Article Text

Abstract
Background: It is unclear whether continuous positive airway pressure (CPAP), the treatment of choice for severe obstructive sleep apnoea (OSA), is effective at improving outcomes in mild OSA.
Methods: To help define the role of humidified CPAP in mild OSA, a randomised crossover study was undertaken of patients with an apnoea hypopnoea index (AHI) of 5–30/hour. Subjective sleepiness, objective wakefulness, mood, reaction time, and quality of life were measured at baseline, after 3 weeks treatment with humidified CPAP and 3 weeks sham CPAP (2 week washout).
Results: Twenty nine of 31 enrolled patients (age 25–67 years, seven women, mean (SD) body mass index 31.5 (6) kg/m2) completed the protocol. Humidified CPAP improved polysomnographic indices of OSA and Epworth Sleepiness Scale (2.4 points (95% CI 0.6 to 4.2)). Objective wakefulness (modified maintenance of wakefulness test) showed a trend towards improvement (5.2 minutes (95% CI −0.6 to 11)). Mood (Hospital Anxiety and Depression Scale), quality of life (SF 36, Functional Outcomes of Sleep Questionnaire), and reaction times (Psychomotor Vigilance Task) were not improved more than sham CPAP. Compliance with humidified and sham CPAP both averaged 4.9 hours/night. Placebo effects were evident in many outcomes and there was no clear treatment preference.
Conclusions: Humidified CPAP improves subjective sleepiness and possibly objective wakefulness but not reaction times, quality of life, or mood. These results do not support the routine use of CPAP in all patients with mild OSA, but offers some support for the trialling of CPAP in those with severe sleepiness.
- obstructive sleep apnoea syndrome
- continuous positive airway pressure
Statistics from Altmetric.com
Obstructive sleep apnoea syndrome (OSA) is a common sleep breathing disorder affecting 2–4% of the middle aged population.1 Most people with OSA have disease of mild to moderate severity with polysomnographically defined apnoea hypopnoea indices of between 5 and 30/hour (hereafter called mild).1 Continuous positive airway pressure (CPAP) is an effective treatment for severe presentations of the syndrome.2,3 However, despite six randomised controlled trials, the role of CPAP in the treatment of mild OSA remains clinically uncertain.4–9 Potential limitations of these studies include suboptimal compliance averaging 2.8 to 4.8 hours/night,7,8 moderate dropout rates of 8% to 33%,5,6 and the use of different treatment comparisons10,11 including orally ingested placebo pill4–7 and conservative management advice.8,9 Humidification of CPAP has been shown to improve adverse upper airway symptoms and initial compliance.12,13 A crossover trial structure is arguably superior for investigating a chronic condition such as OSA but has not previously been combined with sham CPAP. By using a sham CPAP device to mimic CPAP and following identical treatment procedures, it is possible to successfully maintain blinding,14 even in a crossover trial.
The current study aimed to assess the effectiveness of humidified nasal CPAP on mild OSA using a blinded, randomised, sham CPAP controlled crossover trial measuring clinically relevant changes in daytime sleepiness, mood, quality of life, and psychomotor function while measuring the effects of compliance.
METHODS
Study design and inclusion criteria
The protocol was approved by the Wellington ethics committee. Each arm of the trial was 3 weeks long with a 2 week washout period between arms included to control for carryover effects. Data were collected between November 2001 and February 2003. The number of patients in each treatment group was derived from simple coin flipping. Treatment allocation sequence was not predetermined and was achieved by the duty polysomnographic technician blindly drawing a slip of paper without replacement from an urn after testing on the first day had been completed. Patients were randomised to receive either sham CPAP or fully titrated humidified CPAP (Fisher and Paykel HC 221; Fisher and Paykel Healthcare, Auckland, New Zealand) for 3 weeks. Patients were informed that the study was “testing two different pressures of humidified CPAP”. The investigator responsible for daytime study data collection (NSM) was blinded to treatment allocation.
