 42 days between urgent referral and surgery results in almost all patients having stage I or II disease at operation. For patients with potentially operable lung cancer, early thoracic surgical involvement in the assessment and diagnostic process is likely to result in shorter waiting times for treatment and earlier tumour stage at operation.
S83 WHY DON’T WE OPERATE MORE? A STUDY OF NON-SMALL CELL CANCER IN A DEPRIVED INNER CITY AREA
F. Latheef1, D. Booth1, M. Prescott2, P. M. Taylor3, N. Odom4, M. Woodhead1. 1Respiratory Medicine; 2Nuclear Medicine; 3Diagnostic Radiology; 4Cardiothoracic Surgery, Manchester Royal Infirmary, UK
Background: The only realistic option to increase cure in non-small cell lung cancer (NSCLC) is to increase the proportion of patients receiving curative surgery. Surgery is usually denied due to either extensive stage disease or lack of operative fitness. We undertook a study of the importance of these two features in a deprived inner city population with a high lung cancer incidence. The centre has been routinely using PET scanning before surgery which is performed on-site.
Methods: Cases of lung cancer occurring in 2004 were retrieved from the department database and those with small cell lung cancer excluded. Those with proven NSCLC and those without cell type confirmation were included. Data on the reasons for management decisions were retrieved from the case notes.
Results: A total of 112 patients with lung cancer were identified of whom 92 (82%) were NSCLC or cell type undetermined. Surgery with curative intent was performed on nine (10%). Of the 83 on whom surgery was not performed, in 29 (35%) this was due to lack of surgical fitness and in 52 (63%) to extensive disease. PET scan influenced the decision not to operate in nine cases. Lack of surgical fitness was due to pulmonary comorbidity/poor lung function (all seven denied for lung function alone had FEV1 <40% predicted) in 21 (72%), cardiovascular disease in 16 (55%) (11 had both cardiovascular and pulmonary comorbidities), and other causes in three (10%). Of those denied surgery due to disease extent 17 (33%) would have been unlikely to have been fit even if disease had been localised. Thus in total 46 (55%) would have been unlikely to be fit for surgery regardless of disease extent and only 37 (45%) were denied due to disease extent alone.
Conclusions: In the majority of cases lack of surgical fitness and not disease extent would have determined non-operability. This group is larger than in other series, probably reflecting the social deprivation experienced in the local community. Improving the general health of our local population is going to be the most important factor in increasing NSCLC operability rates.
Pleural disease
S84 RANDOMISED TRIAL COMPARING CHEST DRAIN WITH INTRAPLEURAL UROKINASE VERSUS VIDEO ASSISTED THORACOSCOPIC SURGERY FOR THE TREATMENT OF EMPYEMA IN CHILDREN
S. Sonnappa, G. Cohen, C. van Doorn, M. Elliott, C. Owens, A. Jaffe. Great Ormond Street Hospital, London WC1N 3JH, UK
Background: Empyema causes significant childhood morbidity. The recent publication of guidelines on the management of pleural infection in children by the British Thoracic Society highlights the lack of grade A evidence available to inform best management for the many treatment options available.
Aim: A prospective randomised trial was conducted to compare chest drain with intrapleural urokinase and video assisted thoracoscopic surgery (VATS) for the treatment of empyema in children.
Methods: Over a period of three years children under 16 years of age with empyema were randomised to receive either percutaneous chest drain with intrapleural urokinase or VATS. Children with underlying cardiac disease and immunodeficiency were excluded. Chest drains were removed when there was minimal drainage of fluid and patients were discharged if they were afebrile for more than 24 hours at the paediatrician’s discretion. The primary outcome studied was the number of days in hospital post intervention. Secondary end points were number of chest drain days, total hospital stay, failure rate, and radiological outcome—that is, chest x ray changes at six months. We believed that a difference in hospital stay of two days between the two treatment arms would be clinically important. To detect this difference at 5% significance with 80% power 29 patients were needed in each study group. The two groups were compared by using the Mann-Whitney U test. A p value <0.05 was considered significant.
Results: Sixty children were recruited into the study. The VATS and urokinase groups were well matched for age (median (interquartile range) 3.57 (2.28–7) and 3.07 (2.28–5.38) years), sex (16 and 17 males), illness days before intervention (median (interquartile range) 11 (8–14) and 9 (7–15) days), haematological and biochemical parameters (median (interquartile range) CRP 153 (96–241) and 183 (45–292) mg/l; WBC 18 (10.8–23.3) and 15.2 (10.6–20.5)×109/l; platelets 500 (370–640) and 476 (352–682)×109/l) and pleural fluid LDH (median (interquartile range) 10000 (4880–20000) and 6953 (2992–16554) U/l) respectively. No difference was found in the length of stay post intervention between the two groups (p = 0.311). There was a difference of one day in number of chest drain days, in favour of the VATS group (p = 0.055). There was no difference in the total hospital stay or failure rate of assigned treatment between the two groups. Chest x rays at six months post discharge were available in 40 patients (21 from the urokinase group). Mild pleural shadowing was present in 37/40 (92%) patients and there was no difference between the two groups (p = 0.682).
Conclusions: There is no significant difference between chest drain with intrapleural urokinase and VATS for the treatment of empyema in children. This study provides an evidence base to guide the management of empyema in children.
S85 VIDEO ASSISTED THORACOSCOPIC SURGERY FOR CHRONIC POST-PNEUMONIC EMPYEMA: A MISSED OPPORTUNITY?
R. S. Jutley, A. Conybeare, A. Rengarajan, D. A. Waller. Glenfield General Hospital, UK
Background: Video assisted thoracoscopic surgery (VATS) has increased the available treatment options for chronic post-pneumonic empyema (PPE). The approach has proven benefits over fibrinolysis1 and thoracotomy.2 However, it remains underutilised in UK.3 We have continued to explore the use of VAT debridement/decortication for multiloculated PPE irrespective of chronicity and have audited our results in an attempt to explain this anomaly.
Methods: VATS was performed via three 2 cm incisions without rib spreading. Directed suction-debridement of the fibropurulent exudate was followed by visceral and parietal decortication using blunt/sharp dissection. Immediate conversion to thoracotomy was reserved for incomplete lung expansion. A comparison of outcome of VATS and thoracotomy and its effect on overall empyema surgery was also studied.
Results: Expressed as mean (SD): 81 patients had empyema surgery over 98 months. VATS was attempted in 55 (68%) with an overall success rate in 69% (38 patients). Successful VATS could not be predicted by age, sex or preoperative delay but was related to increasing operative experience (p<0.05). Current success rate for VATS was 81% in the last 25 patients. With increasing experience there was a trend to offer primary VATS. Postoperative stay was shorter after VATS (7.0 (5.5) days) than thoracotomy (8.0 (3.9) days) (p<0.05). No patient required additional intervention for non-resolution of symptoms. There was no radiological difference in outcome between the two groups.
Conclusions: VATS for PPE is effective and preferable to thoracotomy, but it has a definable learning curve that must be overcome to change overall empyema surgery practice.
1
2
3
S86 THE SURVIVAL SIGNIFICANCE OF DIFFERENT BACTERIAL CLASSES IN PLEURAL INFECTION: DATA FROM THE MRC/BTS MIST1 TRIAL COHORT
N. A. Maskell1, S. Batt2, E. L. Hedley1, C. W. H. Davies3, S. H. Gillespie2, R. J. O. Davies2. 1Oxford Centre for Respiratory Medicine; 2Royal Free Hospital, London; 3Royal Berkshire Hospital, Reading, UK
The survival consequences of differing bacterial classes of pleural infection are poorly described. The MIST1 trial (
) assembled a large, well characterised patient cohort. This abstract presents the prognostic significance of bacterial classes in this cohort. Pleural fluid from 434 patients underwent standard bacterial culture and a screen for bacteria by amplification and sequencing of the bacterial DNA sequence coding for the 16S ribosomal subunit. DNA sequences were identified by comparison with the GenBank database (http://www.ncbi.nlm.nih.gov). Groups of subjects with bacteria of a particular class were identified blind to these subjects clinical outcome (S pneumoniae 59, S intermedius group 55, Other strep 23, anaerobes/mixed 49, S aureus 34, mixed aerobes 28, Gram neg 22). Mortality was studied in these groups and in hospital/community infection. Mortality was similar in all the streptococcal groups, but was increased in hospital acquired infection (hospital 17/36, 47%, community 53/304, 17%, relative risk 4.24, 95% CI 2.07 to 8.69, p<0.00001, χ2, 1 df = 17.47) and in Gram negative 10/22 (45%), S aureus 15/34 (44%) or mixed aerobic infections 13/28 (46%), compared to streptococcal infection 23/137 (17%) and anaerobic/mixed infection 10/49 (20%). (p<0.00001, χ2 4 df = 23.35).
The increased mortality risks associated with community versus hospital infection and with the different bacterial classes were statistically independent. Compared to S pneumoniae infection, mortality is increased in pleural infection with S aureus, Gram negative and mixed aerobic bacteria, but not in anaerobic/mixed infections. These poor prognosis infections may benefit from early surgical drainage.

The survival significance of different bacterial classes in pleural infection: data from the MRC/BTS MIST1 trial cohort.
S87 STUDY OF PLEURAL FLUID BIOCHEMISTRY: CAN ANION GAP BE A SURROGATE MARKER OF PH?
W. N. Lee, M. M. Cotton. Department of Respiratory Medicine, Glasgow Royal Infirmary, UK
Background: Pleural fluid pH is found to be the most useful index in predicting the need for intercostal drainage in parapneumonic effusions.1 In our hospital, pleural fluid pH is not readily measured in the laboratory due to potential technical problems with the blood gas analyser. Therefore, we set out to explore if an alternative test could be used in place of pleural fluid pH.
Method: We prospectively studied the biochemistry of pleural fluid in patients who were referred to our department for investigation of pleural effusions over a six month period. Visibly purulent samples were excluded. Pleural fluid Na+, K+, Cl−, HCO3−, protein, albumin, glucose, LDH, pH; and concurrent serum protein, albumin, glucose, LDH levels were measured. Pleural fluid anion gap was calculated using the formula (Na++K+)− (Cl−+HCO3−). Light’s Criteria were used to separate transudates and exudates. Pleural fluid acidosis was defined as pH<7.3. The data were analysed using Mann-Whitney U test and Pearson coefficient of correlation.
Results: Data from 21 patients were available for analysis. There were 15 exudates and six transudates. Only three out of 15 exudative effusions were acidic. The median anion gap of exudative effusions was significantly higher than that of transudative effusions, 13 mmol/l versus 4.6 mmol/l (p = 0.011). The median anion gap of acidic effusions was significantly higher than that of non-acidic effusions, 15.1 mmol/l versus 9.7 mmol/l (p = 0.035). A significant inverse linear correlation was found between pH and anion gap (r = −0.7, p<0.001).
Conclusion: No clinical studies have previously looked at how anion gap behaves in different types of pleural effusions. We have shown that pleural fluid anion gap may have a role in differentiating between exudative and transudative, acidic and non-acidic pleural effusions. There was only one patient with parapneumonic effusion which was uncomplicated, so we were not able to evaluate the relation between pH and anion gap in this specific group. Further clinical studies on larger samples are required to look at the role of anion gap in the diagnosis and management of pleural effusions more closely.
1
S88 THE CLINICAL UTILITY OF ULTRASOUND IN DETECTING MALIGNANT PLEURAL DISEASE IN THE PRESENCE OF A PLEURAL EFFUSION
N. R. Qureshi, F. V. Gleeson. Department of Radiology, Churchill Hospital, Headington, Oxford, UK
Background: CT studies have shown that the diagnosis of malignant pleural disease is favoured by the presence of parietal pleural thickening >1 cm, circumferential, mediastinal and nodular pleural thickening. Contrast enhanced CT is therefore widely accepted as the imaging modality of choice when investigating patients with suspected malignant pleural effusions. In a busy radiology department, rapid access to CT is not always possible. Ultrasound is much more readily available and involves no radiation.
Aim: To prospectively assess the role of ultrasound in demonstrating malignant pleural thickening and differentiating malignant from benign pleural disease in the presence of a pleural effusion.
Method and Materials: Thirty nine consecutive patients referred to radiology for further investigation of a pleural effusion of unknown aetiology were recruited. All patients had a chest ultrasound followed by a contrast enhanced CT. Two independent observers (consultant chest radiologist and fellow in chest radiology) assessed the pleural surfaces on ultrasound using the above mentioned established CT criteria for malignant pleural thickening. Additionally diaphragmatic thickness/nodularity, pleural effusion size and liver echotexture for hepatic metastasis was recorded. An ultrasound and CT based diagnosis of malignant or benign pleural disease was made. Definitive diagnosis was based on histological/cytological analysis for malignant disease and clinical follow up in benign disease.
Results: Pleural effusions were malignant in 23 patients and benign in 16 patients. Ultrasound correctly diagnosed malignant pleural disease in 18 of the 23 patients (sensitivity 78%, specificity 94%, positive predictive value 95% and negative predictive value 75%). Benign pleural disease was correctly diagnosed in 15 of the 16 patients (sensitivity 93%, specificity 78%, PPV 75%, NPV 94%).
Conclusion: Ultrasound is safe, easily accessible and is a reliable test for demonstrating malignant pleural disease. In patients presenting with a pleural effusion ultrasound should be considered the first line investigation of choice with CT reserved for problematic cases where ultrasound has been inconclusive.
S89 OUTPATIENT MANAGEMENT OF PNEUMOTHORAX
S. Ambalavanan, J. F. Miles. North Manchester General Hospital, UK
Background: We have previously demonstrated the safety and efficacy of the Tru-close Thoracic vent device (TCTV) on patients presenting with pneumothorax (
). The present study looks at outpatient treatment of pneumothorax across four different sites (North Manchester General Hospital, Fairfield General Hospital, Royal Oldham Hospital, and Rochdale Infirmary).
Methods: All patients with a radiographically confirmed diagnosis of primary spontaneous pneumothorax (PSP) or secondary spontaneous pneumothorax (SSP) who require intervention as per the BTS guidelines (May 2003), were included. Patients with fluid in the pleural space, bilateral pneumothoraces, suspected tension pneumothorax, limited ability to understand or comply with instructions, those receiving ventilatory support, requiring admission for social considerations, living too far from the hospital (that is, >30 minutes by car) or with underlying conditions that require additional treatments which cannot be provided as outpatients (for example, COPD requiring nebulisers, supplemental oxygen, etc), and pneumothorax secondary to trauma were excluded from the study. Endpoints were (a) resolution of pneumothorax, (b) complications requiring subsequent intercostal tube drainage, (c) requiring admission within the study period for an indication connected with the episode, and (d) patient satisfaction. After TCTV insertion, patients were discharged with analgesia, written information, instructions, and contact details of a helpline. All patients received daily telephone calls from a physician for reassurance. After the indicator pressure sensitive diaphragm (PSD) had ceased to oscillate for 24 hours, participants returned for TCTV removal. A satisfaction questionnaire was administered at this point, and final chest radiograph organised in chest clinic in 2–3 weeks’ time.
Results: Seventeen consecutive patients (5 females, 12 males) with pneumothorax between the ages of 22 and 78 (mean 38.6 years, median 30 years) were included. 16 patients had PSP and one patient had SSP. 14 patients (82.4%) had successful resolution after a mean duration of 5.5 days (range 1.8 to 10.5 days), two patients (11.8%) required admission for a conventional intercostal drain due to TCTV catheter dislodgement, eventually needing surgery for resolution, and one patient (5.8%) required admission for suction via TCTV (eventually required surgical intervention). All patients without exception expressed satisfaction with the treatment received.
Conclusions: We conclude that a majority of patients with pneumothorax can be safely treated as outpatients with the use of TCTV.
Funding: North Manchester R+D.
Ethics approval: North Manchester LREC.
Epidemiological studies in asthma
S90 SENSITIVITY TO ALTERNARIA ALTERNATA IN GRASS POLLEN SENSITIVE ASTHMATICS IS AN IMPORTANT FACTOR IN THUNDERSTORM OUTBREAKS OF ASTHMA
T. B. Pulimood1, J. Cordon2, S. M. Nasser3. 1West Suffolk Hospital, A Cambridge University Teaching Hospital, UK; 2Midlands Asthma and Allergy Research Association, Derby, UK; 3Cambridge University Hospitals NHS Trust, Cambridge, UK
Introduction: Epidemics of asthma during thunderstorms have been previously investigated but the cause has not been clearly identified. In the days following 29 July 2002, at the end of the grass pollen season, there was an outbreak of asthma associated with a thunderstorm in Cambridge.
Methods: A case controlled study of 26 patients presenting with thunderstorm asthma to Addenbrooke’s hospital Cambridge, during the outbreak. Patients underwent skin prick allergy tests and had blood drawn for specific IgE serology to a number of inhaled aeroallergens. Controls were a consecutive group of 31 seasonal asthmatics with grass pollen sensitivity confirmed by skin testing.
Results: Twenty three out of 26 cases were positive to Alternaria alternata (AA), 16/26 to Cladosporum cladosporioides (CC) and 22/26 positive to grass pollen on either skin prick testing or IgE serology. 11/31 of our grass pollen allergic control subjects gave a history of exacerbations of asthma during thunderstorms, 10 of whom were also sensitive to AA on skin prick testing.
Abstract S90 Odds ratio for developing thunderstorm asthma based on sensitivities from skin tests and IgE specific serology to AA and CC
Conclusions: IgE mediated sensitivity to fungal spore allergens and particularly Alternaria alternata are a strong predictor of thunderstorm related asthma in seasonal asthmatics with grass pollen allergy and is likely to be an important causal factor in thunderstorm related asthma exacerbations.
S91 CHILDHOOD OBESITY PREDICTS CURRENT INCIDENT ASTHMA IN ADULT WOMEN
J. A. Burgess1, E. H. Walters2, G. B. Byrnes1, M. A. Jenkins1, G. G. Giles1, M. J. Abramson3, J. L. Hopper1, S. C. Dharmage1. 1Department of Public Health, University of Melbourne; 2Respiratory Research Group, University of Tasmania Medical School; 3Epidemiology and Preventative Medicine, Monash University, Australia
Introduction: The parallel rise in obesity and asthma prevalences suggests a possible causal link. We have examined the relation between childhood body mass index (BMI) and adult incident asthma in a large longitudinal study in Tasmania.
Methods: Subjects were participants in the Tasmanian Asthma Study who did not have asthma by age 7. Weight, height, and lung function of over 3500 children were measured at age 7 in 1968. Subjects’ asthma status was later ascertained at ages 14, 21, and 32. Odds ratio were calculated for the association between quartiles of body mass index Z scores at age 7 and asthma incidence at different ages.
Results: BMI at age 7 was associated with having current incident asthma (but not remitting incident asthma) but only for females. For females in the highest quartile of body mass index Z score at age 7, the odds ratio for current incident asthma after age 7 was 2.91 (95% CI 1.20 to 7.08). For females in the same weight group the odds ratio for current incident asthma after 14 and 3.93 (95% CI 1.37 to 11.28) and for current incident asthma after 21 the odds ratio was 3.99 (95% CI 1.24 to 12.81). The associations remained after adjustment for confounders including BMI later in life and early menarche. Effect of childhood obesity on lung function may explain some of the increased risk. The attributable risk of current incident asthma after age 7 for females in the highest quartile of body mass index at age 7 was 31.8% (95% CI 28.3% to 35.3%).
Abstract S91
Conclusions: Higher childhood BMI and current incident asthma are associated in women.
S92 THE DIAGNOSTIC LABEL OF CHILDHOOD WHEEZY BRONCHITIS SHOULD BE REINSTATED
N. Tagiyeva-Milne, G. McNeil, G. Russell, P. J. Helms. Department of Child Health University of Aberdeen UK
Background: Until the 1980s the terms wheezy bronchitis (WB) (
), chronic bronchitis of childhood in North America (
), were commonly used to describe children with recurrent wheezing and cough predominantly provoked by intercurrent respiratory tract, presumed viral, infections, in contrast to children with multitrigger wheeze (MTW) characteristic of atopic asthma. We hypothesised that if the two conditions are merely expressions of the same disease along a severity spectrum the associations with risk factors for asthma and for disease severity should be similar.
Methods: In May to June 2004 the fifth sequential school survey was undertaken including the same questions used in the original 1964 survey (Dawson B et al. Lancet 1969;i:827–30).
Results: 3271 of 5712 questionnaires were returned (57.3%) from primary years 3–7 (age 7–12 years) in 32 participating schools. Overall prevalence of WB at 7.3% was unchanged from 1964 (6.7%) albeit with a higher prevalence in boys (7.8%) than in girls (6.9%). After adjustment for possible confounders, environmental tobacco smoke (ETS) was only significant as a risk factor for WB. Both personal and parental reported eczema and hayfever were more strongly associated with MTW than with WB. Severe disease (>12 episodes per year) was more frequent for MTW (30.7%) than WB (12.5%). Severe WB had no associations with any risk factors in contrast to significant independent associations of deprivation and increasing age with severe MTW.
Conclusions: WB and MTW appear to be distinct entities in children of school age. Further study of the underlying mechanisms of childhood WB and associations with subsequent adult disease are warranted.
S93 HEALTH LOCUS OF CONTROL IN ADULTS WITH WELL AND POORLY CONTROLLED ASTHMA: A CASE CONTROL SURVEY
J. L. Gellatly1, A. Caress1, L. M. Osman2, C. Calder2, C. Garden2, R. Niven3, A. Woodcock3, T. Walsh1, M. Campbell1, K. Luker1, B. Ryan-Woolley1, K. Beaver1. 1The University of Manchester, UK; 2University of Aberdeen, UK; 3North West Lung Centre, Wythenshawe Hospital, UK
Background: Asthma causes high levels of morbidity and hospitalisation, Self management by patients requires confidence in their ability to control symptoms and manage their disease. “Health locus of control” (HLOC) addresses whether individuals consider that they control health outcomes themselves (“internal” HLOC) or view these as being outside their control (“external” HLOC), either arising by chance or from the actions of doctors and other powerful people. Such beliefs may impact on health related behaviour. We studied whether HLOC differs between those with well and poorly controlled asthma.
Methods: A case control survey was undertaken with adult patients (16+) from two hospital sites (Aberdeen, Manchester). Data were collected by postal survey, using the Multi-Dimensional Health Locus of Control Scale Form C. Cases had either clinician defined “difficult to control” asthma (DTCA) or 2+ asthma admissions in the last two years (AA). Well controlled asthma was defined as no admissions or no more than one oral steroid course in the past year (WCA).
