Article Text

Abstract
Background Pulmonary hypertension (PH)-targeted therapy in the setting of pulmonary fibrosis (PF) is controversial; the main clinical concern is worsening of systemic hypoxaemia. We sought to determine the effects of gentle initiation and chronic administration of parenteral treprostinil on right heart function in patients with PF associated with an advanced PH phenotype.
Methods Open-label, prospective analysis of patients with PF-PH referred for lung transplantation (LT). Advanced PH was defined as mean pulmonary artery pressure (mPAP) ≥35 mm Hg. We compared haemodynamics, Doppler echocardiography (DE), oxygenation, dyspnoea and quality of life indices, and 6 min walk distance (6MWD) before and 12 weeks after parenteral treprostinil.
Results 15 patients were recruited in the study. After therapy, there were significant improvements in right heart haemodynamics (right atrial pressure (9.5 ± 3.4 vs 6.0 ± 3.7); mPAP (47 ± 8 vs 38.9 ± 13.4); CI (2.3 ± 0.5 vs 2.7 ± 0.6); pulmonary vascular resistance (698 ± 278 vs 496 ± 229); transpulmonary gradient (34.7 ± 8.7 vs 28.5 ± 10.3); mvO2 (65 ± 7.2 vs 70.9 ± 7.4); and stroke volume index (29.2 ± 6.7 vs 33 ± 7.3)) and DE parameters reflecting right heart function (right ventricular (RV) end diastolic area (36.4 ± 5.2 vs 30.9 ± 8.2 cm2), left ventricular eccentricity index (1.7 ± 0.6 vs 1.3 ± 0.5), tricuspid annular planar systolic excursion (1.6 ± 0.5 vs 1.9 ± 0.2 cm)). These changes occurred without significant alteration in systemic oxygenation, heart rate, or mean systemic arterial pressure. In addition, improvements were seen in 6MWD (171 ± 93 vs 230 ± 114), 36-Item Short Form Health Survey Mental Component Summary aggregate (38 ± 11 vs 44.2 ± 10.7), University of California, San Diego Shortness of Breath Questionnaire (87 ± 17.1 vs 73.1 ± 21), and brain natriuretic peptide (558 ± 859 vs 228 ± 340).
Conclusions PH-targeted therapy may improve right heart haemodynamics and echocardiographic function without affecting systemic oxygen saturation in an advanced PH phenotype associated with RV dysfunction in the setting of PF.
- Primary Pulmonary Hypertension
- Lung Transplantation
- Interstitial Fibrosis
Statistics from Altmetric.com
Key messages
-
What is the key question?
-
What are the effects of parenteral treprostinil on right heart function of patients with pulmonary fibrosis (PF) referred for lung transplantation (LT) with an advanced pulmonary hypertension (PH) phenotype?
-
What is the bottom line?
-
Parenteral treprostinil improves right heart haemodynamics and echocardiographic function without affecting systemic oxygen saturation in PH-PF with an advanced PH phenotype.
-
Why read on?
-
This pilot study suggests parenteral treprostinil improves right ventricle function and is a safe therapeutic option in patients with PH-PF with an advanced PH phenotype; as such, this approach may be a consideration for patients with advanced PH-PF if they are ineligible for, or as a bridge to, LT.
Introduction
Pulmonary hypertension (PH) may complicate pulmonary fibrosis (PF) of different causes, but few studies have focused on the treatment of advanced PH in this context.1–4 Furthermore, no prospective chronic parenteral prostanoid administration studies are available in patients with PF homogenised for the less common advanced PH phenotype, characterised by significantly altered right heart haemodynamics and right ventricular (RV) dysfunction. We previously reported a case where the rationale for parenteral treprostinil as a bridge to lung transplantation (LT) was outlined in the index patient with PF-PH for this study.5 Importantly, parenteral prostanoid therapy associated with worsening of ventilation-perfusion (V-Q) mismatch and subsequent hypoxaemia remains a major clinical concern. The purpose of this pilot study was to evaluate the effects of acute and subsequent chronic parenteral treprostinil therapy on right heart haemodynamics and echocardiographic function in patients with PH referred for LT in the setting of an advanced PH phenotype and right heart dysfunction.
