Article Text

Abstract
Background: A study was undertaken to assess the reliability of the nasal mucociliary transport test using 99mTc-albumin colloid as a screening test for primary ciliary dyskinesia (PCD) and to compare it with the gold standard nasal biopsy for study of ciliary motility and ultrastructure.
Methods: During a 4 year period both tests were performed in 55 children referred with persistent or recurrent respiratory tract infections. Their median age was 4 years (range 1 month to 15 years).
Results: The nasal biopsy results were as follows: PCD, n = 8; secondary ciliary dyskinesia (SCD), n = 19; normal, n = 28. The mucociliary transport test was abnormal in 29 patients (all 8 with PCD, 7/19 with SCD, and 14/28 with a normal biopsy). The sensitivity of the mucociliary transport test to diagnose PCD was therefore 100% (8/8) (95% exact confidence limits 63.06 to 100.00); the specificity was only 55% (26/47) (40.95 to 69.89). The negative predictive value was 100% (26/26) (86.77 to 100.00) and the positive predictive value was 28% (8/29) (12.37 to 47.24).
Conclusion: Mucociliary transport is a non-invasive screening test that can be performed even in infants. The sensitivity of the test is high but its specificity is low. A normal test result excludes PCD.
- PCD, primary ciliary dyskinesia
- SCD, secondary ciliary dyskinesia
- primary ciliary dyskinesia
- screening test
- mucociliary transport
- diagnosis
Statistics from Altmetric.com
Primary ciliary dyskinesia (PCD) is a group of rare autosomal recessive diseases.1 Chronic or recurrent infections of the upper and lower respiratory tract are the usual presenting symptoms but there are no pathognomonic signs or symptoms. The reported incidence is around 1/20 000 but the true incidence is most likely underestimated.2
At present the age at diagnosis of PCD varies from newborn to the fifth decade.3 Chest physiotherapy and antibiotics are the mainstay of treatment and aim at preventing bronchiectasis and progressive lung damage.2 With early diagnosis, proper follow up and treatment prognosis may be good and pulmonary function usually remains stable for many years.4 The definitive diagnosis of PCD requires time consuming tests during which ciliary motion, ultrastructure, and regeneration in vitro are studied.5–7 The gold standard is electron microscopy to demonstrate dynein arm deficiency, the most frequent cause of PCD.8 Recurrent respiratory infections are a very frequent problem but PCD is a rare disease and the diagnostic tests are invasive and expensive. Early diagnosis of PCD by a reliable and relatively easy screening test would limit the number of patients in whom additional tests are necessary.
Abnormal ciliary function results in inefficient mucociliary transport. Tests of mucociliary transport can therefore be used to screen for PCD. The saccharin test is most often used.9,10 A 1–2 mm particle of saccharin is placed on the inferior nasal turbinate and the time to tasting saccharin is noted. Since young children cannot reliably report this, the test cannot be used in young children.2 Hence, it does not allow early diagnosis. Likewise, measurement of nasal nitric oxide (NO) is a promising screening test but the need for the patient to hold his/her breath during the measurement makes it impossible for use in children younger than 6 years.11 As an alternative, nasal mucociliary transport tests using 99mTc-colloid have been suggested.12 These tests do not require patient cooperation.
The aim of the present study was to assess the reliability of the nasal mucociliary transport test with 99mTc-albumin colloid as a screening test for PCD in clinical practice. We therefore performed both nasal biopsies for measurement of ciliary function and structure as well as mucociliary transport tests with 99mTc-albumin colloid in 55 consecutive children referred for evaluation of chronic or recurrent upper and lower respiratory tract infections.
METHODS
Patients
During a 4 year period, mucociliary transport tests and nasal biopsies for study of ciliary motility and ultrastructure were performed in 55 children newly referred to our paediatric pulmonary clinic for recurrent or persistent upper and lower respiratory tract infections. These tests were only performed after diseases more common than PCD such as atopic asthma, cystic fibrosis, humoral immunodeficiency and gastro-oesophageal reflux had been ruled out by “first wave tests” according to the diagnostic schedule of Bush et al.2 In patients with recurrent sinopulmonary disease and dextrocardia, ciliary function was examined before other diagnostic tests. Tests were performed at least 3 weeks after an acute upper respiratory tract infection.
