Article Text

Abstract
Background Bronchopulmonary dysplasia (BPD) remains a main complication of extreme prematurity and currently lacks efficient treatment. Rat bone marrow-derived mesenchymal stem cells (MSC) prevent lung injury in an oxygen-induced model of BPD. Human cord is an advantageous source of stem cells that is especially appealing for the treatment of neonatal diseases. The therapeutic benefit after established lung injury and long-term safety of cord-derived stem cells is unknown.
Methods Human cord-derived perivascular cells (PCs) or cord blood-derived MSCs were delivered prophylactically or after established alveolar injury into the airways of newborn rats exposed to hyperoxia, a well-established BPD model.
Results Rat pups exposed to hyperoxia showed the characteristic arrest in alveolar growth with air space enlargement and loss of lung capillaries. PCs and MSCs partially prevented and rescued lung function and structure. Despite therapeutic benefit, cell engraftment was low, suggesting that PCs and MSCs act via a paracrine effect. Accordingly, cell free-derived conditioned media from PCs and MSCs also exerted therapeutic benefit when used either prophylactically or therapeutically. Finally, long-term (6 months) assessment of stem cell or conditioned media therapy showed no adverse lung effects of either strategy, with persistent improvement in exercise capacity and lung structure.
Conclusions Human umbilical cord-derived PCs and MSCs exert short- and long-term therapeutic benefit without adverse lung effects in this experimental model and offer new therapeutic options for lung diseases characterised by alveolar damage.
- Paediatric Lung Disaese
Statistics from Altmetric.com
Key messages
What is the key question?
-
Is cord-derived cell-based therapy efficient and safe for the prevention and/or treatment of chronic lung disease of prematurity?
What is the bottom line?
-
Currently there is no effective treatment for the most common complication of extreme prematurity.
Why read on?
-
Human cord-derived perivascular cells and cord blood-derived mesenchymal stem cells partially prevent and restore lung structure and function in newborn rats with experimental oxygen-induced arrested alveolar growth through a paracrine effect. Neither whole cell therapy nor cell-free conditioned media therapy adversely affect lung structure and function at 6 months post-treatment.
Introduction
Lung diseases characterised by alveolar damage such as chronic lung disease of prematurity (or bronchopulmonary dysplasia, BPD) and emphysema in adults currently lack efficient treatments. A common denominator of these diseases is the absence of injury resolution leading to distorted tissue repair resulting in arrested alveolar growth in BPD or alveolar destruction in emphysema. Despite intense investigations, current clinical management remains devoid of treatments specifically promoting lung repair.1
Recent insight into stem cell biology has generated excitement over the potential of stem cells to regenerate damaged organs.2 Mesenchymal stem cells (MSCs) have attracted much attention because of their ease of isolation, multilineage developmental potential and immunomodulatory properties.3 Adult rat bone marrow-derived MSCs prevent lung injury in various experimental lung disease models2 including experimental BPD.4 ,5 MSCs can be isolated from different sources including umbilical cord and cord blood, two neonatal cell sources which show unique advantages over the adult MSC counterpart.6
Perivascular cells (PCs) from diverse human tissues give rise to adherent multilineage progenitor cells that exhibit all the features of MSCs and may represent precursors of MSCs, the native identity of which has long been elusive.7 We previously showed that PCs derived in culture from human umbilical cord vessels are candidates for lung repair due to their ability to migrate towards an alveolar type II cell line damaged with bleomycin,8 but their therapeutic potential remains unknown. In this context, we tested two human stem cell populations derived from the perivascular compartment of the umbilical cord (PCs) and from cord blood (MSCs) in newborn rats exposed to hyperoxia, a well-established model mimicking BPD.9 In addition, to select the best possible approach for future clinical applications, we compared two different administration strategies—one prophylactic and one therapeutic—after established lung injury. In order to investigate the mechanisms underlying the beneficial effects and with the perspective of a ‘pharmaceutical’ cell-based therapy, we also tested the therapeutic potential of conditioned media (CdM) from cord-derived PCs and cord blood-derived MSCs. Finally, we evaluated the so far unknown long-term effects of cord-derived cell-based therapies on exercise capacity and lung structure at 6 months of age.
Materials and methods
More details of the methods are available in the online supplement. Procedures were approved by the Institutional Animal Care and Use Committee at the University of Alberta.
PC and MSC isolation, culture and CdM generation
PCs were isolated from the umbilical cords after parental consent as previously described (see online supplementary figure S1).8 CdM was obtained as previously described.5
Animal model of oxygen-arrested lung growth
Rat pups were exposed to normoxia (21% oxygen, control group) or hyperoxia (95% oxygen, BPD group) from birth to P14 in sealed Plexiglas chambers (BioSpherix, Redfield, New York, USA) as described elsewhere.5 ,10
In vivo cell administration
For prevention experiments, newborn rat pups were randomised into seven groups: (1) room air (RA); (2) RA+MSCs; (3) RA+PCs; (4) hyperoxia (oxygen injury model); (5) hyperoxia+human neonatal dermal fibroblast (HNDF); (6) hyperoxia+MSCs; and (7) hyperoxia+PCs. For subsequent rescue experiments only the RA, hyperoxia, hyperoxia+MSC and hyperoxia+PC groups were analysed. Cells were administered at P4 (prevention studies) or P14 (regeneration studies) via an intratracheal injection (300 000/20 μl and 600 000/40 μl, respectively). Lungs were harvested on P22 (prevention studies) or P35 (regeneration studies). Long-term study animals were treated at P4 and lungs were harvested at 6 months.
In vivo CdM administration
CdM was administered daily intraperitoneally at a dose of 7 μl/g from P4 to P21 (prevention studies) or from P14 to P28 (regeneration studies). Lungs were harvested on P22 (prevention studies) or P35 (regeneration studies). Long-term study animals were treated from P4 to P21 and lungs were harvested at 6 months.
Lung function tests
Tests were performed on anaesthetised and paralysed animals using Flexivent (Scireq, Montreal, Quebec, Canada).
Lung morphometry
Alveolar structures were quantified on systematically sampled formaldehyde-fixed lung sections using the mean linear intercept and septal counts.10 ,11
Barium-gelatin angiograms and vessel density counts
Barium was infused in the main pulmonary artery as previously described.5 ,10
Right ventricular hypertrophy and pulmonary artery remodelling
The right ventricle to left ventricle+septum ratio was used as an index of right ventricular hypertrophy.5 Pulmonary artery remodelling was quantified by medial wall thickness.5 ,10
Exercise capacity
Rats were run on a treadmill according to a pre-established protocol.
Total body CT scan
Anaesthetised rats were imaged with a rodent SPECT-CT using Amira software package (Gamma Medica, Northridge, California, USA).
