Article Text

Abstract
Background Vascular remodelling plays a central role in asthma and chronic obstructive pulmonary disease (COPD). Bradykinin (BK) is a vasoactive proinflammatory peptide mediating acute responses in asthma. We investigated the role of angiogenic factors in relation to BK receptors in asthma and COPD.
Methods Bronchial biopsies from 33 patients with COPD, 24 old (≥50 years) patients with (≥50 years) asthma, 18 old control smokers, 11 old control non-smokers, 15 young (≤40yrs) patients with (≤40 years) asthma and 10 young control non-smokers were immunostained for CD31, vascular endothelial growth factor-A (VEGF-A), angiogenin and BK receptors (B2R and B1R). Fibroblast and endothelial co-localisation of relevant molecules were performed by immunofluorescence. BK-induced VEGF-A and angiogenin release was studied (ELISA) in bronchial fibroblasts from subjects with asthma and COPD.
Results In bronchial lamina propria of old patients with asthma, CD31 and VEGF-A+ cell numbers were higher than old control non-smokers (p<0.05). Angiogenin+, B2R+ and B1R+ cell numbers in old patients with asthma were higher than in old control non-smokers, control smokers and patients with COPD (p<0.01). Angiogenin+ cell numbers were higher in patients with COPD than both old control groups (p<0.05). In all patients with asthma the number of B2R+ cells was positively related to the numbers of B1R+ (rs=0.43), angiogenin+ (rs=0.42) and CD31 cells (rs=0.46) (p<0.01). Angiogenin+ cell numbers were negatively related to forced expiratory volume in 1 s (rs=−0.415, p=0.008). Double immunofluorescence revealed that CD31 cells of capillary vessels coexpressed B2R and that fibroblasts coexpressed B2R, VEGF-A and angiogenin. BK (10−6M) induced significant angiogenin release in fibroblasts from asthma and to a lesser extent in COPD.
Conclusions Unlike COPD, this study suggests the involvement of BK receptors in bronchial vascular remodelling in asthma.
- Asthma Mechanisms
- COPD Pathology
Statistics from Altmetric.com
Key messages
What is the key question?
-
Are bradykinin receptors in relation to vascular remodelling in asthma and chronic obstructive pulmonary disease?
What is the bottom line?
-
Bradykinin receptors are overexpressed in the bronchial wall of old patients with asthma in conjunction with an increased expression and fibroblast-derived release of vascular growth factors.
Why read on?
-
The reader will figure out the bradykinin-associated mechanisms of increased vascularity and of overexpressed vascular growth factors in old asthma.
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are chronic inflammatory and obstructive respiratory diseases associated with structural alterations in the airways.1 Angiogenesis has been recognised as a fundamental event in the development of airway remodelling that leads to irreversible airway obstruction.2 ,3
Several proteins are potentially involved in angiogenesis, like vascular endothelial growth factor-A (VEGF-A), angiogenin and bradykinin (BK). VEGF-A is a potent multifunctional cytokine that has several effects on angiogenesis and is associated with asthma and COPD.2 ,4 VEGF-A stimulates endothelial cell migration and proliferation and it is widely expressed in highly vascularised organs, including the lung.5 VEGF-A is modulated by many factors including nitric oxide and fibroblast growth factor.2 ,6 Some studies have shown elevated levels of VEGF-A in bronchial biopsies, induced sputum and bronchoalveolar lavage fluid (BALF) from patients with asthma, and these correlated with increased total airway vascular area 7–9 and smaller airway calibre.7 ,9 Furthermore, VEGF-A expression is increased in small airways of COPD.2 In addition, all VEGF isoforms showed decreased expression with age in the anterior cruciate ligament of rabbits.10
Angiogenin is a member of the ribonuclease superfamily, normally present in the blood circulation.11 It has been implicated as mitogen for vascular endothelial cells, immune modulator, activator of certain protease cascades, as well as adhesion molecule.11 Like VEGF-A, it induces vascular endothelial cell proliferation, migration and tubule formation,12 and its levels are increased in asthma.7 ,13
BK and the related peptide kallidin are formed from high and low molecular weight kininogen precursors following the activation of plasma and tissue kallikreins by pathophysiological stimuli leading to tissue inflammation and damage.14
The biological actions of kinins are mediated via interaction with B2 receptors (B2R) and B1 receptors (B1R). The B2R is constitutively expressed on most cell types and its activation leads to various intracellular events, including nitric oxide release.15 By contrast, B1Rs can be induced during inflammatory insults.14 BK induces acute inflammatory airway responses, including plasma protein extravasation/vasodilation and smooth muscle contraction,16 leading to bronchoconstriction.14 Increased levels of BK have been reported in BALF from patients with asthma,14 and it upregulates the production of VEGF-A in vitro either in human airway smooth muscle cells17 or in bronchial epithelial cells.18 Despite BK, upon stimulation of its receptors, showed a vasoactive role19 and vascular growth effect,18 no reports have been published describing possible associations between BK and angiogenesis in asthma and COPD. No data are available for BK B1 and B2 receptors expression in the bronchial mucosa of patients with asthma and COPD. We investigated the expression of BK B1 and B2 receptors in bronchial biopsies of patients with asthma and COPD and their association with angiogenic factors and we examined the capability of BK to release VEGF-A or angiogenin from asthmatic and COPD bronchial fibroblasts.
Methods
Study design
This cross-sectional study has been primarily designed in order to compare COPD (≥50 years old), asthma and control groups comparable for age. Since an age-dependent expression of VEGF isoforms and receptors in rabbits has been demonstrated,10 we decided to also include in the present study young patients with asthma (YA) and young controls (≤40 years old) in order to evaluate potential differences related to age.
