Article Text

Statistics from Altmetric.com
Acute pulmonary embolism (PE) is of interest to physicians of almost all disciplines, as it is encountered across the entire spectrum of clinical medicine. It is estimated that as many as 200 000 patients die annually from PE in the European Union, with similar numbers reported in the USA. In the past, management of acute PE has been characterised by a high degree of complexity and a disappointing lack of efficacy and efficiency. Complex multistep diagnostic algorithms were successfully tested in management studies, but proved extremely difficult to implement correctly in clinical practice. As a result, the diagnosis of PE was frequently missed in patients who subsequently died of the disease without receiving appropriate treatment, while others unnecessarily underwent hazardous, time consuming and costly procedures because of a vague, poorly documented clinical suspicion. With regard to PE treatment, a more than 30-year-old debate and the lack of adequate data on the appropriate indications for thrombolysis have deprived some patients of potentially life saving treatment, while exposing others to the high bleeding risk of thrombolytic drugs.
Thanks to the technical advances in diagnostic modalities and the findings of recent well designed outcome studies, things are now beginning to look better for patients with PE and for the physicians caring for them. While the revised and updated guidelines of the European Society of Cardiology on the diagnosis and treatment of PE are expected to appear later this year, this review will summarise the relevant current and evolving concepts which already have begun to simplify the management of acute PE while, at the same time, increasing its efficacy and safety.
DIAGNOSTIC STRATEGIES AND ALGORITHMS
At present, there is only one clinical factor which unequivocally determines the diagnostic and therapeutic approach to a patient with suspected acute PE: the presence or absence of haemodynamic instability at presentation. Acute right ventricular (RV) dysfunction resulting from pressure overload results in increased myocardial oxygen demand, myocardial ischaemia and infarction, left ventricular preload reduction, and ultimately inability to maintain the cardiac index and arterial pressure. A clinically massive PE indicates overt RV failure which results in refractory arterial hypotension and shock (commonly defined as systolic blood pressure <90 mm Hg, or a pressure drop ⩾40 mm Hg for at least 15 min). This condition accounts for almost 5% of all cases of acute PE and is associated with a high risk of in-hospital death, particularly during the first few hours after admission. On the other hand, the prognosis for normotensive patients with non-massive PE is considered favourable, provided that the disease is diagnosed correctly and anticoagulation can be instituted without delay.
Approach to the haemodynamically unstable patient with suspected massive pulmonary embolism
As emphasised above, clinically massive PE is a life threatening situation with an extremely poor prognosis. Management of the unstable patient with suspected massive PE should focus on the rapid institution of treatment rather than absolute diagnostic certainty per se. In such an emergency situation, diagnostic algorithms rely mostly on the individual physician’s experience and clinical judgement, rather than on a solid body of evidence and the results of prospective management studies.
In all patients with suspected PE, the clinical probability, or pre-test likelihood, of the disease can be empirically (“implicitly”) classified by the clinician as low, intermediate or high, or it may be semiquantitatively (“explicitly”) calculated on the basis of symptoms, signs and predisposing factors included in validated scores such as those presented in table 1.1 2
Beyond clinical assessment, there is no rationale for performing a D-dimer test in a patient who is hypotensive or in shock.
According to the algorithm proposed in fig 1, a bedside echocardiogram should be performed immediately, since it is the fastest and thus most appropriate initial test for confirming the presence of acute RV failure. The echocardiographic criteria and parameters which have been applied to detect RV pressure overload and dysfunction in previous studies are presented in table 2 and their usefulness and limitations discussed in the third section of this review. Additional valuable information which can be obtained from ultrasound imaging includes the presence of large floating intracardiac thrombi, which indicate an imminent threat of recurrent massive PE and should prompt emergency surgical embolectomy or, alternatively, thrombolysis, if surgery is not immediately available. In addition, patients with clinically massive PE who present with refractory hypoxaemia and/or neurologic abnormalities may have right-to-left shunt or paradoxical thromboembolism through a patent foramen ovale, which can promptly be detected by echocardiography following echo contrast injection. Moreover, and importantly, echocardiography may provide alternative explanations for the patient’s hypotension and shock such as left ventricular failure due to cardiomyopathy or large myocardial infarction, critical valvular disease, pericardial tamponade, or aortic dissection.