English speaking patients, naïve to CPAP, referred from local sleep clinics were prospectively screened for study inclusion if diagnostic polysomnography showed an apnoea hypopnoea index (AHI) of 5–30/hour. Patients were accepted if they were older than 18 years and complained of habitual snoring or nocturnal choking and at least one daytime sleepiness symptom (daytime/evening napping, sleepiness while driving, never or rarely awakening refreshed) or had an Epworth Sleepiness Score ⩾8 and gave written informed consent to be in the trial. Clinical examination, full blood cell count, electrolytes, renal function, random blood glucose and liver function tests were undertaken to exclude medical co-morbidities.
Diagnostic polysomnography was undertaken either in a tertiary level sleep laboratory (WellSleep, Bowen Hospital) or in the patients’ own home (S Series or P Series Sleep System, Compumedics, Melbourne, Australia) in accordance with accepted scientific methodology.15 At least 4 hours of sleep, including at least 30 minutes of REM sleep and 30 minutes sleeping in the supine position were required. Patients were excluded if they had a history of extreme somnolence requiring immediate treatment; performed shift work; had chronic sleep restriction (average total sleep time ⩽6 hours/night); were currently taking sedatives, antidepressants, psychotropics or stimulants; had an alcohol intake of >3 standard units/24 hours or caffeine dependency (unable to forego caffeine on testing days); had undergone upper airway surgery since the diagnostic sleep study; or had any clinically significant co-existing disease or additional sleep disorders.
It was calculated that 31 patients would be required to show a 2.5 point improvement between sham CPAP and CPAP in the Epworth Sleepiness Scale with 90% power, significance set at 0.05 and an intra-individual SD of 4.1 points in a crossover design.6
Daytime procedure
Testing began at 12.30 hours on each of the four study days at the beginning and end of each treatment arm. All testing procedures were time of day fixed. Overnight polysomnography was undertaken at the beginning of each arm for either CPAP titration or to determine the effect of the sham CPAP device.
Polysomnography and analysis
Comprehensive polysomnography included an electroencephalogram (C4-A1/C3-A2), left and right electro-oculogram, submental electromyogram, abdominal and thoracic respiratory effort (piezoelectric bands), left/right leg movements, body position, pulse oximetry, oronasal airflow (by pressure transducer and thermistor), electrocardiogram and, where appropriate, CPAP mask pressure. Studies were scored in 30 second epochs by an experienced sleep scientist (AJC, DSS) using accepted international criteria.16,17
The AHI was calculated by summing the total number of apnoeas and hypopnoeas and dividing by the number of hours of sleep. An obstructive apnoea was defined as cessation of breathing for 10 seconds or more (<20% normal airflow) with ongoing respiratory effort. Without this effort a 10 second apnoea or longer was defined as a central apnoea; combinations of effort/no effort defined a mixed apnoea. Hypopnoea was defined as greater than 50% reduction in the amplitude of at least two of the three respiratory channels (oronasal flow, thoracic, and abdominal effort) or >50% reduction in nasal pressure for at least 10 seconds accompanied by either an arousal from sleep or ⩾4% blood oxygen dip.
Continuous positive airway pressure systems
Therapeutic CPAP was determined by manual titration to abolish apnoeas, hypopnoeas, and reduce respiratory related arousals and confirmed by a sleep physician (AMN). The sham CPAP14 device was set to 8 cm H2O but actually delivered <1.0 cm H2O due to placement of a resistor at the pump outlet and a modified mask with extra holes drilled around the exhalation port (Mirage, ResMed, Sydney, Australia). The sham CPAP created conditions that were identical to CPAP at 8 cm H2O in terms of noise, mask temperature, mask humidity, and airflow through the exhalation port.
