Article Text

Statistics from Altmetric.com
There is a long history of disease caused by inhaled particles that stretches from Agricola and Paracelsus in the 14th century up to the present.1 In this century the twin scourges of asbestos and crystalline silica (quartz) have exerted a terrible toll of death and disease. The bad old days when these dust related lung diseases were unbridled are gone but as we enter the 21st century a new particle type—the ultrafine particle—has emerged as one with a potential role in causing disease. Ultrafine particles have been the subject of several recent reviews.2 3
Ultrafine particles
Particles that are less than 100 nm in diameter are commonly defined as ultrafine. However, all particle populations that are found in the air are polydispersed—that is, they comprise particles with ranges of diameters that are usually summarised as mean or median diameter. There is no reason at the moment to think that there is much difference between a 90 nm and a 110 nm particle in ability to have an adverse effect and there is little evidence for the cut off point for the ultrafine effect. Ultrafine particles are very small compared with the cellular structures and so this may be important in the apparent problems they present to the lung (fig 1).

Relation between ultrafine particles and cellular structures in the lung. Idealised particles of 10, 1, and 0.1 μm are shown compared with a bronchial epithelium; note that the top end of the range of ultrafine particles (0.1 μm, 100 nm) is not really visible. On the right are shown the same three particles relative to cilia.
Particles of diesel exhaust may be taken as an example of an ultrafine particle, albeit complex. They are largely insoluble because of the particulate carbon core, commonly the size of singlet diesel particles, 10–20 nm. However, they tend to group into aggregates with sulphates, metals, and hydrocarbons.4 Particles of diesel soot are ubiquitous in urban air and contribute to particulate air pollution of aerodynamic diameter 10 μm (PM10). However, ultrafine particles in urban air could come from a range of sources other than diesel soot. For experimental purposes toxicologists have used several standard ultrafine particles such as titanium dioxide and carbon black for their studies.5
Importance of ultrafine particles
Ultrafine particles occur as components of urban environmental particulate air pollution. Environmental particulate air pollution is measured by a global sampling convention called PM10 that measures the mass of particles collected with a 50% efficiency for particles with an aerodynamic diameter of 10 μm6; all particles down to the ultrafine size range are collected. This closely corresponds to the International Standards Organisation thoracic convention—that is, the mass fraction of inhaled particles that penetrates beyond the larynx to the airways. The respirable fraction, which penetrates to the unciliated regions of the lung, is approximated by an analogous PM2.5 convention, which is now being considered in the United States as the standard.
Ultrafine particles are found to a large extent in urban air as both singlet and aggregated particles (fig 2), and indeed are the predominant particle size by number in urban PM10, although they contribute modestly to mass.6

High power transmission electron microscopic image of a PM10 particle collected on a filter from Glasgow city centre. The image shows an aggregate that comprises chains and clumps of ultrafine particles in which singlet particles that comprise the clumps can be readily identified (arrows). Aggregates such as these are extremely common in the sample and in urban air in general. Image courtesy of Martin Wilson.
Ultrafine particles are generally made from combustion processes in which growth of the particle is from molecules upwards and so these particles can be extremely small, much smaller than the problem particles in dusty trades that have been studied up until now (fig3).4 Ultrafine particles also have important industrial applications—for example, as ultrafine carbon black—and so there is potential for occupational exposure. However, the extent of the risk to workers has not yet been assessed.