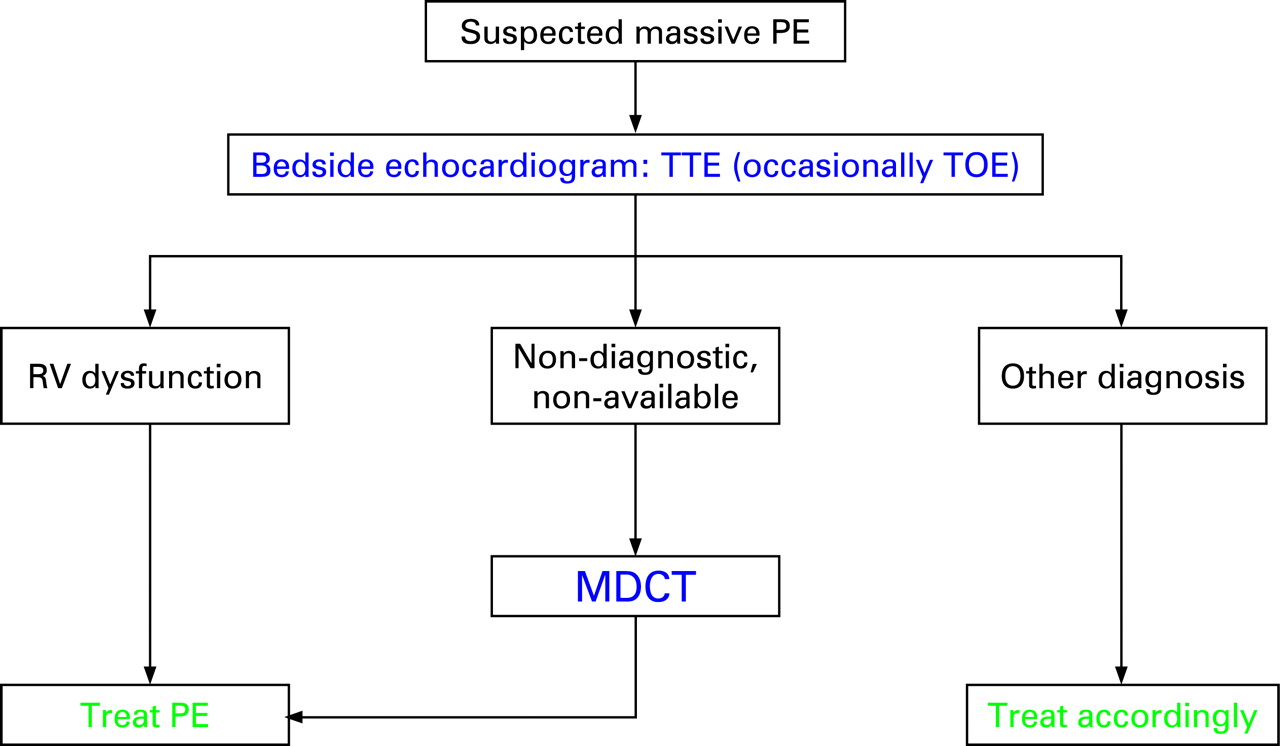
In mechanically ventilated patients, transoesophageal echocardiography is a useful alternative to transthoracic imaging, permitting not only assessment of cardiac function but also direct visualisation of possible thrombi in the right atrium, foramen ovale, right ventricle, or the proximal segments of the common and right pulmonary artery.
If bedside echocardiography is not available on an emergency basis or its findings are non-diagnostic, spiral computed tomography (CT) is the next fastest and most reliable diagnostic and differential diagnostic method (fig 1). Selective invasive pulmonary angiography is rarely necessary, unless the patient is already in the catheterisation laboratory because of suspected myocardial infarction and/or catheter based aspiration of the pulmonary thrombus is a treatment option in the particular institution.
