Article Text

Abstract
Background: Cigarette smoking causes accelerated facial wrinkling and predisposes to chronic obstructive pulmonary disease (COPD). However, it has long been recognised that there is a subgroup of susceptible smokers who are at increased risk of developing airflow obstruction. We have tested the hypothesis that there is a common susceptibility for the development of COPD and facial wrinkling in cigarette smokers.
Methods: One hundred and forty nine current and ex-smokers were recruited from a family based study of COPD genetics, 68 (45.6%) of whom fulfilled the definition of COPD. 124 (83.2%) had no or minor facial wrinkling (Daniell <IV) and 25 (16.8%) were wrinkled (Daniell score ⩾IV). Generalised estimating equations were used to adjust for familial correlations between related individuals and the potential confounding effects of age and pack years smoked.
Results: Forced expiratory volume in 1 second (FEV1) was significantly lower in those with wrinkles than in those without (mean difference in FEV1 % predicted −13.7%, 95% CI −27.5 to 0.0, p = 0.05) and facial wrinkling was associated with a substantially increased risk of COPD (adjusted OR 5.0, 95% CI 1.3 to 18.5, p<0.02). The Daniell score correlated with the extent of emphysema on the CT scan (p<0.05) and facial wrinkling was also associated with a greater risk of more extensive emphysema (adjusted OR 3.0, 95% CI 1.0 to 9.3, p = 0.05).
Conclusion: Facial wrinkling is associated with COPD in smokers, and both disease processes may share a common susceptibility. Facial wrinkling in smokers may therefore be a biomarker of susceptibility to COPD.
- chronic obstructive pulmonary disease
- facial wrinkling
- smoking
Statistics from Altmetric.com
Cigarette smoking is associated with facial wrinkling1–7 that increases with the number of pack years smoked.2,5 Smoking is also the major risk factor for the development of chronic obstructive pulmonary disease (COPD). COPD is a heterogeneous syndrome of chronic bronchitis, small airways disease, and alveolar destruction (emphysema) that varies in proportion between affected individuals. It is well recognised that only a proportion of cigarette smokers develop COPD,8,9 and that this is likely to be the result of genetic susceptibility to the effects of cigarette smoke.10,11 Both smoking related facial wrinkling and emphysema may be likened to premature ageing of the tissues. Thus it is plausible that the genetic factors that predispose smokers to COPD also predispose smokers to wrinkling of the skin.
The objective of our study was to test the hypothesis that there is a common susceptibility for the development of airflow obstruction and facial wrinkling in cigarette smokers. Specifically, we examined whether facial wrinkling predicts the presence of airflow obstruction and emphysema in smokers. We addressed this by assessing the association between facial wrinkling and the prevalence of COPD in a group of middle aged smokers. The presence of lung destruction (emphysema) was assessed by a high resolution CT (HRCT) scan of the thorax.
METHODS
Individuals in this study were a subset of those recruited into the Cambridge arm of the International COPD Genetics Network. This is an international study that aims to identify genes that predispose cigarette smokers to the development of COPD. The study recruited index cases (probands) with relatively advanced COPD at an early age (forced expiratory volume in 1 second (FEV1) <60% predicted aged 65 years or less) and a smoking history of at least 5 five pack years (1 pack year is 20 cigarettes/day for 1 year). One of the objectives of the COPD Genetics Network is to assess the risk of airflow obstruction and emphysema in current and ex-smoking siblings of the probands. Therefore siblings of the probands with a smoking history of 5 or more pack years were invited to participate in the study and were screened with spirometry for COPD (defined as a post-bronchodilator FEV1 <80% predicted and FEV1/VC ratio <0.7). Demographic data and smoking exposure were obtained from probands and siblings using a modified version of the ATS questionnaire,12 and spirometric measures were obtained pre- and post-bronchodilator (salbutamol 180 μg administered via a large volume spacer) using a Collins portable spirometer. All measurements were taken at the participants’ homes by trained operators using a standardised protocol. Predicted values of FEV1 and FEV1/VC were calculated as described previously.13 All probands and siblings were invited to have a high resolution CT scan of the thorax to assess the presence of emphysema. Refusal to have an HRCT scan did not exclude individuals from participating in the COPD Genetics Network. Scans were performed in the radiology department of Addenbrooke’s Hospital, Cambridge. The images were obtained using a Siemens Somatom Plus 4 unit (Siemens Erlangen, Germany) with 1 mm collimation taken at 20 mm intervals in each participant.
