Article Text

Abstract
BACKGROUND There have been important changes in the organisation of care for patients with asthma since asthma deaths were studied in the 1980s by the British Thoracic Association (BTA), with greater emphasis on long term control of symptoms and the use of preventive therapy. Recent trends in routine statistics show a decline in population death rates.
METHODS A confidential review was undertaken of general practice and hospital records and interviews with general practitioners of patients dying in mainland Scotland between January 1994 and December 1996 with a principal diagnosis of asthma recorded by the Registrar General’s Office. Panel assessment of the cause of death was carried out and a number of possible adverse factors were identified. The data from the 15–64 year age group were compared with similar data from the earlier study by the BTA.
RESULTS Over the three year period 95 deaths of 235 studied (40%) were confirmed as being due to asthma. Taking account of different methods of case ascertainment used in the BTA and this study, a fall in the calculated rate of “deaths assessed as due to asthma” was found from 2.51 (95% CI 2.34 to 2.68) per 100 000 population in 1979 to 1.26 (95% CI 1.19 to 1.33) per 100 000 population in 1994–6. Fewer individual adverse factors were identified in clinical management, with appropriate routine management in 59% and management of the final attack satisfactory in 71%. Patient factors such as poor compliance, lack of peak expiratory flow (PEF) measurements, and overuse of reliever medication without inhaled corticosteroids, and psychosocial problems, notably depression, were confirmed as important contributing factors. Four of five patients under 16 years of age who died were found to have problems with routine management.
CONCLUSIONS This population based study documents important improvements in the standard of asthma care as well as a significant decline in the rate of deaths due to asthma over a period during which the organisation of care has changed and the chronic nature of the disease has been acknowledged. Strategies which might have a further impact include the greater use of PEF recordings, particularly during acute attacks, to document recovery, prescription monitoring of the underuse of inhaled corticosteroids, consideration of the use of combined preparations where persistent overuse of bronchodilators is occurring, and increased input for young patients whose routine management is proving difficult.
- asthma
- asthma death
- Scotland
Statistics from Altmetric.com
Study of asthma deaths began in the 1960s with the detailed review of an epidemic of deaths following the introduction of non-selective β agonist inhalers which were available without prescription for a period; that epidemic is usually attributed to those agents.1 ,2 In the late 1970s the then British Thoracic Association (BTA) surveyed deaths from asthma in two regions of England and found undertreatment to be common, with both doctors and patients underestimating the severity of the final attack.3 That study concluded that preventable factors had been identified in 79% of the deaths studied and may well have been the catalyst for the dramatic increase in interest in asthma management which has since taken place. Asthma is now recognised and treated as a chronic illness to which strategies of control of symptoms and prevention of acute attacks can be applied successfully. There has been an increase in general practitioner interest,4 and practice nurses have developed expertise in managing asthma with specialist training courses and qualifications.5 Increasing input to the care of asthma in general practice has been seen to be important, not only because of the high prevalence of asthma,6 which makes it one of the common chronic medical conditions in the UK, but also since most asthma deaths occur outside hospital.7 ,8
A regional inquiry into asthma deaths has been ongoing in East Anglia since 1988.7 ,9 It has recorded a lower proportion of deaths in which care was inappropriate (now based on the explicit recommendations of asthma management guidelines produced by the British Thoracic Society and others10 ,11) and has also identified an increasing contribution made by adverse psychological and social factors of the patients. This has also been reported by workers studying the epidemic of asthma deaths which occurred in New Zealand in the late 1980s12 and in Australia.13
We were interested not only in obtaining information on current practice, since the organisation of care for patients with asthma has changed, but also in evaluating the number of deaths assessed as being due to asthma, recognising that there has been a decline in the number of asthma deaths recorded by the Office of National Statistics.14 For logistical reasons we were obliged to identify deaths from coded data, whereas the earlier BTA study, with which we planned to compare our findings, had used death certificates as the source data. The accuracy of both death certification and of coding practice with regard to asthma have been studied and we would therefore be able to extrapolate from the literature to correct for these differences to arrive at comparable figures.