Subjects
We examined bronchial biopsies from 111 subjects by immunohistochemistry (IHC) and confocal analysis: 24 non-smoking (2 ex-smokers) old patients with asthma (OA; age≥50 years); 15 non-smoking young patients with asthma (YA; age≤40 years); 33 smoking (9 ex-smokers) patients with COPD (age≥50 years), 18 old control smokers (2 ex-smokers) (OCS; age≥50 years), 11 old control non-smokers (OCNS; age≥50 years) and 10 young control non-smokers (YCNS; age≤40 years) (table 1). Patients with asthma and the severity of asthma were identified and treated according to the Global Initiative for Asthma and American Thoracic Society criteria.20 ,21 Patients with COPD were staged and treated using Global Initiative for Chronic Obstructive Lung Diseases criteria.22 All control subjects had no history of respiratory disease and no airflow limitation. The clinical and demographic characteristics of all the subjects are shown in table 1. All subjects were in stable condition (see also online supplementary material). The study conformed to the Declaration of Helsinki, was approved by the local ethics committees (A.O.U. San Luigi Hospital: n. of protocol 1759, 22 January 2008; S. Maugeri Foundation: n. of protocol p81, 20 May 2009), bronchial biopsies were performed according to the local Ethics Committee Guidelines and written informed consent was obtained from each subject.
Subjects’ characteristics
Measurements of lung function, fibre-optic bronchoscopy, IHC, immunofluorescence and confocal microscopy, scoring system for IHC, primary cultures of bronchial fibroblasts, and ELISA tests for in vitro angiogenic factor release are described in online supplementary material.
Data analysis
Group data were expressed as mean±SD for lung functional data or median (range) and IQR for morphological data. We assumed a normal distribution for functional data (ie, forced expiratory volume in 1 s (FEV1), forced vital capacity, age, etc) and a non-normal distribution for morphological parameters. For this reason we applied the analysis of variance in comparing subgroups of patients and control subjects for functional data. The non-parametric Kruskal-Wallis test was applied for multiple comparisons when morphological data were analysed followed by the Mann-Whitney U test for comparison between groups. The correlation coefficient between functional-morphological data was calculated using the Spearman rank method. Data from in vitro experiments are expressed as mean±SEM of three independent experiments (each experiment was performed in duplicate) for each fibroblast culture. Differences between two groups were compared by using unpaired t tests. Probability values of p<0.05 were considered statistically significant. Data analysis was performed by using the Graph Pad Prism program (GraphPad V.5.00 Software Inc, San Diego, California, USA).
Results
Clinical findings
Subjects’ characteristics are shown in table 1. See also online supplementary material.
Inflammatory cells
Quantification of inflammatory cells in bronchial biopsies is summarised in table 2. Data are reported in online supplementary material. IHC of all the inflammatory cells from OA is shown in online supplementary figure E1.
