Article Text

Abstract
Background: The obstructive sleep apnoea/hypopnoea syndrome (OSAHS) is associated with hypertension and increased cardiovascular risk, particularly when accompanied by marked nocturnal hypoxaemia. The mechanisms of these associations are unclear. We hypothesised that OSAHS combined with severe nocturnal hypoxaemia causes impaired vascular function that can be reversed by continuous positive airways pressure (CPAP) therapy.
Methods: We compared vascular function in two groups of patients with OSAHS: 27 with more than 20 4% desaturations/h (desaturator group) and 19 with no 4% and less than five 3% desaturations/h (non-desaturator group). In a randomised, double blind, placebo controlled, crossover trial, the effect of 6 weeks of CPAP therapy on vascular function was determined in the desaturator group. In all studies, vascular function was assessed invasively by forearm venous occlusion plethysmography during intra-arterial infusion of endothelium dependent (acetylcholine 5–20 μg/min and substance P 2–8 pmol/min) and independent (sodium nitroprusside 2–8 μg/min) vasodilators.
Results: Compared with the non-desaturator group, patients with OSAHS and desaturations had reduced vasodilatation to all agonists (p = 0.007 for all). The apnoea/hypopnoea index and desaturation frequency were inversely related to peak vasodilatation with acetylcholine (r = −0.44, p = 0.002 and r = −0.43, p = 0.003) and sodium nitroprusside (r = −0.42, p = 0.009 and r = −0.37, p = 0.02). In comparison with placebo, CPAP therapy improved forearm blood flow to all vasodilators (p = 0.01).
Conclusions: Patients with OSAHS and frequent nocturnal desaturations have impaired endothelial dependent and endothelial independent vasodilatation that is proportional to hypoxaemia and is improved by CPAP therapy. Impaired vascular function establishes an underlying mechanism for the adverse cardiovascular consequences of OSAHS.
Statistics from Altmetric.com
The obstructive sleep apnoea/hypopnoea syndrome (OSAHS) is caused by upper airways obstruction during sleep leading to hypopnoea or apnoea events. This leads to a symptom complex characterised by sleepiness and impaired cognitive function in conjunction with loud snoring.1 The arousals at the terminations of apnoeas and hypopnoeas are associated with transient rises in blood pressure.2 Obstructive sleep apnoea is associated with sustained hypertension in animal models3 and in clinical epidemiological4 and interventional5 ,6 studies. The elevation in blood pressure is most marked in those with more severe sleep related hypoxaemia. Recent evidence indicates that OSAHS is associated with an increased risk of cardiovascular6 and cerebrovascular disease.7 ,8
The mechanism of the association between OSAHS, hypertension and cardiovascular disease is unclear. OSAHS is associated with increased sympathetic tone both in association with arousals from sleep9 and during daytime wakefulness.10 ,11 This could also be associated with activation of the renin–angiotensin–aldosterone system,12 alteration of baroceptor control,9 oxidative stress,13 increased inflammatory responses14 and increased hypercoagulability.15
Altered endothelial and vascular function may be the important link between OSAHS and cardiovascular disease. Current contradictory evidence reports either no effect,16 impaired endothelium dependent vasodilatation,17 impaired endothelium independent vasodilatation18 or even vasoconstriction.16 These findings are limited because of small group sizes (n = 8–10 per group), lack of correlation with nocturnal hypoxaemia and variable use of control groups.
The aims of this study were to determine whether endothelial function is altered in patients with OSAHS and whether potential alterations in endothelial function correlate with the degree of sleep related hypoxaemia. Finally, we sought to establish the reversibility of any alterations in vascular function by using a double blind, randomised, placebo controlled, crossover trial of continuous positive airways pressure (CPAP) therapy.