Outcome measures
Sleepiness
The Epworth Sleepiness Scale (ESS)18 and modified Maintenance of Wakefulness Test (modMWT)19,20 were used. To enhance patient recruitment and study completion we abbreviated the Maintenance of Wakefulness Test to include two 40 minute nap opportunities which were started at 13.30 and 15.30 hours. Three consecutive 30 second epochs of stage 1 or one epoch of stage 2 or higher indicated sleep onset and was measured by live visual scoring of the EEG.
Quality of life
The Functional Outcomes of Sleepiness Questionnaire (FOSQ)21 and Short Form of the Medical Outcomes Survey (SF-36)22,23 were used. The FOSQ scale was employed without the sexual functioning subscale in order to avoid differences in comparison between patients who were and were not in sexual relationships.
Mood
Mood was measured using the Hospital Anxiety and Depression Scale (HADS).24
Psychomotor performance
The Psychomotor Vigilance Task (PVT)25 was administered twice a day with a 1 minute practice session before each 10 minute data collection session at 14.30 and 16.30 hours.
Compliance with treatment
Compliance with treatment was objectively measured by an internal pressure sensor and expressed as the average number of hours of use per night (HC 221, Compliance Maximiser release 1.01; Fisher and Paykel Healthcare, Auckland New Zealand). The active CPAP compliance was the time on the face at pressure, and sham CPAP compliance was the machine run time.
Treatment preference
At the end of the trial, patients were asked which treatment was preferred and which was best for their sleep.
Data handling and statistical analyses