Materials and methods
This study was approved by the IRB at University of California, Los Angeles (UCLA IRB# 07-11-087-03; clinicaltrials.gov Identifier NCT00705133). We recruited 15 outpatients with PF referred to our LT programme between July 2008 and January 2011 who had advanced PH based on right heart catheterisation (RHC) (figure 1). Sarcoidosis and systemic sclerosis spectrum of disease were excluded, as were patients requiring >10 L/min of oxygen at baseline. Importantly, threshold measures of right heart size and/or function were not required for study enrolment. Patients with combined pulmonary fibrosis emphysema were included.6 Formal pulmonary rehabilitation was not prescribed during the study period.

Recruitment of patients (n=15) with pulmonary fibrosis and advanced pulmonary hypertension being evaluated for lung transplantation at a single tertiary medical centre between July 2008 and January 2011. CPFE, combined pulmonary fibrosis emphysema; mPAP, mean pulmonary artery pressure; NSIP-F, non-specific interstitial pneumonia fibrosis; PAH, pulmonary arterial hypertension; PF, pulmonary fibrosis; PVR, pulmonary vascular resistance.
Advanced PH was defined using haemodynamic criteria: mean pulmonary artery pressure (mPAP) ≥ 35 mm Hg, pulmonary artery wedge pressure (PAWP) ≤ 15 mm Hg, and pulmonary vascular resistance (PVR) > 240 dyn s/cm5. Other PH aetiologies were ruled out based on current recommendations.7 All follow-up RHCs were performed after ≥12 weeks of stable dose background PH-targeted therapy, and background PF-related therapy remained unaltered during the study period.
Six minute walk distance and oxygen supplementation protocols
Patients were ambulated per American Thoracic Society criteria with a modification regarding oxygen supplementation (OS), given the inherent hypoxaemia in this patient population (see online supplementary repository).8
Pulmonary function testing and Doppler echocardiogram protocols
Pulmonary function testing (PFT) was obtained at treprostinil initiation and at 12 weeks and included forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), FEV1/FVC ratio and single-breath diffusing capacity for carbon monoxide (DLCO). Total lung capacity (TLC) was only performed at baseline. Doppler echocardiogram (DE) was performed using conventional equipment (Hewlett-Packard, Palo Alto, California, USA) at baseline and 12 weeks (see online supplementary repository).
Dyspnoea and quality of life assessments
Dyspnoea was measured with the University of California, San Diego Shortness of Breath (UCSD SOB) questionnaire and the Borg Dyspnoea Index (BDI) (see online supplementary repository).
Health-related quality of life was measured with the 36-Item Short Form Health Survey (SF-36). SF-36 scales are summarised into Physical Component (PCS) and Mental Component (MCS) Summary scores. The eight SF-36 scales and the PCS and MCS scores are standardised to a mean of 50 and an SD of 10 in the general US population. Minimally important difference (MID) estimates for SF-36 PCS and MCS are 2.5 points (see online supplementary repository).
Parenteral treprostinil titration protocol
All patients were hospitalised for 48 h for treprostinil initiation and uptitration (see online supplementary repository).
High-resolution CT lung parenchymal scoring
Thin slice (<3 mm) CT scans were used for objective assessment of lung parenchymal abnormality at baseline (see online supplementary repository).
Study parameters
Patient assessments were made at baseline and after 12 weeks of parenteral treprostinil and included RHC and systemic haemodynamics, echocardiographic parameters, 6 min walk distance (6MWD), PFT, systemic and central oxygenation, brain natriuretic peptide (BNP), and SF-36/UCSD SOB questionnaires.