Results: 241 patients were recruited (114 Aberdeen, 127 Manchester; mean age 46.1, SD 11.3, range 18–65; 166 (69% female). 58 were DTCA (Aberdeen 24; Manchester 34), 33 AA (Aberdeen 20; Manchester 13), and 150 WCA (Aberdeen n = 70; Manchester n = 80). There was a highly significant difference between groups in Internality score (F(2,235) = 8.04, p<0.001), with AA feeling most in control (mean score 21.7 out of 36) and DTCA feeling least in control (16.5). There was a significant difference between sites in the Chance score (F(1,235) = 5.19, p = 0.024), with Aberdeen (mean score 16.0 out of 36) showing a greater belief in chance compared with Manchester (14.2). There was a significant interaction between group and site for the Doctors score (F(2,235) = 4.29, p = 0.015), with DTCA at Aberdeen showing the greatest reliance on doctors (mean score 15.0 out of 18) and DTCA at Manchester showing the least (11.5). There was also a significant difference between groups for the Other Powerful People score (F(2,235) = 4.65, p = 0.011), with DTCA showing the greatest reliance (mean score 11.3 out of 18) and WCA showing the least (9.5).
Conclusions: The findings demonstrate some similarities, but also some contrasts in HLOC between patients with well and poorly controlled asthma. It was interesting that the AA group felt most in control, despite evidence to the contrary; further exploration of these beliefs appears warranted. Likewise, the apparent dependence of those with DTCA on “powerful others” merits further study.
S94 HETEROGENEITY IN REFRACTORY ASTHMA: THE USE OF CLUSTER ANALYSIS TO IDENTIFY DISTINCT COHORTS
P. Haldar, R. H. Green, M. A. Berry, A. J. Wardlaw, I. D. Pavord. Institute for Lung Health, Glenfield Hospital, Leicester, UK
It is well recognised that difficult asthma represents a significantly heterogenous population in terms of underlying disease pathophysiology, response to treatment, and outcome. For this reason, no single management strategy confers a solution for these patients. We sought to investigate whether subgroups could be identified within a cohort of patients attending the Difficult Asthma Clinic (DAC) at Glenfield Hospital, using the statistical method of cluster analysis. This technique has been used widely in the biological sciences, and in medicine most notably for the classification of psychiatric disorders. Data collected from 271 patients attending DAC over a period of four years were analysed. An agglomerative, hierarchial technique using Ward’s method to construct a dendrogram revealed four or five distinct clusters within our population. A K-means clustering method was then utilised predicting either a four or five cluster model to allocate individual cases to a cluster based upon input variables that best characterised the patient’s disease. These included: demographic variables, smoking history, number of pets, allergy (skin prick tests, eczema, hayfever, serum IgE), inflammation (sputum and blood eosinophils), variable airflow obstruction (bronchodilator reversibility and peak flow variability), and measures of psychosocial wellbeing (hospital anxiety and depression scores). A 4 cluster model best fit the dataset: cluster 1 (25%) were middle aged (mean 54.7 years) with early onset atopic asthma, evidence of airway inflammation, and significantly lower post bronchodilator (PBD) FEV1 than for the study population (71% v 79%); cluster 2 (34%) was a young (mean 29 years), strongly atopic and predominantly female group (80%) with less airway inflammation. This group was also most likely to have pets. Cluster 3 (15%) was made up of middle aged individuals (mean 51.3 years) with a significant smoking history (38.2 pack years), fixed airflow obstruction (PBD FEV1 68%) and minimal eosinophilic airway inflammation. Cluster 4 (25%) was a middle aged cohort (56.1 years) with late onset non atopic asthma. This cluster was characteristically an inflammation predominant group with the least symptoms and best lung function (PBD FEV1 85%). Difference in outcome measures between the clusters was assessed using one way ANOVA. Cluster 2 had significantly more hospital admissions in the year preceding attendance at our clinic than the other groups. Cluster 3 had significantly greater symptoms and psychosocial morbidity than the other groups. Finally, clusters 1 and 3 were associated with significantly more ITU admissions than the other groups which may reflect the greater severity of airflow obstruction (lower PBD FEV1) in these cohorts. We conclude that cluster analysis defines subgroups within difficult asthma that appear to differ significantly in their presentation, characteristics, and respective outcomes and it is likely that effective therapeutic and management strategies may need to be tailored accordingly.
S95 PSYCHOSOCIAL CORRELATES OF PREVALENT ASTHMA AND OF INCIDENT HOSPITAL ADMISSIONS DUE TO ASTHMA: EVIDENCE FROM THE EPIC-NORFOLK POPULATION BASED COHORT OF OLDER ADULTS
N. W. J. Wainwright1, P. G. Surtees1, N. J. Wareham2, B. D. W. Harrison. 1Strangeways Rersearch Laboratory and Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK; 2Medical Research Council Epidemiology Unit and Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK; 3Norfolk and Norwich University Hospital, Norwich, UK
Background: Limited knowledge is available concerning the association between psychosocial factors, asthma prevalence, and incident asthma outcomes in general community samples.
Methods: Participants in the European Prospective Investigation into Cancer population study in Norfolk (EPIC-Norfolk), recruited through general practice age-sex registers, completed a comprehensive postal questionnaire assessment of their social and psychological circumstances. Data on self reported doctor diagnosed asthma were available for 20 888 study participants and on subsequent hospital admissions due to asthma (throughout England and Wales) through linkage with the National Health Services health district database.
Results: Doctor diagnosed asthma was reported by 1699 (8.1%) of participants.
After adjustment (for age, sex, cigarette smoking, social class, obesity, physical functional health, and lung function), prevalence of asthma was approximately 50% higher for those participants reporting a current mood disorder, odds ratio (95% confidence interval) 1.46 (1.19 to 1.79)), 30% higher for those who reported two or more adverse circumstances in childhood (1.28 (1.11 to 1.48)), and 30% higher for those who reported two or more recent events in adulthood (1.28 (1.11 to 1.47)). A total of 424 hospital admissions due to asthma were recorded in 107 423 person-years of follow up. Following adjustment (for age, sex, physical functional health, obesity, and lung function), rates of hospital admission due to asthma were approximately 30% higher for those who reported two or more adverse circumstances in childhood (rate ratio (95% confidence interval) 1.32 (1.02 to 1.71)); 40% higher for those who reported two or more recent events in adulthood (1.37 (1.06 to 1.77)), and 25% higher for those who reported negative aspects of support from their close confidant(e) (1.25 (1.00 to 1.57)).
Conclusions: Adverse psychosocial are associated with increased asthma prevalence and increased rates of incident hospital admission in this population study of older adults.
Outcomes of chronic obstructive pulmonary disease exacerbations
S96 EFFICACY AND ORGANISATION OF EARLY DISCHARGE SCHEMES FOR ACUTE EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE: ANALYSIS FROM THE 2ND UK COPD AUDIT
S. J. Quantrill, H. Hosker, K. Anstey, D. Lowe, C. M. Roberts. Royal College of Physicians Clinical Effectiveness Unit
Background: Studies of Early Discharge Schemes (EDS) for acute exacerbations of chronic obstructive pulmonary disease (AECOPD) have shown that about 25% of such patients can be safely and effectively cared for at home (
). Part of the 2nd UK COPD Audit aimed to ascertain whether such schemes were working in routine practice and if so what the models of care used were.
Methods: All acute Trusts in the UK were surveyed using two questionnaires, one relating to organisation of care and one to record clinical activity relating to 40 consecutive patients admitted with COPD from August to December 2003.
Results:Organisation: Of 193 Trusts eligible to take part 187 registered, comprising 247 hospital units. Of these, 233 had both organisational and clinical data and 103 (44%) had access to EDS. Models of early discharge were: admission prevention from A+E 5 (5%), rapid discharge <48 hours 27 (26%), assisted discharge >48 hours 24 (23%) combinations of these 12 (12%), unknown 35 (34%). A mean of 160 (median 110, interquartile range 61–217) patients were accepted by EDS in the preceding 12 months. 66 (64%) units provided a five day service, and 28 (27%) a seven day scheme. 94% ran EDS for seven hours or more per day, but there was wide variation. 83 (81%) schemes were run primarily by respiratory nurses, 11 (11%) by general nurses, two (2%) by physiotherapists, and two (2%) by both physiotherapists and nurses. General practitioners had input into five (5%) schemes. Numbers of nurses in each scheme varied from 0–5 or more. Clinical activity: Data were available for 7529 patients overall of which 1046/7126 (15%) were accepted into EDS. Within units offering EDS, 1046/3342 (31%) were accepted for EDS. Readmission rates were identical (319/990 (32%) in EDS v 635/1969 (32%) not in EDS). The two main predictors of readmission were previous admission and poor performance status. Median (mean) length of stay (LOS) in hospital was 4 (5.7) days for patients in EDS versus 7 (9.4) for those not in EDS. Median LOS in EDS was 11 days in total (that is, hospital time + EDS time). 56/904 (6%) patients in EDS presented with an initial arterial blood pH<7.26, and 112/904 (12%) with pH 7.26–7.34. 54/1011 (5%) in EDS received non-invasive ventilation during that admission. In units with EDS 90 day mortality was higher in those not accepted on to EDS (18.7% in EDS v 6.5% not in EDS).
Conclusions: About 30% of patients admitted to hospital with AECOPD appear to be suitable for early discharge, which is safe and effective. This figure is higher than that quoted in trials, perhaps because more severely ill patients are excluded from studies, but those who rapidly improve can still be considered for home care. Patients in EDS spend four days longer overall in the scheme than those not in EDS. Most units in 2003 still did not have EDS and there is wide variation in practice across the country, with the best type of scheme still unknown.
S97 THE WARM STUDY: A CASE CONTROL STUDY OF THE RISK FACTORS FOR HOSPITAL ADMISSION IN THE WINTER AMONG THE ELDERLY WITH ACUTE RESPIRATORY DISEASE
R. E. Jordan1, K. K. Cheng2, J. I. Hawker3, B. Olowokure1, J. G. Ayres4, W. Tunnicliffe for the WARM Study Investigators5. 1Health Protection R&D Unit, Department of Public Health & Epidemiology, University of Birmingham, Edgbaston, Birmingham B15 2TT; 2 Department of Public Health & Epidemiology, University of Birmingham, Edgbaston, Birmingham B15 2TT; 3Local & Regional Services Division, Health Protection Agency, 9th Floor, Ladywood House, Birmingham B2 4DY; 4Department of Environmental & Occupational Medicine, University of Aberdeen, UK; 5Critical Care Unit, Selly Oak Hospital, Birmingham, UK
Objective: To study the risk factors for hospitalisation among older people with acute respiratory disease in the winter. The aim is to identify areas of intervention to reduce hospitalisation and identify potential groups for targeting.
Design: Case control study with home interview, lung function test, and GP information.
Setting: Eighty general practices in the West Midlands and neighbouring health regions.
Participants: Patients consulting medical services with respiratory tract infection (excluding simple upper respiratory tract infection) or exacerbation of chronic respiratory disease. 158 hospitalised cases were compared to 639 controls (consulting but managed in the community) matched for age, sex, and week of consultation.
Main exposures: Social, medical, lifestyle, and health and social service organisational risk factors.
Results: Using logistic regression, adjusting for age and sex, the most important independent risk factor for admission was presence of physician diagnosed chronic disease (COPD only OR 3.4 (95% CI 1.4 to 8.4), other chronic disease OR 2.6 (95% CI 1.2 to 5.7), both OR 6.9 (95% CI 3.0 to 15.8)). Decreased mobility was also a statistically significant independent risk factor (OR (housebound) 2.9 (95% CI 1.3 to 6.5)) as was being a smoker OR 2.5 (95% CI 1.2 to 5.2) and being of white-Irish or white-other ethnic group (OR 2.6 (95% CI 1.2 to 5.6)). Living alone, or in poor housing or with low levels of income were not significant risk factors for admission. Vaccination against either influenza or pneumococcal infection did not have a significant protective effect against admissions over the full winter period.
Conclusions: Each independent risk factor above describes a clear group of patients at risk who should be easily identifiable in general practice for targeting of appropriate preventive services. The lack of protective effect of influenza vaccination may reflect the low level of circulating virus during the winter or the use of a broad time period—this needs further exploration. It is not yet clear why being of white Irish ethnic group in particular should be an independent risk factor and this result also deserves further exploration.
We gratefully acknowledge the support of our main sponsors, the British Lung Foundation.
S98 FACTORS AFFECTING SURVIVAL AFTER A HOSPITAL ADMISSION FOR AN EXACERBATION OF RESPIRATORY SYMPTOMS IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
V. Venugopal1, C. E. Bolton2, R. Aul1, M. Udiawar1, R. Cannings3, S. Hand1, D. J. Shale2. 1Prince Charles Hospital, Merthyr Tydfil, Wales, UK; 2Department of Respiratory Medicine, Cardiff University, Llandough Hospital, Wales, UK; 3Department of General Practice, Cardiff University, Wales, UK
Introduction: The recent Royal College of Physicians audit of chronic obstructive pulmonary disease (COPD) care identified significant mortality after an acute exacerbation (AECOPD). We studied possible factors affecting a poor outcome and survival, as an exacerbation may be the only contact with secondary care for such patients. It is not feasible for a respiratory physician to follow up all COPD patients. Body mass index (BMI) and low skeletal muscle mass (SMM) are general prognostic indicators but their use following an AECOPD is unknown.
Method: 103 consecutive, consenting patients (51 male) with previously proven COPD admitted with AECOPD were studied. Height, weight, BMI, spirometry, mid arm circumference (MAC), triceps skinfold thickness (TSF), inspiratory muscle strength (Pimax), creatinine height index (CHI), n = 82, an index of SMM, and circulating CRP and albumin were determined at the onset of the admission. Survival was noted following the admission.
Results: The mean (SD) age of the patients was 70.0 (10.7) years, median (range) FEV1% 45.8 (14.7 to 71.9), BMI 26.6 (6.1) kg/m2 with median length of stay of 9 (3–32) days for the initial stay. The PiMax was 28.6 (1.86) cmH2O and arm muscle area: AMA (derived from TSF and arm circumference) 48.1 (24.2) cm2. 12 patients had a BMI <20 kg/m2. A further 24 patients had a low CHI but normal BMI – hidden loss of SMM. In those that have died (n = 17) to date, BMI, CHI, albumin were lower while CRP, days in hospital, and age were greater, p<0.05 than those who have survived. FEV1% at admission was not different between survivors and non-survivors. CHI, but not BMI, was related to log PiMax (r = 0.33, p<0.01). CHI was also related to the other index of muscle mass: AMA (r = 0.427, p<0.01). To date, 77 patients have been followed up for six months. Actuarial survival, to date, is mean (95% CI) 60.7 (55.8 to 65.5) weeks. Survival for a low CHI: <80% ideal for sex and height (n = 32) was 55.2 (45.3 to 65.1) weeks and normal CHI (n = 50) 66.5 (61.2 to 71.7) weeks, p<0.05.
Conclusions: Assessment of body composition such as CHI, a simple urinary measurement, may be a useful predictive indicator of loss of SMM, impaired inspiratory muscle function, and survival following a hospital admission for AECOPD. Use of BMI and CHI rather than airways obstruction alone may assist in identifying those at a high mortality risk who need subsequent follow up or earlier interventions, such as pulmonary rehabilitation.
S99 CHRONIC OBSTRUCTIVE PULMONARY DISEASE MORTALITY: A 360 DEGREE ANALYSIS
H. S. Jenkins, J. Lazarus, J. Dungu, G. Winnett, K. L. Hattotuwa. Department of Medicine, Broomfield Hospital, Chelmsford, Essex CM1 7ET, UK
Background: The BTS/RCP National chronic obstructive pulmonary disease (COPD) audit identified differences in inpatient COPD mortality between hospitals, with a tendency to greater mortality in smaller non-teaching hospitals. COPD mortality therefore may be a useful, measurable quality indicator in Respiratory Medicine. Data quality issues may affect accurate measurement of COPD mortality from HES (Hospital Episode Statistics).
Methods: In the context of a medium sized district general hospital, which had been criticised for excess COPD mortality in a CHI (Commission for Healthcare Improvement) report, we attempted to analyse inpatient COPD mortality (ie death rate of patients admitted with a primary diagnosis of COPD) by using the following sources, during the period July 2003–June 2004: (1) Prospective audit data from the BTS national COPD audit (69 cases); (2) HES data – via CHKS Clinical Governance tool; and (3) qualitative assessment of deaths with a primary diagnosis of COPD.
Results: Inpatient mortality rate via the COPD national audit was 7%, comparable with national figures (mean 7.5%, median 7%). Inpatient COPD mortality according to CHKS was 9.8%, compared to a peer group average of 9.3%. During the study period 35 deaths were recorded with COPD as a primary diagnosis. Review of casenotes revealed that in 16 cases (46%) the diagnosis of COPD as a cause of death was either clearly inaccurate or very dubious. More appropriate diagnoses included pneumonia, lung cancer, pulmonary embolus, and ischaemic heart disease. Several originated from surgical wards with no physician input.
Conclusions:
-
HES data overestimated COPD mortality.
-
The main cause was inaccurate death certification.
-
These effects observed locally may be occurring nationwide.
-
Mortality assessment is better via a multifaceted approach. Routine use of HES data may be useful over the longer term if data quality and death certification are improved.
S100 NON-ACIDOTIC CHRONIC OBSTRUCTIVE PULMONARY DISEASE EXACERBATIONS REQUIRING HOSPITAL ADMISSION: WHAT HAPPENS TO PATIENTS FIVE YEARS ON?
S. Majid, A. Kwok, L. Davies. Aintree Chest Centre, University Hospital Aintree, Lower Lane, Liverpool L9 7AL, UK
Exacerbations of chronic pulmonary obstructive disease (COPD) are the commonest respiratory cause of hospital admission, accounting for around 1500 admissions annually in our hospital. The Acute Chest Triage Rapid Intervention Team (ACTRITE) was developed in 1999 to provide a hospital at home service for patients who would otherwise require hospital admission with non-acidotic exacerbations of COPD. (
). In this initial study, 150 patients were randomised to “hospital at home” care or conventional hospital admission.
five years after initial recruitment to the ACTRITE study, we carried out a retrospective casenote audit on a random selection of 97/150 of these patients. At recruitment, mean (SD) age 74 (7) years, FEV1 0.71 (0.29) l, 55% female, 35 (37%) current smokers. During the period of follow up 18/35 (51%) patients successfully quit smoking. 76/97 (78%) patients were readmitted, due to any cause, to our hospital at least once over the five years, accounting for 3003 bed days. These 76 patients had 272 episodes of hospital admission, with an average readmission rate of 2.8 per patient in five years. Only 21 patients had no further hospital admissions, 61 had 1–5, 12 had 6–10, two had 11–15, and one patient had more than 16 admissions. Only eight patients reused the ACTRITE service.
During admissions for COPD exacerbations, 24/76 (32%) patients were treated with one or more of the following; intravenous aminophylline, doxapram, NIV, and IPPV. These interventions were used 63 times during the 272 admissions (23%). Aminophylline was used during 38 admissions, doxapram during 10, NIV during six, and IPPV during four admissions. At five years, no patient receiving doxapram or IPPV was alive, and there was only one survivor in the NIV treated group. More patients treated with one of the above interventions had died compared to those who had not received these treatments (22/24 (92%) v 37/73 (51%); χ2<0.001).
Only 38 patients survived at five years. Of those dying, more than two thirds died from a respiratory illness (29 COPD/respiratory failure, 6 lung cancer, 4 pneumonia). In 11 patients, the cause of death was not documented. Survival at five years was no different in those patients initially managed by the “hospital at home” service compared to hospital admission. Neither the initial presciption of LTOT (20/97, 7 survived) nor inhaled corticosteroids (80/97, 29 survived) affected five year survival.
The five year survival in this group of COPD patients initially presenting with non-acidotic exacerbations was poor. The great majority were readmitted, often on multiple occasions and many required “respiratory support” on subsequent admissions. Few patients reused the hospital at home service. The reasons for this need further study, but may be related to the severity of subsequent exacerbations.
Smoking cessation
S101 PERCEIVED SAFETY OF NICOTINE REPLACEMENT PRODUCTS AMONG GENERAL PRACTITIONERS IN THE UK: IMPACT ON UTILISATION
D. M. G. Halpin1, A. Bobak2, J. Bery3. 1Department of Respiratory Medicine, Royal Devon & Exeter Hospital; 2The Medical Centre, Garrett Lane, Wandsworth; 3Path House Medical Practice, Fife, UK
Despite nicotine replacement therapy (NRT) being a safe and effective aid for smoking cessation, most smokers try to quit without it. All GPs see smokers and the damage caused by smoking as part of their daily work. On average, GPs said that 16 patients per week were given advice on smoking cessation.
Following recent publications demonstrating smoker misconceptions on nicotine safety we investigated the understanding of nicotine safety among general practitioners (GPs). An internet survey that included questions regarding the safety of nicotine and NRT was answered by 205 UK GPs. GPs with nicotine safety misconceptions were defined as those who either agreed or neither agreed nor disagreed with statements indicating that nicotine in NRT or cigarettes is harmful.
While few GPs (6%) endorsed the statement that “stop smoking products with nicotine are just as harmful as cigarettes” more than one in six (16%) neither agreed nor disagreed with the statement. Hence, approximately 22% met the criteria of having nicotine safety misconceptions.
Furthermore, a substantial proportion of all GPs incorrectly asserted that nicotine in cigarettes causes cardiovascular disease (51%), strokes (49%), or lung cancer (41%), with a further 20–27% being unsure. The respective percentages for those agreeing that nicotine in stop smoking products cause these conditions were 11%, 8%, and 5%, with a further 22–33% being unsure. Despite this, GPs with safety misconceptions were no less likely to prescribe NRT.
In a second study of 2062 GB residents, all respondents who reported being smokers (30%; n = 605) were asked about their attitudes towards smoking and smoking cessation products. A large proportion of smokers (69%) had nicotine safety misconceptions when comparing NRT and cigarettes and less than one in three smokers correctly believe that NRT does not cause heart attacks (26%), lung cancer (29%), strokes (25%), or asthma (30%). Smokers who expressed safety concerns around nicotine in NRT were less likely to use it during future quit attempts (24% v 51%; p<0.001) and were more likely to attempt to quit unassisted (49% v 31%; p<0.01).
There are significant misconceptions among GPs about the safety of nicotine. These need to be addressed in order to reassure smokers regarding the safety of NRT.
This study was supported with a grant from GlaxoSmithKline Consumer Healthcare.
S102 CUTTING DOWN SMOKING THEN STOPPING WITH NICOTINE REPLACEMENT THERAPY: AN INNOVATIVE APPROACH TO SMOKING CESSATION
P. Tonnesen1, T. Danielsson2. 1Department of Pulmonary Medicine, Gentofte University Hospital, Hellerup, Denmark; 2Pfizer Consumer Healthcare, Helsingborg, Sweden
Background: One quarter of the UK population currently smoke. Smoking cessation rates are dependent on the number of smokers making quit attempts, but fewer than 30% of smokers try to stop each year. Many smokers are unable or not ready to abruptly stop smoking. We investigated whether reducing smoking with the aid of NRT could be a prelude to quitting for smokers not ready to abruptly stop.
Methods: A total of 2424 smokers were enrolled in six, double blind, randomised, placebo controlled trials. The studies enrolled adult smokers who were smoking at least 15 cigarettes per day (cpd), had smoked for at least three years and had failed at least one serious quit attempt. At baseline, all subjects were unable or unwilling to quit abruptly, but wanted to reduce their smoking. Two studies used the nicotine inhaler, and four studies used nicotine gum. Subjects were randomised to active or placebo NRT, and instructed to cut down their smoking as much as possible. Successful smoking reduction was defined as a reduction in cpd by at least 50% versus baseline, sustained from week 6 to month 4, verified by a sustained decrease in carbon monoxide. The effect of reducing smoking on subsequent cessation, and safety of concomitant use of NRT and smoking, were also evaluated.
