Article Text

Abstract
Background: Idiopathic pulmonary fibrosis (IPF) is a chronic progressive disorder with a poor prognosis. Epithelial instability is a crucial step in the development and progression of the disease, including neoplastic transformation. Few tissue markers for epithelial instability have been reported in IPF. Squamous cell carcinoma antigen (SCCA) is a serine protease inhibitor typically expressed by dysplastic and neoplastic cells of epithelial origin, more often in squamous cell tumours. At present, no information is available on its expression in IPF.
Methods: SCCA and transforming growth factor β (TGFβ) expression in surgical lung biopsies from 22 patients with IPF and 20 control cases was examined. An in vitro study using A549 pneumocytes was also conducted to investigate the relationship between SCCA and TGFβ expression. SCCA and TGFβ epithelial expression was evaluated by immunohistochemistry and reverse transcription–PCR (RT-PCR). SCCA values were correlated with different pathological and clinical parameters. Time course analysis of TGFβ expression in A549 pneumocytes incubated with different SCCA concentrations was assessed by real time RT–PCR.
Results: SCCA was expressed in many metaplastic alveolar epithelial cells in all IPF cases with a mean value of 24.9% while it was seen in only two control patients in up to 5% of metaplastic cells. In patients with IPF, SCCA correlated positively with extension of fibroblastic foci (r = 0.49, p = 0.02), expression of TGFβ (r = 0.78, p<0.0001) and with carbon monoxide transfer factor decline after 9 months of follow-up (r = 0.59, p = 0.01). In vitro experiments showed that incubation of cultured cells with SCCA induced TGFβ expression, with a peak at 24 h.
Conclusion: Our findings provide for the first time a potential mechanism by which SCCA secreted from metaplastic epithelial cells may exert a profibrotic effect in IPF. SCCA could be an important biomarker in this incurable disease.
Statistics from Altmetric.com
Idiopathic pulmonary fibrosis (IPF), morphologically characterised by an usual interstitial pneumonia (UIP), represents a progressive disease of unknown aetiology that continues to be associated with high morbidity and mortality.1
The key pathological features of this disorder include epithelial damage/activation, fibroblastic/myofibroblastic foci formation and extracellular matrix remodelling.2 Although previous studies on fibrogenesis have focused on the role of inflammation in favouring fibroblast activation and fibrosis, the current paradigm suggests the pivotal role of epithelial deregulation in the disease pathogenesis.2 3 Epithelial injury and subsequent deregulated repair result in cytokine release, excess of extracellular matrix deposition and abnormal mesenchymal cell activation and proliferation. Among profibrogenetic cytokines, transforming growth factor β (TGFβ) represents the key growth factor which leads to mesenchymal differentiation, myofibroblast infiltration and proliferation. As a consequence, the areas of immature fibrosis are progressively invaded by small aggregates of actively proliferating myofibroblasts and fibroblasts termed fibroblastic foci (FF) whose number and extension have been associated with the prognosis of the disease.4
Epithelial instability has been largely documented by the presence of frequent evidence of morphological changes through variegated cellular alterations, such as hyperplasia, atypia, squamous metaplasia, dysplasia and eventually carcinoma.5–9 The frequent occurrence of lung carcinoma, particularly squamous cell type, in patients with IPF/UIP is one of the contributing factors to a poor prognosis.10 A few tissue markers for epithelial instability have recently been described as being overexpressed in lung tissue from patients with IPF/UIP, including the expression of the K-ras gene with point mutation and the presence of multiple mutations of p53, which have been detected in type II alveolar pneumocytes of IPF/UIP lungs.11 Also, overexpression of wild-type p53 has been reported by several authors. Its upregulation in the face of chronic DNA damage may increase the potential p53 mutation leading to an imbalance of different growth factors and consequently increased tumorigenesis in IPF.12 13 A more frequent occurrence of guanine nitration has recently been found in metaplastic and neoplastic cells from patients with IPF/UIP, indicating that nitrative stress is an important step in epithelial damage at risk of neoplastic transformation.14
Squamous cell carcinoma antigen (SCCA) is a serine protease inhibitor typically expressed by dysplastic/neoplastic cells of epithelial origin, including lung cancer.15 Recent studies indicate that both SCCA1 and SCCA2, the two isoforms so far identified,16 protect neoplastic cells from apoptotic death induced by several types of stimuli, and in vivo experiments demonstrate that SCCA can promote tumour growth.17 The main goal of the present study was to assess expression of SCCA both as mRNA and protein in lung biopsies from patients with IPF/UIP and from controls. To analyse the pathogenetic and prognostic value of SCCA, the association between its value and different clinical and pathological data, including TGFβ tissue expression, was studied. An in vitro study was also conducted to investigate the biological activity of SCCA on TGFβ expression.
