Article Text

Abstract
Background Lung cancer resection rates are low in England, but reports have indicated an increase in recent years. We analysed the recent trends in surgical resection by age, sex, socioeconomic deprivation and surgical procedure in England.
Methods Data on 286 217 patients with non-small cell lung cancer diagnosed between 1998 and 2008 were extracted from the English Cancer Repository Dataset and information on surgical resection for these patients was retrieved from linked Hospital Episode Statistics records. We calculated the OR of undergoing surgery per 1-year increment by age, sex, socioeconomic deprivation and surgical procedure. A multinomial logistic regression model was used to assess the association between age and type of surgery.
Results The proportion of patients with non-small cell lung cancer undergoing surgery increased from 8.8% in 1998 to 10.6% in 2008. The increase was similar between levels of socioeconomic deprivation, slightly more pronounced among women (OR=1.023 per 1-year calendar increment, 95% CI 1.016 to 1.029) than men (OR=1.010, 95% CI 1.005 to 1.015) and most prominent with increasing age (75–79 age group: OR 1.051, 95% CI 1.041 to 1.062; 80–84 age group: OR 1.102, 95% CI 1.080 to 1.124; and 85+ age group: OR 1.130, 95% CI 1.069 to 1.193). Increasing age was associated with a decreased likelihood of undergoing pneumonectomy (OR 0.88, 95% CI 0.87 to 0.89 per 5-year age increment) or sleeve resection (OR 0.75, 95% CI 0.71 to 0.79) compared with lobectomy, and a slightly increased likelihood of undergoing a wedge resection (OR 1.08, 95% CI 1.06 to 1.10).
Conclusion Resection rates have increased in England in recent years and most markedly so in the older age groups.
- Lung cancer
- resection
- age
- surgery
- epidemiology
- England
Statistics from Altmetric.com
Key messages
What is the key question?
Do recent trends in surgical resection rate vary by age, sex, socioeconomic deprivation and surgery type in England?
What is the bottom line?
Resection rates in England are reportedly low compared with other countries. However, in recent years there has been an increase in resection rate.
Why read on?
This manuscript shows a clear increase in the resection rate in England, which mainly affects the older age groups.
Introduction
Non-small cell lung cancer (NSCLC) accounts for about 85% of all lung cancers. The National Institute for Health and Clinical Excellence (NICE) recommends offering surgical resection as the treatment of first choice to patients with NSCLC who are medically fit and suitable for treatment with curative intent.1 Although observational studies often show survival benefit with surgical resection, the lack of evidence in the form of randomised clinical trials for lung cancer surgery and particularly in relation to radiotherapy and chemotherapy for more advanced disease has recently been raised.2
Differences in the frequency of surgery for patients with respect to their age, sex and socioeconomic deprivation have been described.3–5 Older patients have been found to be less likely to undergo surgery compared with younger patients even when they have similar performance status.3 Many investigators have proposed that there needs to be an increase in the rate of surgery for older patients.3 ,6 ,7 Finally, it has been shown that patients with lung cancer living in deprived areas are less likely to undergo surgery.5
The resection rate in England is low compared with other countries with similar healthcare systems,8 and we have previously shown that resection rates in England were variable.9 Over the past 5 years an increase in resection rate has been reported,10–12 and this trend was accompanied by a decrease in pneumonectomy in favour of more limited surgery.10
Herein, we describe the recent trends in surgical resection rate by age, sex, socioeconomic deprivation and surgery type.
Methods
Data
We extracted data on 348 579 patients with lung cancer (International Classification of Diseases, 10th revision, C33–C34) diagnosed between 1998 and 2008 from the National Cancer Data Repository (NCDR). The NCDR contains data on all cancers in England. These data are quality assured in each cancer registry before being merged into the English dataset. We excluded all cancers registered as death certificate only (n=19 832 (6%)) and 42 532 (12%) patients with small-cell lung cancer, leaving 286 217 patients eligible for analysis.
Information on surgery was retrieved from linked Hospital Episode Statistics records. Surgery information from 1 month before to 6 months after the NCDR date of diagnosis was included. If patients had more than one recorded surgery type, the most extensive procedure was used in the analysis.
Surgical procedures in Hospital Episode Statistics are defined according to codes from the Office of Population, Censuses and Surveys Classification of Surgical Operations and Procedures (4th revision, OPCS-4).13 We classified the surgical procedures as indicated in table 1.