Real-time PCR
Real-time PCR was performed on frozen lungs from three animals per group harvested at various time points after injection as described elsewhere.10
Immunofluorescence
Staining was performed on non-adjacent 5 µm paraffin-embedded lung sections using rabbit anti-human β2-microglobulin (Abcam, Cambridge, Massachusetts, USA) and appropriate secondary antibodies (Invitrogen, Carlsbad, California, USA).
Statistical analysis
Values are expressed as means±SEM. Intergroup differences were assessed using analysis of variance with post hoc test (Fisher probable least significant difference test) (SPSS V.18). A p value of < 0.05 was considered statistically significant. All investigators performing evaluations were blinded to the experimental groups.
Results
Airway delivery of cord-derived PCs or cord blood-derived MSCs prevents and rescues arrested alveolar growth
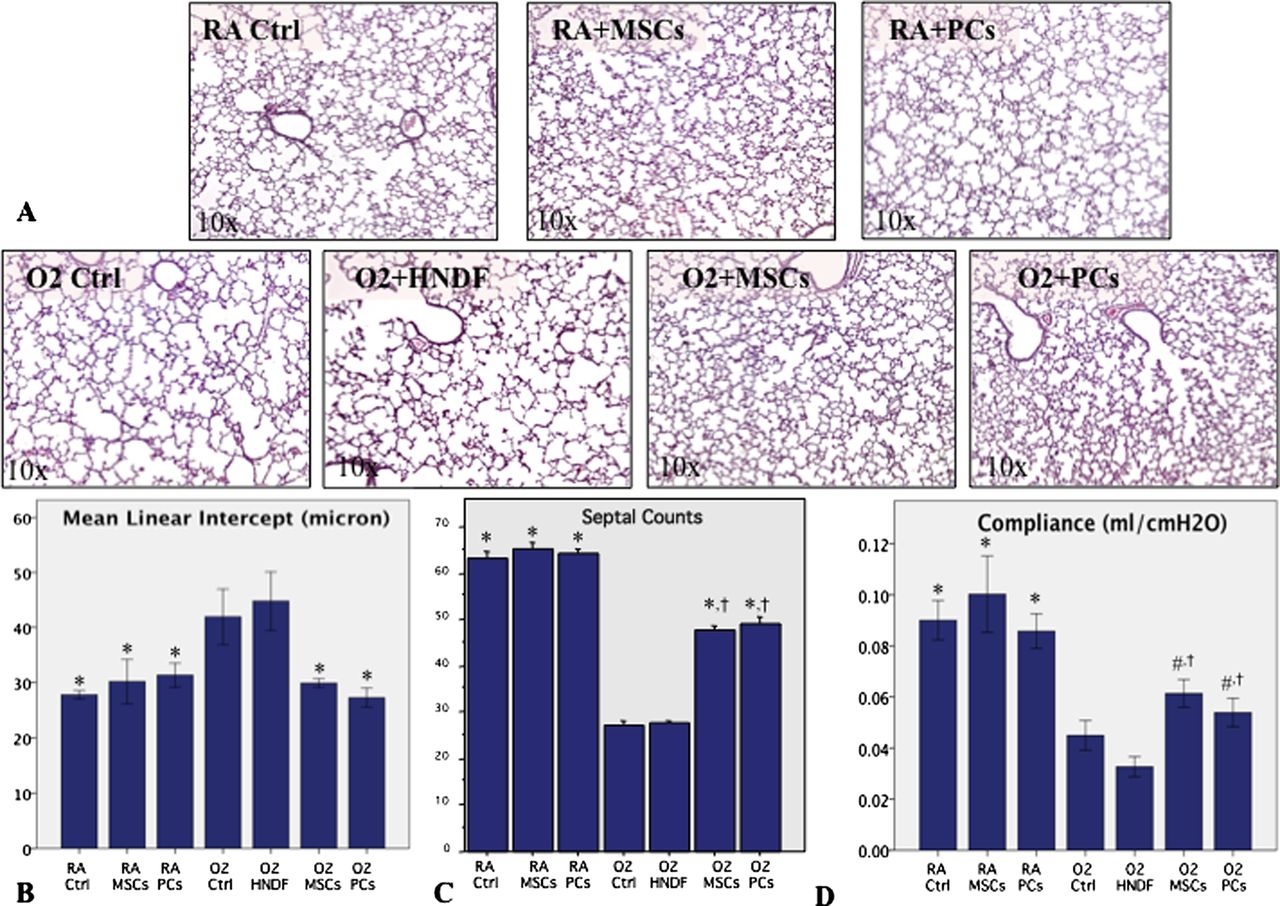
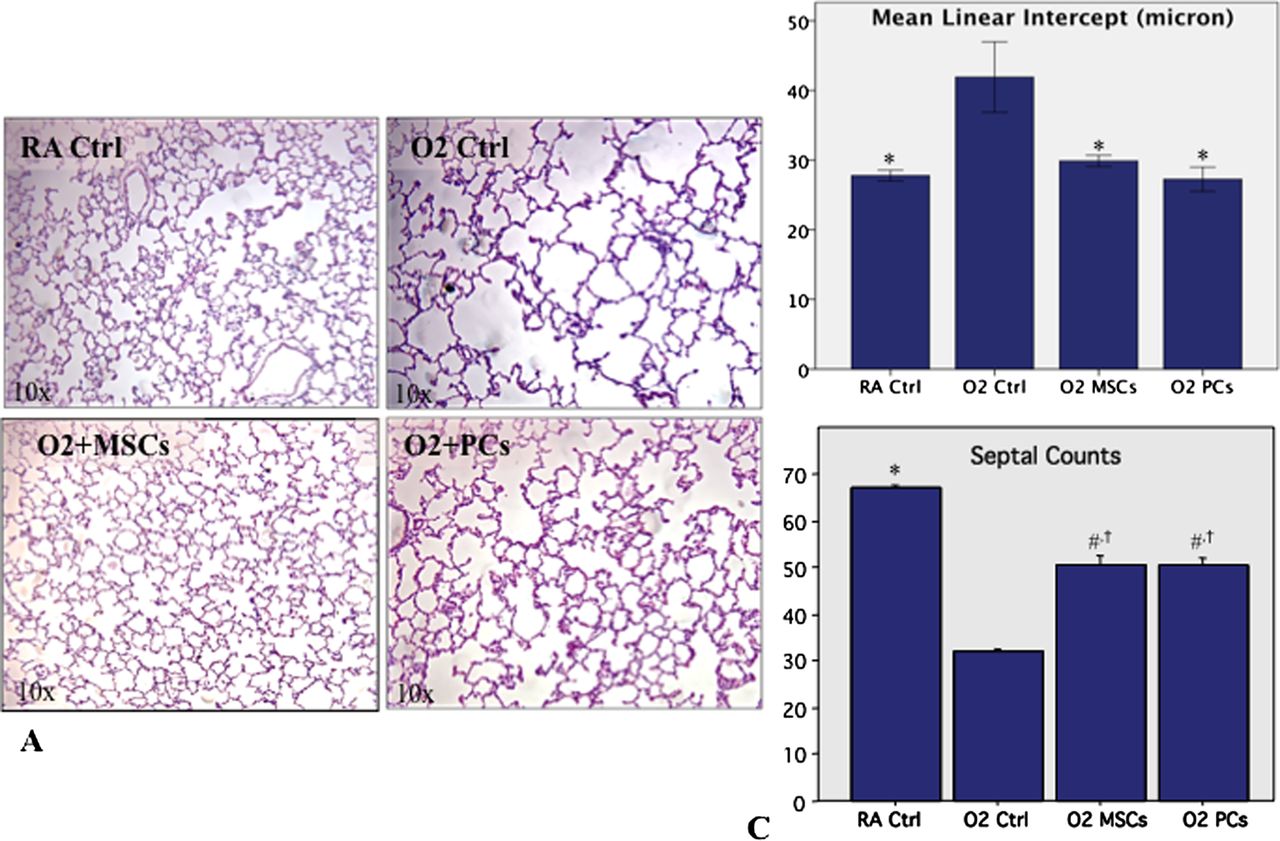
A total of 42 animals were used in the prevention experiments. Exposure of newborn rats to oxygen from P4 to P14, a well-established model mimicking BPD, led to distal air space enlargement, alveolar simplification (figure 1A–C) and decreased lung compliance (figure 1D) compared with RA-housed animals. Prophylactic intratracheal delivery of PCs and MSCs partially preserved alveolar growth (figure 1A–C) and prevented the decrease in lung compliance (figure 1D). Conversely, HNDF used as control cells had no effect on lung function and structure (figure 1). PCs and MSCs had no adverse effect on lung function and structure in RA control animals (figure 1).

