Article Text

Abstract
A review of the evidence that the prevention of COPD works and, if so, the effectiveness of this strategy
- COPD, chronic obstructive pulmonary disease
- FEV1, forced expiratory volume in 1 second
- NAC, N-acetylcysteine
- chronic obstructive pulmonary disease
- exacerbations
- prevention
Statistics from Altmetric.com
- COPD, chronic obstructive pulmonary disease
- FEV1, forced expiratory volume in 1 second
- NAC, N-acetylcysteine
The periodic worsening in clinical state which most patients with chronic obstructive pulmonary disease (COPD) recognise (but do not always describe) as a disease exacerbation1 is one of the greatest burdens associated with this condition. Patients are concerned about the occurrence of uncontrolled breathlessness which accompanies an exacerbation2 and are aware that their well being, measured using health status questionnaires, is impaired for weeks to months after episodes which their doctors describe as “simple bronchitis”.3 Patients reporting exacerbations have a significantly worse state of health than those spared these events,1,4 while their rate of deterioration—whether described by the decline in forced expiratory volume in 1 second (FEV1)5 or in health status4—is more rapid if they exacerbate frequently. Exacerbations drive health costs,6 especially when they lead to admission to hospital, irrespective of the medical setting in which they occur. Although treatment can improve the rate of resolution of an exacerbation7,8 and is effective in reducing breathlessness9 and mortality,10 it is entirely reasonable that considerable effort has been directed to the prevention of these episodes.
This review will consider the evidence that this strategy works and, if so, how effective it is. Unfortunately, interpreting even apparently methodologically sound data is not easy, and apparently trivial differences in which events are counted can change the exacerbation rate considerably. As a result, the overall data are, at best, semi-quantitative despite the considerable rigor that has gone into data acquisition in many recent studies.
METHODOLOGICAL PITFALLS
Several factors can easily confuse the unwary and, when taken together, may lead to despondency about our ability to decide whether treatment works at all. This will be considered under the following headings:
-
Diagnosis.
-
Definition.
-
Study design.
-
Phenotypic variation and statistics.
Diagnosis
The term exacerbation was borrowed from the concept of an acute exacerbation of chronic bronchitis, one of the component conditions now subsumed within the concept of COPD.11 As chronic bronchitis can occur without airflow obstruction being present,12 it is no surprise that many studies have focused on the relatively easy to define symptoms of cough and sputum production and have not gone on to establish whether airflow obstruction was present. This has been particularly true when the effects of antibiotics and mucolytic agents have been studied,13,14 but recent reports have clearly identified the effects of these agents in patients who undoubtedly have COPD.15,16
Definition
Clinical trials usually seek a practical way of identifying the episodes of interest and this need has almost certainly influenced the choice of definition used for the identification of COPD exacerbations. The so-called “consensus definition” formulated at the Aspen Lung Conference in 2000 is primarily based on healthcare utilisation—usually but not always involving the use of oral corticosteroids and/or antibiotics17—and this definition is the one most frequently used. It is clear that not all exacerbations are captured by reliance on healthcare contacts,18 and the agreement between exacerbations defined by change in symptoms recorded on a diary card and those where the patient has sought medical help is surprisingly poor, at least in one 12 month clinical trial recently reported (fig 1).19 Although reliance on healthcare contacts may work well in a single country,20 it does not necessarily reflect what happens in different healthcare systems where the availability of treatment and the threshold for its use can differ. Inferring that more severe episodes require treatment with oral corticosteroids may be true in Europe21 but has not been established elsewhere. The likelihood of seeing a doctor or of being admitted to hospital will depend on the intensity of the precipitating inflammatory stimulus and the severity of the underlying obstructive lung disease. Patients with a lower initial FEV1 commonly report greater numbers of healthcare use related events, and this is true within a single study population22 or between clinical trials.23 Finally, how data are collected can influence the event rate. Reliance on spontaneously reporting an adverse event at a clinical study visit usually yields a lower exacerbation rate than actively enquiring about whether an exacerbation has occurred.8

(A) Mean symptom scores taken from diary cards for a study group of 468 patients. Around the first protocol defined exacerbation, patients are experiencing appropriate symptoms when they attend their doctor (•, shortness of breath; ▪, cough; ♦, chest tightness; ▴, night time awakening; day 0, first day of exacerbations). (B) In individual patients there is a much weaker relationship between symptom change and medical contact whether the symptoms are viewed singularly or in combination. Reproduced with permission from Calverley et al.19
Study design
Differences in the run-in period before treatment randomisation can have an important influence on the likelihood of exacerbations early in the study but in practice do not seem to be crucial to the overall exacerbation rate. A longer run-in period may exclude less stable patients who exacerbate readily, an important factor when treatment is changed during the run-in.24 However, withdrawing or intensifying treatment did not modify the exacerbation rate in two studies recruiting comparably severe patients to the same range of treatments.25,26 In general, longer trials increase the likelihood of an event occurring and hence the discriminatory power of the study. Studies of bronchitis can be influenced by the seasonality of the condition and ideally should involve at least two winter periods.27 Some trials have only followed patients until they withdrew which was mandated if a set number of exacerbations occurred in a particular period.28 This non-random withdrawal from study does have effects on the subsequent power of the trial to show a difference29 and may underestimate the true exacerbation rate.