MATERIALS AND METHODS
Patients
The study was performed on lung samples from 22 patients with IPF consecutively evaluated from June 2003 to August 2006 at our centre and on 20 samples from non-IPF subjects. The diagnosis of IPF was based on the diagnostic criteria of the American Thoracic Society/European Respiratory Society Consensus Classification System.18 Samples from patients with IPF were obtained from video assisted thoracoscopic lung biopsies. Written informed consent was obtained from each patient and the work was approved by the Institutional Ethics Committee. Histological examination revealed all of the major features of UIP, which is a prerequisite for the diagnosis of IPF. Mean age of the patients was 60.2 years (range 44–69); 17 of the patients were males and five were females. All patients underwent routine pulmonary function testing, including spirometry, lung volume measurement, measurement of carbon monoxide transfer factor (Tlco), arterial blood gases at rest and after exercise, chest radiography and high resolution CT. The main characteristics of the subjects are shown in table 1.
Lung function data were recorded less than 6 weeks before biopsies in all IPF cases and re-evaluated after a median period of 9 months (range 6–11). At follow-up, clinical data were completed for 18 patients, two patients died before undergoing the second pulmonary function test and spirometry results were not evaluable for two cases. Data were expressed as percentage of values predicted from the subject’s age, sex and height.
Fifteen patients underwent biopsies at two different sites (upper and lower lobes), and the other seven patients were biopsied at three separate sites (upper, middle and lower lobes), giving a total number of 51 biopsies. The majority of the patients were treated after biopsy with a high dose of steroids alone or in combination with azathioprine. Control lungs were obtained from non-implanted donor lungs (10 cases) and from other forms of interstitial lung diseases (ILDs, 10 cases): two non-specific interstitial pneumonias, one desquamative interstitial pneumonia, one Langerhans-cell histiocytosis, one lymphangioleiomyomatosis, two respiratory bronchiolitis interstitial lung diseases, one cryptogenic organising pneumonia, one mixed pneumoconiosis and one hypersensitivity pneumonitis. The donors (five males and five females, mean age 30 (17) years, all no smokers) died of cerebral trauma and stayed less than 2 days in intensive care without evidence of lung infections or other complications. Patients affected by other forms of ILDs (three males and seven females; mean age 45 (15) years, all smokers except patients with lymphangioleiomyomatosis and hypersensitivity pneumonitis) were defined by the presence of clinical, radiological and histological evidence of specific ILD. All lung tissues were formalin fixed and paraffin embedded following standard protocols.
Histology and morphometry
Fibroblastic foci (FF) and inflammatory cells (IC) were evaluated using a semiquantitative method. In particular, FF were analysed using a Brompton score4 and IC was scored as follows: less than 10% of lung tissue examined (score 1), more than 10% and less than 30% of lung tissue examined (score 2) and more than 30% of lung tissue examined (score 3). In all samples from each patient, the extent of fibrosis, inflammation and FF were also measured by computerised morphometric analyses (Image Pro-plus V.5). The extent of fibrosis was quantified on lung sections stained by Azan–Mallory, as previously described.19 FF, IC and fibrosis were analysed on 10 random fields in the same section of imaged lesions at 50-fold magnification, excluding the areas of honeycombing. In each selected field, the ratio of FF, IC and fibrotic areas (AFF, AIC, AFIB) were calculated, dividing the total AFF, AIC and AFIB by the total tissue area (excluding airspaces) of the section (where n = the number of fields):
FF ratio = ΣnAFF/total area × 100
IC ratio = ΣnAIC/total area × 100
Fibrosis ratio = ΣnAFIB/total area × 100.
For each patient, the ratios obtained from the analysed sections were then averaged and this value was correlated with all pathological and clinical parameters. In contrast with the authors recently supporting the value of quantitative analysis of FF,20 we measured all parameters, including FF, exclusively related to lung tissue (excluding air spaces) to normalise the effect of collapse or expansion of lung tissue during biopsy or tissue fixation.
Immunohistochemical analysis
All cases were immunoassayed with a novel polyclonal rabbit antibody anti-SCCA (Hepa-Ab, Xeptagen, Venice, Italy) and mouse monoclonal anti-TGFβ (NovoCastra, Newcastle, UK), as previously described.21 22 All samples were processed using a sensitive avidin–streptavidin–peroxidase technique and stained with a mixture of 3,3-diaminobenzidine tetrahydrochloride and hydrogen peroxide. Parallel control slides were prepared either lacking primary antibody or lacking primary and secondary antibodies, or were stained with normal sera to control for background reactivity. Consecutive serial sections immunostained for SCCA and TGFβ were evaluated and the quantification was restricted to strongly stained metaplastic epithelial cells (cuboidal, squamous, bronchiolar). A total of 500 metaplastic epithelial cells for each patient were counted in remodelled lung parenchyma (at least two sections) and the value was expressed as a percentage of positive cells/500 for each case. This value was correlated with all pathological and clinical values.
Molecular analysis
Manual tissue dissection
Manual tissue dissection of representative areas, positive for SCCA and TGFβ, was performed in half of the cases (11 cases) in which metaplastic epithelial aggregates were easily dissected. Briefly, five sequential 5 μm sections from formalin fixed paraffin embedded blocks were placed on non-coated glass slides and coupled with SCCA and TGFβ immunostained tissue sections. The areas (at least 1 mm in diameter) carefully marked to easily compare the unstained levels were gently scraped with a sterile scalpel. The procured tissue fragments were then placed in a tube, deparaffinised and washed in xylene and alcohol before nucleic acid extraction. After this procedure, the remaining unselected tissue was stained with haematoxylin–eosin to verify the isolated tissue parts.