Perivascular cells (PCs) and mesenchymal stem cells (MSCs) prevent hyperoxia-induced lung injury. (A) Representative H&E-stained lung sections showing larger and fewer alveoli in hyperoxia-exposed lungs compared with lungs from rats housed in room air (RA) and RA animals treated with MSCs (RA MSCs) and PCs (RA PCs). Intratracheal administration of MSCs (O2+MSCs) and PCs (O2+PCs) in O2-exposed animals partially preserved alveolar growth. Human neonatal dermal fibroblast (HNDF) administration (O2 HNDF) did not show any improvement in oxygen-exposed animals. (B,C) Quantitative confirmation is provided by the mean linear intercept (n=6/group; *p<0.001 vs O2 Ctrl and O2 HNDF. No differences between O2+MSCs and O2+PCs and RA+MSC and RA+PCs) and the septal counts (n=6/group, *p<0.001 vs O2 Ctrl and O2 HNDF, †p<0.01 vs O2+MSCs and O2+PCs vs all RA groups). (D) Lung function testing shows decreased lung compliance in untreated oxygen-exposed animals compared with RA Ctrl and RA MSC and RA PC groups. Compliance was significantly improved in oxygen-exposed animals treated with MSCs and PCs. HNDF administration (O2 HNDF) had no effect on lung compliance (n=6/group; #p<0.05 vs O2 Ctrl; *p<0.001 vs O2 Ctrl and O2 HNDF; †p<0.01 O2+MSCs and O2+PCs vs all RA groups). This figure is only reproduced in colour in the online version.
A total of 24 animals were used in the rescue experiments. Administration of both PCs and MSCs at P14 as rescue therapy after established arrested alveolar growth restored normal alveolar architecture (figure 2A–C).
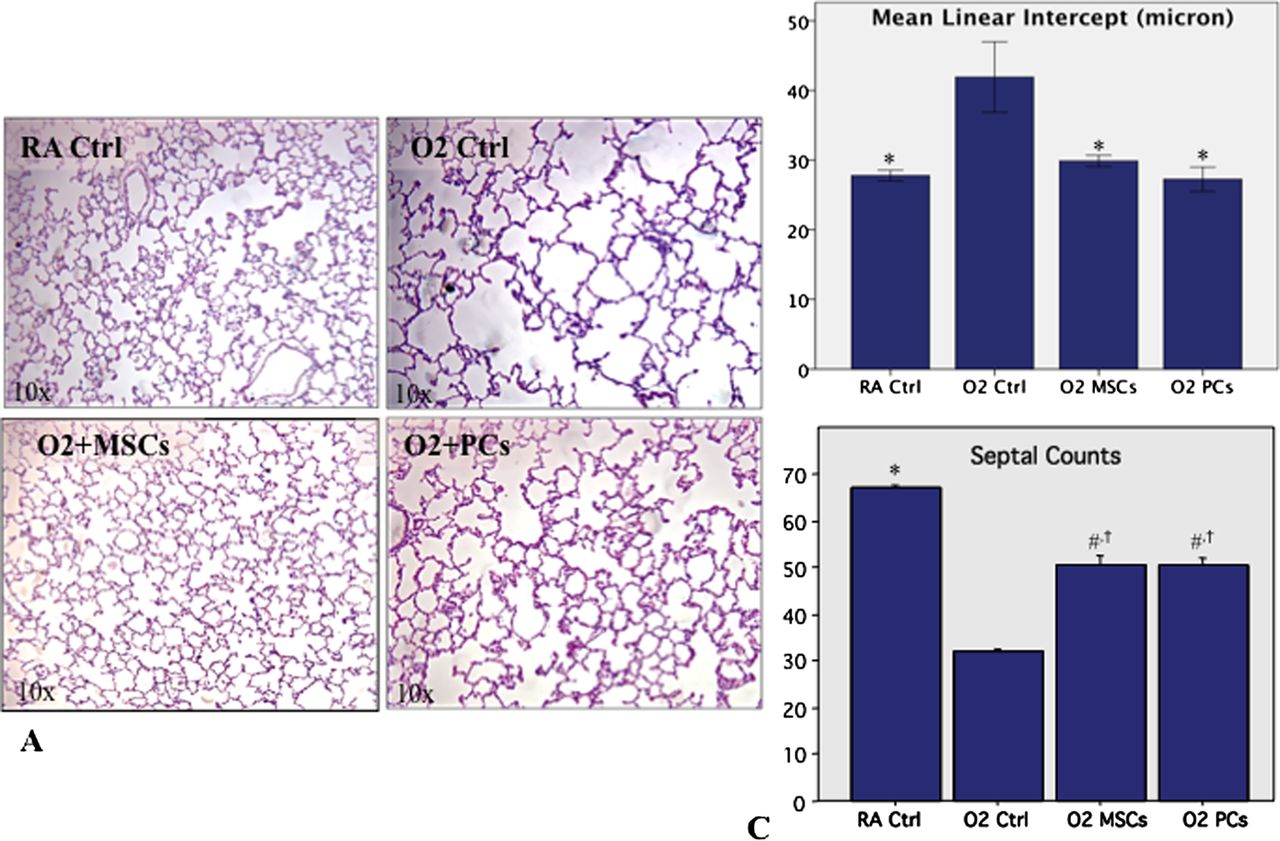
Perivascular cells (PCs) and mesenchymal stem cells (MSCs) rescue hyperoxia-induced lung injury. (A) Representative H&E-stained lung sections of animals treated intratracheally with MSCs and PCs at P14 after established lung injury and harvested at P28. MSCs (O2+MSCs) and PCs (O2+PCs) in oxygen-exposed animals partially restored alveolar growth. (B,C) This is confirmed by the mean linear intercept (n=6/group; *p<0.001 vs O2 Ctrl; no differences between O2+MSCs and O2+PCs and room air (RA)+MSCs and RA+PCs) and the septal counts (n=6/group; #p<0.01 vs O2 Ctrl; *p<0.001 vs O2 Ctrl; †p<0.01 vs RA control). This figure is only reproduced in colour in the online version.
