Article Text

Abstract
BACKGROUND The rate of failure of non-invasive mechanical ventilation (NIMV) in patients with chronic obstructive pulmonary disease (COPD) with acute respiratory insufficiency ranges from 5% to 40%. Most of the studies report an incidence of “late failure” (after >48 hours of NIMV) of about 10–20%. The recognition of this subset of patients is critical because prolonged application of NIMV may unduly delay the time of intubation.
METHODS In this multicentre study the primary aims were to assess the rate of “late NIMV failure” and possible associated predictive factors; secondary aims of the study were evaluation of the best ventilatory strategy in this subset of patients and their outcomes in and out of hospital. The study was performed in two respiratory intensive care units (ICUs) on patients with COPD admitted with an episode of hypercapnic respiratory failure (mean (SD) pH 7.23 (0.07), Paco 2 85.3 (15.8) mm Hg).
RESULTS One hundred and thirty seven patients initially responded to NIMV in terms of objective (arterial blood gas tensions) and subjective improvement. After 8.4 (2.8) days of NIMV 31 patients (23%; 95% confidence interval (CI) 18 to 33) experienced a new episode of acute respiratory failure while still ventilated. The occurrence of “late NIMV failure” was significantly associated with functional limitations (ADL scale) before admission to the respiratory ICU, the presence of medical complications (particularly hyperglycaemia), and a lower pH on admission. Depending on their willingness or not to be intubated, the patients received invasive ventilation (n=19) or “more aggressive” (more hours/day) NIMV (n=12). Eleven (92%) of those in this latter subgroup died while in the respiratory ICU compared with 10 (53%) of the patients receiving invasive ventilation. The overall 90 day mortality was 21% and, after discharge from hospital, was similar in the “late NIMV failure” group and in patients who did not experience a second episode of acute respiratory failure.
CONCLUSIONS The chance of COPD patients with acute respiratory failure having a second episode of acute respiratory failure after an initial (first 48 hours) successful response to NIMV is about 20%. This event is more likely to occur in patients with more severe functional and clinical disease who have more complications at the time of admission to the ICU. These patients have a very poor in-hospital prognosis, especially if NIMV is continued rather than prompt initiation of invasive ventilation.
- non-invasive mechanical ventilation
- chronic obstructive pulmonary disease
- acute respiratory failure
- survival
Statistics from Altmetric.com
- non-invasive mechanical ventilation
- chronic obstructive pulmonary disease
- acute respiratory failure
- survival
In recent years non-invasive mechanical ventilation (NIMV), delivered through a facial or nose mask, has been successfully used in selected populations as an effective treatment for acute respiratory failure1-4 and as a technique for weaning intubated patients.5 Despite NIMV having also been used in patients affected by “pure” hypoxic respiratory failure,6 most studies have concentrated on patients with chronic obstructive pulmonary disease (COPD). The rate of failure of NIMV in these patients ranges from 5% to 40%.1-4 ,7 ,8 Recognition of this subset of patients is very important both from a clinical and ethical point of view since prolonged application of NIMV may unduly delay the time of intubation. Failure of NIMV has usually been defined as: (a) need for intubation because of lack of improvement in arterial blood gas tensions and clinical parameters after a few hours of ventilation (usually 1–3 hours); (b) clinical deterioration and subsequent intubation during hospital stay, and (c) death.