Areas of normal tissue (negative for SCCA and TGFβ immunoassaying) from the same paraffin block and from donor lung were also dissected and processed in the same way.
RT-PCR of SCCA and TGFβ
Total RNA was extracted using the modified RNAzol method, as previously described.23 The RNA pellet was redissolved in 15 μl of sterile diethylpirocarbonate treated water and incubated with 1 μl of RNAse inhibitor (Applied Biosystems, Milan, Italy) and 20 U of DNAse I (Sigma Aldrich, Milan, Italy) for 2 h at 37°C in a total volume of 20 μl. The oligonucleotides used to ascertain the quality of extracted RNA were complementary to the mRNA glyceraldehyde-3-phosphate dehydrogenase (GAPDH). The sequences of primers for GAPDH, SCCA and TGFβ, annealing temperature condition and amplicon sizes are listed in table 2. At least 1 μg of extracted total RNA was used for the first cDNA synthesis and conventional RT-PCR was used. The PCR mix was made up to a volume of 50 μl using 1×PCR Buffer II, 1 mM MgCl2 solution, 200 μM each of dATP, dCTP, dGTP and dUTP, 400 nM of each primer and 1.25 U of AmpliTaq Gold. After the initial denaturation at 95°C for 10 min, cDNA was amplified by 40 three step cycles (30 s at 95°C, 30 s at annealing temperature, 1 min at 72°C). SCCA and TGFβ amplicons were both verified by a previously described gene sequencing protocol.21
In vitro study
Cell culture
Lung epithelial cell line A549 was obtained from the American Type Culture Collection (Manassas, Virginia, USA). Cells were maintained routinely in Dulbecco’s modified Eagle’s medium with 10% fetal bovine serum (Gibco, Milan, Italy) and supplemented with 100 mg/ml penicillin G (Gibco) and 100 mg/ml streptomycin sulfate (Gibco, Milan, Italy). Cells were then seeded in Dulbecco’s modified Eagle’s medium with 10% fetal bovine serum at a density of 0.3×106 cells per well in six well plates. All experiments were performed at 100% cell confluence. Time course analysis was carried out to assess the effect of SCCA on TGFβ expression. Cells were incubated with SCCA (Xeptagen, Venice, Italy) at increasing concentrations (range 1–1000 pg/ml) and checked for TGFβ expression at 6 h intervals (range 6–48). Cells were collected and lysated immediately with RLT buffer (Qiagen, Milan, Italy) and β-mercaptoethanol 14.5 M 1% (Sigma Aldrich, Milan, Italy).
Quantitative RT-PCR of TGFβ
RNA was extracted using RNeasy Mini Kit (Qiagen, Milan, Italy) according to the manufacturer’s instructions. RNA was reverse transcribed using the Reverse Transcription System (Promega Corporation, Madison, Wisconsin, USA) according to the manufacturer’s instructions. Real Time PCR was performed using a standard TaqMan PCR kit protocol on an Applied Biosystems 7000 Sequence Detection System (Applied Biosystems, Milan, Italy). The TaqMan PCR was carried out in a 96 well microtitre plate format (Applied Biosystems). The PCR mix was made up to a volume of 25 μl using ready to use Universal Mastermix containing AmpliTaq DNA polymerase, uracil-N-glycosilase, dNTPs, KCl, MgCl2 and ROX as passive reference, all in optimised concentrations. After uracil-N-glycosilase treatment at 50°C for 2 min and initial denaturation at 95°C for 10 min, DNA was amplified by 40 two step cycles (15 s at 95°C, 1 min at 57°C). All reactions were run in triplicate. Reactions and cycling were performed as recommended by the manufacturer. GAPDH was used as a reference gene for the adjustment of relative expression data. Naive cells collected at the same time were used as calibrators. All assays were performed in triplicate to ensure their reproducibility, and a negative control was included in each run. Primers and probes for GAPDH and TGFβ were commercially available (4333764 and 4327054; Applied Biosystems).
Statistical analysis
Normality of distribution for quantitative variables was assessed by means of Shapiro–Wilk statistics. Normally distributed quantitative variables are described as mean (SD), not normal quantitative variables are expressed as median, range and interquartile range (IQR), while categorical variables are presented as percentage distribution. To evaluate simple linear relationships between quantitative variables, Pearson’s or Spearman’s correlation coefficients were applied, as necessary. To evaluate the independent association of each factor with the dependent variable, the partial correlation coefficients were estimated.
In the analysis of the relationship between SCCA and scores, to allow greater set sizes, foci and inflammation scores were used to group IPF subjects. For foci, subjects were ranked: 1 (score 1–2), 2 (score 3–4) or 3 (score 5–6). For inflammation, the variable was dichotomised (score⩽1, score >1). The mean value of SCCA of the different groups was compared by means of one way analysis of variance (ANOVA).