Lung engraftment of PCs and MSCs is low
Immunofluorescent staining for human β2-microglobulin in P22 lungs 18 days after administration of PCs and MSCs localised very few cells within the lung (figure 3A). Quantification of human cells using qRT-PCR confirmed the low rate of engraftment in recipient lungs with a dramatic decrease in detected human Alu sequences from the first day after injection to almost undetectable levels within 4 days (figure 3B). A total of 42 animals were used (3/time point/cell type).

Low engraftment rate after intratracheal injection of perivascular cells (PCs) and mesenchymal stem cells. (A) Immunofluorescent staining for human β2-microglobulin (HB2-MG) at P22, performed in order to detect cells of human origin in the recipient lungs, showed a low rate of engraftment of both cell types. (B) Quantitative RT-PCR for Alu sequences revealed a dramatic decrease during the first day after injection. Human DNA became almost undetectable 4 days after injection. Values indicate 2ΔΔCT for human/rat 18s and Alu sequences. The control samples were non-injected lungs (n=3 animals/time point). This figure is only reproduced in colour in the online version.
Therapeutic benefit of PCs and MSCs is mediated via a paracrine effect
Low cell engraftment suggests the therapeutic benefit is unlikely to be due to cell replacement. Evidence suggests that stem cells act in a paracrine fashion. To verify this hypothesis, we assessed in vivo the therapeutic potential of CdM harvested from PC and MSC serum-free cultures. A total of 36 animals were used in the prevention experiments to assess lung morphometry, lung function and features of pulmonary hypertension. Prophylactic daily intraperitoneal CdM injections (7 μl/g) from P4 to P21 improved alveolar architecture (figure 4A–C) and lung function (figure 4D). CdM from PCs or MSCs had no adverse effects on lung function and structure in RA control animals.

Conditioned media (CdM) from perivascular cells (PCs) and mesenchymal stem cells (MSCs) prevent hyperoxia-induced lung injury. (A) Representative H&E-stained lung sections showing larger and fewer alveoli in hyperoxia-exposed lungs compared with lungs from rats housed in room air (RA) and RA animals treated with MSC CdM and PC CdM. Daily intraperitoneal administration of MSC CdM and PC CdM in oxygen-exposed animals improved alveolar growth. (B,C) Quantitative confirmation is provided by the mean linear intercept (n=6/group; *p<0.001 vs O2 Ctrl; no differences between O2+CdM MSCs and O2+PC CdM and RA+MSC CdM and RA+PC CdM) and the septal counts (n=6/group; *p<0.001 vs O2 Ctrl; †p<0.01 vs all RA groups). (D) Invasive lung function testing shows decreased lung compliance in untreated oxyten-exposed animals compared with RA Ctrl and RA MSC CdM and RA PC CdM groups. Lung compliance was significantly improved in oxygen-exposed animals treated with MSC CdM and PC CdM (n=6/group; *p<0.001 vs O2 Ctrl; #p<0.05 O2+MSC CdM vs RA+CdM MSC and O2+PC CdM vs RA+PC CdM). This figure is only reproduced in colour in the online version.
Another hallmark of BPD is rarefaction of pulmonary vessels.12 Lung CT scans of barium-injected pulmonary arteries showed severe rarefaction of pulmonary vessels in oxygen-exposed animals (figure 5A). PC and MSC CdM partially prevented the arrest in lung angiogenesis (figure 5A). Quantification of barium gelatin-injected pulmonary vessels (a total of 24 animals were assessed for lung vessel density) confirmed the severe decrease in pulmonary vascular density in the hyperoxic group (figure 5B). Both PC and MSC CdM significantly attenuated the decrease in pulmonary vascular density (figure 5B), but to a lesser extent than the improvements seen in lung morphometry and function.
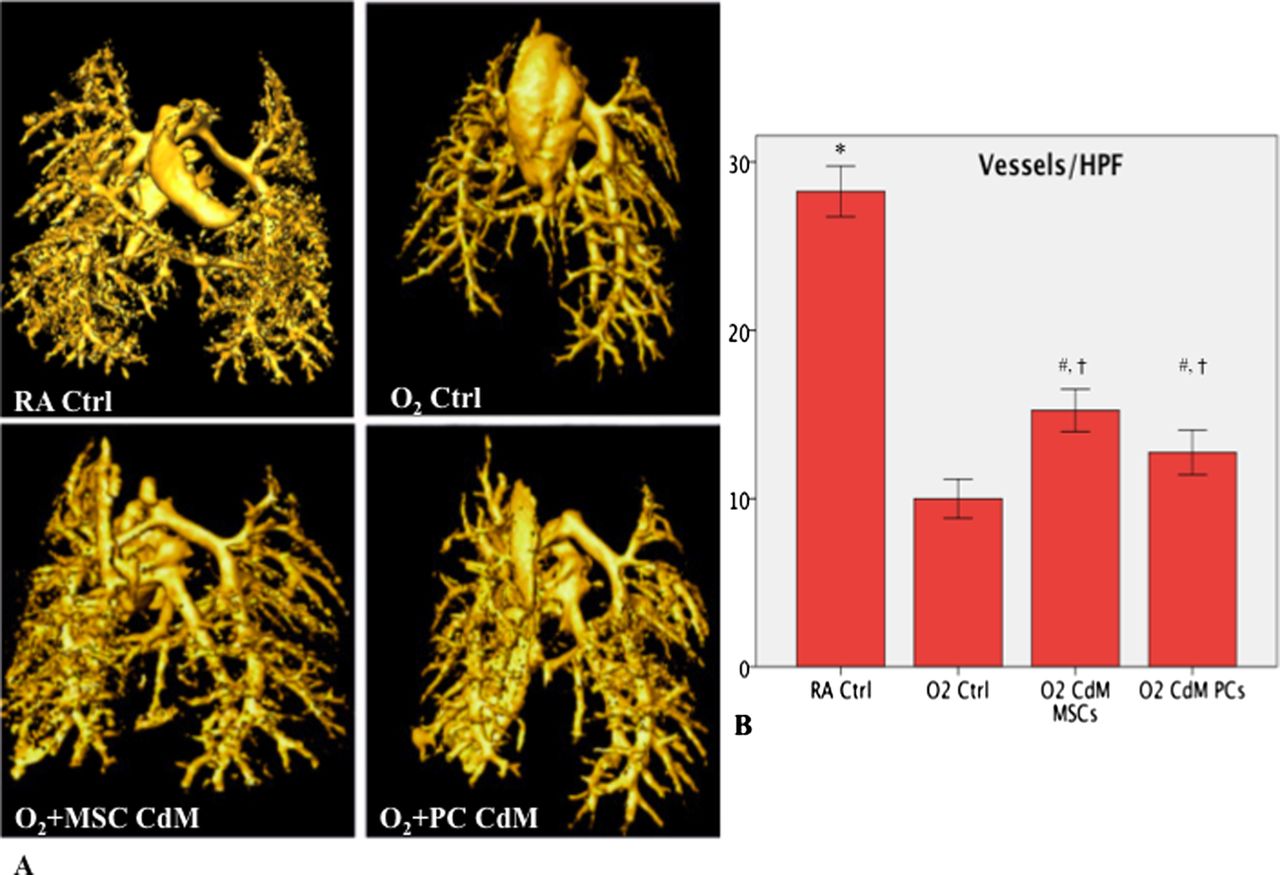
Conditioned media (CdM) from perivascular cells (PCs) and mesenchymal stem cells (MSCs) improve lung angiogenesis. (A) Representative micro-CT scans of the pulmonary vasculature after barium injection into the pulmonary artery. (B) Mean vessel density assessed on barium-injected lungs was significantly decreased in the lungs of oxygen-exposed animals. Daily intraperitoneal administration of MSC CdM and PC CdM improved lung vessel density (n=6 animals/group; *p<0.001 vs O2 Ctrl; #p<0.05 vs O2 Ctrl; †p<0.001 vs all room air Ctrl). This figure is only reproduced in colour in the online version.
