Article Text

Abstract
Background The assessment of treatment response in idiopathic pulmonary fibrosis (IPF) is complicated by the variable clinical course. We examined the variability in the rate of disease progression and evaluated the effect of continued treatment with pirfenidone in patients who experienced meaningful progression during treatment.
Methods The source population included patients enrolled in the ASCEND and CAPACITY trials (N=1247). Pearson's correlation coefficients were used to characterise the relationship between changes in FVC during consecutive 6-month intervals in the placebo population. Outcomes following a ≥10% decline in FVC were evaluated by comparing the proportion of patients in the pirfenidone and placebo groups who experienced a ≥10% decline in FVC or death during the subsequent 6 months.
Results A weak negative correlation was observed between FVC changes during consecutive intervals in the placebo population (coefficient, −0.146, p<0.001), indicating substantial variability. Thirty-four (5.5%) and 68 (10.9%) patients in the pirfenidone and placebo groups, respectively, experienced a ≥10% decline in FVC by month 6. During the subsequent 6 months, fewer patients in the pirfenidone group compared with placebo experienced a ≥10% decline in FVC or death (5.9% vs 27.9%; relative difference, 78.9%). There was one (2.9%) death in the pirfenidone group and 14 (20.6%) deaths in the placebo group (relative difference, 85.7%).
Conclusions Longitudinal FVC data from patients with IPF showed substantial intrasubject variability, underscoring the inability to reliably assess therapeutic response using serial FVC trends. In patients who progressed during treatment, continued treatment with pirfenidone resulted in a lower risk of subsequent FVC decline or death.
Trial registration numbers NCT01366209, NCT00287729, NCT00287716.
- Idiopathic pulmonary fibrosis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is the key question?
To further inform clinical decisions regarding the assessment and management of patients with idiopathic pulmonary fibrosis, we sought to characterise the variability in the rate of disease progression and evaluate the effect of continued treatment with pirfenidone in patients who experience meaningful progression during treatment.
What is the bottom line?
In patients with idiopathic pulmonary fibrosis who experienced a ≥10% absolute decline in FVC during the first 6 months of treatment, continued treatment with pirfenidone reduced the risk of a second ≥10% decline in FVC or death compared with placebo.
Why read on?
Our findings provide the first available evidence to suggest that continued treatment with pirfenidone may confer a benefit to patients with idiopathic pulmonary fibrosis who exhibit evidence of meaningful disease progression during treatment.
Introduction
The recent regulatory approval of pirfenidone and nintedanib marked an important milestone in the decades long search for a safe and effective treatment for idiopathic pulmonary fibrosis (IPF)—a chronic, irreversible and almost uniformly fatal lung disease characterised by worsening dyspnoea and progressive pulmonary insufficiency.1 While the emergence of proven therapeutic options for patients with IPF is a welcome development, clinicians will now be confronted with a series of practical issues for which there are no available data to guide clinical decision making. Chief among these are the assessment of therapeutic response in the individual patient and the management of patients who experience meaningful progression of disease despite therapeutic intervention.
The clinical efficacy and safety of pirfenidone and nintedanib in patients with IPF were demonstrated in three and two multinational phase 3 trials, respectively.2–4 The primary clinical efficacy end point in each of these trials was the change from baseline in forced vital capacity (FVC), a widely used test that has been shown to be a reliable, valid and responsive measure of disease status and an independent predictor of mortality in patients with IPF.5–11 However, while the favourable test performance characteristics of FVC make it a suitable end point for randomised controlled trials, considerable intersubject and intrasubject variability may be observed in the rate of FVC decline in patients with IPF.1 ,12 As a result, the clinical assessment of disease progression and therapeutic response in an individual patient represents a distinct challenge.
In the present exploratory analysis, we sought to characterise the variability in the rate of disease progression in IPF by comparing the change in FVC during two consecutive 6-month intervals in the pooled placebo population from the phase 3 multinational trials evaluating pirfenidone. To further inform the management of patients who experience meaningful progression during treatment, we then performed a post hoc exploratory analysis of outcomes following 6 months of continued treatment with pirfenidone or placebo in patients who experienced a ≥10% decline in FVC during the first 6 months of treatment in the phase 3 trials.
Methods
Patients
The source population included all patients randomised to treatment with pirfenidone 2403 mg/day or placebo in the CAPACITY or ASCEND studies. Eligibility criteria for these studies have been described elsewhere.2 ,3 For assessments of FVC variability, the analysis population included all patients randomised to placebo in CAPACITY or ASCEND. Treatment outcomes following a clinically meaningful decline in FVC were evaluated in the pooled pirfenidone 2403 mg/day and placebo populations from the CAPACITY and ASCEND studies.
