Article Text

Abstract
Introduction: Lung function impairment may be a risk factor for cardiovascular disease (CVD) events.
Objective: To determine the relationship between the severity of airflow obstruction based on modified Global Initiative on Obstructive Lung Disease (GOLD) criteria and the prevalence and incidence or recurrence of CVD in a cohort of US adults, aged 45–64 years, from 1987 to 2001.
Methods: We analysed data from 14 681 adults using logistic regression to determine the cross sectional association between lung function impairment and prevalent CVD at baseline and Cox regression to examine the prospective association of lung function impairment at baseline with CVD over 15 years of follow-up. Models were adjusted for age, sex, race, smoking, comorbid hypertension and diabetes, cholesterol levels and fibrinogen level.
Results: At baseline, the crude prevalence of CVD was higher among subjects with GOLD 2 (OR 2.9, 95% CI 2.4 to 3.6) and GOLD 3 or 4 chronic obstructive pulmonary disease (COPD) (OR 3.0, 95% CI 2.0 to 4.5), compared with normal subjects. These relative risks were greatly reduced after adjusting for covariates (OR 1.4, 95% CI 1.1 to 1.8 for GOLD 2 and OR 1.3, 95% CI 0.8 to 2.1 for GOLD 3 or 4). Similarly, the association between COPD and risk of incident or recurrent CVD was much stronger in the unadjusted models (hazard ratio (HR) 2.4, 95% CI 2.1 to 2.7 for GOLD 2 and 2.9, 95% CI 2.2 to 3.9 for GOLD 3 or 4) than in the adjusted ones (HR 1.2, 95% CI 1.03 to 1.4 for GOLD 2 and 1.5, 95% CI 1.1 to 2.0 for GOLD 3 or 4).
Conclusion: We observed a crude association between lung function impairment and prevalent and incident or recurrent CVD that was greatly reduced after adjusting for covariates, including age, sex, race, smoking, comorbid hypertension and diabetes, cholesterol levels and fibrinogen level. These data suggest that this association may be, in part, mediated through established CVD risk factors included in our adjusted models.
Statistics from Altmetric.com
Ischaemic heart disease and cerebrovascular disease are currently the top two leading causes of death worldwide, responsible for more than one-fifth of all deaths, and are projected to remain so until 2020.1 ,2 Chronic obstructive pulmonary disease (COPD) is expected to be the third leading cause of worldwide mortality by 2020 and the fifth leading cause of disability adjusted life years lost.2 This triad of cardiac disease, stroke and COPD have an enormous economic, medical and social burden on adults in the USA.3–10 Processes that result in restriction on spirometry, which comprise interstitial lung diseases, diabetes mellitus, congestive heart failure and other causes of small lung volumes, also impart significant morbidity and mortality in the US.6 ,7 The role of systemic inflammation and systemic inflammatory markers such as C reactive protein, fibrinogen and tumour necrosis factor α may be important in all of these disease processes.11–15
Cardiovascular mortality has been shown to be up to twofold higher in patients with COPD than in a matched population without COPD.5 ,16 Previous studies have linked lung function impairment with the risk of developing cardiovascular disease and stroke, even after adjusting for factors such as body mass index (BMI), physical activity, hypertension, diabetes and smoking status.5 ,17–23 However, lung function impairment in these studies has been classified by quartiles of forced expiratory volume in 1 s (FEV1) or mean FEV1 which are not routinely used clinically to assess the severity of impairment.18 ,20 ,21
In 2001, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) was formed to improve investigation and management of this complex disease and treatment strategies have been recommended based on GOLD staging.24 Our goal was to examine the prevalence, incidence and recurrence of cardiac events and stroke in the Atherosclerosis Risk in Communities (ARIC) cohort of adults, aged 45–64 years, and followed from 1987 to 2001 using a modification of the GOLD classification of lung function impairment.
METHODS
Study population
The ARIC study was initiated in 1987 as a longitudinal, population based study of the aetiology and clinical sequelae of atherosclerosis. Study protocols were approved for protection of human subjects. Participants were selected from the entire population by probability sampling from four US communities: Forsyth County, North Carolina; Minneapolis, Minnesota; Washington County, Maryland; and Jackson, Mississippi (where only African Americans were sampled). Specific details of the ARIC study are published elsewhere.25 Our analysis was limited to ARIC participants aged 45–64 years at baseline, who provided information on respiratory symptoms and diagnoses, cardiovascular events or stroke, and medical history, had lipid profiles available and who underwent adequate pulmonary function testing at the baseline examination. Only those participants for whom follow-up data were available were analysed (n = 14 681).