The accuracy of death certification has been studied by a number of authors. Wright et al 15reviewed asthma deaths in Northern Ireland. With clinical evidence, death certificates, and coded cause of death a false negative rate for death certification of 31% (in the 0–64 year age group) was found. A further study in south-east London of a cohort of asthmatic patients aged 16–64 years followed for three years following an admission with acute asthma identified 22 deaths due to asthma, 18 recorded as such and a further four with other diagnoses given on death certificates—a false negative rate for death certification due to asthma of 18%.16
The Office of Population and Censuses operates a number of rules for coding deaths from death certificate information and Wright’s study also calculated the false negative rate for coding death as due to asthma. Using clinical networks as well as official sources to identify deaths, information on patients was obtained from hospital notes and GP interviews; a false negative rate for coding death as due to asthma of 34% was found.
We therefore aimed to study both quantitative and qualitative aspects of deaths from asthma in a larger UK population, including older patients excluded from other studies, but with subgroup analysis of the 15–64 year age group in order to allow comparison with the 1979 BTA study.3
Methods
Deaths occurring in mainland Scotland coded as due to asthma (ICD-9 code 493, any suffix) were identified from week to week by the Registrar General’s Office from January 1994 to December 1996. Cases with a principal coded cause of death of asthma had their registered GP identified. They were contacted by letter by RS and subsequently by telephone by a local GP interviewer; if they agreed to participate, an appointment for interview was made. There were GP interviewers located in 10 geographical areas throughout Scotland.
For a pilot period cases with asthma coded as a subsidiary diagnosis had their registered GP identified and these were contacted by letter, inviting them to identify the cause of death and allow inclusion of the case if death had been due to asthma. Two cases from 174 contacts were generated by this strategy and neither of these was assessed by panels as a death due to asthma; this practice was therefore abandoned.
Attempts to obtain GP interviews were pursued until 30 June of the year following that in which the death occurred. Cases were considered time barred thereafter and excluded from the study.
At the GP interview a proforma of relevant questions was completed by the GP interviewer in the course of a semi-structured interview. If the GP consented, case notes were retained by the GP interviewer in case additional information was requested by the panel. There were a number of occasions when data were extracted from GP files by the interviewer without further GP contact, but with their consent. Attempts were made to involve other members of the primary health care team using the critical incident technique.17 ,18 This is a learning technique which encourages systematic review of a single experience to identify positive and negative factors so that these can influence future practice. Further details of this aspect of the study will be reported separately.
When the GP proforma was completed, RS obtained any hospital notes identified as relevant and details of regular follow up and recent hospital admissions were extracted from them by respiratory physicians on the regional panels or CEB. Details of post mortem findings, particularly cases referred to the procurator fiscal (coroner), were recorded on a separate proforma by RS. When all the available information was collated, this was sent to panel members in advance and formed the basis for panel judgments on a number of aspects of care. Additional data were culled from hospital records (by a respiratory physician) or GP notes (by the GP interviewer) during the panel meetings as needed.
The panel assessment was returned to the patient’s GP unless specifically requested otherwise. Where an adverse assessment of hospital care was made, with implications which might affect other patients, this was fed back to the hospital consultant responsible for the patient. When all relevant parties had received feedback on the case the database was anonymised.
Regional panels consisted of two local respiratory physicians and three GPs, with a quorum of three to include at least one GP and one respiratory consultant; GP interviewers attended whenever this was feasible. There was some movement of panel members among panels in order to ensure that similar judgments were being made and, at an early stage of the study, an assessor from previously undertaken studies (Dr David Stableforth) attended to advise. Four regions were identified for the purposes of the study—East, West, Central and Northern Scotland.
Consent for the study was obtained from all relevant area medical or clinical audit committees and from the Glasgow local medical committee whose findings were made known in subsequent submissions to the audit committees elsewhere. Lothian Health Board ethics committee also approved the study. Where hospital case notes were requested, consent for their perusal was sought from the consultant in charge where this could be identified, or from the hospital’s medical director.
Descriptive data are recorded as numbers with percentages as appropriate. Where there are missing data the denominator is recorded explicitly. The deprivation category was described using the Carstairs coding method for Scotland.19 Comparisons between groups were made using χ2 tests for categorical data and non-parametric tests were used for numerical results (Mann-Whitney and Moods median test, which is particularly robust against outliers).