Study design
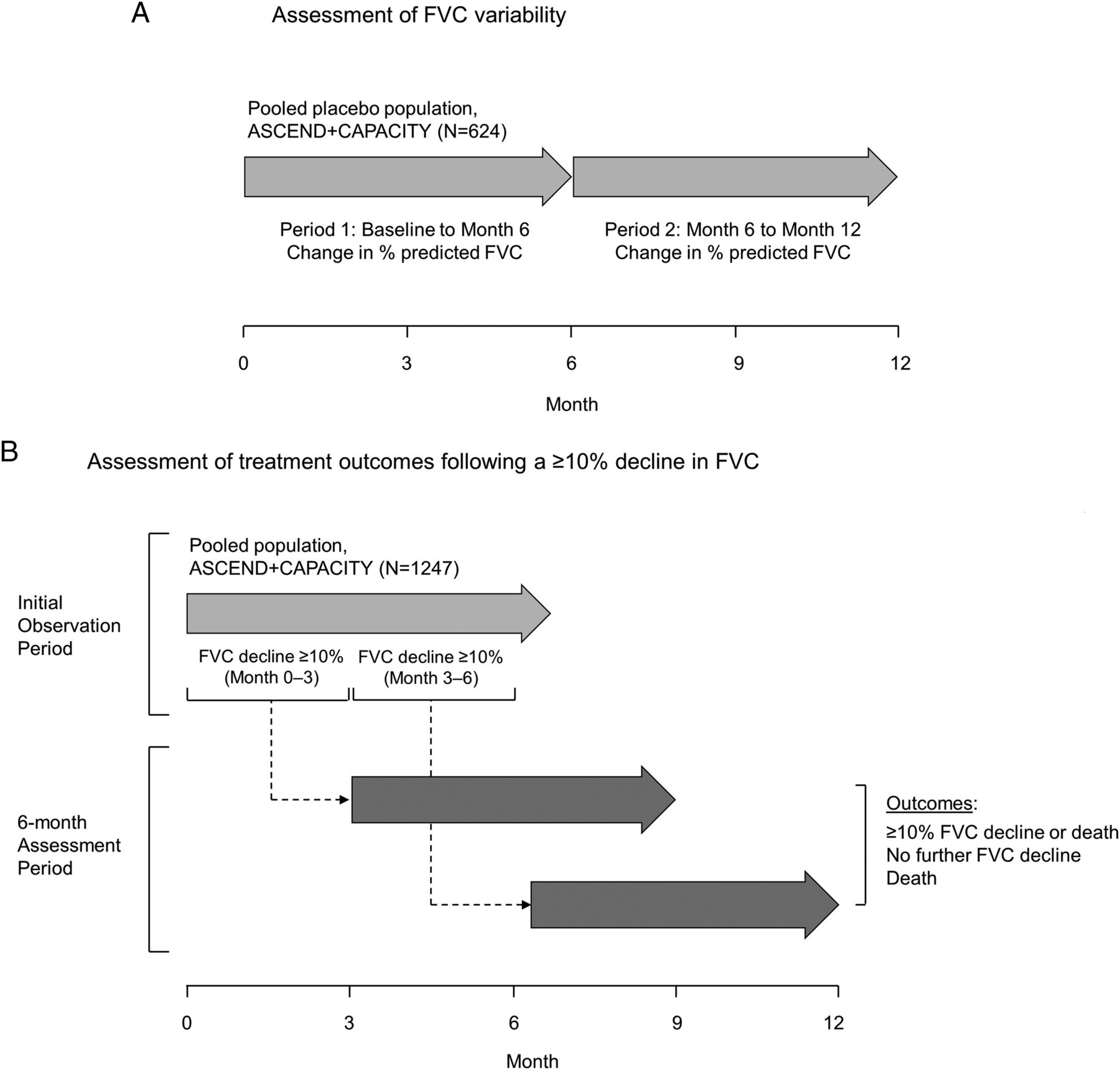
Figure 1 depicts the study design for the two components of the study. To characterise the variability in the rate of disease progression, the change in per cent predicted FVC (%FVC) from baseline to month 6 was compared with the change from month 6 to month 12 in the pooled placebo population from the CAPACITY and ASCEND studies. To examine the effect of continued treatment following a clinically meaningful decline in FVC, all patients in the pooled pirfenidone 2403 mg/day and placebo groups from the CAPACITY and ASCEND studies who experienced a ≥10% absolute decline in %FVC during the initial observation period were selected for inclusion in the analysis of outcomes during the subsequent 6-month assessment period. For patients who experienced an initial ≥10% decline in %FVC by the month 3 study visit, subsequent outcomes were assessed between the month 3 and month 9 study visits; for those who experienced an initial decline between the month 3 and month 6 study visits, subsequent outcomes were assessed between the month 6 and month 12 study visits.