Phenotypic variation and statistics
Not every COPD patient exacerbates even when they have relatively advanced disease. Thus, in a 3 year study of symptomatic patients selected by their initial spirometric parameters, 23% never reported needing a course of oral corticosteroids or antibiotics.22 Selection for and participation in a clinical trial reduces the exacerbation rate compared with their historically reported frequency. The placebo treated patients in the TRISTAN trial had an exacerbation rate of only 1.30 events per year despite all being recruited because they had had at least two episodes of exacerbation in the preceding year.30 Patients who report regular cough and sputum production31 and are less active at home32 are significantly more likely to exacerbate and/or be admitted to hospital although age (a surrogate for FEV1 and disease severity) and prior exacerbation history are the major determinants of the risk of subsequently exacerbating.
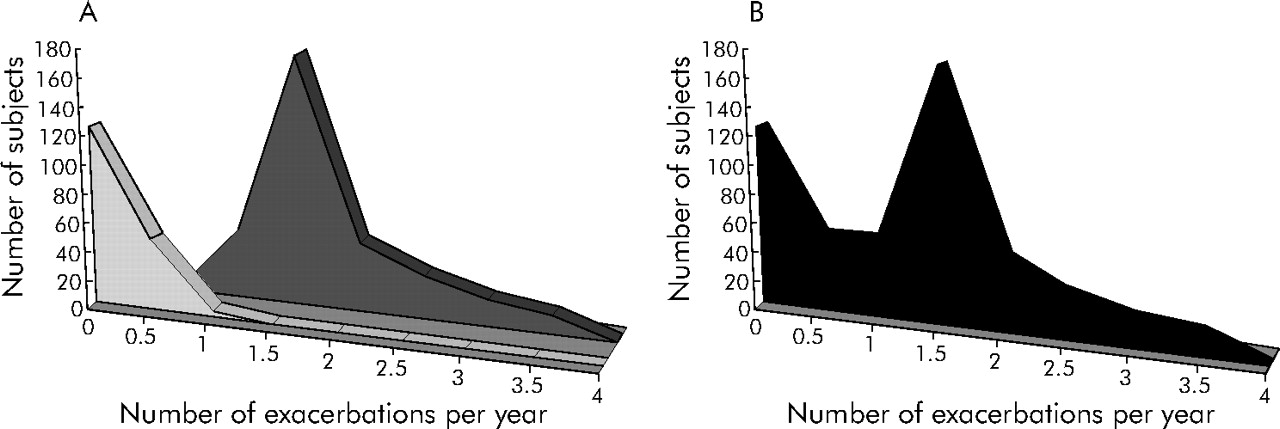
One poorly appreciated effect of this difference in the likelihood of exacerbating is on the estimates of the exacerbation rate during the clinical trial. Data are usually reduced to a mean and variance measure when reporting exacerbation frequency but this simplification may be unhelpful given the non-normal distribution of these events (fig 2). Simple statistical tricks to normalise these data have proved to be ineffective, leading to the use of more complex techniques like the Poisson distribution to improve the data fitting and allow a true mean event rate to be presented.30 Even this method may “over fit” the data requiring further statistical adjustment. This leaves the suspicion that we are trying to approximate two different types of biological behaviour into a single number, and this problem may have to be addressed in future studies. Reporting the number needed to prevent an event in a population may be a more useful approach, given the difficulty in identifying individuals who themselves will exacerbate.