The rate of deaths assessed as due to asthma was calculated by first applying the appropriate false negative rate for recording death as due to asthma for the BTA study, in which deaths were identified from death certificates, and for coding death as due to asthma for the current study (SCIAD), in which deaths were identified from coded data. A further correction was applied to the SCIAD figures to correct for the cases not reviewed, there being no such cases in the BTA study. The appropriate population figures were then applied to derive annual rates per 100 000 population.
Results
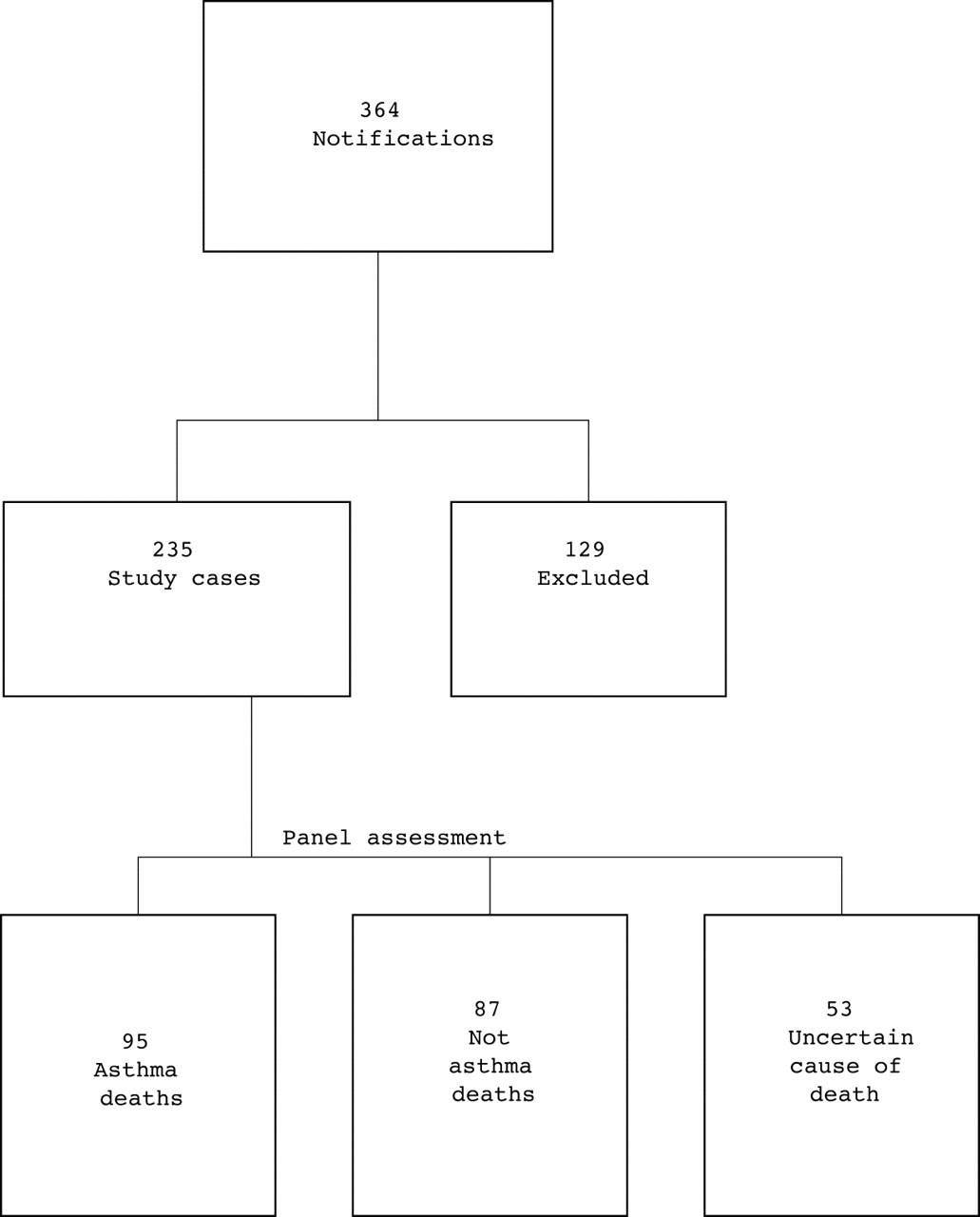
Three hundred and sixty four patients with a principal coded cause of death from asthma were identified during the period from January 1994 to December 1996, 235 of which were included in the study. Figure1 outlines the cases identified and those included and excluded. Among those excluded were 21 cases where no alternative cause of death was proposed although the GP was confident that death had not been due to symptoms compatible with acute severe asthma. GPs often expressed surprise that the case they had certified as dying from causes described below had been coded as a death principally due to asthma.