Study profile. (A) Assessment of FVC variability. (B) Assessment of treatment outcomes following a ≥10% absolute decline in FVC.
In each of the trials included in the analyses, eligible patients were randomised to treatment with oral pirfenidone 2403 mg/day or placebo. Study drug was administered in three equally divided daily doses for either 1 year (ASCEND) or a minimum of 72 weeks (CAPACITY). Clinical efficacy outcomes were measured at baseline and at 3-month intervals in each trial. Spirometry was performed in accordance with standard American Thoracic Society (ATS) guidelines in all three studies; results were reviewed centrally in the ASCEND and locally in the CAPACITY studies.
Statistical analysis
For assessments of FVC variability, categorical shift analysis and Pearson's correlation coefficients were used to characterise the relationship between longitudinal changes in %FVC during two consecutive 6-month intervals in the pooled placebo population. For the latter, the strength of the relationship was designated according to Cohen's criteria as follows: >0.5, large; 0.5–0.3, moderate; 0.3–0.1, small; and <0.1, trivial.13 To further assess the relationship between changes in %FVC in the first and second 6-month intervals, a weighted κ coefficient was calculated for the following categories of change: stable or improved, 0% to <5% decline, ≥5% to <10% decline and ≥10% decline. Spaghetti plots of the change in %FVC from baseline to 1 year were also constructed for a randomly selected sample of 50 patients from the pooled placebo population from the CAPACITY and ASCEND studies. The random sample was generated using SAS software, V.9.2 (SAS Institute).
The stability of two temporally proximate measures of FVC was assessed using Pearson's correlation coefficients for the two assessments of %FVC performed on separate days as part of the final study visit (week 52A and week 52B in the ASCEND study and week 72A and week 72B in the CAPACITY studies). The strength of the relationship was designated according to Cohen's criteria as noted.
Treatment outcomes following a clinically meaningful decline in FVC were evaluated in patients from the pooled pirfenidone and placebo populations who experienced a ≥10% absolute decline in %FVC by the month 3 or month 6 study visits. The primary analysis compared the proportion of patients in each treatment group who experienced any of the following during the subsequent 6 months: (1) ≥10% absolute decline in %FVC or death; (2) no further decline in %FVC; or (3) death. To minimise bias, patients who discontinued study treatment were included in the analysis. Absolute change in %FVC during the first 3 months or 6 months was based on observed data only. For the subsequent 6-month assessment period, missing %FVC values due to death were assigned to the worst category for the categorical analysis and replaced with the worst possible value (%FVC=0) for measures of central tendency. Missing values due to reasons other than death were replaced with the average value from the three patients with the least sum of squared differences (SSD) across study visits. Categorical differences between treatment groups were evaluated using a two-sided Fisher's exact test.
The change in %FVC during the 6-month period following an initial decline was also evaluated in the pooled pirfenidone and placebo groups using a rank analysis of covariance model. Missing values due to death were assigned the worst ranks according to time of death and missing values due to reasons other than death were imputed using the SSD methodology. Data are presented as median (range) values.
An on-treatment analysis evaluated outcomes in the subset of patients who remained on study treatment during the 6-month period following an initial ≥10% absolute decline in %FVC. Patients were considered to have remained on treatment if they had not discontinued treatment before the end of the second 6-month observation period. Patients with missing data due to death were considered to have remained on treatment if the last dose of study drug was within 28 days of death.
FVC and mortality outcomes following hospitalisation were evaluated in patients in the pooled pirfenidone and placebo groups who were hospitalised due to any cause within the first 6 months of study treatment. Outcomes were assessed during the 6-month period beginning with the first scheduled study visit following the date of hospitalisation.
Results
A total of 1247 patients met the criteria for enrolment in the CAPACITY or ASCEND studies and were assigned to treatment with pirfenidone 2403 mg/day (N=623) or placebo (N=624). Demographics and baseline characteristics for the pooled pirfenidone and placebo groups are summarised in online supplementary table S1.
Supplemental material
FVC change in the placebo population
Categorical shift analysis of change in %FVC during two consecutive 6-month intervals in the pooled placebo group showed marked variability in the magnitude of change during the first and second observation periods (table 1; see online supplementary figure S1). A total of 59 (9.5%) patients experienced a ≥10% decline in FVC between baseline and month 6; of these, 16 (27.1%) had stable or improved FVC values during the subsequent 6 months. Conversely, of the 162 (26.0%) patients who had stable or improved FVC values between baseline and month 6, 121 (74.7%) experienced a decline in FVC during the subsequent 6 months, including 19 (11.7%) patients who experienced a ≥10% decline. Shift analysis of absolute change in %FVC oneline using 5% categorical thresholds, as well as relative (rather than absolute) change in %FVC showed similar variability (see online supplementary tables S2 and S3, respectively).
Categorical shift analysis of absolute change in per cent predicted FVC during two consecutive 6-month intervals in the pooled placebo population
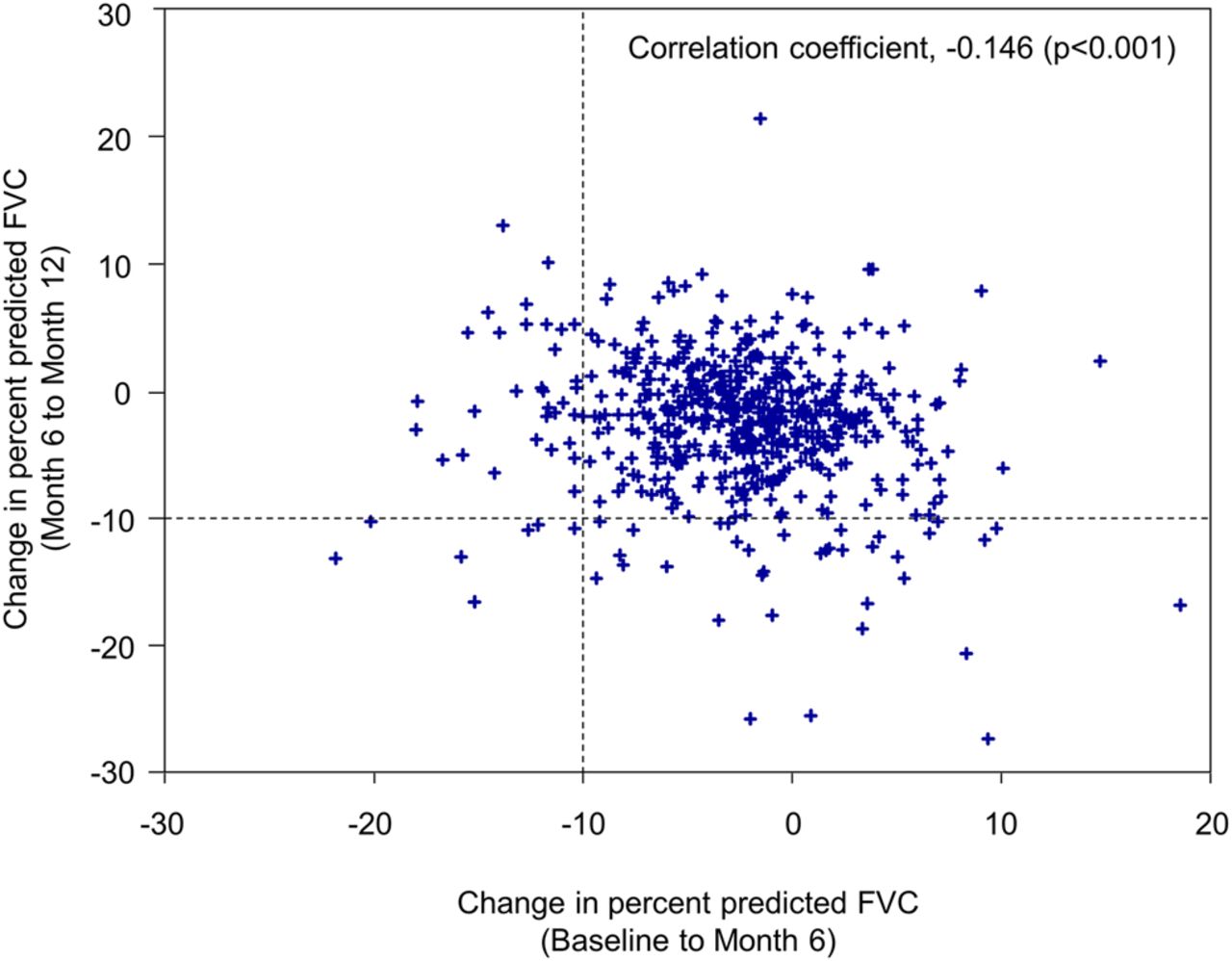
A weak negative correlation was observed between changes in %FVC during two consecutive 6-month intervals (correlation coefficient, −0.146, p<0.001; figure 2), indicating substantial variability in both the magnitude and direction of change. Additionally, FVC change during the first interval was not predictive of change during the second interval (weighted κ coefficient, −0.024; 95% CI −0.084 to 0.037). A sensitivity analysis using relative (rather than absolute) change in %FVC yielded similar results (Pearson's correlation coefficient, 0.034, p=0.426; weighted κ coefficient, −0.039; 95% CI −0.101 to 0.023).

Relationship between changes in per cent predicted FVC during two consecutive 6-month intervals*. *Pooled placebo population, CAPACITY and ASCEND studies (N=540).
The spaghetti plot depicted in figure 3 shows the change in %FVC from baseline to 1 year in a randomly selected sample of 50 patients from the pooled placebo population. While the general trend was characterised by a marginal overall decline in lung volume, there was substantial intersubject and intrasubject variability in both the magnitude and direction of change.

Spaghetti plot of change from baseline to 1 year in per cent predicted FVC*. *Randomly selected patients from the pooled placebo population from the CAPACITY and ASCEND studies (N=50).
Treatment outcomes following evidence of disease progression
A total of 34 (5.5%) and 68 (10.9%) patients in the pooled pirfenidone and placebo groups, respectively, experienced a ≥10% absolute decline in %FVC between baseline and month 6 (relative difference, 49.5%; p<0.001). The initial decline occurred by month 3 in 14 (2.2%) patients in the pirfenidone group and 24 (3.8%) patients in the placebo group, and between month 3 and month 6 in 20 (3.2%) and 44 (7.1%) patients in the pirfenidone and placebo groups, respectively.
Analysis of outcomes during the subsequent 6-month period showed that fewer patients in the pirfenidone group compared with placebo experienced a second ≥10% decline in %FVC or death (2/34 (5.9%) in the pirfenidone group vs 19/68 (27.9%) in the placebo group; relative difference, −78.9%; p=0.009), and more patients in the pirfenidone group compared with placebo had no further decline in %FVC (20/34 (58.8%) vs 26/68 (38.2%); relative difference, 53.8%; p=0.059; table 2). There was 1 death among 34 patients (2.9%) in the pirfenidone group and 14 deaths among 68 patients (20.6%) in the placebo group (relative difference, −85.7%; p=0.018). Similar results were observed among patients who experienced an initial FVC decline by month 3 compared with those who experienced an initial decline between month 3 and month 6 (see online supplementary tables S4 and S5). Additionally, sensitivity analyses using alternative methods for handling missing data showed a consistent treatment effect across analyses (see online supplementary tables S6 and S7), as did the analysis of outcomes using relative (rather than absolute) change in %FVC (see online supplementary table S8).
Outcomes after 6 months of continued treatment following an initial decline in per cent predicted FVC ≥10%*
The on-treatment analysis also yielded similar findings (see online supplementary table S9). A total of 24/34 (70.6%) and 60/68 (88.2%) patients in the pirfenidone and placebo groups, respectively, remained on treatment during the 6-month period following an initial ≥10% decline in %FVC. Of these, 1 (4.2%) patient in the pirfenidone group and 15 (25.0%) patients in the placebo group experienced a second ≥10% decline in %FVC or death (relative difference, −83.3%; p=0.032). No further decline in %FVC was observed in 14 (58.3%) patients in the pirfenidone group compared with 22 (36.7%) patients in the placebo group (relative difference, 59.1%; p=0.089). There were no deaths in the pirfenidone group and 10 (16.7%) deaths in the placebo group during the 6 months following the initial decline in FVC (relative difference, −100%; p=0.056).
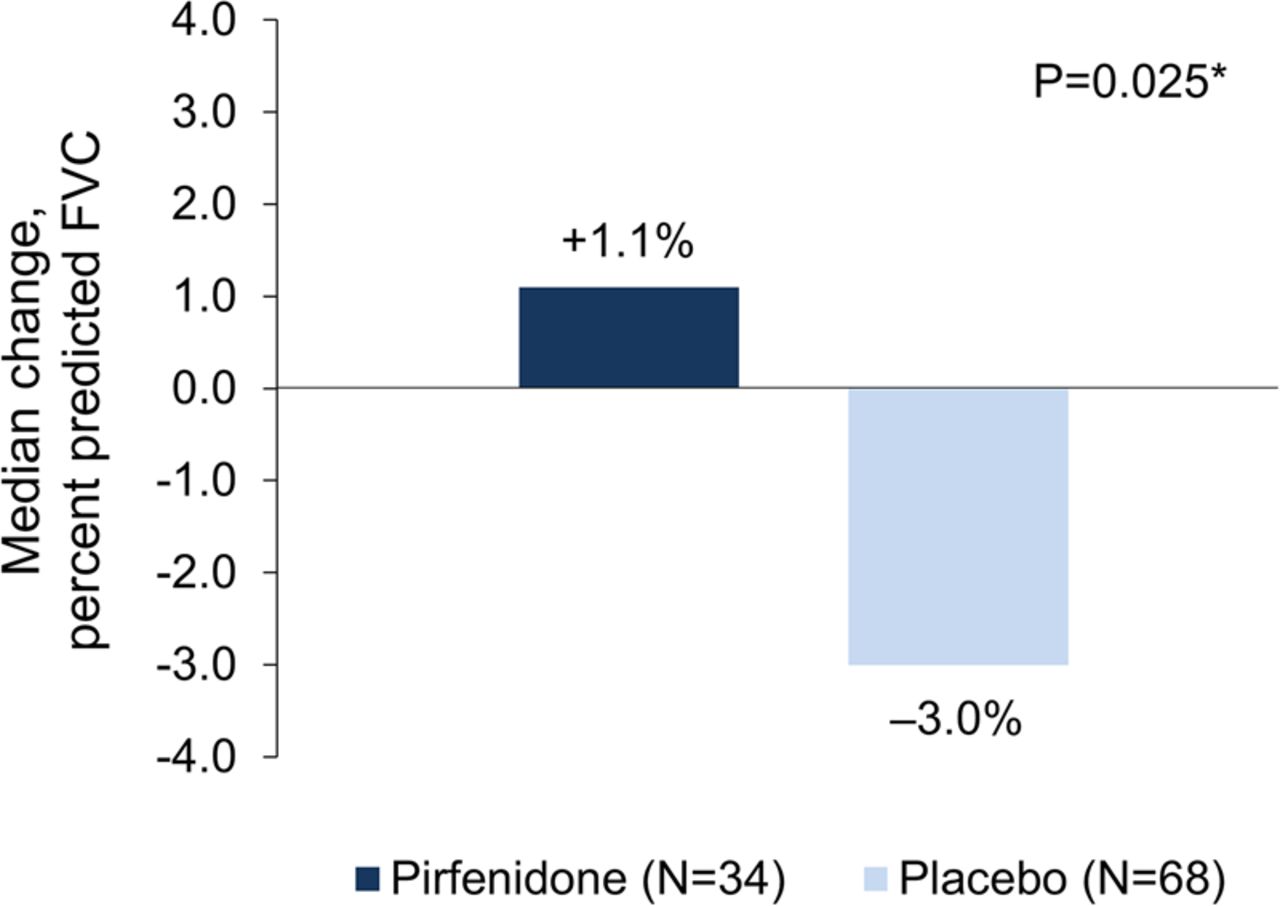
The median change in %FVC during the 6-month period following an initial ≥10% decline was 1.1% (range, −84.6, 16.2) in the pirfenidone group and −3.0% (range, −67.3, 13.0) in the placebo group (p=0.025; figure 4). In the on-treatment analysis, the median change in %FVC was 2.1% (range, −10.6, 16.2) and −3.0% (range, −59.1, 13.0) in the pirfenidone and placebo groups, respectively (p=0.154).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Median change in per cent predicted FVC during the 6-month period following an initial decline in FVC ≥10%. *Rank analysis of covariance with ranked change from baseline as the outcome variable; study, treatment, and region as fixed effects; and ranked baseline FVC as a covariate. Deaths are ranked worst according to time until death.
Treatment outcomes following hospitalisation
A total of 44 (7.1%) and 49 (7.9%) patients in the pooled pirfenidone and placebo groups, respectively, were hospitalised due to any cause between baseline and month 6. Among these, 4 (9.1%) patients in the pirfenidone group and 16 (32.7%) patients in the placebo group experienced a ≥10% decline in %FVC or death during the subsequent 6-month observation period (relative difference, −72.2%; table 3). The median change in %FVC during this period was −1.8% (range, −56.3, 11.5) in the pirfenidone group and −4.2% (range, −80.6, 8.3) in the placebo group. There were 2 (4.5%) deaths in the pirfenidone group compared with 14 (28.6%) deaths in the placebo group during the second 6-month assessment period. Seven (1.1%) and 15 (2.4%) patients in the pirfenidone and placebo groups, respectively, experienced both a ≥10% decline in FVC and hospitalisation between baseline and month 6 (Pearson's correlation coefficients, 0.086 and 0.101 in the pirfenidone and placebo groups, respectively). Among these, there were no deaths in the pirfenidone group and four (26.7%) deaths in the placebo group during the subsequent 6-month period; however, the limited number of events precludes meaningful interpretation.