Results: NRT was superior to placebo in achieving sustained smoking reduction. At four months, 15.9% (193/1215) of subjects using NRT had reduced their smoking by 50%, compared to 6.7% (81/1209) in the placebo group. Successful smoking reduction promoted cessation; at one year, seven day point prevalence cessation rates were 8.2% in the NRT group versus 4.1% in the placebo group (odds ratio 2.1, 95% CI 1.4 to 2.8). In the active treatment group, one third of subjects who had successfully reduced their smoking at four months were abstinent at one year (58/193 subjects). At study end, most subjects (60–80%) were more interested in quitting than at baseline. Concomitant use of nicotine gum or inhaler and smoking was well tolerated. The most common adverse events were hiccups and nausea with nicotine gum, and cough and throat irritation with nicotine inhaler.
Conclusions: NRT is twice as effective as placebo at helping smokers to cut down their smoking. Cutting down promotes cessation in smokers not ready to abruptly stop; one third of smokers who reduced their cigarette consumption by half with NRT stopped smoking within one year. This treatment strategy could boost the number of smokers attempting to quit.
S103 SMOKING ATTITUDES OF HOSPITAL STAFF: A FOLLOW UP SURVEY
A. Ponnuswamy, I. A. Campbell. Department of Chest Diseases, Llandough Hospital, Penarth CF64 2XX, UK
Introduction: Health care staff constantly encounter to patients with tobacco related conditions. Their views and attitudes may be different to the general public. It would be advantageous to capitalize on these attitudes to effect policies both in hospitals and public places. Two earlier surveys from this hospital were reported in 1989 and 1991. We have re-surveyed these attitudes to assess changing trends.
Methods: In February 2005, anonymous questionnaires were sent out to each paid member of staff working at the Llandough site. Data collected included like age, sex, smoking, and professional status. The survey also examined knowledge about risks both of active and of passive smoking, attitudes towards smoke free public places including the hospital campus and concepts regarding cessation. A deadline of six weeks was fixed for the return of completed questionnaires. Most of the questionnaires were distributed personally by Dr AP to maximise the response rate.
Results: A total of 1565 questionnaires were distributed. The responses were received from 69% in comparison to 70% in 1987 and 82% in 1991. Eight hundred and forty six (78%) were females and 21% were males. Among the respondents, 14% were smokers, 66.5% non-smokers, and 19% ex-smokers. Nurses had the highest rate of smoking (87%) compared to previous studies wherein the porters, catering, and domestic staff were predominantly smokers. Awareness of the risks of active smoking as a cause of heart disease, lung cancer, and chronic obstructive pulmonary disease (COPD) ranged from 97 to 99%. However the knowledge of the risks of passive smoking in relation to heart disease, lung cancer and COPD was less good. Only 78% felt passive smoking was a risk factor for stroke. Eighty four per cent of staff wanted smoking banned in public places. Seventy five per cent of the staff population felt that risks fell after cessation. Less than 2% believed that cessation strategies did not work, while 45% felt they worked. Seventy per cent felt that designated smoking areas should be made available for patients whilst 55% felt that staff need a designated area for smoking. Only 20% felt that their jobs were affected by their own smoking habits or those of their colleagues. The proportion of employees who wanted designated areas for patients had increased from 56% in 1991 to 70%.The need for staff smoking areas had come down form 60 to 55% and that for visitors was reduced by 3% to 41%.
Conclusion: This study has identified that the incidence of smoking has declined from 20% to 14% in the last 14 years and the proportion of ex-smokers has increased from 15 to19%. Nurses had a higher rate of smoking than others. Majority of the smokers belong to the age group 25–45 years which gives us a clear indication that smoking cessation strategies are required for this group. Education needs have been identified with regards to the risks of passive smoking and in relation to the advantages of cessation advice and treatment.
S104 SMOKING CESSATION IS ASSOCIATED WITH A SUSTAINED INCREASE IN BODY MASS INDEX
B. Patel1, R. Luben2, A. Welch2, S. Bingham2, K. T. Khaw2, N. Day2, N. Wareham2. 1Royal Devon & Exeter Hospital; 2Institiute of Public Health, University of Cambridge, UK
Introduction: Smoking cessation is associated with an increase in weight. However, little is known about whether the increase in weight is transient or sustained. Using data from the EPIC-Norfolk cohort, we looked at the association between smoking status and body mass index (BMI). In ex-smokers we also looked at the association between the period of abstinence and BMI.
Methods: Data were collected from 25 442 individuals, age 45–75 years, recruited from general practices in and around Norwich, UK. Between 1993 and 1997 all participants attended for a health a check at which height and weight was measured. They also completed a health and lifestyle questionnaire that included detailed questions on smoking history.
Results: Data were available for 11 681 non-smokers, 10 781 ex-smokers, and 2980 current smokers. After adjustment for age and sex, current smokers had a lower BMI (mean 25.7 kg/m2, 95% CI 25.6 to 25.9), and ex-smokers a higher BMI (26.8 kg/m2, 26.7 to 26.8) than non-smokers (26.2 kg/m2, 26.1 to 26.2, p<0.001 for difference between groups). The mean time of abstinence in ex-smokers was 20.0 years (SD 11.8 years), and each year of abstinence was associated with a reduction of age and sex adjusted BMI of −0.03 kg/m2 (p<0.001). The table shows the relation between period of abstinence and difference in age and sex adjusted BMI in ex-smokers relative to non-smokers.
Conclusion: Smoking cessation is associated with a long term increase in BMI. However, the increase in BMI is relatively small over the medium to long term and any adverse health effects of this are likely to be small in relation to the health gains from smoking cessation.
Abstract S104
S105 WHERE DO SMOKERS PREFER THEIR SMOKING CESSATION SERVICE TO BE BASED?
K. E. Lewis1,2, H. Rajanna1, J. Murphy1, O. Edgewhere1, P. Crossland1. 1Carmarthenshire NHS Trust; 2School of Medicine, Swansea University, UK
Introduction: Attendance to smoking cessation services has been variable. In other healthcare settings, siting the location of the service according to patient’s preferences has improved attendance. This may be especially important, if patients are expected to recurrently travel when they do not perceive themselves to be unwell. We asked smokers in two different healthcare settings to chose where they would most prefer any smoking cessation service to be located.
Methods: Concurrent, cross sectional surveys of (62) consecutive patients attending a general respiratory clinic and a random sample of (120) patients attending a GP practice for a variety of reasons. Sampling was continued until we interviewed 40 current smokers, >16 years old, in both areas. Ex and non-smokers all had exhaled CO <4 ppm. No patient refused to participate. Patients completed the questionnaires anonymously and away from interviewers. They could choose only one option. The proportions preferring each option was compared between both groups by χ2. As expected, our chest clinic group comprised of slightly more males (47% v 37%, p = 0.37), of older age (mean 65 v 51 years, p<0.001) with a heavier smoking history (median 37 v 15 pack years, p = 0.01).
Results: The table illustrates the proportion preferring each option.
Conclusions: smokers tend to prefer a service to be based where they are already attending. Importantly, the majority of smokers already attending secondary care would like their service to be wholly or partially based in secondary care. Funding a service exclusively in only one setting could adversely affect attendance rates and could exclude many smokers, already at high risk with comorbidity. A unified service covering both secondary and primary care may result in better attendance, and reflect local health needs more.
Abstract S105
S106 TEENAGE SMOKING IN HOSPITALS: A SURVEY OF ALL WELSH PAEDIATRIC UNITS
N. Pickerd, S. Morris, M. Pierrepoint. Nevill Hall Hospital, Abergavenny, UK
Introduction: Approximately 22% of 15 year olds smoke regularly, girls more than boys. A problem faced by staff in hospitals is the patient under 16 years of age requesting to smoke. On one hand it is their duty to promote adolescents health, but they also have the duty of care to look after adolescents who have to leave the ward to smoke. Are teenagers therefore indirectly supported by hospital staff to smoke when research in adults has shown that smoking cessation intervention in hospital can be effective (
)?
Aims: To assess how hospitals are dealing with teenagers requesting to smoke while admitted and if policies are in place to ensure adolescents health promotion.
Methods: We contacted the nurse in charge of adolescent inpatient services of all 13 hospitals in Wales admitting children and of five tertiary referral hospitals for Welsh children in England and conducted a standardised structured telephone interview.
Results: All hospitals had experienced patients under 16 years of age wanting to smoke while admitted to the ward. This occurred once per week in 8/18 units (Wales 6/13, England 2/5), once per months in 6/18 units (Wales 5/13, England 1/5) and a few times per year in 4/18 units (Wales 2/13, England 2/5). A designated adolescent ward was there in 6/18 hospitals (Wales 4/13, England 2/5). None of the 18 hospitals had a formal policy on patients under 16 wanting to smoke while in hospital. One unit admitted patients under 16 who wanted to smoke routinely to an adult ward and one hospital in Wales and one in England were formulating a policy on teenage smoking. A smoking area within the hospital was there in 16/18 (Wales 12/13. England 4/5). None of the hospitals allowed patients under 16 to go to the smoking area alone, 5/17 (Wales 3/12, England 2/5) only allowed the patients to go there if a parent accompanied them and in 12/17 (Wales 9/12. England 3/5) units nursing staff would accompany the patient to the smoking area. There were no data available from the hospital who admitted the patients to an adult ward. Help with smoking cessation was offered in 10/18 hospitals (Wales 6/13, England 4/5). These were smoking cessation leaflets alone (4), together with some form of verbal advice (2), together with counseling (1), verbal advice alone (2), or counseling alone (1).
Conclusion: Smoking in patients less than 16 years of age in hospitals is a common problem and more than two thirds of adolescent services are complicit in it. There is a need for clearly written policies and initiatives for smoking cessation.
Occupational lung disease
S107 POSITIVE SPECIFIC BRONCHIAL CHALLENGES DESPITE NORMAL BRONCHIAL HYPERRESPONSIVENESS
A. Brant, J. Arbery, P. Cullinan. Department of Occupational and Environmental Medicine, Royal Brompton Hospital, London SW3 6LR, UK
Introduction: It is commonly believed that a normal response to inhaled histamine (or metacholine) helps exclude a diagnosis of occupational asthma. Specific bronchial challenge is probably the gold standard in the diagnosis of occupational asthma. We reviewed our specific bronchial challenges to see whether the outcome was determined by pre-challenge bronchial hyperresponsiveness.
Method: We reviewed all the specific bronchial challenges that had been undertaken at the Royal Brompton Hospital from 1995 until 2005. A positive response was defined as a replicated and dose-dependent fall in FEV1 following exposure to a workplace allergen. Before each challenge PC20 was measured to incremental concentrations (0.03–16 mg/ml) of inhaled histamine.
Results: 123 patients underwent a specific bronchial challenge over this period. 52 tests were positive, 71 negative, and five were inconclusive. Of those with PC20<2.0 mg/ml prior to challenge 71% (n = 17) had a positive response; for those with PC20 between 2.0 mg/ml and 8 mg/ml this figure was 27% (n = 15), and for those with PC20>8 mg/ml 46% (n = 91). Of those with a PC20>16 mg/ml 40% (n = 33) had a positive bronchial challenge.
Conclusion: A normal response to inhaled histamine does not predict the response to specific bronchial provocation testing and cannot be used to exclude a diagnosis of occupational asthma.
S108 CROSS SHIFT CHANGES IN FEV1 BEST PREDICT WORK RELATED RESPIRATORY SYMPTOMS IN TEXTILE WORKERS
R. M. Barraclough, R. Lewis, M. Henson, C. Warburton, D. Fishwick. Health & Safety Laboratory, Harpur Hill, Buxton, Derbyshire SK17 9JN, and University Hospital Aintree, Longmoor Road, Liverpool L9 7AL, UK
Exposure to textile dust is characteristically associated with airways disease and byssinosis, although other respiratory conditions such as occupational asthma are described. While work related respiratory symptoms are common in these workers, little is known about the acute pulmonary response to such exposures, and the relation between serial PEF patterns, airway responsiveness, and across shift changes in FEV1.
We studied 34 cotton exposed, and 19 manmade fibre exposed textile spinners, with a mean age of 45 years (range 18–63). 64% were male, and 49% current smokers. All completed a modified MRC respiratory questionnaire, and underwent resting and across shift FEV1 measurement, and serial PEF measures analysed by OASYS 2 software. A positive work effect index was taken as those over 2.5. In addition, non-specific assessment of airway responsiveness was made using histamine.
The prevalence of work related symptoms were as follows; chronic bronchitis cotton workers 26.5% (manmade fibre 0%), persistent cough 11.8% (21.1%), chest tightness 17.7% (10.5%), wheeze 20.6% (10.5%), and dyspnoea 11.8% (5.3%).
Both work related cough and chest tightness were associated with an exaggerated across shift fall in FEV1 on the first working day of the week (for example, work related cough 8% fall, no cough 2% rise, p = 0.006). Work related wheeze was also associated with cross shift change in FEV1, but only on the 4th working day of the week (work related wheeze 4.1% fall, no wheeze 1.6% rise, p = 0.023). There was no significant relation between work related symptoms and OASYS scores.
However, positive OASYS scores (suggesting a work effect on serial PEF patterns) were associated with airway responsiveness measurements. Five of the seven workers with a positive OASYS score had evidence of airway hyperresponsiveness, in comparison to 12 of the 46 with a negative OASYS chart (p = 0.017). Analysis of log dose response slopes confirmed this difference (p = 0.05).
Our results suggest that although serial PEF measures are the mainstay of investigating work related respiratory symptoms, and did relate to airway responsiveness, in this population across shift changes in FEV1 were more closely associated with work related respiratory symptoms.
S109 FALL IN THE INCIDENCE OF OCCUPATIONAL ASTHMA FOLLOWING AN INTERVENTION IN A DETERGENT ENZYME FACTORY
A. Brant, C. Zekfeld, J. Helms, F. Barnes, A. J. Newman Taylor, P. Cullinan. Department of Occupational and Environmental Medicine, Royal Brompton Hospital, London SW3 6LR, UK
Introduction: Few studies have investigated the effectiveness of a primary intervention programme to prevent occupational asthma in a workforce; and fewer still have reported associated changes in disease rate. Following a very large outbreak of occupational asthma in a European detergent factory, the company implemented new work practices and re-engineered their production methods in 1998. Subsequently, measured personal and static dust and enzyme exposures fell steeply. We investigated whether the incidence of occupational asthma had also fallen.
Method: We undertook two cross sectional surveys, in 2000 (n = 414) and 2002 (n = 292), following the factory improvements in 1998. These surveys included questionnaires on respiratory symptoms and measurement of specific IgE to detergent enzymes. We compared those individuals who had started employment 2.5 years before the changes in 1998 to those who started employment after 1998.
Results: In new employees the annual incidence of work-related chest symptoms fell from 11% to 3% and specific enzyme sensitisation from 12% to 7%. The incidence of the combination of specific sensitisation and work related chest symptoms, a marker of occupational asthma, fell from 6% to 2%.
Conclusion: Our findings demonstrate a reduction in the incidence of occupational asthma in new employees, which was associated with a reduction in measured airborne enzyme concentrations, following an intervention programme within a detergent enzyme factory.
Supported by BOHRF.
S110 THE RESPONSE OF HUMAN ALVEOLAR MACROPHAGES TO THE STIMULI OF COTTON DUST AND CYCLIC PRESSURE
S. Mylchreest1, D. Singh2, J. G. Andrew3, C. Starkey2, C. E. Evans1. 1Laboratory and Regenerative Medicine, Medical School, University of Manchester UK; 2Northwest Lung Research Centre, Wythenshawe Hospital, Manchester UK; 3Department of Orthopaedic Surgery, Ysbyty Gwynedd, Bangor UK
Cotton dust causes respiratory diseases such as chronic bronchitis and byssinosis. The effects of cotton dust particles on lung cells are poorly understood. We have previously shown in peripheral blood macrophages that there is a synergistic effect of particulate matter and cyclic pressure on macrophage activation.1 We proposed that this may also be the case for alveolar macrophages (AM). We have studied the effects of cotton dust particles and cyclic pressure changes (to study conditions similar to those during respiration) on AM.
Broncho-alveolar lavage (BAL) samples were obtained from eight subjects (age range 41–65 years, 6 male and 2 female, 4 current smokers with normal lung function, 2 ex-smokers of which 1 had COPD, and 2 non-smokers) undergoing investigative bronchoscopy. BAL was filtered, centrifuged and the washed cells resuspended in culture medium. AM were isolated by adherence, seeded at a density of 5×105/ml and cultured for 48 hours.
Cultures were exposed to cotton particles (⩽40 μm) for 24 hours before being subjected to hydrostatic cyclical pressure in our unique pressure device. Pressure regime was one hour at 3psi (20.7 kPa), two seconds on/off.
Abstract S110 Synthesis of cytokines by alveolar macrophages (pg/ml, mean (SE))
Media was removed from cultures 23 hours post-pressure and analysed for TNFα, IL-1β, and IL-6 by ELISA. TNFα, IL-1β, and IL-6 were significantly increased by exposure to either pressure (non-parametric Wilcoxon Rank Signs Test p<0.001 for TNFα and IL-6, p<0.028 for IL-1β) or cotton dust (p<0.001). Cultures exposed to both stimuli showed a dramatic increase in cytokine synthesis when compared to either stimulus alone or to the controls (p<0.001).
Exposure to both stimuli was found to have a synergistic effect on TNFα and IL-1β production and an additive effect on IL-6. Cyclical pressure is an important modulator of AM activity. The mechanism of synergy with cotton particles for induction of pro-inflammatory cytokine production requires further investigation.
1
S111 NON-INVASIVE MEASUREMENT OF MARKERS OF OXIDATIVE STRESS IN ASBESTOS INDUCED LUNG DISEASE
C. P. Campbell1, A. S. Jackson1, S. Chow1, P. S. Thomas2, D. H. Yates1. 1Thoracic Medicine, St Vincent’s Hospital, Sydney, Australia 2010; 2Prince of Wales Hospital, Sydney, Australia
Introduction: Oxidative stress may play a role in the pathogenesis of adverse effects of asbestos in the lung. Collection of exhaled breath condensate allows measurement of hydrogen peroxide, 8isoprostane and other markers, and exhaled nitric oxide can be measured directly by chemiluminescence. We report our findings in subjects attending the Dust Diseases Board (DDB) of New South Wales with different asbestos conditions.
Methods: Patients attending the DDB for screening of asbestos related diseases were invited to participate. All had a confirmed history of workplace exposure to asbestos. Examination, radiology, and lung function were performed by the DDB, and a diagnosis made of: normal, asbestosis, pleural plaques, or asbestos related diffuse pleural thickening ARPD, according to international guidelines. The patients were asked questions regarding potential confounding factors: sinusitis, recent upper respiratory tract infection, asthma/COPD or obstructive spirometry, inhaled or oral steroids. They then underwent collection of exhaled breath condensate over 10 minutes, which was then frozen and analysed later for oxidative markers. They also performed exhaled nitric oxide measurements.
Results: 125 patients were studied in total. After excluding those with potential confounding factors, 70 were analysed: 33 controls, 16 pleural plaque, 12 asbestosis, and nine ARPD-diffuse pleural thickening (see table). Hydrogen peroxide levels in EBC, and FeNO levels were significantly higher in asbestosis than normal subjects.
Conclusion: Markers of oxidative stress appear to be raised in asbestosis compared to normal controls and other asbestos conditions.
Supported by funding from the Dust Diseases Board of New South Wales, Australia.
S112 INVESTIGATION OF AN OUTBREAK OF ALVEOLITIS IN A CAR ENGINE MANUFACTURING PLANT
W. Robertson1, A. S. Robertson2, C. Burge2, V. Moore2, P. S. Burge2. 1Public Health, Warwick Medical School, University of Warwick; 2 Occupational Lung Disease Unit, Birmingham Heartlands Hospital, UK
Eleven workers from a car engine manufacturing plant were diagnosed as having extrinsic allergic alveolitis (EAA) from 2003 to May 2004. The plant machined aluminium alloy and cast iron, using metal working fluid (MWF) for lubrication & cooling. Similar outbreaks in the USA have been linked to MWF (
).
The aim of a three phase investigation was to identify other affected workers and provide epidemiological data to help identify the cause: In total, 86 workers have been diagnosed as having probable or definite work related respiratory disease, including 20 with EAA, seven with humidifier fever, 73 with occupational asthma, and one lipoid pneumonitis. Some had more than one disease. 10% of the workforce are affected (disease ratio 10.3 per 100 (95% CI 8.4 to 12.5)).
Abstract S112
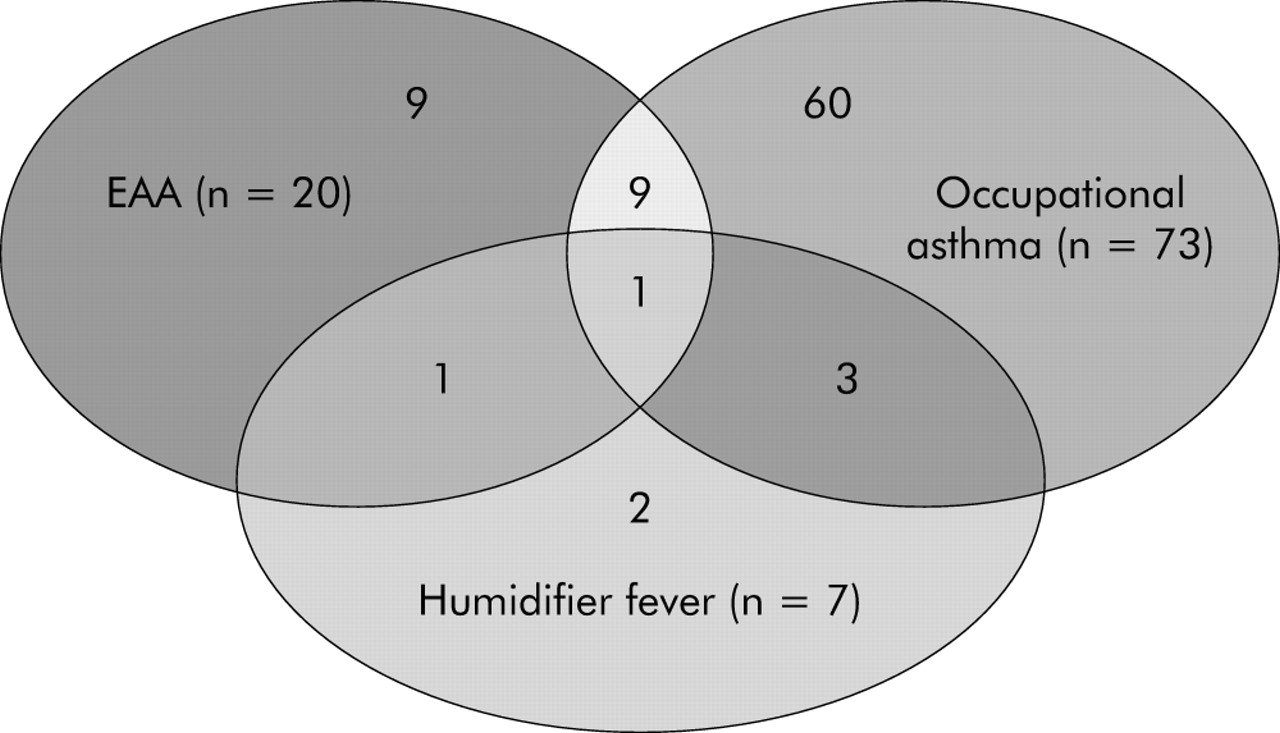
The “epidemic curve” of the onset of work related breathlessness showed a large peak in March 2003, three months after a new hydraulic oil was introduced which contaminated the MWF. Four work locations in the factory have a significantly higher ratio of disease, which has focused the investigation on the MWF and washers in these locations. There is a wide range of occupational lung disease at the factory, likely to be related to contaminated aerosol from the MWF or washer fluids.