Established and evolving diagnostic algorithms in the normotensive patient with suspected pulmonary embolism
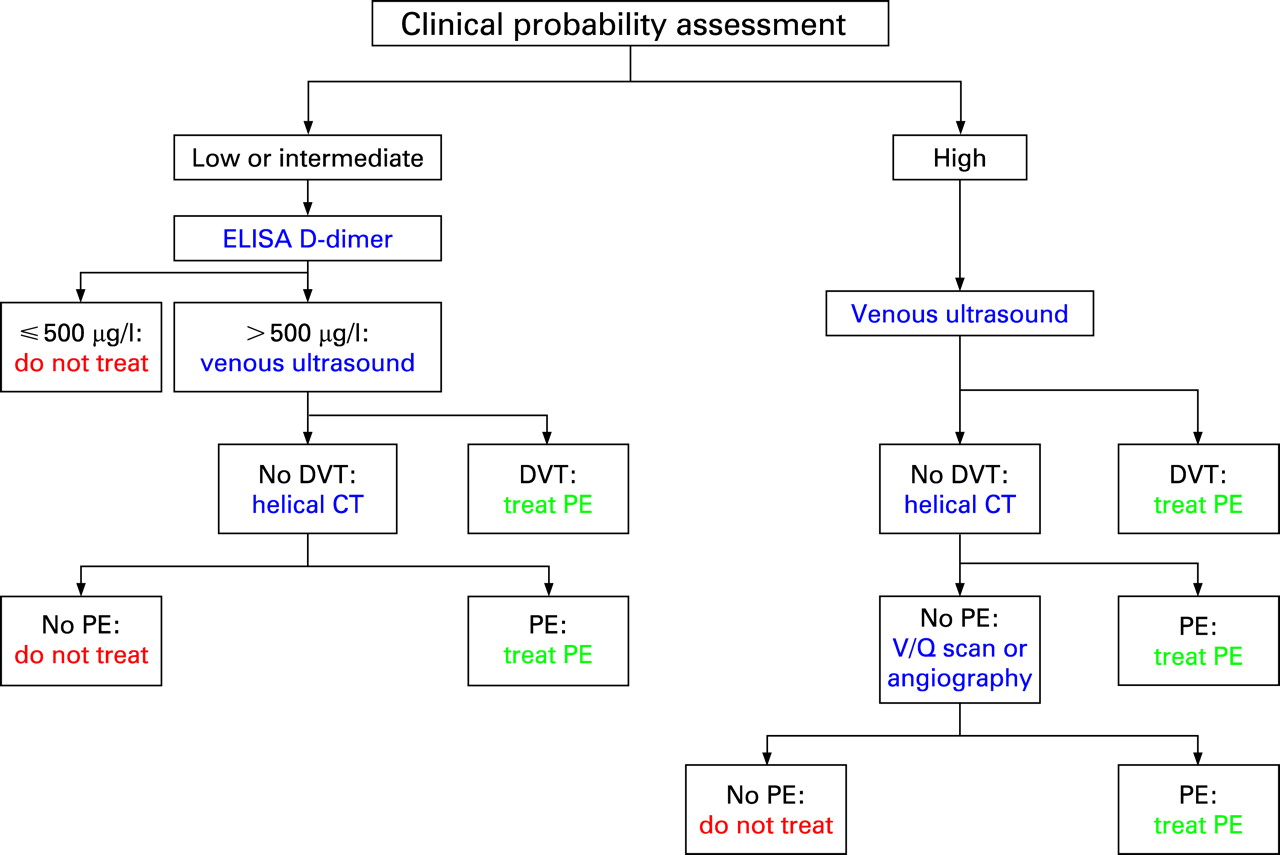
Over the past 10 years, numerous algorithms have been proposed and prospectively validated for the diagnostic workup of normotensive patients with suspected non-massive PE. The diagnostic algorithm presented in fig 2 is based on spiral (or helical) CT, since this is the imaging modality currently used in the majority of European institutions. The steps followed in the algorithm are very similar if ventilation–perfusion lung scan is used instead of spiral CT.3

As discussed above, the clinical (pre-test) probability of acute PE may be implicitly classified by the clinician as low, intermediate or high, or it may be calculated on the basis of explicit validated scores such as those presented in table 1. Measurement of D-dimer values as the second step will permit PE to be ruled out without further testing in around 30% of patients in the emergency department. Importantly, D-dimer values are negative in only 10% of patients with a high clinical probability who, in turn, represent only 10% of all patients with suspected PE. Thus, as the absolute number of patients with the high probability–negative D-dimer test combination is very low, D-dimer assays are not reliable and thus not recommended in patients with a high clinical probability for PE. On the other hand, a negative D-dimer test has been established as a reliable rule-out criterion in patients with low or moderate clinical probability for PE when using a highly sensitive (ELISA) D-dimer assay, and in patients with a low clinical probability when using a less sensitive semiquantitative assay.
Lower limb venous compression ultrasonography is the following step in patients with an elevated D-dimer level and in those with a high clinical probability for PE (fig 2). It will detect deep venous thrombosis in about 10% of the patients and can thus help establish a definite diagnosis in approximately 15% of the entire initial cohort. Accordingly, a CT scan or ventilation–perfusion lung scan ultimately needs to be performed in only 50–60% of all patients with suspected PE.
Single detector (first generation) CT scan has, by itself, a relatively low diagnostic sensitivity of 60–70%, but the combination of a negative CT, a negative lower limb ultrasound and a low or intermediate clinical probability can safely rule out PE as shown by outcome studies. In hospitals in which ventilation–perfusion lung scan is the preferred imaging modality, the combination of a low probability scan and a low clinical probability of PE can be used to safely exclude PE. At the other end of the spectrum, a high probability ventilation–perfusion scan generally establishes the diagnosis of PE, although further tests may be necessary in patients with low clinical probability due to the low positive predictive value of the lung scan in this setting. In all other combinations of lung scan findings and clinical probability, further tests such as spiral CT or even selective pulmonary angiography are necessary.