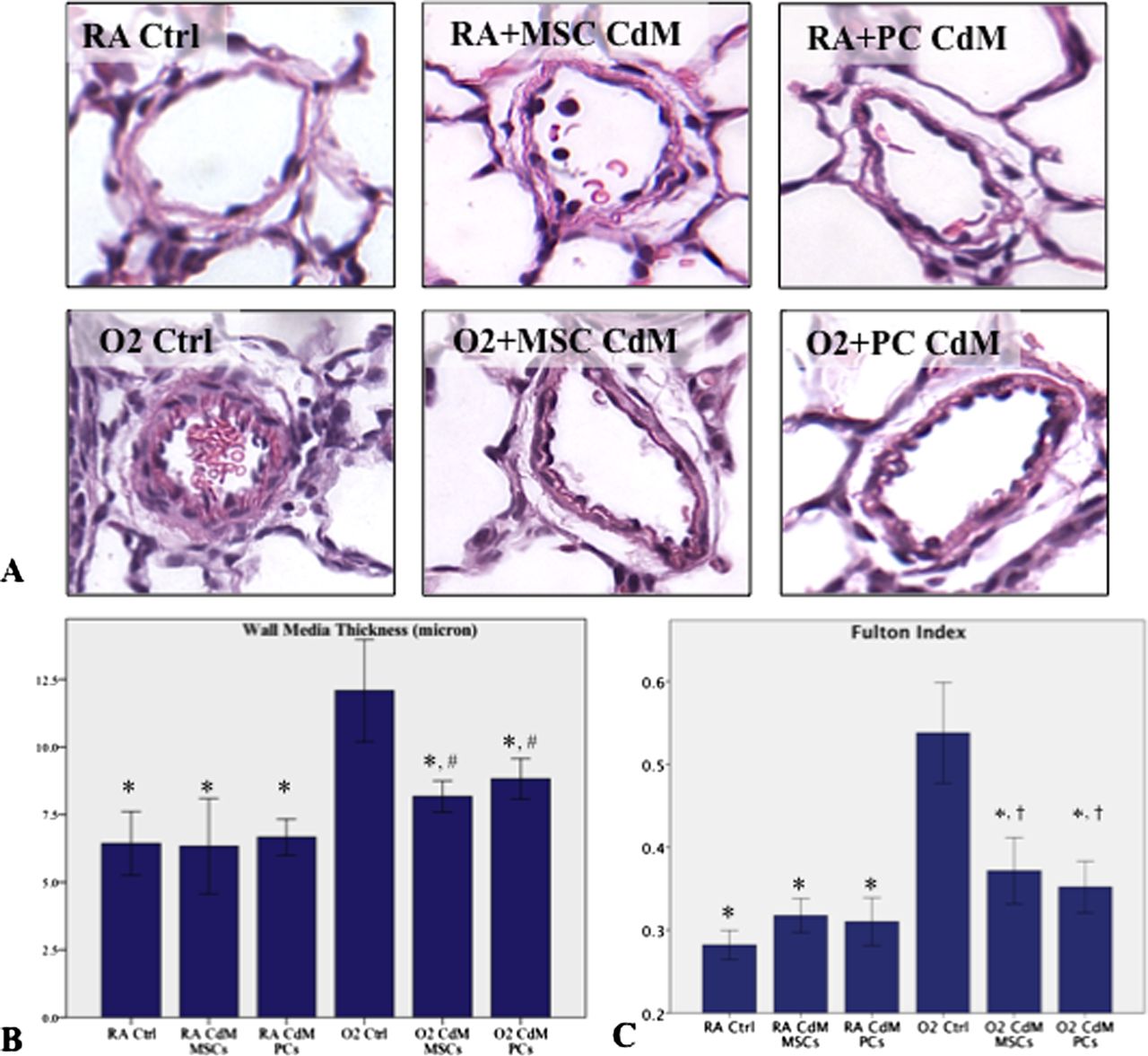
Pulmonary hypertension is a common complication of BPD and significantly worsens the prognosis.13 PC and MSC CdM were effective in preventing pulmonary arterial wall remodelling (figure 6A,B) and right ventricular hypertrophy (figure 6C), two structural features of pulmonary hypertension.