Mucociliary transport study with 99mTc-albumin colloid
Two radioactive reference sources were applied: one beside the nasal tip and one anterior to the right tragus. 99mTc-colloid particles labelled with 50 µC 99mTc dissolved in 2.5 µl saline were deposited on the nasal floor about 1 cm past the right naris using a Hamilton syringe. To minimise patient discomfort, young children were placed on the nurse’s or mother’s lap, the camera facing the right profile of the patient (fig 1). A series of 30 second planar images was acquired during a 10 minute period. The motion of the deposited droplet relative to the reference sources was evaluated on these images and displayed dynamically in an endless loop cinematographic mode. Coughing, crying, sniffing, and sneezing did not influence the test result. We confirmed this by using a very small test volume (2.5 μl) and by asking adult volunteers to simulate these actions and also by observing the data sets in children who cried during part of the data collection. The effective dose equivalent of administration of 50 µC 99mTc is 25 µSv (that is, minimal). The effective dose for a chest CT scan is 8000 µSv.

Toddler sitting on the nurse’s lap, the camera facing the profile of the child. Two radioactive reference sources are applied, one beside the nasal tip and the other anterior to the right tragus.
When mucociliary transport is normal, the droplet travels at least halfway towards the posterior reference point within 10 minutes (fig 2). The test is considered abnormal when no motion towards the posterior reference source is detected or when the droplet travels less than half the distance (fig 3). If the child does not sit very still the images are somewhat blurred, but usually still easily interpretable. Total lack of cooperation during the test is very rare and only occurred three times during the 4 year study period.
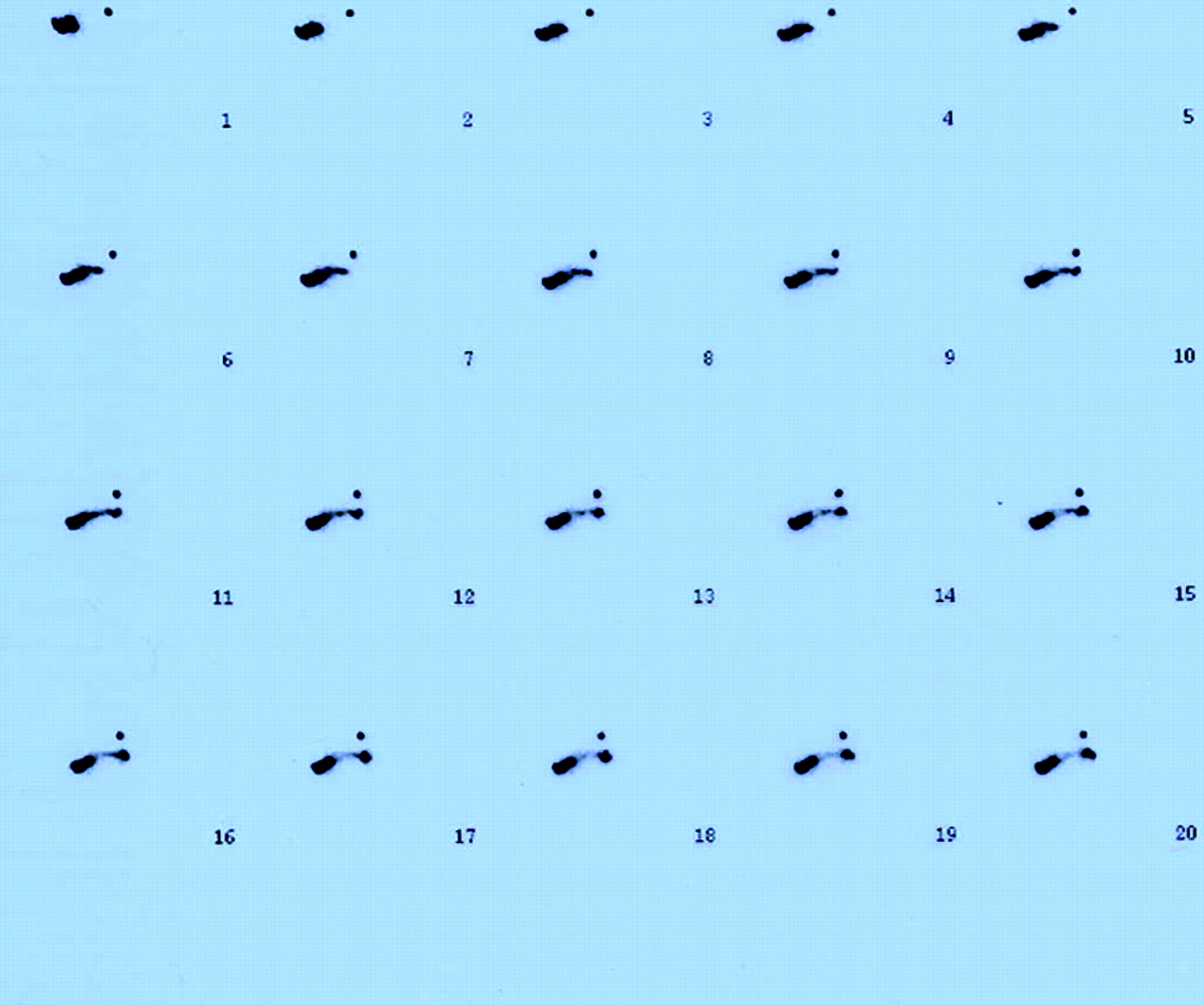
Normal mucociliary transport study using 99mTc in a 3 year old girl. Series of 30 second planar images. On all the images the reference sources remain in the same position but over time the droplet deposited on the nasal floor progressively moves from the anterior radioactive reference source towards the posterior reference radioactive source.