Pulmonary function data
Spirometry was conducted using contemporary American Thoracic Society guidelines.26 ,27 We developed sex and race specific internal prediction equations for FEV1 and FVC following standard methods previously described.28 We defined a subject as having a respiratory symptom if they reported cough, phlegm, dyspnoea or wheeze.
A modification of the GOLD criteria was used to classify subjects according to their stage of COPD24 ,29: GOLD 3 or 4 (FEV1/forced vital capacity (FVC) <0.70 and FEV1<50% predicted), GOLD 2 (FEV1/FVC <0.70 and FEV1 ⩾50 to <80% predicted), GOLD 1 (FEV1/FVC <0.70 and FEV1 ⩾80% predicted), restricted (FEV1/FVC ⩾70% and FVC <80% predicted), GOLD 0 (presence of respiratory symptoms in the absence of any lung function abnormality) and no lung disease (table 1). Bronchodilator response was not evaluated so classification was based on “prebronchodilator” level. Only the baseline pulmonary function data were used to stratify participants, and they remained in these groups for interpretation of prevalent risk and incident or recurrent events.
Ascertainment of baseline cardiovascular status and incident or recurrent events
Cardiovascular disease (CVD) events included cardiac disease and stroke. CVD was considered present at baseline if the subject self-reported a myocardial infarction, coronary artery bypass graft, angioplasty, had been hospitalised for a myocardial infarction, had evidence on the ECG of a myocardial infarction or had a self-reported stroke at the baseline examination (table 1).25 Incident cardiac events were defined as a definite or probable hospitalised myocardial infarction, coronary heart disease death or myocardial infarction that was detected at follow-up by ECG changes (major Q wave or a minor Q wave with ischaemic ST-T changes or a myocardial infarction by computerised NOVACODE criteria,30 confirmed by side-to-side ECG comparison) who did not meet this criterion at baseline.31 ,32 CVD recurrence was defined as a definite or probable hospitalised myocardial infarction, coronary heart disease death or myocardial infarction that was detected at follow-up by ECG changes (major Q wave or a minor Q wave with ischaemic ST-T changes or a myocardial infarction by computerised NOVACODE criteria, confirmed by side-to-side ECG comparison) in those participants identified as having baseline cardiovascular disease. Stroke was defined according to published criteria related to the occurrence and duration of neurological signs and symptoms, the results of neuroimaging and diagnostic procedures, and treatments provided.10 ,33 The analysis was restricted to definite or probable ischaemic stroke only.
Variable definitions
Participants were classified as “former smokers” or “current smokers” based on positive responses to “Have you ever smoked cigarettes?” and “Do you now smoke cigarettes?”, respectively. Pipe or cigar smokers were considered as “smokers” (ie, subjects who denied current cigarette smoking but reported current or former pipe or cigar smoking were considered current or former smokers, respectively). Never smokers were defined as persons who had not smoked more than 400 cigarettes in their lifetime and had never smoked pipes or cigars. Diabetes mellitus was defined as a baseline glucose level ⩾126 mg/dl or use of a medication for diabetes or high blood sugar. Subjects were classified as having hypertension if they either reported a physician diagnosis of hypertension, were on treatment for hypertension or had evidence of hypertension at the examination (either a diastolic blood pressure ⩾90 mm Hg or a systolic blood pressure ⩾140 mm Hg, based on three measurements). BMI was calculated as weight divided by height squared (kg/m2), measured at the baseline examination. Education level was categorised as less than high school, completion of high school or more than high school. High density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C) and fibrinogen levels were measured in serum samples.34
Analysis
All analyses were conducted with SAS V.9.1 (SAS Institute, Cary, North Carolina, USA), SUDAAN V.9.0 (RTI, Research Triangle Park, North Carolina, USA) and SPSS V.10 (SPSS, Chicago, Illinois, USA).