Statistics
Baseline characteristics were described as frequencies (%) for categorical variables and means (SD) for continuous variables. Clinical, haemodynamic, and echocardiographic data were reported at baseline and 12 weeks, and the Shapiro–Wilk test was used to assess the normaility of the distributions of baseline and week 12 data. For variables where normality was rejected at the p<0.05 level, median (IQR) values were reported and the Wilcoxon signed rank test was used to compare DLCO (% predicted), FVC%/DLCO%, 6 min walk 10 L face mask (FM) (% saturation), SF-36 Physical Functioning, stroke volume (SV), and systolic blood pressure (SBP) measures at baseline and week 12. For all other clinical, haemodynamic, and echocardiographic variables, mean (SD) were reported and paired t tests were used to compare variables at baseline and week 12. Q-values were computed to assess the impact of multiple comparisons in the domains of pulmonary function, quality of life, and haemodynamics. Analyses were conducted with Stata V.13 (Stata Corp LP, College Station, Texas, USA), and p values <0.05 were considered statistically significant.
Results
Demographics
Fifteen patients aged 63 ± 15 years (mean ± SD) (20% female) referred for LT met all study criteria and agreed to enrolment (figure 1). Baseline WHO functional class was equally split with 53% class III (n=8) and 47% class IV (n=7). Background PH therapy (≥12 weeks of stable dose therapy) and the underlying clinical diagnoses regarding the aetiology of the PF are displayed in table 1. A subgroup of clinical diagnoses (n=10) had pathological confirmation made by surgical lung biopsy (n=2), eventual explantation (n=7), or autopsy (n=1) (see online supplementary repository table S2). Individual patient data are presented in the repository (see online supplementary table S1). The extent of baseline lung parenchymal abnormality by high-resolution CT (HRCT) chest imaging is reported for each patient in the repository (see online supplementary table S2).
Patient demographics, underlying fibrotic lung disease clinical subtype, and background PH-targeted therapy
Safety/adverse events
Of the 15 patients, 14 patients received subcutaneous treprostinil and 1 patient was placed on intravenous treprostinil.5 The treprostinil dose for the group at 12 weeks was 34 ± 21 ng/kg/min (mean ± SD) and a range of 18–97 ng/kg/min. During inpatient treprostinil initiation, there were no changes in vital signs, particularly oxygen saturation by peripheral pulse oximetry (PPO), or adverse haemodynamic changes that led to acute discontinuation of the medication. During inpatient and outpatient treprostinil uptitration, patients experienced typical prostanoid effects, including jaw pain, diarrhoea, lower extremity bone pain, site pain/reaction, headache, and/or flushing.9
Pulmonary function testing, 6MWD, and oxygen status
The mean (±SD) baseline % predicted values for FEV1, FVC, TLC, and FEV1/FVC ratio were 62 (17), 62 (21), 70 (15), 77 (11), and 24 (13), respectively and the median (IQR) baseline % predicted value for DLCO was 24 (13); for the cohort of patients without CPFE (n=12), baseline TLC was 67 (16). There were no significant changes in PFT parameters following 12 weeks of treprostinil (table 2). Comprehensive individual patient data are presented in the repository (see online supplementary table S3).