Individuals who attended for their CT scan between February 2002 and March 2003 were also invited to take part in this additional study to assess the association between facial wrinkling and COPD. If they agreed, photographs of the left and right temporal region of the face were taken at the medical photography department of Addenbrooke’s Hospital on the same day that the HRCT scan was performed. Photographs were taken under standardised lighting conditions with a marker placed on the skin to allow accurate determination of scale. The extent of emphysema was determined by two respiratory radiologists (ADT and NJS) who independently assessed each HRCT scan. The amount of lung with emphysema was scored (<1%, 1–4%, 5–9%, 10–24%, 25–49%, and >50%). If the radiologists disagreed on the extent of emphysema by more than one adjacent category, the films were re-examined and a consensus score was obtained. Otherwise the more conservative estimate of the extent of emphysema was used in the analysis.
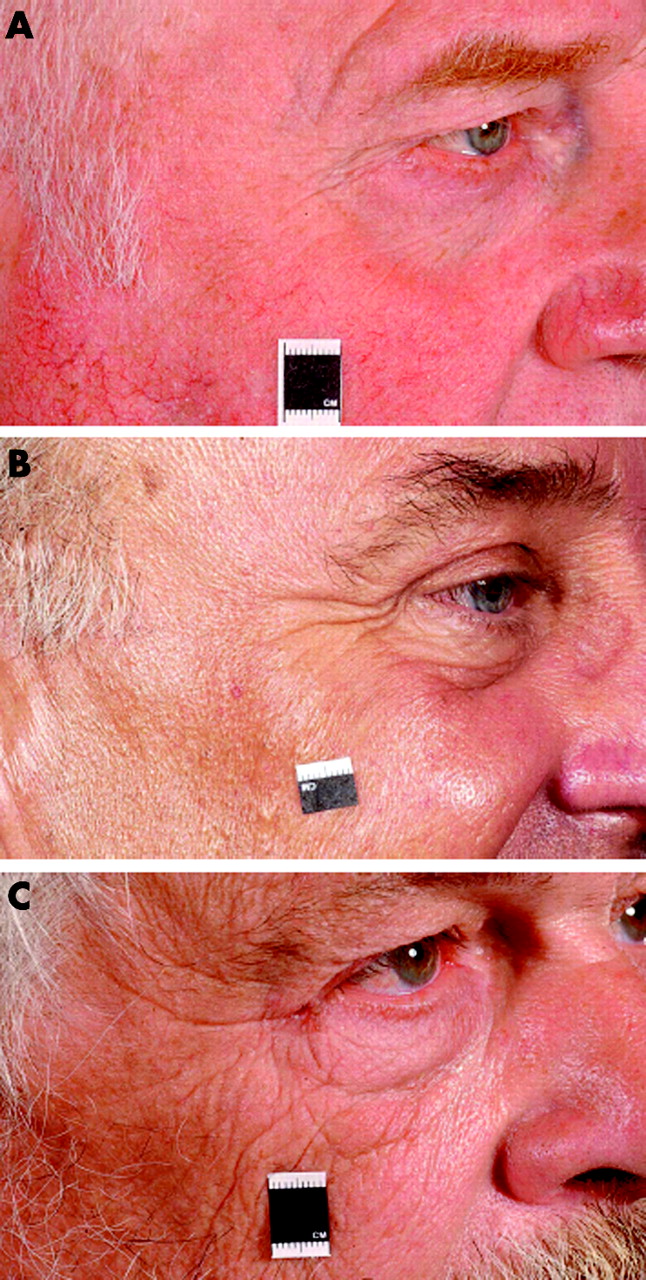
The extent of facial wrinkling was determined from photographs of the left and right temporal region of the face. Each photograph was independently scored by two dermatologists (WJL and NPB) and the extent of facial wrinkling in the “crows’ feet area” determined using the scoring system described by Daniell.1 This scores wrinkling from I to VI (grade I, essentially unwrinkled; grade II, several wrinkles (up to 6) up to 3 cm in length; grade III, several prominent wrinkles on each side 3–4 cm long; grade IV, wrinkles extend superiorly and inferiorly and are >5 cm long; grade V, wrinkles extend from the crows’ feet area and are prominent over cheeks and forehead; and grade VI, profound wrinkling extending over most of the face (fig 1). Where there was disagreement between the scores, both readers reviewed the photographs and a consensus score was obtained. For the analysis the mean of the left and right wrinkle score was used. The radiologists and dermatologists were blind to the individuals’ smoking history and spirometry results.
{kind=link}
Daniell system for scoring the extent of facial wrinkling of the crows’ feet area: (A) grade I, (B) grade III, (C) grade VI. Photographs reproduced with permission.
An additional questionnaire was completed by the participants to obtain information on sunlight exposure. The questionnaire asked the individual to record if they had ever worked outdoors, lived abroad in a hot sunny climate, took regular holidays abroad in sunny climates (and if so, how many), and if they regularly used sunscreen.
This study was approved by the Addenbrooke’s Hospital research ethics committee.