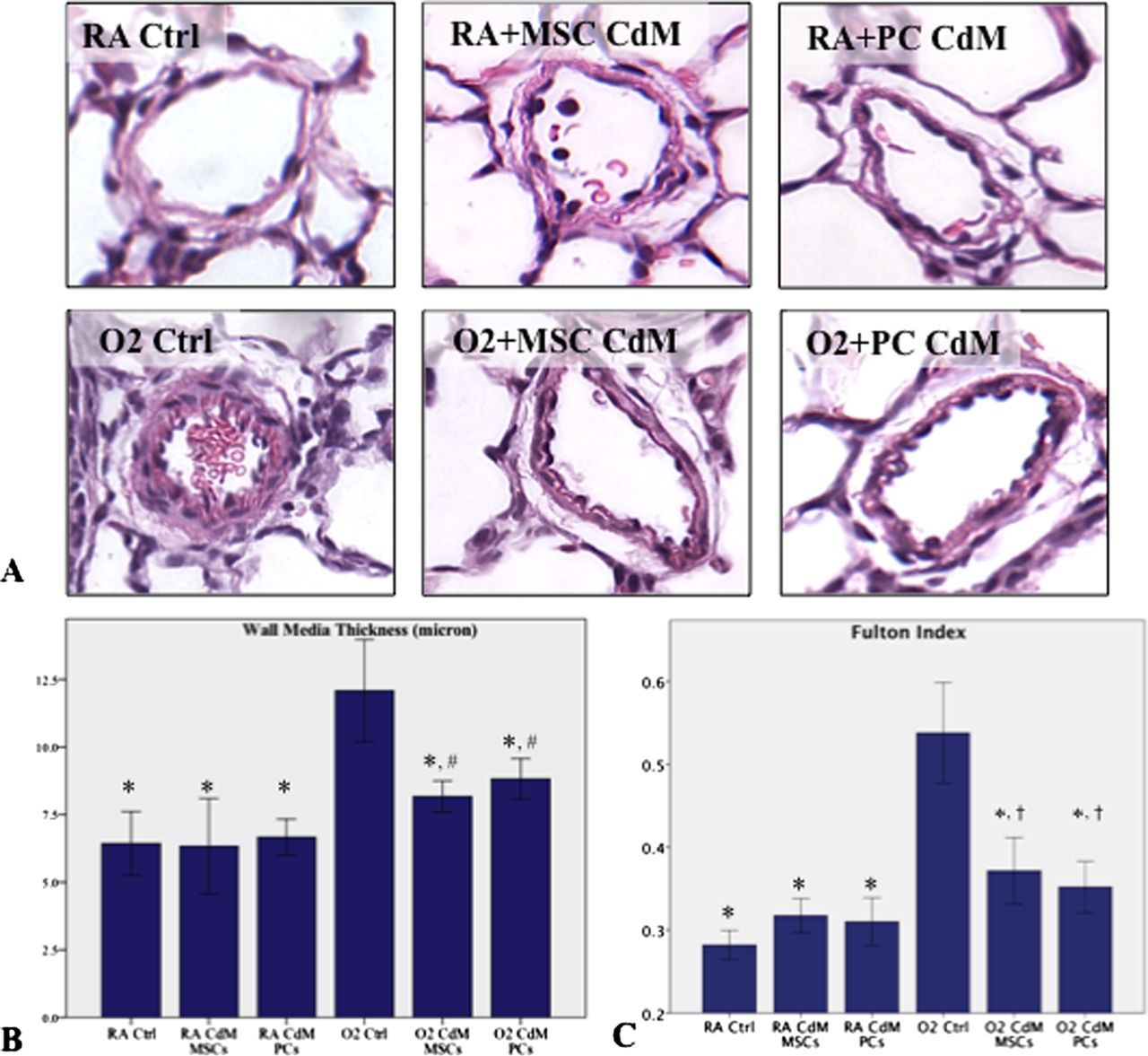
Conditioned media (CdM) from perivascular cells (PCs) and mesenchymal stem cells (MSCs) prevent features of pulmonary hypertension. (A) Representative H&E sections of pulmonary arteries from the six experimental groups. (B) Hyperoxic-exposed rats had a significant increase in media wall thickness (MWT) compared with room air (RA) housed rat pups. MSC CdM and PC CdM significantly reduced MWT (n=5 animals/group; *p<0.001 vs O2 Ctrl; #p<0.01 vs all RA groups). (C) Fulton index, reflecting right ventricular hypertrophy, was significantly increased in untreated oxygen-exposed rats compared with RA Ctrl, RA MSC CdM and RA PC CdM groups. MSC CdM and PC CdM significantly reduced MWT (n=5 animals/group; *p<0.001 vs O2 Ctrl; †p<0.05 vs all RA groups). This figure is only reproduced in colour in the online version.
Similar to whole cell therapy, therapeutic administration of PC and MSC CdM (from P14 to P28 assessed in 24 animals) after established lung injury improved alveolar architecture (figure 7A–C) and lung function (figure 7D).

Conditioned media (CdM) from perivascular cells (PCs) and mesenchymal stem cells (MSCs) rescue hyperoxia-induced lung injury. (A) Representative H&E-stained lung sections showing larger and fewer alveoli in hyperoxia-exposed lungs compared with lungs from rats housed in room air (RA) and RA animals treated with MSC CdM and PC CdM. Daily intraperitoneal administration of MSC CdM and PC CdM after established arrested alveolar growth restored almost normal lung architecture in oxygen-exposed animals. (B,C) Quantitative assessment by the mean linear intercept (n=6 animals/group; #p<0.05 vs O2 Ctrl; *p<0.001 vs O2 Ctrl; †p<0.05 vs RA Ctrl) and the septal counts (n=6 animals/group; *p<0.001 vs O2 Ctrl; †p<0.05 vs RA Ctrl) confirms larger and fewer alveoli in hyperoxia-exposed lungs compared with lungs from rats housed in RA and RA animals treated with CdM MSC and CdM PC. CdM MSC and CdM PC restored alveolar growth. (D) Invasive lung function testing shows decreased lung compliance in untreated oxygen-exposed animals compared with RA Ctrl and RA MSC and RA PC groups. Compliance was significantly improved in oxygen-exposed animals treated with CdM MSC and CdM PC (n=6 animals/group; # p<0.05 vs O2 Ctrl). This figure is only reproduced in colour in the online version.
PCs and MSCs display long-term safety
Seventy-two animals were kept alive for 6 months for long-term evaluation of whole cell therapy (36 animals) and CdM therapy (36 animals).
Intrapulmonary delivery of PCs and MSCs at P4 was safe up to 6 months of life. Total body CT scans did not reveal any suspicious images suggesting tumour formation (figure 8A). A single suspicious CT scan picture was ruled out as a congested vessel at histology (figure 8B). Exercise capacity, using a graduated treadmill exercise protocol by a blinded observer, was significantly decreased in untreated oxygen-exposed rats (figure 8C). This was associated with persistent enlarged and simplified distal airspaces (figure 8D–F). Rats treated with whole cell therapy exhibited significantly improved exercise capacity (figure 8C) and showed almost normal alveolar architecture (figure 9D–F) at 6 months of age. Control RA housed animals treated with whole cell therapy showed no adverse effect on exercise capacity (figure 8C) or lung structure (figure 8D–F).