Pulmonary function testing, oxygen requirements, and 6 min walk distance with Borg Dyspnoea Index (BDI) scores at baseline and end of study
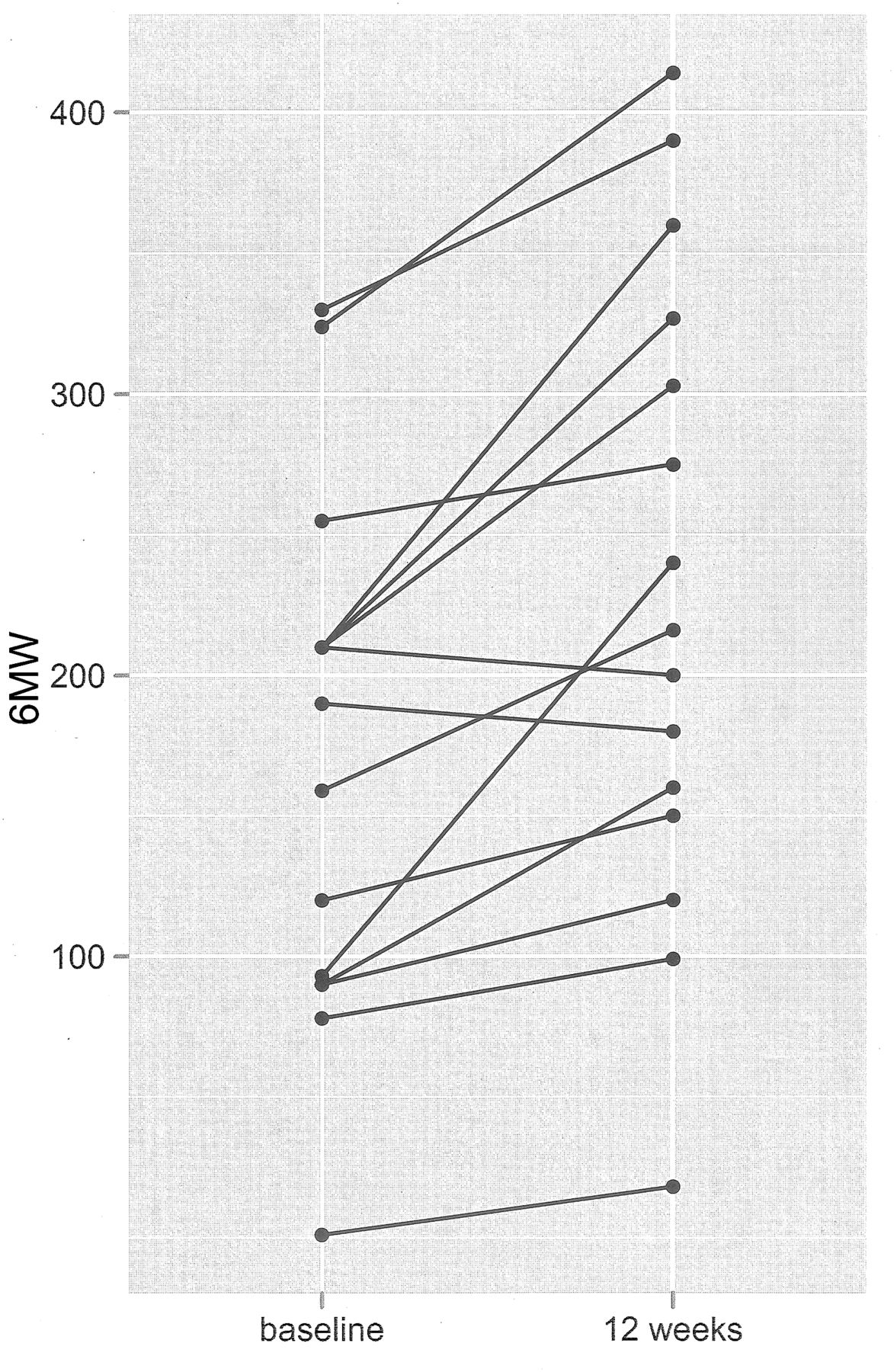
The baseline 6MWD (mean ± SD) was 171 ± 93 m with a resting room air pulse oximetry of 83 ± 7%. All except one patient required oxygen supplementation at rest; 11 of 15 (73%) required ≥3 L of oxygen supplementation at rest. Table 2 shows the 6MWD improvements following 12 weeks of parenteral treprostinil therapy (mean 59 m; p<.001). Specifically, 8 of 15 patients improved by ≥57 m (range 57–150); 5 improved by ≥17 m (range 17–30); and 2 patients each declined by 10 m (figure 2). At 12 weeks, there were no significant differences in baseline oxygen requirements (see online supplementary repository figure S1) or oxygenation parameters by PPO either at rest on room air, at rest on 10 L FM, or at the completion of the 6MWD test on 10 L FM (table 2). Individual patient data are presented in the repository (see online supplementary table S3).