Classification of surgical procedures according to Office of Population, Censuses and Surveys Classification of Surgical Operations and Procedures, fourth revision codes
Socioeconomic deprivation information on patients was obtained by mapping the postcode of residence at diagnosis of each patient with lung cancer to a lower super output area (LSOA). LSOAs are geographic areas of a consistent size that cover a population of approximately 1500 persons. Using the income domain of the Indices of Multiple Deprivation 2010,14 LSOAs were grouped into five socioeconomic deprivation quintiles, each containing 20% of LSOAs in England. Thus each patient was assigned to a quintile of socioeconomic deprivation.
Data analysis
We used logistic regression analysis to assess the change in the proportion of patients with NSCLC undergoing surgery per 1-year increment by age, sex, socioeconomic deprivation and type of surgery. A multinomial logistic regression model was used to assess the odds of undergoing a pneumonectomy, wedge resection, sleeve resection or other limited surgery compared with a lobectomy per 5-year age increment.
Results
From 1998 to 2008 the proportion of patients with NSCLC undergoing a surgical resection increased from 8.8% to 10.6%.
The proportion of men and women undergoing surgery increased, however the increase was slightly greater among women (OR=1.023 per one calendar year increment, 95% CI 1.016 to 1.029) than men (OR 1.010, 95% CI 1.005 to 1.015) (table 2). In the most recent year, 11.2% of women underwent surgery compared with 10% of men.
Odds and 95% CIs ratio per one calendar increment for the trends over the 1998–2008 period of surgical resection among patients with non-small cell lung cancer diagnosed in England
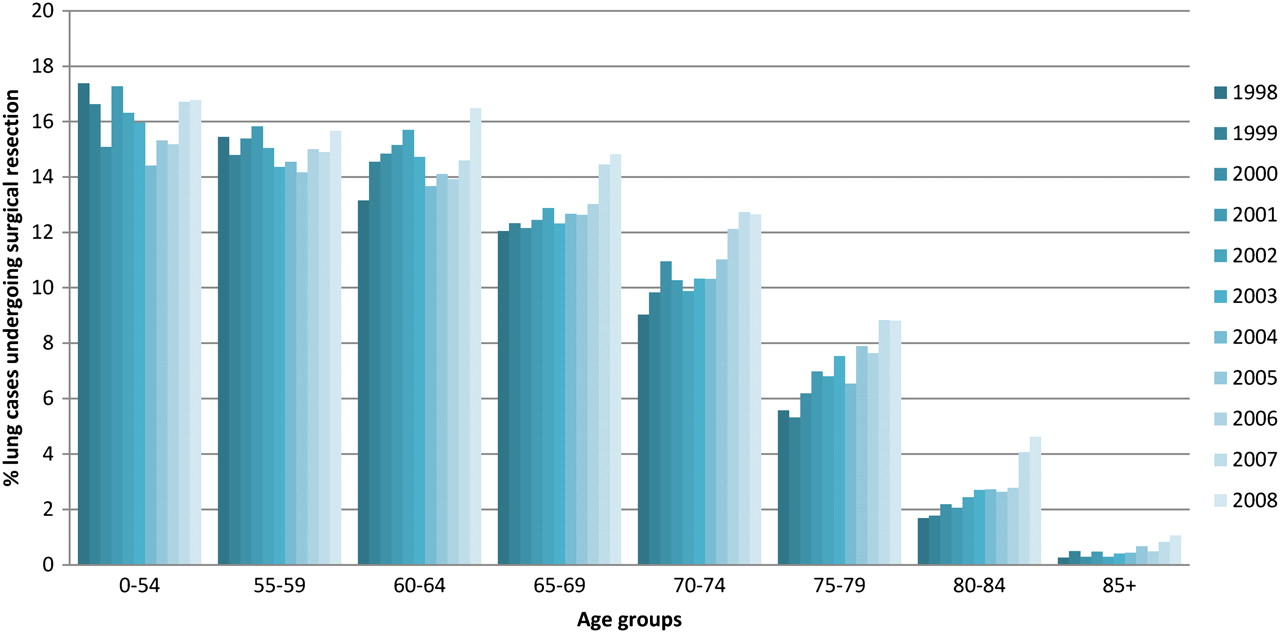
The resection rate varied by age, ranging from 16.1% in patients younger than 55 years to 0.6% in those aged 85 years and over (figure 1). Figure 1 also shows that between 1998 and 2008, the resection rate remained relatively stable up to the 60–64 year old age groups, and increased from the 65–69 to the 85+ year old age groups. The odds of undergoing surgery over the 11-year time period increased with increasing age (from OR 0.994, 95% CI 0.982 to 1.006 per 1-year increment for patients <55 years old to OR 1.130, 95% CI 1.069 to 1.193 for patients aged 85 years and over).