Sleep disordered breathing and obstructive sleep apnoea
S113 SCREENING QUESTIONNAIRES IN PATIENTS REFERRED TO A SLEEP CLINIC CANNOT PREDICT WHICH INDIVIDUALS DO NOT REQUIRE CONTINUOUS POSITIVE AIRWAY PRESSURE TREATMENT FOR OBSTRUCTIVE SLEEP APNOEA
S. M. Menzies, J. R. Stradling. Oxford Centre for Respiratory Medicine, Churchill Hospital, Oxford OX3 7LJ, UK
Introduction: A questionnaire that could reliably identify individuals referred to the sleep clinic that will not subsequently require treatment for obstructive sleep apnoea (OSA) with continuous positive airway pressure (CPAP), would reduce unnecessary sleep studies, follow up, associated costs, and longer waiting lists.
Methods: From May 2004, all new letters of referral to the Oxford Sleep Unit were sent back to the referring doctor with a questionnaire for the patient to complete. This contained questions on snoring, apnoea and choking history during sleep, neck circumference, weight, and an Epworth Sleepiness Score (ESS). Direct Sleep Studies and subsequent follow up plans were organised in the usual way following receipt of the completed questionnaire. Referrals returned with completed questionnaires from May to December 2004 were audited, and sleep study and outcome information were recorded for each case.
Results: 208 referrals were sent questionnaires, of which 128/208 (63%) were returned completed and included in the study. 77/208 (37%) were never returned, and hence no further investigations were organised. An additional 55 patients were referred in the first instance with a fresh copy of our questionnaire generated by the general practitioner. A total of 163 patients were audited, 98% of whom were able to correctly complete the questionnaire. Sleep Study (SS) information was available in 152 cases (11 patients did not attend). 97/152 (60%) of the audited referrals were subsequently not offered CPAP, based on the SS and, in most cases, the outpatient review. There was no significant difference between this group, and the group offered CPAP (n = 66), in the snoring or apnoea history, or the neck circumference. Patients not offered CPAP were more likely to “never choke” during sleep (52% v 35%), and less likely to “sometimes choke” (20% v 41%) (p = 0.027, χ2 test). A higher percentage of non-treated patients had an ESS<10 (36% v 12%) (p = 0.001, χ2 test).
Conclusions: This study demonstrates that a screening questionnaire for sleep clinic referrals can be successfully completed, but cannot predict adequately who does not merit OSA treatment with CPAP. This may be because patients have usually undergone an initial “screen” in primary care, and hence predictors identified when screening a general population do not apply to this already preselected population. To our surprise, it prevented 37% of referrals being re-referred, and reasons for this are unknown. Reasons for non re-referral, and whether some cases of OSA have been missed, cannot be established. Using the ESS to screen this population is also unreliable, as some cases of OSA requiring treatment will be missed.
S114 DAYTIME ACTIVITY LEVELS AND SLEEP FRAGMENTATION IN MILD TO MODERATE CONGESTIVE HEART FAILURE PATIENTS WITH SLEEP DISORDERED BREATHING
P. C. Hastings1, A. Vazir1,2, M. Dayer2, D. M. O’Driscoll1, M. R. Cowie2, M. J. Morrell1, A. K. Simonds1. 1Sleep & Ventilation and 2Cardiac Medicine, National Heart & Lung Institute, Royal Brompton Hospital, UK
Introduction: Sleep disordered breathing (SDB) is common in patients with severe congestive heart failure (CHF) (Javaheri et al, 1998, Sin et al, 1999). Yet, unlike patients with obstructive sleep apnoea (OSA), CHF patients with SDB frequently do not report subjective symptoms of daytime sleepiness, although objective sleepiness may be increased (Pepperell et al, 2003). We hypothesised that CHF patients with SDB would have decreased daytime activity, compared to CHF patients with no SDB (NoSDB), which may explain the lack of excessive daytime sleepiness.
Methods: 24 hour activity levels, subjective and objective measures of daytime sleepiness where measured in 39 CHF patients, NYHA class 2–3, on optimal medication. 22 had SDB, 17 had no SDB. SDB was defined as an Apnoea-Hypopnoea Index (AHI) ⩾15 events/hour. Patients were assessed by; 24 hour activity monitoring (actigraphy) worn for up to 14 days; daily sleep diaries; a single objective sleepiness test (OSLER), and the Epworth Sleepiness Scale (ESS). Ethical approval was given and signed informed consent obtained by all patients.
Results: The duration of daytime activity was significantly shorter in the SDB group compared to no SDB group. The SDB group had increased time in bed (TIB) and poorer sleep quality, as shown by fragmentation index (see table). There was no difference between the groups with and without SDB for ESS, yet objectively (OSLER) the SDB group was significantly sleepier. Polysomnography showed no significant differences in the sleep architecture between the two groups.
Abstract S114
Conclusion: CHF patients with SDB are less active during the day than a group of matched CHF patients without SDB, and show objective daytime sleepiness without reporting subjective daytime sleepiness. We speculate that CHF patients with SDB may underestimate their daytime sleepiness symptoms due to reduced activity levels throughout the day. A further explanation for the lack of subjective daytime sleepiness is that despite significant sleep fragmentation, CHF patients with SDB are able to maintain relatively normal levels of slow wave sleep.
Funding: British Heart Foundation, Wellcome Trust, & ResMed UK.
S115 ACUTE CARDIOVASCULAR RESPONSE TO AROUSAL IN OBSTRUCTIVE SLEEP APNOEA BEFORE AND AFTER CONTINUOUS POSITIVE AIRWAY PRESSURE TREATMENT
D. M. O’Driscoll, A. K. Simonds, M. J. Morrell. Clinical and Academic Unit of Sleep and Breathing, National Heart and Lung Institute, Imperial College, Royal Brompton and Harefield NHS Trust, London, UK
Background: In obstructive sleep apnoea (OSA), the acute surge in blood pressure (BP) associated with an arousal from sleep at the termination of an apnea is more than double that to a spontaneous arousal (Davies et al, J Appl Physiol (1993); Okabe et al, Thorax (1995)). We tested the hypotheses that the cardiovascular response to an arousal at the termination of an obstructive apnoea is determined by the increasing ventilatory effort (negative intrathoracic pressure), and that the augmented cardiovascular response to arousal is reduced following continuous positive airway pressure (CPAP) treatment.
Methods: Interventional study: The BP and heart rate (HR) response to arousals were measured at the termination of obstructive apneas/hypopneas induced by rapid CPAP pressure dialdowns (from optimal pressure (mean (SEM) 10.5 (0.9) cmH2O) to 2 cmH2O) in 13 male OSA patients (mean age 54.2 (SD 2.8) years; AHI, 75.7 (10.4) events per hour). Non-interventional study: The BP and HR response to arousals were also measured during spontaneous obstructive apneas/hypopneas (that is, patients were not on CPAP) before and after three months CPAP treatment. Obstructive events were closely matched within patients for length and subsequent oxygen desaturation. The Brompton and Harefield Ethics Committee approved this study and all subjects gave written informed consent.
Results: Interventional study: The increases in mean BP and HR to an arousal from sleep at the termination of an obstructive apnea/hypopnea were weakly but significantly correlated with the change in negative intrathoracic pressure (BP, r = −0.39, p = 0.009. HR, r = −0.50, p<0.001). Whereas the increases in mean BP and HR were not significantly correlated with the length of the obstructive event (BP, p = 0.37. HR, p = 0.90) or the subsequent oxygen desaturation (BP, p = 0.27. HR, p = 0.12). Non-interventional study: The increases in mean BP and HR associated with arousal at the termination of an obstructive apnea/hypopnea were reduced post CPAP treatment, although only the change in mean BP reached statistical significance (BP, Pre CPAP, 28.2 (3.3) mm Hg; Post CPAP, 22.2 (2.0) mm Hg; p = 0.04. HR, Pre CPAP, 17.8 (2.4) bpm; Post CPAP, 16.9 (1.4) bpm; p = 0.67).
Conclusion: The cardiovascular response to arousal from sleep at the termination of an obstructive apnoea is linked to the level of increasing ventilatory effort. Furthermore, CPAP treatment in OSA reduces the acute cardiovascular response to arousal from sleep to levels achieved in healthy individuals. We speculate that CPAP treatment not only normalises sleep and ventilation in patients with OSA, but also normalises the acute cardiovascular response to arousal from sleep thereby reducing cardiovascular risk.
Funding: Wellcome Trust.
S116 PATIENTS WITH OBSTRUCTIVE SLEEP APNOEA HAVE IMPAIRED CARDIAC METABOLISM AND DIASTOLIC DYSFUNCTION COMPARED TO CONTROLS
S. D. West1, M. Scheuermann-Freestone2, G. C. Watson2, D. J. Tyler2, J. M. Francis2, S. Neubauer2, J. R. Stradling1, K. Clarke2. 1Oxford Centre for Respiratory Medicine, Churchill Hospital, Oxford; 2University of Oxford Department of Physiology and Centre for Clinical Magnetic Resonance Research, John Radcliffe Hospital, Oxford, UK
Introduction: Obstructive sleep apnoea (OSA) is associated with increased cardiovascular morbidity and mortality. In the normal adult heart, free fatty acids (FFA), glucose, and lactate are metabolised for ATP production in the mitochondria. Increased fatty acid availability results in increased FFA uptake and oxidation in the mitochondria which decreases the amount of ATP produced per molecule of oxygen consumed in the mitochondrial electron transport chain. Previous work has found that patients with heart failure have impaired cardiac function and energy metabolism which is negatively correlated with raised FFA levels, but it is unknown whether cardiac energetics or function are altered in patients with OSA.
Methods: We measured fasting circulating metabolites and cardiac high energy phosphate metabolism (phosphocreatine PCr/ATP ratios) and function using magnetic resonance (MR) spectroscopy and imaging respectively, in 19 patients with untreated obstructive sleep apnoea (mean >4% dip rate/hour 26.1, range 10.2–57.6, mean ESS 15.4, range 10–24) and normal cardiac function as assessed by echocardiography and compared them with 15 age, sex, and body mass index matched control subjects.
Results: Fasting plasma concentrations of FFA were significantly increased from 0.37 (SD 0.04) mmol/l in healthy control subjects to 0.51 (SD 0.06) mmol/l in patients with OSA (p<0.05), without any changes in fasting plasma glucose or insulin concentrations. Cardiac PCr/ATP was significantly reduced, from 2.11 (SD 0.10) in healthy control subjects, compared to 1.77 (SD 0.07) in patients with OSA (p = 0.01), and correlated negatively with circulating concentrations of FFA (r = −0.38, p<0.05). Left ventricular systolic function was preserved, but diastolic function was impaired in patients with OSA compared to control subjects. Provisional uncontrolled data following continuous positive airway pressure (CPAP) treatment for OSA suggests improvements in some of these affected variables.
Conclusion: OSA is associated with increased plasma FFA concentrations, reduced cardiac high energy phosphate metabolism, and reduced diastolic dysfunction. These results suggest that the increased cardiovascular morbidity and mortality in OSA may be due to alterations in myocardial energetics caused by metabolic abnormalities.
S117 RANDOMISED CONTROLLED TRIAL EVIDENCE THAT CONTINUOUS POSITIVE AIRWAY PRESSURE IMPROVES VASCULAR FUNCTION IN OBSTRUCTIVE SLEEP APNOEA HYPOPNOEA SYNDROME
M. D. Cross1, M. Al-Abri1, D. E. Newby2, R. Riha1, M. Vennelle1, N. J. Douglas1. 1Department of Sleep Medicine, University of Edinburgh; 2The Department of Cardiovascular Research, University of Edinburgh, UK
Background: Recent studies have shown abnormal vascular responses in patients with obstructive sleep apnoea hypopnoea syndrome (OSAHS). Although the mechanism is unknown it is suggested that impaired endothelial function plays a pivotal role.
Aims: To evaluate the effect of continuous positive airway pressure (CPAP) therapy on endothelial function in patients with OSAHS.
Methods: Studies were conducted in a double blind randomised controlled crossover design with 31 patients (one female) with severe OSAHS (two major symptoms of OSAHS, >20 of 4% desaturations/hour on polysomnography), mean age 51 (SD 5) years; BMI 40.1 (SD 8.4) kg/m2, AHI 63 (SD 26). Bilateral forearm blood flow was measured using venous occlusion plethysmography with unilateral intrabrachial (endothelium dependent) Sub P(2–8 pmol) and ACH (5–20 μg) and (endothelium independent) SNP(2–8 pmol) infusions were performed at baseline, post six weeks sham CPAP therapy and post six weeks CPAP therapy.
Results: There was no difference in resting blood flow following all treatment limbs. There was a dose dependent increase in blood flow with each vasodilator (p<0.001).
Abstract S117 Forearm venous occlusion plethysmography
CPAP treatment (compliance 5.5 (1.2) hours/night) resulted in increased endothelium dependent and endothelium independent vasodilatation compared to SHAM CPAP (compliance 3.3 hours, (2.2) hours/night).
Conclusions: In patients with severe OSAHS six weeks of CPAP improved peripheral vasomotor function.
S118 THE EFFECT OF SIBUTRAMINE INDUCED WEIGHT LOSS ON SLEEP APNOEA SEVERITY AND METABOLIC PARAMETERS IN OBESE MEN
D. Banerjee1,2, B. J. Yee2, R. R. Grunstein2. 1Sleep and Ventilation Unit, Birmingham Heartlands Hospital, Heart of England Foundation NHS Trust, Bordesley Green East, Birmingham, UK; 2Centre for Respiratory Failure and Sleep Disorders, Royal Prince Alfred Hospital, Missenden Road, Camperdown, Sydney, NSW 2050, Australia
Introduction: Obstructive sleep apnoea (OSA), obesity, and metabolic syndrome are closely associated with each other and are increasing in prevalence. CPAP is the treatment of choice in OSA. Sibutramine is a serotonin/noradrenaline re-uptake inhibitor recommended by NICE as a weight loss promoting agent. Surgical induced weight loss has been shown to improve the severity of sleep apnoea, but there are no data on whether sibutramine induced weight loss may improve sleep apnoea severity and metabolic parameters
Methods: A six month open uncontrolled study using 10–15 mg sibutramine once daily in obese male subjects with OSA was undertaken. Measurements of sleep apnoea severity were made by in-house full multichannel polysomnography on day one and at six months. At the same time, measurements of leptin, insulin, liver enzymes, HDL cholesterol, and glucose were undertaken.
Results: 74 patients, mean age 46.8 (SD 9.7) years, BMI = 34.3 (SD 2.8), weight = 107.8 (SD 12.4) kg, total apnoea/hypopnoea index (AHI) = 44.8 (SD 22.1), Epworth sleepiness score (ESS) = 13.4 (3.6) were recruited and 66 completed the six months. Dropsouts (due to non-compliance) were not included in the analysis (paired t testing). There was a mean weight loss of 8.1 (SD 4.5) kg. There were significant decreases in neck and waist circumference (p<0.0001). The tables show the changes in sleep apnoea severity and metabolic parameters. There were no significant changes in glucose and leptin levels. Paired differences are in mean (SD).
Abstract S118, table 1
Abstract S118, table 2
Conclusions: Weight loss using sibutramine improved the severity of sleep apnoea and some metabolic parameters. Weight loss strategies using sibutramine may be considered as an adjunct therapy to CPAP in those individuals who are obese and have metabolic syndrome, in order to potentially reduce the risk of cardiovascular disease and diabetes.
Clinical trials in airways disease
S119 EVIDENCE OF A ROLE FOR TNFα IN REFRACTORY ASTHMA
M. A. Berry, B. Hargadon, D. E. Shaw, M. Shelley, R. H. Green, C. E. Brightling, A. J. Wardlaw, I. D. Pavord. Department of Respiratory Medicine, Glenfield Hospital, Groby Road, Leicester, UK
TNFα has been proposed as an important mediator in the genesis of refractory asthma. The development of TNFα antagonists has made it feasible to investigate the role of TNFα in refractory asthma. We have measured markers of TNFα activity on peripheral blood monocytes in 10 patients with refractory asthma, 10 patients with mild to moderate asthma, and 10 normal controls and have performed a pilot study of the effects of treatment with the soluble TNFα receptor etanercept 25 mg by subcutaneous injection twice weekly in a placebo controlled double blind cross over study in the patients with refractory asthma. We found a significantly increased membrane TNFα enzyme cell surface density on peripheral blood monocytes in patients with refractory asthma (8.9-fold over isotype control) compared to patients with mild to moderate asthma (3.3) and normal controls (3.8, p<0.001). There was also significantly higher expression of TNF-α receptor 1 and TNF-α converting enzyme but not TNFα receptor 2 in refractory asthma. When compared to placebo, 10 weeks’ treatment with etanercept was associated with a significant reduction in fluorescence of peripheral blood monocyte cells for membrane TNFα (mean difference 6.8, 95% CI 0.5 to 13.1; p = 0.037), a 3.5 (95% CI 0.06 to 7.0; p = 0.046) doubling dose increase in methacholine PC20, 0.85 point (95% CI 0.16 to 1.54; p = 0.02) increase in asthma quality of life score, and a 320 ml (95% CI 8 to 550; p = 0.013) improvement in post bronchodilator FEV1. There was a significant reduction in sputum supernatant histamine concentration with etanercept compared to placebo (−22 ng/ml v 4 ng/ml, mean difference 26 ng/ml, 95% CI 5 to 48; p = 0.022) but no changes in other markers of airway inflammation. Both net change in PC20 and asthma quality of life with etanercept treatment were independently associated with baseline peripheral blood monocyte membrane TNFα expression (adjusted r squared 0.73, p = 0.004). Patients with refractory asthma have evidence of up regulation of the TNFα axis. Treatment with etanercept leads to improvement in airway hyperresponsiveness, asthma quality of life and FEV1 at 10 weeks. These findings provide evidence of a role for TNFα in the pathogenesis of refractory asthma.
S120 EFFECT OF ROFLUMILAST ON LUNG FUNCTION AND EXACERBATIONS IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE: RESULTS OF A ONE YEAR STUDY
P. M. A. Calverley1, L. M. Fabbri2, P. Teichmann3, D. Bredenbroeker3. 1University Hospital Aintree, Liverpool, UK; 2University of Modena and Reggio Emilia, Modena, Italy; 3ALTANA Pharma AG, Konstanz, Germany
Rationale: Roflumilast is an investigational, oral, once-daily phosphodiesterase 4 inhibitor, which has been shown to improve lung function and reduce the rate of mild exacerbations (defined by rescue medication use) in patients with Stage II/III chronic obstructive pulmonary disease (COPD) (Rabe KF et al. Lancet 2005 (in press)). In this study, we have examined the effect of roflumilast on lung function and more severe exacerbations in patients with Stage III/IV COPD over one year.
Methods: In this double blind, placebo controlled, parallel group, multicentre study, 1513 patients (median age 66 years; 76% males; mean prebronchodilator FEV1 percent predicted 37%; mean FEV1 reversibility 11%) were studied. After a four week, single blind, placebo run-in period, patients were randomised to receive oral roflumilast 500 μg or placebo once daily. Inhaled corticosteroids (used by 62% of patients), short acting anticholinergics (used by 58%), and short acting beta-agonists were allowed as concomitant medication. Spirometry was measured at weeks 4, 8, 12, 20, 28, 36, 44, and 52. Exacerbations (defined by use of antibiotics and/or oral corticosteroids and/or hospitalisation) were monitored. Primary endpoints were postbronchodilator FEV1 and annualised exacerbation rate as defined above. Statistics were performed in the intent to treat population. Analysis of covariance was used for within- and between-treatment differences in lung function; Wilcoxon rank sum test was used to assess treatment effect on exacerbation rate, together with a Poisson regression model to estimate the magnitude of the treatment effect. Adverse events (AEs) were recorded.
Results: At study endpoint, roflumilast improved postbronchodilator FEV1 by 39 ml (p = 0.0005) compared with placebo. This was confirmed by repeated measures analysis of FEV1 (48 ml; p<0.0001). Exacerbation rate with placebo was lower than anticipated (0.92/year), and was similar to that observed with roflumilast (0.86/year). However, roflumilast significantly reduced exacerbations requiring oral steroids (p = 0.015), with an estimated reduction of 18%. The majority of drug related AEs occurred in the first two months of study and resolved with continued therapy. The most frequently reported drug related AEs were diarrhoea (6% of patients) and nausea (3%).
Conclusions: This study shows that roflumilast improved postbronchodilator FEV1 in Stage III/IV COPD patients when compared with placebo, but did not change overall exacerbation rate. This result may reflect the low exacerbation rate observed in this study.
S121 PRESCRIBING OF HIGH DOSE INHALED CORTICOSTEROIDS AND ADD-ON THERAPY IN CHILDREN FROM 1999–2004: AN OBSERVATIONAL STUDY
M. Thomas1, S. Turner1, J. von Ziegenweidt2, D. Price1. 1University of Aberdeen; 2Thorpe Medical Research, Norfolk, UK
Background: Asthma is a common disease of childhood managed principally in the community, and inhaled corticosteroids (ICS) are the principal agents used to control persistent asthma. Recent evidence has suggested caution is needed in using high doses of ICS, and the 2003 UK guidelines recommend that for children uncontrolled on standard doses of ICS, add-on therapy should be tried before increasing ICS doses to greater than 400 μg/day of beclomethasone or equivalent. Previous guidelines had however recommended higher doses of ICS as an option.
Objective: To estimate temporal trends in ICS and add-on therapy use in a representative sample of UK children aged 0–11 years treated in primary care.
Abstract S121
Methods: The General Practice Research Database was used to assess prescribing patterns from 1999–2004 for children aged 11 or below with asthma. The records of all children will full database records since 12 months before first diagnosis of asthma and who had received a prescription for any ICS preparation with quantifiable daily ICS dose instructions in the 12 months to 1 June each year were accessed. The proportion of children with an ICS daily dose instructions of >400 and >800 μg/day on the latest prescription and the proportion of children prescribed add-on therapy (long acting B agonists, leucotriene receptor antagonists, chromones, or theophyllines) were noted.