Quantification of inflammatory cells in the lamina propria of patients with COPD, asthma, control smokers and control non-smoking subjects
Immunoreactivity of VEGF-A, CD31 and angiogenin
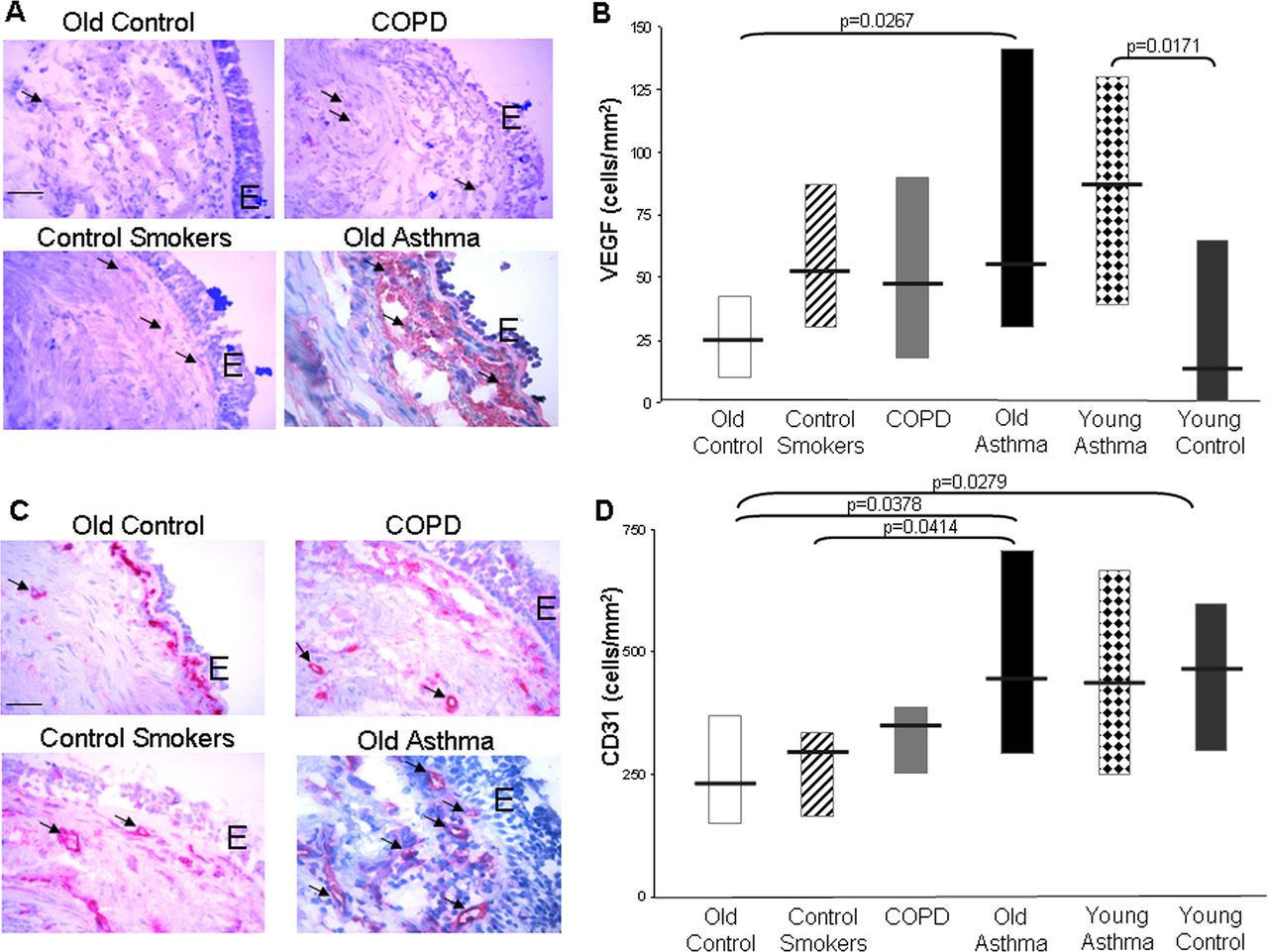
VEGF-A was mainly present in fibroblasts of lamina propria and in epithelial cells (figure 1A). Cells expressing VEGF-A immunoreactivity were significantly higher in lamina propria of OA than OCNS (p=0.0267) but not higher than other groups (figure 1B). VEGF-A expression was significantly higher in YA than in YCNS (p=0.0171) (figure 1B). In OA (p=0.0103), and also in patients with asthma as a whole (p=0.0269), non-atopic subjects showed increased expression of VEGF-A in lamina propria compared with atopic subjects. Furthermore, COPD as well as OCS had higher numbers of VEGF-A+ cells compared with OCNS without reaching statistical significance (figure 1B). CD31 was present in endothelial cells of lamina propria (figure 1C). The number of CD31 cells was significantly increased in OA compared with OCNS (p=0.0378) and OCS (p=0.0414) but it did not significantly differ with COPD (figure 1D). A significant increase of CD31 cells was observed in YCNS compared with OCNS (p=0.0279).

Vascular endothelial growth factor-A (VEGF-A) (A and B) and CD31 (C and D) expression in bronchial biopsy specimens obtained from old control non-smokers, healthy smokers, patients with chronic obstructive pulmonary disease (COPD), old and young patients with asthma, young control non-smokers. (A and C) Photomicrographs showing the bronchial immunostaining for VEGF-A and CD31, respectively, are representative of those from 11 old control non-smokers, 18 healthy smokers, 33 patients with COPD and 24 old patients with asthma. Original magnification 400×. Internal scale: 25 μm. E, epithelium. (B and D) Number of VEGF-A+ and CD31 cells/mm2 of bronchial lamina propria from old control non-smokers, healthy smokers, patients with COPD, old and young patients with asthma, young control non-smokers. Each bar indicates the median value in the respective groups and boxes represent lower and upper quartiles. The comparisons are made on the basis of age (old groups or young groups) and between asthma or control groups. Access the article online to view this figure in colour.
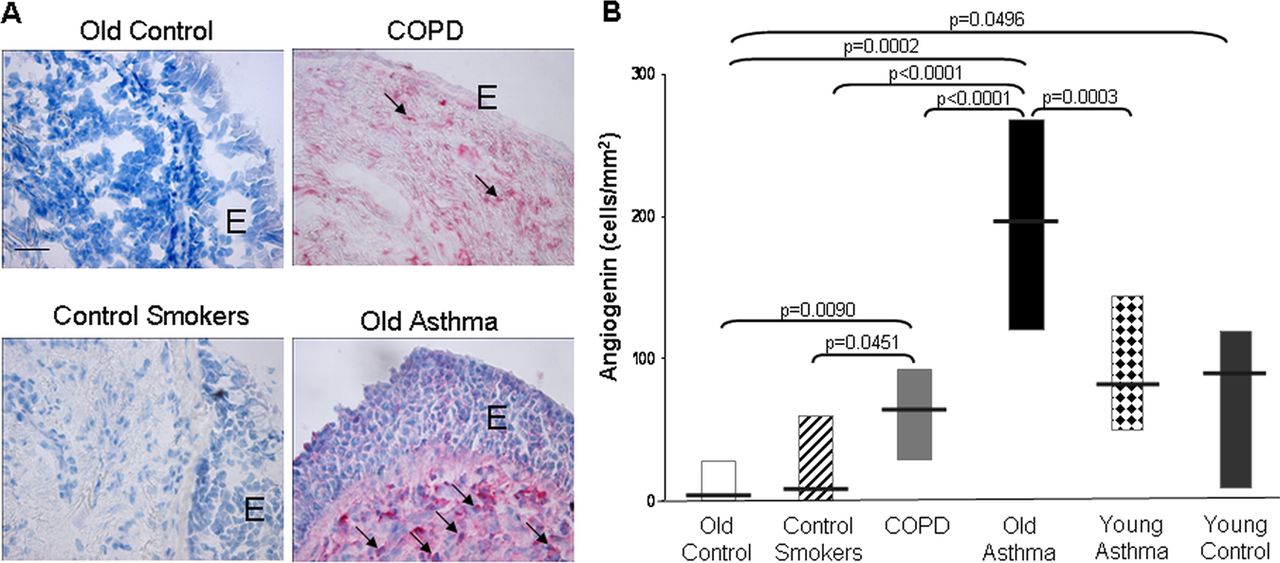
Immunostaining for angiogenin was localised in endothelial cells and fibroblasts of lamina propria and, to a lesser extent, in epithelial cells (figure 2A). The number of angiogenin+ cells was significantly higher in OA compared with OCNS (p=0.0002), OCS (p<0.0001) and COPD (p<0.0001) (figure 2B). Similarly, the number of angiogenin+ cells were also significantly elevated in patients with COPD compared with OCNS (p=0.0090) and OCS (p=0.0451) (figure 2B). Furthermore, angiogenin expression in lamina propria of OA was significantly higher than in YA (p=0.0003) (figure 2B). Finally, angiogenin+ cells were significantly lower in lamina propria of OCNS compared with YCNS (p=0.0496) (table 2). Data are reported in online supplementary material.