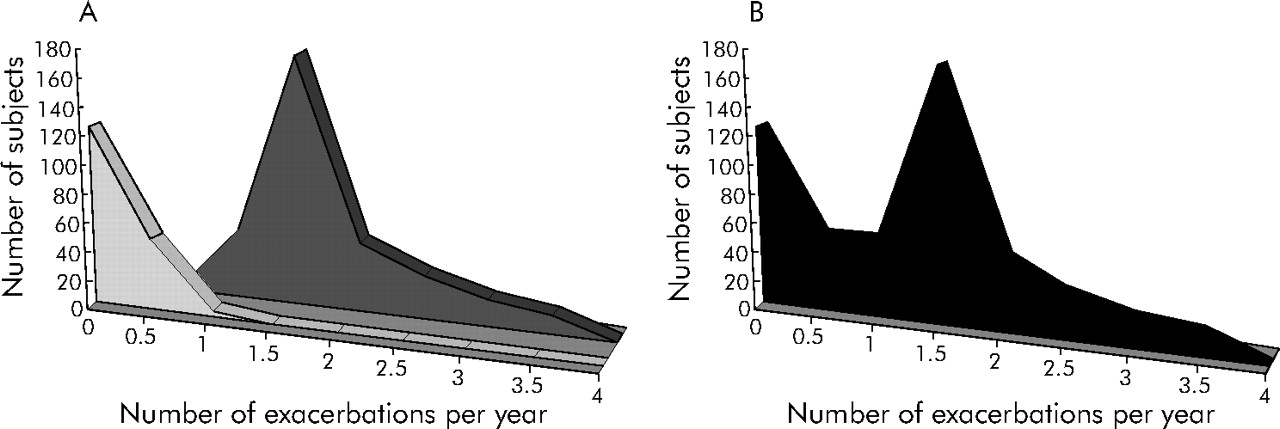
Effect of combining two separate groups within a study population (A) to generate a composite distribution curve for the whole population (B). Within a certain population we may not recognise that one phenotype has few exacerbations while another phenotype is a more frequent exacerbator. This non-normal distribution can present problems in interpreting data and pooling data from different studies in a meta-analysis.
To date, all of the above factors tend to reduce the difference between the active and placebo limbs of treatment and hence our estimation of the effectiveness of treatment on COPD related events is likely to be a conservative one. This may explain why reports based on database analysis of treatment choices seem to suggest a more impressive treatment effect,33,34 although there are many reasons why such retrospective data may be flawed.35 For this review the evidence supporting specific approaches to exacerbation prevention is based on randomised control trials whenever possible. More extensive data resources can be accessed through the National Institute of Clinical Excellence report on COPD management,11 although these data have been modified in the light of more recent publications in the current review.
TREATMENT APPROACHES TO EXACERBATION PREVENTION
Improving immune function
Many exacerbations occur as a consequence of viral and/or bacterial lower respiratory tract infections,36–38 with the latter especially important when chronic colonisation has occurred.39 In this setting a change in the bacterial serotype, at least with Haemophilus influenzae colonisation, is associated with a greater likelihood of an exacerbation occurring.40 Although the most common viruses identified either serologically or by the PCR technique are rhinoviruses and respiratory syncytial virus, we presently lack effective methods of preventing infection with these agents. Influenza A and B account for 5.4% of exacerbations,37 but there is reasonable evidence showing that immunisation with an appropriate polyvalent vaccine is effective.11 In part, the evidence for this comes from studies in nursing home residents where the presence of COPD is inferred rather than established.41 However, in one trial in a country with only limited access to immunisation, acute respiratory infections caused by influenza were reduced by 76% when active immunisation was used.42 Unsurprisingly, this amounted to only a small number of episodes, but this remains a very cost effective treatment. The use of pneumococcal vaccination in COPD patients is now advocated,43 which is reasonable given that Streptococcus pneumoniae is one of the most frequently identified bacterial pathogens in COPD exacerbations. However, a direct test of the value of pneumovax in patients identified as having COPD is not available. This is worrying since this form of vaccination—which prevents pneumonia in younger adults—is less effective in older individuals with chronic disease, and there are issues about whether the current vaccine contains sufficient immunological coverage.44 How effective this form of immune augmentation is in patients who have already developed lower respiratory tract colonisation is equally uncertain. Better data and possibly more immunogenic vaccines are needed before this problem can be fully resolved.