Individual 6 minute walk (6MW) distance responses to parenteral treprostinil at baseline and 12 weeks.
SF-36, UCSD SOB and BDI assessments
Patients had a statistically significant improvement in UCSD SOB and SF-36 MCS scores at the end of the study (p<0.05; table 3). When we assessed the clinical significance of these improvements, 77% and 50% had improvement ≥MID estimates for UCSD SOB and SF-36 MCS, respectively. Additionally, there was no significant change in SF-36 PCS and BDI (table 3) between baseline and 12 weeks. Individual patient data are presented in the repository (see online supplementary table S4).
Quality of life and dyspnoea score changes using Short Form 36 (SF-36) and University of California San Diego Shortness of Breath (UCSD SOB) questionnaire
Haemodynamics, BNP and Doppler echocardiography
All 15 patients had baseline mPAP ≥ 35 mm Hg; 10 (66%) had mPAP ≥ 40 mm Hg and 7 (47%) had mPAP ≥ 50 mm Hg. The transpulmonary gradient (TPG) at baseline was ≥20 mm Hg for all patients and ≥30 mm Hg in 12 of 15 (80%) patients. The average PVR was 698 ± 278 dyn s/cm5, representing 44% of the mean systemic vascular resistance (SVR). The baseline PVR was ≥480 dyn s/cm5 in all but three patients. Following 12 weeks of treprostinil, there was evidence of decreased RV afterload, as per significant reductions in mPAP, TPG, PVR, and increased pulmonary capacitance (table 4; see online supplementary repository figure S2). Right heart function improved, as per reductions in right atrial pressure and increased mixed venous oxygen saturation, cardiac index and SV index (table 4). Although the SBP fell by 11 mm Hg (124 ± 21 to 113 ± 13 mm Hg; p=0.028), the mean systemic arterial pressure was not altered and there was a downward trend in the PVR/systemic vascular resistance (SVR) ratio (p=0.060), suggesting proportionally greater pulmonary than systemic vasodilation. Importantly, there were no significant changes in resting heart rate, arterial oxygen content, or oxygen delivery. Individual patient data are presented in the repository (see online supplementary table S5).
Systemic and pulmonary haemodynamics and oxygenation at baseline compared with 12 weeks after parenteral treprostinil therapy
The two-dimensional echocardiographic examination at baseline revealed normal left ventricular cavity size (LV end-diastolic dimension 4.1 ± 0.5 cm) and systolic function (LV ejection fraction 64 ± 6%), and Doppler evidence of normal left atrial pressure (transmitral Doppler E/e’ ratio 5.4 ± 1.4). In contrast, subjects were noted to have severe RV dilatation (RV end-diastolic area 36.4 ± 5.2 cm2), marked right-to-left displacement of the interventricular septum (systolic eccentricity index 1.7 ± 0.6) and moderate RV systolic dysfunction (tricuspid annular planar systolic excursion (TAPSE) 1.6 ± 0.5 cm; see online supplementary repository figure S3). Doppler estimated pulmonary artery systolic pressure at baseline was 72 ± 12 mm Hg. The RV outflow tract (RVOT) acceleration time was markedly reduced (66 ± 16 ms) and 100% of subjects showed evidence of systolic flow deceleration or ‘notching’ of the RVOT Doppler envelope. Of note, 85% of subjects showed evidence of both a TAPSE <2.0 cm and RVOT Doppler notching, consistent with afterload-dependent RV dysfunction at baseline.
Figure 3 illustrates that following 12 weeks of parenteral treprostinil treatment, there were significant reductions in RV size (p=0.021), less evidence of interventricular septal flattening (p=0.037), and improved RV systolic function (p=0.006). In parallel with haemodynamic and echocardiographic evidence of RV unloading, BNP levels fell significantly in subjects at 12-week follow-up (table 4).