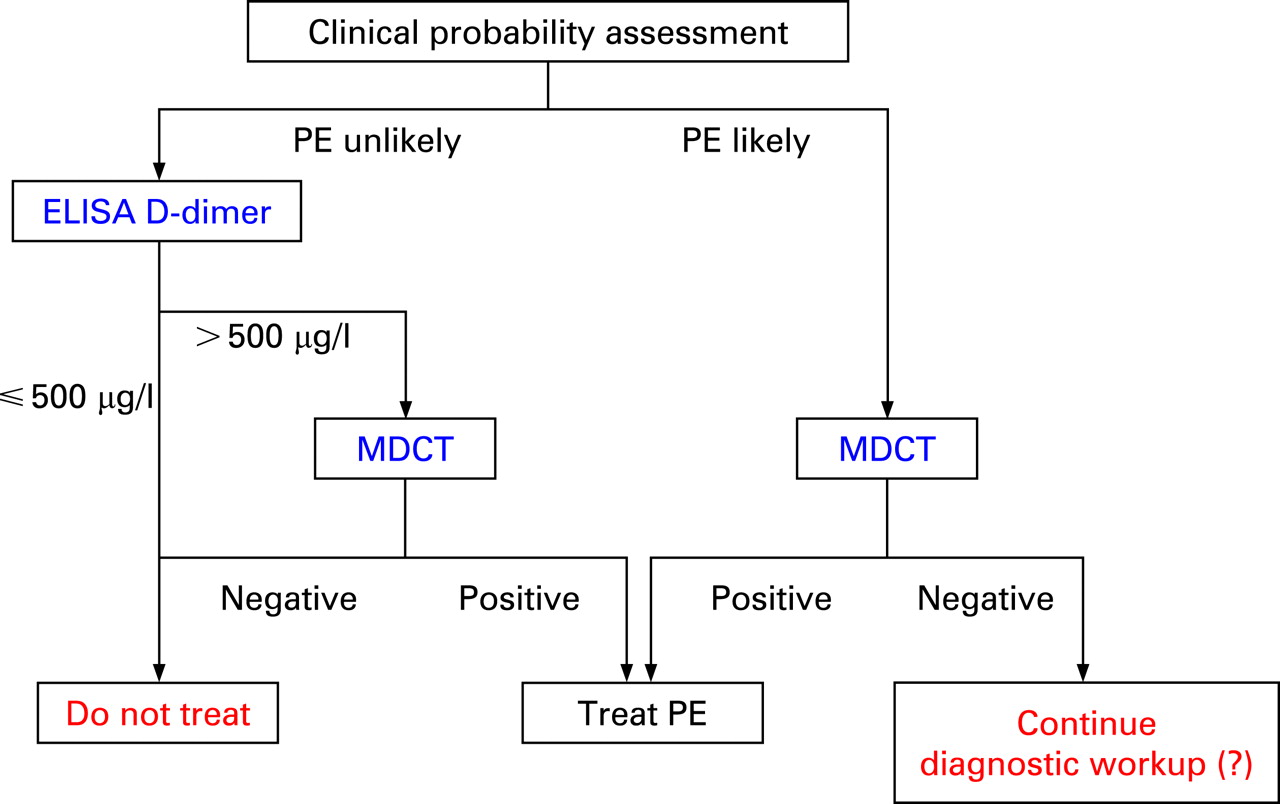
More recent algorithms, such as the one shown in fig 3, are based on the high sensitivity of multidetector row CT (MDCT)4 and its ability to confirm or exclude PE without the need for venous ultrasound as an intermediate step. In a recent management trial, patients in whom PE was considered unlikely based on the dichotomised Wells score (table 1) and in whom D-dimer was negative were left untreated and had only a 0.5% risk of 3 month thromboembolism recurrence. Similarly, if PE was ruled out by CT scan (without further imaging tests), the 3 month thromboembolic risk was 1.3%.5 The simplified diagnostic algorithm shown in fig 3 is also supported by a quasi-outcome study which did perform venous ultrasound but found that the overall 3 month risk of thromboembolism in patients left untreated (without anticoagulation) would have been only 1.5% if D-dimer and MDCT had been the only tests to rule out PE.6

Recently, false negative results with MDCT were reported in patients with a high clinical probability of PE.4 This is, however, a rare combination in clinical practice, and its implications regarding the need for further testing to exclude PE remain controversial in light of the reassuring results of management trials.5 Overall, the algorithm presented in fig 3 is already considered reliable enough to be recommended in future guidelines.