METHODS
Subjects
Fifty-one patients with OSAHS, Epworth Sleepiness Score >10, aged 34–62 years participated in this study. Patients with clinical evidence of atherosclerotic vascular disease, asthma, respiratory failure or an inter-current illness were excluded from the study. OSAHS was diagnosed on the basis of symptoms, an Epworth Sleepiness Score19 >10 and an apnoea–hypopnoea index (AHI) of greater than 15/h on overnight polysomnography. Patients were stratified as desaturators (two major symptoms of OSAHS, AHI >15, >20 of 4% desaturations/h) or non-desaturators (two major symptoms of OSAHS, AHI >15, <5 of 3% desaturations/h and no 4% desaturations/h).
Study design
Study 1: Comparison of baseline vascular function in desaturators versus non-desaturators
All patients with OSAHS (n = 51) attended for a screening visit that included a clinical history, physical examination and polysomnography. Desaturators and non-desaturators were identified a priori according to the polysomnographic findings from an inpatient sleep study, and all were invited to attend for a vascular assessment: 27 desaturators and 19 non-desaturators completed the study protocol (fig 1).
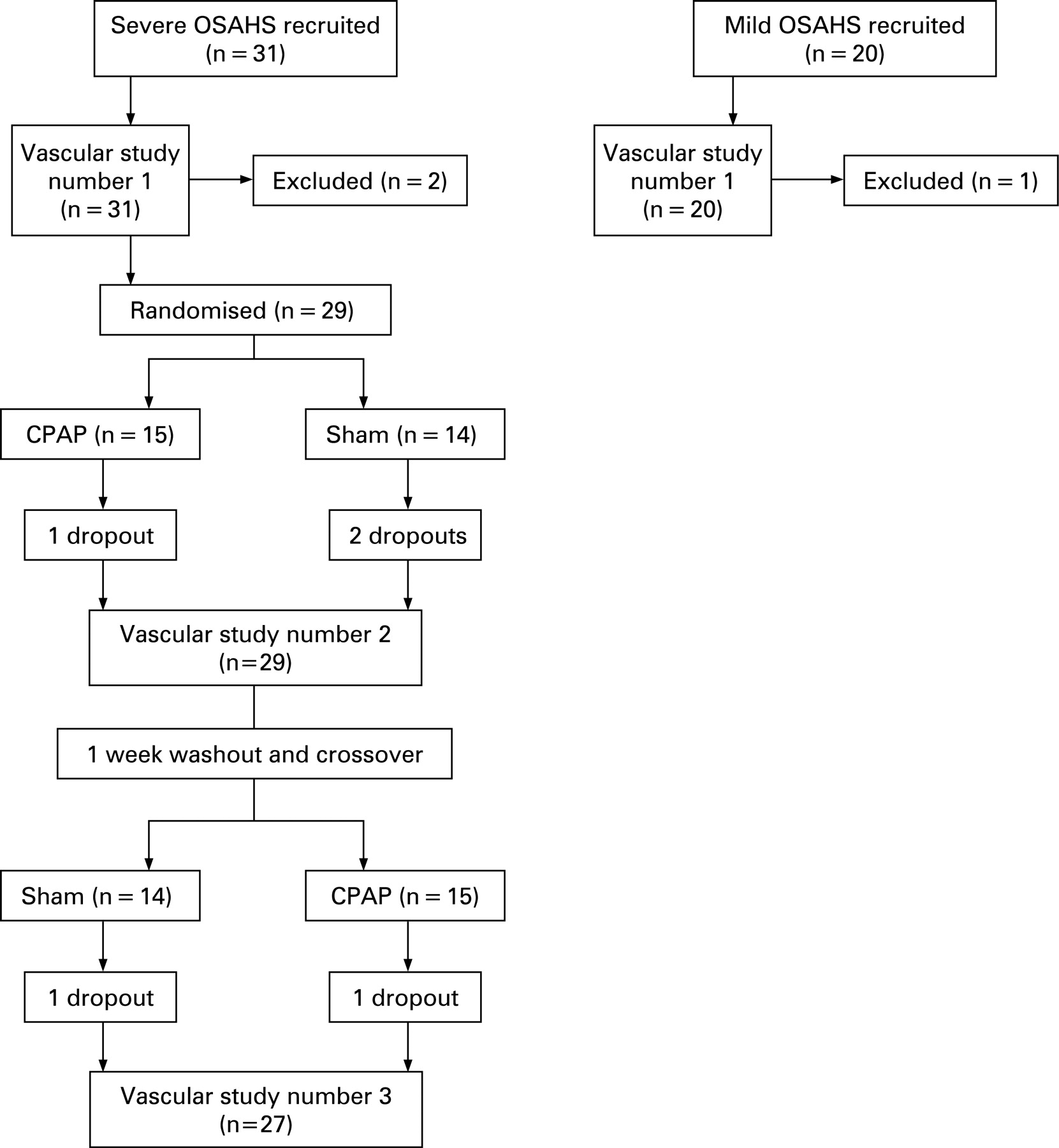
Study 2: Randomised placebo controlled trial of CPAP in desaturators
Patients with OSAHS and significant nocturnal desaturation (n = 27) had inhospital CPAP autotitration using a ResMed Spirit (ResMed, Poway, California, USA). The next morning they were randomised in a double blind, crossover study to receive 6 weeks of CPAP at the fixed pressure determined from the CPAP titration, and 6 weeks of sham CPAP with a 1 week washout period between treatment periods. Patients underwent a repeat vascular assessment at the end of both treatment phases (fig 1). Patients and researchers were blinded to the randomised treatment allocation.