{kind=link}
{kind=link}
{kind=link}
Abnormal mucociliary transport study using 99mTc in a 6 year old girl. Series of 30 second planar images. On all the images the reference sources remain in the same position and over time the droplet deposited on the nasal floor stays in the same position relative to the reference sources.
Ciliary motility and structure
After local anaesthesia a mucosal biopsy specimen was taken from the inferior border of the middle turbinate or from the posterior part of the inferior turbinate. Biopsy specimens were placed in cell transport medium before being evaluated for coordinated ciliary beating and beat frequency both before and after ciliogenesis.7,13,14
Coordinated ciliary beating was defined as the presence of rotation of cells or cell clusters in the medium, or the presence of active and directed movement of fluid and particles along the ciliary lining caused by ciliary beating. The ciliary beat frequency was measured using computerised microscope photometry at room temperature. It was defined as the first harmonic of a Fast Fourier Transform analysis of a record of the variations in light intensity. For each biopsy, 10 cells were recorded during 1 minute, giving 10 data based on 10 consecutive 5 second periods. At our laboratory the normal mean (SD) value for ciliary beat frequency at room temperature is 7.9 (1.8) Hz.13
Part of the biopsy specimen was processed for transmission electron microscopy. The material was fixed in 3% glutaraldehyde in 0.1 M sodium cacodylate buffer (pH 7.4) for 2 hours. It was additionally fixed in OsO4 in 0.1 M phosphate buffer (pH 7.4) for 1 hour, dehydrated in a graded ethanol series, and then embedded in epoxy resin. Before preparing the material for transmission electron microscopy (Philips 201) the 1 μm sections were evaluated for cilia. The following variables were qualitatively and quantitatively evaluated and specific abnormalities were scored before and after ciliogenesis: outer and inner dynein arms, central pair of microtubules, spokes, peripheral microtubules, ciliary membrane, and compound cilia.
The major part of the biopsy specimen was treated for cell culture in the sequential monolayer suspension culture procedure to evaluate the cilia after ciliogenesis as described above. In case the cell culture did not grow, a repeat biopsy was performed and processed in the same way. This occurred in 13 (24%) of the 55 patients.
A diagnosis of PCD was made when ciliary motility was absent after ciliogenesis or when we found outer and/or inner dynein arm deficiency, absent central pair or radial spokes in an abnormal proportion of ciliary cross sections. A PCD diagnosis was always confirmed in a second biopsy sample. Secondary ciliary dyskinesia (SCD) was diagnosed when more than 50% of ciliary cross sections contained anomalies such as compound cilia, an abnormal number of peripheral microtubules or ciliary membrane abnormalities.14,15
RESULTS
Over a 4 year period both a mucociliary transport screening test and a nasal biopsy with study of ciliary motion and structure were performed in 55 children aged 1 month to 15 years (median age 4 years; quartile range 2–6 years).
The nasal biopsy results were: PCD, n = 8; SCD, n = 19; normal, n = 28 (table 1). The mucociliary transport test was abnormal in all eight patients with PCD, in seven of 19 patients with SCD, and in 14 of 28 patients with normal biopsy results. For calculation of sensitivity, specificity, and predictive values, all patients without PCD (normal biopsy results and SCD) were combined. The sensitivity of the mucociliary transport test to diagnose PCD was therefore 100% (8/8) (95% exact confidence limits 63.06 to 100.00) but the specificity was only 55% (26/47) (40.95 to 69.89). The negative predictive value was 100% (26/26) (86.77 to 100.00) and the positive predictive value was 28% (8/29) (12.37 to 47.24).