SEVERITY ADJUSTED THERAPEUTIC CONCEPTS
Urgent pulmonary recanalisation (thrombolysis or surgery) for high risk patients with haemodynamic instability
In view of the very high mortality and complication risk associated with clinically massive PE, experts and current guidelines7–9 agree that patients who present with persistent arterial hypotension or shock are in need of immediate recanalisation of the occluded pulmonary arteries using thrombolytic agents or, alternatively, surgical/interventional procedures. In fact, although only one very small randomised trial specifically addressed the prognostic benefits of thrombolysis in clinically massive PE, pooled data from five trials which included haemodynamically unstable patients appear to suggest a significant reduction of death or PE recurrence after thrombolysis in this high risk group.10
Benefits, response rates, and risks of thrombolysis in acute high risk pulmonary embolism
A number of randomised trials performed since the early 1970s have confirmed that thrombolytic treatment of PE rapidly resolves thromboembolic obstruction and exerts beneficial effects on haemodynamic parameters. One of the largest thrombolysis trials also demonstrated a significant improvement in RV function (assessed by echocardiography; see below) 3 h after treatment with recombinant tissue plasminogen activator (rtPA).11 Overall, as many as 92% of patients receiving thrombolysis for PE appear to respond favourably to this type of treatment as indicated by the clinical and echocardiographic improvement within the first 36 h.12 The greatest benefit is observed when treatment is initiated within 48 h of symptom onset, but thrombolysis can still be useful in patients who have had symptoms for 6–14 days. Importantly, however, the haemodynamic benefits of thrombolysis over heparin appear to be confined to the first few days. Follow-up studies showed that, 1 week after treatment, the improvement in the severity of vascular obstruction and the reversal of RV dysfunction no longer differs between thrombolysis treated and heparin treated patients. These data further support the notion that thrombolysis should be reserved for those patients in whom a high risk of early PE related death is anticipated.
Data derived from all thrombolysis trials in acute PE reveal a 13% cumulative rate of major bleeding and a 1.8% rate of intracranial/fatal haemorrhage. However, the results of the most recent of these studies suggest that the risk of major or life threatening bleeding may be lower if non-invasive imaging methods are used to diagnose PE (as opposed to the dominant role of selective pulmonary angiography in the 1970s, ’80s and early ’90s).11 13 This is an encouraging observation in light of the technical advances in CT pulmonary angiography which has become the gold standard in PE diagnosis.
Currently approved thrombolytic regimens for PE include: (1) streptokinase, 250 000 IU as a loading dose over 30 min, followed by an infusion of 100 000 IU/h over 12–24 h; (2) urokinase, 4400 IU/kg as a loading dose over 10 min, followed by 4400 IU/kg/h over 12–24 h; and (3) alteplase (rtPA), 100 mg infusion over 2 h. Alteplase is generally considered to be the most effective thrombolytic agent, but the small differences found in comparative trials were mostly due to the shorter administration period of this drug. An even shorter (over 15 min) infusion regimen of alteplase at the dosage of 0.6 mg/kg (maximum dosage 50 mg) can be used in emergency situations—for example, during cardiopulmonary resuscitation. Satisfactory haemodynamic results also have been obtained with double bolus reteplase, two injections (10 U) 30 min apart, although this drug is not officially approved for PE. Finally, preliminary uncontrolled data appear to support the efficacy and safety of tenecteplase in acute PE.
Surgical pulmonary embolectomy remained a rarely performed rescue operation over several decades, and limited data existed regarding its efficacy and safety. Recently, however, it was reported that technical advances in transportable extracorporeal assist systems, and particularly the timely involvement of the cardiac surgeon as part of an interdisciplinary approach to high risk PE, may be associated with better postoperative outcomes.14 Currently, pulmonary embolectomy is a recommended therapeutic option in patients with high risk PE in whom there are absolute contraindications to thrombolysis, or if thrombolysis has failed. The same recommendations and restrictions apply to interventional (catheter) embolectomy or fragmentation of proximal pulmonary arterial clots.
Inferior vena cava filters may be used when there are absolute contraindications to anticoagulation and a high risk of PE recurrence including, for example, the period immediately following neurosurgery or other major surgery. They may also be considered in pregnant women who develop extensive thrombosis in the weeks before delivery. On the other hand, routine use of (either retrievable or permanent) venous filters is not recommended in the general population with PE. There are no data from prospective randomised trials to indicate the optimal duration of venous filter use, but it is generally agreed that retrievable filters should be removed as soon as it is safe to use anticoagulants.