Long-term (6 months) safety and efficacy of stem cell therapy. (A) Representative CT scan performed at 6 months of age showed no suspicious images in the perivascular cell (PC) group and one doubtful image in the mesenchymal stem cell (MSC) group (n=4 animals/group). The corresponding histology samples (B, insert) ruled out the presence of a possible tumour and indicated a congested blood vessel. (C) Oxygen-exposed animal experienced reduced exercise capacity at 6 months of age compared with animals housed in room air (RA). Oxygen-exposed animals treated with MSCs and PCs had improved exercise capacity (n=6 animals/group; # p<0.05 vs O2 Ctrl; no differences between O2+MSC and RA+MSC and O2+PC and RA+PC). (D) Representative H&E-stained lung sections show persistent alveolar simplification at 6 months of age in hyperoxia-exposed animals compared with lungs from rats housed in RA. Oxygen-exposed animals treated with MSCs and PCs presented with improved lung histology. (E,F) The mean linear intercept (n=6 animals/group; #p<0.05 vs O2 Ctrl; *p<0.001 vs O2 Ctrl; †p<0.05 O2+MSC vs RA+MSC and O2+PC vs RA+PC) and the septal counts (n=6 animals/group; *p<0.001 vs O2 Ctrl, †p<0.01 O2+MSC vs RA+MSC and O2+PC vs RA+PC) confirm arrested alveolar growth in untreated oxygen-exposed animals and preserved alveolar structure with MSC and PC treatment. This figure is only reproduced in colour in the online version.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
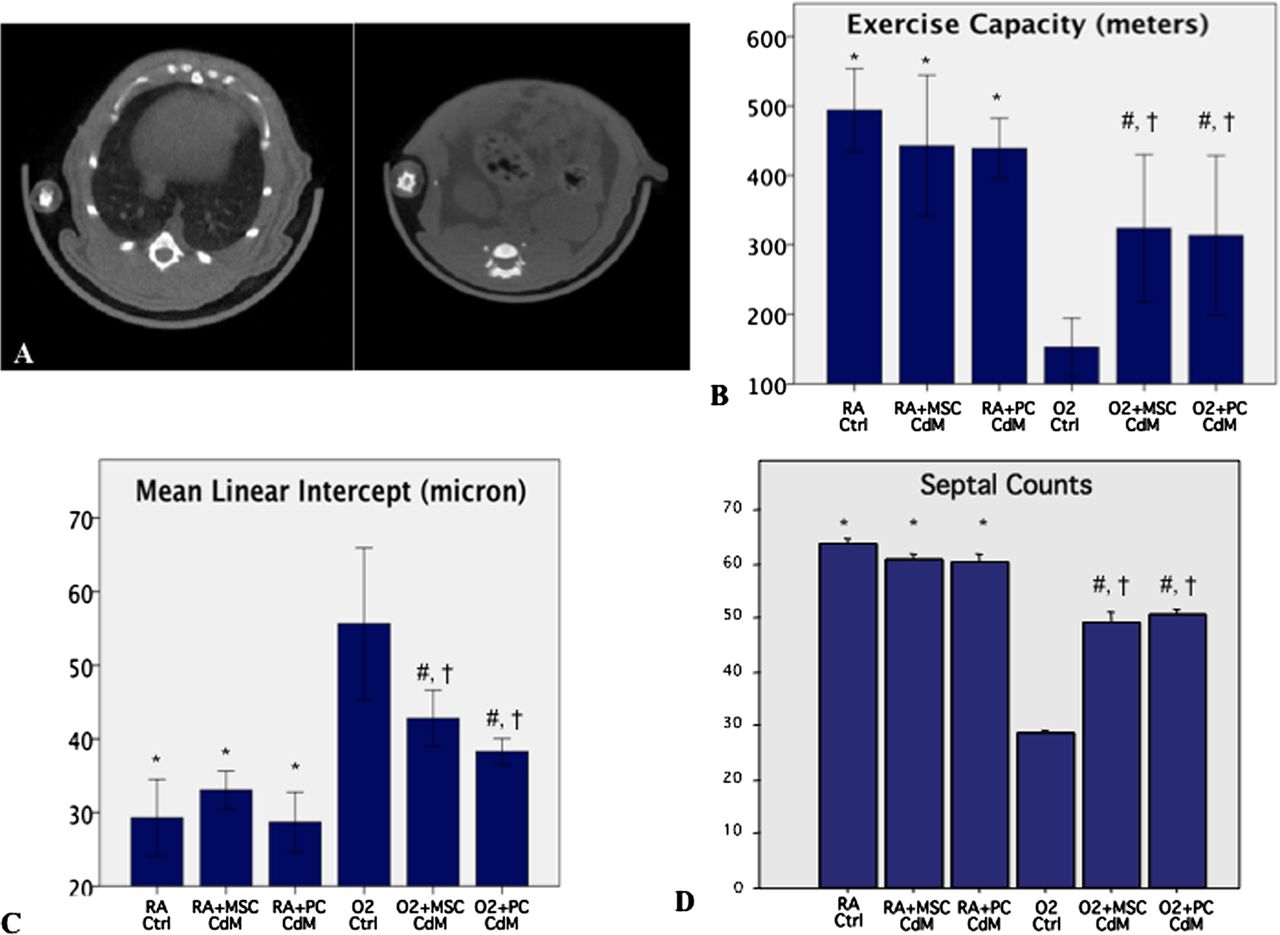
Long-term (6 months) safety and efficacy of conditioned media (CdM) therapy. (A) Representative CT scan performed at 6 months of age in a CdM perivascular cell (PC) treated animal. There were no suspicious images in the treated groups (n=4 animals/group). (B) Oxygen-exposed animals experienced reduced exercise capacity at 6 months of age compared with animals housed in room air (RA). Oxygen-exposed animals treated with CdM mesenchymal stem cells (MSCs) and CdM PCs had improved exercise capacity (n=6 animals/group; #p<0.05 vs O2 Ctrl; *p<0.001 vs O2 Ctrl; †p<0.05 O2+MSC vs RA+MSC and O2+PC vs RA+PC). (C, D) Quantitative assessment of lung structure confirms the persistent alveolar simplification at 6 months of age in hyperoxia-exposed animals compared with lungs from rats housed in RA. Oxygen-exposed animals treated with CdM MSC and CdM PC presented with improved lung histology (n=6 animals/group; #p<0.05 vs O2 Ctrl; *p<0.001 vs O2 Ctrl; †p<0.01 O2+MSC vs RA+MSC and O2+PC vs RA+PC). This figure is only reproduced in colour in the online version.
Likewise, animals evaluated 6 months after PC- and MSC-derived CdM treatment showed no suspicious CT scans (figure 9A). These animals also had significantly improved exercise capacity (figure 9B) and alveolar architecture (figure 9C,D).
Discussion
The major findings in this study include: (1) the efficacy of human cord-derived PCs and cord blood-derived MSCs in preventing and rescuing oxygen-induced arrested alveolar growth; (2) PCs, similar to MSCs, exert their therapeutic benefit primarily through a paracrine effect; and (3) the long-term efficacy and absence of adverse lung effects of whole cell or CdM therapy at 6 months.