Significance and size of treatment effects were tested in SAS (SAS Institute, version 8) after double data entry. Paired sample t tests were used to detect changes from baseline sleep variables (or normal transformations) due to sham CPAP and to test for carryover effects between the start of each treatment arm. χ2 tests were used to test for differences in patient preferences between CPAP and placebo. Mixed model analyses of variance were employed to investigate treatment induced improvements. Results for the modMWT and PVT were averaged within the day. CPAP compliance was split at 4 hours per night and used to classify patients as high or low compliers. Treatment, order of treatment, compliance and interactions between treatment by compliance were fixed effects; individuals were random effects. Main effects and any interactions were regarded as statistically significant when p<0.05. Main effects were interpreted as favouring treatment when CPAP was significantly better than sham CPAP and the pattern from the treatment by compliance interaction subanalyses indicated a significant benefit of high compliance on CPAP over both sham CPAP compliance combinations. Effect sizes were used to verify the magnitude of the net treatment induced changes. They were calculated by dividing each mean net effect by the standard deviation of the baseline distribution for that measure. Small effect sizes were between 0.20 and 0.50, medium 0.50 and 0.80, and large effect sizes >0.80.26 All analyses were undertaken under the intention to treat principle.
RESULTS
Patient characteristics and retention
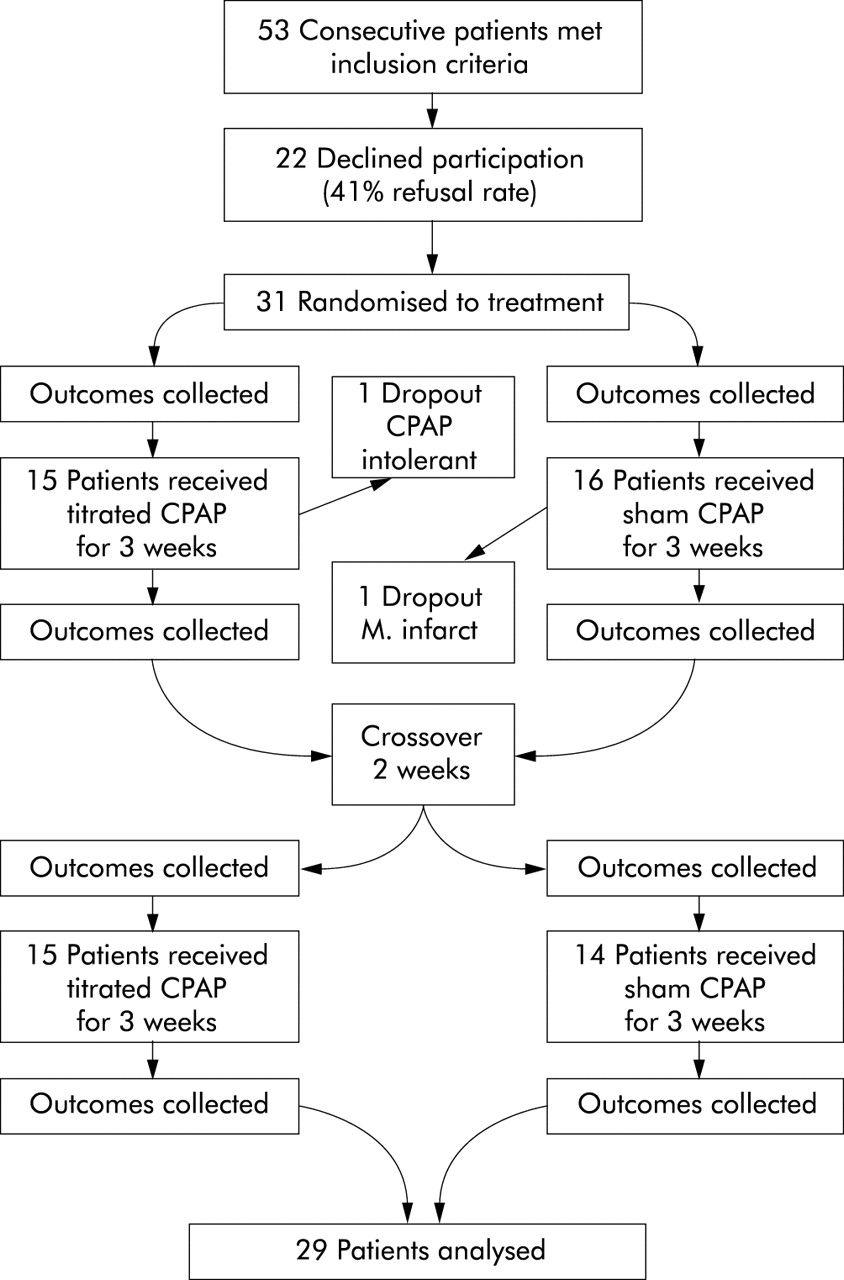
Thirty one of the 53 eligible patients (58.5%) agreed to participate. Non-participants were not significantly different in terms of age, sex, body mass indices, referral source, or AHI. Two of the 31 patients dropped out after randomisation, both in the first arm (fig 1). One suffered a non-fatal myocardial infarction during sham treatment and the other was CPAP intolerant. Patients were on average overweight (mean (SD) body mass index 31.5 (6.0) kg/m2), middle aged (mean 50.5 years, range 25–67), and predominantly male (n = 22, 76%).