Vascular assessment
All patients abstained from alcohol for 24 h and from food, tobacco and caffeine containing drinks for at least 4 h before each vascular study. Studies were carried out in a quiet temperature controlled room maintained at 22–24°C with subjects lying supine.
Patients underwent brachial artery cannulation with a 27 standard wire gauge steel needle under controlled conditions. Following a 30 min baseline saline infusion, acetylcholine at 5, 10 and 20 μg/min (endothelium dependent vasodilator; Clinalfa AG, Bubendorf, Switzerland), substance P at 2, 4 and 8 pmol/min (endothelium dependent vasodilator; Clinalfa AG) and sodium nitroprusside at 2, 4 and 8 μg/min (endothelium independent vasodilator; David Bull Laboratories, UK) were infused for 6 min at each dose. The three vasodilators were separated by 20 min saline infusions and given in a randomised order, although this order was kept constant on each visit for each individual subject.
Forearm blood flow was measured in the infused and non-infused arms by venous occlusion plethysmography using mercury-in-silastic strain gauges, as described previously.20 Supine heart rate and blood pressure in the non-infused arm were monitored at intervals throughout each study using a semi-automated non-invasive oscillometric sphygmomanometer.
Data analysis and statistics
Plethysmographic data were determined as described previously.11 All data were analysed, finalised and locked by researchers blind to treatment type before treatment codes were assigned to the data set. Continuous variables are reported as mean (SEM). Statistical analyses were performed with GraphPad Prism (Graph Pad Software) using analysis of variance (ANOVA) with repeated measures and two tailed Student’s t test where appropriate.
