Article Text

Abstract
Background: Considerable research has been conducted into the nature of airway inflammation in chronic obstructive pulmonary disease (COPD) but the relationship between proximal airways inflammation and both dynamic collapse of the peripheral airways and HRCT determined emphysema severity remains unknown. A number of research tools have been combined to study smokers with a range of COPD severities classified according to the GOLD criteria.
Methods: Sixty five subjects (11 healthy smokers, 44 smokers with stage 0–IV COPD, and 10 healthy non-smokers) were assessed using lung function testing and HRCT scanning to quantify emphysema and peripheral airway dysfunction and sputum induction to measure airway inflammation.
Results: Expiratory HRCT measurements and the expiratory/inspiratory mean lung density ratio (both indicators of peripheral airway dysfunction) correlated more closely in smokers with the severity of airflow obstruction (r = −0.64, p<0.001) than did inspiratory HRCT measurements (which reflect emphysema severity; r = −0.45, p<0.01). Raised sputum neutrophil counts also correlated strongly in smokers with HRCT indicators of peripheral airway dysfunction (r = 0.55, p<0.001) but did not correlate with HRCT indicators of the severity of emphysema.
Conclusions: This study suggests that peripheral airway dysfunction, assessed by expiratory HRCT measurements, is a determinant of COPD severity. Airway neutrophilia, a central feature of COPD, is closely associated with the severity of peripheral airway dysfunction in COPD but is not related to the overall severity of emphysema as measured by HRCT.
- COPD, chronic obstructive pulmonary disease
- E/I ratio, expiration/inspiration ratio
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- HRCT, high resolution computed tomography
- Kco, lung carbon monoxide transfer coefficient
- LAA, area of low attenuation
- MEF, mid expiratory flow
- MLD, mean lung density
- RV, residual volume
- TLC, total lung capacity
- Tlco, carbon monoxide lung transfer factor
- emphysema
- smoking
- chronic obstructive pulmonary disease
- HRCT scanning
Statistics from Altmetric.com
- COPD, chronic obstructive pulmonary disease
- E/I ratio, expiration/inspiration ratio
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- HRCT, high resolution computed tomography
- Kco, lung carbon monoxide transfer coefficient
- LAA, area of low attenuation
- MEF, mid expiratory flow
- MLD, mean lung density
- RV, residual volume
- TLC, total lung capacity
- Tlco, carbon monoxide lung transfer factor
Chronic obstructive pulmonary disease (COPD) develops in smokers as a result of a combination of varying degrees of peripheral airway remodelling and emphysema, both of which are associated with airway inflammation and distortion of the pulmonary vascular morphology.1–3 The study of surgical and post-mortem samples has provided an insight into parenchymal and small airway changes,4–7 while high resolution computed tomography (HRCT) density mask analysis has enabled non-invasive quantitation of emphysema, showing that it correlates with the pathological changes seen in tissue samples.8,9 Complementing these studies, bronchial biopsy, bronchoalveolar lavage (BAL) and, more recently, induced sputum analysis have been used to describe a number of pathological features such as infiltration of the airways with neutrophils,10 macrophages,11 and CD8+ T cells12 as being typical of COPD.
Despite the availability of induced sputum (to analyse large airway inflammation) and objective HRCT indicators of lung density which provide measurements of emphysema and peripheral airways dysfunction, no studies have combined these approaches to see whether there is any relationship between proximal airway inflammation and distal airway changes.
In this study we combined a number of validated methods to study subjects from a wide clinical spectrum of COPD. We correlated lung function measurements, as an index of disease severity, with expiratory HRCT densitometry measurements and the expiratory/inspiratory mean lung density ratio (E/I ratio), which are affected by peripheral airway obstruction and air trapping,13–17 and inspiratory HRCT measurements which reflect the extent of emphysematous destruction.8,9 We then sought to relate the type and intensity of large airway inflammation (as assessed in induced sputum) to the severity of small airways dysfunction and emphysema (as determined by HRCT).