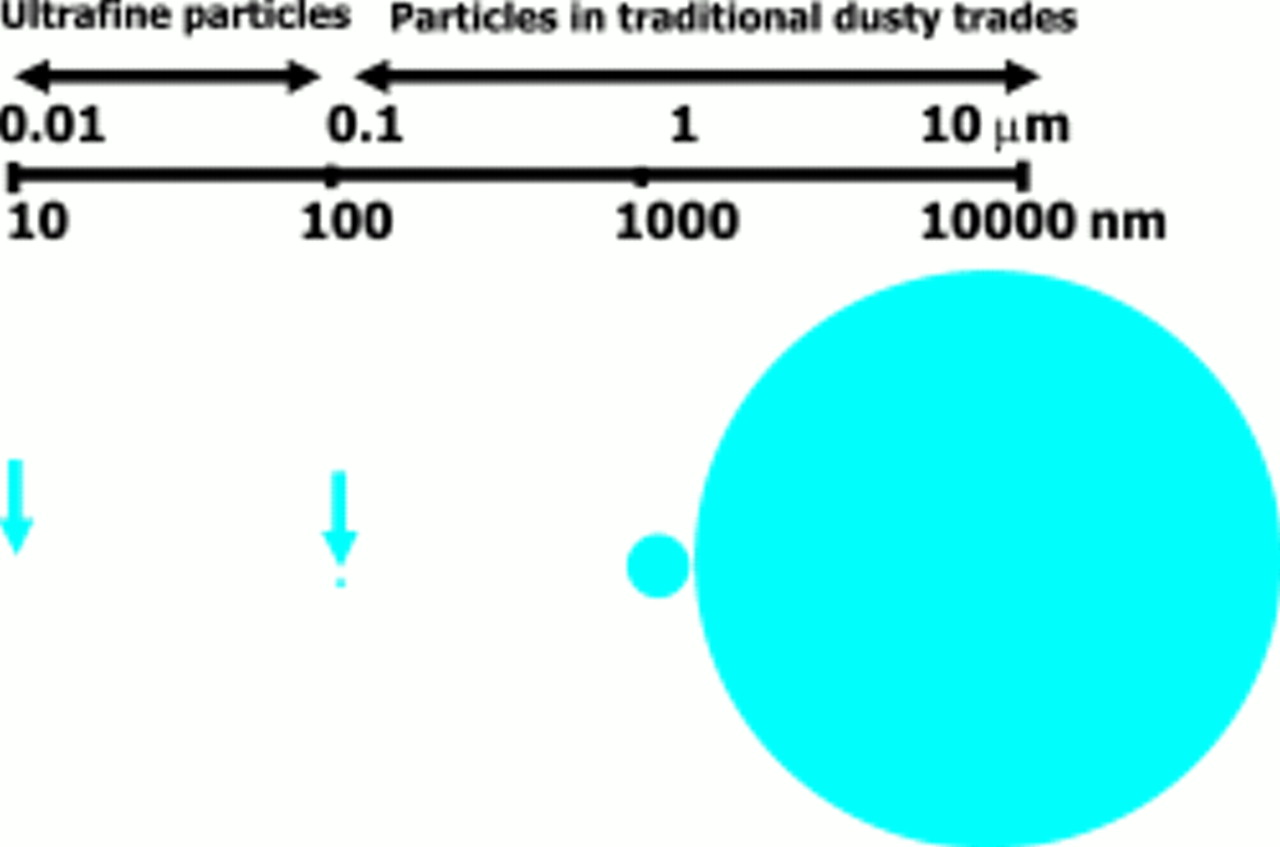
Relative size of ultrafine particles compared with particles in traditional dusty trades.
Increases in PM10 pollution have been found to be associated with a range of adverse health effects and these are very well documented (box 1).7 The components of PM10 are not on the whole very toxic, comprising in large part sulphates, nitrates, chlorides, ammonium, carbonaceous material, metals, and wind blown crustal dust.6 Therefore attention has turned to the components that are most likely to have toxic potential, and the ultrafine particles have been identified as potential mediators of some of the toxicity of PM10, largely on the basis of toxicological findings plus some epidemiological data that are summarised in box 1. The other components of PM10 that are most likely to mediate adverse health effects are the transition metals and endotoxin.
Box 1: Components of PM10
PM10 is a complex mixture of airborne particles including salts, metals, ultrafine particles, and biological material. Among the well documented adverse health effects associated with increases in PM10 are:
- ▸
- Increased use of medication for asthma
- ▸
- Attacks of asthma in patients with pre-existing asthma
- ▸
- Attacks of chronic obstructive pulmonary disease (COPD)
- ▸
- Admission to hospital for cardiovascular causes
- ▸
- Deaths form heart attacks
- ▸
- Deaths from strokes
- ▸
- Deaths from respiratory causes
Susceptibility to PM10
It is notable that the acute adverse health effects of PM10 are found in susceptible subgroups and not, on the whole, in normal healthy people except at very high concentrations.7 This may help to explain the rather puzzling statement already made that the components of PM10are not, by and large, very toxic. The lungs of susceptible people may be in some way primed—for example, by the presence of inflammation—to hyperrespond in a way that normal lungs do not. Therefore, if the effects of PM10 are mediated to some extent by ultrafine particles then the lungs of patients with asthma, COPD, and cardiovascular disease must have some “factor of susceptibility” that normal people do not have and which leads to a greater response to ultrafine particles—for example, pre-existing inflammation in their lungs. This has an important bearing on toxicological studies and on studies of mechanism: the very low concentrations to which people are exposed may have no effect in toxicological test systems that use normal animals and cells but effects may become evident in animal and cellular models of susceptibility.