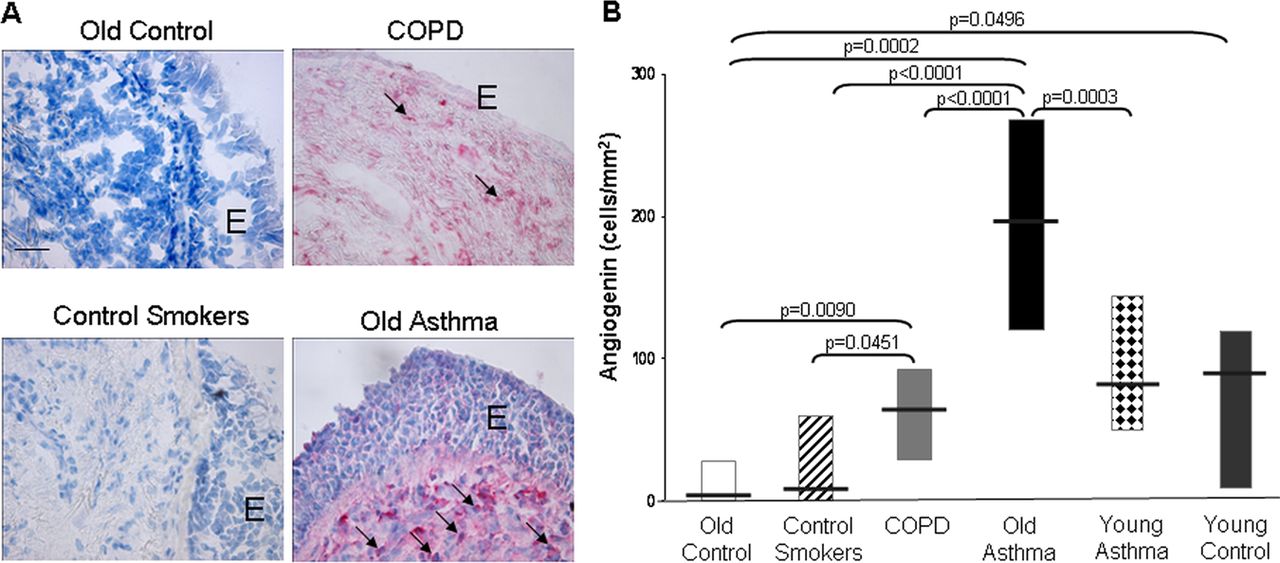
Angiogenin expression in bronchial biopsy specimens obtained from old control non-smokers, healthy smokers, patients with chronic obstructive pulmonary disease (COPD), old and young patients with asthma, young control non-smokers. (A) Photomicrographs showing the bronchial immunostaining for angiogenin are representative of those from 11 old control non-smokers, 18 healthy smokers, 33 patients with COPD and 24 old patients with asthma. Original magnification 400×. Internal scale: 25 μm. E, epithelium. (B) Number of angiogenin+ cells/mm2 of bronchial lamina propria from old control non-smokers, healthy smokers, patients with COPD, old and young patients with asthma, young control non-smokers. Each bar indicates the median value in the respective groups and boxes represent lower and upper quartiles. The comparisons are made on the basis of age (old groups or young groups) and between asthma or control groups. Access the article online to view this figure in colour.
Immunoreactivity of BK B2R and B1R
B2R was mainly present in fibroblasts within the lamina propria, in epithelial cells and in endothelial cells of capillary vessels (figure 3A). Cells expressing B2R immunoreactivity were significantly higher in lamina propria of OA compared with OCNS (p=0.0004), OCS (p<0.0001) and COPD (p<0.0001) (figure 3B). Similarly, immunostaining for B1R was localised in fibroblasts within the lamina propria and in endothelial cells and epithelial cells (figure 3C). Quantitative analysis showed significantly greater B1R expression in OA compared with OCNS (p=0.0014), OCS (p<0.0001) and COPD (p<0.0001) (figure 3D), as well as in comparison with YA (p=0.0160) (figure 3D). No significant differences were observed in the numbers of cells expressing B2R or B1R between any other groups studied (figure 3B,D). Data are reported in online supplementary material.