Outcomes after 6 months of continued treatment following hospitalisation*
Discussion
The emergence of the first safe and efficacious therapies for patients with IPF heralds the dawn of a new era in the treatment of this devastating disease. However, while both pirfenidone and nintedanib have been proven to significantly reduce the decline in lung function in patients with IPF, neither agent is a cure, and aggregate data from large, randomised, controlled trials demonstrate that patients will likely continue to experience disease progression despite therapeutic intervention. Therefore, clinicians will be confronted with two important questions. First, what constitutes evidence of an inadequate clinical response to therapy and, second, how should such patients be managed?
To further inform clinical decisions related to the assessment and management of patients who experience meaningful progression during treatment, we analysed pooled data from a large and well-defined population of patients with IPF who were followed prospectively for at least 1 year. Our analyses yielded two important observations with implications for the clinical assessment and management of patients with IPF. First, disease progression—as measured by longitudinal change in FVC—is highly variable and cannot be predicted based on prior trends. Analysis of longitudinal FVC data showed a weak inverse correlation between changes in FVC during two consecutive 6-month intervals, highlighting the variability in both the magnitude and direction of change in this prospective, clinical trial population. These results are similar to observations from a retrospective analysis of a real-world IPF cohort, which suggested that FVC decline in the first year of follow-up after diagnosis was not predictive of future declines in physiology.14 The consistency of the findings in two different populations, each of which is subject to a different type of bias, strengthens the observations from both studies. Importantly, these findings also demonstrate that in an individual patient comparison of serial pulmonary function trends during the intervals preceding and following initiation of therapy is not a reliable method of assessing therapeutic response. Clinical decisions related to therapeutic efficacy should therefore be guided by aggregate data from prospective, randomised, controlled trials.
Second, in patients who exhibit clinically meaningful progression of disease during treatment, our findings show that continued treatment with pirfenidone may reduce the risk of a subsequent ≥10% decline in FVC or death. This observation is particularly relevant to clinicians given the absence of data regarding second-line treatment strategies. While sequential monotherapy and combination therapy are common strategies for patients who have a suboptimal response to therapy in other pulmonary diseases, no such data yet exist in patients with IPF.15 Until such data are available, our findings provide the first available evidence to suggest that continuing treatment with pirfenidone despite evidence of disease progression confers a meaningful benefit. We observed a 78.9% reduction in the proportion of patients with a second ≥10% decline in FVC or death and an 85.7% reduction in the proportion of patients who died during the 6 months following an initial FVC decline in the pirfenidone group compared with placebo. A similar treatment effect was observed during the 6 months following hospitalisation; although there was some collinearity observed between hospitalisation and FVC decline, the majority of patients were unique. While the sample size was relatively small, the large magnitude of treatment effect observed in our analyses suggests that pirfenidone might have an important role in the management of patients with progressive disease.
A major goal of therapy in patients with IPF is to attenuate the decline in lung function.16 ,17 Inherent in this goal is the assumption that one can predict the expected rate of decline based on prior trends and measure therapeutic response against the expected rate of decline. However, as our results demonstrate, the markedly variable clinical course observed in patients with IPF precludes any such assumption. In light of this dilemma, it might be suggested that the threshold of a 10% decline in FVC that was used in the categorical assessment of outcomes in the recent phase 3 trials could serve as a benchmark for defining treatment failure in the clinical setting. A ≥10% decline in FVC has been shown in multiple studies to be an independent predictor of mortality,6–11 and a change of this magnitude is well above the estimated minimal clinically important difference in patients with IPF.5 Additionally, the 2011 guidelines for the diagnosis and management of IPF published by an expert committee endorsed by ATS/European Respiratory Society (ERS)/Latin American Thoracic Association (ALAT)/Japanese Respiratory Society (JRS) identified an absolute decline in per cent predicted FVC greater than 10% as evidence of meaningful disease progression.1 It should be noted, however, that while a decline of this magnitude is incontestably clinically meaningful, it is not necessarily evidence of treatment failure, as one cannot preclude the possibility that an even greater decline might have been observed in the absence of treatment or that treatment might impart a benefit that is not captured by change in FVC. Moreover, as our results suggest, continued treatment might confer subsequent benefits in terms of a decreased risk of further FVC decline or death.
There are certain limitations to our analysis. First, while temporally proximate measures of FVC demonstrated high test-retest reproducibility, the contribution of measurement error to the observed variability in FVC change over longer periods cannot be precisely defined. Accordingly, the degree to which the observed variability reflects true variability in the clinical course is uncertain. We note, however, that this distinction is largely academic, as the clinical implication of the observed variability in FVC change remains the same regardless of the relative contribution of measurement error. Specifically, variability in the rate of change in FVC precludes the ability to reliably predict the expected rate of change during subsequent periods based on prior trends. As a result, therapeutic response cannot be evaluated in an individual patient by comparing serial pulmonary function trends during the intervals preceding and following the initiation of treatment. A strength of our current analysis is that we evaluated individual patient data rather than population-based means, which enabled greater insight into this variability. Second, we selected FVC and hospitalisation as measures of initial disease progression because they are readily and reliably ascertainable in virtually all patients in the typical clinical setting. We did not evaluate outcomes following evidence of disease progression based on other measures like 6-min walk distance or diffusing capacity for carbon monoxide (DLCO); the effect of continued treatment following meaningful decrements in these and other measures is therefore not known. Finally, the analysis of outcomes following evidence of disease progression was a post hoc exploratory analysis; accordingly, the results should be interpreted with caution.
In conclusion, analysis of longitudinal FVC data from a large cohort of patients with IPF demonstrated high intersubject and intrasubject variability in the rate of disease progression, underscoring the inability to reliably assess therapeutic response in an individual patient based on serial FVC trends. In patients who experienced a ≥10% decline in FVC or hospitalisation, continued treatment with pirfenidone resulted in a lower risk of FVC decline or death during the subsequent 6 months. These findings suggest a potential benefit to continued treatment with pirfenidone in patients with IPF who experience disease progression during therapy.
Acknowledgments
The authors thank the patients, family members and participating staff at all study sites.
References
Footnotes
Twitter Follow David Lederer at @davidlederer
Contributors SDN, CA, WZB, UC, RMdB, EAF, RSF, IG, MKG, TEK, LL, DJL, CAP, JJS, DV and PWN contributed to the conception and design of the original studies as well as the acquisition and interpretation of data. SDN, WZB, KFG, ZL and AUW contributed to the design of the subsequent analyses, and all authors participated in the interpretation of these data. ZL was responsible for the statistical analyses. KFG drafted the manuscript, which was critically reviewed by all authors. The final version of the manuscript was approved by each author.
Funding The study was sponsored by InterMune Inc. (Brisbane, California, USA).
Competing interests SDN is a consultant for Genentech/Roche and Boehringer Ingelheim; he is also on the Speakers Bureau and has received research funding from Genentech/Roche and Boehringer Ingelheim. CA has received grant support, personal fees and non-financial support from Roche (InterMune). UC has served as a consultant for Centocor, Gilead and GSK; and served as a consultant and received honoraria for lectures from Bayer, Boehringer Ingelheim and InterMune (Roche). RMdB has served on an advisory board for Actelion and GSK and served as a consultant for Boehringer Ingelheim and InterMune, Inc. IG has served on an advisory board for AstraZeneca, Boehringer Ingelheim and Roche; and has received grant support from Boehringer Ingelheim and Roche. MKG has received personal fees from Genentech during the conduct of this study, and has received personal fees from Boehringer Ingelheim, France Foundation and Mesoblast outside of the submitted work. TEK has served as a consultant for Boehringer Ingelheim and served on a scientific advisory board for GSK, Immune Works and InterMune. LL has received grant support from InterMune (Roche/Genentech) and served on a scientific advisory board for Genentech. DJL has served on a scientific advisory board for Boehringer Ingelheim, Gilead, Immune Works, and InterMune, Inc. CAP has received a research grant from InterMune, Inc. JJS has served on a scientific advisory board and received research funding from InterMune, Inc., and served as a consultant to Boehringer Ingelheim and Roche/Genentech. DV has served as a consultant for Roche (InterMune) and Boehringer Ingelheim. PWN has served as a consultant for Boehringer Ingelheim, Bristol-Meyers Squibb, InterMune, Inc., Moerae Matrix, Roche/Genentech and Takeda. AUW has received advisory board fees from Roche (InterMune), Boehringer Ingelheim, Gilead, MSD, Bayer and Chiesi; and has received speaker's fees from Roche (InterMune), Boehringer Ingelheim and Bayer. WZB, EAF, RSF, KFG and ZL were employees of InterMune, Inc. (now a wholly-owned Roche subsidiary) at the time of submission.
Ethics approval The study was approved by the ethics committee/institutional review board for each participating study site.
Provenance and peer review Not commissioned; externally peer reviewed.