Article Text

Abstract
Introduction The rising disease burden from chronic obstructive pulmonary disease (COPD) requires new approaches.
Method We suggest an approach based around three elements: inflammometry and multidimensional assessment to identify therapeutic targets and case management to design and implement an individualised treatment programme based on these assessments.
Discussion This tailored approach to treatment would maximise efficacy, limit cost and permit a better risk–benefit ratio of treatment. The advantages include the ability to add up the benefits of individual therapies leading to a cumulative therapeutic benefit that is greater than each individual therapy alone. We can now design a multifaceted inflammometry intervention for airway diseases based on targeting eosinophilic inflammation, non-eosinophilic pathways and systemic inflammation. COPD is a complex and challenging disease. The use of inflammometry and multidimensional assessment is necessary to identify relevant treatment targets and maximise the scope of therapy while limiting unnecessary use of drugs. An individualised programme of management can be designed and coordinated by using a case manager. This new approach may provide tangible benefits to people with COPD.
- COPD Pharmacology
- Systemic disease and lungs
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a high impact disease,1 with a global trajectory that predicts an alarming increase in illness burden.2 Current approaches are unlikely to be sufficient to address this problem since they are largely based around disease management concepts that have been available for several years, at a time when the global COPD burden is escalating. New approaches are required and we suggest an approach that is based around three elements: the use of inflammometry and multidimensional assessment to identify therapeutic targets, and case management to design and implement an individualised treatment programme based on these assessments.3 Some see this as self-evident (common sense), whereas others see it as idealistic (respiratory utopia). We maintain it is both of these things, and more, since it offers a pragmatic and achievable approach to a complex condition, with the prospect of major health gains.
At the core of this approach is recognition of the heterogeneity in COPD. There is now considerable editorial space devoted to this subject.3–6 But do we actually apply this knowledge to the management of COPD?
Improvement in health status and avoidance of exacerbations are the key goals of management7 and it is now time to consider the heterogeneity of this disease in terms of treatment approaches. The current method is to apply a blanket approach to pharmaco-therapy that is informed by disease severity. The recently revised Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy suggests a graded approach to managing COPD, which involves short-acting bronchodilators and active reduction of risk factors (smoking cessation and vaccinations) across all COPD severity classifications.7 Pharmacotherapies including inhaled corticosteroids, long acting β agonists (LABAs), long-acting antimuscarinics (LAMAs), theophylline and phosphodiesterase-4 inhibitors (PDE4) are recommended as severity, exacerbation frequency and symptoms increase.7 Newer therapeutic choices that target the inflammatory processes in COPD show great promise and their evidence base is increasing. These agents include macrolides as antibiotic/immunomodulatory agents8–10 and 3-hydroxy-3-methyl coenzyme A reductase inhibitors (statins) for systemic inflammation.11 However, because of the heterogeneity of COPD, the positioning of these agents in COPD pharmacotherapy is unclear. The currently recommended anti-inflammatory treatment (inhaled corticosteroid) does not improve systemic inflammation,12 may worsen neutrophilic airway inflammation13 and when applied generally in COPD has a worrying pneumonia risk.14 Recent and ongoing studies (http://www.clinicaltrials.gov) of anti-inflammatories in COPD apply single agents generally to all patients with COPD. This approach fails to recognise the heterogeneity of inflammation in this disease and results in a therapeutic paradox, when key pathophysiological processes can escape therapeutic intervention.
This raises the question of whether a tailored approach to treatment would maximise efficacy, limit cost and permit a better risk–benefit ratio. With this approach the benefits of individual therapies are each added together to bring a cumulative therapeutic benefit. Such multifactorial intervention is common with non-pharmacological therapies, such as pulmonary rehabilitation and asthma self-management education. Together with multidimensional assessment, it is also used successfully in other chronic diseases. The core elements of this approach are inflammometry (table 1), multidimensional assessment3 and case management. This article reports the concept, design and pilot testing of this approach.