Studies specifically designed to assess the best predictors of NIMV outcomes agree that changes in pH in the first hour of ventilation and the clinical condition of the patients before ventilation are the most powerful factors linked to success or failure.7 ,9 It has also been shown that, despite an initial improvement in blood gas tensions and clinical condition, a subset of patients go on to die or need to be intubated days after the successful application of NIMV. For example, the multicentre randomised study performed by Brochardet al 1 showed that 15% of their patients with COPD, initially successfully treated with NIMV, needed endotracheal intubation after at least 48 hours. This subgroup of patients is reported to have a very bad prognosis. Similarly Meduriet al,10 in their large prospective study performed on patients with a miscellany of diseases, reported that 28% of the “initial” responders needed endotracheal intubation >48 hours later, with this subgroup having a mortality rate of 22%. The clinical and physiological characteristics of this subgroup of patients have never been assessed, nor has the capacity to predict the occurrence of “late NIMV failure” accurately at the time of instituting ventilation. We have therefore undertaken a multicentre study in which a series of clinical and physiological parameters were recorded in patients with COPD who were initially successfully ventilated with NIMV. The primary aims of the study were (1) to assess the incidence of late failure (at least 48 hours after institution of NIMV) and (2) to determine the parameters, if any, predictive of this failure. The secondary aims of the study were to evaluate the best clinical management and the outcomes in and out of hospital in this subgroup of patients with late NIMV failure.
Methods
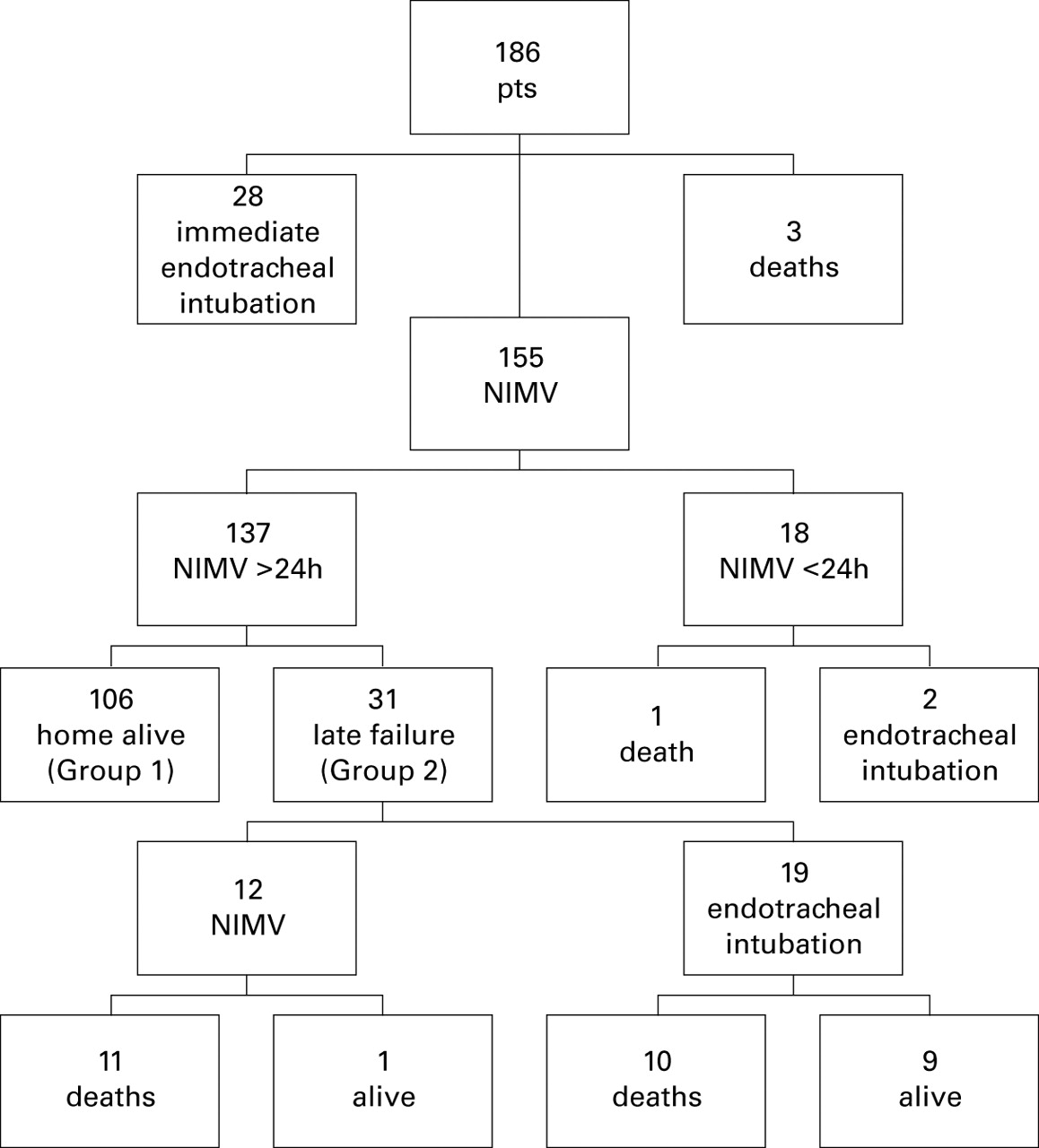
The study was conducted in the respiratory intensive care units (ICUs) of Montescano and Modena for a 29 month period between January 1996 and May 1998. Both ICUs are officially recognised by the Italian Association of Pneumologists and consist, respectively, of four and six monitored beds, with the possibility of using ICU or home care ventilators. The study was approved by the local ethics committees of both institutions and oral informed consent was given by the patients or next of kin. Figure 1 illustrates the distribution of the study population according to treatment and outcome. Of a total of 186 consecutive COPD patients admitted because of an episode of acute hypercapnic respiratory failure, 137 (74%) were successfully ventilated non-invasively at first and were therefore enrolled for data analysis. Acute hypercapnic respiratory failure was defined as the presence of all of the following: acute decrease in pH to ⩽7.34, sudden increase in Paco 2 to more than 60 mm Hg (8 kPa), tachypnoea and/or paradoxical abdominal movements, and