{kind=link}
Study population 1 January 1994 to 31 December 1996.
Of the 129 exclusions, 74 were excluded because an alternative cause of death was obtained from the GP, in 15 cases we were unable to obtain GP involvement, 33 were time barred, and seven had moved out of the area or their data were uncollectable. The alternative causes of death given by their GPs for 74 patients included chronic obstructive pulmonary disease or respiratory failure (n = 15), cardiac failure or ischaemic heart disease (n = 12), cerebrovascular accident or other long term neurological condition (n = 7), pneumonia (n = 7), malignancy (n = 4), pulmonary embolism (n = 2), other specified acute condition (n = 6), and unspecified (n = 21).
DEATHS ATTRIBUTABLE TO ASTHMA
There were 95 deaths attributable to asthma; the demographic and descriptive clinical details are given in table 1. Seventy four patients had peak expiratory flow (PEF) recordings in their GP case notes, a further 10 had hospital PEF records only, eight had no evidence of these at all, and for three this information was not available. Of the 18 with no GP PEF records, 13 were regarded by their GP as having severe asthma. Of the 74 with GP PEF records, 54 had further information on the timing of the most recent record; 16 (30%) had none within a year of death and only nine (17%) had one within four weeks of death. There were insufficient data to comment on the degree of diurnal variability of PEF.
Clinical details of 95 deaths attibuted to asthma by panel review
ASTHMA DEATHS: PANELS’ ASSESSMENTS OF MANAGEMENT
The proportion of cases assessed as due to asthma by the four regional panels is shown in table 2. Of the 95 deaths attributable to asthma, two were due to well recognised drug contraindications—the administration of a β blocker and of diclofenac in a patient previously known to be sensitive to mefenamic acid.
Population data for four regions of Scotland: study cases and asthma deaths
Background asthma control was poor in 50 cases (53%); routine management of 56 cases (59%) was judged appropriate. Of the 33 cases categorised as having inappropriate routine management, 17 were also included in the category of those whose prescribed therapy was judged inappropriate (see below). Poor compliance, lack of follow up (“too much left to the patient’s own discretion”), both excessive repeat prescribing of bronchodilators and failure to recognise that prescriptions were not being requested, frequent use of oral corticosteroids in the face of inadequate inhaled steroid therapy, and lack of objective measurement of air flow obstruction were the common themes. Cultural/communication difficulties were only identified in a single case although there were a number of other examples of the system failing patients—for example, an attack of acute asthma occurring in prison, no follow up after hospital discharge, failure to continue oral corticosteroids after the hospital discharge of a patient previously on long term corticosteroids.
The panels assessed the use of recent oral corticosteroids as appropriate in 56 cases (59%) and the use of inhaled corticosteroids was considered appropriate in 50 cases (53%). Among the 46 cases in whom inhaled corticosteroid use was judged inappropriate there were 23 cases where insufficient doses had been prescribed and 23 where the prescribing was appropriate but there was evidence that the treatment had not been taken by the patient. Taking account of the use of oral and inhaled corticosteroids and other therapy, the panels judged drug treatment to be inappropriate in 23 cases (24%). Poor compliance was a major factor; eight of these patients were definitely not prescribed any inhaled corticosteroids and, from other comments made by the panels, an additional seven were either known or strongly suspected to be poorly compliant (as judged by uptake of inhaled corticosteroid prescriptions).