Bradykinin B2 receptor (B2R) (A and B) and bradykinin B1 receptor (B1R) (C and D) expression in bronchial biopsy specimens obtained from old control non-smokers, healthy smokers, patients with chronic obstructive pulmonary disease (COPD), old and young patients with asthma, young control non-smokers. (A and C) Photomicrographs showing the bronchial immunostaining for B2R and B1R, respectively, are representative of those from 11 old non-smokers, 18 healthy smokers, 33 patients with COPD and 24 old patients with asthma. Original magnification 400×. Internal scale: 25 μm. E=epithelium. (B and D) Number of B2R+ and B1R+ cells/mm2 of bronchial lamina propria from old control non-smokers, healthy smokers, patients with COPD, old and young patients with asthma, young control non-smokers. Each bar indicates the median value in the respective groups and boxes represent lower and upper quartiles. The comparisons are made on the basis of age (old groups or young groups) and between asthma or control groups. Access the article online to view this figure in colour.
Inflammatory cells, angiogenic factors, B2R and B1R expression in severe versus mild asthma
We also investigated the differences in inflammatory cells, angiogenic markers and BK receptors expression in the groups of severe (n=16) and mild (n=23) asthma (irrespective of age). Data are reported in online supplementary material (see also online supplementary figure E2A).
Angiogenin+ cells (see online supplementary figure E2B) were significantly increased in the patients with severe asthma compared with the patients with mild asthma (p=0.019), whereas no difference was found in the number of VEGF-A+ cells, CD31 cells, B2R+ cells and B1R+ cells (data not shown).
Correlations between angiogenic markers, BK receptors, inflammatory cells and clinical parameters
In the whole asthma group, the number of angiogenin+ cells was negatively related to FEV1 (rs=−0.415, p=0.008, figure 4A) and positively related to the number of B2R+ cells in lamina propria (rs=0.417, p=0.008, figure 4B). Moreover, the number of B2R+ cells in lamina propria was significantly related to the number of B1R immunoreactive cells (rs=0.432, p=0.0060, figure 4C) as well as the number of CD31 cells (rs=0.465, p=0.004, figure 4D). In all patients with asthma, the number of neutrophils was positively related to CD31 cells (rs=0.47, p=0.02), to angiogenin+ cells (rs=0.34, p=0.04) and to B2R+ cells in the lamina propria (rs=0.44, p=0.007).

Relationship between angiogenin positive cells and forced expiratory volume in 1 s (FEV1) (% predicted) levels (A) or the number of B2R+ cells (B) in the bronchial lamina propria of all patients with asthma. In (C–D) the correlation between B2R+ cells number and B1R immunoreactive cells (C) or the number of CD31 cells (D) in the bronchial lamina propria of all patients with asthma are shown. The correlation coefficient was obtained using the Spearman rank method (rs).
No other statistically significant correlations were found between angiogenic markers, BK receptors, inflammatory cells or any clinical parameters.
Immunofluorescence with confocal microscopy double staining for localisation of BK B2 receptor in CD31 cells
Double immunofluorescence staining of B2R with CD31 was performed using laser-scanning confocal microscopy. Endothelial cells of capillary vessels in lamina propria of OA were immunoreactive for CD31 (figure 5A). Epithelial cells and endothelial cells of capillary vessels in lamina propria were immunoreactive for B2R (figure 5B). Merging of the red (B2R) and green (CD31) images revealed that CD31 cells of capillary vessels coexpressed B2R (figure 5C).

Representative photomicrographs obtained by confocal microscopy after immunofluorescence staining of CD31 and bradykinin B2 receptor (B2R) in bronchial lamina propria from an old patient with asthma. In (A) Alexa Fluor 488-green staining represents CD31, in (B) Alexa Fluor 647-red staining represents B2R whereas co-localised pixels are displayed in yellow (C). Arrows indicate B2R and B2R/CD31 positive cells (B and C, respectively). Original magnification: 630×. E, epithelium; LP, lamina propria; V, vessel. Access the article online to view this figure in colour.
Immunofluorescence with confocal microscopy double staining for identification of 5B5 cells coexpressing BK B2 receptor and angiogenic growth factors
Double immunofluorescence staining of B2R, VEGF-A or angiogenin with 5B5 (marker for fibroblast) was performed using laser-scanning confocal microscopy. The large majority of cells in lamina propria of OA was immunoreactive for 5B5 (figure 6A,E,I). Merging of the red (B2R, VEGF-A or angiogenin) and green (5B5) images revealed that 5B5+ cells in lamina propria coexpressed B2R (C), VEGF-A (G) or angiogenin (M). Co-localisation quantitative analysis (figure 6D,H,N) confirmed 5B5 and B2R (72±12%) coexpression as well as 5B5 and VEGF-A (87±2%) or angiogenin (80.5±3.5) co-localisation in lamina propria of OA.

Representative photomicrographs obtained by confocal microscopy after immunofluorescence staining of prolyl 4-hydroxylase (5B5), bradykinin B2 receptor (B2R), vascular endothelial growth factor-A (VEGF-A) and angiogenin expression in bronchial lamina propria from an old patient with asthma. (A, E and I) show, the Alexa Fluor 488-tagged anti-5B5 (green) whereas (B, F and L) represent Alexa Fluor 647-tagged anti-B2R, anti-VEGF-A or antiangiogenin (red) respectively. In (C, G and M) the co-localised pixels representing coexpression of 5B5 and B2R (C), VEGF-A (G) or angiogenin (M) are displayed in yellow. (D, H and N) show the correlation cytofluorogram of the images in (A and B, or E and F or I and L), respectively. Original magnification 630×. Access the article online to view this figure in colour.