severe dyspnoea. The remaining 49 patients were excluded from the study because they needed immediate intubation (n=28), died immediately after intubation (n=3), needed no further ventilatory support after 24 hours of NIMV (n=15), died (n=1), or needed intubation within the first 24 hours while receiving NIMV (n=2). “Initial” success of NIMV was defined as objective and subjective improvement in the first few hours.10 Objective criteria included the following changes from spontaneous breathing in these parameters: pH⩾7.35, decrease in Paco 2 of >15–20% with Sao 2 (with or without oxygen) of ⩾90%, a decrease of ⩾20% in respiratory rate compared with spontaneous breathing, and normal sensory state. Subjective criteria included improvement of dyspnoea and the patient's comfort. Late failure (>48 hours) was defined as a sudden or progressive worsening of arterial blood gas tensions (pH ⩽7.34 with an increase in Paco 2 of >15–20% compared with previous arterial blood gas tensions), dyspnoea and/or sensory deterioration while still on mechanical ventilation for at least 6 hours/day. The diagnosis of COPD was made in accordance with the ATS statement.11 All but 12 patients were receiving long term oxygen therapy. Causes of relapses were pulmonary exacerbations, as defined elsewhere,12 or community acquired pneumonia (for diagnosis of pneumonia, see below).

Distribution of the study population according to the outcome of the NIMV trial.
NIMV was added to standard medical treatment including inhaled β2 agonists, anticholinergic agents, intravenous corticosteroids, xanthines and, when appropriate, antibiotics, furosemide (frusemide), antiarrhythmics or vasoactive agents. Patients were ventilated with pressure support ventilation (PSV) using a full face mask. The inspiratory pressure was adjusted according to the patient's tolerance to obtain an expired tidal volume of 8–10 ml/kg with external PEEP not exceeding 6 cm H2O. Both ICU and home care ventilators (all of which allowed exhaled tidal volume to be recorded) were used. When available, flow and pressures curves were used to detect the possible occurrence of patient/ventilator mismatching.13 Trigger sensitivity was set at –1 cm H2O or the one imposed by the machine was used if setting was not possible. Oxygen was added to achieve an Sao2 of >90%. The patients' ECG, Sao 2, blood pressure, and respiratory rate were continuously monitored. NIMV was delivered almost continuously in the first 24 hours with short intervals of spontaneous breathing with oxygen supplementation to allow the patients to drink and expectorate (and, in some cases, eat). In the following days the levels of PSV and PEEP were gradually decreased using a modality described in detail elsewhere,5 if the patient's condition allowed. Weaning from NIMV was defined as complete freedom from mechanical ventilation for at least 72 hours.