It is likely of course that there are also chronic effects of exposure to PM10,8 which may affect normal people, but these are difficult to study. It is important to point out that concentrations of ultrafine particles were not measured in these studies and so a role for them remains hypothetical. In the case of occupational exposure to ultrafine particles, where the exposure would be anticipated to be greater than the environmental exposure, adverse effects on normal people might be anticipated.
Ultrafine particles and the lungs
DEPOSITION OF ULTRAFINE PARTICLES
Ultrafine particles may exist as singlet particles or as aggregates. In the form of aggregates their deposition characteristics can change as the aggregates will have a greater aerodynamic diameter than the singlet particles. The aerodynamic characteristics of the aggregates will, however, vary depending on their compactness. If the aggregate is more open with chains and extensions then, like thistledown, it will have greater aerodynamic resistance, less likelihood of settling, and hence a smaller aerodynamic diameter. For singlet particles there is good evidence that particles with aerodynamic diameter down to 10 nm deposit readily in the airways and centriacinar regions of the lung9 and that pathological changes in the lungs such as the airway narrowing found in COPD and asthma cause an increase in the efficiency of deposition of ultrafine particles.10 This may well be a factor that contributes to susceptibility in populations with airways disease. It is important to note, however, that there are no studies that show the sites of deposition of the various components of the urban aerosol.
Aggregates of ultrafine particles may disperse in the fluid of the epithelial lining so that the lung receives a dose of singlet particles. Alternatively the aggregates may persist, and so the lung has to deal with an irregular clump or chains. It is conceivable that the lung might respond differently to one or the other of these outcomes and more research on this is warranted.
EVIDENCE THAT ULTRAFINE PARTICLES ARE TOXIC TO THE LUNG
There is not a great deal of evidence describing the effects of ultrafine particles on people. The bulk of the evidence to support the contention that the ultrafine component of PM10 mediates some adverse health effects comes indirectly from studies with surrogate ultrafine particles in toxicological studies.
HUMAN STUDIES
Peters et al 11 reported that decrement in evening peak flow in a group of asthmatic patients was best associated with the ultrafine component of the airborne particles during an episode of severe air pollution. This showed the best association with the ultrafine fraction, although there were associations with fractions of other sizes.
ANIMAL STUDIES
The phenomenon of “overload” occurs in rats when they are exposed to high concentrations of airborne particles which accumulate in the lungs to a point where there is failure of clearance, increased build up of dose, inflammation, proliferation, fibrosis, and tumour production.12 Even low toxicity particles—such as carbon black and titanium dioxide—can cause this overload pathology in rats. Therefore sufficiently high exposure to a low toxicity particle that is non-pathogenic at plausible concentrations of human exposure, could cause a false positive pathological outcome in rats if given at high enough exposure to cause overload. The high volume of particles inside macrophages was thought to be the mechanism of this overload but recent work13 with two poorly soluble dusts with different specific surface areas has shown that the surface area is the measure that controls overload. This is especially relevant to ultrafine particles because at relatively low mass ultrafine particles have a high surface area. Why surface area is the most appropriate measure of dose is not understood but may be related to free radical activity and oxidative stress produced at particle surfaces as discussed later.
A given mass of ultrafine particles has a much greater surface area than the same mass of fine, yet respirable, particles (box 2) and so is more likely to cause overload. Thus, from a toxicological and regulatory viewpoint, it is important to separate the effects of ultrafine particles at overload from effects at non-overload, if they occur.
Overload of inhaled ultrafine particles
Ferin et al 14 showed that when rats were exposed to an equal airborne mass concentration of fine and ultrafine TiO2 particles, there was far more bronchoalveolar inflammation in the group with ultrafine exposure. Concomitantly these rats showed a notable increase in interstitial and lymph node transfer of the ultrafine compared with the fine particles. The airborne mass concentration of 23 mg/m3 was clearly an overload exposure and long term studies at high exposure have produced fibrosis and tumours with other ultrafine particles—such as diesel soot and carbon black.