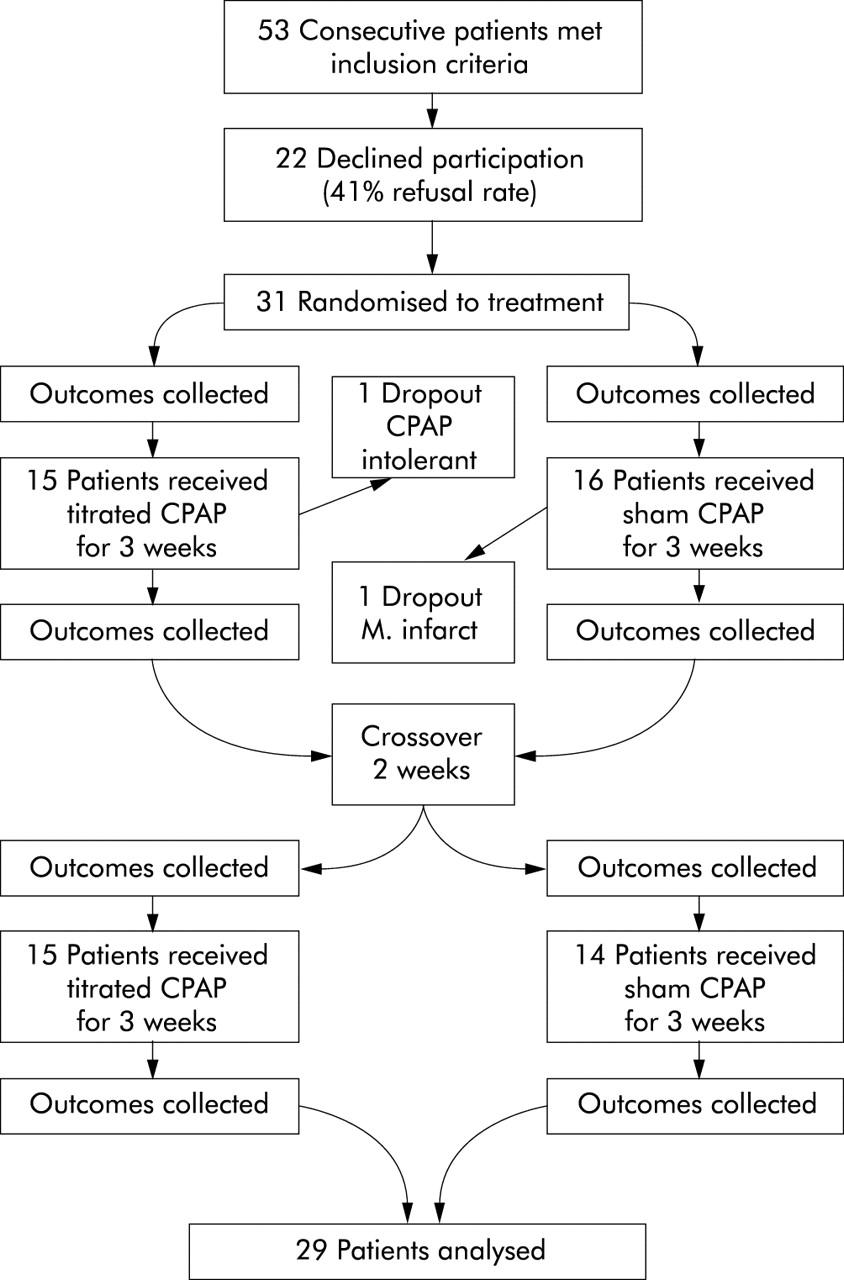
Trial flow chart.
Polysomnography at baseline and effects of placebo CPAP
Baseline polysomnography findings are shown in table 1 together with the full night effects of sham CPAP. Compared with baseline, sham treatment increased sleep latency, the percentage of stage 2 sleep, and mildly reduced sleep efficiency. There were no significant effects on the total AHI or arousal index.
Effects of a sham CPAP device on polysomnographic variables
Main effects of treatment
The main effects of CPAP and sham CPAP on all outcome measures are shown in table 2. No carryover effects were observed. Humidified CPAP improved subjective sleepiness (measure by the Epworth Sleepiness Scale). This effect size of humidified CPAP on Epworth scores (SD 4.1) was moderate at 0.58 (2.39 points, 95% CI 0.6 to 4.2). There was evidence of a dose-response relationship with subjects with a high compliance rate (⩾4 hours/night) improving by a mean (SE) of 2.6 (0.6) points while those with a low rate of compliance improved by only 0.7 (0.7) points (p = 0.04). The effects of treatment and compliance were additive; high compliance on CPAP (3.9 points) was better than both low compliance (0.4) and high compliance (1.3) on sham CPAP (fig 2).
Summary of mixed models comparing the effects of humidified CPAP with sham CPAP and effects of order, compliance, and interactions

Effects of treatment and compliance on the Epworth Sleepiness Scale. Diamonds indicate mean effects; extended vertical bars are the 95% confidence limits of the means. The figure shows that subjects with a high rate of compliance with CPAP use had improvements in sleepiness that were better than those with a high or low rate of compliance with sham CPAP.