RESULTS
Study 1: Desaturators versus non-desaturators
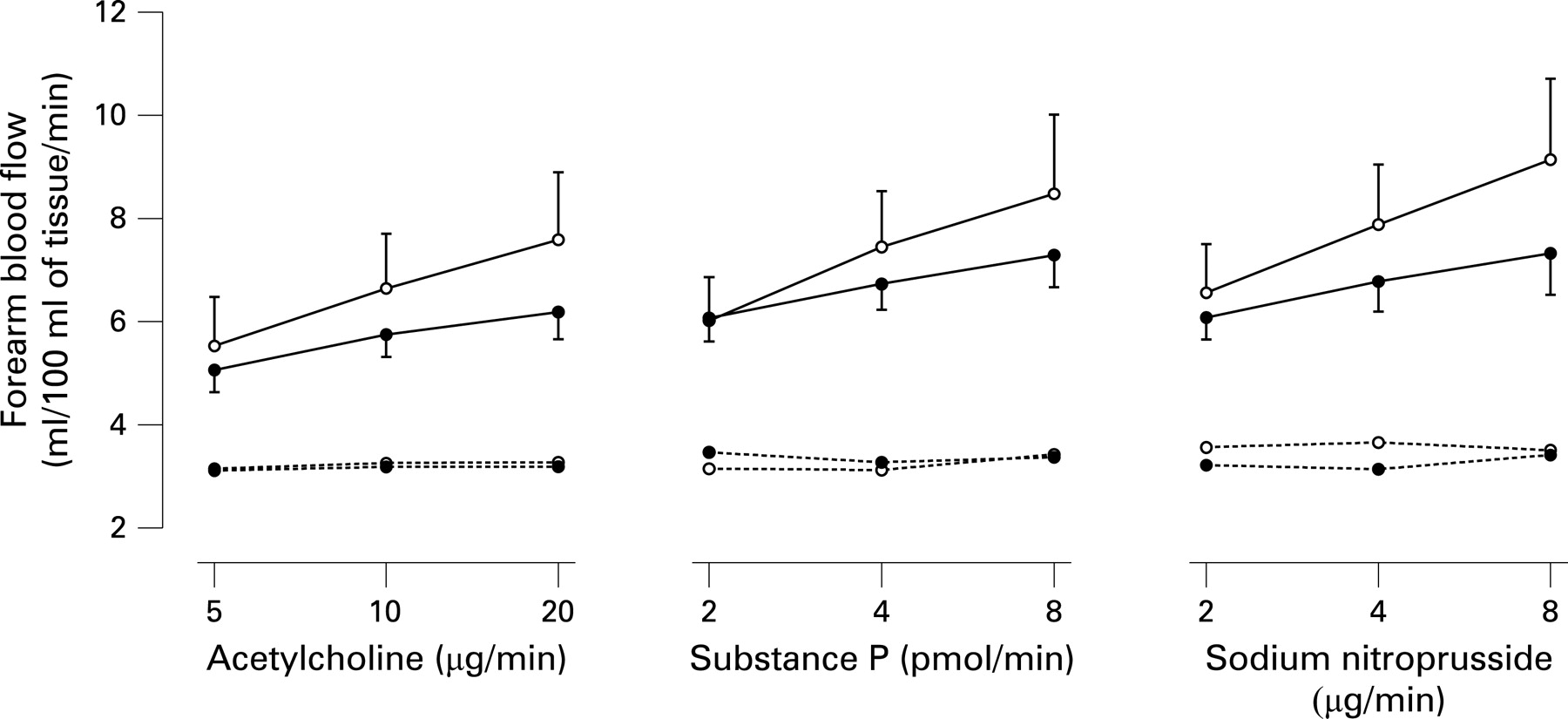
Desaturators had greater AHI than non-desaturators (63 (5) vs 21 (1); p<0.0001). The patient groups were otherwise well matched except for body mass index, where the desaturators were more obese (37 (1) vs 30 (1) m2/kg; p = 0.0003). There were no differences in resting heart rate, blood pressure or baseline forearm blood flow between desaturators and non-desaturators (table 1).
Acetylcholine, substance P and sodium nitroprusside caused a dose dependent increase in forearm blood flow in all patients (p<0.001). The increase in blood flow was blunted in desaturators compared with non-desaturators (fig 2) for each vasodilator: acetylcholine (p<0.001), substance P (p = 0.007) and sodium nitroprusside (p<0.001). Maximal vasodilatation was negatively correlated with AHI (fig 3A–C) and desaturation frequency (fig 3D–F).