Inflammation-based algorithm
Real world example of airway inflammometry case management
Older adults (>55 years) with stable COPD (defined in online supplement) were recruited and allocated to usual care (n=19) or multidimensional assessment and management (n=17). The intervention consisted of individualised management based on the baseline multidimensional assessment. A personalised care plan was developed by the study physician and case manager. The clinicians and participants agreed on the tailored interventions for each of the identified problems.15 An inflammometry algorithm (table 1) was used to inform treatment decisions for airway inflammation, systemic inflammation and mucus hypersecretion. Other tailored interventions were standardised according to the best available evidence.3 The case manager coordinated the plan. The interventions were delivered over 3 months during individualised visits (see online supplement table 1). Pulmonary rehabilitation participation occurred concurrently.
The participant characteristics are presented in table 2. The baseline multidimensional assessment identified a mean (95% CI) of 10.5 (9.7 to 11.2) clinical management problems per participant. These problems clustered into four domains: airway related problems, comorbidity, risk factors and behavioural issues.3
Baseline participant characteristics
The primary outcome of health status improved significantly from baseline to 3-month follow-up in the intervention group. The mean (95% CI) difference in St George's Respiratory Questionnaire (SGRQ) for multidimensional assessment, airway inflammometry and individualised management (MDAIM) was 14 (20.7 to 8.5) versus 3.5 (−3.8 to 10.8); p=0.0003 for control (figure 1A). The mean (95% CI) SGRQ score post intervention for MDAIM was 42.8 (35.3 to 50.4) versus 52 (45.1 to 58.9); p=0.06 for control.
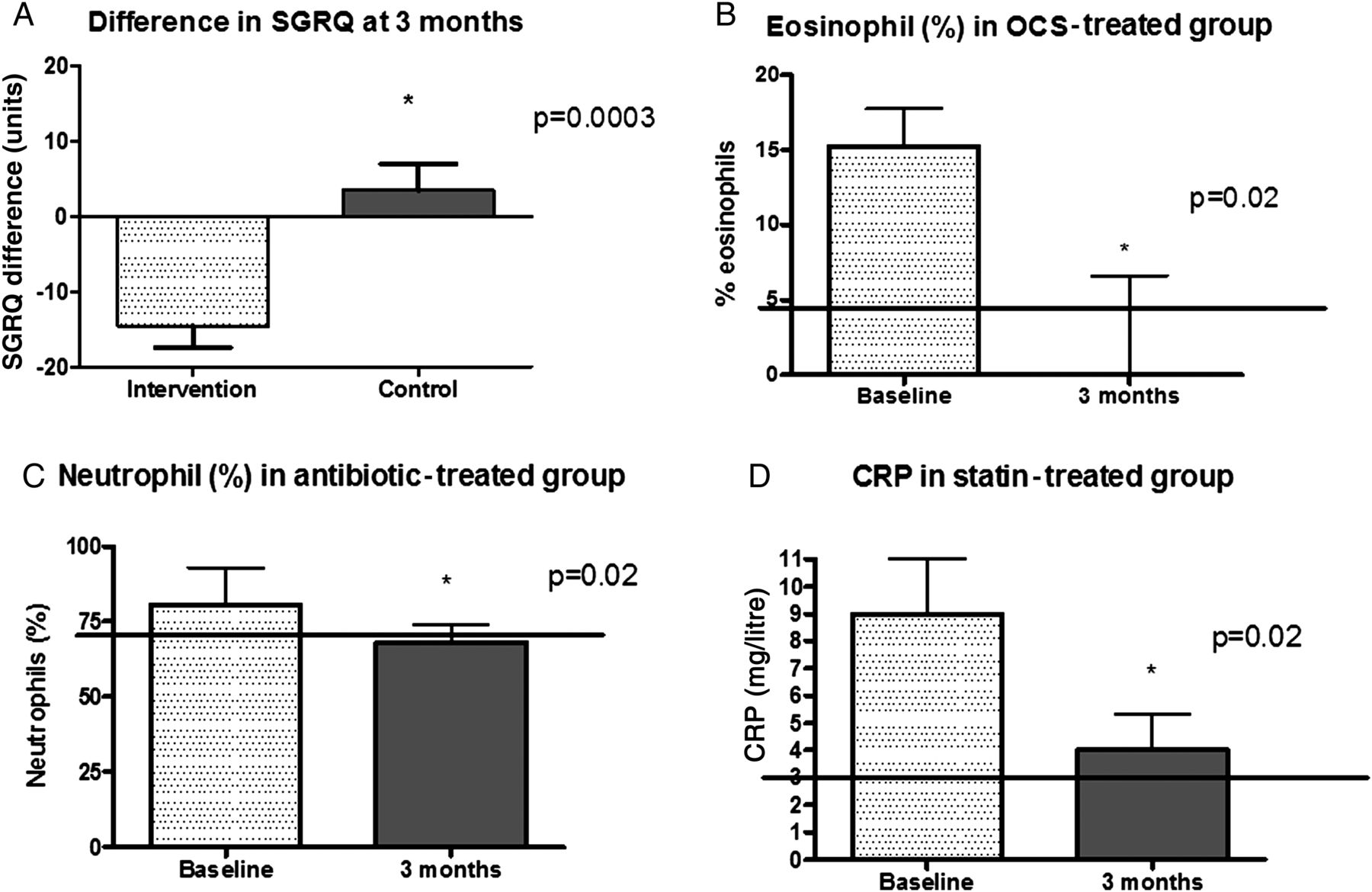
Biomarkers of inflammation in the group receiving treatment tailored to inflammation using the inflammation treatment algorithm. (A) Health status measured by St George's Respiratory Questionnaire (SGRQ) improved significantly (lower score) in the intervention group and worsened in the control group, as measured at 3 months. (B) In the group within multidimensional assessment, airway inflammometry and individualised management (MDAIM) that received oral corticosteroids (OCS) sputum eosinophils (%) had normalised post intervention. The solid line represents the upper limit of normal for sputum eosinophils. (C) In the group within MDAIM that received antibiotics as anti-inflammatory agents sputum neutrophils (%) had normalised post intervention. The solid line represents the upper limit of normal for sputum neutrophils. (D) In the group within MDAIM that received statins for systemic inflammation there was a statically significant reduction in serum high-sensitivity C-reactive protein (hs-CRP). The solid line represents the upper limit of normal of hs-CRP.