BK-induced VEGF-A and angiogenin release by HBF in vitro
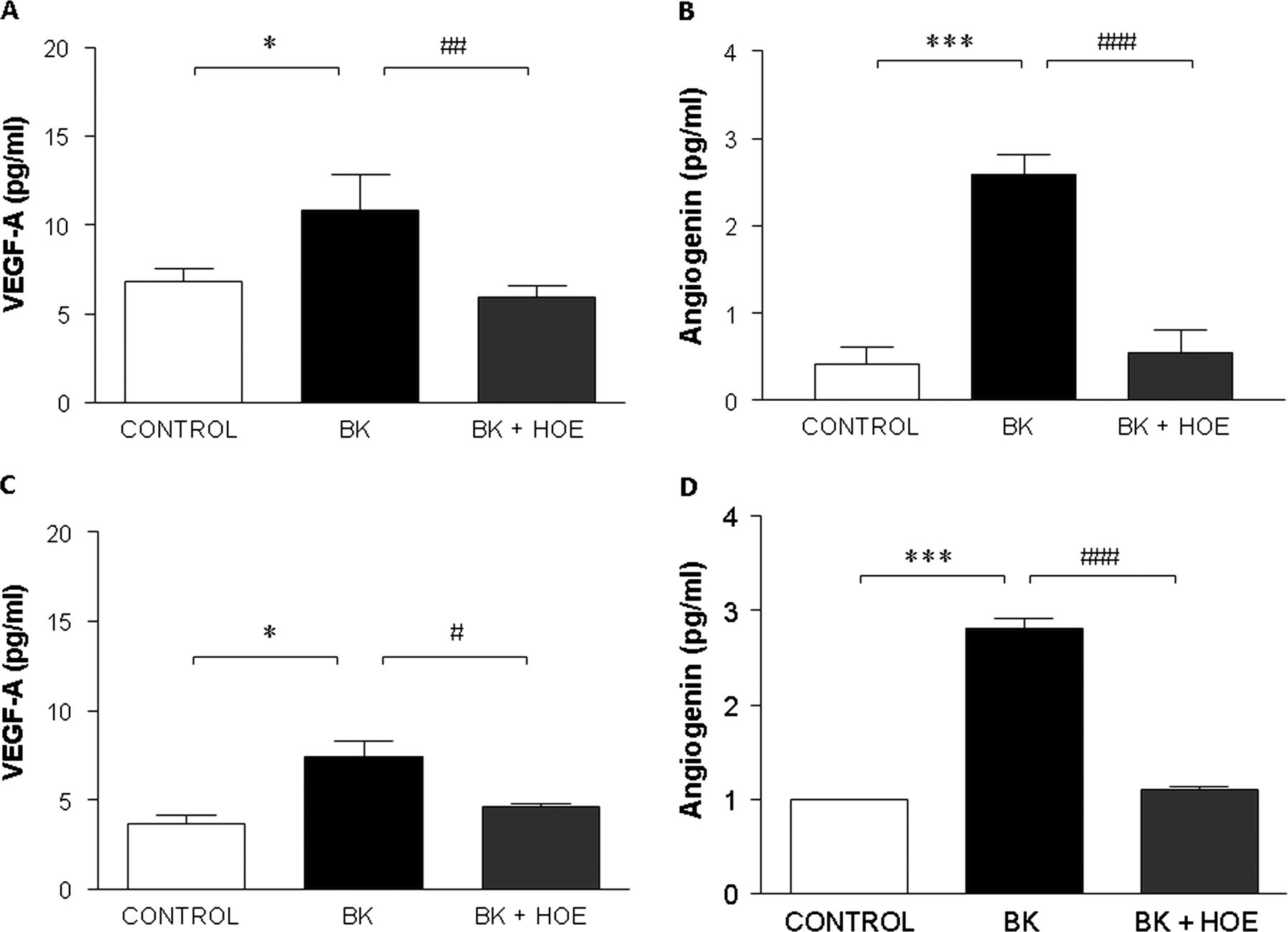
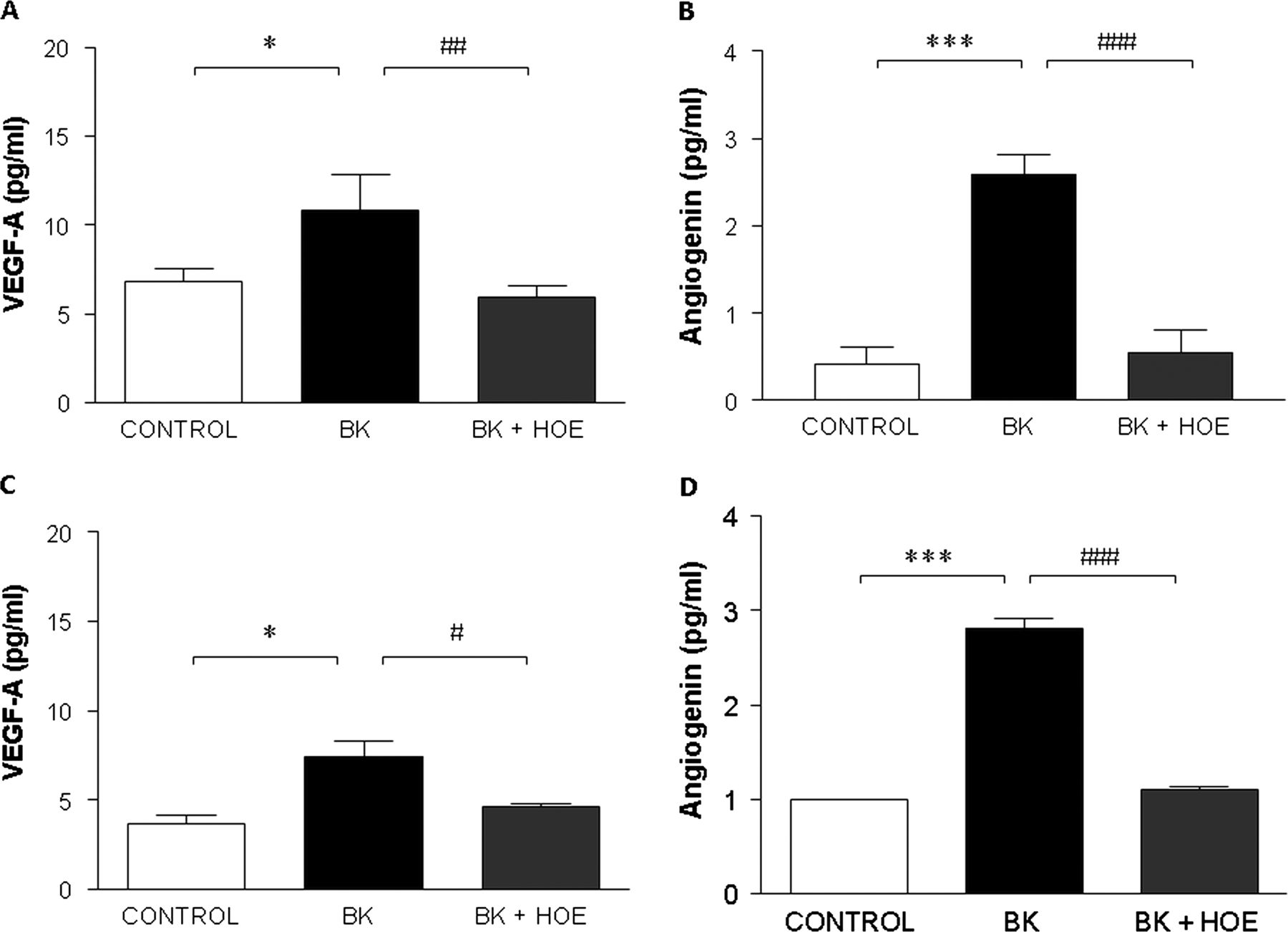
Unstimulated human bronchial fibroblasts (HBF) from OA (n=3) and COPD (n=3) release VEGF-A and angiogenin (figure 7). Incubation with BK (10−6M) induced a significant increase in VEGF-A (figure 7A: p=0.0248; figure 7C: p=0.016) and angiogenin release (figure 7B: p<0.0001; figure 7D: p<0.0001) in HBF from patients with asthma and COPD, respectively. BK (1 h exposure) similarly increased VEGF-A levels in HBF from patients with asthma (160±25%) and COPD (208±34%; p>0.05), while BK elevated angiogenin levels differently in asthma fibroblasts (669±111%) compared with COPD fibroblasts (280±10%; p=0.013). Details of these experiments are reported in online supplementary material.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of bradykinin (BK) B2 receptor antagonist HOE140 on BK-induced vascular endothelial growth factor-A (VEGF-A) release (A and C) and angiogenin release (B and D) by human bronchial fibroblasts from patients with asthma (n=3; A and B) and from chronic obstructive pulmonary disease (n=3; C and D). Cells were pretreated with or without HOE140 (1 μM) for 30 min before incubation with BK (10−6M) for 1 h. At the end of the incubation period, the culture supernatants were collected and the VEGF-A or angiogenin contents were evaluated by ELISA. Data are presented as mean±SEM of three independent experiments for each fibroblast culture. *p<0.05, ***p<0.001 versus unstimulated cells; and #p<0.05, ## p<0.01, ###p<0.001 versus cells stimulated with BK.
Discussion
This study demonstrates that BK receptors (B2R and B1R) are upregulated in the lamina propria of OA compared with age-comparable healthy control subjects and COPD in conjunction with increased number of vessels (CD31 cells) and expression of angiogenin and, to a lesser extent, VEGF-A. Furthermore, angiogenin expression was significantly increased in patients with severe compared with mild asthma. Angiogenin was also negatively related to FEV1 in all patients with asthma and positively related to B2R expression. Finally, we showed localisation of B2R, VEGF-A and angiogenin in bronchial fibroblasts from OA and the ability of BK to release VEGF-A and angiogenin in bronchial fibroblasts from patients with asthma and, to a lesser extent, from patients with COPD.