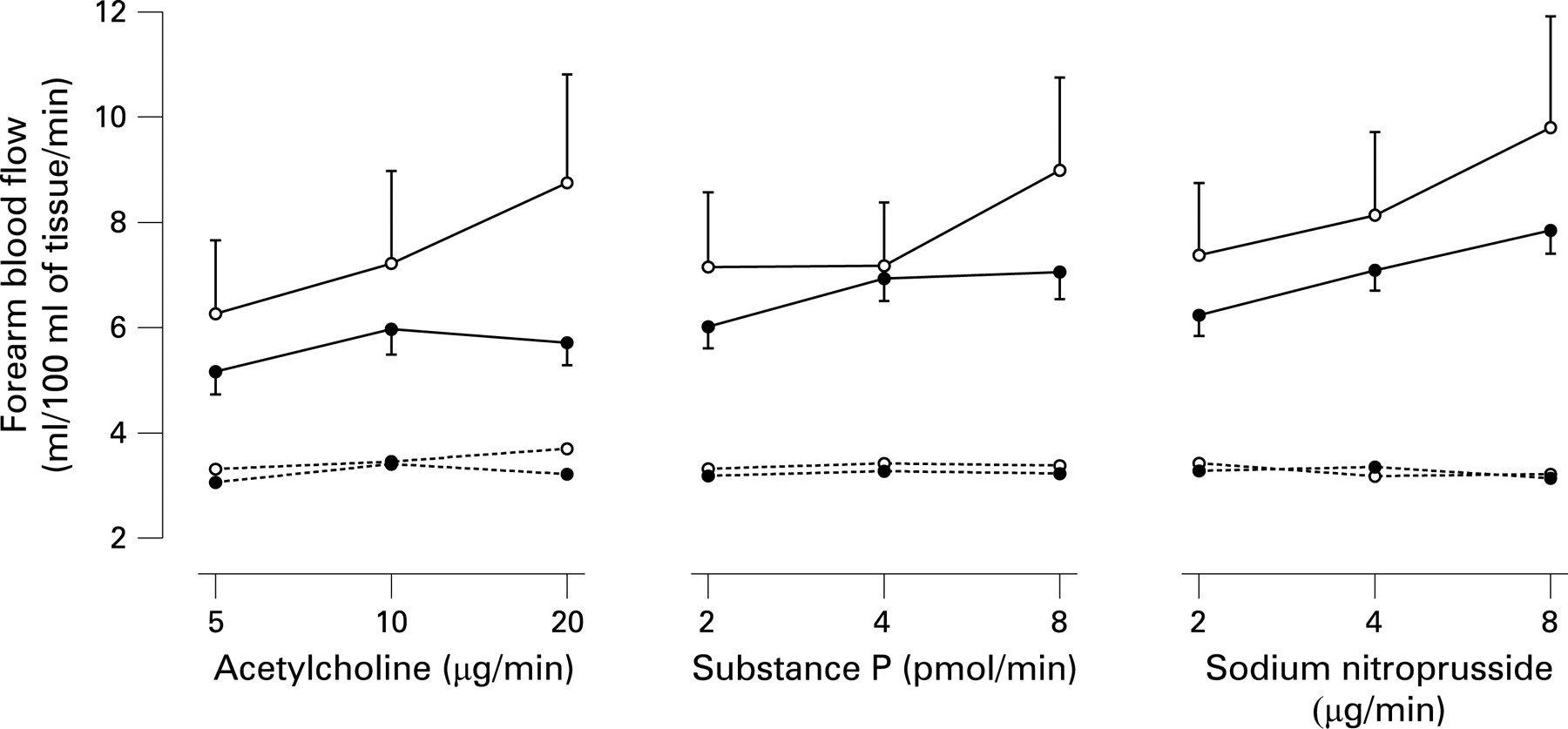
As the desaturators were heavier than the non-desaturators, a post hoc analysis was performed in which the five heaviest desaturators and four lightest non-desaturators were excluded—these deletions were made without knowledge of the patient’s vascular function. While the resulting groups (22 desaturators, 15 non-desaturators) had similar body mass indices (34.2 (SEM 1.1) and 31.4 (0.9) kg/m2; p = ns), vasodilatation remained impaired in the desaturators compared with the non-desaturators: acetylcholine (p = 0.0002), substance P (p = 0.009) and sodium nitroprusside (p = 0.005).