Our primary outcome of interest was incidence or recurrence of cardiac events or stroke that occurred during the study period. Secondary outcomes were the relationship between prevalent CVD and lung function impairment at the baseline examination and the relationship between lung function impairment and CVD in the study population stratified by gender, age, race and smoking status. For CVD events, censoring occurred on the first CVD related hospitalisation or event, death or the date the person was last known to be alive. We developed Cox proportional hazards models using the procedure SURVIVAL in SUDAAN. Plots of the log–log survival curves for each covariate were produced to ensure that the proportional hazards assumptions were satisfied. Age, sex, race, smoking status, pack-years of smoking, BMI, education level, HDL-C, LDL-C, fibrinogen, diabetes mellitus and hypertension at baseline were included in the adjusted models. Analyses were also performed on subsets of subjects stratified by sex, race, smoking status and age category, and interactions were evaluated between these variables and our modified GOLD categories.
RESULTS
Our analysis included 14 681 of the initial 15 732 ARIC cohort participants. Excluded subjects did not differ significantly with regard to age, sex or smoking status (p>0.05 for all) from included subjects, but were more likely to be of black race (p<0.01). The demographic distribution of the analysis cohort is included in table 2. Baseline 5 year age groups were evenly distributed from 45 to 64 years. The cohort was 55.2% female and 74.2% white. Diabetes was present in 11.2%, hypertension in 34.0%, overweight (BMI 25–29) in 39.4% and obesity (BMI ⩾30) in 27.1%. Mean HDL-C level was 52.0 (SE 0.1) mg/dl, mean LDL-C was 137.7 (0.3) mg/dl and mean fibrinogen level was 303.3 (SE 0.5) mg/dl.
The baseline prevalence of CVD was 6.0% and higher among those with advanced age, male sex, presence of diabetes and hypertension, higher BMI and lower education level (table 2). The prevalence was also increased among current or former smokers and related to the number of pack-years. In the unadjusted model, the prevalence of CVD was significantly higher in those with GOLD 2 (odds ratio (OR) 2.9, 95% confidence interval (CI) 2.4 to 3.6) and GOLD 3 or 4 COPD (OR 3.0, 95% CI 2.0 to 4.5), compared with normal subjects. Adjustment for covariates decreased the relative risk for prevalent disease compared with the unadjusted model (OR 1.4, 95% CI 1.1 to 1.8 for GOLD 2 and OR 1.3, 95% CI 0.8 to 2.1 for GOLD 3 or 4). The highest overall multivariate association between baseline CVD and lung function impairment was observed for those classified as restricted (OR 2.3, 95% CI 1.9 to 2.9).
The association between lung function impairment and risk of incident and recurrent CVD events over 15 years are shown in table 3. Subjects with baseline CVD were more likely to have a CVD event (41.8 events vs 8.1 events per 1000 person years) and to die (34.9 deaths vs 8.8 deaths per 1000 person years) than those without baseline CVD. Subjects with GOLD 2 (hazard ratio (HR) 2.4, 95% CI 2.1 to 2.7) and GOLD 3 or 4 COPD (HR 2.9, 95% CI 2.2 to 3.9) had the highest univariate risk of CVD events. This finding was decreased in the adjusted models (HR 1.2, 95% CI 1.03 to 1.4 for GOLD 2 and 1.5, 95% CI 1.1 to 2.0 for GOLD 3 or 4 COPD).
We did not find any significant interaction between the GOLD category and smoking status, age category, race or sex (p>0.10 for each) for our primary outcome of time to CVD event. When the cohort was stratified by smoking status, the rate of CVD events and deaths was higher among current smokers (14.6 CVD events and 16.7 deaths per 1000 person years) than among former (10.0 CVD events and 9.8 deaths per 1000 person years) or never smokers (6.2 CVD events and 6.1 deaths per 1000 person years) (table 4). In the stratified analyses, the relation between lung function impairment, in the adjusted models, was weakest among the current smokers, but there was a large degree of overlap between all three smoking categories (table 4). The tables examining the relationship between CVD events and lung function impairment stratified by gender, age and race are available as an online supplement (supplementary ⇑⇑tables 1–3). Men had twice the rate of CVD events than women (13.9 vs. 6.5 per 1000 person years), older subjects (age 55–64 years) had twice the rate of events than younger subjects (13.4 vs 6.5 per 1000 person years) and black patients had a slightly higher rate of events than white subjects (12.1 vs 8.9 per 1000 person years).
Figure 1 depicts the Kaplan–Meier curve of the relation between lung function impairment and incident or recurrent CVD, while fig 2 shows the fully adjusted Cox proportional hazards model curves.