Asthma and COPD are chronic inflammatory diseases of the lung associated with structural remodelling that contributes to airway obstruction (see also online supplementary material). We found significant and positive correlations between numbers of neutrophils and B2R+, CD31 or angiogenin+ cells suggesting a role for this inflammatory cell in vascular remodelling of OA. In a previous study BK-induced interleukin 8 production due to B2R stimulation in lung fibroblasts is in part dependent on the activation of ERK1/2 and p38 MAPK-pathway.23 These data, together with our report on positive correlations between neutrophils and angiogenic molecules suggest a role for neutrophil-released mediators (including proteases) in modulating angiogenesis in asthma through activation of protease activated receptors.24
Vascular remodelling and reactivity of the airways including angiogenesis, vasodilation and microvascular leakage are the most prominent and uniform findings in asthma.2 Furthermore, bronchial vascular changes may also occur in COPD, particularly in the small airways.2 ,25 Microvascular changes in asthma and COPD may contribute to an increase in airway wall thickness which may be associated with severity of airway obstruction and disease progression.25 Angiogenesis is a complex multiphase process involving a great number of growth factors, cytokines, chemokines and other factors. Some bronchial biopsy studies7 ,8 as well as induced sputum studies9 observed higher VEGF-A levels, related to vascularity, in asthmatic airways than those of healthy controls.7 ,8 Angiogenin induces vascular endothelial cell proliferation, migration and tubule formation. In biopsies from patients with asthma, a higher expression of basic fibroblast growth factor and angiogenin was reported, with significant correlations between the vascular area and the number of angiogenic factor-positive cells within the airways.7 Furthermore, VEGF-A and angiogenin are able to promote in vitro angiogenesis expressed as induction of primitive vascular tubule structures in culture with BALF collected from patients with mild asthma.13 A recent study also showed increased levels of VEGF-A and angiogenin in induced sputum from stable COPD compared with healthy smokers and non-smokers.26 We extend these observations by comparing patients with asthma, COPD and controls in relation to age. This is the first study in humans showing that the number of CD31 and angiogenin+ cells was significantly reduced in old compared with young controls demonstrating that vascularity is probably influenced by age per se. VEGF-A appears to be more expressed in lamina propria of OA while angiogenin is significantly higher in OA (also in comparison with YA) and in COPD. Furthermore, angiogenin+ cell expression in lamina propria negatively correlated with the level of FEV1 in the group of patients with asthma, suggesting that angiogenin expression in lamina propria is associated with the severity of asthma, confirming previous findings.25 The modest increase of angiogenin in the bronchi of our COPD may be related to apoptosis of endothelial cells induced by VEGF-A reduction due to oxidative stress as described elsewhere.27 Finally, we showed for the first time a marked increase of VEGF-A expression in the lamina propria of non-atopic patients with asthma compared with atopic patients with asthma suggesting that in ‘intrinsic’ asthma higher release of VEGF-A could specifically contribute to the formation of vascular remodelling scenario.
BK exerts several effects in airways through direct and indirect pathways which are mediated by activation of two main BK receptor subtypes, B1 and B2, that differ in expression and ligand specificity. In tissues B1 receptors are inducible, whereas B2 receptors are constitutively expressed.14 The distribution of B2 receptors has been mapped out in human and guinea pig lung by autoradiography with [3H] BK.28 See also online supplementary material. In this study, for the first time we demonstrated the expression of BK B1R and B2R in fibroblasts, epithelial cells and endothelial cells of the human bronchial lamina propria (by IHC and immunofluorescence analysis), and that their total expression is significantly increased in OA compared with OCNS, OCS and COPD (and for B1R also compared with YA), suggesting a potential role for these receptors in the vascular remodelling of old asthma. BK promotes angiogenesis by upregulation of basic fibroblast growth factor through the B1 receptor or by stimulation of VEGF-A formation following B2 receptor stimulation.17 ,29 In our study, B2R showed a positive correlation with B1R and with CD31 endothelial cells and angiogenin suggesting that B2R may promote angiogenesis leading to blood vessel neoformation. We also found by immunofluorescence that the large majority of bronchial fibroblasts in OA coexpressed B2R, angiogenin and VEGF-A indicating a major role for fibroblasts in producing vascular growth factors potentially released upon stimulation of BK B2R.
BK is involved in the repair processes inducing fibroblast proliferation and differentiation.30 BK also regulates angiogenic growth factors expression (angiogenin and VEGF-A) in human dental pulp fibroblasts.31 Other authors showed that human airway smooth muscle cells secrete VEGF-A and this secretion is induced by BK via B2R.17 In our in vitro study, we demonstrated for the first time that BK induced VEGF-A and angiogenin release in primary cultures of HBF from patients with asthma and that this effect is mediated by B2R, as confirmed by the use of the B2R antagonist HOE140 which completely blocked BK-induced VEGF-A and angiogenin release. We also showed similar effects, but to a lesser extent, in bronchial fibroblasts from COPD suggesting that bronchial fibroblasts from patients with asthma are more prone to release angiogenic factors.
In conclusion, this study demonstrates an increased expression of BK receptors in relation to vascular remodelling in asthma and suggests a role for bronchial asthmatic fibroblasts in releasing vascular growth factors upon activation of BK B2 receptors. Our study showed that markers of vascular remodelling are major features of OA and are potentially involved in fixed airway obstruction by increasing airway wall thickness and stiffness. The increased vascular reactivity of asthmatic airways, due to stimuli like BK,32 in disease-related vascular remodelling might participate in airway variability which is a typical pattern of airway patency in asthma. Previous observations showed kinin involvement in airway hyperresponsiveness in asthma,33 and the capability of selective B2R antagonists to treat acute attacks of hereditary angioedema,34 and to improve pulmonary function in patients with asthma.35 These data, combined, lead us to encourage the planning of long term studies using these selective antagonists in asthma treatment in order to inhibit BK B2 receptor-mediated angiogenic effects and its related remodelling processes.
Acknowledgments
The authors thank Dr Gian Mario Massaglia for his contribution in collecting bronchial biopsies.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All authors included in this paper fulfil the criteria of authorship. In addition we assure that there is no one else who fulfils the criteria that has not been included as an author.
-
Funding This study was supported by MIUR ex-60% 2008.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study conformed to the Declaration of Helsinki. Ethics consent was obtained, bronchial biopsies were performed according to the local ethics committee guidelines.
-
Provenance and peer review Not commissioned; externally peer reviewed.