Article Text

Abstract
Automatically titrated O2 flows (FreeO2) was compared with constant O2 flow on exercise capacity, O2 saturation and risk of hyperoxia-related hypercapnia in patients with severe COPD with baseline hypercapnia and long-term oxygen therapy (LTOT). Twelve patients were enrolled in a randomised double-blind cross-over study to perform exercise with either FreeO2 or constant flow. Endurance time (primary outcome) and SpO2 were both significantly improved with FreeO2compared with constant flow (p<0.04), although pCO2 was similar in both conditions. Automated titration of O2 significantly and clinically improved endurance walking time in patients with severe COPD receiving LTOT, without worsening of pCO2.
Trial registration number Results , NCT01575327
- ambulatory oxygen therapy
- copd ÀÜ mechanisms
- exercise
Statistics from Altmetric.com
Introduction
Acute oxygen (O2) supplementation improves oxygenation and exercise tolerance in patients with severe COPD when used in a laboratory setting.1 However, home-based and long-term use of oxygen supplementation is generally unsuccessful in improving exercise tolerance in COPD.2 This could be related to insufficient oxygen flow rates to correct exercise-induced hypoxaemia during daily tasks. For example, 24-hour home-based SaO2 monitoring performed in patients while breathing O2 at their prescribed flow rate (1–3 L/min) showed inadequate oxygenation during daily tasks3 and mean SaO2 of 88% during walking.4 Indeed, current recommendation is to increase O2 flow rates during exercise by adding 1 L/min to resting O2 flow, which might be insufficient. On the other hand, high O2 flow rates may be considered at risk to worsen hypercapnia in patients with severe COPD.5 Closed-loop titration of oxygen flow rates based on pulsed oxygen saturation (SpO2) continuous measurements may help in optimising oxygen supplementation during exercise.6–8 We hypothesised that the FreeO2 system, a new closed-loop O2 device that automatically titrates O2 flows to maintain SpO2 within predetermined targets, would improve exercise tolerance in patients with severe COPD without worsening hypercapnia.7
Methods
Intervention
In a randomised double-blind cross-over study, we compared the effects of automatically titrated versus constant O2 flows on exercise tolerance during walking in patients with Global Initiative for Chronic Obstructive Lung Disease (GOLD) 3–4 COPD. We also studied the impact of these two oxygen supplementation systems on oxygenation and capillary pCO2 (PcCO2) during and after exercise. (ClinicalTrials.gov number: NCT01575327, Results).
Outcomes
The primary outcome of the study was endurance time (and the corresponding walking distance) during the endurance shuttle walking test (ESWT) performed at 85% estimated peak VO2.9 Secondary outcomes included time spent within pre-specified SpO2 targets (<88%, 88%–91%, 92%–96% and >96%), capillary blood gases (pH, PcCO2), heart rate (HR), dyspnoea and leg fatigue. In addition to the parameters continuously collected by the FreeO2 system, O2 flow rates, SpO2, HR and earlobe capillary blood gases were obtained before, at the end and 10 min after exercise. A modified Borg scale was used to assess dyspnoea and leg-fatigue scores at 1 min intervals during exercise and at the end of exercise. Isotime exercise was assessed for HR, dyspnoea and leg fatigue. It corresponded to the longest time duration reached during the ESWT under both conditions (automatically adjusted O2 flows and constant O2 flows). Warm-up was included in the calculation of the endurance time. The washout period between the two walking tests averaged 4.0±4.6 days.