Of the five deaths in patients under 16 years of age, four were identified as having problems with routine management. Poor compliance was again noted in four of these cases and, although in two cases the fatal attack was of sudden onset, this may have been related to poor symptom control and undertreatment. In the fifth case both GP and hospital management was assessed as inappropriate in terms of treatment given and lack of follow up or agreement on a self-management plan.
The management of the final attack was judged to have been appropriate in 47 of 66 cases (71%). Of the 19 cases whose final management was deemed inappropriate the panels commented most often on the lack of assessment and, presumably, of appreciation of the severity of the episode by both patients and professionals.
There was a delay in obtaining help in 19 of 83 cases (23%), most often due to patients delaying in calling for help, but this included two cases where ambulances were slow to arrive and one case where there were also delays by nursing, medical, and prison staff.
PSYCHOLOGICAL AND SOCIAL FACTORS
Specific questions were asked of GPs about possible risk factors for asthma deaths identified previously. These findings are shown in table 3. GPs assessed their patients’ responses to the fatal episode as being appropriate in 30 of 52 cases (58%); where there was enough information available to make an assessment of the response of relatives, GPs assessed this as appropriate in 19 of 24 cases (79%).
GP assessment of psychosocial factors in 95 asthma deaths
ANALYSIS OF DEATH RATES IN THE 15–64 YEAR AGE GROUP: COMPARISON WITH BTA STUDY IN 1979
In the current study 65 deaths out of 105 coded as due to asthma in the age group 15–64 which were investigated were attributed to asthma (62%). Forty six further cases also coded as due to asthma were not investigated, although often because the GP felt that death had been due to some other condition which had often been recorded as the main cause of death on the death certificate. Nevertheless, applying the same proportion (62%) to this number gives a further 29 deaths, a total of 94, in this age group. If the false negative rate for coding death as due to asthma from Wright15 of 34.2% (95% CI 26.6 to 41.9) is now applied, an extra 32 (95% CI 25 to 39) deaths may have occurred, giving a derived number of deaths due to asthma in the 15–64 year age group of 126 (95% CI 119 to 133) during a three year period. The population aged 15–64 from which deaths included in SCIAD were identified was 3 337 841, giving an annual rate of 1.26 (95% CI 1.19 to 1.33) per 105 population.
In 1979 the BTA3 identified 90 deaths due to asthma in a population of 4.89 million aged between 15 and 64 years during a single year. There is no need for any correction for cases not evaluated as this did not occur. Combining the information on false negative recordings of death due to asthma from Wright15 and Guite16 gives a false negative rate of 36.3% (95% CI 26.9 to 45.6). Applying this rate gives a total of 123 (95% CI 114.2 to 131.0) deaths in the BTA study in a single year and a calculated annual rate of 2.51 (95% CI 1.89 to 2.45) per 105 population.
Discussion
This is one of the largest studies of deaths coded as due to asthma, notably including all age groups. It provides an important update on the management of asthma in the UK and, since it was conducted in a similar manner, the findings on the subgroup of patients aged 15–64 years can be compared with the 1979 cohort studied by the BTA.3 The main differences in the current study are the use of several panels in assessing cases, in view of the larger numbers and geography, the inclusion of a majority of GPs on the assessment panels, and the identification of cases from coded cause of death rather than from the death certificates themselves.
Quality control of panel assessments was limited to the interchange of members at the beginning of the study, including one of the assessors from the original BTA study. It is therefore reassuring that the proportion of deaths judged due to asthma was similar in three of the four regions (table 2). We believe that lack of information rather than any difference in panel assessments was the more likely reason for the observed difference in one region where one third of cases were found to have insufficient data to reach a conclusion on the cause of death. The greater involvement of GPs in the panel assessments was deemed to be appropriate with the change in emphasis in asthma management where long term management in primary care, often by interested practitioners, is the norm. We have no information on any difference this may have made to the review process but accept that each study used the appropriate panel for the then current circumstances.
The different method of case ascertainment was due to the impossibility of reviewing all death certificates within the Registrar General’s Office (RGO) without disrupting their operations; coded cause of death derived from death certificates by RGO staff using ICD and a series of agreed coding rules14 was therefore our starting point. These coding rules probably account for the majority of the 74 cases where GPs were confident that patients had died of other causes, often having noted asthma only as a subsidiary diagnosis on the death certificate.