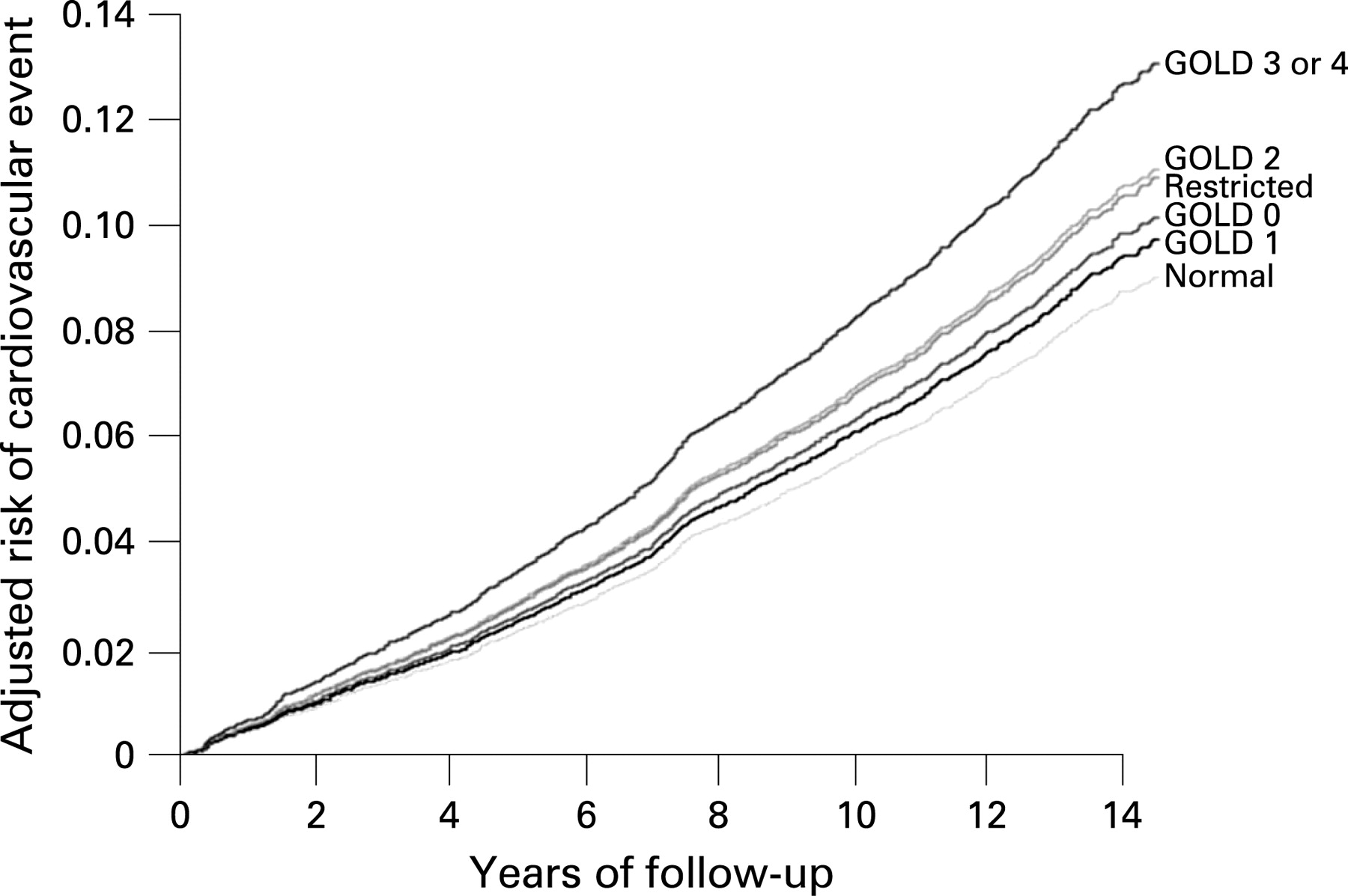
{kind=link}
{kind=link}
DISCUSSION
In this analysis of a large, prospective, population based cohort, lung function impairment was associated with an increased risk of having or developing CVD in adults; the highest risks were observed among those with GOLD 2 (moderate) and GOLD 3 or 4 (severe/very severe) COPD. After adjusting for multiple covariates, including age, sex, race, smoking status, diabetes, hypertension, cholesterol levels and fibrinogen levels, the relation between lung function impairment and CVD was reduced, suggesting that some of this relation may be mediated through these other factors.