Patient characteristics
Twelve patients (age 65±10 years, Body Mass Index 25±7 kg/m2) with GOLD 3 (n=4) or 4 (n=8) COPD, long-term oxygen therapy (LTOT, mean baseline O2 flow rates: 1.9±1.0 L/min for 5.5±4.5 years) and resting hypercapnia (mean PaCO2 48.7±3.0 mm Hg) were included in the study. The pulmonary function is described in online supplementary table E1. Briefly, FEV1 was 0.70±0.25 L, 30%±9% predicted, FEV1/FVC was 50%±15%, TLC was 124%±25% predicted, RV was 225%±76% predicted, inspiratory capacity was 1.42±0.50 L and diffusing capacity of lung for CO was 32%±18% predicted. Patients had a smoking history of 41±19 pack-years (three current smokers) and with 1.3±0.5 respiratory exacerbation per year. They had a 6 min walking distance of 363±72 m, a modified Medical Research Council dyspnoea score of 3.3±0.7 and a self-reported spontaneous physical activity of <10 min per day. Sixty-six and 33% of patients respectively exhibited cardiovascular and metabolic comorbidities (see online supplementary table E1). Following baseline assessment, patients performed, on two separate visits, one ESWT receiving either automatically titrated O2 flows with the FreeO2 system aiming for a SpO2 target of 94%7 or constant O2 flows (usual O2 flow rate +1 L/min). The FreeO2 system can deliver O2 flows from 0 to 20 L/min, with 0.1 L/min incremental/decremental steps, on a per-second basis.7 More information on the methodology can be found in online supplementary data.
Supplementary file 1
Statistical analysis
Data are expressed using mean±SD. Variables were analysed using a mixed model (and a log-transformed for some variables to fulfil the model assumptions) or using a statistical approach replacing observations by their rank within subjects, called rank transformation. Posteriori comparisons were performed using Tukey’s comparison. The level of significance was set at p values <0.05 (R V.3.0.2 and SAS V.9.4).