Heparin anticoagulation for normotensive patients with non-massive pulmonary embolism
In view of early data showing high recurrence and mortality rates in patients with acute PE as long as they remain untreated, current guidelines recommend the early initiation of anticoagulant treatment in all patients with clinically suspected PE—that is, during (and not after completion of) diagnostic workup. If intravenous unfractionated heparin is given, a weight adjusted bolus injection of 80 U/kg is followed by an infusion rate of 18 U/kg/h. Subsequent infusion rates should be adjusted using activated partial thromboplastin time (aPTT) based nomograms in order to achieve and maintain therapeutic aPTT prolongation (between 1.5–2.5 times control).15 The aPTT should be measured 4–6 h after the bolus injection, and subsequently 3 h after each dose adjustment, or once daily when the target therapeutic dose has been achieved.
Intravenous unfractionated heparin is still the preferred mode of initial anticoagulation for patients with severe renal impairment (creatinine clearance <30 ml/min), as it is not eliminated by the kidneys; for those at high risk of bleeding, as its anticoagulant effects can be rapidly reversed; and, usually, for extremely overweight, underweight, or old patients. In all other cases, unfractionated heparin has been replaced by low molecular weight heparin (LMWH) given subcutaneously at weight adjusted doses. A meta-analysis of 12 trials confirmed that LMWHs are at least as efficacious (regarding the rates of recurrent venous thromboembolism) and at least as safe (regarding major bleeding) as unfractionated heparin.16 Routine anticoagulation monitoring—that is, measurement of anti-factor Xa values—is not necessary in patients receiving LMWH, but it should be considered in patients with severe renal failure as well as during pregnancy. In these cases, anti-Xa values should be determined 4 h after the morning injection; the proposed target range is 0.6–1.0 IU/ml for twice daily administration and 1.0–2.0 IU/ml for once daily administration.
Currently approved LMWHs include: (1) enoxaparin at the dose of 1 mg/kg every 12 h (1.5 mg/kg once daily is also an approved regimen in some countries); (2) tinzaparin, 175 U/kg once daily; and (3) the pentasaccharide fondaparinux at doses of 5 mg (for body weight <50 kg), 7.5 mg (body weight 50–100 kg), or 10 mg (body weight >100 kg), once daily. Because of the risk of heparin induced thrombocytopenia, monitoring of the platelet count is mandatory during treatment with unfractionated heparin or LMWH.
Of note, LMWHs are not recommended for high risk patients with clinically massive PE, as such patients were excluded from randomised trials comparing their efficacy and safety to that of unfractionated heparin in acute PE.
Long term secondary prophylaxis of pulmonary embolism
Anticoagulation with unfractionated heparin or LMWH should be continued for at least 5 days. Oral anticoagulants (vitamin K antagonists) should be initiated as soon as possible in all haemodynamically stable patients, preferably on the same day as heparin. Parenteral anticoagulation can be stopped when the international normalised ratio (INR) lies between 2.0–3.0 for at least 2 consecutive days.
A detailed discussion of the recommended duration of oral anticoagulation after an episode of acute PE has been reviewed in recent guidelines9 and is beyond the scope of the present article. As a rule, treatment with vitamin K antagonists should be continued for 3 months after a first episode of PE triggered by a transient risk factor (for example, trauma, surgery, immobilisation, contraceptive use or hormonal replacement therapy), and for longer periods (preferably 6–12 months) for patients with unprovoked PE. As the risk of PE recurrence remains high beyond the first year following the initial episode, indefinite oral anticoagulation should be considered for patients with a first manifestation of unprovoked PE and a low risk of bleeding, and it is clearly recommended for most patients with a second unprovoked episode of venous thromboembolism. Patients with high risk thrombophilia or active cancer are also candidates for long term oral anticoagulation.
Novel, vitamin K independent oral anticoagulants are currently under investigation for primary and secondary prophylaxis of venous thromboembolism. In particular, the selective oral thrombin inhibitor dabigatran and the oral factor Xa inhibitors rivaroxaban and apixaban have already yielded promising data. If eventually approved, these drugs will hopefully increase the safety and efficacy of chronic oral anticoagulation.
IS THERE A NEED FOR RISK STRATIFICATION OF NORMOTENSIVE PATIENTS WITH NON-MASSIVE PULMONARY EMBOLISM?
As mentioned above, the presence and severity of RV dysfunction is a major determinant of the clinical course of acute PE. Several years ago, registry data generated the hypothesis that the detection of subclinical RV dysfunction in a normotensive patient with acute non-massive PE may help define an elevated, intermediate mortality risk in the acute phase. It was further postulated that these patients may benefit from early thrombolytic treatment. This is currently a topic of intensive research, and table 2 summarises the methods and parameters which have been proposed for risk stratification of normotensive patients with acute PE.