Previous research suggests that systemic inflammation present in COPD leads to the increased CVD risk, and that treatment aimed at decreasing inflammation in those with COPD may decrease the development of cardiovascular disease or reduce event recurrence. Vascular inflammation may also contribute to impaired airway vascular smooth muscle relaxation in COPD. Treatment with agents that affect systemic inflammation or vascular disease such as corticosteroids, statins, angiotensin converting enzyme inhibitors or angiotensin receptor blockers have been shown to alter the prognosis of patients with COPD,35–39 and one retrospective meta-analysis has suggested a reduction in all-cause mortality in patients with COPD treated with inhaled corticosteroids.40 Our finding that the risk of CVD was greatly reduced in the models that adjusted for HDL-C, LDL-C, fibrinogen and comorbid disease suggests that part of the CVD risk seen in COPD is mediated by these other factors that may be responsive to intervention.
Although low grade chronic systemic inflammation likely contributes to the association between lung function impairment and CVD, factors such as the role of the lungs in the capture and elimination of external toxic agents may also be important.20
Previous research has shown a relationship between lung function impairment based on quartile of FEV1 per cent predicted or diagnosed COPD and incident cardiac disease or ischaemic stroke, with an increased risk primarily noted within population subsets, such as whites patients,18 women20 ,41 and younger populations.23 These analyses, however, were not able to make a distinction between those with mild, moderate or severe impairment in lung function or separate out those with restrictive impairment. Our study, however, used the clinically relevant GOLD staging to classify COPD, which does make this distinction.
An interesting finding in our study was the association between restriction on spirometry and CVD risk. As shown in table 2, restriction was a stronger risk factor for CVD than either GOLD 2 or GOLD 3 or 4 COPD, the risk for incident or recurrent CVD in those with restriction was similar to that seen in GOLD 2 COPD. Neither the degree nor causes of restricted lung disease were examined in this analysis, but future studies may be undertaken to further investigate the relationship between CVD and restriction on spirometry.
Strengths of this study include the large cohort of patients, length of follow-up and well defined outcome events. Even though this was a very large sample, certain subgroups had small numbers. For example, the number of subjects with prevalent CVD was 150 for GOLD 2 and 29 for GOLD 3 or 4. Also, subjects were classified based on initial pulmonary function tests which may not have represented a true baseline, and the restriction category was categorised based on a decreased FVC with a normal FEV1/FVC ratio rather than the gold standard, total lung capacity measurements. The effect of lung function impairment on CVD outcomes was decreased in the fully adjusted models, suggesting that additional confounders that were not included in the analysis might explain these findings. Conversely, it is also possible that our models “over adjusted”. For example, if the effect of lung function impairment on CVD is mediated through inflammation or comorbid disease, then adjusting for these factors might mask the true association between lung function impairment and CVD.
CONCLUSION
We observed an association between lung function impairment and risk of prevalent, and incident or recurrent, CVD in a large population based cohort. This association was reduced in models that adjusted for age, sex, race, smoking status, diabetes mellitus, hypertension, cholesterol levels and fibrinogen levels, suggesting that these effects may be mediated in part through these other factors. The implications of these findings are that clinicians should consider spirometry in their patients with CVD or follow markers of systemic inflammation, such as C reactive protein, in COPD patients to help assess or manage their CVD risk. Future studies may be directed towards better identifying reasons for the linkage between lung function impairment and CVD risk and determining if interventions can improve outcomes.
Acknowledgments
The authors thank the staff and participants in the Atherosclerosis Risk in Communities Study for their important contributions. The ARIC Study is conducted and supported by the National Heart Lung and Blood Institute (NHLBI) in collaboration with the ARIC Investigators. This manuscript was not prepared in collaboration with investigators of the ARIC and does not necessarily reflect the opinions or views of the ARIC or the NHLBI.
REFERENCES
Supplementary materials
web only tables 63/7/599
Files in this Data Supplement:
Footnotes
Supplementary tables 1–3 are published online only at http://thorax.bmj.com/content/vol63/issue7
Funding: Funded by a research grant from GlaxoSmithKline.
Competing interests: GW, KD, and VK are employees of GlaxoSmithKline (GSK). DM has received research funding from GSK, Pfizer and Novartis and is a consultant to GSK, Pfizer, AstraZeneca, Boehringer-Ingleheim, Dey and Sepracor. AJ has no competing interests.
Ethics approval: Ethics approval was obtained.