METHODS
The study was approved by the Southampton University and General Hospitals ethics committee. Volunteers were prospectively recruited for the purpose of the study and gave their written informed consent.
Clinical assessment and classification by disease severity
A detailed clinical history was taken and physical examination performed. Lung function testing consisted of spirometry, carried out according to the ATS guidelines,18 flow-volume loop with flow rate measurements at 50% expiration (MEF50), measurement of the ratio of residual volume to total lung capacity (RV/TLC), and carbon monoxide gas transfer coefficient (Kco) and factor (Tlco). Bronchodilator responsiveness to 400 μg salbutamol was assessed and post-bronchodilator spirometric values were recorded. Histamine bronchial provocation challenge was carried out as reported previously.19
Based on clinical assessment and HRCT scanning, a total of 65 subjects were enrolled and classified into five groups according to the GOLD criteria:20 (1) healthy control subjects (n = 10) with normal lung function and no emphysema; (2) healthy smokers (n = 11) without chronic bronchitis and emphysema (as judged by the radiologists’ (CP and DJD) interpretation of their HRCT scan) and with normal lung function; (3) stage 0 COPD (n = 17)—that is, smokers with cough and sputum production but normal spirometry; (4) stage I COPD (n = 10) with mild airflow limitation (forced expiratory volume in 1 second (FEV1) >80% of predicted, and FEV1/forced vital capacity (FVC) <70%); and (5) stage II–IV COPD (n = 17) with moderate to severe airflow obstruction (FEV1 <80% and FEV1/FVC <70% (table 1)). Of the 17 subjects with stage II–IV COPD, 12 were stage II, three were stage III, and two were stage IV. None of the volunteers was atopic and none showed significant bronchodilator reversibility (either >15% of baseline FEV1 or >200 ml). Five subjects with more severe COPD did not undergo histamine bronchial provocation challenge as their baseline FEV1 was too low (<50%). All of the other subjects had normal responsiveness to histamine. All had been free of chest infections and in all cases sputum microbiological culture results were negative with no evidence of bacterial infection of the airways. No subject had had oral corticosteroid therapy for at least 3 months. Furthermore, none had ever been on inhaled corticosteroids.
Clinical characteristics and HRCT measurements performed on inspiration and expiration of the five subject groups
HRCT
HRCT scanning was used for the evaluation of both emphysema and peripheral airways dysfunction. Scans (Hi-speed CTi scanner, General Electric) were performed on full inspiration and expiration at 10 mm intervals with a collimation (slice thickness) of 1 mm. The scanner was subject to a weekly quality assessment with a phantom check including uniformity, linearity, and noise. In addition there was a 3 monthly engineering check of spatial and contrast resolution and an annual medical physics check. Scanning voltage was 140 kV and current was 250 mA. Hard copy images were photographed at a window level of –650 HU and a window width of 1500 HU, as appropriate for viewing lung parenchyma. The scans were evaluated for the presence of emphysema both qualitatively by two radiologists independently of the remaining research and quantitatively by computerised density mask analysis. Two lung density parameters were measured: % area of low attenuation (% LAA) with low attenuation being defined as <−950 Hounsfield density units,9 and mean lung density (MLD)—that is, the mean attenuation value of all voxels excluding the mediastinum and trachea. Peripheral airways dysfunction and expiratory gas trapping were assessed radiologically by calculating the ratio of the MLD on expiration to MLD on inspiration (E/I ratio), as described in previous studies.15,16
Assessment of airway inflammation
Airway inflammation was assessed in induced sputum. Sputum induction was carried out as previously reported.21 Cytospins were made, coded, and differential cell counting was performed on 600 cells. Results are shown as absolute and relative counts (percentage of non-squamous inflammatory cells). In addition, sputum samples were sent for microbiological culture to allow exclusion of subjects with detectable bacterial infection of the airways.