Objective wakefulness (modified MWT) exhibited a trend towards improvement for CPAP over sham CPAP (5.2 minutes (95% CI −0.6 to 11)) with a small effect size (0.40). Mood (Hospital Anxiety and Depression Scale), quality of life (SF 36, Functional Outcomes of Sleep Questionnaire), and reaction times (Psychomotor Vigilance Task) were not improved by CPAP. Sham effects were observed in many of the measures of quality of life and mood (table 2). In the PVT mean reaction time an interaction was observed between compliance and treatment (p = 0.03) due to deterioration by poor compliers on CPAP treatment (−14 (8) ms, p = 0.07) while other groupings improved non-significantly. A significant order effect indicated a slight improvement on the first arm (10 ms) and slight worsening on the second arm (−7 ms).
Titrated CPAP pressure ranged between 5 and 10 cm H2O. Average compliance with humidified CPAP was objectively measured at 4.9 hours/night (range 0–8.4 hours). Eighteen patients (62%) used the device more than 4 hours/night, and 16 (55%) used the device on average more than 6 hours/night. Average compliance on sham CPAP was also 4.9 hours/night (range 0–8.32 hours) and followed a very similar pattern to compliance with humidified CPAP.
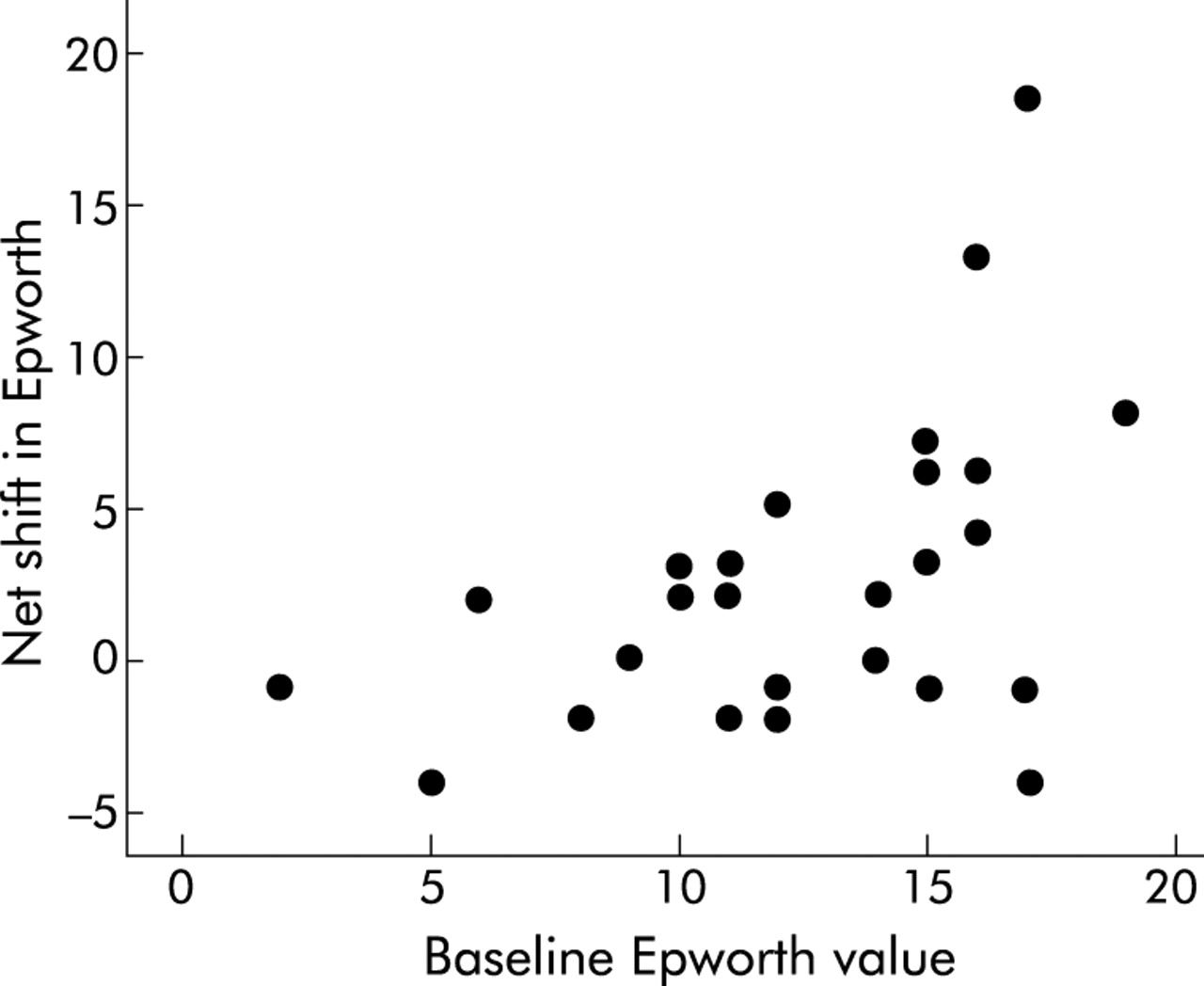
General patient preference favoured neither treatment, with 17 of 29 preferring placebo (χ2 = 0.86, p = 0.35). Nineteen thought that sham treatment was the most beneficial for their sleep (χ2 = 2.79, p = 0.09). Baseline Epworth scores were positively correlated with the sham CPAP adjusted improvements in Epworth after CPAP treatment (Pearson’s r = 0.48, p<0.01; fig 3).

{kind=link}
{kind=link}
{kind=link}
Baseline Epworth values predict response to treatment after controlling for placebo and regression to the mean effects.
DISCUSSION