Statistical analysis
Individuals were classified as wrinkled using a method similar to that previously described by Kadunce et al.2 The median wrinkle score in our study group was II (IQR 1). For the analysis we classified those individuals in the 90th centile (Daniell score ⩾IV) as wrinkled and those with scores of <IV as unwrinkled. Means of continuous variables were compared using the Student’s t test or Kruskal-Wallis test and proportions were compared using a χ2 test. The association between facial wrinkling and COPD was assessed with lung function as a continuous variable (FEV1 % predicted) and categorical variable (COPD defined as a post-bronchodilator FEV1 <80% predicted and FEV1/VC ratio <0.7). Spearman’s rank correlation was used to test for correlation between ordinal categorical variables.
The individuals in this study are a subgroup of those recruited into the Cambridge arm of the International COPD Genetics Network. As this is a family based study, some of the individuals in the current study were related (siblings) and, in the analysis, data from related individuals could not be treated as independent observations. This meant that conventional linear and logistic regression models were inappropriate for the analysis and an alternative regression model was required to allow for the fact that some individuals were from the same family. Generalised estimating equations (GEE)14,15 were therefore used which allowed for the inclusion of common familial correlations.10 GEE models also allow adjustment for potential confounding exposures such as pack years smoked, age, and sun exposure by inclusion as covariates.
RESULTS
Complete data on post-bronchodilator spirometry, wrinkle scores, and CT scores of emphysema were available for 149 individuals recruited from 78 families. Thirty two individuals were unrelated to any other participant in the study while the remaining 117 represent two or more siblings from 46 families. The maximum number of siblings recruited from a single family was eight. Of the 149 individuals, 50 (33.6%) were probands and therefore by definition had COPD; 18 (18.2%) of the 99 non-probands fulfilled the spirometric criteria for COPD. The characteristics of the study population are summarised in table 1. Individuals with COPD were significantly older, had a greater pack year smoking history, and were more likely to be male than people without COPD.
Characteristics of the study population
One hundred and twenty four (83.2%) of the study group had no or minor wrinkling (Daniell score I, II or III) and 25 (16.8%) were wrinkled (Daniell score ⩾IV; table 2). The prevalence of COPD was greater and the mean FEV1 lower in individuals with wrinkling than in those without wrinkling. Indeed, 21 of 25 (84%) individuals with wrinkling had COPD. The odds ratio for COPD in individuals with facial wrinkling was 8.6 (95% CI 2.8 to 26.6, p<0.001) relative to those without facial wrinkling.
Characteristics of individuals by presence of facial wrinkling
Individuals with wrinkling were significantly older and had smoked significantly more pack years than those without wrinkling (table 2). Generalised estimating equations were used to adjust for age and pack years smoked, and to adjust for potential familial correlations between related individuals. In these analyses, FEV1 % predicted was significantly lower in wrinkled than in non-wrinkled individuals (adjusted mean difference in FEV1 % predicted −13.7%, 95% CI −27.5 to 0.0, p = 0.05). Moreover, facial wrinkling was associated with a fivefold increased risk of COPD after adjustment for age and pack years smoked (adjusted OR 5.0, 95% CI 1.3 to 18.5, p<0.02 relative to people without wrinkles). In these analyses, pack years smoked (but not age) was significant as a covariate. Compared with individuals without wrinkles, those with facial wrinkles also had an increased risk of more severe airflow obstruction (FEV1 <60% predicted and FEV1/VC <0.7) that was again independent of age and pack years smoked (adjusted OR 4.8, 95% CI 1.5 to 15.8, p⩽0.01).
Complete data on sun exposure was available for 128 individuals. Confounding of the association between facial wrinkling and COPD was explored by including history of working outdoors, living abroad in a sunny climate, taking holidays in sunny climates (and the number of holidays taken), and the use of sun screens in the model. In these analyses, none of the sun exposure variables were significant as covariates and their inclusion did not affect the association between facial wrinkling and COPD (adjusted OR 5.6, 95% CI 1.2 to 27.3, p = 0.03) or more severe airflow obstruction (4.5, 95% CI 1.3 to 15.6, p<0.02).
Emphysema was more prevalent in individuals with facial wrinkling (table 2). Moreover, the severity of emphysema was significantly correlated with the mean Daniell score (Spearman’s rho 0.16, p<0.05). Forty four percent of those with wrinkling had emphysema affecting more than 10% of their lung compared with 18.6% of people without wrinkling (OR 3.5, 95% CI 1.4 to 8.6, p<0.01). After adjustment for age, pack years smoked and familial correlations, facial wrinkling was associated with an increased risk of emphysema affecting more than 10% of the lung (adjusted OR 3.0, 95% CI 1.0 to 9.3, p = 0.05). Inclusion of the sun exposure variables in the analysis did not affect the association (adjusted OR 3.3, 95% CI 0.9 to 10.8, p = 0.05), and none of the sun exposure variables were significant when included as covariates.