Data analysis
Statistical analysis was performed using SPSS version 10.0. Normally distributed data (lung function and HRCT) were compared between multiple groups by ANOVA, followed by the Scheffe examination for individual comparisons. Cell counts in sputum were compared using the Kruskal-Wallis test followed by the Mann-Whitney test. Trend analysis for the clinical groups was performed using the Jonckheere-Terpstra test. Correlations were sought by Pearson’s and Spearman’s tests for normally and non-normally distributed data, respectively. Correction for multiple correlations was carried out using the Holm method,22 which is a modification of the Bonferroni method but has higher power at the same type I error rate. Thus, if pj is the p value corresponding to variable j and there are k variables (hypotheses) to test, the Holm method consists of multiplying the jth smallest p value by k − j + 1. p values <0.05 were regarded as significant.
RESULTS
The five subject groups were matched for age. Although the three COPD groups were matched for the number of pack years, smokers with stage II–IV COPD had a significantly greater pack year history than healthy smokers (table 1). The Tlco was significantly reduced in all three COPD groups compared with non-smokers and in patients with stage II–IV COPD compared with healthy smokers also. Kco measurements were lower in all smoking groups than in non-smokers but did not differ significantly between smoking groups. Using the Jonckheere-Terpstra test, a significant trend was observed for the Tlco, but not the Kco, to fall with advancing disease stage (p<0.001, table 1).
Appraisal of HRCT scans by radiologists
None of the healthy non-smokers and, by definition, the healthy smokers had emphysema on HRCT scans as assessed by the radiologists. In contrast, 11/17 subjects with stage 0 COPD, 7/10 subjects with stage 1 COPD, and 11/17 with stage II–IV COPD were identified as having HRCT evidence of emphysema. The amount of emphysema in all 11 cases of stage 0 COPD was described as minimal (<5% of total lung area) while in stage I and II–IV disease the extent of emphysema ranged from minimal to severe (>30% of total lung area).
Computerised density mask analysis of HRCT
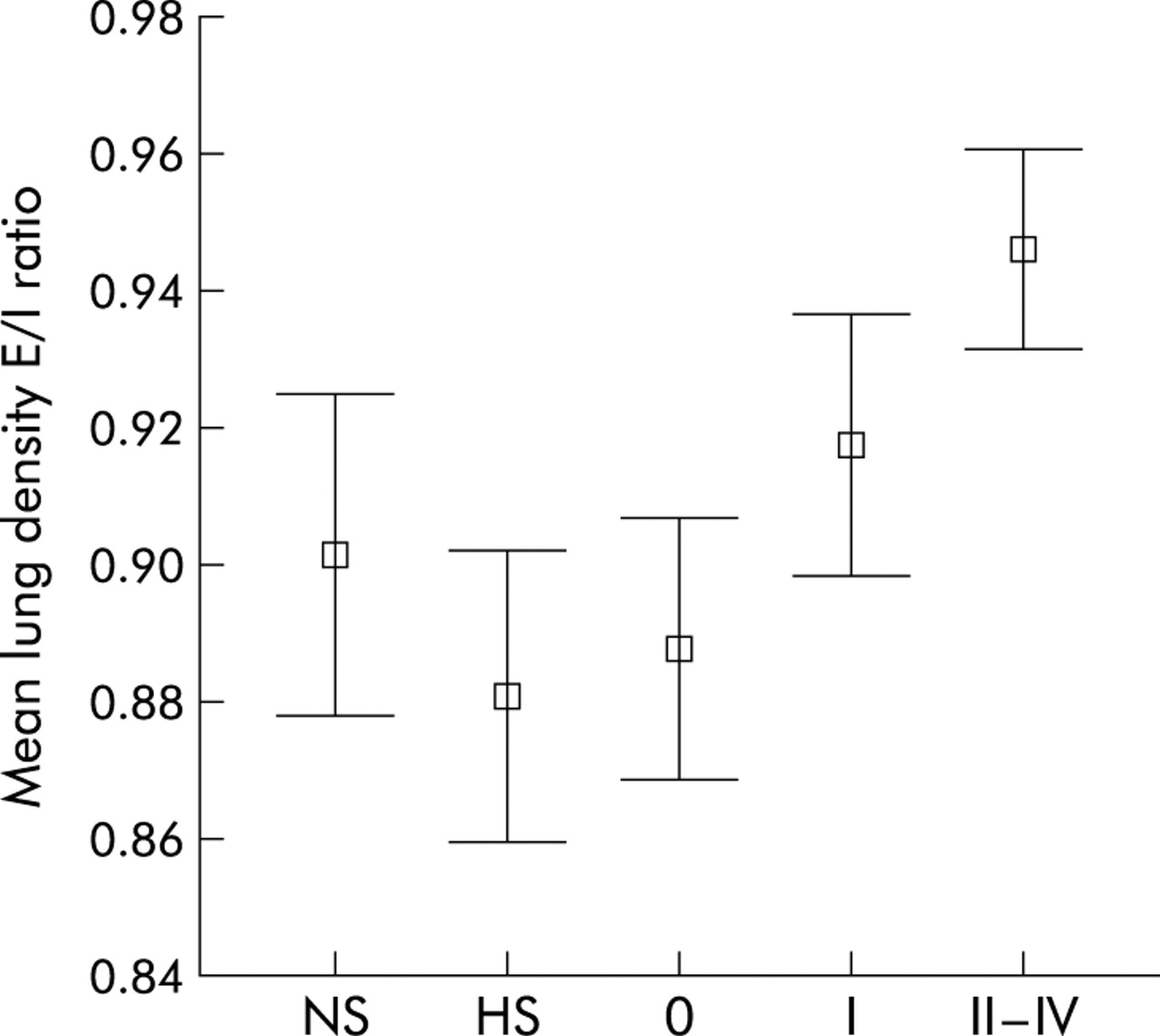