Clinically significant quality of life improvement (decreased SGRQ score > 4 units at 3 months) was achieved in 14 (82.3%) participants in the MDAIM group and 5 (31.2%) in the control group (p=0.003). The number needed to treat in order for one person to achieve a clinically significant change in SGRQ was 2.
In the MDAIM group health status continued to improve at 6-months follow-up (mean (95% CI) decrease of 17.1 (7.1 to 27.1) units, p=0.002)) and was maintained at 12 months with a 13.5 (4.7 to 22.3) unit decrease from baseline (p=0.005). In the control group there was no statistically significant difference at either 6 months (4. 5 (−1.2 to 10.3); p=0.1) or 12 months (3.1 (−3.5 to 9.7); p=0.3).
Targeted inflammation-based management reduced eosinophilic and neutrophilic airway inflammation and systemic inflammation (figure 1B–D).
Discussion
Airway and systemic inflammation in COPD is heterogeneous and since any one person can exhibit more than one inflammatory process (figure 2), any individual may require more than one therapeutic approach. For example, targeting neutrophilic inflammation alone will treat 57% of people with COPD (figure 2).16 Targeting eosinophilic inflammation will treat a further 34% and targeting systemic inflammation will manage this problem in 59% of the COPD group. Drug therapy is increasingly pathway specific, and to target all of these different pathways in all people with COPD would require three drugs, that is, macrolide, statin and corticosteroid. A less costly and potentially safer approach is to use individual assessment and multicomponent therapy. We have developed a multifaceted approach that is likely to be highly effective and may be safer.3 ,17 The additive effects of targeted anti-inflammatory treatment to eosinophilic, neutrophilic and systemic inflammation should show at least cumulative benefits, and result in a greater proportion of the COPD population receiving effective anti-inflammatory therapy. We recognise that anti-inflammatory treatment in COPD needs to balance the nature of inflammation, treatment efficacy and the potential for adverse effects. For example, the broad application of macrolides is effective 8 but there is a concern about side effects and microbial resistance. Consequently, an individually targeted approach may be a better way to maximise efficacy and minimise side effects.