The following variables were recorded on admission and during the hospital stay: demographic data (age, sex);
serum biochemistry (albumin, potassium and sodium);
breathing rate;
haemodynamic variables (blood pressure, heart rate);
arterial blood gas tensions from the radial artery by means of a blood gas analyser (Radiometer ABL 300 Copenhagen, Denmark) recorded at admission, 1–2 hours, and 24 hours after institution of NIMV and then on a daily basis, according to the clinical condition of the patients;
a score of compliance with the ventilation, recorded on a daily basis. This score was arbitrarily given by a respiratory therapist, based on what he judged to be the tolerance of the patient to NIMV, and was calculated using a five point scale already used in other studies where 1 = poor, 2 = quite bad, 3 = sufficient, 4 = good, 5 = excellent14;
severity of illness assessed using the APACHE II (Acute Physiology and Chronic Health Evaluation) score15;
days on mechanical ventilation;
total duration of stay in ICU;
functional limits caused by chronic pulmonary disease evaluated using a score correlated to home activities of daily living (ADL) according to Seneff et al 16 where 1 = severe limits (patient short of breath at rest and does not perform any ADL); 2 = moderate limits (patient short of breath with light activities and unable to perform two or more ADL); 3 = no limits (no more than one limitation in ADL). Data were usually obtained directly from the patients or from family members where there was a lack of collaboration by the patient;
number of complications associated with acute respiratory failure;
number of complications appearing during the stay in the respiratory ICU while still on NIMV.
The definitions of associated complications, modified by Jimenezet al,17 were as follows:
Pneumonia: a new lung infiltrate on the chest radiograph associated with at least two of the following conditions: fever, leucocytosis (WBC >10 000 cells/mm3), purulent sputum in which a Gram stain showed one or more types of bacteria. This was considered as a hospital complication (nosocomial pneumonia) when diagnosed after the third day of admission. If pneumonia was the primary cause of hospital admission for acute respiratory failure, it was considered as being community acquired.
Sepsis syndrome: positive blood cultures and fever of >39°C together with positive cultures from suspected sources (urine, ascites, pleural fluid).
Shock: systolic blood pressure of <90 mm Hg with decreased urinary output or hypotension requiring infusion of vasoactive amines to obtain a blood pressure of >90 mm Hg.
Acute renal failure: an acute rise in serum creatinine of >265.2 μmol in patients with previously normal renal function.
Cardiac impairment: acute arrhythmia requiring quick therapeutic intervention or tachycardia along with clinical and radiographic or echocardiographic evidence of pulmonary congestion which resolved with diuretic therapy.
Gastrointestinal tract complications: macroscopic bleeding, or hepatic dysfunction defined as a twofold increase in glutamic pyruvic transaminase or alkaline phoshatase concentrations or development of jaundice or pancreatitis with a twofold increase in amylase or lipase enzyme concentrations.
Metabolic complications: hyponatraemia of <120 mmol/l or hypercalcaemia or serum potassium levels of <3 mmol/l or >6 mmol/l, or alkalosis with pH >7.6 or metabolic acidosis, fasting hyperglycaemia >200 mg/dl.
Coma: points 4 and 5 of the Kelly and Matthay neurological scale.18
Pulmonary embolism: clinically and echocardiographically suspected and confirmed by perfusion and ventilation lung scans or spiral CT scan, when possible, with normal chest radiography.