Results
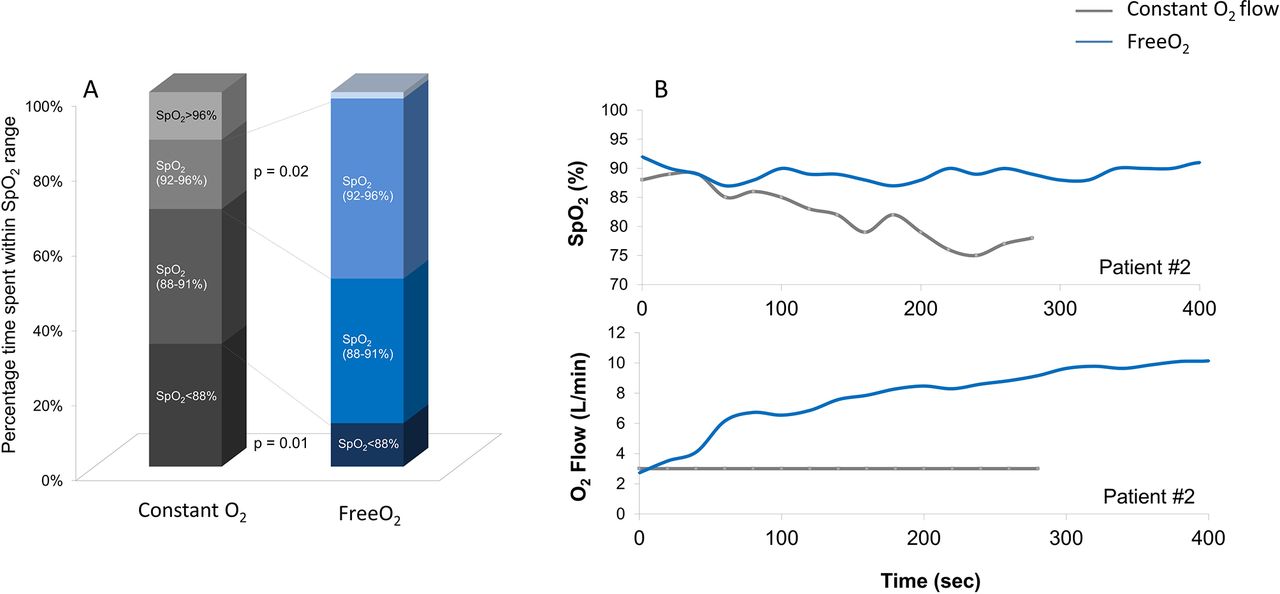
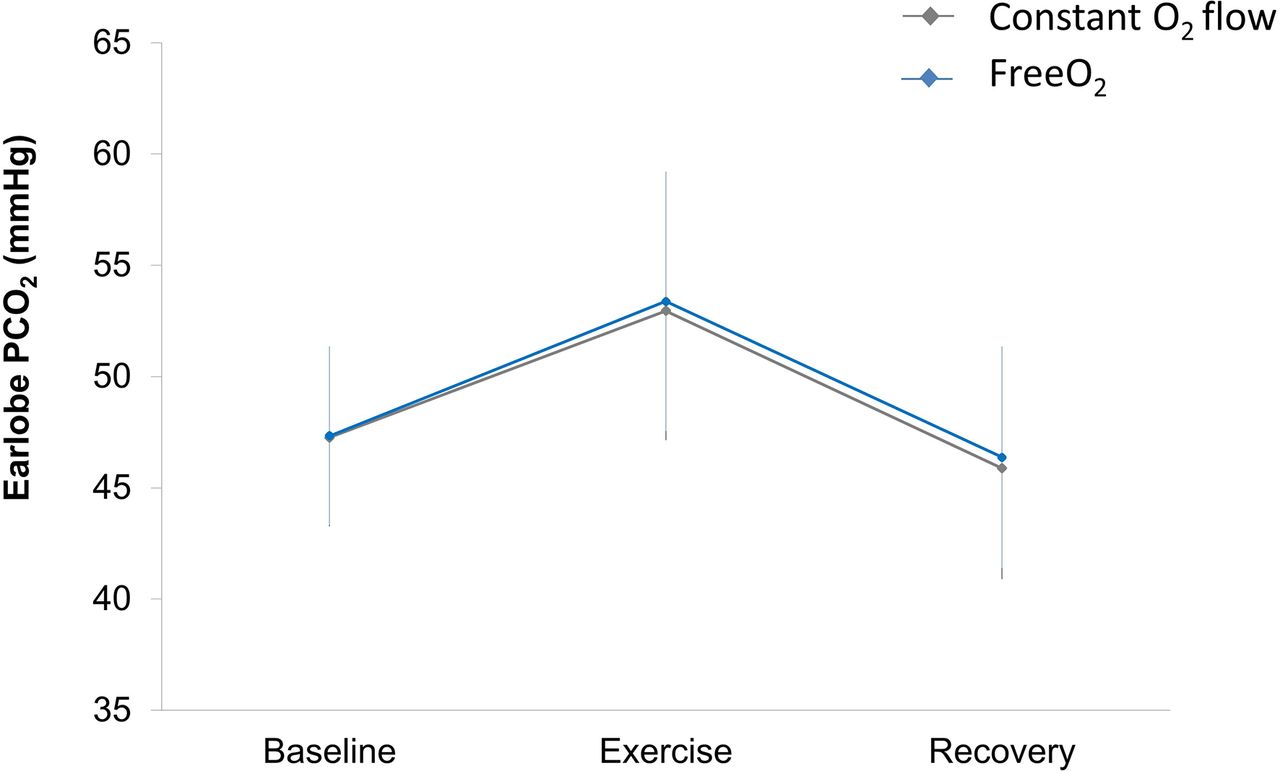
Here, we found for the first time that patients with severe COPD improved endurance time and walking distance when using automatically titrated O2 flow compared with constant O2 flows (+127±236 m, p=0.02 and +138±269 m, p=0.03, respectively, figure 1A and B). This functional improvement was associated with greater O2 flow rates during exercise (FreeO2: 5.4±2.7 vs constant O2 flows: 3.1±1.2 L/min, p=0.01) leading to better O2 saturation. Indeed, patients spent less time with hypoxaemia while also avoiding hyperoxia with FreeO2 (figure 2). The lowest O2 saturation was 83.6%±7.0% with constant O2 flow versus 89.5%±3.9% with FreeO2 (p<0.001). Patients spend more time exercising within the pre-specified SpO2 target (88%–92%) while using FreeO2 compared with constant O2 flows while avoiding hyperoxia (figure 2). Despite higher O2 flow rates with FreeO2, PcCO2 was similar in both conditions across resting, walking test and recovery, suggesting that hypercapnia was not worsened using higher O2 flows in these patients (p=0.71, figure 3). Lastly, dyspnoea and leg fatigue scores were significantly reduced at isotime with FreeO2 compared with constant O2 flow (5.3±2.1 vs 7.0±2.8, p=0.048 and 1.4±2.0 vs 2.6±2.7, p=0.028, respectively). Changes in endurance time with FreeO2 correlated with diffusing lung capacity (r=−0.78, p=0.02). No other relationship was found between baseline pulmonary function, blood gas parameters or O2 flows during exercise.