{kind=link}
{kind=link}
Venn diagram showing the prevalence of different inflammatory processes in chronic obstructive pulmonary disease. This figure is only reproduced in colour in the online version.
Inflammometry
Current evidence can now be used to design a multifaceted inflammometry intervention for airway diseases. High-quality evidence reports the superior effects of targeting airway eosinophilic inflammation in asthma and COPD,9 ,18–23 with a 50% reduction in exacerbations. Non-eosinophilic inflammatory pathways are addressed using macrolide antibiotics as immunomodulatory agents and studies demonstrate reductions in exacerbations, improved lung function and improved health status.8 ,9 Systemic inflammation represents a further pathway that could be identified by inflammometry and targeted by statins. In COPD an increasing number of observational studies report the positive effects of statins, including a reduced number of COPD exacerbations,24–26 reduced lung function decline,25 improved exercise capacity27 and reduced mortality.11 ,26 ,28 ,29 These published studies have targeted specific inflammatory processes in isolation, and while they show efficacy, to date there are no other published studies other than these pilot data that treat the overlapping features of the inflammatory processes present in individuals with COPD. Our composite inflammatory algorithm is described (table 1).
Case management
The needs of patients with COPD are complex and multidimensional, and as clinicians, our responses must also be multidimensional and integrated to meet these needs. Case management is an approach that offers a solution to these healthcare delivery issues in COPD. This approach can be used to complement individualised and phenotype-based treatments in this complex population.
This approach brings together multidimensional assessment, inflammometry and case management. It need not be restricted to COPD, but could usefully be applied to other chronic airway diseases, such as severe asthma and bronchiectasis. We have targeted problems that clustered into four domains: airway-related problems, comorbidity, risk factors and behavioural issues. There are additional issues that could be addressed and require further consideration, such as end of life care and whether disease severity using either GOLD stage or BODE (body mass index/airflow obstruction/dyspnea/exercise capacity) index has an impact on problem assessment and management.
When looking at the prospects and challenges of COPD management in the future, this form of respiratory utopia makes a certain amount of commonsense!
Acknowledgments
The pilot study was funded by the Hunter Medical Research Institute and the John Hunter Hospital Charitable Trust Grants. VMMcD was the recipient of an NHMRC Centre for Respiratory and Sleep Medicine PhD scholarship, and a Cooperative Research Centre for Asthma PhD scholarship. PGG is an NHMRC Practitioner Fellowship recipient. The authors would like to thank and acknowledge Heather Powell for her statistical advice. Additionally we would like to thank and acknowledge Amber Smith for the dietary intervention, Kelly Steel, Rebecca Oldham and Joanne Smart for data collection, the CARD laboratory team for sample processing and the participants for taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors VMMcD: project conception, study design, data collection, data analysis, data interpretation, writing and revisions of the manuscript, study design and revisions of the manuscript. IH: study design and review of manuscript. LGW: study design and review of manuscript. PGG: project conception, study design, data interpretation, and writing/revision of manuscript.
-
Competing interests Dr Vanessa McDonald has been reimbursed for participation in educational meetings from AstraZeneca, Boehringer Ingelheim GlaxoSmithKline and Novartis. She has participated in studies funded by GlaxoSmithKline. Professor Isabel Higgins has no competing interests to declare. Dr Lisa G Wood has no competing interests to declare. Professor Peter Gibson holds an NHMRC Practitioner Fellowship. He has been reimbursed for participation in symposia funded by AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline and Novartis. He has participated in studies funded by Pharmaxis and GlaxoSmithKline.
-
Ethics approval Hunter New England Human Research and Ethics Committee and University of Newcastle.
-
Provenance and peer review Not commissioned; internally peer reviewed.