Results: Over the six year time period from 1999 to 2004, the proportion of children receiving high dose ICS for asthma (>400 μg day) remained fairly constant (8.3–10.9%), but there was a progressive increase in the proportion prescribed very high dosages (>800 μg/day) from 2.8% in 1999 to 7.3% in 2004 (p<0.001). There was a progressive increase in the overall use of add-on therapy in children prescribed ICS from 5.0% in 1999 to 32.9% in 2004 (p<0.001), and greater add-on use in those prescribed high dose ICS (from 23.1% in 1999 to 80.1% in 2004, p<0.001).
Conclusions: Community prescribing analysis for children with asthma shows high dose ICS treatment continues to be prescribed to over one in 10 children. In spite of guideline recommendations, there is increasing prescribing of very high ICS dosages. In keeping with guideline recommendations, the use of add-on therapy is increasing particularly in those on high dose ICS.
S122 AN OBSERVATIONAL INVESTIGATION OF HYPERVENTILATION AND BREATHING CONTROL THERAPY IN A PROBLEM ASTHMA CLINIC
A. E. Stanton, P. Vaughn, C. E. Bucknall. Department of Respiratory Medicine, Glasgow Royal Infirmary, Glasgow, UK
Aims: Hyperventilation (or hyperventilation syndrome, HVS) or dysfunctional breathing pattern is often considered to be an associated problem in patients with asthma. We conducted an observational study to determine if our protocol of referring patients with a positive Nijmegen score (of ⩾23, suggestive of hyperventilation) for breathing control therapy resulted in improved Nijmegen scores or asthma related quality of life (as measured by mini-AQLQ).
Methods: 102 patients attending our clinic completed Nijmegen and Mini-AQLQ questionnaires. Patients with a positive Nijmegen score (HVS group) were referred for breathing control therapy (BCT), delivered by our respiratory specialist physiotherapist in parallel with attendance at the problem asthma clinic. We aimed to collect follow up data on above parameters at six months since we sought a long term effect from this intervention.
Results: 102 patients with moderate to severe asthma (77 receiving BTS step 4 or 5 level therapy) were studied. 80 had definite asthma, based on bronchodilator reversibility (52), bronchial hyper reactivity (8), PEF variability (19) or a trial of steroids (1)). The average Nijmegen score for the whole group was 26.4 (range 1–61). Those with Nijmegen score ⩾23 (HVS group, n = 65) had significantly lower Mini-AQLQ scores (mean 42.4) than the non-HVS group (those with negative Nijmegen scores, n = 37, mean 61.9, 95% CI for difference 13 to 28). There was a strong relation between Nijmegen score and Mini-AQLQ (r = −0.63, p<0.001) at baseline. Nine of the 65 HVS patients did not attend BCT at any given time with the remaining 56 patients being reviewed on a median (range) of three (1–15) occasions. Follow up questionnaire data were available for Mini-AQLQ in 46 patients (17 non-HVS, 29 HVS), with no difference from baseline seen (95% CIs for difference −17 to 15 (non-HVS), −13 to 5 (HVS)). Nijmegen scores in the 44 (15 non-HVS, 29 HVS) patients with available data also showed no significant change (95% CIs for difference −9 to 2 (non-HVS), −1 to 9 (HVS)) following BCT.
Conclusion: We found no evidence that a moderate intensity breathing control physiotherapy intervention had any impact on Nijmegen scores or asthma related quality of life in patients with moderate to severe asthma.
S123 EFFICACY OF CICLESONIDE IN SMOKERS AND NON-SMOKERS WITH ASTHMA
C. G. Langdon1, K. R. Chapman2, A. Escher3, H-JWeber3, T. Welte4. 1The Holyport Surgery, Holyport, UK; 2University of Toronto, Toronto, Canada; 3ALTANA Pharma AG, Konstanz, Germany; 4 Hannover Medical School, Hannover, Germany
Insensitivity to short term treatment with inhaled corticosteroids—for example, beclomethasone dipropionate (BDP) or fluticasone propionate—has been observed in smokers with asthma (
;
). Ciclesonide (CIC) is a novel lung activated inhaled corticosteroid with once-daily efficacy. Data from two double-blind, randomised, placebo controlled studies were used to compare the efficacy of CIC in patients with or without smoking history.
Asthma patients (n = 689, intention to treat) were randomised if they met the following criteria: pre-treatment with a constant dose of 400 to 800 μg/d BDP (or equivalent; continued during the two week baseline period), FEV1 between 60 and 90% of predicted. Patients with chronic obstructive pulmonary disease (COPD) were excluded. For 12 weeks, patients received either 80 to 640 μg CIC (ex-actuator, HFA-MDI) once daily in the morning (n = 454), or placebo (n = 235). Primary variables were change in morning PEF and “lack of efficacy” (LOE, that is, clinical asthma exacerbation, or decrease in FEV1 ⩾20%, or FEV1 <50% of predicted, or decrease in PEF ⩾20% on two consecutive days, or defined increase in asthma symptoms). Secondary variables included FEV1, asthma symptom scores, and use of rescue medication.
Ciclesonide was superior to placebo with regard to morning PEF in non-smokers as well as smokers. Compared with placebo, morning PEF (LSMean (SEM)) increased in non-smokers by 24 (5) l/min (p<0.0001) and in smokers by 21 (5) l/min (p<0.0001). The probability of completing the study without experiencing LOE was statistically significantly higher in patients treated with CIC than in patients receiving placebo (p<0.0001, non-smokers and smokers). In patients treated with ciclesonide, the probability of not meeting LOE criteria (Kaplan-Meier estimates) was comparable in non-smokers (68%) and smokers (72%). Treatment with ciclesonide resulted in a statistically significant increase in FEV1 (LSMean (SEM)) as compared with placebo: 182 (46) ml (p<0.0001) in non-smokers, 131 (50) ml (p = 0.0048) in smokers. When using treatment by smoking habit interaction term, the treatment effect on morning PEF and FEV1 was similar in smokers and non-smokers (p = 0.69 and p = 0.43, respectively). Compared with placebo, asthma symptom scores and rescue medication use improved significantly in patients treated with ciclesonide. No differences were observed between smokers and non-smokers.
In contrast to other inhaled corticosteroids, ciclesonide appears to be equally effective in smokers and non-smokers with asthma.
S124 EFFICACY AND SAFETY OF ONCE-DAILY CICLESONIDE 160 μG AS COMPARED WITH ONCE-DAILY BUDESONIDE 400 μG IN PAEDIATRIC ASTHMA PATIENTS
A. von Berg1, P. Minic2, M. Sreckovic3, C. Bollrath1, S. Hellbardt4, R. Engelstätter4. 1Marien-Hospital Wesel, Wesel, Germany; 2Institute of Health Protection, Belgrade, Serbia and Montenegro; 3Pediatric Hospital for Lung Diseases, Belgrade, Serbia and Montenegro; 4ALTANA Pharma AG, Konstanz, Germany
Ciclesonide is a novel lung activated inhaled corticosteroid for the treatment of paediatric and adult patients with asthma. The aim of this double blind, double dummy, parallel group study was to compare the efficacy and safety of once-daily ciclesonide 160 μg with once-daily budesonide 400 μg in paediatric patients with moderate and severe persistent asthma.
After a baseline period of 2–4 weeks (rescue medication only), randomised patients (n = 513; 6–11 years; mean FEV1 = 78% of predicted) were treated once daily in the evening with either ciclesonide 160 μg (n = 340; ex-actuator, equivalent to 200 μg ex-valve, HFA-MDI with spacer), or budesonide 400 μg (n = 173; Turbuhaler).
Ciclesonide and budesonide comparably improved lung function at the end of the 12 week treatment period (p = 0.9347, between treatments). The increase in FEV1 from baseline was statistically significant (p<0.0001): 0.22 l in the ciclesonide treatment group, and 0.25 l in the budesonide group. Likewise, a statistically significant increase in FVC (p<0.0001 from baseline) was achieved by ciclesonide (0.204 l) as well as budesonide (0.236 l). Asthma symptom scores improved statistically significantly with no differences between ciclesonide and budesonide (both −1.21; p<0.0001). Similarly, both treatments were equally effective in reducing the use of rescue medication (both −1.64 puffs/d; p<0.0001). Ciclesonide was superior to budesonide (p = 0.0025) with respect to increase in body height (measured by stadiometry). There were statistically significant differences in favour of ciclesonide with regard to impact on HPA-axis as assessed by change in 24 hour urine free cortisol levels (p = 0.0001).
Once-daily ciclesonide 160 μg and once-daily budesonide 400 μg similarly improved lung function, asthma symptom scores, and need for rescue medication in children with asthma. Thus, at half the daily dose, ciclesonide was as effective as budesonide. Data on urine free cortisol and body height indicated a favourable systemic safety profile of ciclesonide.
Tuberculosis: basic science
S125 MYCOBACTERIAL HEAT SHOCK PROTEIN 70 TRIGGERS RAPID DENDRITIC CELL-T CELL IMMUNE SYNAPSE FORMATION VIA THE CHEMOKINE RECEPTOR CCR5
R. A. Floto1, P. A. MacAry1, J. M. Boname1, M. Singh2, P. J. Lehner1. 1Cambridge Institute for Medical Research and Department of Medicine, University of Cambridge, Addenbrooke’s Hospital, Cambridge CB2 2XY, UK; 2Lionex Diagnostics & Therapeutics GmbH, Mascheroder Weg 1b, D-38124, Braunschweig, Germany
Microbial heat shock proteins (HSPs) have been shown to modulate both innate and adaptive immune responses. We have previously shown that human dendritic cells (DC) pulsed with peptide loaded mycobacterial HSP70 complexes generate potent antigen-specific cytotoxic T cell responses, which are dependent on an HSP70 stimulated calcium signaling (Macary et al Immunity 2004). We have also shown that endotoxin-free mycobacterial HSP70 is a relatively weak stimulus for DC cytokine and chemokine secretion in the absence of a second proinflammatory stimulus, usually provided by T cell-DC interactions.
We have now established that mycobacterial HSP70 induces morphological and functional changes in human DC which result in the rapid formation of immunological synapses between DC and T cells. This is triggered by calcium induced redeployment of cytoskeletal actin and the projection of membrane pseudopodia from the DC (visualised by real time fluorescence/DIC microscopy). We show that whilst the formation of these synapses is antigen independent, they remain essential for the generation of antigen specific T-lymphocyte responses. Through pharmacological dissection of the signaling pathway and a heterologous functional screen, we establish that mycobacterial HSP70 signals through the G-protein coupled chemokine receptor, CCR5. We confirm this finding by demonstrating that the CCR5 specific inhibitor TAK-779 blocks HSP activity and that DC from subjects homozygous for the CCR5Δ32 inactivating mutation fail to respond. This study is the first to explain the mechanism of HSP adjuvanticity and the receptor responsible for it and has important, wide reaching implications both for the rational design of HSP based vaccines and for our understanding of dendritic cell behaviour during mycobacterial infection.
S126 VITAMIN D ENHANCES ANTIMYCOBACTERIAL IMMUNITY IN VIVO AND IN VITRO
A. R. Martineau1,2,7, B. M. Hall1, S. M. Newton2, K. A. Wilkinson2,7, B. Kampmann2, G. E. Packe3, R. N. Davidson4, Z. Maunsell5, S. Rainbow5, A. W. Norman6, S. Eldridge1, R. J. Wilkinson2,7, C. J. Griffiths1. 1Centre for Health Sciences, Barts and The London, London, UK; 2Wellcome Centre for Tropical Medicine, Imperial College, London, UK; 3Newham Chest Clinic, London, UK; 4Tuberculosis Clinic and 5Department of Clinical Biochemistry, Northwick Park Hospital, London UK; 6Department of Biochemistry, University of California, Riverside, USA; 7Institute of Infectious Diseases and Molecular Medicine, University of Cape Town, South Africa
Background: Vitamin D was used to treat tuberculosis (TB) in the pre-antibiotic era. Calcitriol, its active metabolite, restricts growth of M tuberculosis in macrophages in vitro. We present results of the first clinical trial to investigate the effect of in vivo vitamin D supplementation on antimycobacterial immunity, and describe an investigation of the mechanisms by which in vitro addition of calcitriol modulates antimycobacterial immunity in peripheral blood mononuclear cells (PBMC).
Methods: We conducted a double blind, randomised, placebo controlled trial among 202 healthy London TB contacts powered to determine the effect of a single oral dose of 2.5 mg vitamin D2 on antimycobacterial immunity as determined by the BCG lux assay (
). This measures the ability of whole blood to restrict luminescence (and thus metabolic health) of the recombinant mycobacterium BCG lux, expressed as a luminescence ratio (LR = luminescence 24 hours post-infection/baseline luminescence). We also infected PBMC of healthy blood donors with BCG lux, and investigated the effects of in vitro addition of calcitriol, (23S)-25-dehydro-1αOHD3-26,23-lactone (a selective nuclear vitamin D receptor antagonist) and 1β,25(OH)2D3 (a selective membrane vitamin D receptor antagonist) on antimycobacterial immunity in this system.
Results: 121/202 (60%) participants were vitamin D deficient (serum 25-hydroxy-vitamin D<27.5 nmol/l) at recruitment. Vitamin D supplementation reduced mean LR at six weeks compared with placebo (0.58 v 0.70, p = 0.04); this effect was particularly marked among participants with baseline serum 25-hydroxy-vitamin D <11 nmol/l (0.40 v 0.73, p<0.01). In PBMC, calcitriol suppressed BCG lux luminescence despite decreasing the secretion of type 1 cytokines. Calcitriol induced suppression of BCG lux luminescence was attenuated by (23S)-25-dehydro-1αOHD3-26,23-lactone, but not by 1β,25(OH)2D3.
Conclusions: Oral vitamin D supplementation enhanced antimycobacterial immunity among TB contacts as measured in a whole blood model. This effect was particularly marked in individuals with profound vitamin D deficiency at baseline. Calcitriol induced antimycobacterial immunity in PBMC in vitro: this effect appears to be mediated primarily by nuclear events other than the transcription of protective cytokines.
S127 MONOCYTE FIBROBLAST NETWORKS DRIVE MATRIX DEGRADATION IN TUBERCULOSIS
C. M. O’Kane, M. D. Jones, P. T. G. Elkington, J. S. Friedland. Department of Infectious Diseases, Imperial College, Hammersmith Campus, London, UK
Background: Tuberculosis (TB) is characterised by tissue destruction, with breakdown of extracellular matrix proteins in the lung including type I collagen. Matrix metalloproteinases (MMPs) have been implicated in this (
). Fibroblasts are the major pulmonary source of MMP-1, the most potent type I collagenolytic enzyme at neutral pH. Granuloma fibroblasts (not previously implicated in matrix destruction in TB) are exposed to inflammatory cytokines from Mycobacterium tuberculosis (Mtb) infected monocytes. We hypothesised that monocyte-fibroblast interactions drive MMP-1 secretion in TB.
Methods: Human lung fibroblasts grown in a 3D type I collagen gel to mimic in vivo tissue conditions, were stimulated with conditioned media from Mtb-infected monocytes (CoMTb). MMP-1 was analysed by casein zymography, TIMPs-1/-2 (tissue inhibitors of metalloproteinases) by ELISA and gene expression by RNase protection assay. Transcriptional regulation was investigated by TransAm Transcription factor ELISA for NFκB, western blot for IκB, and transient transfection of cells with a series of deletion and site-directed mutation constructs of the MMP-1 or TIMP-1 promoters linked to luciferase. MAP kinases and STATs were analysed by western blotting. TB granulomas were stained for MMP-1/TIMP.
Results: CoMTb induced a dose dependent increase in MMP-1 secretion over 120 hours. MMP-1 mRNA peaked at 24 hours, accompanied by a corresponding increase in MMP-1 promoter activation (twofold at 8 hours, and threefold at 24 hours, p<0.05). Truncation at 2001 base pairs upstream of transcriptional start site abrogated promoter activation. The NFκB site at -2878bp was critical for CoMTb induced MMP-1 activation. Nuclear translocation of NFκB p65 and p50 subunits occurred within 15 minutes of CoMTb stimulation. Cytoplasmic IκBα degradation was evident at 15 minutes, reforming by one hour, while sustained downregulation of IκBβ was detected between ½ hour and 8 hours. Upstream, p38 MAP kinase was phosphorylated within 15 minutes, and inhibition of p38 pathway by SB203580 reduced MMP-1 secretion from 45+/−1.1 to 27+/−2.2 ng/ml, p<0.05. CoMTb also induced JNK and STAT-1/-3 phosphorylation. In contrast CoMTb downregulated TIMP-1 (approx 2.5-fold at 120 hours) via a p38 dependent mechanism and TIMP-2 secretion (from 68.8+/−6.3 ng/ml in controls to 31.7+/−8.3 ng/ml at 120 hours, p = 0.004) via the JNK pathway. TIMP-1 promoter was suppressed (by sevenfold, p<0.05) as was TIMP-1/-2 mRNA expression. MMP-1 and TIMP-1 immunostaining were demonstrable in the periphery of TB granuloma.
Discussion: Mtb drives unopposed fibroblast MMP-1 secretion via a monocyte dependent network. Maximal MMP-1 induction by fibroblasts in this model is NFkappaB dependent and p38-requiring. Fibroblasts may be key mediators of the tissue destruction that characterises TB
S128 MESSENGER RNA AS A MARKER OF TREATMENT RESPONSE IN PULMONARY TUBERCULOSIS
F. M. R. Perrin, Y. N. Parsons, R. A. M. Breen, J. Islam, T. D. McHugh, M. C. I. Lipman, S. H. Gillespie. Royal Free Hospital, Pond Street, Hampstead, London NW3 2QG, UK
Introduction: The only validated prognostic indicator of response during treatment of pulmonary Mycobacterium tuberculosis (MTB) disease is sputum culture conversion after two months of therapy (
). Molecular markers provide a more rapid assessment of mycobacterial burden. Commonly used nucleic acid amplification techniques are unable to distinguish between DNA from live or dead organisms. However, quantitative analysis of mRNA can indicate MTB viability (
) and may be helpful in evaluating early treatment response. We undertook an exploratory, prospective study of patients with smear positive pulmonary tuberculosis (TB) and compared (1) change in colony count (CFU)—a validated measure of bacterial burden, (2) time to culture positivity (TTP) in the liquid culture system, and (3) fall in mRNA levels during treatment.
Method: To date, six patients have been assessed. Sputum samples were collected pretreatment and whilst on therapy. Sputum was split into three aliquots for colony counts (plated on selective agar), liquid culture (using the MB-Alert system), and mRNA analysis. mRNA was detected using quantitative real-time reverse transcriptase PCR (qRT-PCR) of the rpoB gene. Data are given as median and (range).
Results: See table.
Abstract S128
Conclusion: There is a rapid fall in bacterial load within the first few days of treatment and a corresponding prolongation in time to culture positivity. Changes in mRNA correlate with this, suggesting that this assay reflects mycobacterial viability. As such, qRT-PCR appears to provide an early and rapid assessment of treatment response. This is being evaluated further in a larger cohort study with more frequent sputum sampling.
S129 SPUTUM INDUCTION IS A NON-INVASIVE ALTERNATIVE TO BAL ALLOWING A LUNG ORIENTATED APPROACH TO INVESTIGATE IMMUNE RESPONSES IN PATIENTS WITH TUBERCULOSIS
R. A. M. Breen, G. Hardy, F. Perrin, M. A. Johnson, G. Janossy, M. C. I. Lipman. Royal Free & University College Medical School, London NW3 2QG, UK
Introduction: Assays measuring cytokine production by lymphocytes responding to tuberculosis (TB) antigens may have potential in both diagnosis and management. Blood is convenient to sample, but responses are generally low frequency and hence difficult to detect in lymphopenic states—for example, HIV. We sought to ascertain the utility of lung based immunology in TB patients with HIV co-infection. We attempted to extend the method to use sputum induction as a non-invasive, patient friendly alternative to BAL in this setting.
Methods: Broncho-alveolar lavage (BAL) was performed on patients with a variety of respiratory conditions. BAL derived cells were incubated overnight with PPD or with no antigen. After fixation and permeabilisation, cells were stained with monoclonal antibodies against CD3 and CD4 and intracellularly for IFN-γ production. When possible, paired blood samples were also analysed. Sputum induction was performed on individuals with suspected TB with 3% hypertonic saline delivered via an ultrasonic nebuliser for 20 minutes. Following mucolysis, sputum was processed identically to BAL.
Results: Forty seven HIV+ individuals with a median blood CD4 count of 131 cells/μl (range: 6–661) had BAL for investigation of possible infection. 19 of 47 with culture confirmed TB (14 pulmonary; 12 non-pulmonary) had a median CD4+IFN-γ+ PPD response = 10.65% (range: 0–67.11%) versus 0.03% (range: 0–16.12%) in those with a diagnosis other than TB (p<0.0001). By comparison 25 HIV negative TB culture positive patients (21 pulmonary; 4 non-pulmonary) displayed a median CD4+IFN-γ+ PPD response = 13.94% (range: 0.12–79.32%) (p = 0.85 v HIV+TB+). 27 cases had a paired blood sample analysed (9 HIV+) with a median CD4+IFN-γ+ PPD response = 0.19% (range: 0–1.63%) (p<0.0001 versus BAL). 12 individuals with culture-positive TB (9 pulmonary; 3 non-pulmonary) had sputum induced without incident. Six of 12 were HIV co-infected with a median blood CD4 count of 217 cells/μl (12–709). Median CD4+IFN-γ+ PPD response in sputum = 3.71% (range: 0–23.79%). Responses in induced sputum from seven cases were compared to paired BAL with a median CD4+IFN-γ+ PPD response of 8.77% (range: 0–23.79%) in sputum versus 20.35% in BAL (range: 2.63–61.04%).
Conclusion: Lung orientated immunological investigation of TB can provide information in settings such as advanced HIV infection where blood tests start to fail. We have successfully translated the specific methodology from BAL to sputum induction. This simple approach also provides samples for microbiological investigation—maximising the information gained; and thus making it suitable for resource poor settings.
Mechanisms of lung remodelling and regeneration
S130 LOCALISATION OF ADAM33 TO BRONCHIAL SMOOTH MUSCLE IN ASTHMATIC AIRWAYS AND HUMAN EMBRYONIC LUNGS
H. M. Haitchi1, R. M. Powell1, T. J. Shaw1, P. H. Howarth1, S. J. Wilson1, D. I. Wilson2, S. T. Holgate1, D. E. Davies1. 1The Roger Brooke Laboratories, Division of Infection Inflammation & Repair and 2Human Genetics, University of Southampton, Southampton, UK
Rationale: Polymorphic variation in ADAM33 is strongly associated with asthma and bronchial hyperresponsiveness (BHR) (
.). As there are several alternatively spliced forms of ADAM33 (
), we studied its expression in normal and asthmatic bronchial biopsies and embryonic airways.