New exacerbation of COPD: this was considered as a complication only if the episode requiring admission to the respiratory ICU was resolving, as assessed by improvement in arterial blood gas tensions, normal WBC, and absence of fever, but with the patient still requiring mechanical ventilation for >6 hours/day.
STATISTICAL ANALYSIS
Univariate analysis
Continuous variables were analysed using a Student'st test for independent data, while a pairedt test was applied to compare data of each patient before and after treatment. The categorical values were analysed using the χ2 test (Fisher's two tailed exact test for small samples of data). A p value of <0.05 was considered to be statistically significant.
Multiple logistic regression analysis
This method was employed to build up a predictive model to identify the variables associated with “late failure” in 137 patients treated with NIMV. Patients who did not have a new relapse and who were discharged alive from the respiratory ICU were compared with those who had a “late failure”, therefore needing more aggressive NIMV (see Results) or intubation. The variables considered (univariately significant or of clinical relevance according to the literature, see Discussion), added according to the “forced enter” method, included those measured on admission (haemodynamic variables, number of associated complications on admission, ADL, arterial blood gas tensions, APACHE II, age).
Categorical variables were recoded as dichotomous variables.
Results
As shown in table 1, NIMV resulted in an immediate and sustained improvement in blood gas tensions in COPD patients enrolled after an episode of acute respiratory failure, requiring more than one day of ventilation. The arterial blood gases continued to improve in most of the responders (n=106, 77.3%) so that weaning and discharge from the hospital became possible (group 1). Despite an initially favourable response to NIMV, the clinical condition and arterial blood gas tensions of the remaining 31 patients (22.7%; 95% CI 18 to 33) deteriorated during the hospital stay while NIMV was still being administered (>6 hours/day), so that a new episode of respiratory distress was said to have occurred (group 2).
Mean (SD) demographic, clinical, and functional characteristics recorded at baseline and during non-invasive mechanical ventilation (NIMV) at 1 and 24 hours in patients with COPD grouped according to the success of NIMV (group 1 = successful, group 2 = “late respiratory failure”)
Table 1 shows the arterial blood gases of the two groups of patients during the first 24 hours of ventilation and some clinical and functional characteristics of the patients recorded at enrollment. Heart rate was significantly higher and mean blood pressure significantly lower in patients in group 2 who also had a lower ADL score. On admission the number of associated complications was also higher in patients in group 2, with almost 75% having at least one complication on admission. As shown in table 2, the most frequent complication in both groups was cardiac impairment. Sixteen patients in group 1 had evidence of pulmonary congestion, five had atrial fibrillation, and one had acute arrhythmia while four patients had evidence of pulmonary congestion and three had atrial fibrillation in group 2. The percentages of the other complications, with respect to the total, were equally distributed between the two groups, with the exception of metabolic complications which were significantly more frequent in the “late failure” patients. Interestingly, all the metabolic complications included hyperglycaemia (fasting blood glucose in the three patients in group 1 and the seven in group 2 = 278 (63) mg/dl and 342 (82) mg/dl, respectively).
Number and type of complications on admission and during the hospital stay in groups 1 (successfully treated) and 2 (“late failures”). Note that pneumonia and COPD exacerbations were considered causes of acute respiratory failure necessitating mechanical ventilation
The logistic analysis performed on the variables recorded at the time of admission showed that activities of daily living, the number of complications, and pH recorded on admission strongly predicted the occurrence of “late failure” during NIMV. In the logistic analysis metabolic complication was, among the other complications recorded on admission, the only independently significant predictor of late failure.