{kind=link}
{kind=link}
{kind=link}
Bar graphs comparing indices of right ventricular size (RV end diastolic area), interventricular septal position (systolic eccentricity index), and RV systolic function (tricuspid annular planar systolic excursion) at baseline (open bars; n=15) and following 12 weeks of parenteral treprostinil (solid black bars; n=14), with error bars indicating SE. Paired t test results indicate significant improvements in RV size (p=0.021), interventricular septal flattening (p=0.037), and RV systolic function (p=0.006) indices from baseline to week 12. TAPSE, tricuspid annular planar systolic excursion.
Patient status
Of the 15 patients, 8 were actively listed for LT (figure 1). Of the 7 patients not offered LT, 5 died (mean ± SD) 504 ± 295 days after treprostinil initiation, while 2 patients remained alive 1059 and 1401 days after treprostinil initiation. After active listing, 7 patients were successfully bridged to LT which occurred at a median of 268 days (range 140–1379 days) after the baseline RHC and treprostinil initiation. The remaining listed patient died 272 days after treprostinil initiation.
Discussion
The purpose of this investigation was to assess the effects of chronic parenteral treprostinil administration on right heart haemodynamics and echocardiographic function in a PF population referred for LT with an advanced PH phenotype, characterised by significantly increased PVR and RV dysfunction.10 We studied this population either as a bridge to LT or to achieve clinical stabilisation in otherwise transplant ineligible patients at risk of clinical deterioration due to advanced PH and right heart dysfunction.5 ,7 ,10 Significant improvements were demonstrated in right heart haemodynamics and echocardiographic function in response to chronic parenteral treprostinil infusion, without significant decrement in peripheral oxygen saturation, arterial oxygen content, or oxygen delivery.
At baseline, our subjects had a markedly elevated PVR, moderate to severe RV dysfunction, and thus abnormal coupling between the RV and pulmonary vascular load. In the context of significant RV–pulmonary artery uncoupling, RV afterload reduction leads to a predictable, afterload-dependent improvement in right heart function, as was seen in our cohort by way of improved haemodynamics and echocardiographic parameters.11 These improvements in RV afterload and RV function (enhanced RV coupling) likely augmented the circulatory reserve of our patients, explaining their functional advantage and decreased dyspnoea.
The potential for worsening gas exchange with PH-targeted therapy deserves particular attention. We did not appreciate any significant hypoxaemia as assessed by PPO after treprostinil therapy, either at rest or after 6MWD testing. Importantly, pulmonary function (ie, degree of PF) remained unaltered during the study and did not likely confound these findings. Although arterial blood gases (ABG) were not obtained to confirm this finding, we can suggest a rationale based on the available literature. Prior work using multiple inert gas elimination technique (MIGET) has demonstrated a relatively preserved V-Q spectrum at rest, manifesting absent or mild resting hypoxaemia in patients with either WHO Group I pulmonary arterial hypertension (PAH)12 or isolated PF.13 Importantly, during exercise, the MIGET-derived V-Q spectrum remains preserved in both conditions, despite predictable widening of the alveolar-arterial gradient and hypoxaemia.13–15 In PAH, this hypoxaemia is driven by a low mixed venous pO2,14 while in PF, hypoxaemia is characterised by a relative augmentation in diffusion abnormality, which in turn is further accentuated by low mixed venous oxygenation.16 Consequently, a PH-targeted therapy that augments mixed venous oxygenation may be particularly desirable in a cohort of patients with PF and advanced PH to attenuate any predisposition for hypoxaemia at rest or during exercise.