In patients with mild OSA, humidified CPAP reduced subjective sleepiness compared with sham CPAP. Objective wakefulness was also improved, but this effect did not reach significance and was likely to be subject to a type II error. CPAP did not improve reaction time, mood, or quality of life. Statistically significant placebo effects were observed in a number of the subjective outcome measures. Significant strengths of the study include the use of humidification as an adjuvant to CPAP, a low level of drop outs (6.5%), relatively high compliance (4.9 hours/night), and the novel use of sham CPAP in a crossover trial.
Potential explanations for the lack of significant improvements due to CPAP therapy in the majority of outcome measures include: a small numbers of participants (type II error), lack of initial impairment, suboptimal compliance, insufficient treatment duration, or that CPAP is not an effective treatment for patients with mild OSA.
Type II errors were a potential problem with this study. Using the observed differences and variability with 80% power and a significance level of 5% in a crossover design, only two of the 19 non-significant outcome measures indicated that a reasonable number of extra patients would have been required to show the observed difference. The modMWT would have required 38 patients and the FOSQ social outcomes scale 64 patients to show the observed differences were significant. However, most of the observed modMWT effect was due to a worsening on the sham arm and would not be observed in clinical practice (table 2). All other outcomes either favoured sham CPAP over CPAP (n = 10) or would have required more than 340 patients (three required many thousands) to show significance. The vast numbers of people required to show these tiny differences lends strength to the conclusion that the effects observed are largely indistinguishable from zero and are not evidence of type II errors.
Twenty mixed models were run to test for the efficacy of CPAP therapy; improvements in subjective sleepiness might have been a type I error but, as the improvement fitted within an hypothesised dose-response relationship and is consistent with the known effects of CPAP in severe OSA,3 the result is likely to be clinically relevant. The effect size for the Epworth Sleepiness Scale (0.58) and the Maintenance of Wakefulness Test (0.40) were moderate to small, indicating potential clinical significance.