Statistical analysis was performed using SAS statistical software V.9.1 (SAS Institute, Carry, North Carolina, USA). A p value <0.05 was considered statistically significant.
RESULTS
Pathological findings and clinicopathological correlations
Median histological score (range, IQR) was 3.0 (1–6, 2) and 1.0 (1–3, 1) for FF and for IC, respectively. Among all quantitative variables, only fibroblastic foci area (AFF) showed a distribution different from normality (p = 0.02). Median value for AFF was 8.4% (4.3–21.8%, 5.6%). Mean value for inflammation area (AIC) and fibrosis extension were 3.0 (1.4)% and 35.6 (7.4)%, respectively (table 1). A direct correlation was observed between AFF and AFIB (r = 0.56, p = 0.007). A statistically significant correlation was observed only between AFIB and decline in Tlco at 9 months (r = 0.5156, p = 0.0302).
Immunohistochemical findings and correlations with morphological and clinical data
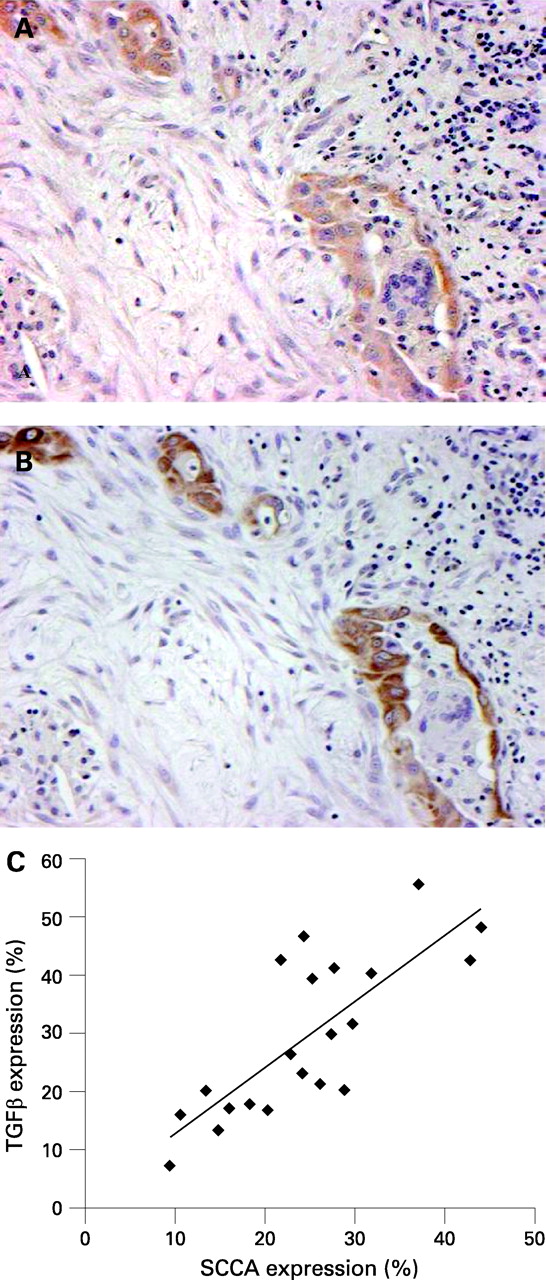
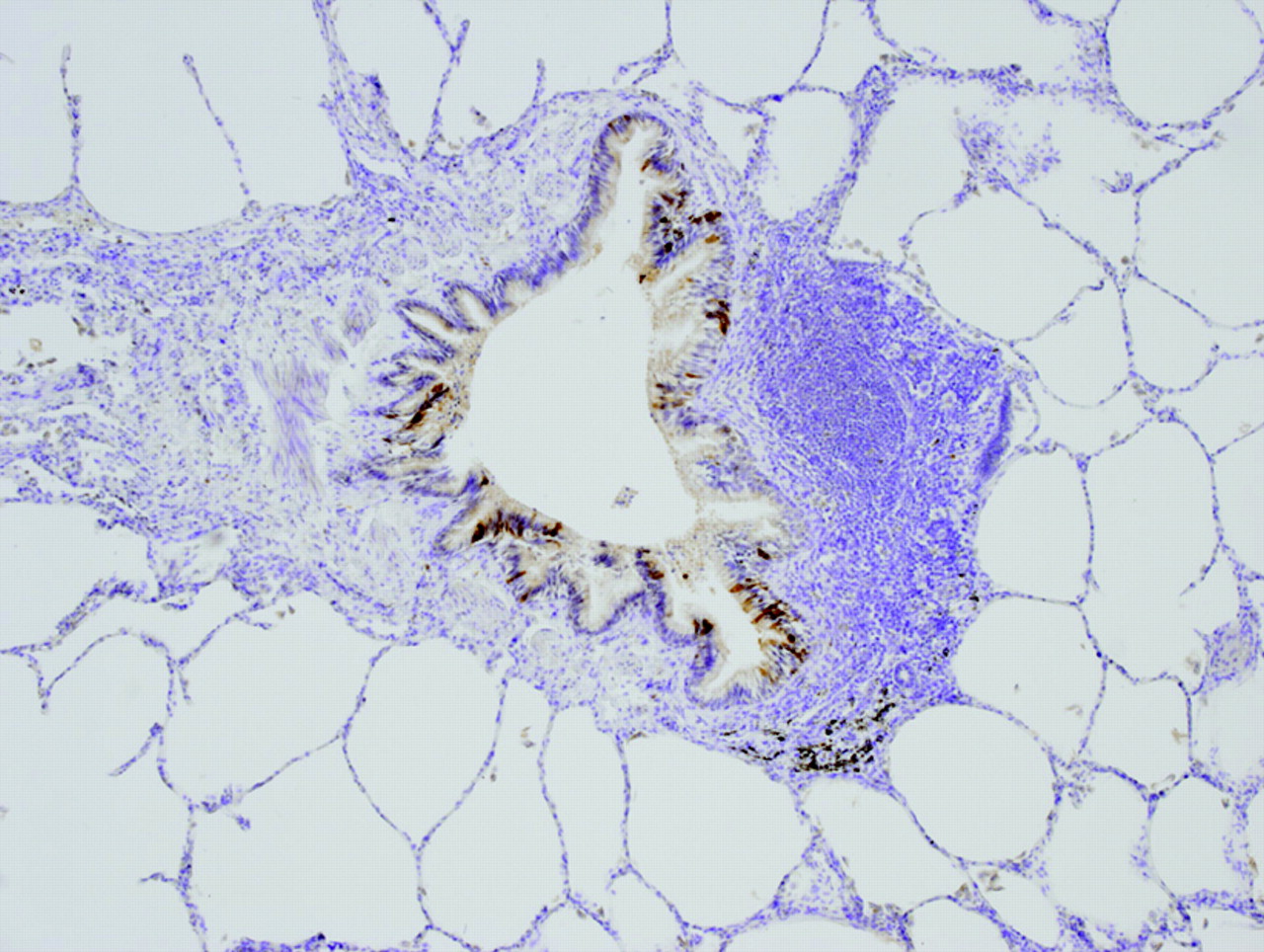
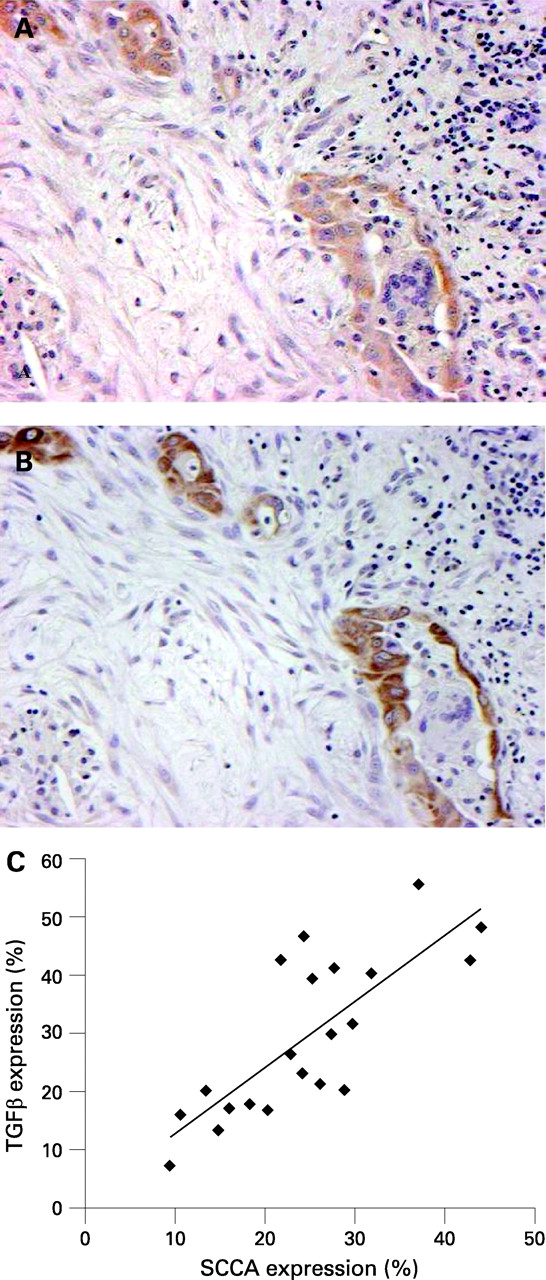