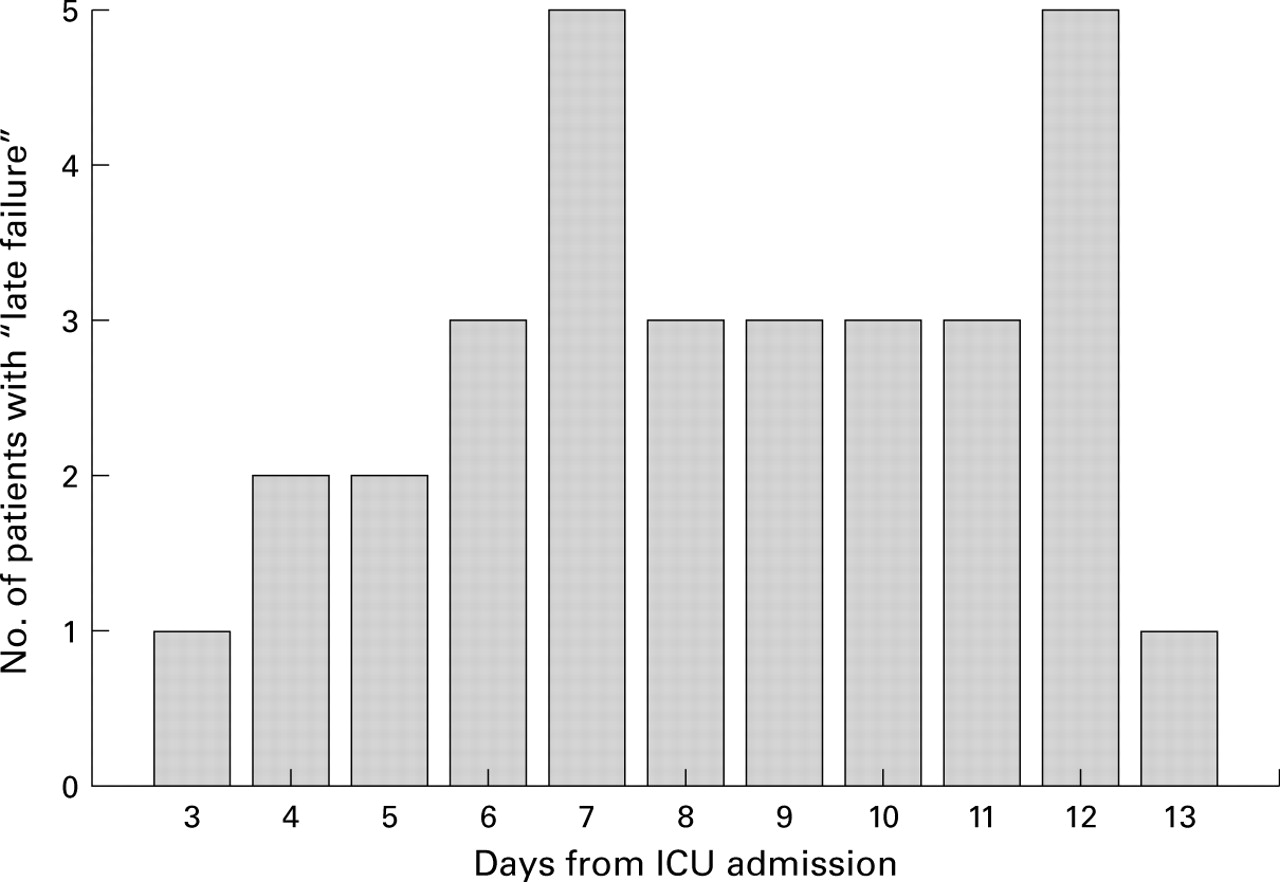
Table 2 also shows the occurrence of complications during the stay in the respiratory ICU while the patients were still receiving NIMV. Only a few patients in group 1 developed a new complication, while all the “late failure” patients suffered at least one, the most frequent being new exacerbations of COPD, cardiac impairment, and nosocomial pneumonia. These complications appeared at a mean of 8.4 days (range 3–13) after admission to the ICU. Figure 2 illustrates the rates of new episodes of acute respiratory failure while still on NIMV.
{kind=link}
{kind=link}
Rate of new episodes of acute respiratory failure in the 31 patients who responded to NIMV in the first 48 hours.