Methods: Biopsies were obtained from normal (n = 21) and asthmatic (n = 19) volunteers; human embryonic lungs were collected under the guidelines of the Polkinghorne Committee after fully informed consent and local ethical approval. Samples were processed for quantitative RT-PCR, Western blotting, immunohistochemistry (IHC), or whole mount immunofluorescence confocal microscopy (IFCM) using PCR primers or antibodies against ADAM33 and α-smooth muscle actin (αSMA).
Results: Several ADAM33 mRNA splice variants were detected in bronchial biopsies and embryonic lung; however, the beta isoform and variants encoding the metalloprotease domain were rare. Western blotting of bronchial biopsies confirmed the presence of multiple isoforms of ADAM33 with molecular weights of 22, 37, 55, and 65 kDa. IHC and IFCM of bronchial biopsies showed that αSMA and ADAM33 immunoreactivity were mostly co-localised to smooth muscle and isolated cells in the submucosa. There was no significant difference in ADAM33 mRNA amplicons or protein in asthmatic compared with control subjects. In developing lung, ADAM33 was found around the bronchi, however immunoreactivity was more widely distributed than αSMA within undifferentiated mesenchyme; on western blots an additional 25 kDa ADAM33 variant was detected.
Conclusions: Several ADAM33 protein isoforms occur in adult bronchial smooth muscle and in embryonic bronchi and surrounding mesenchyme, strongly suggesting that its genetic association with BHR is linked to smooth muscle development and/or function. Although simple up or down regulation of ADAM33 is unlikely to explain its contribution to asthma pathogenesis, the occurrence of ADAM33 in embryonic mesenchymal cells suggests that it may be involved in airway wall “modelling” that contributes to the early life origins of asthma.
Supported by: Asthma, Allergy and Inflammation Research Charity (AAIR), UK; HOPE Wessex Medical Research, UK; Medical Research Council,UK; The British Lung Foundation, UK.
S131 MICRO ARRAY ANALYSIS OF REGENERATING ADULT MOUSE LUNG
A. Gilthorpe, A. Annan, M. Maden. MRC centre for Developmental Neurobiology, King’s College London, UK
Rationale: Presently, most lung disorders such as emphysema are incurable as the lung is incapable of spontaneously regenerating new alveoli. Studies have shown that all-trans-retinoic acid (tRA), a derivative of vitamin A, has a significant effect on the regeneration process in a dexamethasone (dex) induced emphysemic mouse model. Daily intraperitoneal injections of tRA for a 10 day period are sufficient to promote the regeneration of new alveoli and restore alveolar size. The following study presents the results of a micro array time course analysis from non-regenerating and regenerating emphysemic lungs during RA administration. We have used this to identify the molecular pathways that underlie this remarkable regeneration event.
Methods: Emphysemic mice generated by dex treatment were injected with tRA (2 mg/kg bodyweight) in DMSO/peanut oil for a 4, 7, and 10 days. Control mice received DMSO/peanut oil only. Mice were sacrificed 24 hours after the last tRA administration total RNA was extracted from lung tissue. This was used to generate biotin labelled cRNA probes to hybridise with Affymetrix Mouse Genome 430 2.0 array chips. Micro array data were analysed using GeneSpring 6.0 (Silicon Genetics).
Results: We have analysed subsets of genes (transcription factors, cell surface receptors, signalling molecules, etc) that are regulated during the time course of lung regeneration by the addition of tRA. We have used this to identify candidate genes that may be instrumental in regulating the process of regeneration.
Conclusion: Characterisation of the molecular basis of tRA induced lung regeneration provides the foundation for the development of clinical treatments for emphysema and other degenerative lung disorders.
1
2
3
S132 RETINOID INDUCTION OF ALVEOLAR REGENERATION IN A MOUSE MODEL OF EMPHYSEMA
M. Maden, A. Gilthorpe, A. Annan, S. Stinchcombe. MRC Centre for Developmental Neurobiology, King’s College London, Guy’s Campus, London SE1 1UL, UK
We have previously shown that dexamethasone treatment of newborn mice inhibits alveolar development resulting in a greatly decreased surface area for gaseous exchange. Subsequent treatment of these mice with all-trans-retinoic acid (tRA) for two weeks results in a complete restoration of histological structure and alveolar surface area. This may represent a valuable model system and potential treatment for the human disease of emphysema. We have now used this same model system to compare the efficacy of a range of retinoids at inducing alveolar regeneration and to begin an analysis of the time course of alveolar cell response to tRA.
After dexamethasone treatment as pups mice at 4–5 weeks of age were administered various retinoids at a concentration of 2 mg/kg body weight dissolved in DMSO/peanut oil. The retinoids tested included 13-cis-RA, 9-cis-RA, retinol, 4-oxo-RA, three retinoic acid receptor agonists and a retinoid X receptor agonist. All animals were killed at P90, their lungs were inflation fixed, lung volumes determined and Lm measurements obtained from histological sections. Retinol, the metabolic precursor of RA is inactive, as is the RARb agonist whereas all the other retinoids are highly efficient at inducing regeneration and restoring Lm and alveolar surface area. The haematopoetically active growth factor granulocyte colony stimulating factor is not active at inducing regeneration. We have also analysed at what time alveolar cells begin to respond to RA in terms of proliferation and septal outgrowth. Since the active retinoids are those that bind to the retinoid receptors these results suggest that the mechanism of action of retinoids in this regenerating system is via a nuclear pathway involving an alveolar cell type rather than an effect via the cell surface or a cytoplasmic signalling cascade and also suggest that it is the alveolar cells themselves which respond to retinoids rather than a source of cells external to the lung.
S133 DIFFERENTIAL EXPRESSION OF P63 AND CYTOKERATINS IN “CUBOIDAL” AND “SQUAMOUS” EPITHELIAL METAPLASIA FROM ASTHMA AND CHRONIC OBSTRUCTIVE PULMONARY DISEASE SUBJECTS
K. Pinnion, S. E. Stinson, M. L. Foster*. Department of Pathology, AstraZeneca R&D Charnwood
Introduction: Airway epithelial change in asthma and chronic obstructive pulmonary disease (COPD) is characterised by cuboidal and squamous metaplasia respectively. There is a paucity of data on phenotypic differences in these cells in an ostensibly similar morphological group. Here we report the results of a preliminary study stratifying epithelial phenotype using p63, cytokeratin (CK) 5/6, 7, 18, and 19.
Methods: Samples of asthmatic and COPD trachea, 1°–4° bronchus and peripheral asthmatic lung tissue were acquired through an ethically approved tissue bank. COPD peripheral tissue from consented individuals undergoing LVRS for emphysema was acquired from Glenfield Hospital, Leicester. Sections were stratified using H&E staining. Immunohistochemistry of p63, CK 5/6, CK 7, CK18, and CK 19 was carried out using standard, well validated, protocols.
Results: Asthmatic tissue showed extensive CK 5/6 and p63 protein expression in areas of metaplastic repair, whereas the COPD tissue showed a more diffuse expression within similar regions. In the peripheral lung of both the asthmatic and COPD (both LVRS and non-LVRS) samples there were fewer CK 5/6 and p63 positive cells compared to the central airways. The morphology of the CK 5/6 and p63 positive cells in the asthma samples was cuboidal, whereas in the COPD central airway tissue positive cells were of a more flattened squamous appearance. In the peripheral COPD lung (LVRS) CK 7, 18, and 19 expression was diffuse involving both normal and metaplastic cells.
Conclusion: These data suggest considerable phenotypic heterogeneity in the airway epithelial response. The p63 expression in both cuboidal and squamous cells suggests that disease stratification on morphology alone is inadequate. The cytokeratin profile again suggests phenotypic variation within cell populations with similar morphology. The asthmatic epithelial response is more extensively cuboidal, characterised by CK5/6 and p63 positivity. In COPD there is much greater heterogeneity in CK expression and much greater variation in p63 expression, thus we hypothesise that COPD involves multiple phenotypes compared to a single stem cell involved in asthma repair.
S134 MURINE MESENCHYMAL STEM CELLS GENERATE OSTEOSARCOMA-LIKE LESIONS IN THE LUNG: IMPLICATIONS FOR STEM CELL THERAPY
S. Aguilar1, M. Loebinger1, E. Nye2, B. Spencer-Dene2,3, G. Stamp2,3, D. Bonnet4, S. M. Janes1. 1Centre for Respiratory Research, University College London; 2Experimental Pathology Laboratory, London Research Institute, Cancer Research UK; 3Department of Histopathology, Imperial College London; 4Hematopoietic Stem Cell Laboratory, London Research Institute, Cancer Research UK
Murine mesenchymal stem cells are capable of differentiation into multiple cell types both in vitro and in vivo. This potential predicts that mesenchymal stem cells could be good candidates for cell therapy treatments for diseased or damaged organs. Such therapies will require short in vitro culture times to expand cell populations. Unlike embyonic stem cells, murine mesenchymal stem cells have not been reported to form spontaneous tumours.
We have previously demonstrated a new method of isolating a purified population of murine mesenchymal stem cells which demonstrated a diverse differentiation potential both in vitro and in vivo. In this study, we show that this purified population of murine mesenchymal stem cells embolise within lung capillaries following systemic injection and then rapidly expand within, and invade into, the lung parenchyma forming hyperproliferative tumour-like nodules. These lesions rarely contain cells bearing the immunohistochemical characteristics of lung epithelial cells but aggregates of bone and cartilage cells that have the appearance of immature bone resembling exuberant fracture callus or well differentiated osteosarcoma. Our findings indicate that murine mesenchymal stem cells can behave in a manner similar to tumour cells with dysregulated growth and aberrant differentiation within the alveolar niche after only short culture periods. Further, we demonstrate that these cells can invade underneath and replace, rather than differentiate into, the endothelium of pulmonary vessels. These findings potentially have major implications for stem cell therapies.
Thoracic surgery and interventional procedures
S135 THE USE OF PREDICTED POST OPERATIVE LUNG FUNCTION TO PREDICT DURATION OF INTENSIVE CARE UNIT ADMISSION FOLLOWING PULMONARY RESECTION FOR MALIGNANCY
A. Jha1, E. M. Thomson1, D. D. Melley1, G. Ladas2, T. W. Evans1. Departments of 1Intensive Care Medicine & 2Thoracic Surgery, Royal Brompton Hospital, London, UK
Background: Pulmonary resection is associated with significant morbidity necessitating protracted postoperative intensive care unit (ICU) admission. Predicted postoperative FEV1 (ppo-FEV1) and DLCO (ppo-DLCO) have been employed to predict fitness for such surgery (
) and associated mortality (
) We therefore assessed the potential value of ppo-FEV1 and ppo-DLCO as predictors of ICU length of stay (LOS, less than or greater than 24 hours) and markers of illness severity (APACHE II) in patients undergoing pulmonary resection.
Methods: ppo-FEV1 and ppo-DLCO were calculated for patients undergoing pulmonary resection for suspected malignant disease that subsequently required ICU admission.
Results: Of 50 patients needing ICU admission after lung resection, 21(42%) were admitted for less than 24 hours and 29 (58%) for more. Median ppo-FEV1 for these groups was 61.6% and 46.6% respectively (p>0.05) and ppo-DLCO was 51.3% and 49.3% (p>0.05). ppo-LF did not correlate with ICU LOS (mean 11.3 days in greater than 24 hour group) Further, no significant differences in other lung function indices, PaO2:FiO2 or APACHE II emerged between the two groups. Mean cost per admission was £1805 (<24 hour) and £23,983 (>24 hour).
Conclusions: Up to 60% of patients requiring intensive care following pulmonary resection need a protracted stay at considerable cost however, ppo-LF is not useful to predict LOS in intensive care post lung resection.
S136 THE STRENGTH OF BRITISH THORACIC SOCIETY GUIDELINES IN DETERMINING THE OUTCOME FOR LUNG CANCER SURGERY: BIRMINGHAM HEARTLANDS HOSPITAL’S EXPERIENCE
P. S. Krishna Moorthy*, R. Khan, J. F. Khalil Marzouk, P. B. Rajesh. Department of Thoracic Surgery, Birmingham Heartlands Hospital, UK
Objective: Surgical resection is the treatment of choice for patients with lung cancer. However patients with limited pulmonary function are often denied curative resection. This study evaluates the risks of lung cancer surgery in patients with post bronchodilator forced expiratory volume in one second (FEV1) <1.5 for lobectomy and FEV1 <2.0 for pneumonectomy.
Methods: It is a retrospective study of 171 patients from January 2002 to December 2004 who underwent pulmonary resection for lung cancer under a single surgeon. The patient were divided into two groups: Group A (non-compliant of BTS Guidelines; FEV1 <1.5 l/s for lobectomy and FEV1 <2.0 l/s for pneumonectomy) (n = 53 (31%)); Group B (compliant of BTS Guidelines) (n = 118 (69%)). The demography, diagnosis, preoperative pulmonary studies, functional status, and operations were compared between the groups. Postoperative complications were divided into two groups: respiratory complications and other complications. Univariate analysis used to identify risk factors for 30 days mortality. Postoperative survival curve charted to compare both groups.
Results: In general 31% of the patients were in Group A and 16.4% were in high risk.Lobectomy was done in 118 (69%),bilobectomy in 15 (8.8%), pneumonectomy in 34 (19.9%), bronchoplastic resection in 4 (2.3%). Overall mortality was 6.4% with the breakdown according to groups and type of resection (see table) showing no significance difference.
Abstract S136
The univariate analysis showed type of histology and stage were significant predictor (p = 0.038 and p = 0.002) of early mortality though this was not the case in multivariate test. There was no significant difference in the survival between the groups (p = 0.11).
Conclusions: Although many patients were high risk as judged by BTS guidelines,overall mortality was lower than generally accepted. A significant number of patients who be turned down in the guidelines due to pulmonary insuffiency had an ueventful procedure suggesting they may be unnecessarily conservative.
S137 PREOPERATIVE PREDICTORS OF PROLONGED AIR LEAK FOLLOWING LOBECTOMY FOR PRIMARY LUNG CANCER
N. Chaudhuri, J. McShane, A. D. Grayson, N. K. Mediratta, M. Carr, A. S. Soorae, R. D. Page. The Cardiothoracic Centre NHS Trust, Liverpool, UK
Objective: Intraoperative factors are well known to contribute towards prolonged air leaks (PAL). What is not clear is the preoperative predisposition of a patient to PAL. We aimed to identify preoperative predictors for the development of PAL following lobectomy for primary lung cancer.
Methods: Data were prospectively collected for 540 consecutive patients undergoing lobectomy for primary lung cancer between October 2001 and September 2004. 36 (6.7%) patients developed PAL postoperatively; defined as air leak lasting more than six days. A forward stepwise multivariate logistic regression analysis was undertaken to identify preoperative predictors of developing PAL. Variables offered to the model included patient demographics, prior cancer treatment, pulmonary function, smoking status, and anatomical lobe removed. A receiver operating characteristic (ROC) curve was calculated to assess the predictive ability of the logistic model.
Abstract S137
Results: Preoperative predictors of postoperative PAL are shown in table below. Predictive ability of this model was reasonable with a ROC curve of 0.67. Inhospital mortality for patients who developed PAL was 5.6% (n = 2) compared to 2.4% (n = 12) for others (p = 0.25). Postoperative length of stay was significantly longer in patients with PAL (14 days v 8 days; p<0.001).
Conclusions: PAL places a significant burden on both patients and hospital resources. We have successfully identified two preoperative factors, which significantly predispose a patient to PAL following lobectomy for primary lung cancer. It remains to be seen if prior knowledge of emphysematous lungs or previous radiotherapy in a patient allows modification of intraoperative and postoperative factors to lead to reduced PAL.
S138 THE ROLE OF MEDIASTINOSCOPY IN THE SELECTION FOR EXTRAPLEURAL PNEUMONECTOMY IN MALIGNANT MESOTHELIOMA
A. Nakas, J. G. Edwards, D. Stewart, A. E. Martin-Ucar, D. A. Waller. Glenfield Hospital, Leicester, UK
Objectives: To evaluate the role of video assisted cervical mediastinoscopy (CM)as part of mediastinal staging in a radical surgery protocol for malignant mesothelioma (MM).
Methods: Pathology reports and case notes were analysed from 92 consecutive patients undergoing extrapleural pneumonectomy (EPP) for MM. The distribution of nodal metastasis was evaluated according to the UICC TNM staging system. Differences in survival between groups were estimated using Kaplan-Meier analysis and the Log Rank test. The negative predictive value (NPV) of cervical mediastinoscopy was assessed, comparing CM to systematic lymph node dissection at the time of EPP.
Results: Mediastinal staging by CM +/− PET was performed in 34 patients (Group M). Clinical staging, by CT and/or MRI, was performed in 58 patients (Group C). Overall median survival (MS) from diagnosis was 448 days, but survival in Group M was significantly longer than group C (p = 0.03). There was no difference in the distribution of known prognostic factors or nodal stage between the groups. N2 positive nodes were associated with poor survival (p = 0.02). MS among the N2 patients in Group C was 269 days versus 438 for Group M (p = 0.09). Unexpected N2 disease was found in 11 patients of Group M (NPV 68%). The NPV for stations 7, 4R, and 4L was 79%, 94%, and 97% respectively. Positive N2 nodes inaccessible to CM were found in six patients.
Conclusions: N2 disease is a negative prognostic indicator in MM. CM may allow selection of patients with a better prognosis for EPP.
S139 NEOADJUVANT AND ADJUVANT CHEMOTHERAPY IN A RADICAL TREATMENT PROTOCOL FOR MALIGNANT MESOTHELIOMA WITH EXTRAPLEURAL PNEUMONECTOMY
A. Conybeare, J. G. Edwards, D. J. Stewart, K. J. O’Byrne, D. A. Waller. Glenfield Hospital, Groby Road, Leicester, UK
Aims: To evaluate the feasibility and effects of neoadjuvant and adjuvant chemotherapy as part of a radical surgery protocol for malignant mesothelioma (MM).
Methods: Case notes were analysed from 101 consecutive patients undergoing extrapleural pneumonectomy (EPP) for MM. Case notes were reviewed to determine how many successfully completed the planned trimodality treatment programme, including chemotherapy and radiotherapy. The reasons for non-compliance were recorded. Differences in survival between groups were estimated using Kaplan-Meier analysis and the Log Rank test.
Results: Referrals were received from 28 oncology centres nationwide. Overall median survival from diagnosis was 14.9 months. Neoadjuvant chemotherapy was administered to 22 patients, all of whom underwent successful EPP. Referral to an oncologist to consider adjuvant chemotherapy was made in 53 patients; treatment within threemonths was received by 11 patients. Eight died before assessment for adjuvant therapy and a further nine were considered too unwell. However adjuvant chemotherapy was not offered to 10 patients as there was no residual disease. Five patients refused adjuvant therapy and four were refused therapy as it was too long post operation. Overall survival in the patients receiving neoadjuvant or adjuvant chemotherapy was greater than those not receiving chemotherapy (p = 0.02).
Conclusions: Survival in patients receiving chemotherapy as well as EPP was greater than surgery alone. The success rate at achieving adjuvant chemotherapy was low, therefore we advocate incorporation of neoadjuvant chemotherapy in future trials.
S140 AN INNOVATIVE, AUTOCLAVABLE, SEMIRIGID THORACOSCOPE: IS THIS THE WAY FORWARD?
M. Munavvar, M. A. I. Khan, Z. Waqaruddin, J. Edwards, J. Mills. Lancashire Teaching Hospitals, Preston, UK
Introduction: Thoracoscopy is “the evaluation of the pleural space in a nonintubated patient under conscious sedation” (
). Its yield is far superior to blind pleural biopsy and there is no requirement for GA. The conventional rigid thoracoscope is not widely used in the UK (
). We have for the first time used a semirigid prototype, which is similar in design to a bronchovideoscope. It easily interfaces with standard processors and light sources used for flexible bronchoscopy.
Materials and Methods: The instrument (LTF-160; Olympus; Tokyo, Japan; supplier KeyMed UK) has a handle similar to a standard flexible bronchoscope. The working shaft’s outer diameter is 7 mm and length 27 cm (distal flexible portion 5 cm). It has the advantage of being autoclavable as well. In our series, a single operator (MM) performed 30 procedures on 29 patients between June 2004 and July 2005. All had a unilateral pleural effusion evaluated by contrast CT and had undergone pleural aspiration which had been either unsuccessful or non-diagnostic. The procedure was done in our endoscopy suite under local anaesthesia and sedation with a single puncture technique using a trocar in the midaxillary line. Following suction of fluid the instrument was introduced and the pleural surfaces were examined. Pleural fluid and parietal pleural biopsy samples were obtained. Where appropriate, talc poudrage was performed. A 24 Ch chest drain was inserted routinely and removed following re-expansion of the lung.
Results: 19 men and 10 women were examined. One procedure was abandoned as no fluid could be aspirated. The average age was 69 (range 23–89) years. The combination of clinical findings, CT and pathology achieved a definite diagnosis in 25 of the 28 patients (89.2%). The diagnoses were mesothelioma (8), metastatic carcinoma (6), small cell lung cancer (2), B cell non-Hodgkin’s lymphoma (1), adenocarcinoma lung (1), tuberculosis (1), rheumatoid effusion (1), reactive fibrosis/hyperplasia (2), and chronic pleural inflammation (3). There were no complications.
Conclusions: This is the first ever use of an autoclavable semirigid thoracoscope. There is great potential for its use in the diagnosis and management of pleural disease. With its similarity in design to the standard flexible bronchoscope, respiratory physicians should be able to adapt to its use easily. It is compatible with standard video processors and light sources so little additional investment is required. Even patients with impaired lung function can undergo this procedure safely. It may reduce the need for VATS, which requires general anaesthesia.
Abstract S140
Interstitial lung disease
S141 FACTORS INFLUENCING SUCCESS OF ACHIEVING LUNG TRANSPLANTATION IN PATIENTS WITH PULMONARY FIBROSIS PLACED ON THE WAITING LIST 1999–2004
L. S. Mackay, R. L. Anderson, J. Lordan, J. H. Dark, P. A. Corris, A. J. Fisher. Cardiopulmonary Transplant Unit, Freeman Hospital, Newcastle upon Tyne, UK
Lung transplantation is the only treatment modality proven to provide a survival advantage in pulmonary fibrosis. This therapeutic option is only available to selected carefully assessed patients, however many patients deemed suitable will never achieve transplantation and will die while waiting. The shortage of donor organs undoubtedly contributes to this but in addition late referral to the transplant centre due to the unpredictable progression of the disease may play a role. We evaluated factors influencing successful outcome for patients with pulmonary fibrosis listed for lung transplantation over a five year period. A retrospective review of patient demographics, results of assessment investigations and subsequent clinical outcomes was performed in a single large lung transplant centre.