The comparison of %LAA and MLD by ANOVA (allowing for multiple comparisons) showed significant differences between the groups only when comparing expiratory HRCT measurements. Post hoc analysis using the Scheffe test showed no differences between non-smokers and any of the smoker groups for expiratory HRCT measurement (%LAA and MLD; table 1), while the E/I ratio was significantly higher in patients with stage II–IV COPD than in non-smokers, healthy smokers, and those with stage 0 COPD (table 1 and fig 1). Further comparison of %LAA on expiration showed a significant increase in both stages I and II–IV COPD compared with both healthy smokers and patients with stage 0 COPD (table 1). Moreover, MLD on expiration was significantly reduced in patients with stage II–IV COPD compared with healthy smokers and those with stage 0 COPD, and in stage I COPD compared with healthy smokers (table 1).

Lung density expiratory/inspiratory (E/I) ratio in non-smokers (NS), healthy smokers (HS), and patients with stage 0, I, and II–IV COPD. The ratio was significantly higher in smokers with airflow obstruction than in healthy smokers, patients with stage 0 COPD, and non-smokers. Values are expressed as means with standard deviation.
When smoking related trends in HRCT densitometry were analysed in the four smoking groups in isolation using the Jonckheere-Terpstra test, significant trends were observed for %LAA to rise and MLD to fall with advancing disease stage on both inspiration and expiration (p<0.001 in all cases). There was also a significant trend for the E/I ratio to rise with advancing disease stage (p<0.001).
Correlations between HRCT and lung function
Lung function correlated moderately strongly with HRCT parameters (table 2). The strongest correlations seen in smokers were between the E/I ratio on the one hand and airway obstruction (FEV1 % predicted; fig 2), mid expiratory flow (MEF50), and gas trapping (RV/TLC) on the other, with no correlation being seen with Tlco or Kco. Strong and highly significant correlations were also observed between MLD and FEV1, MEF50, and RV/TLC but not either Tlco or Kco. These correlations were stronger on expiration than inspiration. Both expiratory and inspiratory %LAA correlated weakly to moderately strongly with FEV1 and RV/TLC but also, albeit weakly, with Tlco but not at all with Kco. These correlations were only marginally stronger on expiration.
Correlation in smokers between HRCT measurements performed on inspiration and expiration and lung function
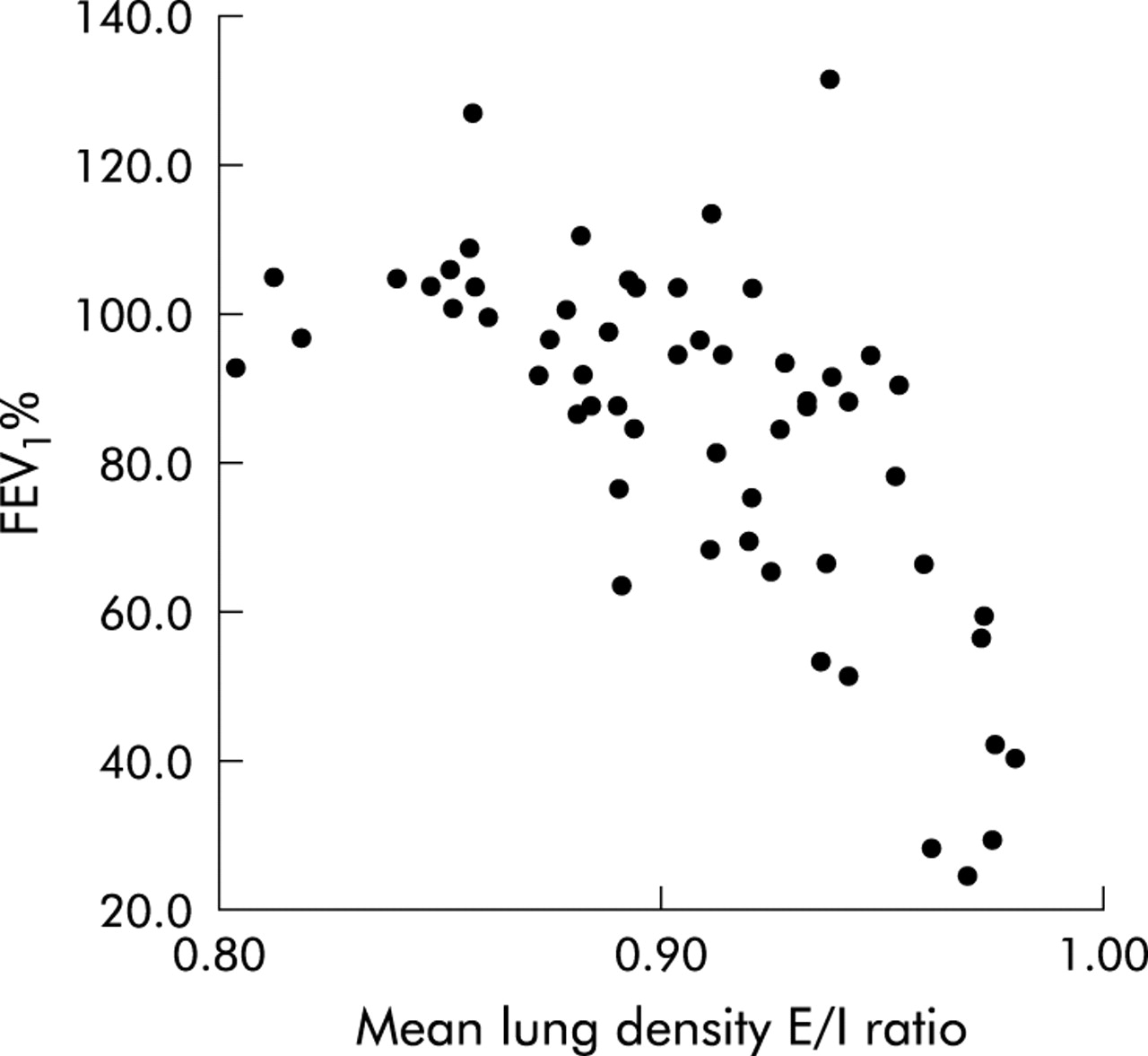
Relationship between the lung density E/I ratio and FEV1 % predicted (r = −0.66, p<0.001).
Assessment of airway inflammation
No significant differences were observed between any of the groups with regard to the total numbers of cells in induced sputum. The only cell counts that were different between the groups were the relative counts of neutrophils and macrophages. Relative neutrophil counts were significantly higher in stage II–IV COPD than in all other groups (table 3). The relative macrophage counts followed a reciprocal pattern to the neutrophils, being significantly reduced in stage II–IV COPD compared with all the other groups. Despite the absence of significantly increased absolute neutrophil counts, significant trends were observed using the Jonckheere-Terpstra tests for both relative (p = 0.001) and absolute (p = 0.007) neutrophil counts to rise with advancing disease stage (table 3).
Relative (percentage of non-squamous cells) and absolute (total number of cells × 106 expectorated over 20 minutes) neutrophil and macrophage counts in induced sputum
Relative neutrophil counts correlated significantly with measurements of airway obstruction and gas trapping (FEV1 % predicted (r = −0.54, p<0.001), FEV1/FVC ratio (r = −0.52, p<0.001), RV/TLC (r = 0.56, p<0.001)) and with the E/I ratio (r = 0.55, p<0.001; fig 3). Relative neutrophil counts correlated more strongly with expiratory MLD (r = −0.59, p<0.001) than with inspiratory MLD (r = −0.42, p< 0.005). No significant correlations were observed between relative neutrophil counts and either inspiratory %LAA or Tlco % predicted. Absolute sputum neutrophil counts correlated only weakly with the FEV1/FVC ratio (r = −0.36, p<0.001) and with the RV/TLC (r = 0.3, p<0.05) but not with any other lung function or HRCT parameter. Like relative neutrophil counts, no significant correlations were observed between absolute neutrophil counts and either inspiratory %LAA or Tlco % predicted.

{kind=link}
{kind=link}
{kind=link}
Relationship between relative sputum neutrophil counts and lung function measurements of (A) airflow obstruction (FEV1 % predicted: r = −0.54, p<0.001), (B) gas trapping (RV/TLC: r = 0.56, p<0.001) and (C) the expiratory/inspiratory (E/I) ratio (r = 0.54, p<0.001).
DISCUSSION
We have investigated the relationship in COPD between proximal airway inflammation, as judged by induced sputum, and quantitative HRCT measurements of peripheral airway dysfunction and emphysema. The study shows that peripheral airway dysfunction is significantly associated with airflow limitation in mild and moderate COPD, although it does not establish whether this occurs due to small airway remodelling or loss of elastic recoil caused by emphysema. As shown previously,12,23 sputum neutrophil counts were significantly related to COPD severity. However, the results show for the first time that neutrophil counts are significantly associated with HRCT indices of peripheral airways dysfunction but not with the severity of emphysema.
HRCT is a useful non-invasive tool to assess emphysema.24 Its interpretation depends on whether scans are taken on inspiration or expiration. Thus, %LAA correlates better with emphysematous destruction of the lungs on inspiration8,9 while both MLD and %LAA correlate more closely with functional impairment (airflow obstruction and gas transfer) when analysed during expiration,13,14 and CT scanning on expiration differentiates better between COPD subjects and healthy controls.17 Calculation of the MLD E/I ratio allows indirect evaluation of gas trapping and small airway dysfunction.15,16 These differences have been explained by the fact that expiratory, but not inspiratory, CT scanning25,26 also reflects peripheral airway dysfunction that causes air trapping.8,15,27 By contributing to both airway obstruction and gas trapping, peripheral airway dysfunction is believed to provide an explanation for the stronger correlation between spirometric and expiratory HRCT parameters.14,15,28
The current study shows that both expiratory HRCT measurements and the MLD E/I ratio correlate more closely with lung function impairment and are more effective in distinguishing smokers with and without airflow obstruction than either inspiratory HRCT, Tlco or Kco. Although the Tlco, which may be affected by peripheral airways obstruction,14 displayed a significant downward trend with advancing disease stage and was associated with %LAA, the Kco, which is more closely related to diffusion impairment, was statistically similar in smokers with and without COPD. The results support the view that small airway dysfunction is a major determinant of reduced lung function in mild to moderate COPD, and a greater predictor of functional impairment than the percentage volume of emphysema as measured by inspiratory %LAA in the current patients.
Whether peripheral airways dysfunction is principally determined by emphysematous destruction of the lung or small airways remodelling cannot be determined by HRCT scanning because it is not as sensitive as histological analysis of lung tissue and may not be sensitive enough to detect early or mild emphysematous changes that can be seen by pathological examination.24,29 Even histological assessment has limitations; peripheral airway instability and loss of elastic recoil linked to destruction of alveolar attachments30 may be present in smokers without emphysema being detected even by pathological examination.31 Thus, subjects with significant airflow limitation may have more parenchymal destruction than can be appreciated by HRCT but which, nonetheless, is contributing to peripheral airway dysfunction.
An important objective of this study was to relate sputum inflammatory cells to airflow limitation and the HRCT indicators of air trapping and emphysema. The finding of raised relative sputum neutrophil counts in COPD is consistent with other studies.32,33 Importantly, the counts correlated strongly with measurements of peripheral airway obstruction and gas trapping (RV/TLC ratio), MLD on expiration and the E/I ratio but, interestingly, no correlation was observed with either inspiratory %LAA or Tlco, both indicators of emphysema. Only subjects with moderate to severe COPD had significantly raised neutrophil counts. In keeping with these results, it has previously been shown that, although smokers with very severe emphysema have prominent neutrophilic inflammation in the alveolar walls and air spaces,6 smokers with mild emphysema without airflow obstruction have neither BAL34 nor alveolar neutrophilia.6 Our results therefore suggest that relative sputum neutrophil counts in smokers are of much greater clinical relevance as an indicator of peripheral airways dysfunction than of emphysema detected by HRCT scanning. We speculate that increased relative sputum neutrophil counts reflect the more distal neutrophilic inflammation that is associated with bronchiolitis and/or destruction of peripheral airway alveolar attachments. To what degree, however, the results may be affected by chronic bacterial colonisation of the airways is uncertain. Although the study only included subjects without either a history of lower respiratory tract infection or evidence of bacterial infection as determined by microbiological culture, undetected bacterial airway colonisation in some smokers remains an important potential influence on neutrophil counts. Finally, when neutrophilic inflammation was assessed in terms of absolute counts, the differences between COPD and healthy subjects did not achieve significance although there was also a significant trend for counts to increase with advancing disease stage. This observation is in contrast to previous studies.32,33 The counts correlated only weakly with airflow obstruction and not at all with any other lung function or HRCT parameter, suggesting that they are of limited value as indicators of COPD severity.
In conclusion, this study provides evidence that peripheral airways dysfunction is a key determinant of COPD severity and that airway lumen neutrophilia is associated with this dysfunction but is not associated with the overall extent of emphysema as determined by quantitative HRCT. These findings suggest that the study of proximal airway secretions is of limited value in identifying the pathological determinants of emphysema severity.
Acknowledgments
The authors thank the staff of the Histochemistry Research Unit, Division of Infection, Inflammation and Repair, University of Southampton for their assistance with sample analysis.
REFERENCES
Footnotes
-
This work was funded by AstraZeneca.