SCCA was expressed in many metaplastic alveolar epithelial cells in all UIP cases, ranging from 9.4% to 44.0%, and was normally distributed with a mean of 24.9 (9.3)% (fig 1A, 1B). Immunoassaying was mainly detected in the cytoplasm but in a few cases cytoplasmic and nuclear staining was also observed (fig 2A). Cuboidal, flattened metaplastic epithelial cells showed a wide spectrum of staining from strong to weak SCCA positivity (fig 2B) in contrast with squamous and bronchiolar metaplastic epithelial cells which frequently showed strong staining (fig 2C), more often well evident in or close to the honeycomb changes. Interstitial cells were negative for SCCA expression and a weak cytoplasmic staining was observed in some alveolar macrophages. Metaplastic epithelial SCCA positive staining was seen in only two ILDs different from IPF (non-specific interstitial pneumonia and desquamative interstitial pneumonia). The positivity was weak and mainly detected in cytoplasmic areas with a mean of 0.4 (1.3)% (from 0–5%). The pseudostratified columnar epithelial cells lining the bronchi and bronchioles often exhibited strong cytoplasmic immunoreactivity for SCCA, thus representing a good internal immunostaining control. No alveolar cells were detected in normal lung tissue from donor subjects when only some bronchial cells were marked (fig 3).