Study 2: Randomised, placebo controlled trial
Treatment with CPAP or sham CPAP for 6 weeks did not affect resting heart rate, blood pressure or baseline forearm blood flow (table 2). On an intention to treat basis, compliance for the CPAP limb of the study was 4.49 (0.4) h, and compliance for the sham CPAP limb of the study was 3.08 (0.48) h (p = 0.015, two tailed t test).
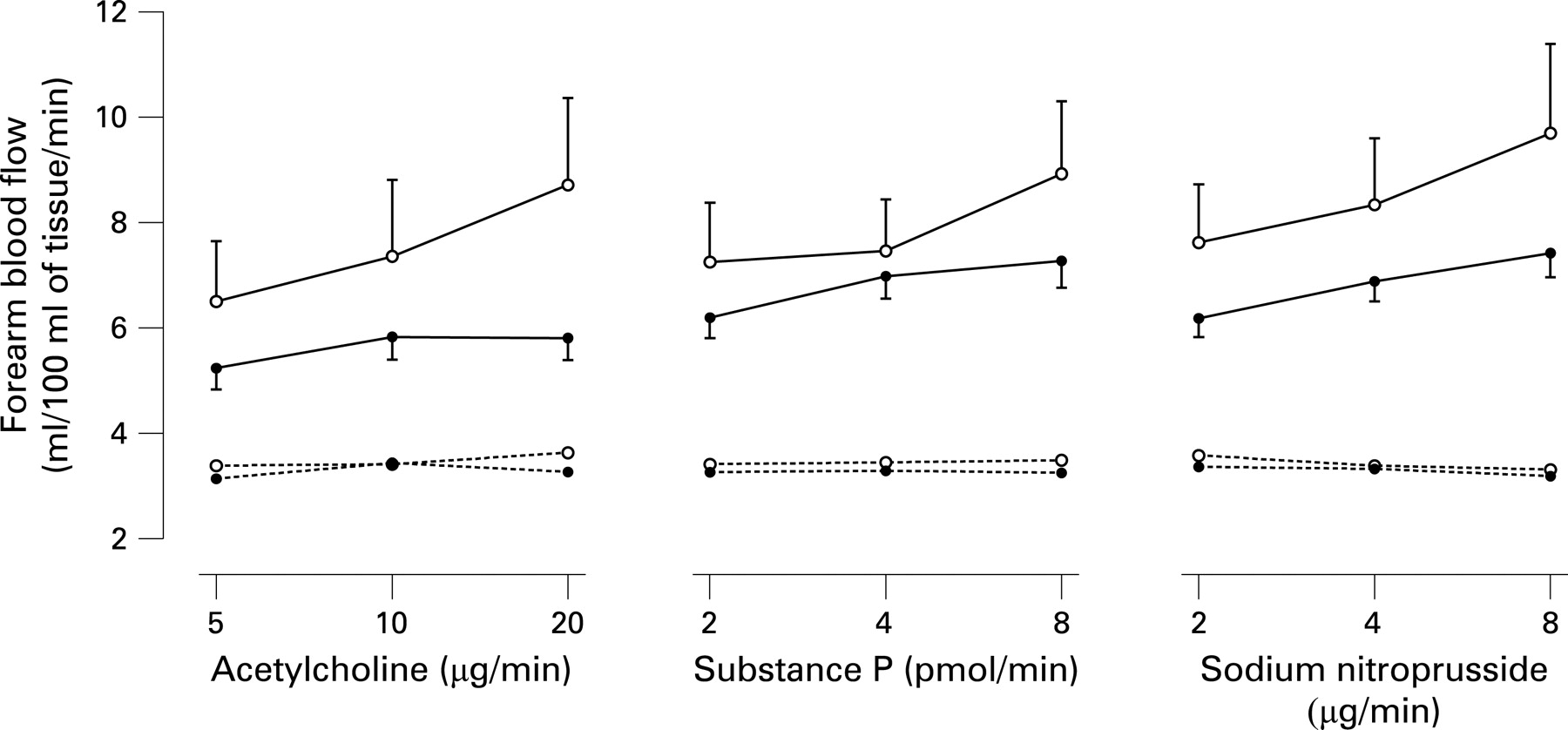
Intrabrachial infusions of acetylcholine, substance P and sodium nitroprusside caused dose dependent increases in forearm blood flow at each visit (p<0.001) that was unaffected by sham CPAP (data not shown). In comparison with results after sham CPAP, treatment with CPAP for 6 weeks improved forearm blood flow to all vasodilators (fig 4): acetylcholine (p = 0.002), substance P (p = 0.01) and sodium nitroprusside (p = 0.003).