Individual data and mean±SE of endurance time (A) and walking distance (B) during the endurance shuttle walking test when using constant O2 flows (grey bars) or automatically titrated O2 flows (FreeO2) (blue bars). Both endurance time and walking distance were improved in the FreeO2 condition as compared with constant O2 flows (p=0.02 and p=0.03, respectively).
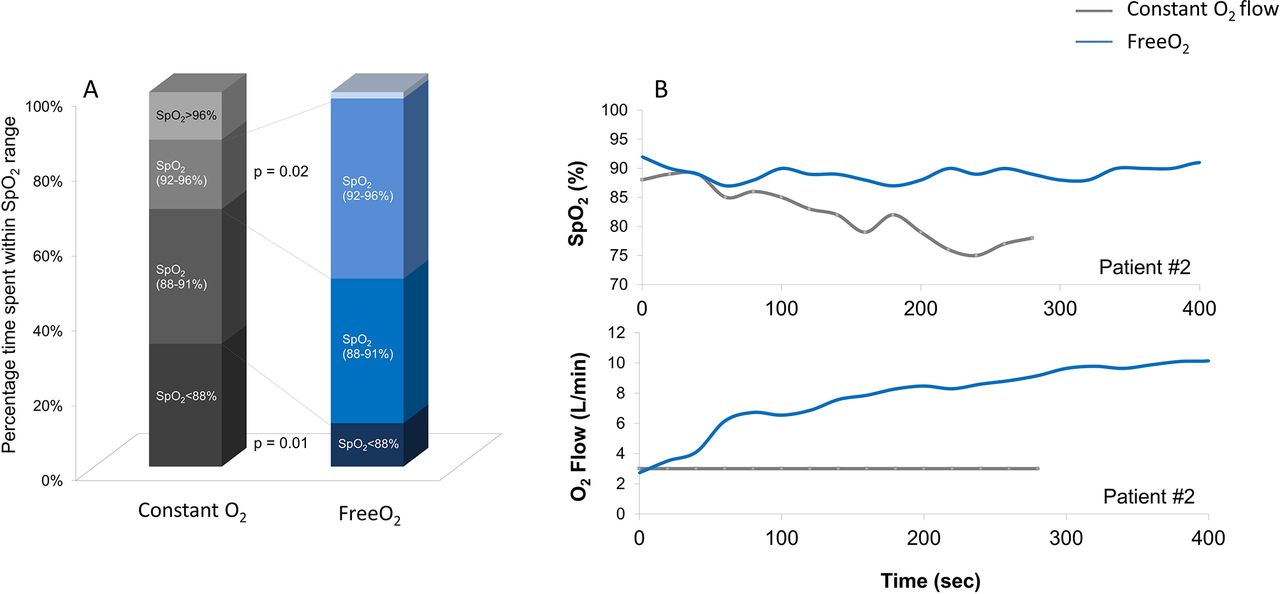
(A) Percentage of time spent in different ranges of SpO2 during the endurance shuttle walking test when using constant O2 flows (grey bar) or automatically titrated O2 flows (FreeO2) (blue bar). Time spent in the range SpO2 <88% was reduced when using FreeO2 compared with constant O2 flow (p=0.01), although time spent in the range SpO2 (92%–96%) was increased (p=0.02). Hyperoxia (time spent in the range of SpO2 >96%) was not increased by FreeO2 compared with constant O2 flow but rather tended to be reduced (p=0.51). (B and C) Example of individual traces of SpO2 (%) (B) and corresponding O2 flows (C) for a given patient (#2) during the endurance shuttle test while using constant O2 flows (grey line) or automatically titrated O2 flows (FreeO2) (blue line).