A further approach, usually viewed with some scepticism, is to non-specifically increase immune function or augment the innate defence mechanisms. Trials are available with two agents which claim to do this.45,46 In one case there was a reduction in the number of days spent in hospital and in the other in the quality of life, although in neither was the exacerbation rate as defined modified significantly. A meta-analysis suggests these drugs may have an effect on exacerbations, but the trial quality is poor.47 More information is needed and further large trials will be required to validate this approach to exacerbation prevention.
Non-pharmacological treatment
Unlike immunomodulation, this approach is likely to act by improving the host capacity to withstand the consequences of an acute infective/inflammatory insult that has precipitated the exacerbation. To date, few studies have been powered sufficiently well to determine whether this type of intervention really influences the exacerbation rate. Studies in which exacerbations have been an important secondary outcome do suggest that some treatments can be effective. Several different types of non-pharmacological treatment are commonly advocated in the management of COPD patients, some in fairly specific settings.
Surgery
Lung volume reduction surgery improves lung function, exercise capacity and, in a subset of individuals, survival.48 It has also been shown to improve patient well being identified by different health status questionnaires.49 This does not appear to be due to an impact on exacerbations, at least as far as can be determined. The failure to report exacerbation data in the follow up of these patients may reflect the selection criteria for patients who undergo this type of surgery. In general, those who have chronic cough or sputum production or who are clinically unstable do not qualify for this intervention, making subsequent exacerbation rates harder to interpret.
Non-invasive ventilation
Non-invasive ventilatory support is clearly effective in patients admitted with acute respiratory failure,10 and has been advocated in those who have persistent hypercapnia as a means of improving exercise performance and health status.50 Disappointingly, there are no data available on subsequent hospitalisation rates in one of the only randomised control trials to study non-invasive ventilation.51,52 However, the re-admission rate in such patients is high,53 and one observational series suggests that selective patients who are admitted to hospital frequently with episodes of respiratory failure can be effectively managed with home non-invasive ventilation.53,54 Although this would apply to relatively few people with advanced disease, it could still be a cost effective use of resources and requires further study.
Domiciliary oxygen
None of the original studies comparing long term oxygen therapy with an appropriate control treatment reported exacerbation rates although the British MRC study found no difference in the number of days in hospital between patients receiving oxygen and those not.55 This was attributed to the lengthy periods of hospitalisation associated with the trial assessment. Retrospective observational data from the Scandinavian Oxygen Registry suggest that there is a significant reduction in hospital admissions and exacerbations after long term oxygen is started, although other factors related to patient care could be influencing this result.56
Pulmonary rehabilitation
The evidence for the effectiveness of pulmonary rehabilitation is very strong, but its impact on exacerbation rate is less studied than other more direct outcomes such as exercise performance and health status. Conducting such studies now will be difficult, given the ethics of withholding rehabilitation for long enough for an exacerbation to occur. Nonetheless, retrospective analysis of Italian data suggests that patients who participated in pulmonary rehabilitation were less likely to exacerbate,57 while the most convincing evidence comes from the prospective randomised control trial conducted some years ago in South Wales where patients who received pulmonary rehabilitation had on average 10.4 days in hospital compared with 21.0 days in those randomised to receive conventional medical treatment.58 There is no direct report of the number of courses of corticosteroids or antibiotics, but the hospital admissions when they occurred were briefer which helped to justify the cost effectiveness of this intervention.59
Pharmacological treatment
Most maintenance drug treatment in COPD is given for reasons other than exacerbation prevention, and the realisation that treatment also reduced exacerbations came as something of a surprise. Some medications such as β agonists60 and inhaled corticosteroids61 have definite non-bronchodilator effects which have proved hard to establish for anticholinergic bronchodilator drugs. Yet these latter appear to produce comparable improvements in exacerbation rate (with all the caveats already noted) to those seen with drugs that “reduce inflammation”. The most likely explanation is the improvement in lung mechanics (usually assessed by an increase in post-bronchodilator FEV1), that is a feature of all these active treatments. There is little relationship between the size of this spirometric change and the magnitude of the exacerbation reduction, probably reflecting the importance of changes in lung volume rather than expiratory flow when exacerbations occur62 and differences in the initial degree of overinflation.63 Nonetheless, bronchodilators increase inspiratory capacity acutely64 and this translates into a delay in the time taken to reach a given degree of hyperinflation, at least during exercise.65 Whether the same holds true for inhaled corticosteroids alone or in combination with long acting β agonists is yet to be established.