Therapeutic potential of cord-derived cells
We harnessed the potential of umbilical cord and cord blood as stem cell sources because of their numerous advantages, in particular for neonates. Indeed, among the various sources of stem cells, umbilical cord and cord blood represent an ethically non-controversial, clinically relevant and easily accessible source of potent stem cells.6 ,14
Among stem cells, MSCs have attracted most attention and numerous clinical trials are underway (http://clinicaltrials.gov/ct2/results?term=mesenchymal+stem+cells) to test their therapeutic potential for regenerative purposes.3 Recently, PCs in numerous human organs have been characterised based on expression of CD146, NG2 and PDGFRβ and the absence of haematopoietic, endothelial and myogenic cell markers.7 In addition to their vascular functions, human PCs are multilineage progenitor cells that natively exhibit features of MSC and give rise in culture to adherent cells indistinguishable from conventional MSCs, confirming previously documented similarities between pericytes and MSCs.7 The capacity of human pericytes to generate skeletal muscle, bone, cartilage7 ,15 ,16 and to form vascular grafts15 has already been documented, but the therapeutic potential of these cells in lung diseases has not yet been investigated.
Here we show that, similar to MSCs, cord-derived PCs demonstrate repair potential by preserving lung function and preventing oxygen-induced arrested alveolar growth in newborn rats. Our observation, combined with previous findings showing that bone marrow- and cord-derived MSCs attenuate lung inflammation in this model,4 ,17 make cord-derived cell-based therapies appealing for the prevention of lung injury. The prevention approach is legitimate in BPD as one can predict which premature infants are at high risk for developing the disease. Furthermore, we have shown that PCs and MSCs restore lung function and structure after established lung injury. This is relevant for lung diseases characterised by currently irreversible alveolar destruction, including emphysema.
Paracrine effect of cord-derived stem cells
Very few engrafted cells were detected by immunofluorescence and analysis of human-specific Alu sequences, consistent with previous reports suggesting that engraftment does not account for the therapeutic benefit.18 ,19 The current concept supports the view that MSCs act via a paracrine effect.20 Indeed, MSCs produce and secrete a variety of cytokines, chemokines and growth factors that may contribute to tissue repair.21 There is evidence that pericytes exert their benefit through a similar mechanism. In the vicinity of peripheral nerves, pericytes secrete neurotrophic soluble factors facilitating axonal regeneration in peripheral neuropathy.22 We have previously documented the secretion by cultured human pericytes of diverse cytokines23 and observed that cord-derived PCs produce higher levels of keratinocyte growth factor (KGF)—a factor recently demonstrated to mediate the therapeutic benefit of human bone marrow-derived MSC CdM in endotoxin-induced acute lung injury in the ex vivo perfused human lung24 and in ventilation-induced lung injury25—when co-cultured with damaged lung cells.8
In the present study we provide in vivo evidence for the therapeutic benefit of cord-derived PC CdM. Prophylactic CdM administration improved lung function and structure. Moreover, CdM preserved lung angiogenesis—known to contribute to normal lung growth and to be impaired in BPD10—and prevented pulmonary hypertension, a life-threatening complication of BPD.13 We opted for daily intraperitoneal administration of CdM, reasoning that repetitive dispensation would be required to insure a constant release of protective factors to achieve a therapeutic benefit. Accumulating evidence, however, suggests that a single dose of CdM is enough to prevent oxygen-induced lung injury in neonatal mice.4 ,26 This is consistent with recent data suggesting that MSCs act through the release of microparticles27 or via mitochondrial transfer.28 These observations may explain why a single injection of CdM may be sufficient to obtain a therapeutic benefit. This also opens new therapeutic avenues for cell-based therapies. Indeed, the recognition of MSC release of microparticles acting as micropackages containing a combination of healing factors may circumvent the complex task of identifying each of the various healing compounds and determining the most potent healing combination of these factors. This may also be relevant for the design of clinical trials to determine the most efficacious and safest stem cell-based approach: whole cell therapy versus cell-derived CdM versus single or multiple identified CdM-derived compounds. Ex vivo preconditioning may further enhance the efficacy and also facilitate the discovery of MSC-derived repair molecules.29
The discrepancy between the striking improvement in lung morphometry and lung function with CdM and a more moderate effect on pulmonary vessel density is unexpected. One may speculate that secretion of epithelial growth factors by MSCs—KGF in particular—promotes preferential alveolar epithelial cell protection leading to improved lung histology.24 ,25 However, MSCs also produce many pro-angiogenic factors to stimulate vascular growth and Hansmann et al recently showed efficient restoration of the pulmonary vascular bed with intravenous MSC CdM in neonatal mice exposed to hyperoxia.26 ,30 Further studies in various animal models of chronic neonatal lung injury are required to clarify these observations.
Long-term effects of whole cell therapy and CdM
BPD can have life-long consequences including impaired lung function, asthma, early onset emphysema and pulmonary hypertension.31 Similarly, our model showed long-lasting alterations in lung function and structure following neonatal hyperoxia. Animals exposed to oxygen from P4 to P14 still displayed altered exercise capacity and arrested alveolar growth at 6 months of age (life span 2–3 years). More importantly, the therapeutic benefit of both whole cell therapy and CdM administration was sustained, showing improved exercise capacity and lung histology 6 months after treatment. Furthermore, 6 months after injection of PCs and MSCs or their CdM, no tumours were detectable on total body CT scans.
A limitation of the well-established neonatal rodent model to mimic BPD via hyperoxic exposure is that oxygen represents only one among many deleterious factors contributing to BPD such as mechanical ventilation and pre- and postnatal inflammation. Recent observations suggest that MSCs prevent ventilation-induced lung injury in adult rats.25 In the developing lung, human amnion epithelial cells prevent ventilation- and inflammation-induced lung injury in fetal sheep.32 ,33 These studies add another interesting reparative cell source for cell-based therapies.
In conclusion, human umbilical cord-derived PCs, as whole cell therapy or growth factor producers, show promise as a new cell-based therapy for lung diseases characterised by arrested alveolar growth/loss of alveoli.
Acknowledgments
The authors thank Dr Lakshmi Puttagunta for expert advice on lung pathology.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors MP, LI, GO, FM and BT designed the study. MP, LI, AV, GW and FE performed the experiments. SB carried out the western blots. DM read the CT scans. TM and LL harvested and characterised the cord-derived cells. MP, BP, LL, TM and BT drafted the manuscript and are guarantors of the paper.
-
Funding This work was supported by the Canadian Institutes of Health Research (CIHR MOP 84429). AV and LC were supported by a stipend from the Maternal Fetal Neonatal Health Training Program (MFN) sponsored by CIHR-IHDCYH. BT is also supported by the Alberta Heritage Foundation for Medical Research (AHFMR)/Alberta Innovates Health Solutions, Canada Foundation for Innovation (CFI), the Canada Research Chairs Program and by the Stollery Children's Hospital Foundation. This study was also supported by grants from the 6FP EU Project—THERCORD and the 7FP EU Project—CASCADE and REBORNE (TM and LL).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves