Article Text

Abstract
Background: The debate as to whether asthma is a single or heterogeneous disease remains unresolved although pathological studies, mostly using fibreoptic bronchoscopy on small numbers of subjects, have emphasised the similarities between different clinical phenotypes.
Methods: Lower airway inflammation was assessed non-invasively using induced sputum in 34 normal controls and 259 adults with symptomatic asthma receiving treatment at steps 1–3 of the British Thoracic Society (BTS) guidelines. A subgroup of 49 patients treated with as required β2 agonists only who met BTS criteria for a step up in treatment were studied before and 2 months after treatment with inhaled budesonide 400 μg twice daily.
Results: There was considerable heterogeneity in induced sputum cell counts, particularly in non-atopic patients. A subgroup of 60 patients had a distinctive sputum cell profile with a neutrophil count higher than our normal range (>65.3%) and a normal sputum eosinophil count (<1.9%). These patients were older, predominantly female, and were more likely to be non-atopic but otherwise had similar clinical and physiological features to the group as a whole. Among the 49 subjects studied before and after inhaled budesonide, 11 patients had an isolated sputum neutrophilia. Following treatment, these patients showed significantly less improvement in visual analogue symptom scores (–5.5 v –19.4 mm; mean difference 13.9; 95% CI 0.7 to 27.0), forced expiratory volume in 1 second (FEV1) (–0.08 v 0.13 l; mean difference 0.21; 95% CI 0.03 to 0.39), and concentration of methacholine provoking a fall in FEV1 of 20% or more (PC20) (0.15 v 1.29 doubling doses; mean difference 1.11; 95% CI 0.13 to 2.15) than the remaining 38 patients.
Conclusions: These results suggest the presence of a distinct subgroup of patients with mild to moderate asthma who have predominantly neutrophilic airway inflammation and who respond less well to treatment with inhaled corticosteroids.
- asthma
- induced sputum
- neutrophilic inflammation
Statistics from Altmetric.com
Clinicians have long regarded asthma as a heterogeneous disease,1,2 although detailed clinicopathological studies have tended to emphasise the similarities in the underlying airway pathology and disordered function between patients.3–9 Airway inflammation in asthma has usually been assessed invasively using bronchoscopic techniques, so studies are largely confined to young adults with mild atopic asthma. Whether the findings can be generalised to a wider more heterogeneous population analogous to that seen in clinical practice is unclear.
More recent studies where airway inflammation has been assessed non-invasively using induced sputum in a more diverse range of patients have shown predominant neutrophilic airway inflammation in some patients with severe asthma10,11 and in others studied during acute exacerbations.12 Whether these changes reflect the severity of the disease or the effect of treatment is unclear. We have measured airway inflammation in 34 normal and 259 subjects with symptomatic asthma receiving treatment at British Thoracic Society (BTS) steps 1–313 and have related sputum cell counts to the response to inhaled corticosteroids in 49 subjects. We have used these data to test the hypothesis that a predominant neutrophilic airway inflammation is present in a subset of patients with milder asthma and that this phenotype is associated with a poor response to inhaled corticosteroids.
METHODS
Subjects
Patients and controls were recruited from patients, staff, and volunteers attending the Department of Respiratory Medicine at the Glenfield Hospital. Normal controls had no symptoms suggestive of asthma, were non-smokers or ex-smokers who had not smoked within 12 months of study entry and had a past history of less than 10 pack years, had normal spirometric values (forced expiratory volume in 1 second (FEV1) >80% predicted and ratio of FEV1 to forced vital capacity (FVC) >80%), and normal methacholine airway responsiveness (PC20 >16 mg/ml). Subjects with asthma had consistent symptoms and one or more of the following: a methacholine PC20 of <8 mg/ml; a >15% increase in FEV1 10 minutes after 200 μg salbutamol or a >20% maximum within day variability in peak expiratory flow (PEF) measured twice daily over 14 days. Patients had no clinical or radiological evidence of bronchiectasis and no symptoms suggesting acute lower respiratory tract infection within a month of entering the study. All patients had an FEV1 % predicted of >65% and a smoking history of less than 10 pack years. Clinical records were used to corroborate patients’ smoking histories and exhaled carbon monoxide was measured where there was any doubt.
All patients with asthma treated at BTS steps 1–3 attending our respiratory outpatient clinic who fulfilled the entry criteria and who agreed to participate were included. Assessments were carried out following informed consent as part of a project examining the validity, repeatability, and responsiveness of induced sputum differential inflammatory cell counts which was approved by the Leicestershire Hospitals research ethics committee.
Study design and protocol
Patients and controls attended on two occasions. On the first occasion allergen sensitivity was measured by radioallergosorbent tests for specific IgE or skin prick testing to Dermatophagoides pteronyssinus, cat fur, grass pollen, and Aspergillus fumigatus and atopy was defined as one or more positive skin tests (weal >2 mm larger than negative control) or raised specific IgE (>0.34 kU/l) to one or more antigen. Spirometric tests before and after inhaled salbutamol and chest radiography were performed. Subjects recorded PEF twice daily as the best of three blows over a 14 day period.
On the second visit methacholine airway responsiveness was measured using the tidal breathing method14 followed, after recovery, by sputum induction and processing as previously described.15 The duration of inhalation of hypertonic saline was standard. A subgroup of patients taking as required β2 agonists only who met the BTS criteria for a step up in treatment (using rescue β2 agonists more than once per day, having nocturnal wakening or limitations in activities, peak flow variability ≥20%, or PEF ≤80% of predicted or best)13were given inhaled budesonide 400 μg twice daily for 2 months. These patients identified their predominant symptom (breathlessness, wheeze, or cough) and the severity of this was assessed using a 100 mm visual analogue scales (VAS) from no symptom (0 mm) to the worst ever symptom (100 mm). This scale was the most responsive outcome measure in our earlier study16 and has been validated.17
The patients then attended for a third visit when the spirometric tests, methacholine inhalation test, and VAS symptom scores were repeated 12 hours after the last dose of treatment.
Data from some of these patients have been presented previously.16
Analysis of data
Normal ranges were derived from the eosinophil and neutrophil counts of the control subjects as the mean + 2SD and the mean + 1.7SD using one tailed and two tailed tests, respectively. One tailed tests were used for eosinophil counts since there is no lower reference limit. Spirometric values, induced sputum macrophage, neutrophil, lymphocyte and epithelial differential cell counts and maximum PEF amplitude % mean were described as mean (SE) values. Methacholine PC20 results were log normally distributed and were log transformed and described as geometric mean (log SE) values. Sputum eosinophil counts were expressed as median and interquartile range (IQR). Differences between groups were analysed for normally distributed variables using the independent t test and for variables not observing a normal distribution using the Mann-Whitney U test. The correlation between sputum eosinophils and methacholine PC20, PEF amplitude % mean (A%M), and FEV1 were assessed using the Spearman rank test. Differences in methacholine PC20 were expressed as doubling doses. The χ2 test was used to compare the percentage of patients using inhaled steroids and the percentage of atopic patients between groups.
RESULTS
All subjects
Normal ranges derived from normal subjects were <65.3% for sputum neutrophil counts and <1.9% for sputum eosinophil counts. 143 patients had intermittent asthma treated with as required β2 agonists only (step 1 of the BTS guidelines)13; 116 had more persistent symptoms requiring regular inhaled corticosteroids (steps 2 and 3) (table 1).13 Twenty patients (11 steroid naïve, nine atopic) were current smokers and 78 (42 steroid naïve, 26 atopic) were ex-smokers, but all had a history of <10 pack years. Patient details categorised according to atopic status and use of inhaled corticosteroids are shown in table 1. The mean (SE) daily dose of inhaled steroid (in beclomethasone equivalent doses) for atopic and non-atopic subjects was 424 (56) μg and 416 (50) μg, respectively. Non-atopic asthma was associated with less methacholine airway responsiveness (methacholine PC20 1.34 mg/ml v 0.68 mg/ml; geometric mean difference 1.0 doubling doses; 95% CI of difference 0.4 to 1.6; p=0.002) and higher mean neutrophil count (54.1% v 45.0%; mean difference 9.1%; 95% CI of difference 2.3 to 15.8; p=0.008).
Patient details and sputum cell counts in normal controls, atopic and non-atopic subjects
Sputum evidence of eosinophilic airway inflammation was the most common abnormality in the group as a whole with 135 patients (52%) having an induced sputum eosinophil count outside our normal range (fig 1). The median sputum eosinophil count was significantly lower in atopic subjects receiving inhaled corticosteroids (1.1%) than in similarly treated non-atopic subjects. (3.3%, p<0.05; table 1). Among the whole study population there was no correlation between the sputum eosinophil count and the methacholine PC20 (r=–0.03; p>0.05), the maximum PEF amplitude % mean (r=–0.02, p>0.05), or the % predicted FEV1 (r=–0.03, p>0.05). Among the 114 atopic patients a weakly negative correlation was observed between the sputum eosinophil count and the methacholine PC20 (r=–0.30, p<0.01), while the 145 non-atopic patients demonstrated a weakly positive correlation between these two measurements (r=0.22, p<0.05).

{kind=link}
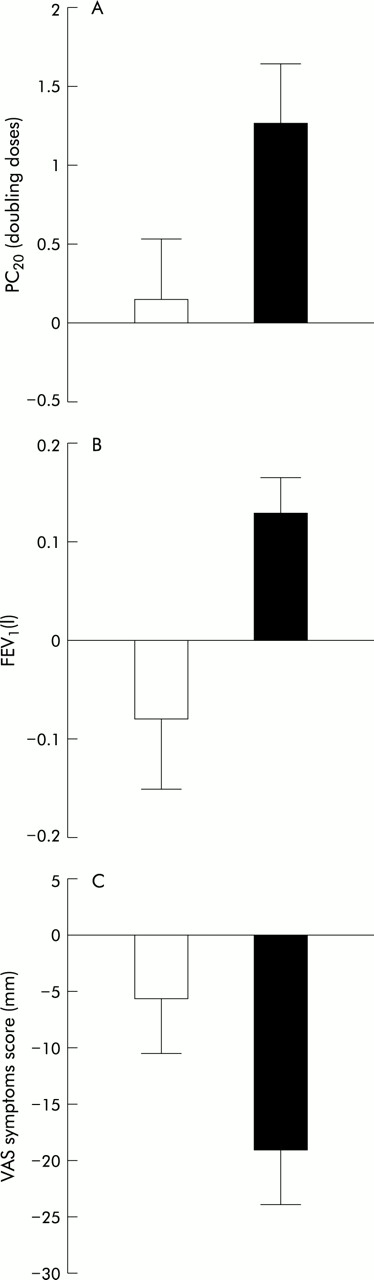
Change in (A) concentration of methacholine provoking a fall in forced expiratory volume in 1 second (FEV1) of 20% or more (PC20), (B) FEV1, and (C) VAS symptom score following 2 months of treatment with budesonide 400 μg twice daily in neutrophilic patients (open bars) and all other patients (closed bars).
Subgroup with isolated neutrophilic inflammation
There was considerable heterogeneity in induced sputum eosinophil and neutrophil cell counts, even among those patients treated with as required β2 agonists alone. A subgroup of 60 patients, including 35 who were steroid naive, had a distinctive sputum cell profile with a sputum neutrophil count outside the normal range and a normal sputum eosinophil count. Five of these were current smokers and 20 were ex-smokers. These patients were older, tended to develop asthma later, and were more likely to be female and non-atopic than the group as a whole. Clinical and physiological features were otherwise similar (table 2).
Characteristics of patients with isolated sputum neutrophilia and all other patients studied
Patients studied before and after treatment with inhaled corticosteroids
Ninety two of the patients treated with as required β2 agonists only met the BTS criteria for a step up in treatment. Forty nine such patients were randomly selected and agreed to attend again 2 months after treatment with inhaled budesonide 400 μg twice daily. Of these subjects, 11 were included in the subgroup described above, having an isolated sputum neutrophilia with a normal sputum eosinophil count (table 3). Compared with the other 38 patients studied before and after treatment, these subjects had significantly less improvement in VAS scores (–5.5 v –19.4 mm; mean difference 13.9; 95% CI 0.7 to 27.0; p=0.04), FEV1 (–0.08 v 0.13 l; mean difference 0.21; 95% CI 0.03 to 0.39; p=0.026), and PC20 (0.15 v 1.29 doubling doses; mean difference 1.11; 95% CI 0.13 to 2.15; p=0.029; fig 1).
Baseline characteristics of patients studied before and after treatment with budesonide 400 μg twice daily for 2 months
DISCUSSION
We have analysed the extent and nature of airway inflammation in induced sputum in normal controls and in a large population of well characterised patients with asthma. Our estimates of normal ranges, although derived from small numbers, are very similar to findings in larger populations.18,19 In the adults with asthma receiving treatment at BTS stages 1–3 and with relatively normal spirometric parameters, we found considerable heterogeneity in induced sputum inflammatory cell counts. Importantly, a number of predominantly female, non-atopic patients with adult onset asthma had a distinctive sputum inflammatory cell profile consisting of sputum neutrophilia and a normal sputum eosinophil count. Furthermore, a subgroup of steroid naïve subjects with this isolated neutrophilic inflammation had an impaired response to treatment with inhaled corticosteroids.
Previous studies have noted sputum evidence of isolated neutrophilic airway inflammation in some patients with severe asthma10,11 and in a minority of adults studied during asthma exacerbations.12 Gibson et al used induced sputum to assess 56 patients with persistent asthma taking high doses of inhaled corticosteroids and found that 59% of patients had suppressed sputum eosinophil counts but evidence of neutrophilic inflammation.20 Wenzel et al used bronchoscopic techniques to characterise the underlying airway immunopathology of a group of patients with severe refractory asthma who had severely impaired lung function and were treated with high dose inhaled steroids and oral prednisolone and have suggested the presence of a subgroup who have a predominant neutrophilic airway inflammation, absence of eosinophils, and normal basement membrane thickness.21 It is not clear whether the findings are peculiar to severe asthma or reflect the effects of treatment with high doses of corticosteroids. Our results provide support for the presence of such a distinct asthma phenotype and, for the first time, show that it is a relatively common finding in patients with milder asthma and, in some subjects at least, that it is not an artefact due to corticosteroid treatment. The incidence of neutrophilic inflammation was higher in the population studied by Gibson et al20 and in the patients with severe asthma studied by Wenzel et al,21 and it remains possible that this phenotype is particularly associated with more severe disease. We have further extended these earlier findings by showing a significantly impaired response to inhaled corticosteroids in a subgroup of the subjects with an isolated neutrophilia. The poor response to inhaled corticosteroid is not only of obvious clinical significance, but it also provides a possible mechanism by which subjects might be particularly likely to evolve into more severe refractory cases.
We do not have a clear explanation for the development of neutrophilic airway inflammation in these patients. All patients had a smoking history of less than 10 pack years, only a few were current smokers, and the patients with isolated sputum neutrophilia were no more or less likely to have ever smoked than the remaining group. We therefore doubt that current smoking and early chronic obstructive pulmonary disease were important explanations for the unusual inflammatory cell profile. All the patients presented with symptoms consistent with asthma, had normal chest radiographs and no clinical evidence of acute infection, although we cannot exclude the possibility of subtle subclinical bronchiectasis or lower respiratory tract infections. Idiopathic chronic cough has a similar female predominance and age at onset of symptoms and is associated with a sputum neutrophilia.22 These similarities suggest there might be parallels between these conditions. Further work is required to define the lower airway immunopathology in more detail and to investigate its aetiology.
This large observational study of adults with asthma provided us with the opportunity to compare sputum markers of airway inflammation in subjects categorised according to atopic status and use of inhaled corticosteroids, variables that have been traditionally used to phenotype asthma. We identified several differences between atopic and non-atopic subjects that have not been reported before. The higher sputum neutrophil count in non-atopic subjects could reflect the higher incidence of neutrophilic asthma in this group. Non-atopic subjects also had less airway hyperresponsiveness and were more likely to have sputum evidence of persistent eosinophilic airway inflammation despite treatment with inhaled corticosteroids.. These differences support suggestions that non-atopic and atopic asthma represent distinct disease phenotypes.1 Further work is required to determine whether they are clinically significant. The sputum eosinophil count was significantly lower in atopic subjects treated with inhaled corticosteroids than in non-atopic subjects, so one possibility is that atopic patients might not respond as well to a higher dose of inhaled corticosteroids.
There was no correlation between airway hyperresponsiveness and eosinophilic airway inflammation in the population as a whole, although there was a weak negative correlation when atopic subjects were considered alone. These findings challenge the widely held view, reflected by recent definitions of asthma,23,24 that there is a simple causal association between eosinophilic airway inflammation and disordered airway function and suggest a more complex relationship. Other studies examining the relationship between the sputum eosinophil count and airway responsiveness have produced mixed results,25–30 although it is notable that those studies showing a significant correlation have been largely confined to atopic subjects.28–30
We describe a single observation, and in a disease characterised by variability we cannot be sure that the distinctive phenotype seen in our population of adults with asthma is stable. Our estimates of incidence might also be incorrect since we have studied subjects referred for secondary care who might be particularly likely to display unusual features. Longer term studies of a more typical population of asthmatic subjects are required to estimate the true prevalence of this asthma phenotype and to determine whether it is stable. Placebo controlled longer term intervention studies with inhaled corticosteroids and other treatments are also required to assess the efficacy of these interventions fully. Our findings raise the possibility of a distinct phenotype of asthma, with active neutrophilic and suppressed eosinophilic airway inflammation, across the range of severity of asthma that differs in response to treatment and could have important implications for our understanding and treatment of the disease.
Acknowledgments
We thank William Monteiro and Richard Ward for help with sputum processing and members of the department of respiratory physiology for performing the sputum inductions. This work was supported by grants from Astra Zeneca, Trent Region and Glenfield Hospital Research fund. Ruth Green is supported by a National Asthma Campaign grant.
REFERENCES
Footnotes
-
This work was supported by grants from Astra Zeneca, Trent Region and Glenfield Hospital Research fund. Ruth Green is supported by a National Asthma Campaign grant.