The use of acute15 or chronic17–20 PH-targeted, non-prostanoid therapy does not appear to alter gas exchange in patients with PF without advanced PH during rest or exercise, which challenges the notion of predictable V-Q inequality and hypoxaemia as a direct result of underlying fibrotic lung disease. Despite this finding, acute parenteral prostanoid administration in patients with PF and advanced PH raises concern for predictable intrapulmonary shunt and hypoxaemia.3 ,21 Interestingly, even patients with PAH (WHO Group I) demonstrated increased shunt by MIGET during acute parenteral prostanoid administration.22 The question is whether this potential shunt and hypoxaemia are related to the parenteral route of administration or to the aggressive uptitration strategy routinely implemented when initiating parenteral prostanoid therapy.23 In fact, prior studies evaluating acute parenteral prostanoid administration in PAH22 and PF associated with advanced PH3 ,21 employed this same aggressive uptitration protocol and report relatively worsened gas exchange, V-Q spectrum, and systemic haemodynamic data specifically at the prostanoid dose associated with intolerable adverse reaction and/or unacceptable haemodynamic deterioration. Similar and predictable V-Q inequality has also been demonstrated with other aggressively titrated, non-prostanoid vasodilators in patients with PAH.24
This approach may result in undesired physiology driven by decreased SVR, including reflex tachycardia, increased cardiac output (CO), systemic hypotension, and unchanged or increased PVR/SVR ratio. Comparable untoward physiology was recently demonstrated after riociguat therapy in patients with PF and advanced PH with resultant mild hypoxaemia.25 While a patient with PAH may be able to tolerate an aggressive uptitration of parenteral prostanoid,22 this strategy may place a patient with PF and advanced PH at risk of acute cardiopulmonary decompensation.3 Consequently, a more gradual parenteral prostanoid uptitration approach may attenuate shunt physiology and subsequent hypoxaemia, especially if significant systemic vasodilation and the resulting abrupt rise in CO are avoided. Cardiac output may itself be associated with increased intrapulmonary shunt.26 Based on the above, we surmise that a gentler uptitration of parenteral prostanoid, as employed in our study PF population with advanced PH, may lessen the potential for haemodynamic instability and/or hypoxaemia and rather parallel the chronic parenteral prostanoid administration haemodynamic and gas exchange data reported in WHO Group I PAH.
The inclusion of patients restricted to a severe baseline PH phenotype likely decreased the predisposition to arterial oxygen desaturation in response to treprostinil. Our subjects had a markedly elevated PVR and borderline reduced CO at baseline with evidence of significantly improved right heart function following treprostinil infusion, delineated by less septal bowing, a falling right atrial pressure, and improved CO. These salutary effects on right heart function may further optimise arterial oxygen content via enhanced mixed venous oxygen saturation.16 ,27
The improvement of 59 m in 6MWD following 12 weeks of parenteral treprostinil was noted in parallel with improvements in the UCSD SOB questionnaire and the SF-36 MCS, representing preliminary but encouraging findings. Recent independent studies in subjects with idiopathic pulmonary fibrosis (IPF) and Group I PAH suggested the minimally clinically important significant 6MWD difference to be 24–45 m and 25–38 m, respectively.28 ,29 The augmentation in functional capacity seen in our subjects with PF-PH in response to treprostinil does not contravene prior studies reporting a lack of improvement in functional parameters in patients with PF treated with PH-targeted therapies.17–19 Patients in these prior studies had no or mild PH, while our subjects had an average mPAP>45 mm Hg, a markedly elevated PVR, and degrees of RV dilatation and dysfunction comparable to severe WHO Group I PAH.30
These physiological differences are likely critical when considering the potential response to PH-targeted therapies, given that patients with advanced lung disease in the absence of advanced PH typically do not possess evidence of a circulatory limitation to exercise.31 ,32 In contrast, patients with parenchymal lung disease (COPD or PF) and advanced PH demonstrate (in addition to their inherent ventilatory limitation) a circulatory limitation on exertion and an overall cardiopulmonary exercise stress test profile similar to isolated Group I PAH, with blunted oxygen pulse and marked ventilatory inefficiency (ie, increased VE/VCO2).31 ,32 Importantly, the moderate degree of restrictive lung disease in our patient cohort may not have warranted consideration of LT, had it been isolated from the severe extent of superimposed PH. Interestingly, a recent post hoc analysis of a placebo-controlled randomised clinical trial in IPF20 showed that the subgroup of patients with, compared with those without, RV dysfunction and RV hypertrophy improved their 6MWD in response to sildenafil.33 In addition, the Royal Brompton group retrospectively reported a significant 6MWD improvement with sildenafil in a mixed interstitial lung disease population with pulmonary function and right heart haemodynamics similar to our experience.2
The combined observations of improved right heart function and stable arterial oxygen saturation in our PF-PH cohort after chronic parenteral treprostinil suggests the advanced PH phenotype may be critical when considering PH-targeted therapy, as it lends itself towards an increased likelihood of improved circulatory reserve and decreased risk of hypoxaemia. As such, an advanced PH phenotype in the context of chronic respiratory disease may be essential for predicting a beneficial response and minimising potential adverse effects of therapy.