DISCUSSION
The association between smoking and premature ageing of the skin is well established.1–7 In this study we have shown that severe facial wrinkling (Daniell score ⩾IV) is significantly associated with a lower mean FEV1 and COPD. Indeed, more than 80% of smokers with facial wrinkling fulfilled the spirometric criteria for COPD. Facial wrinkling was also associated with the presence of tissue destruction (emphysema) on the HRCT scan. Moreover, we found that these associations were independent of the effects of age and cumulative pack years smoked. In an earlier study Kadunce and colleagues found smoking to be associated with an increased risk of severe (modified Daniell score >3.5) facial wrinkling. However, they observed that only 27% of smokers with more than 50 pack years exposure were affected. They postulated that, as with COPD, there may be a subgroup of smokers who are susceptible to facial wrinkling.1 Our findings support this hypothesis and suggest that there may be a common susceptibility to the two conditions.
We have considered the possibility that the results presented here may be the result of chance, confounding, or bias. The association between wrinkling and airflow obstruction was highly significant and unlikely to be explained by chance variation. In our analysis we adjusted for the key confounding exposures of age and cumulative smoking. People with more severe facial wrinkling and COPD were significantly older and had smoked significantly more pack years than those without. However, only cumulative pack years remained significant when both variables were included in the generalised estimating equation. That age was not a significant risk factor in the multivariate model may be because, in correcting for pack years, we were in part correcting for age. Moreover, the spirometric parameter used as the dependent variable (FEV1 % predicted) was already corrected for age. We adjusted for sun exposure as this has been associated with facial wrinkling.6,16 However, to be a significant confounder of the association between wrinkling and airflow obstruction, sun exposure would also have to be also associated with the risk of COPD. Since we have no reason to suppose that sun exposure is associated with the risk of COPD, it is not surprising that sun exposure was not significant as a covariate in the regression analyses.
This study recruited individuals from a larger study that aimed to recruit families identified through a proband with early onset COPD. An alternative method of looking at the association between facial wrinkling and COPD would have been to look at discordant sib-pairs. However, enrolment into this sub-study was not conditional on a sibling also giving consent to take part in the study. A significant number of individuals in this study were therefore “singletons” and a sib-pair analysis would not have been appropriate. It was, however, necessary to allow for the fact that some of the individuals were related, so we used generalised estimating equations to adjust for potential familial correlation between individuals from the same family.
The findings of this study inevitably raise the question “Is it possible to predict the presence of COPD in smokers from their facial appearance?” The predictive value of severe wrinkling for airflow obstruction in smokers is dependent upon the sensitivity and specificity of wrinkling for predicting COPD and the prevalence of COPD in the population assessed. In a cross sectional study of over 13 000 individuals, severe facial wrinkling was found to be associated with a mean reduction in FEV1/FVC of 1.2–1.9% predicted in current and ex-smokers (but not in non-smokers).17 Although this finding is consistent with the current study, the magnitude of the association is far smaller. It is unclear what proportion of smokers in that study had COPD, so the relatively modest association may be a consequence of an over-representation of healthy (that is, non-susceptible smokers) in the study population. In contrast, we have studied a group of individuals with a high prevalence of COPD. We recruited families identified through a proband with relatively early onset COPD. We have previously shown that the siblings of probands who smoke have a greater risk of developing airflow obstruction than unrelated controls, and this suggests that there may be a genetic predisposition to the development of COPD.10,11
Our results suggest that the presence of facial wrinkling in this susceptible group is strongly predictive of the presence of airflow obstruction and emphysema. Severe facial wrinkling may therefore be a marker of COPD susceptibility and should alert the clinician to assess such individuals for the presence of COPD. Moreover, the association between facial wrinkling and COPD suggests that there may be a common mechanism and perhaps a common genetic susceptibility. It seems likely that changes in the collagen and elastin are important in the pathogenesis of both lung and skin pathology. Wrinkling may be the consequence of metalloproteinases that are activated as a consequence of smoking18 or a defect in repair mechanisms that affects both the skin and the lungs.
In summary, we have found that facial wrinkling is strongly associated with the risk of airflow obstruction. This increased risk is independent of cumulative tobacco exposure. Extensive facial wrinkling may be a marker of susceptibility to the effects of cigarette smoke and should promote the screening of affected individuals for airflow obstruction.
Acknowledgments
The authors thank the radiographers and the staff of the medical photography department of Addenbrooke’s Hospital for their contribution to this work, and are especially grateful to all the study volunteers for their time and willingness to take part in the study. The photographs in fig 1 are reproduced with the permission of the individuals.
REFERENCES
Footnotes
-
Published Online First 14 June 2006
-
This work was supported by an NHS R&D Fellowship to BDP, Glaxo Smith Kline and Papworth NHS Trust.
-
Competing interests: none.
Linked Articles
- Airwaves