Bronchodilator drugs
It has proved difficult to establish whether short acting bronchodilators reduce exacerbation rates, possibly for methodological reasons such as poor study design, but also because the need for four times daily treatment—which is now recommended with short acting maintenance treatment—is not well adhered to and the effect of short acting treatment on health status and symptoms of breathlessness declines over time.66 Post hoc analysis of trials involving ipratropium bromide suggested that regimes that included this drug prevented exacerbations more effectively than a β agonist alone,67 although the sample sizes in each population were not matched. Better data became available when long acting inhaled bronchodilators were developed, and some representative studies are presented in table 1. These drugs were able to produce 12 hour68,69 or 24 hour70 bronchodilatation with a convenient dosage regime which was effective throughout the night. Initial data with salmeterol and formoterol suggested that exacerbations rates were unaffected over a 3 month study period,71 although the time to first exacerbation was lengthened.72 However, the salmeterol treatment limb of the TRISTAN study was associated with a reduction in exacerbations of approximately 20% compared with those randomised to placebo.30 Formoterol was effective in reducing the number of “bad days” (equivalent to milder exacerbations) in some studies69,73 but did not change the overall rate of moderate to severe exacerbations in two studies in more severely affected patients (fig 3).25,26
Representative studies of the effect of long acting bronchodilators in COPD

{kind=link}
{kind=link}
{kind=link}
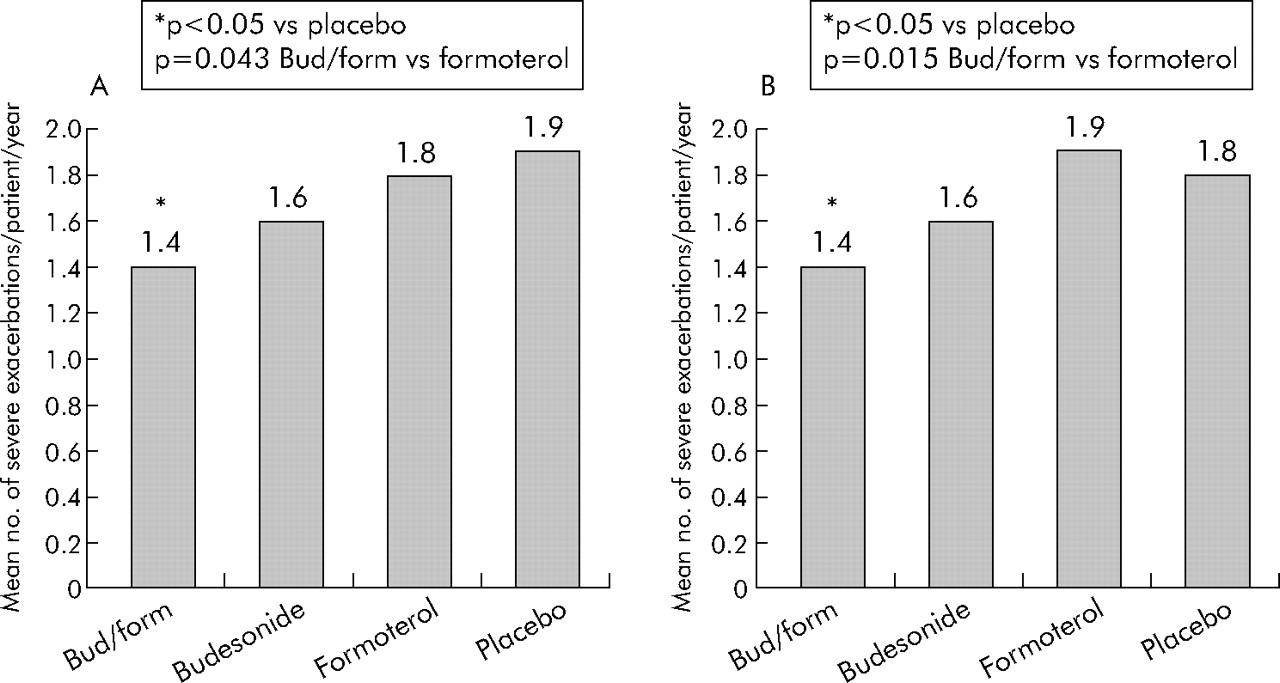
Mean number of severe exacerbations per patient per year in studies by (A) Szafranski et al25 and (B) Calverley et al26 using budesonide/formoterol combinations compared with the single components or placebo. In these trials with different run-in protocols, neither the inhaled corticosteroid nor the long acting β agonist individually reduced the exacerbation rate. However, when given in combination there was a significant reduction in the exacerbation frequency.