Limitations
Limitations of this study include the heterogeneity of the PF population, variable background PH-targeted therapy, and the absence of ABG testing. The absence of a placebo arm is a particularly significant limitation; therefore, our findings must be confirmed with a randomised, placebo-controlled trial. At this point, the routine use of PH-targeted therapy in PF-PH is not recommended and should only be cautiously considered at specialised PH centres to avoid the serious potential for worsening cardiopulmonary status in this patient population. In addition, the explanation proposed for the lack of significant hypoxaemia with parenteral prostanoid in our PF-PH cohort remains speculative and requires further investigation. To address the limitation of multiple comparisons in the domains of pulmonary function, quality of life, and haemodynamics, we calculated that observed p values < 0.05 corresponded to a maximum q-value of 0.067, indicating that the proportion of significant findings attributable to false discovery is small. As such, we were reassured to see encouraging results in a real-world cohort of patients with PF referred for LT, characterised by an ‘advanced PH and right heart dysfunction’ phenotype. The lack of ABG testing is offset by stable arterial oxygen content, oxygen delivery, and oxygen saturation values at rest and 6MWD testing, following treprostinil therapy.
Conclusion
This open-label study suggests that gradual initiation and chronic administration of parenteral treprostinil therapy may improve haemodynamics and right heart function without compromising systemic oxygenation in an advanced PH phenotype with RV dysfunction in the setting of PF. These findings are only hypothesis generating and require confirmation in a multicentre, randomised study design. Future studies of PH-targeted therapy for PF should focus on patients with PF with the combination of advanced PH and RV dysfunction, as these subjects may have greater capacity for benefit. Finally, given the high mortality inherent to this population, a future study may consider survival as an endpoint.
Acknowledgments
The authors would like to acknowledge Lynne Yoder RN, Bryant Torres BS, Glenna Traiger RN, Eileen Callahan CCRP, and Paul Lopez LVN for their dedicated support with data collection and study coordination as well as NHLBI HL112990 to JAB.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
- Data supplement 2 - Online repository
- Data supplement 3 - Online tables
Footnotes
-
*PRF and RS contributed equally
-
Contributors RS: conceptual design; patient care and procedures; writing of manuscript; data collection. DK: conceptual design; editing of manuscript; statistical support. AV: blinded review of echocardiograms. AD: patient care and procedures; statistical support. PM: statistical support. ED: statistical support. JAB: patient care and procedures. SSW: patient care and procedures. SD: patient care and procedures; data collection. SSS: patient care. JGG: blinded review of chest CT scans. FA: blinded review of chest CT scans. JPLIII: conceptual design; patient care. DJR: patient care. PRF: editing of manuscript; blinded review of echocardiograms. RS: conceptual design; patient care and procedures; writing of manuscript; data collection.
-
Funding NHLBI and United Therapeutics.
-
Competing interests None.
-
Ethics approval Institutional Review Board at University of California, Los Angeles.
-
Provenance and peer review Not commissioned; externally peer reviewed.