Box 2: Surface area, particle number, and size
The table shows the physical characteristics of a cloud of particles with airborne mass concentration of 10 μg/m3 when it is composed of particles of various diameters. The number of particles per unit volume in the air increases dramatically along with the surface area per unit volume of air, as the particle size decreases.
Non-overload studies
To examine effects of ultrafine particles at low airborne mass concentration the authors have exposed rats to ultrafine carbon black (UfCB 14 nm primary particle size) and non-ultrafine carbon black (CB 260 nm mean primary particle size) at 1 mg/m3 for 7 hours. In the preliminary experiments there were no effects in the rats exposed to non-ultrafine carbon black but the ultrafine carbon black caused detectable proinflammatory effects—such as modest neutrophil influx, protein leak, and modulation of glutathione, a small molecular weight antioxidant. Systemic changes were also found with ultrafine carbon black. There was evidence of global oxidative stress in the plasma and increased plasma factor VII.15 This result is particularly interesting as increased factor VII is an independent risk factor for cardiovascular disease. In summary, these data show both a local inflammatory effect and a systemic effect of ultrafine particles at low doses. However, these interesting data need to be interpreted with caution when extrapolated back to the human exposure scenario.
Importance for exposure standards
Serita et al 16 exposed rats to metallic ultrafine nickel at around the Japanese occupational exposure level (OEL). This OEL was based on non-ultrafine particles, but exposure to concentrations around the OEL (1.4 mg/m3) in the form of ultrafine nickel caused severe lung injury after a single exposure. This finding supports the concept that surface area is the dose measure that predicts pulmonary response, rather than mass and this has far reaching potential consequences for occupational standards that are based on mass (box 3).
Box 3: Importance of the measure of dose
To give the best advice on how to manage risk from inhaled toxins we need to be able to accurately describe the hazard—that is, the intrinsic toxicity. Ideally this would then be the chosen measure of exposure. For example, in the case of an PM10 the following aspects could be the measure of exposure:
Physical measures:
- ▸
- Total airborne mass concentration (μg/m3)
- ▸
- Particle number concentration (millions of particles/m3)
- ▸
- Specific surface area (m2/m3)
Chemical measures:
- ▸
- Polycyclic aromatic hydrocarbon (PAH) concentration (μg/m3)
- ▸
- Sulphate concentration (μg/m3)
- ▸
- Others
The choice of which of these to use for risk management would depend on several factors that include:
- ▸
- How does PM10 exert its harmful effects on the lungs? (knowledge is incomplete)
- ▸
- How practical is it to carry out the measurement routinely? (For example, it is not presently possible to routinely measure surface area of airborne clouds)
- ▸
- What health end point is of interest? (there could be several).
It is important to note that the most important measure may be only a tiny part of the overall mixture. For instance, PAHs may be a very small portion of the overall mass but could have very important effects in causing cancer.
Mechanism of proinflammatory effects
EFFECTS OF ULTRAFINE PARTICLES ON PHAGOCYTOSIS
Phagocytosis by alveolar macrophages is important in the clearance of particles from the lungs. In a study in our own laboratory we have examined phagocytosis by a macrophage cell line (J774.2) exposed to ultrafine and fine samples of both titanium dioxide (TiO2) and carbon black (ultrafine diameter approximately ∼20 nm; fine diameter ∼200 nm). The cells were then exposed to 2 μm diameter indicator fluorescent latex beads and the uptake of these was used to judge phagocytic ability. Both ultrafine carbon black and ultrafine TiO2 had a deleterious effect on phagocytosis ofthe latex indicator beads compared with their fine counterparts. The effect was not apparently mediated by soluble mediators but by cell to cell contact.
From this study, and others showing effects of ultrafine particles on the ability of macrophages to phagocytose, it seems that the adverse effects of ultrafine particles may be mediated in part by their ability to inhibit phagocytosis. This may go towards explaining a previous findings that the threshold lung mass burden for overload, which has an important component related to failure of macrophage clearance, was much lower with ultrafine TiO2 than fine TiO2.