Echocardiography is capable of visualising the changes occurring in the morphology and function of the right ventricle as a result of acute pressure overload. A number of parameters, including those listed in table 2, permit the non-invasive diagnosis of RV dysfunction at the bedside. Several registries and cohort studies could demonstrate an association between these parameters and a poor in-hospital outcome in terms of PE related death and complications.17 18 Nevertheless, the prognostic value and potential implications of cardiac ultrasound in normotensive patients with PE have not been unequivocally demonstrated. Indeed, the largest randomised thrombolysis trial to date, which included 256 normotensive patients with RV dysfunction on echocardiography, did not find a significant influence of the type of treatment on mortality rate during the acute phase of PE.13 Apart from the lack of standardisation of the echocardiographic criteria, transthoracic imaging may yield inconclusive findings in some individuals, and the echocardiographic distinction between acute RV dysfunction due to PE and chronic cor pulmonale can be particularly difficult in clinical practice.
Four chamber views of the heart on MDCT may detect RV enlargement due to PE and thus possibly predict early death. In a large retrospective series of 431 patients, 30 day mortality was twice as high in patients with RV enlargement, defined as right/left ventricular (LV) dimension ratio >0.9, compared to those without this finding (15.6% vs 7.7%).19 Another retrospective study evaluated the prognostic value of a predefined diameter ratio of 1.0 (axial four chamber views without post-processing of the CT images) during a 3 month follow-up.20 The negative predictive value of a small right ventricle reached 100%, whereas the positive predictive value of an RV/LV ratio >1.0 for PE related mortality was rather low (10.1%). Clearly, several limitations of the method (shown in table 2) still exist, and a number of issues need to be resolved before MDCT can replace echocardiography for diagnosing RV dysfunction. This would be very practical, since this imaging technique has already evolved into the gold standard in the diagnostic workup of patients with suspected PE (figs 1 and 2). At present, however, it appears unlikely that risk stratification of PE can be based on CT parameters alone.
Biomarkers
Elevated cardiac troponin I or T concentrations, which are a sensitive indicator of myocardial cell damage and microscopic myocardial necrosis, are found in 11–50% of patients with acute PE. A large number of studies, which were recently included in a meta-analysis,21 showed that cardiac troponin elevation correlates with the presence of RV dysfunction on echocardiography and possesses a high (97–100%) negative predictive value with regard to death or complication risk in the acute phase. Thus, normal troponin values may rule out an adverse outcome in patients with PE. However, the positive predictive value of these biomarkers is probably low. Consequently, troponin elevation alone is not sufficient to predict early death or complications in patients with acute PE, and it is unlikely that it could, by itself, identify intermediate risk patients as potential candidates for thrombolytic treatment. Moreover, troponin values may still be undetectable on admission and thus not suitable for assessment of prognosis and guidance of early therapeutic decisions (table 2).
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit = men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal’s username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Natriuretic peptides are released as a result of cardiomyocyte stretch and are very sensitive indicators of neurohormonal activation due to ventricular dysfunction. In general, both brain natriuretic peptide (BNP) and N-terminal proBNP (NT-proBNP) are characterised by extreme prognostic sensitivity and a negative prognostic value which is probably even higher than that of the cardiac troponins. On the other hand, they exhibit a very low specificity and positive prognostic value in the range of 12–25%. Furthermore, appropriate cut-off values for distinguishing between a “positive” and a “negative” BNP or NT-proBNP test have not yet been prospectively validated (table 2).
Heart-type fatty acid binding protein (H-FABP) is a small cytoplasmatic protein which is abundant in the heart. Following myocardial cell damage, it diffuses rapidly through the interstitial space and appears in the circulation as early as 90 min after symptom onset, reaching its peak within 6 h. Recent data suggest that it may provide prognostic information superior to that of cardiac troponins in acute PE.