The situation with tiotropium, the only long acting anticholinergic bronchodilator currently available, is rather different. Trials with this drug have been less restrictive than with others, with no requirement for prior bronchodilator reversibility or limitation on the use of inhaled corticosteroids. Thus, around two thirds of patients in most studies have used these latter drugs which may have influenced the reported exacerbation rates. This helps explain why the exacerbation rates in the two 1 year tiotropium trials66,74 comparing placebo and an ipratropium limb were significantly less than in other studies. Once again the method of identifying exacerbations may be important, but this methodological difference did not influence the effectiveness of the drug treatment where a significant reduction in exacerbations of approximately 20–25% was seen in each study when tiotropium was added to the usual therapy. More recent studies suggest that this improvement in exacerbation rate can be replicated in a wider population of COPD patients and is associated with a reduced incidence of hospitalisation for those involved in the US Veterans Administration trial.75
Inhaled corticosteroids
The effect of inhaled corticosteroids on COPD continues to be controversial with some evidence of a reduction in the decline of FEV1 being seen when trial data are combined.76 However, the studies included in these data overviews report very different exacerbation rates in the placebo treated patients (2.1 per patient year in the Lung Health Study II77 compared with 0.99 in ISOLDE28), reflecting the differing recruitment criteria and differences in the baseline lung function. Data on exacerbations or surrogates for this outcome are shown in table 2. There is evidence for an effect in patients with a mean FEV1 of about 44% predicted,28,30 but not in studies where the FEV1 falls to 36% predicted.25,26 Unfortunately, different inhaled corticosteroids administered by different delivery systems were used in these trials which further complicates their interpretation.
One year studies of the effect of inhaled corticosteroids on COPD exacerbations
As many patients receive inhaled corticosteroids before entering a clinical trial, two other studies have examined whether withdrawing this treatment produces clinical deterioration—something that was originally suggested in an observational study based on the run-in phase of the ISOLDE trial.24 In patients with moderately severe FEV1 (mean FEV1 57% predicted) exacerbations were more frequent in those randomised to corticosteroid withdrawal (57% v 47%).78 In the COSMIC study where inhaled corticosteroids were withdrawn but salmeterol was continued in both limbs of the trial, similar findings were seen with the annual moderate or severe exacerbation rate reduced from 1.6 to 1.3.79
Combination treatment
Although combinations of short acting bronchodilator drugs have been used for decades in COPD management, there are no good clinical studies reporting their effectiveness in reducing exacerbations. Different classes of long acting bronchodilator have been combined with additional improvements in lung function but, to date, the studies have been too brief for exacerbations to be a reliable outcome. In contrast, the combination of twice daily inhaled long acting β agonists and corticosteroids, now widely used in the treatment of asthma, has also been studied in patients with COPD and representative data are shown in table 3. In general, inhaled corticosteroids and long acting β agonists produce greater changes in lung function than either drug alone relative to placebo—that is, regular/as needed short acting bronchodilators.26,30,80 In keeping with this, healthcare related exacerbations were less frequent during combination treatment in the two trials which have reported this outcome over 1 year, significantly so in the studies of budesonide and formoterol (fig 3). A pre-specified subgroup analysis of the TRISTAN data suggests that the fluticasone/salmeterol combination is superior to salmeterol alone in the most severe subset of patients, although it is worth pointing out that there was no treatment by disease severity interaction across the trial as a whole.30
Representative studies of the effect of a combination of long acting bronchodilators and inhaled steroids in COPD
Phosphodiesterase inhibitors
Although theophylline remains the most widely used non-specific phosphodiesterase inhibitor, data about its effects on exacerbations are lacking and the situation is scarcely better for the more specific PDE4 inhibitors. These drugs have many attractive pharmacological properties which might potentially reduce the patient’s likelihood of exacerbating81,82 but, to date, there are few published data to support this action. Cilomilast has been studied in several unpublished clinical trials which can be accessed via the Food and Drug Administration website (http//:www.fda.gov). Overall there was a small (32 ml) improvement in lung function with the drug and no effect on exacerbation rates compared with placebo. More recently a different drug in this class, roflumilast, has been shown to produce sustained improvements in FEV1 (97 ml difference with roflumilast compared with placebo) over 24 weeks of treatment with an acceptable side effect profile.83 This is accompanied by a reduction in the overall exacerbation rate from/to events. However, no more than 80% of these events were defined by an increase in the use of rescue medication rather than as moderate or severe exacerbations which have been reported in the other studies. Whether this improvement in symptom control translates to a greater effect on more severe exacerbations remains to be determined.