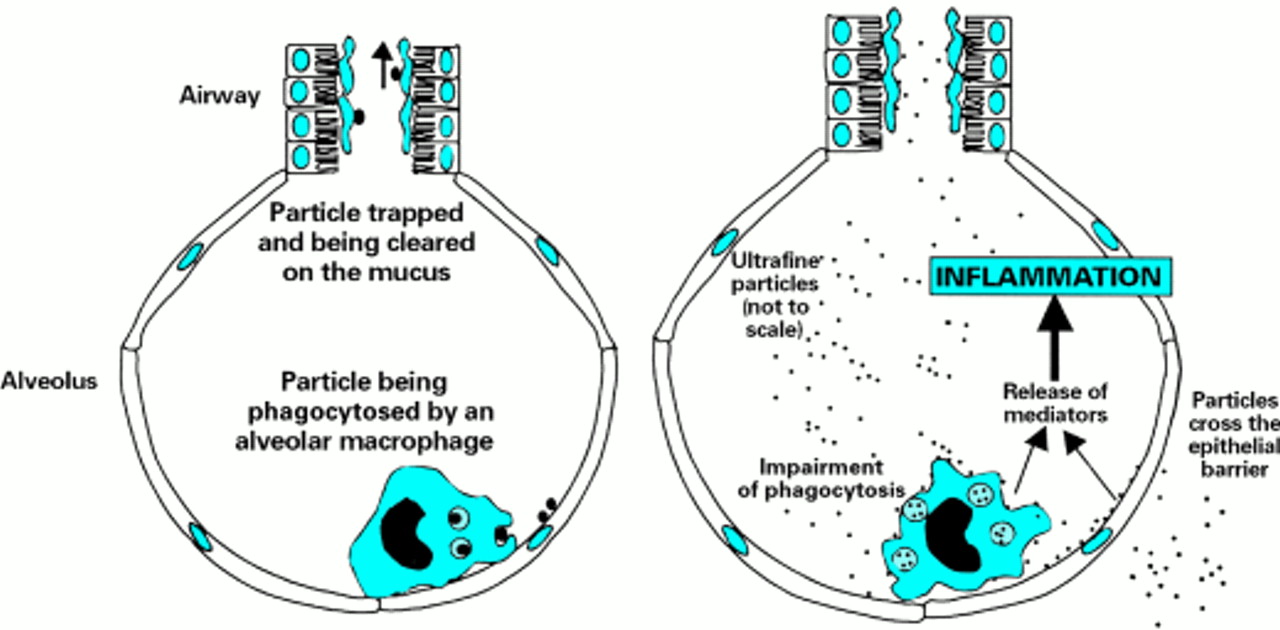
The mechanism for the effect on macrophages may be the increased oxidative stress from the large surface area of ultrafine particles.5 In human exposures to low masses of ambient ultrafine particles the impact that impairment of phagocytosis could have had is unknown. However, decreased phagocytosis could allow enhanced interaction between ultrafine particles and the epithelium which occurs in any case because of the sheer number of ultrafine particles. This leads to pro-inflammatory cytokine production by macrophages because of oxidative stress from the surface of the ultrafine particles and chemokine production by the epithelium (fig 4) through similar pathways. Increased interstitial transfer of particles may also arise because of interactions between particles and epithelial cells.13
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagrammatic representation of the hypothetical events after exposure to ultrafine particles (right) compared with fine particles (left). The essential elements of the ultrafine response are many particles outside and inside macrophages. Release of mediators from the macrophages and epithelial cells due to activation of signalling pathways mediated by oxidative stress, may then lead to inflammation. The enhanced interaction of particles with the epithelium leads to their transfer to the interstitium.
PROINFLAMMATORY EFFECTS AND THE ROLE OF OXIDATIVE STRESS AND CALCIUM
Using carbon black we have shown greater oxidative stress and proinflammatory effects of ultrafine particles than fine particles by instillation in rats.17 18 It is important to determine whether ultrafine particles have a role in PM10 toxicity beyond their ability to deliver transition metals, which are implicated in the proinflammatory effects and toxicity of PM10.19 We have excluded transition metals as a source of oxidative stress in the proinflammatory effects of ultrafine carbon black,19 but ultrafine carbon black does cause oxidative stress to cells in culture and in cell free systems. Further research on the mechanism of this oxidative stress is ongoing in our laboratory.