Without independent review of case notes and other evidence relating to patients who were excluded because their GP considered death was not due to asthma, it is difficult to draw any firm conclusions about these cases. The format of inviting GP feedback on the cause of death and not pursuing cases which they deemed inappropriate was necessary in order to secure as many interviews as possible. Most concern centres on the 48 cases where GP cooperation was not obtained, although this was often by omission with only 15 cases (over three years) where active non-cooperation was encountered; this group may have included a greater proportion of cases with adverse management factors, raising the possibility that the current study overestimates the improvement in practice. Seventy five of 122 cases excluded were over 65 years of age so that the comparison with the BTA study is relatively protected from any bias introduced by this. A similar proportion of deaths in the comparable age group in the current study were attributed to asthma as in the BTA study.3 Furthermore, the large number of cases studied (235), which constitutes a 65% sample of all cases with asthma coded as the principal cause of death over a three year period, has sufficient similarity to the Scottish population figures, both in terms of age and deprivation spread (data not shown), to be considered representative.
We may have missed obtaining relevant information because we were not able to interview patients’ relatives. Nevertheless, the findings largely agree with those of the East Anglia study9 in which it was also deemed inappropriate to interview some relatives.
We have observed a fall in the rate of deaths assessed as due to asthma between 1979 and 1994–6, arguably the closest rate to a gold standard asthma death rate as possible. The two studies from which the data are derived were conducted in a similar manner except that deaths were identified differently for logistical reasons. We have allowed for this difference by correcting each figure for the appropriate false negative rate (for death certification and coding of death as due to asthma) derived from the existing literature. There are no sequential studies of false negative rates. Results from studies carried out in the 1990s have therefore been applied to the BTA study performed in the late 1970s. It is impossible to comment on any error introduced by this. Since the studies from which these were derived involved only small numbers, the 95% confidence intervals for the false negative rates and the derived population rates are also calculated. A statistically significant difference is shown.
The comparison of death rates “assessed as due to asthma” relates to the 15–64 year age group in two regions of England in 1979 and the entire Scottish mainland in 1994–6. There was no difference in the age and sex structure of the population in the 15–64 year age bands in these two regions of England and Scotland in the relevant time periods (data not shown). There is therefore no merit in converting the figures to standardised mortality ratios (SMRs) which would correct for differences in population structure but would also make future comparisons more difficult.
Possible causes for this observed difference are regional differences in asthma death rates or a secular trend. Review of regional death rates for asthma shows that the SMR for Scotland lay mid way between the regional SMRs for the two English regions at the time of the BTA study and a significantly lower SMR in the 45–84 year age group at the time of the current study in Scotland (tables 4 and 5 which summarise data from references 14 and 20).
Regional SMRs for asthma, 1974–8, at the time of the BTA study20
Regional SMRs (95% CI) for asthma, 1991–5, at the time of the current study14
The small but significant difference in the (only partly overlapping) 45–84 year age group is insufficient to explain the large difference in the death rates calculated here. Another observation which suggests that the populations were similar is that similar proportions of reviewed cases were attributed to asthma (90 of 153 cases (59%) in the BTA study and 62% of SCIAD cases). The observed difference in rates can therefore reasonably be attributed to the passage of time and events associated with this. This decline is doubly significant in the face of the increasing prevalence of asthma.21
Turning to the qualitative aspects of the study, the identification of problems with the routine management of four of the five deaths occurring in patients under 16 years of age is important and disturbing; the management of teenagers with asthma is recognised to present particular problems22 and this study confirms the implications of failure.
Comparison with the BTA study shows that smaller numbers of individual adverse factors are identified (table 6). Although patients in different regions have been studied (West Midlands and Mersey in 1979, Scottish mainland in 1994–6), there is no reason to believe that systematic differences in the process of care exist. Routine management and management of the final attack were appropriate in two thirds of cases in 1994–6 and 28% of cases had no adverse management factors identified compared with 21% “with no preventable factors” in the BTA study.3 Medical management of asthma has altered considerably over the past 15 years and the findings of this study reflect this improvement, although it has been shown that adverse factors are more likely to be identified by retrospective review of cases where there is a bad outcome.23
Comparison of BTA (1979) and SCIAD (1994–6) asthma deaths including subgroup of SCIAD cases in same age range as BTA study
The findings of the current study still allow room for much improvement. In particular, further emphasis on objective measurements of PEF in order to improve the recognition both of acute severe asthma and chronic poor asthma control might encourage more intensive and appropriate management to optimise lung function and quality of life.