DISCUSSION
We have demonstrated that patients with OSAHS have markedly impaired vascular function that is proportional to the degree of hypoxaemia. Using a rigorous double blind, randomised, placebo controlled, crossover trial, we have further demonstrated that CPAP therapy resulted in a clear improvement in vascular function in patients with OSAHS. Together these important and novel findings suggest that vascular dysfunction is related to disease severity in OSAHS, and that effective treatment with CPAP can improve vascular function and consequently reduce the associated cardiovascular complications.
Vascular dysfunction in OSAHS
Our findings add to the evidence base that OSAHS is associated with vascular dysfunction and disease. Our study represents the largest investigation of vascular function in patients with OSAHS. The study population is ∼3-fold larger than previous studies15–17 and we have incorporated the use of two distinct endothelium dependent vasodilators. We have found a marked impairment in endothelium dependent and independent vascular reactivity in patients with OSAHS. Given the associations with hypoxaemia, our findings also suggest that severity of OSAHS directly affects vascular reactivity with greater impairment in more severely desaturating patients (fig 3).
Animal models have suggested that hypoxia,21 cyclical hypoxia and reoxygenation22 can have detrimental vascular effects; existing evidence23 suggests that vascular dysfunction can be induced by hypoxia in susceptible individuals. We therefore speculate that the adverse vascular effects of OSAHS are mediated through nocturnal hypoxaemia.
Effect of CPAP on vascular dysfunction in OSAHS
Previous studies into the effect of treatment in OSAHS on vascular function have been either observational24–26 or had no placebo control.24 ,25 ,27 We have conducted a double blind, randomised, placebo controlled, crossover trial that maximises the study power while minimising the potential for treatment bias. Our findings provide robust evidence that OSAHS related dysfunction of vasomotor tone is reversible with CPAP within 6 weeks of initiating therapy. This provides a potential explanation for our own5 and other6 observations that CPAP lowers blood pressure most in severely desaturating patients with OSAHS.
In a subgroup of patients with OSAHS and hypertension, blood pressure does not fall appropriately during sleep (“non-dippers”).28 This may lead to increased left ventricular mass29 and an increased risk for cardiovascular events.30 These patients have most to gain from CPAP use, by avoiding the vascular dysfunction associated with OSAHS, mediated through repetitive hypoxaemia.
Mechanism of vascular dysfunction
Impaired endothelium dependent and independent function in the forearm vascular bed is associated with an increased risk of acute cardiovascular events, including cardiac death.31 We initially hypothesised that endothelial dependent mechanisms alone were responsible for vasomotor dysfunction in the OSAHS. However, our findings suggest that both endothelium dependent and independent mechanisms are impaired. It is unclear whether the observed impairment is mediated primarily by the endothelium or is a result of vascular smooth muscle dysfunction.