CONCLUSIONS AND OUTLOOK
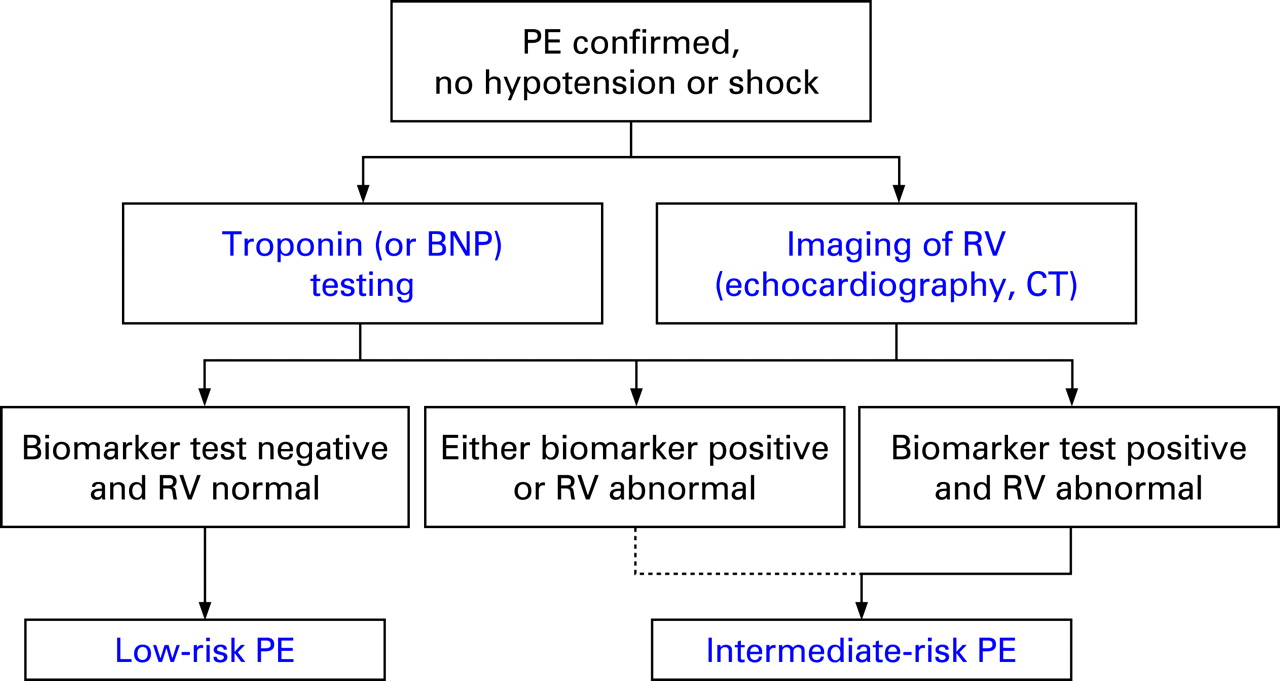
Although the diagnostic approach to patients with suspected acute PE has made significant progress in the past years, the indications for thrombolytic treatment beyond the setting of clinically massive PE, and the need for risk stratification of normotensive patients, remain controversial. Due to the numerous limitations explained above, it is unlikely that imaging methods or cardiac biomarkers alone will prove sufficient for guiding therapeutic decisions, particularly with regard to early thrombolysis versus heparin alone in normotensive patients with acute non-massive PE. At present, the existing evidence appears to support the use of risk assessment algorithms (such as the one proposed in fig 4), which combine the information provided by an imaging procedure (echocardiogram or CT) and a biomarker test, preferably troponin I or T. The therapeutic implications of such an algorithm are currently being evaluated in a large multinational trial which was recently initiated and plans to randomise more than 1000 normotensive patients with acute PE, RV dysfunction on echocardiography or CT, and a positive troponin test. It is expected that this large European study will be able to resolve the longstanding debate on the existence of an intermediate risk group of patients with PE (formerly termed submassive PE) which may benefit from early thrombolytic treatment. At the same time, novel biomarkers and combined risk assessment strategies continue to be evaluated in cohort studies.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
REFERENCES
- 1.↵
- 2.↵
- 3.↵
A comprehensive up-to-date review of validated diagnostic strategies for the diagnosis of pulmonary embolism.
- 4.↵
This landmark study helped establish MDCT as the contemporary diagnostic standard for acute PE, while also revealing the weaknesses (false-positive and false-negative results) of the method when the findings are discordant with clinical (pre-test) probability.
- 5.↵
An important management study which demonstrated that withholding anticoagulation therapy is safe in patients in whom MDCT excludes pulmonary embolism.
- 6.↵
- 7.↵
- 8.
These guidelines still reflect the state of the art in the management of acute PE. The updated guidelines of the European Society of Cardiology are expected later this year.
- 9.↵
- 10.↵
This meta-analysis provides further support for the life saving role of thrombolysis in clinically massive PE with arterial hypotension and shock.
- 11.↵
- 12.↵
- 13.↵
- 14.↵
A relatively large series which supports the integration of emergency surgical embolectomy into the management of acute massive PE.
- 15.↵
- 16.↵
- 17.↵
The data derived from a large registry confirm the prognostic role of echocardiography in normotensive patients with acute PE. They support the existence of an “intermediate risk” group.
- 18.↵
- 19.↵
- 20.↵
- 21.↵
This meta-analysis demonstrated the prognostic value of elevated troponins in acute PE although it did not address the possible therapeutic implications of a positive troponin test.
Footnotes
Competing interests: In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. The author has no competing interests.