With the decline in the number of adverse factors associated with clinical management, patient related factors assume greater significance. Adverse psychological and social factors were identified in 58% of deaths attributed to asthma. This makes such factors a more common occurrence here than in the New Zealand study,12also based on case notes, in which there was a maximum incidence of adverse psychosocial factors of 17 of 44 deaths (39%). Such factors were identified more commonly in the East Anglia cohort (27 of 34, 79%) where the additional information from interviews with relatives may have been significant.7 There was no excess of adverse psychosocial factors in the deaths attributed to asthma in the our study compared with other cases investigated. Depression and denial of symptoms or of the need for treatment were the commonest factors. Depression has been identified by others as a risk factor24 and, although denial of symptoms and the need for treatment has been argued to be a useful psychological strategy, both extremes of denial and overdependence are associated with greater hospital utilisation rates.25 With only retrospective judgments of compliance, albeit based on prescribing information where possible, it was not possible to comment on any association between poor compliance and depression, although this has been observed by others.26 A case control study of psychosocial factors is currently in the planning stages and should give more definitive information on the relevance of these factors in the UK. Meanwhile, identifying and treating patients with depression should be emphasised as important.
Although always difficult to identify, poor compliance—or, perhaps more correctly stated, inadequate agreement between doctor and patient on the need for treatment—is confirmed as a common issue. Information on poor compliance was based wherever possible on evidence from prescription monitoring. Several GPs commented on the need to be able to identify poor compliance with inhaled corticosteroids which often occurred in tandem with the collection of large numbers of prescriptions for inhaled bronchodilators. Software for this is available for use with G-Pass, the repeat prescribing system in most common use in Scotland, and could usefully be developed for other systems. Perhaps the combination of suspected poor compliance and overuse of β agonists should trigger patient review; this may be a situation where a combined preparation (inhaled corticosteroid and short acting β agonist) has advantages, although study of stable patients has shown no benefit.27
The lack of objective measurements is an issue for both patients and professionals. With the increasing emphasis on self-management, patients’ own responsibilities to know how good (or bad) their asthma is and not to delay in seeking help need to be clearly laid out. Several comments were made on the usefulness of written self-management plans which might have included specific levels of PEF at which the patient should seek help. The more regular recording of PEF in the surgery would serve both to emphasise the importance of this measurement to patients and also provide written evidence of previous variability and absolute levels on which to base management plans.
In summary, this study shows good evidence of improving asthma care in a UK population, both in terms of numbers of deaths and quality of care, and identifies a number of strategies which might have a further impact; these include the greater use of PEF measurement by patients and professionals, greater emphasis on the involvement of patients in their own care, and for patients’ responses to their illness and its treatment to be taken into consideration.
Acknowledgments
We gratefully acknowledge the time given up by participating GPs, the efforts of hospital staff, especially medical records officers, in obtaining case notes for review, as well as the work of GP interviewers and panel members and the support of Drs Brian Harrison and David Stableforth in setting up the study. The National Asthma Campaign and Clinical Resource and Audit Group, Scottish Office provided the majority of the funding, with smaller contributions from Glaxo Wellcome, Boehringer, and the Astra Foundation. We also thank anonymous reviewers for their detailed comments.
SCIAD collaborators in addition to the authors:
GP interviewers: A Buchan, C Burton, C Campbell, K Cassidy, G Crosby, A Crowe, D Gemmell, A P Lees, P Manson, R Macrae, F McGregor, A J McIntyre, J Robson, I Russell, P Scanlan, M J Somerville.
Panel members: C Brown, R Clark, D Dobbie, J Elliot, J Friend, J Gaddie, J M Herbert, G Hulks, J C Laird, G Leitch, J R M Lough, M J Macrae, G E McIntosh, T N McLeod, A Melville, K M Onorie, R D Stevenson, K F Whyte.