Between March 1999 and September 2004, 129 patients with pulmonary fibrosis underwent formal inpatient assessment. Sixty nine (53%) were suitable candidates and were listed for lung transplant. Of these 17 (25%) were successfully transplanted, 37 (54%) died on the waiting and 11 (16%) were still waiting at the conclusion of the study. Waiting time on the list for those transplanted was mean 179 (SD 230) days compared with 175 (SD 155) days in those dying on the list, p = 0.99. Mean time on the list for those still waiting was longer at 468 (SD 407) days. Objective differences between those transplanted and those dying on the waiting list were investigated using unpaired student’s t test. There was no significant difference in age, spirometric measures, total lung capacity, gas transfer measures, or six minute walk distance between these two groups. However there was a significant difference in the time from initial diagnosis to initial assessment for transplant, this was significantly less mean 38 (SD 28) months in those dying on the list compared with those transplanted 72 (SD 63) months, p = 0.045. Furthermore, ABO blood group appeared to have a significant effect on the chance of achieving transplant. Thirty seven of those listed were group O, of which only five were transplanted (14%) in comparison with nine transplanted from the 25 blood group A patients (36%) and three transplanted from five blood group B patients (60%). The two group AB patients were not transplanted, (χ2 test, p = 0.042).
Our results suggest that patients with pulmonary fibrosis dying on the transplant waiting list are not waiting longer than those transplanted but appear to come from a phenotype of rapidly progressive disease. Furthermore, we have demonstrated that patients with blood groups A and B are much more likely than group O to receive a transplant due to donor availability. We conclude therefore that rate of disease progression, which is not included in current referral guidelines, should form an important trigger for early transplant referral.
S142 FIBROSING ALVEOLITIS IN SCLERODERMA TRIAL (FAST): A MULTICENTRE PROSPECTIVE RANDOMISED DOUBLE BLIND PLACEBO CONTROLLED TRIAL
R. Hoyles1, R. Ellis1, A. Herrick2, N. Foley3, N. McHugh3, S. Pearson4, P. Emery4, D. Veale4, C. Denton5, C. Black5, A. Wells1, R. duBois1. 1Royal Brompton Hospital, UK; 2Hope Hospital, UK; 3Royal United Hospital, UK; 4Leeds General Infirmary, UK; 5Royal Free Hospital, UK
Introduction: Pulmonary fibrosis in systemic sclerosis (SSc-PF) is associated with significant morbidity and mortality. Cyclophosphamide (Cyc) is the most studied immunosuppressive agent in SSc-PF; however the lack of well constructed randomised controlled trials has hampered advances towards an evidence based approach. Here we report results from the first placebo controlled trial of intravenous Cyc followed by azathioprine in SSc-PF.
Methods: Fotry five patients aged 18–75 years with SSc-PF were recruited from five UK centres. 22 were randomised to receive (A) prednisolone (20 mg alt die) and six intravenous infusions (monthly) of Cyc (600 mg/m2) followed by oral azathioprine (2.5 mg/kg/day); 23 received matched placebo formulations (B). Primary outcome measures were change in forced vital capacity (FVC) and carbon monoxide diffusing capacity (DLCO). Secondary outcomes included changes in high resolution computerised tomography (HRCT) appearance and dyspnoea scores. An intention to treat (ITT) statistical analysis was employed.
Results: At baseline, no significant differences were identified between groups in a number of factors linked to outcome, including age, sex, smoking status, autoantibody profile, disease severity (FVC, DLCO, HRCT), and extent (HRCT), bronchoalveolar lavage cellularity, lung epithelial permeability assessed by 99mTc-diethylenetriamine penta-acetate clearance, and pulmonary artery pressure assessed by echocardiography. 62% of patients completed the first year of the study. Nine patients (20%) were withdrawn due to a significant (>15%) decline in FVC or DLCO (6/9 in group B), two patients (4%) were withdrawn due to treatment side effects (both group A), and six (14%) were withdrawn for non-trial related comorbidity. No episodes of haemorrhagic cystitis or thrombocytopenia in group (A) were identified; persistent haematuria was identified in only one case (group B) with a prior diagnosis of SSc related interstitial nephritis. Group (A) when compared with group (B) demonstrated a statistically significant improvement/stabilisation of FVC at one year; an estimated adjusted treatment effect (treatment B-treatment A) revealed that group (B) had a worse outcome of −4.76% predicted FVC (range −9.38 to −0.14), p = 0.04. No improvement with active therapy was identified for DLCO or secondary outcome measures.
Conclusion: The positive response of FVC to active therapy is consistent with data from the Scleroderma Lung Study of oral Cyc, and supports the use of Cyc with low dose prednisolone in SSc-PF (Tashkin DP, ATS 2005 (B72)). The treatment advantage with active therapy is likely to be understated due to the ITT analysis. Intravenous Cyc appears to confer an advantage over previous reports of toxicity with the oral regimen (
).
S143 OUTCOMES OF PULMONARY RENAL SYNDROME IN PATIENTS WITH ANCA ASSOCIATED VASCULITIS
A. Patel1, P. Ind2, C. D. Pusey1, G. Gaskin1, A. Salama1. 1Renal & 2Respiratory Sections, Division of Medicine, The Hammersmith Hospital, Imperial College London, UK
Pulmonary haemorrhage is a recognised serious complication of antineutrophil cytoplasmic antigen (ANCA) associated vasculitis and antiglomerular basement membrane disease (anti-GBM). However, outcome data are lacking in this subgroup of patients. We retrospectively analysed all such patients in our database from the last 21 years with pulmonary haemorrhage proven by increased KCO and consistent clinical features. This group of patients were initially managed in a similar way with plasma exchange, steroids and cyclophosphamide.
We identified 71 patients (32 male and 39 female with a mean age of 67.2 years) with antibodies to ANCA (58) or anti-GBM (8). 34 patients were positive for cANCA with a mean PR3 of 67.3% (SD = 33.5; 23 Wegners, 1 Churg-Strauss, 1 polyarteritis nodosa, 4 necrotising glomerulonephritis with crescents, 5 undifferentiated vasculitis) and 24 for pANCA with a mean MPO of 50.0% (SD 31.2; 3 lupus, 3 necrotising glomerulonephritis, 2 Churg-Strauss, 1 Wegners, 1 polyarteritis nodosa, 1 microscopic polyangitis, 13 undifferentiated vasculitis). Five patients had non-ANCA associated vasculitis (2 Wegners, 2 Churg-Strauss, 1 undifferentiated vasculitis).
The mean creatinine at presentation was 298.5 (SD 273.9). Only 13 chest radiographs (CXRs) were suggestive of pulmonary haemorrhage in view of the clinical presentation (mean creatinine 573.2). Seven exhibited signs of localised parenchymal or pleural fibrosis.
Mean creatinine at last follow up was 250.6 (SD 250.2) with a mean time from pulmonary haemorrhage of 1918.6 days (SD 1472.7). At this is time, 30 patients were alive (mean creatinine 131.2; 2716.1 days mean follow up), 28 died (mean creatinine 366.5; 1185.7 days mean time to death) and three were lost to follow up. 23 patients required long term renal replacement therapy (16 of these patients died). 10 additional patients developed parenchymal or pleural fibrosis on CXR. These appeared to be non-significantly more frequent in the ANCA group but did not exhibit a relation with immunefluorescence or antibody titre.
CXRs were consistent with pulmonary haemorrhage in only 18% cases. A high creatinine was associated with an abnormal CXR during pulmonary haemorrhage and a raised creatinine at follow up or requirement of renal replacement therapy was associated with a higher mortality. Pulmonary fibrosis was more likely with ANCA associated pulmonary haemorrhage.
S144 ASSOCIATION BETWEEN THE GENOTYPE OF THE TNF LOCUS AND ACUTE REJECTION FOLLOWING LUNG TRANSPLANT
I. A. Forrest1, C. Ward1, S. Scorfield2, D. M. Murphy1, C. E. Chapman3, V. Carter3, P. Botha1, J. H. Dark1, P. A. Corris1, P. G. Middleton2. 1Applied Immunology and Transplantation Group, Freeman Hospital and the University of Newcastle upon Tyne; 2Haematological Sciences, School of Clinical and Laboratory Sciences, The Medical School, University of Newcastle upon Tyne NE2 4HH, UK; 3Department of Histocompatibility & Immunogenetics, National Blood Service, Newcastle-upon-Tyne NE2 4NQ, UK
Background: The G-308A polymorphism in the promoter region of the TNFA gene has been shown to associate with acute rejection following heart transplant. The effect of this polymorphism on acute rejection following lung transplant has not been investigated.
Methods: We investigated 199 chronologically sequential adult lung transplant recipients from UK and Ireland who underwent transplantation in the Freeman Hospital transplant programme. Genotypes for candidate TNF polymorphisms were determined independently on both groups and the results compared with clinical outcomes.
Results: We found that possession of the TNF –308 A allele associated with increased likelihood of acute rejection. This characteristic was seen in both individual study groups and in the overall cohort (p = 0.022, Fisher’s exact test) and did not include extended haplotypes of the MHC, within which the TNFα locus resides. Possession of the A allele also suggested an association with earlier development of BOS, but this effect did not achieve statistical significance in our study.
Conclusion: The A allele of the TNF-308 polymorphism, previously associated with rejection in other forms of organ transplant, also associates with acute rejection following lung transplant and may represent a marker for an extended risk haplotype.
S145 THE F2R (PROTEINASE ACTIVATED RECEPTOR-1) -506INS POLYMORPHISM ASSOCIATES WITH SUSCEPTIBILITY TO SARCOIDOSIS IN TWO POPULATIONS
P. Lawson1, H. Booth1, H. Beynon2, C. Read1, G. Laurent1, R. Chambers1, M. Hill1. 1Centre of Respiratory Research, UCL, London; 2Royal Free Hospital, London, UK
Background: The activation of proteinase activated receptor-1 (PAR1) by coagulase proteases such as thrombin plays a major role in lung inflammation and fibrosis.1,2 Expression of the PAR1 gene (F2R) is raised in fibroproliferative lung disease;2 however, its regulation and the role of genetic influences has not been fully characterised. Several polymorphisms have been reported in the F2R gene, including two promoter polymorphisms, -506ins (a 13 base pair insertion) and -1427C>T, and an intronic polymorphism, -14 (IVS) A>T.3 We sought to determine whether these polymorphisms associate with susceptibility to sarcoidosis, a granulomatous disease with variable outcome, in which 5–10% of patients with lung involvement develop a persistent progressive disease leading to pulmonary fibrosis.
Methods: The F2R polymorphisms were genotyped in a North European white population using PCR technique, restriction digest, and sequencing. We sought to replicate any positive findings in a second population of UK Afro-Caribbeans.
Results: Our main finding of the three polymorphisms investigated was that, for the -506ins polymorphism, carriage of the insertion associates with susceptibility to disease in both ethnic groups. In the whites (309 controls, 281 sarcoidosis patients), carriage of the -506ins (-/ins and ins/ins combined) gave an OR of 1.45 (95% CI 0.97 to 1.86), p = 0.032. A gene dose effect was seen, with the heterozygote (-/ins) risk being 1.35 (95% CI 0.95 to 1.91), p = 0.091 and the homozygote (ins/ins) risk being 2.49 (95% CI 1.11 to 5.57), p = 0.027. This result was replicated in the Afro-Caribbeans (using 262 controls, 98 sarcoidosis patients), where carriage of the -506ins gave an odds ratio (OR) of 2.63 (95% CI 149 to 4.66), p<0.001. A gene dose effect was again seen, with the heterozygote (-/ins) risk being 2.15 (95% CI 1.18 to 3.95), p = 0.013 and the homozygote (ins/ins) risk being 4.01 (95% CI 2.01 to 8.03), p<0.001. No association with sarcoidosis was found for the -1427C>T or-14 (IVS) A>T polymorphisms.
Conclusion: This is the first report of an F2R polymorphism associating with respiratory disease. Replication of the association in two different ethnic groups supports a role of F2R polymorphisms in susceptibility to sarcoidosis. The Afro-Caribbean association is interesting as this ethnic group has a more severe clinical phenotype than whites. Confirmation of this finding in a larger cohort is warranted. Elucidation of the function of these and other F2R polymorphisms may shed light on the mechanism by which this receptor contributes to fibroproliferation.
1
2
3
Respiratory muscle function in obstructive lung disease
S146 QUADRICEPS MUSCLE ENDURANCE IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE: CORRELATION WITH MUSCLE BIOPSY DATA
E. B. Swallow1, H. R. Gosker2, K. A. Ward2, A. J. Moore1, N. S. Hopkinson1, A. M. W. J. Schols2, J. Moxham3, M. I. Polkey1. 1Respiratory Muscle Laboratory, Royal Brompton Hospital, London SW3 6NP; 2Department of Respiratory Medicine, Maastricht University, The Netherlands; 3Respiratory Muscle Laboratory, Kings’ College Hospital, London SE5 9RS, UK
Introduction: Quadriceps muscle endurance is reduced in patients with chronic obstructive pulmonary disease (COPD) (Couillard et al. AJCCRM 2003:167). It has also been found that there is a reduction in Type 1 fibres (Jakobsson et alERJ 1990:3) and a reduction in oxidative enzyme activity (Maltais et al. AJCCRM 1996:153) in the quadriceps muscle of patients with COPD compared to healthy control subjects. Current methods to assess quadriceps endurance, however, are effort dependent. Here we report a non-volitional method to assess quadriceps endurance in patients with COPD and healthy control subjects, and have related the physiological findings to muscle biopsy data.
Methods: Eight patients with COPD (FEV1 24.8 (SD 4.04)% predicted) and eight healthy age matched control subjects (FEV1 95.5 (SD 20.7)% predicted, p<0.001) were studied using a Magstim Rapid repetitive magnetic stimulator (RMS) with a specially designed mat coil wrapped around the quadriceps muscle. Subjects were studied supine, with the knee flexed at 90° over the end of the bed. The ankle was linked, by an inextensible strap, to a strain gauge. Subjects relaxed for 20 minutes prior to the RMS protocol. The stimulator was run at 30 Hz, at a duty cycle of 0.4 (2 s on, 3 s off) for 45 trains. The stimulator output was adjusted for each subject so as to generate 15–20% of the subjects’ supine maximal isometric voluntary contraction (MVC). Quadriceps surface EMG was recorded simultaneously. All subjects underwent a quadriceps muscle biopsy and the samples were analysed with respect to enzymatic activity (citrate synthase, CS and phosphofructokinase, PFK) and myosin heavy chain (MyHC) isoforms protein expression as an index of fibre type composition.
Results: Time to fatigue to 70% of baseline force (T70) was significantly shorter in the COPD group than the control group (55.6 (SD 25.9) s v 121 (SD 38.7) s, p = 0.0014). There was no decrement in EMG signal throughout the endurance run. There was a reduction in oxidative capacity seen in the COPD group (CS/PFK 0.074 (SD 0.02) v 0.13 (SD 0.04), p = 0.007) and a reduction in expression of MyHC Type 1 (29.4 (SD 11.8)% v 48.1 (SD 6.4)%, p = 0.0015). Positive correlations were observed between T70 and CS/PFK (r = 0.66) and % MyHC Type 1 (r = 0.68).
Conclusion: Quadriceps performance assessed using RMS, detects reduced endurance in patients with COPD compared to control subjects. The magnitude of this reduction correlates with the severity of quadriceps myopathy, whether judged by oxidative enzyme activity or by fibre type proportions.
S147 QUADRICEPS STRENGTH PREDICTS MORTALITY IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
D. Reyes, E. B. Swallow, E. Cetti, A. Moore, N. S. Hopkinson, M. Khan, J. Moxham, M. I. Polkey. Respiratory Muscle Laboratories, Royal Brompton and Kings College Hospitals, London, UK
Introduction: Prognosis in chronic obstructive pulmonary disease (COPD) is only poorly predicted by indices of airflow obstruction. Recently it has been reported that quadriceps cross sectional area, an index of muscle mass, is an accurate predictor of mortality in COPD (Marquis et al. AJCCRM 2002:166). However measurement of quadriceps cross sectional area requires a CT scan and, at least in the UK, there is strong competition for access to CT scanners. We therefore hypothesised that a physiological measure of quadriceps bulk, the maximum voluntary contraction force (MVC), might also predict mortality in patients with COPD.
Methods: We identified 171 patients with COPD who had had a quadriceps MVC over the last five years.
). The greatest value obtained was reported and expressed as a % of predicted using the formula proposed by Edwards et al. The status of the patient (alive/dead) was ascertained by a written questionnaire sent to the patients GP. The response rate was 82%. The end point measured was death or lung transplantation (n = 2).
Results: Overall survival of the cohort was 96% at one year and 91% at two years. Cox regression analysis was used to identify factors predicting mortality. In univariate analysis the following hazard ratios (95% confidence intervals) were observed: age 1.04 (0.99 to 1.08) p = 0.12, body mass index (BMI) 0.99 (0.93 to 1.06) p = 0.81, quadriceps MVC (% predicted) 0.98 (0.97 to 0.99) p = 0.007, FEV1 (%predicted) 0.98 (0.95 to 1.007) p = 0.15. In multivariate analysis, with adjustment for BMI and other covariates, we observed that only Quadriceps MVC wielded a prognostic effect with the following hazard ratios (95% confidence intervals): age 1.05 (0.99 to 1.1) p = 0.08, Quadriceps MVC (% predicted) 0.98 (0.96 to 0.9967) p = 0.004, FEV1 (%predicted) 0.97 (0.94 to 1.0) p = 0.08. Thus for each fall in quadriceps MVC of 1% an approximate 2% increased risk of death was observed.
Conclusion: Quadriceps MVC is a more powerful predictor of death in COPD than FEV1 or BMI. Like CT measured quadriceps cross sectional area, we believe the MVC to reflect quadriceps muscle bulk but MVC is radiation free and does not require expensive equipment.
S148 LIMB AND INSPIRATORY MUSCLE DYNAMIC STRENGTH IN PATIENTS WITH MODERATE CHRONIC OBSTRUCTIVE PULMONARY DISEASE
A. A. Ionescu1, T. D. Mickleborough2, C. E. Bolton1, M. R. Lindley2, K. Chatham1, L. S. Nixon1, D. J. Shale1. 1Respiratory Medicine, Cardiff University, Llandough Hospital Cardiff, Wales; 2Department of Kinesiology, Indiana University, USA
We investigated the upper and lower limb and inspiratory muscle strength in relation to the habitual physical activity in 25 patients (age 70.5 (6.9) years) with moderate chronic obstructive pulmonary disease (COPD) (FEV1 = 49.4 (16.4)% predicted) and 10 healthy subjects (HS). Spirometry, body composition by dual energy x ray absorptiometry and physical activity by questionnaire (METs, metabolic equivalents of resting energy expenditure per day, and separately for activities using mainly upper or lower limb force) were recorded during clinical stability (no exacerbation for at least one month). In random order the following were performed on different days: weight lifting with upper and lower dominant limbs and inspiratory muscle resistance test, all at 75% of the maximum weight lifted, or maximum inspiratory pressure (MIP), to voluntary exhaustion; pulse and oxygen saturation (SaO2) were recorded during the activities and a Borg dyspnoea score at the end. The number of repetitions (every 10 seconds) and the weight lifted were recorded. All patients had a fat free mass greater than the lower 25th percentile for a healthy age matched population. Patients were less physically active than HS (36.2 (5.9) versus 43.4 (4.5) METs per day, p<0.01); no difference was found between the METs per day activities involving mainly upper compared to those involving mainly lower limbs. The weight lifted and repetitions for lower limb were lesser in patients (3.5 (1.2) v 4.4 (0.7) kg and 26.9 (11.6) v 48.0 (22.2) repetitions p<0.05), for upper limb only the number of repetitions was less for patients (24.1 (10.8) v 41.6 (25.3) p<0.05). The Borg score was similar for patients and HS. MIP was less for patients, p<0.01. SaO2 was less for patients, p<0.05 for all activities than for HS. For patients both SaO2 and the pulse increased after the inspiratory muscle test, p<0.05, while SaO2 decreased for upper and lower limb weight lifting, p<0.01 (96.3 (1.4) v 95 (1.5) for upper and 96.1 (1.3) v 95.1 (1.7) for lower limb activity). For patients and HS the METs during habitual activities were directly related to SaO2 post weight lifting (upper and lower limb) and MIP (p<0.01 for all), but not to FEV1.
In conclusion, patients with moderate COPD have reduced dynamic strength of upper and lower limbs and reduced SaO2, independent of FEV1.
These data suggest that muscle reconditioning and rehabilitation may need to be initiated early in the course of COPD in an attempt to improve the muscle strength and to reduce the reduction in oxygen saturation during activity in patients with moderate COPD.
Acknowledgements: Dr P Edwards, Ely Bridge Surgery; Dr S Edwards, North Cardiff Medical Centre.
Supported by the British Lung Foundation, CAPRICORN, and GSK.
S149 THORACO-ABDOMINAL ASYNCHRONY BETTER PREDICTS EXERCISE TOLERANCE THAN FEV1 IN PATIENTS WITH SEVERE PERSISTENT ASTHMA
C. O. Prys-Picard, R. M. Niven. North West Lung Research Centre, South Manchester University Hospital Wythenshawe, Manchester, M23 9LT, UK
Introduction: Thoraco-abdominal asynchrony (TAA) exists when the rib cage (RC) and abdominal (AB) compartments move paradoxically—that is, when the rib cage expands, the abdomen contracts and vice versa. This induces inefficiency into respiratory effort. The effect of this on exercise tolerance in severe asthma has not been investigated so far.
Methods: Thirty one non-smoking patients (24 female, 7 male, mean age 40 years) with severe persistent asthma (treatment with inhaled corticosteroids, long acting beta agonists and at least two unexpected healthcare resource usage episodes in the last year) were recruited. Respiratory patterns were measured using respiratory inductance plethysmography (LifeShirt, Vivometrics Inc, CA, USA) both at rest and during an incremental shuttle walk test (SWT). Raw traces were analysed using Vivologic software. Phase Relation Total Breath (PhRTB) is a measure of TAA. Mean values were calculated from samples totaling at least 200 breaths at rest, and from the entire duration of the walk test. Exercise tolerance was recorded. Spirometry was performed before SWT.