In all UIP cases, TGFβ, which often marked the same metaplastic epithelial cells positively stained for SCCA, showed a mean value of 29.8 (13.5)% (7.1–55.6%) and was significantly correlated with the expression values of SCCA (r = 0.78, p<0.0001) (fig 4A–C). TGFβ epithelial expression was occasionally seen in the control group (up to 2%).
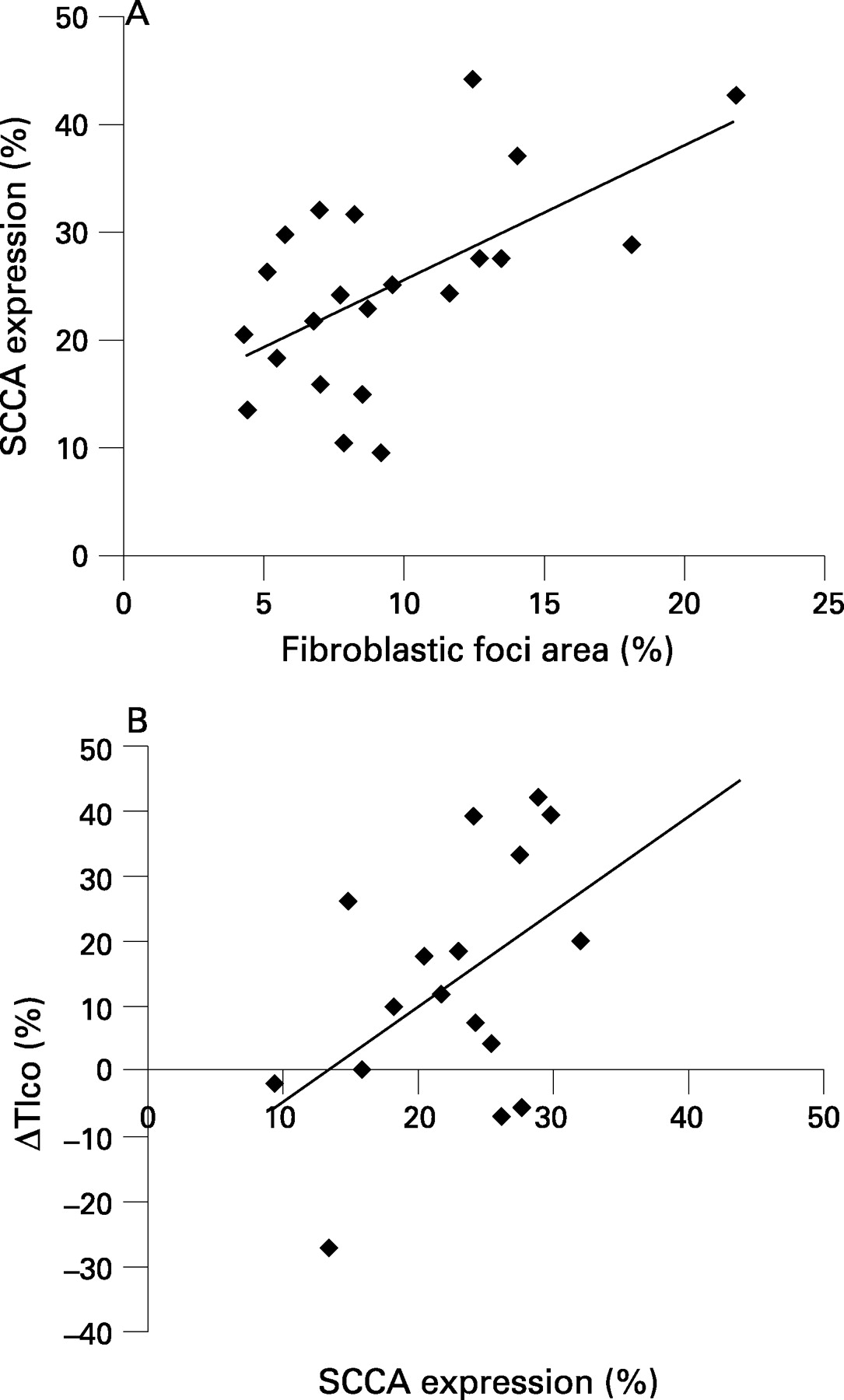
A direct correlation was observed between expression of SCCA and AFF (r = 0.49, p = 0.02) (fig 5A) and between TGFβ and AFF (r = 0.44, p = 0.04). Controlling for SCCA values, the correlation between TGFβ and AFF was no longer statistically significant (partial r = 0.10, p = 0.67). Mean SCCA values did not significantly differ both among foci score groups (F = 0.65, p = 0.53) and inflammation score groups (F = 0.36, p = 0.56). The only statistically significant relationship between SCCA values and lung clinical data variation during follow-up was observed with decreasing Tlco (ΔTlco) at 9 months (r = 0.38, p = 0.04) (fig 5B).