Our patient group exhibited sleep related morbidity, potentially amenable to treatment, with significant decrements compared with the normative population estimates of the Epworth Sleepiness Scale,27 Maintenance of Wakefulness Test,19,20 and in some subscales of the Functional Outcomes of Sleepiness21 and the SF-36.23
Treatment durations in previous studies of mild OSA have ranged from 4 weeks to 6 months, while this study used 3 week arms. The two trials6,7 employing 4 week treatment durations showed both treatment and placebo effects, while trials of only 1 week CPAP in a broad spectrum of OSA have also shown benefits to mood28 and neuropsychological function.29 The onset of CPAP induced reduction in sleepiness occurs within a single night of treatment and is further improved at 2 weeks but not after 6 weeks.30 In this study 3 weeks of treatment resulted in improvements in sleepiness in addition to a number of sham CPAP effects in mood and quality of life measures, indicating sensitivity over this period.
The six previously published studies4–9 of CPAP in mild OSA show few outcome measures that are consistently sensitive to CPAP therapy after adjustment for a placebo or conservative management. Patel and colleagues3 have published a meta-analysis of CPAP trials in OSA and concluded that there was insufficient evidence to show that CPAP reduced sleepiness in patients with mild to moderate levels of OSA.
As this was the first full crossover trial employing a compliance monitored sham CPAP device, it is possible to quantify some important effects. A true physiological dose-response relationship would be exhibited when highly compliant CPAP users exhibit improvements that are better than all sham CPAP effects. Only the Epworth Sleepiness Scale exhibited this expected pattern. Other significant compliance effects (table 2) do not show this pattern. Patients are not blind to their own compliance levels and are thus able to infer some of the benefit they might expect, independent of the objective benefit CPAP might confer.
This trial shows that CPAP devices set at <1 cm H2O can be effective placebo controls in a crossover design. Patients tended to prefer sham CPAP and think it better for their sleep. Despite the published concerns11 and an observation in a clinical trial31 that sham CPAP might have lower compliance rates than active CPAP, no significant difference in compliance rates were observed, nor were patients unblinded.32 Unlike other studies using a low pressure CPAP device,28,29 this device did not improve the major indices of sleep disordered breathing (table 1). Despite some worsening of overall sleep quality, 19 of 20 daytime outcome measures showed some improvement, addressing worries that sham CPAP might bias in favour of positive findings by worsening daytime function.32 Only in the modMWT did sham CPAP tend towards worse daytime function (p = 0.15). It is possible that this non-significant effect was due to poorer sleep quality caused by the sham device. These observations lend strength to the conclusion that the placebo effects on the outcome measurements are due to the expectation of benefit of the patients and not a partially beneficial effect on sleep indices of the device.
These findings show that humidified CPAP reduces subjective sleepiness and possibly objective wakefulness in a sample of symptomatic patients with mild OSA. The observed effect on subjective sleepiness could be viewed as a result of statistical chance, but the pattern of improvement is consistent with an hypothesised physiological dose-response relationship. These findings are consistent with the overall picture from other similar trials4–9 and a meta-analysis.3 The findings of this study, when viewed in context, offer little evidence that CPAP should be routinely used in the treatment of mild OSA, but offer support for the practice of trialling CPAP in patients with mild OSA and severe daytime sleepiness (fig 3).33
Acknowledgments
The authors thank Gordon Purdie for excellent statistical advice; Margo van den Berg, Karyn O’Keeffe, and Michi Imazu for polysomnograhic expertise; Nick Burgess who was largely responsible for the development of the placebo CPAP interface; and two anonymous reviewers for their excellent and expert advice regarding our manuscript.
REFERENCES
Footnotes
-
This research was supported by a grant from the Health Research Council of New Zealand (to AMN) and by a PhD stipend from Massey University (to NSM).
-
The authors declare that they have no competing interests with regard to this study. The study was not funded by industry interests and the authors at all times retained the exclusive access to the data and rights to publish.
Linked Articles
- Airwaves