At the time of “late failure” patients in group 2 were still receiving NIMV for a mean of 9.2 hours/day. Newly intensified mechanical ventilation was then started, either by increasing the hours/day of NIMV (group 2A, n=12) or by administering the ventilation via endotracheal intubation (group 2B, n=19). The decision as to which of these two therapeutic strategies to use was made by the attending physician based on whether or not the patient was willing to be intubated.
The overall mortality rate for all groups of patients at hospital discharge was 15.4%. None of the patients in group 1 died compared with 21/31 (68%) in group 2 (11/12 (92%) in group 2A and 10/19 (53%) in group 2B). The main causes of death were cardiac failure, pneumonia, pulmonary embolism, shock, and multiple organ failure. The two groups did not differ in the most common variables recorded at the time of “late failure” or for the number of complications on admission. Both subgroups had a high mean number of hospital complications with cardiac impairment, metabolic complications, and pneumonia being the most frequent.
The clinical characteristics of the patients in group 2B who did or did not survive after intubation were not significantly different at the time of intubation, but the improvement in Paco 2 and pH after 24 hours of invasive ventilation was significantly higher in those who survived (p<0.001).
The out of hospital mortality at 90 days after discharge in groups 1 and 2 was similar at 20% and 19%, respectively.
Discussion
This study, performed in a large population, confirms that NIMV may be useful for avoiding intubation or death in about 70% of patients with COPD who suffer an episode of severe hypercapnic respiratory failure. We found that some initial responders later deteriorate so that, despite an initial brief improvement with NIMV, they may go on to die or to need intubation. The principal finding of our study was that the presence of one or more complications at admission together with a lower pH and more severe clinical condition (ADL scale) are strong predictors of “late failure”. Patients with these characteristics have a very poor prognosis if further hospital complications ensue, especially if “more aggressive” NIMV is preferred to intubation.
The end points of most of the studies of NIMV are need for endotracheal intubation and death.1-4 Most such studies report a substantial percentage of “late” NIMV failure in patients with COPD,1 ,7 ,8 ,10 suggesting that an initial improvement in arterial blood gas tensions and clinical condition during NIMV is not always synonymous with success. This is true for both COPD patients and those with “pure hypoxaemic” respiratory failure.19Predictive models were developed to try to determine which COPD patients with acute respiratory failure would or would not avoid endotracheal intubation. Improvements in Paco 2and pH after the first hour of ventilation were found to be very powerful predictors of the success or failure of NIMV,9together with clinical condition, body weight, and compliance with the ventilator. Most of the studies have considered the patient with COPD to be affected by a single pulmonary pathology and have not taken account of the fact that COPD is a disease which is often accompanied by other pathologies such as cardiovascular complications.20 Seneff et al 16 showed that the presence of non-respiratory physiological abnormalities in patients with COPD with an acute exacerbation of disease, rather than the pulmonary disease itself, may be associated with the worst prognosis.
Using logistical analysis we have shown that, in patients with an episode of acute respiratory failure, the presence of one or more associated complications, a limitation of functional daily life as assessed by the ADL scale, and lower values of pH on admission are associated with the development of “late failure”. We are, however, aware of the limitations of these statistical predictive models, so that our model needs to be prospectively tested in future studies. On admission almost all patients in group 2 had at least one associated complication compared with less than half in group 1. The occurrence of the different types of complications was similar in the two groups, with the exception of metabolic complications which were significantly more frequent in group 2. The most common complications were cardiovascular and occurred with approximately the same incidence in the two groups. On the other hand, the presence of metabolic complications (found in >20% of group 2 patients) was statistically powerful in predicting the occurrence of “late failure”. The most frequent was hyperglycaemia due to diabetes which was present in all the patients with metabolic complications. The iatrogenic form of the disease (mean daily dose of corticosteroids in the days preceding admission to hospital in patients developing hyperglycaemia was 24 (10) mg deflazacort) may lead to a decrease in immunological defences so that patients are more prone to infections.21 All the patients in the “late failure” group with hyperglycaemia on admission developed an infectious pulmonary complication during their hospital stay and, in 13 of the 21 patients who died, pneumonia was a direct or indirect cause of death. Obviously the presence of complications at admission can only partly explain the development of “late failure” since the general clinical respiratory condition at the time of hospital admission is also important. For example, poor gas exchange at admission has recently been shown by Connorset al 22 to be associated with a poorer prognosis together with impairment of daily functional activity. The presence of community acquired pneumonia on admission was higher in group 2 than group 1; the difference was not significant because of the small number of cases but may be of some relevance in the development of “late failure”.