{kind=link}
{kind=link}
{kind=link}
Earlobe blood capillary pCO2 measured at baseline (rest), end of exercise (exercise) and 10 min after exercise (recovery) when using constant O2 flows (grey line and markers) or automatically titrated O2 flows (FreeO2) (blue line and markers). There was no significant difference between groups in PcCO2 at any time before, during exercise or during recovery (p=0.71).
Discussion
This is the first study to demonstrate that automated oxygen titration improves exercise tolerance in patients with severe COPD. This is a novel and promising result in this population. Indeed, previous studies did not report significant improvement in this outcome compared with constant O2 flows, despite reduction in hypoxaemia.6 8 10 In addition, the +127±236 s increase in endurance time (+33%) found in the present study was beyond the minimal clinically relevant difference for this parameter.11 The severity of the disease may account for the discrepancy between studies since patients with advanced disease are more responsive to adequate oxygenation during exercise.12 Moreover, the shuttle walking test used in the present study is more responsive to interventions than the 6 min walking test used in previous studies.6 8 Lastly, the ability to deliver high oxygen flows is superior with the FreeO2 device (delivering up to 20 L/min) than other devices.6 8 In our study, FreeO2 enabled 7 out of 12 patients (58%) to use O2 flow rates above 5 L/min during exercise. Hence, patients with advanced COPD and chronic respiratory failure seem to be good candidates for automatically titrated O2 supplementation during exercise.12
Several mechanisms may explain the improvement in exercise performance with oxygen supplementation in severe COPD. By reducing hypoxaemia, O2 supplementation may have reduced VE and decreased dynamic hyperinflation.1 The significant reduction in dyspnoea score found at isotime exercise in the present study with automatically titrated O2 would support this hypothesis. In addition, the lower leg fatigue score suggests a reduced respiratory metaboreflex allowing better perfusion and oxygenation of contracting muscles, in turn reducing fatigue occurrence.13 It is to note, however, that not all the patients were good responders to automated O2 titration (figure 1). Our results suggest that patients with lower diffusing lung capacity had higher gain in endurance time with FreeO2 compared with constant O2 flow. In these patients, it is likely that higher O2 flows increased O2 diffusion, which in turn increased muscle oxygenation and consequently aerobic capacity.
Physicians might be reluctant to use high O2 flows in patients with severe COPD, particularly those with resting hypercapnia, fearing to induce further CO2 retention.5 In the present study, the absence of worsening in hypercapnia was likely linked to the reduced time with hyperoxia due to the working principle of the FreeO2 device. Indeed, the FreeO2 device is set to automatically reduce O2 flow rates when the measured SpO2 is above the set SpO2 target.