Mucolytics and antioxidants
As already noted, many trials evaluating these drugs have been conducted in patients defined by the presence of bronchitic symptoms rather than airflow obstruction. This is sensible given the proposed mechanism of action which is to modify the physical properties of mucus and improved secretion clearance. The selection of exacerbation prevention as a target for this treatment came after many studies had failed to show any effect of this class of drugs on more conventional end points such as lung function, exercise performance, or symptoms. A well conducted systematic review has suggested that there is reasonable evidence for a treatment effect.14 Much of this related to studies involving the use of N-acetylcysteine (NAC) which has also been shown in vivo to have a significant antioxidant effect. This provides a biologically more attractive mechanism for exacerbation prevention in COPD. Database studies84 and systematic review of the existing evidence suggested that NAC would have an important effect on exacerbation prevention.85 Disappointingly, there is now a well performed prospective randomised control trial conducted over 3 years in 523 patients which found that the exacerbation rate in those randomised to NAC was no different from that in the placebo group.16 A subgroup analysis suggested that patients who were not receiving concomitant inhaled corticosteroids had fewer exacerbations if they were randomised to NAC (0.76 v 1.11 moderate or severe exacerbations per year), but this conclusion requires prospective confirmation. It does raise the possibility that treatment may not be cumulative and that only a certain percentage of exacerbations are preventable by whatever treatment is available.
FUTURE DEVELOPMENTS
The importance of COPD exacerbations as a clinical end point means that any future treatment strategy is likely to be tested against this outcome, a point recognised in the recent Global initiative in Obstructive Lung Disease (GOLD) document on outcome measures (http//:www.copd.com). Better and more specific approaches to boosting immune competence are likely in the next decade, while the effect of antibiotic treatments on lower respiratory tract bacterial colonisation is currently under study. There is a clear need to properly evaluate the effectiveness of non-invasive ventilatory support in patients with recurrent hypercapnic respiratory failure. We need better evidence to support the use of case management as a system of caring for recurrently hospitalised COPD patients, although this has not stopped it growing in popularity in both Europe and North America. New long acting anticholinergic drugs are under study and their combination with once daily inhaled corticosteroids and/or long acting β agonists will be an important test of the need for more than one treatment to prevent exacerbations. A large Canadian multicentre trial is already underway testing the value of tiotropium, the corticosteroid long acting β agonist combination and all three drugs together in patients with COPD, and the results of this are awaited with interest.86
Despite the bewildering complexity and potential pitfalls of study design that characterise this field, several consistent and simple messages have emerged. The most important is that exacerbations—so important for patients and expensive for those who care for them—are preventable, at least in part. This can be done by using a range of treatments, although the optimum combination remains to be defined and may vary depending upon the phenotype of the patient. Defining these events from a healthcare perspective focuses attention on the ability of exacerbations to drive symptoms and healthcare contacts and says little about the underlying biology of this process. Hopefully a better understanding of the nature of exacerbations and the pathophysiology of those patients who most frequently report them will help us to develop more rational preventative regimes in the future.
REFERENCES
Supplementary materials
In the paper entitled 'COPD exacerbations � 4 ? Prevention' by S Scott, P Walker and P M A Calverley which appeared in the May issue of Thorax (2006;61:440�7), the dose of tiotropium used in the studies by Casaburi and Brusasco referred to in table 1 on page 444 which currently reads '18 mg twice daily' should read '18 mg once daily'. The publishers apologise for this error.
Footnotes
-
Funding: none.
-
Competing interests: none declared.
Linked Articles
- Correction