Results: PhRTB at rest was associated with PhRTB during exercise (Pearson correlation coefficient 0.42 sig = 0.019). PhRTB during exercise was significantly associated with exercise distance on SWT (Pearson correlation coefficient −0.452 sig = 0.011) (see fig). PhRTB during exercise is also correlated to FEV1 expressed as percentage predicted (Pearson correlation −0.366 sig 0.043). After regression analysis with SWT distance as the dependant variable and FEV1 as a co-variable, the β coefficient for PhRTB was −0.343 sig 0.056, and for FEV1 β coefficient = 0.3 sig 0.092). Stepwise regression analysis suggested that FEV1 did not significantly add to the predictive power of PhRTB.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
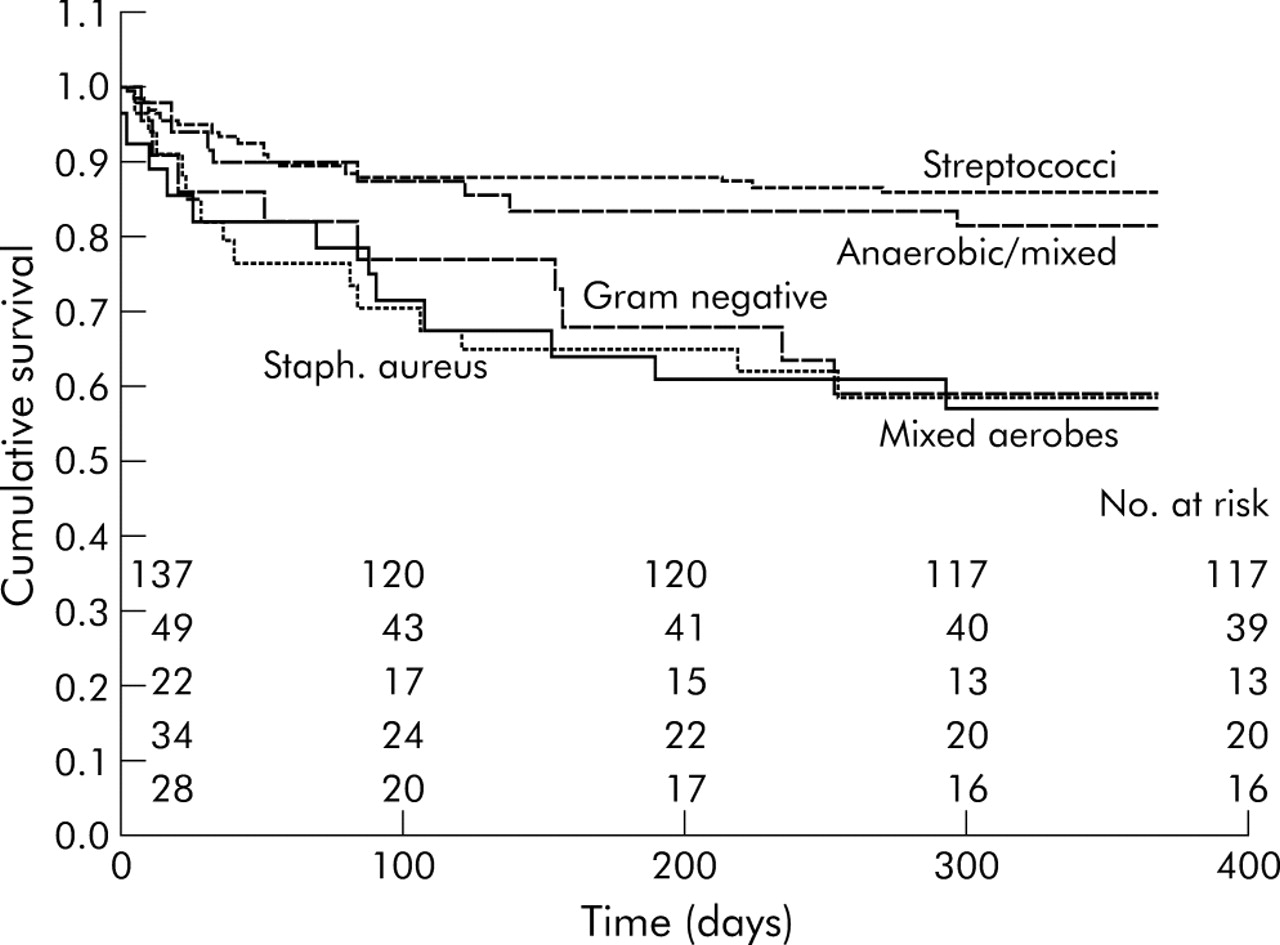{kind=link}
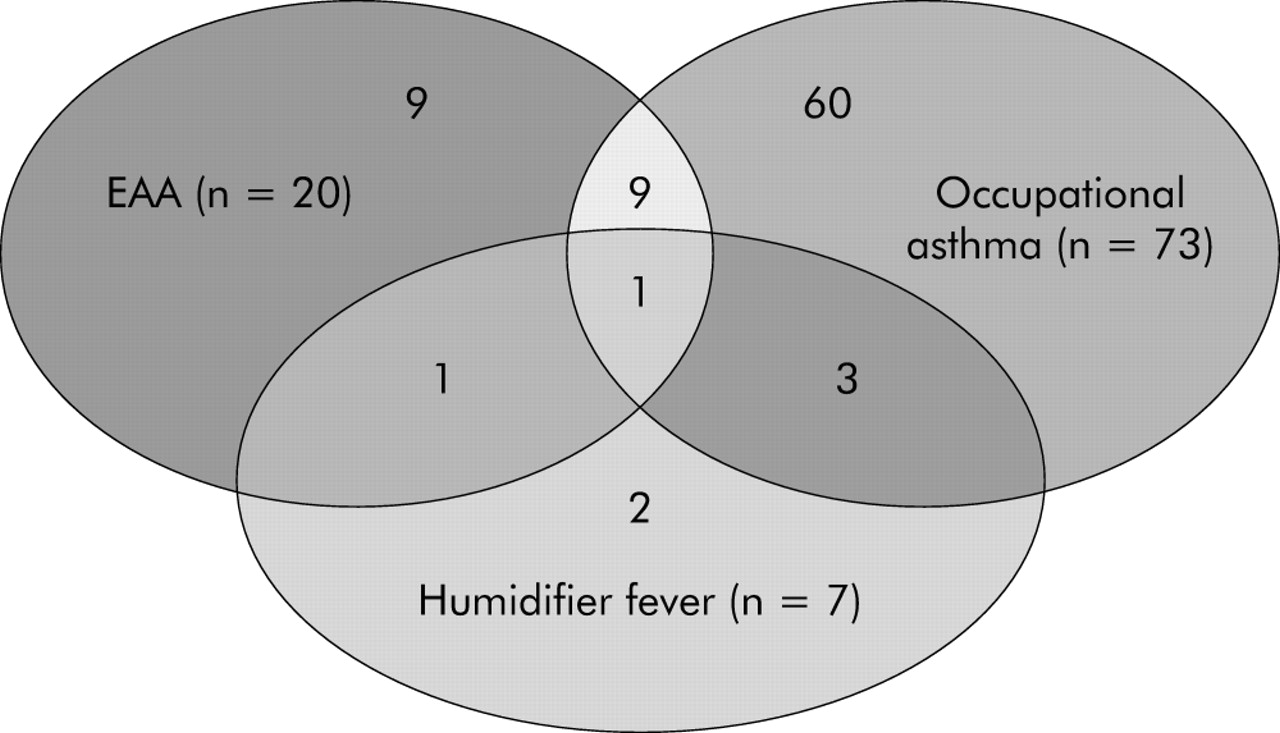{kind=link}
{kind=link}
Conclusion: TAA may be a contributing factor to exercise tolerance in patients with moderate to severe asthma that has previously been unrecognized. Studies in COPD suggest that TAA is not related to FEV1 but is related to hyperinflation (
). In asthmatic subjects TAA may be secondary to the disease process or may exist as a primary acquired phenomenon. If the latter is true it may represent a form of dysfunctional breathing that is amenable to therapy.
S150 INSPIRATORY LUNG FUNCTION MEASUREMENTS CORRELATE WITH MRC BREATHLESSNESS SCORE IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS
T. Powell1, E. C. Smith1, J. Bell2, N. A. Jarad1. 1Department of Respiratory Medicine, Bristol Royal Infirmary, Bristol; 2Clement Clarke Ltd, Harlow, Essex: now Canday Medical Ltd, Newmarket, Suffolk, UK
Background: We have shown that inspiratory measurements are repeatable in patients with chronic obstructive pulmonary disease (COPD). The relation between forced expiratory volume (FEV1) and effort tolerance score in patients with COPD is well established. We investigated the relation of inspired volumes with MRC dyspnoea score in patients with COPD.
Methods: Patients with a clinical diagnosis of COPD, ⩾40 years of age and ⩾20 pack-years smoking history were studied. Subjects scored their effort tolerance on the MRC Breathlessness scale. All inspiratory measurements were made on a Clement Clarke handheld inspiratory meter. Patients took a maximum inspiratory breath from residual volume and we measured five times FIV1, FIVC, and PIF; the maximum values were used for analysis. Analysis of variance was used to compare inspiratory measurements and MRC scores.
Results: This study was completed by 81 patients (54M, 27F), mean age 68 years (range 49–90), mean FEV1/FVC% 48% (range 20–69) who were recruited and completed all tests. Two patients withdrew from the study.
Abstract S150
A significant inverse relation between the mean value for all inspiratory parameters and effort tolerance score for patients and control subjects is shown in the table.
Conclusion: Maximum inspiratory measurements in patients with COPD are inversely correlated with the MRC effort intolerance score. These measurements could provide important objective outcome measures in patients with COPD.
Sponsored by Clement Clarke International.
Diagnosis and management of pulmonary embolism
S151 BTS STUDY OF THREE VERSUS SIX MONTHS’ ANTICOAGULATION FOR PULMONARY VENOUS THROMBOEMBOLISM
I. A. Campbell on behalf of the Research CommitteeLlandough Hospital, Cardiff, UK
The optimum duration of oral anticoagulant therapy after an episode of pulmonary venous thromboembolism (PVTE) is unknown, with recommendations ranging from three months to lifelong prophylaxis. The Research Committee has conducted a prospective, randomised study comparing three months’ with six months’ anticoagulation, with heparin for five days accompanied and followed by warfarin (target INR between 2.0 and 3.5) in patients experiencing an episode of PVTE, but with no known underlying risk factors for recurrence.
Physicians from 44 UK hospitals entered 807 patients over a 41 month period, of whom 742 fulfilled the inclusion criteria. Patients were followed up for one year from the start of treatment. There were 361 (50% male) and 381 (57% male) subjects in the three months’ and six months’ groups and mean ages were 58.8 (SD 15.7) and 58.6 (SD 15.1) years respectively.
During treatment PVTE failed to resolve, extended or recurred (failure of treatment) in six patients (1 with fatal consequences) in the three months’ group compared with 13 in the six months’ group (3 fatal). After the end of treatment there were 25 recurrences (1 fatal) in the three months’ group compared with 16 (none fatal) in the six months’ group. Failures of treatment plus recurrences after treatment thus occurred in 8.6% who had received three months’ anticoagulation compared with 7.6% who had received six months’ (p = 0.72; 95% CI −3.0% to +4.9%), with death due to PVTE in 0.6% and 0.8% respectively.
There were no major haemorrhages during treatment in the three months’ group whereas in the six months’ group 8 (2.1%) experienced non-fatal, major haemorrhages (p = 0.69; 95% CI OR <0.70) and one further patient died during treatment from a cerebrovascular accident of unknown cause.
Adverse outcomes (death due to PVTE or haemorrhage, non-fatal failures of treatment, non-fatal recurrences after treatment and non-fatal, major haemorrhages) were seen in 31 (8.6%) in the three months’ group and 37 (9.7%) of those in the six months’ group (p = 0.69; 95% CI −5.3% to +3.0%).
The evidence from this trial suggests that, for patients in the UK with PVTE where there are no known risk factors for recurrence, there is little, if any, advantage in increasing the duration of anticoagulation from three months to six months. The confidence intervals indicate that any possible advantage would be small and would need to be judged against the increased risk of haemorrhage associated with the longer duration of warfarin therapy.
S152 DIAGNOSIS AND TREATMENT OF PULMONARY EMBOLISM: FINDINGS FROM THE VERITY VTE TREATMENT REGISTRY
N. Scriven1, P. Rose2, F. Pressley3, R. Arya4, D. O’Shaughnessy5 on behalf of the VERITY investigators1The Calderdale Royal Hospital, Halifax; 2Warwick Hospital, Warwick; 3Royal Gwent Hospital, Newport; 4King’s College Hospital, London; 5Southampton General Hospital, Southampton, UK
Background: The diagnosis and treatment of pulmonary embolism (PE) is evolving. The British Thoracic Society (BTS) guidelines for the management of suspected acute PE offer scientifically validated clinical algorithms for diagnosis, and a number of hospitals in the UK now offer outpatient management of venous thromboembolism (VTE), including PE. It is not clear to what extent the BTS guidelines are implemented, or whether outpatient treatment provides improved care and outcome.
Methods: The diagnosis and treatment of PE was investigated in centres enrolling patients in VERITY (VEnous thromboembolism RegIsTrY), a multicentre, observational registry, initiated in the UK to assess and improve VTE practice patterns at centres using low molecular weight heparin (LMWH) for outpatient treatment.
Results: At 33 outpatient centres, PE was confirmed in 507 of 993 patients with suspected PE. Review of Wells pre-test probability (PTP) and D-dimer (d-d) validate the strategy of excluding PE on the basis of a low PTP in combination with a negative d-d. Only one patient with low PTP and negative d-d was recorded as PE positive, but this was not confirmed after several radiology opinions. V/Q scan was the most common diagnostic test, undertaken in almost 50% (458/993) of cases of suspected PE. Few CT pulmonary angiography (CTPA) scans were performed (222/993; 22% of all suspected cases of PE), despite the fact that CTPA is now the recommended initial lung imaging modality for non-massive PE. In all, 69% (688/993) received a chest x ray (CXR); worryingly, it appears that 40% (203/507) of patients with proven PE, and a proportion of patients undergoing V/Q scan, did not have a CXR. 28% (281/993) of patients were investigated with Doppler ultrasound, which may reflect replacement of an imaging test, such as CTPA, or use within a diagnostic algorithm. About half of patients with PE were deemed suitable for outpatient treatment (53%; 259/487), compared with 89.6% treated in the outpatient setting for DVT. Patients suspected of PE received a mean of three doses of LMWH, reflecting recommended practice of initiation of LMWH while waiting for confirmatory imaging tests. The mean number of doses in patients with confirmed PE was higher and as expected (n = 8). The 90 day fatality rate in patients diagnosed with PE was 12%, and was higher than patients treated for DVT (3%).
Conclusions: These analyses provide initial insight into PE practice patterns and show that CTPA and CXR are underused. Future analysis of the registry will examine the impact of these diagnosis and treatment patterns on patient outcomes.
S153 CAN THE USE OF BTS PULMONARY EMBOLISM GUIDELINES HELP IN REDUCING UNNECESSARY CT PULMONARY ANGIOGRAM SCANNING?
P. K. Sarkar1, S. Kaneri2, M. Farrugia2, G. E. Wilson1. 1Department of Medicine, 2Department of Radiology, Newham University Hospital NHS Trust,Glen Road, Plaistow, London E13 8SL, UK
Aim: The diagnosis of pulmonary embolism (PE) requires several investigations including some form of imaging. The British Thoracic Society (BTS) guidelines recommend a systematic approach based on assessment of clinical probability and a negative D-dimer to decide which patients will need CT pulmonary angiogram (CTPA). In a university hospital where V/Q scan is not available on site, we wanted to see whether doctors are following BTS guidelines in cases of suspected PE. We also aimed to find out what percentage of CTPAs could be avoided if we had followed the guidelines. Our hospital does not have a locally agreed protocol for investigation of suspected PE.
Methods: We prospectively collected data from the notes of 85 consecutive patients who attended the Accident & Emergency department or were admitted and underwent CTPA for suspected PE. We recorded the reason for considering PE, whether clinical probability was assessed, alternative diagnoses considered, and the sequence of investigations, D-dimer, if done, and CTPA result. Wherever clinical probability was not assessed, it was assigned by the audit team for the sake of our analysis. Our laboratory uses NycoCard a rapid semiquantitative immunoassay (negative predictive value 97%).
Results: In total two patients with probable massive PE, seven patients high clinical probability, 32 patients intermediate, and 12 patients low. 32 patients could not be assigned a clinical probability because of inadequate data. In only 22 cases were BTS guidelines followed, in 55 cases they were not and in eight cases no conclusion could be reached because of insufficient data. Out of 85 cases, a CTPA scan was positive for PE in 13 (15%). In only nine of these were BTS guidelines followed. Analysing the data showed that a further 12 CTPAs could have been avoided in those patients with intermediate or low clinical probability and a negative D-dimer (CTPA was negative in this group). In 37 cases CTPA was chosen as the initial investigation, whereas D-dimer assay should have been used first. CTPA was positive in only four of these patients. We presume that in many of these 37 patients CTPA studies could be avoided if BTS recommendations were adhered to.
Conclusion: We found that there is very poor adherence to BTS guidelines in our hospital when investigating cases of suspected PE. In the absence of a locally agreed protocol, this is leading to unnecessary CTPA use. Considering the high costs of CTPA and the radiation dose to patients, the use of BTS guidelines is recommended for the investigation of suspected PE.
1
S154 THE UTILITY OF MULTISLICE COMPUTED TOMOGRAPHIC PULMONARY ANGIOGRAPHY IN THE DIAGNOSIS OF PULMONARY EMBOLISM: A REVIEW OF 800 CASES FROM A DISTRICT GENERAL HOSPITAL
N. W. H. Townsend, C. F. Loughran. Department of Clinical Radiology, Macclesfield District General Hospital, Nucleus Branch, Victoria Road, Macclesfield, Cheshire SK10 3BL, UK
Aim: At our institution, computed tomography pulmonary angiography (CTPA) is now the examination of choice for clinically suspected pulmonary embolus (PE). The purposes of this study were (1) to determine the incidence of PE in a district general hospital (2) to identify the other findings reported on CTPA that may be clinically relevant.
Methods: This was a retrospective review of 800 CTPA reports from 20 November 2001, when this service was introduced, to 31 March 2005. Images were acquired on a four slice Toshiba Aestion scanner with 1 mm slice thickness. Surestart contrast media administration was used during a single breath hold. Data were tabulated and coded for analysis.
Results: 800 CTPAs were performed during the 40 month study period. There were 344 (43.0%) males and 456 (57.0%) females with a median age 70 years (range 19–98 years). Five (0.6%) scans were suboptimal for the diagnosis of PE and excluded from further analysis. The incidence of PE in this cohort was 164/795 (20.6%). There were no differences in median age or sex distribution between those that had or did not have PEs. No abnormality was found in 158/795 (19.9%) cases. In the remaining 473 (59.5%) CTPAs, 973 alternative pathologies were identified. These included pleural effusion 203/973 (20.9%), consolidation 180/973 (18.4%), atelectasis 115/973 (11.8%) and suspected or confirmed malignancy 63/973 (6.5%). Less common findings were classified as bronchopulmonary 179/973 (18.4%), cardiovascular 94/973 (9.7%), gastrointestinal 77/973 (7.9%), and miscellaneous 62/973 (6.4%).
Conclusions: The incidence of PE in this cohort was 20.5%. When PE was excluded, CTPA identified other findings in 59.1% of studies. These may help establish an alternate diagnosis in the absence of PE.
S155 OUTPATIENT TREATMENT OF PATIENTS WITH PULMONARY EMBOLISM: RESULTS OF AN OBSERVATIONAL STUDY
C. W. H. Davies1, J. Wimperis2, E. S. Green3, K. Pendry4, J. Killen5, I. Medhi6 on behalf of the UK PE Study Group1Royal Berkshire NHS Trust, Reading; 2Norfolk and Norwich Healthcare NHS Trust, Norwich; 3Great Western Hospital, Swindon; 4Wrightington, Wigan and Leigh NHS Trust, Wigan; 5Queen Elizabeth Hospital, Gateshead; 6Milton Keynes General Hospital, UK
Introduction: Pulmonary embolism (PE) can be a serious and occasionally fatal disease, but many patients have a very low risk level for morbidity or mortality and might be treated as outpatients (OP) once diagnosis is confirmed. We have previously reported phase 1 of this study and showed that 44% patients (
) did not develop significant adverse events during the first eight days—that is, while inpatients and so could have been managed as OP. This is an interim report of phase 2, using exclusion criteria derived from phase 1, to assess safety and acceptability of an OP protocol.
Methods: 107 patients with confirmed PE from 6 centres were recruited. All patients were treated with 175 IU/kg tinzaparin (Innohep) daily and warfarin to achieve a target INR 2.5 and were discharged within 72 hours of presentation with PE symptoms. Patients were excluded from OP treatment if: age <18, required admission for additional monitoring or treatment, active bleeding or bleeding disorder, poor compliance or mobility, pregnant, previous PE, co-existing major DVT, or patient preference. Outcome measures were: death, recurrent thrombotic events, anticoagulation complications (early and late), bed days saved, and patient satisfaction using a 10 point visual analogue score.
Results: Mean length of stay was 1.3 (SD 1.2) days. Total duration of tinzaparin was 7.6 (SD 2.4) days. All patients completed the acute treatment phase with tinzaparin and data from this period was available for 100% patients. Completed three month follow up data were available for 93 (86.9%) patients. No significant adverse events occurred within the tinzaparin treatment period—that is, when they would normally have been inpatients, but one patient experienced an anxiety episode requiring reassessment. During the three month follow up there were 2/93 (2.2%) deaths, 1/93 (1.1%) thromboembolic and 0/93 (0%) bleeding events. None of these events was related to OP treatment. Tinzaparin was continued for a mean of 5.5 (SD 2.4) days after discharge, indicating that up to 5.5 hospital bed days were saved by OP treatment protocol. 79.5% of patients completed the satisfaction score—the mean score was 9.3 (SD 1.3) indicating patients were highly satisfied with OP treatment.
Conclusion: This study shows that selected patients with confirmed PE can be safely discharged and receive OP anticoagulation without leading to any significant adverse events during the immediate anticoagulation phase where patients may usually remain in hospital. This treatment which is similar to current treatment for DVT may save up to 5.5 bed days per episode and is highly acceptable to patients.
S156 PULMONARY EMBOLISM AND PULMONARY HYPERTENSION: IS OUR FOLLOW UP ADEQUATE?
N. Simmonds, A. Sheth, B. P. Madden. St Georges’ University Hospital, UK
Background: Pulmonary embolism (PE) may subsequently lead to the development of pulmonary hypertension (PH). We wished to assess the incidence of PH in patients with PE referred to us. Furthermore, we studied whether there was an association between the number, site, and extent of thrombus formation and the subsequent development of PH.
Methods: Patients referred to the pulmonary hypertension clinic with a diagnosis of PE were followed prospectively to assess the impact of the thrombotic episode on their pulmonary haemodynamics. The diagnosis of PE was made on V/Q scan and CT pulmonary angiogram appearances. 35 consecutive patients were referred (18 male, 17 female, age range 21–80 years). All had been on full anticoagulation for at least six months.
Results: Three patients had subsegmental thrombus and the remainder had segmental or central vessel thrombus. The lower lobes were affected more than the upper lobes (18 v 11). Five patients had large central thrombus in the main pulmonary arteries and one had significant intracardiac thrombus present. Eight patients had multiple V/Q defects throughout both lung fields.
59% showed signs of PH on 2D echocardiography. At right heart catheterisation (RHC), the following measurements were obtained: RA mean (median 10 mm Hg; range 3–26), PA mean (31; 6–85), PCWP mean (19; 6–50), RV systolic (41; 16–130), cardiac output (5 l/min; 2.3–12), and PVR (2.6 wood units; 0.4–8.3). 68% had PH based on echo/RHC findings. There was no significant correlation between the extent and region of the clot/s and the degree of PH. Currently all the patients with PH continue on warfarin.
Conclusions: This study reinforces the significance of PH following PE and highlights the importance of having a comprehensive follow up service. It also suggests that using an arbitrary duration of anticoagulation for all patients, without knowledge of pulmonary haemodynamics in selected patients, may not be appropriate.
Linked Articles
- Miscellaneous