Further research from our laboratory has provided a possible explanation for the effects of ultrafine carbon black in promoting inflammation, which may be applicable to other ultrafine particles. Ultrafine carbon black has been shown to increase the resting cytosolic calcium concentration of a human monocytic cell line MonoMac 6 (MM6).20 This effect was not found with the same dose of larger, respirable carbon black particles. Further studies used thapsigargin, an agent that inhibits the endoplasmic reticulum Ca2+ATPase causing an increase in cytoplasmic Ca2+. These showed that ultrafine carbon black, but not carbon black, caused a 2.6-fold increase in the calcium current stimulated by thapsigargin.20 These results were repeatable with rat alveolar macrophages and could be prevented with antioxidants—highlighting the role of oxidative stress from the ultrafine particles. The amplification of a key second messenger system such as Ca2+ by ultrafine carbon black could underlie its proinflammatory effects and also could be an important synergising factor in susceptible people who already have increased Ca2+ concentrations because of other stimulatory molecules such as inflammatory cytokines. Thus the cellular events shown in figure 4—cytokine and chemokine gene transcription—can be seen as being driven by oxidative stress and calcium changes, both of which are known to have proinflammatory effects.20
Summary
Ultrafine particles are potential mediators of the well documented adverse health effects of PM10 pollution in ambient air, and could also pose a problem in occupational scenarios. They are extremely small compared with the cellular structures of the lungs and have a large surface area per unit mass compared with the classic toxic particles. They form aggregates but readily deposit in the lungs as singlets or aggregates and in the lungs the aggregates may disaggregate. There are only a few human studies that show that ultrafine particles are harmful and the weight of evidence comes from toxicological studies. The toxicological studies of surrogate particles—such as carbon black, show very clearly greater inflammatory effects of ultrafine than large particles of the same material. The mechanism remains unclear but the large surface area of the ultrafine particles seems to lead to oxidative stress, and calcium changes in macrophages and epithelial cells that could be important in priming and activating cells for inflammation. Research into ultrafine particles has had extensive ramifications and the potential importance of the surface area as a measure of dose has been highlighted for regulatory scenarios. There are more gaps in our knowledge about ultrafine particles than there are certainties and more research is needed on the part that ultrafine particles play in the adverse health effects of PM10, the mechanisms of toxicity of ultrafine particles to the lungs, and the potential for ultrafine particle exposure in the workplace.
Acknowledgments
We acknowledge the work of others who contributed to the current knowledge base on ultrafine particles—David Brown and Martin Wilson of Napier University, Lang Tran (Institute of Occupational Medicine), and Gunter Oberdorster (University of Rochester). We also acknowledge the funding of the Medical Research Council, British Occupational Health Research Foundation, and the Colt Foundation in particular. We thank Dr Robert Maynard of the UK Department of Health for his continuing encouragement and support for this work. Thanks to Lang Tran and Colin Dick for reading this article and making useful comments and to Dr Alan Jones (Institute of Occupational Medicine) for a discussion on the aerodynamics of particles. KD is the British Lung Foundation Transco Fellow in Air Pollution and Respiratory Health.
This article is dedicated to the memory of the late Dr Graham Patrick of the MRC Toxicology Unit, University of Leicester. UK, whose work on particles in the lung was internationally known.
References
QUESTIONS (see answers on page 199)
- (1)
- Which of the following is the correct defined size of ultrafine particles?
(a) > 100 μm
(b) < 100 nm
(c) < 1000 μm
(d) < 500 nm
(e) < 10 nm
- (2)
- Are the following associated with increases in PM10?
(a) Deaths from respiratory causes
(b) Symptoms of fever
(c) Worsening of symptoms of asthma in patients with pre-existing asthma
(d) Deaths from heart attacks
(e) Attacks of chronic obstructive pulmonary disease (COPD)
- (3)
- Which of the following is true of PM10 sampling convention measures?
(a) Mass of particles with a 50% efficiency for those with an aerodynamic diameter of 50 μm
(b) Mass of particles with 50% efficiency for those with an aerodynamic diameter of 10 nm
(c) Mass of particles with 10% cut off for those with an aerodynamic diameter of 50 μm
(d) Mass of particles with a 50% efficiency for those with an aerodynamic diameter of 10 μm
(e) Number of particles with 50% efficiency for those with an aerodynamic diameter of 50 μm
- (4)
- Which of the following statements on ultrafine particles is not correct?
(a) They are found in large numbers in urban air
(b) They have a large surface area per unit mass
(c) The form aggregates
(d) They have a smaller surface area than the same mass of larger particles
(e) They can exert their effects through mechanisms other than transition metals
- (5)
- Which of the following groups are susceptible to the adverse effects of PM10?
(a) Patients with asthma
(b) Patients with cystic fibrosis
(c) Patients with COPD
(d) Patients with cardiovascular disease
(e) Patients with hayfever