The deterioration in arterial blood gas tensions was caused by significant clinical worsening, after the initial improvement, resulting from a new complication or a recurrence of one present at admission. Most of the complications (55% of total), either alone or together with one or more other complication, were infectious (pneumonia or exacerbation of COPD).
Ventilator associated pneumonia is an important clinical problem, the risk of which increases after the first three days of mechanical ventilation. It carries a high mortality rate.23 However, recent studies5 ,6 ,19 ,24 have shown that the probability of developing pneumonia is much lower in patients being ventilated non-invasively, so it has been suggested that the term “ventilator associated pneumonia” should be changed to “intubation associated pneumonia”.25 In reality, the incidence of pneumonia in our group of patients was relatively low (13%), especially compared with the higher rate described with intubation. Nevertheless, the possibility of developing a pulmonary infection such as pneumonia or COPD exacerbation in an ICU does not depend only on the presence of the endotracheal tube, but also, as descibed by Meduri et al,26 on the insertion of other catheters such as a Foley catheter or an intravenous line.
The second point to arise from our study concerns what treatment should be given when a patient with COPD, who initially responded to NIMV, suffers another episode of acute respiratory failure. Our data show that relapse has a high mortality rate (67.7%) which is significantly higher if the NIMV is maintained (91.6%) than if the patient is given invasive ventilation (52.6% mortality). Before discussing this point, it is important to note that the choice of ventilatory modality was not randomised but depended upon the wishes of the patients or their relatives, so that the results obtained must be interpreted with caution. Firstly, the patients treated with more aggressive NIMV were older than those who were intubated because age was an important factor for relatives when deciding clinical management. The worse response of this subgroup may therefore be related to this potential bias. However, it has been shown that elderly patients with COPD may respond as well as middle aged patients to NIMV.27 Secondly, the pH at the time of “late failure” in the group who continued treatment with NIMV was markedly lower than in the intubated patients (7.11 versus 7.29). Although this finding was not statistically significant, probably because of the small number of patients, it is in agreement with most of the published studies which show that NIMV is less likely to be successful in patients with acidosis. Another possible explanation is that NIMV may not be as efficient as invasive ventilation in treating a life threatening episode of acute respiratory failure when, for example, there is sensory impairment which is usually accompanied by a weak cough reflex. Pneumonia and pulmonary exacerbations (the main causes of “late NIMV failure”) require improved removal of secretions, and gas exchange may not improve if there is an accumulation of secretions.
The overall hospital mortality was 15.4% in our study which is within the range of values reported in the literature for NIMV (6–25%).28 The overall 90 day mortality was 21% compared with 25%22 and approximately 35%16observed in recent studies which included patients on invasive ventilation. Comparison of mortality rates between studies in this relatively short time period is difficult as the inclusion criteria, ventilation modalities, and standard treatment are often different.
In conclusion, our study shows that NIMV may be useful for avoiding intubation in patients with COPD during an episode of severe hypercapnic respiratory failure. After the initial success of NIMV, a significant subset of patients (>20%) may experience a new episode of acute respiratory failure resulting from the appearance of new complications or the recurrence of those present at the start of treatment so that more aggressive ventilatory treatment becomes necessary. These patients have a high mortality rate, especially if NIMV is continued and intubation avoided.