Global results of mucociliary transport test versus nasal biopsy result
There was no age difference between patients with or without PCD (p = 0.24; Mann-Whitney U test) nor between patients with a normal screening test and those with an abnormal screening test (p = 0.53; Mann-Whitney U test). Five patients with PCD had outer dynein arm deficiency, associated in one patient with inner arm deficiency. In these patients the mean (SD) number of dynein arms per cilium ranged from 1.0 (0.9) to 1.6 (1.1) compared with the normal value of 8.4 (0.8). Three patients had absent motility but normal ultrastructure. Three patients with PCD had situs inversus.
DISCUSSION
This is the first large field study to validate the mucociliary transport test using 99mTc-albumin colloid as a screening test for PCD. Over a 4 year period mucociliary transport as well as ciliary motility and ultrastructure were assessed in 55 children with recurrent or chronic respiratory symptoms. All patients were newly referred for diagnostic work-up. The test has an excellent sensitivity: all children with an eventual diagnosis of PCD were correctly identified. However, the positive predictive value of the test is poor since only eight of 29 patients with an abnormal test in fact had PCD. The negative predictive value of the mucociliary transport screening test is excellent: a normal test makes the diagnosis of PCD highly improbable. In the present work-up further diagnostic tests could have been avoided in 26 of the 55 examinations performed, thus saving the patient pain and discomfort and the parents, physicians and technicians time and resources.
A normal test is also seen in patients with SCD, a non-specific diagnosis in patients with acute or chronic respiratory conditions of several aetiologies.14,15 Indeed, certain infectious agents, smoke, and other noxious substances may induce ciliary damage that results in mucociliary transport dysfunction. These changes are often transient and disappear after ciliogenesis in cell culture.14
Previous authors have alluded to the usefulness of a mucociliary clearance nasal screening test reporting abnormal results in isolated patients with PCD,16–18 but the reliability of the test in clinical practice has never been evaluated. When on their mother’s lap, even small children are only briefly and minimally disturbed during the mucociliary transport test and, because of the small test volume needed, the radiation dose is also minimal.
Other screening tests have been suggested. Santamaria et al19 report that the study of ciliary motility using light microscopy is not reliable, and the saccharin screening test10 cannot be performed in non-cooperative children.2 Apart from mucociliary screening tests, measurements of exhaled and nasal nitric oxide are useful. Exhaled and—even more so—nasal nitric oxide (NO) levels have consistently been reported to be low in patients with bronchiectasis (with or without cystic fibrosis) and very low in patients with PCD.11,20–22 Although there is a significant overlap in NO values between these patient groups, using 187 ppb and 2.4 ppb for nasal and exhaled NO, respectively, the sensitivity to diagnose PCD was 98% and the positive predictive value 92%.11 However, the study group consisted of adult patients with known diagnoses. In the study by Narang et al21 all patients were older than 6 years “to enable measurements of NO”. Although the specificity of NO measurements as a screening test for PCD may be very high, it has not yet been evaluated in a field study in young children. We did measure nasal NO levels in some of the patients with PCD and found it to be low. We have, however, been unable to measure nasal NO reliably in infants. Indeed, one cannot ask infants and toddlers to hold their breath, as required for NO measurements. The main need for an alternative screening test is that, at present, NO measurements are not applicable in infants and toddlers—the age at which a screening test is most warranted. Indeed, in a recent paper the mean age at diagnosis of PCD using the conventional diagnostic methods was reported to be 4 years.23
The diagnostic work-up of a patient with PCD is complex and time consuming. Most physicians would exclude other more common diseases by appropriate tests before embarking on the tedious ciliary function and structure tests. The reported mucociliary screening test is easy and can even be performed in infants. In older children it can be an alternative to using nasal and exhaled NO as a screening test if an NO analyser is not available. It has the potential of excluding the diagnosis in young children earlier in the work-up, thus favouring correct diagnosis of PCD at an earlier age.
In conclusion, the mucociliary transport test using 99mTc is a non-invasive and reliable screening test that can be performed even in infants. The sensitivity of the test is high but its specificity is low. A normal test result excludes PCD. Patients with an abnormal test result need to be further evaluated by definitive diagnostic tests.
Acknowledgments
The authors thank Professor Em R Eeckels for valuable criticism and Mrs E Aertgeerts for excellent secretarial assistance.