Methodological considerations
One limitation of our study is the relatively small sample size. However, a predefined sample size calculation was performed based on preliminary data in this very specific population (see online supplementary data). Another potential limitation was the slightly high SpO2 target (94%) compared with general recommendation in patients with COPD (88%–92%).14 However, this threshold was based on previous observations showing that the use of this 94% SpO2 target did not induce hypercapnia compared with constant O2 flows.10 Lastly, we used arterialised capillary instead of arterial blood samplings. However, capillary samplings were cautiously collected after adequate vasodilation of the earlobe and, in this condition, they are considered as appropriate replacements for arterial samplings.15
Clinical impact
Ambulatory oxygen therapy had failed to demonstrate long-term benefits in COPD,2 perhaps due to insufficient correction of hypoxaemia during daily activities. By allowing adequate oxygenation during activities of daily life such as walking, continuous and precise O2 titration with automated devices may improve exercise tolerance, a strong determinant of quality of life and survival in patients with COPD.16 Hence, automated titration such as FreeO2 may increase the clinical benefits of oxygen therapy in this population.
In summary, we found that automatic titration of O2 during walking had significant and clinically relevant impact on endurance time in patients with severe COPD receiving LTOT, without worsening pCO2. Such technological improvements should improve titration of O2 therapy tailored to individual needs who are constantly changing during daily activities. Nevertheless, caution should be used before generalising the present results to a broader population of patients. Further studies will be necessary to determine which SpO2 upper limit represents the best trade-off value between optimised oxygenation and minimised CO2 retention risk. In addition, the fact that larger and heavier O2 source may be mandated to allow higher O2 flows during exercise needs to be further considered in subsequent studies .
Acknowledgments
The authors wish to thank Mrs Marion Perrin, MSc and M Serge Simard, MSc for the statistical analysis.
References
Footnotes
Contributors Study concept and design: IV, FL, J-LP. Acquisition of data: IV, GV, CY, RT. Analysis and interpretation of data: IV, J-LP. Drafting of the manuscript: IV, J-LP. Critical revision of the manuscript for important intellectual content: IV, E L’H, RT, FM, FL, J-LP. Study supervision: IV, J-LP.
Funding Endowment fund ‘Fondation de l’Avenir’, France; Endowment fund ‘Agir pour les Maladies chroniques’, France; French National Research Agency (framework of the ‘Investissements d’avenir’ program) (ANR-15-IDEX-02).
Competing interests The authors declare that IV, GV and CY have no financial interests that may be relevant to the submitted work. FL is co-inventor of the FreeO2 system. FL is co-founder of Oxynov, a R&D company to develop automated systems for respiratory support. No support from this company was provided for the study; EL’H is co-inventor of the FreeO2 system. ELH is co-founder of Oxynov, a R&D company to develop automated systems for respiratory support. He received grants for participation to expert boards or speaking at conferences sponsored by Smiths Medical, Air Liquide Medical Systems, Sedana Medical and General Electrics. No support from this company was provided for the study; FM participates in Innovair, a company that owns shares in OxyNov; FM reports grants for participating in multicentre trials sponsored by GlaxoSmithKline, Boehringer Ingelheim, AstraZeneca and Novartis; and unrestricted research grants from Boehringer Ingelheim, Novartis and Grifols; others from Boehringer Ingelheim, Novartis and Grifols. FM holds a CIHR/GlaxoSmithKline research chair on COPD. No support from those companies was provided for the study; J-LP has received lecture fees from Resmed, Perimetre, Philips, Fisher and Paykel, JAZZ pharmaceutical, AstraZeneca and SEFAM. J-LP has received conference travelling grant from Agiradom and Teva. J-LP has also received unrestricted research funds from ResMed, Philips, GSK, Fondation de la recherche medicale, Direction de la recherche Clinique du CHU de Grenoble, Fond de dotation ‘Agir pour les maladies chroniques’. No support from those companies was provided for the study; RT reports grants from Resmed, grants from Philips, other from Resmed and other from Agiradom. No support from those companies was provided for the study.
Patient consent Obtained.
Ethics approval CPP Sud Est V, 11-AGIR-01.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unpublished data are available: exercise parameters: HR, pH, HCO3 (earlobe blood samples). Please contact Isabelle Vivodtzev at ivivodtzev@partners.org.