SCCA and TGFβ mRNAs
The expected 80 and 161 bp PCR products of SCCA and TGFβ, respectively, were detected from all pathological microdissected lung tissues, confirming epithelial transcription (data not shown).
TGFβ mRNA expression in A549 cells incubated with SCCA
Time course analysis of the effect of SCCA on TGFβ transcription in A549 cell lines is reported in fig 6. Peak induction of TGFβ transcription was achieved at 24 h, with the highest activity of SCCA at the 100 pg/ml concentration.

DISCUSSION
The serpin superfamily includes inhibitors of a number of serine proteases with roles in a variety of cellular processes, including fibrinolysis, inflammation, cell migration, adhesion and proliferation. SCCA is transcribed from the tandemly repeated genes, SCCA1 and SCCA2, which have 98% sequence identity at the nucleotide level and 92% identity at the amino acid level.16 The products of the two genes have different protease targets; SCCA1 inhibits papain-like cysteine proteases (cathepsin S, L and K)24 and SCCA 2 chymotrypsin-like serine proteases (eg, catepsin G and mast cell chymase).25 While some studies have reported increased SCCA expression (mainly in blood serum) in many tumours, particularly those with squamous cell differentiation,26 27 and in preneoplastic bronchial lesions,28 little is known about the behaviour of this serpin in a non-neoplastic clinical setting.
In the present study, we have demonstrated for the first time overexpression of SCCA in lung tissue of IPF/UIP patients compared with other forms of ILDs and normal lungs. In IPF, SCCA was abnormally secreted by metaplastic epithelial cells other than bronchial cells where it is normally expressed. The normal presence of SCCA at this level, as was demonstrated in our control cases, could have a protective function against inflammatory cells and microorganisms because SCCA 1 and 2 are inhibitors of serine and cysteine proteinase. Previous studies have reported that SCCA can have an important influence on epithelial growth through inhibition of different apoptotic pathways.29 30 The marked positivity of SCCA in the honeycomb area suggests that this site is more frequently subjected to injury favouring epithelial proliferation, which could be highly unstable when recurrent injuries occur.
Several years ago, Meyer and Liebow already showed atypical epithelial lesions in honeycombing pulmonary areas in IPF, raising the possibility that atypical epithelial lesions in IPF might be precancerous lesions.5 Squamous metaplasia in our samples showed frequent and strong staining with SCCA. It is probable that this epithelial setting represents a regeneration epithelial site of high instability at risk of neoplastic transformation. A recent in vitro study has shown overexpression of SCCA in squamous metaplastic tracheobronchial cell lines, increasing with tumour progression.31 Squamous-type carcinoma has in fact been detected in IPF/UIP lungs more frequently than in other tumour types.9
The nuclear/cytoplasmic concomitant SCCA immunoreactivity observed in our samples is difficult to interpret. Other works have recently described nuclear–cytoplasmic positive staining of serpin (maspin and SCCA) in non-small cell lung carcinoma. In this work, the nuclear maspin positivity was correlated with a better survival than with cytoplasmic staining.32 The synthesis of SCCA is thought to be essentially in the cytoplasm. However, when it is overexpressed, nuclear import might occur, thus playing a role in influencing the transcription of different growth factor genes, such as TGFβ. Significant overexpression of TGFβ was detected in our cases and interestingly it was significantly correlated with SCCA expression. The increased TGFβ transcription by SCCA observed in A549 pneumocytes confirms clinical observations detected in patients with IPF/UIP. Unfortunately, it is nearly impossible to work with primary alveolar epithelial cells, and we had to resort to the epithelial cell line A549, used in numerous studies of IPF. There are different sources of TGFβ in IPF/UIP lungs, and active TGFβ transcription was detected in many metaplastic epithelial cells obtained by microdissection of our samples. Active epithelial secretion of this profibrogenetic cytokine was first reported by Corrin and colleagues33 and subsequently by other authors,34 thus underlining the important contributing role of epithelial cells in the development/progression of the fibrotic process in IPF/UIP.
The significant correlation between expression of SCCA and extension of FF and fibrosis could be mediated through the increased transcription of the fibrotic cytokine TGFβ, confirming the role of this cytokine as one of the most important inducers of fibrotic processes in IPF/UIP. Our morphological evaluation confirms the prognostic significance of the quantitative measure of fibrosis and FF (instead of semiquantitative evaluation) in that these are the only pathological findings significantly correlated with Tlco decline and SCCA expression, as reported above. The significant correlation of SCCA with Tlco decline observed in our patients after 9 months of follow-up could be related to progressive fibrosis favoured by increased TGFβ transcription. However, it remains to be established if alveolar epithelial dysfunction could represent an important contributing factor for progressive impaired gas exchange.