Reduced nitric oxide bioavailability32 in the presence of increased systemic vascular oxidative stress33 is an attractive hypothesis. Here, increased consumption of nitric oxide, whether it is endogenously derived from endothelial nitric oxide synthase or from an exogenous source, such as sodium nitroprusside, would explain the observed impairment to both endothelial dependent and independent vasodilators. The endothelium is a major target of oxidative stress, which plays an important role in the pathophysiology of cardiovascular disease. In OSAHS, recurrent episodes of hypoxaemia followed by reoxygenation may trigger oxidative stress and endothelial damage. Urinary 8-isoprostane concentrations are elevated in patients with moderate–severe OSAHS, suggesting that the syndrome is associated with systemic oxidative stress.34 Furthermore, 8-isoprostane levels correlate with the duration of nocturnal hypoxia, and fall following treatment with CPAP. However, the occurrence and role of oxidative stress in OSAHS is controversial13 ,33 ,35 ,36 and measuring systemic oxidative stress is notoriously difficult.
Alternative explanations for the pattern of vascular impairment should also be considered. Compared with wakefulness, heart rate, blood pressure and sympathetic nerve traffic to the vasculature decrease progressively throughout sleep.29 ,37 In contrast, sympathetic activity and blood pressure increase during arousals. Thus the autonomic nervous system and its response to sleep and arousals may play a key role in the mechanism of vascular dysfunction in OSAHS. Sleep disordered breathing and hypoxia may contribute to the elevation of endothelin-1 concentrations in patients with OSAHS induced hypertension.12 ,33 ,38
Study limitations
A limitation to the study included the absence of a normal control group. It would not have been feasible to find weight matched healthy volunteers who did not have some degree of irregular breathing during sleep. Obesity and insulin resistance are associated with vascular dysfunction,39 and this could be partly responsible for our observed differences. We took the pragmatic approach of using a non-desaturating OSAHS group as a control.
We did not include non-desaturators in the treatment trial, and therefore cannot comment on the potential benefits to vascular function of therapy in these patients. We focused on the desaturating group in this trial as our objective was to determine whether any vascular function abnormality was reversible and we decided a priori that changes with CPAP were most likely to be demonstrated in the more hypoxaemic group.
We acknowledge the inevitable mismatch in body mass index that resulted from consecutively recruiting desaturating and non-desaturating patients. However, our post hoc analysis matching for body mass index (fig 5) and by post hoc multivariate analysis strongly suggest that weight was not a factor in the difference in vascular responses between the groups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
There was no statistically significant carryover effect but also no measurements were made until 7 weeks after crossover—1 week washout plus 6 weeks of treatment—and the known effects of CPAP wear off within a few days.
There is no ideal placebo for CPAP. CPAP improves patency of the upper airway and is the treatment of choice for patients with OSAHS by pneumatically splinting open the upper airway. Sham CPAP, using a similar device altered to deliver a sub-therapeutic airway pressure, is arguably the best placebo.6 However, sham CPAP use was significantly lower than actual CPAP and this suggests that patients received positive reinforcement from the benefits of actual CPAP use. The clear difference in vascular function after active rather than sham CPAP is robust evidence of abnormal function in OSAHS that is reversible with effective treatment.
CONCLUSIONS
Patients with OSAHS and frequent nocturnal desaturations have markedly impaired endothelial dependent and independent vasodilatation. In these patients, treatment with CPAP for 6 weeks resulted in marked improvements in vascular function. These findings suggest that disease severity is an important modulator of vascular function, and that CPAP treatment may play an important role in reducing the cardiovascular complications associated with nocturnal apnoeas.
Acknowledgments
We thank all the staff in the Wellcome Trust Clinical Research Facility, Edinburgh, for their assistance with the studies.
REFERENCES
Footnotes
Funding: MDC was supported by the Wellcome Trust Director’s Support Fund and the BMA Josephine Landsell Grant (2004). The study was supported by a British Heart Foundation Project Grant (PG/02/078/14122).
Competing interests: None.
Ethics approval: Ethics approval was obtained.
Linked Articles
- Airwaves