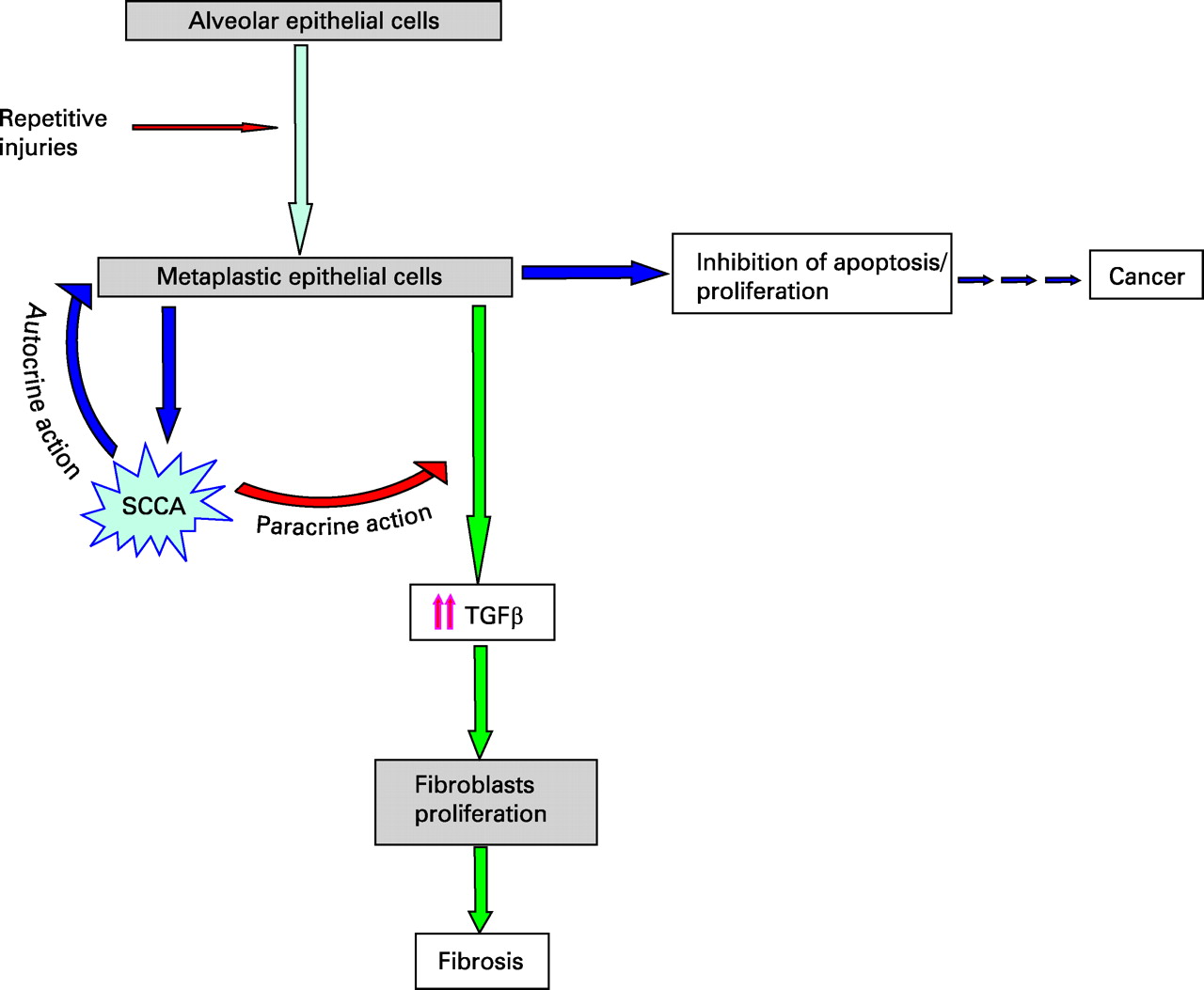
Although our findings need to be confirmed in larger case series, we consider SCCA an important molecular target in the disease as it could orchestrate two of the most peculiar aspects of the disease: this serpin could act in an autocrine way favouring epithelial proliferation and metaplastic dysplastic transformation while in a paracrine way it could influence myofibroblast proliferation and collagen synthesis through increased TGFβ transcription (fig 7). Monitoring of tissue SCCA expression during the clinical course of IPF/UIP could be useful for more precise patient stratification. It could be advisable to use a non-invasive approach such as innovative serological analysis of SCCA–immunoglobulin M complex, a more sensitive and appropriate technique35 that those used previously.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A final issue that needs to be taken into account is the possible role of SCCA in the development of lung cancer in IPF/UIP. Analysis of this specific aspect could be proven in studies of tissue samples of cancer in UIP and by using specific experimental models, such as those involving transgenic SCCA animal models recently engineered in our laboratory.
Acknowledgments
The authors thank Luca Braghetto and Laura Vignato for their excellent technical assistance and Judith Wilson for English revision.
REFERENCES
Footnotes
Funding: This study was supported by the Italian Ministry of Instruction, University and Research.
Competing interests: None.
Ethics approval: The study was approved by the Institutional Ethics Committee.