{kind=link}
Proportion of patients with non-small cell lung cancer undergoing surgical resection by year of diagnosis and age group, England, 1998–2008.
The increase in resection rate over time was similar in all socioeconomic deprivation quintiles. A difference remained in the proportion of patients with NSCLC undergoing a surgical resection in each group. In 2008, the resection rate was 11.6% in the most affluent group and 9.1% in the most deprived group.
With regard to the type of surgery, there was a 7.4% decrease per year in the odds of patients undergoing pneumonectomy. In contrast, the odds of undergoing sleeve resection increased at 14.9% per year. There were also small increases in the odds of undergoing wedge resection and lobectomy at 3.3% and 3.2% per year, respectively.
Increasing age was associated with a decreased likelihood of undergoing a pneumonectomy (OR 0.88, 95% CI 0.87 to 0.89 per 5-year age increment) or sleeve resection (OR 0.75, 95% CI 0.71 to 0.79) compared with lobectomy, and an increased likelihood of undergoing a wedge resection (OR 1.08, 95% CI 1.06 to 1.10). No association between age and other limited surgical resection was observed (OR 1.01, 95% CI 0.97 to 1.04).
Discussion
We observed an increase in the proportion of patients with NSCLC in England undergoing a surgical resection between 1998 and 2008, which is in accordance with previous reports.10–12
We found an increase in the proportion of patients in older age groups undergoing surgical resection. A study in Northern Ireland covering the period 1994–2008 found an increase in patients over 70 years of age undergoing surgery.15 A study in Leicestershire, England also found an increase in surgical resection among patients over 75 years of age from 1994–1996 to 1997–1999 periods.11 Since the median age of men and women with NSCLC in England remained stable throughout the studied period, it appears that older patients are increasingly being considered for surgery.
We observed a decrease in the proportion of patients undergoing a pneunomectomy in favour of an increase in lobectomies and sub-lobar resections. The decrease in the proportion of pneumonectomy in favour of lobectomy possibly reflects a better selection of patients for surgery, whereas the increase in the proportion of patients treated with sub-lobar resections may be an indication of the increased willingness to operate on patients with borderline fitness to preserve lung parenchyma.10
The increase in the odds of undergoing a surgical resection over time was particularly evident in the older age groups. However, we also found that with increasing age patients were less likely to undergo a pneumonectomy and slightly more likely to undergo a wedge resection. This indicates that increasingly older patients are considered for surgery and they are predominantly undergoing limited surgery. A large study that compared adjusted mortality among types of surgery, compared with lobectomies, limited wedge resections were associated with an increased death rate.16 The same study found that in patients over the age of 71 years, survival rates among those receiving lobectomies and limited resections were similar but low in comparison to younger patients, possibly indicating the limited survival advantage with lobectomies or wedge resections in older people, either as a function of suboptimal resection or as an association with underlying comorbidities.
Since the increase in the odds of undergoing a surgical resection was associated in particular with age, it is of interest whether this translates into better survival. The study from Leicester11 that showed an increase in the resection rate as a result of the establishment of specialist thoracic surgery showed no difference in survival between the groups before and after the increase, which they attributed to the similar stage distribution in both groups. Since that study was based on a single health authority, but made no comparison to the patients who did not undergo a surgical resection, it is not possible to draw inference on the effect on the survival of all patients with NSCLC in the area. Although many studies identify advanced age as a negative prognostic factor for hospital mortality and long-term survival, other studies have shown that acceptable operative mortality rates can be achieved in older patients (reviewed in Birim et al17). A large observational study in the USA found similar survival rates between older patients with stage I disease and their younger counterparts.18
We did not assess the effect of the observed increases in surgical resection rate on survival. In a previous study, we found that among all patients with NSCLC, higher resection rates are associated with increased survival, but also noted an association between high resection rates and a small increase in the death rate among those who had surgical resection, indicating that there may be diminishing returns from increasing the resection rate.9
The increase in surgical resection rates in England could be influenced by changes in patient characteristics, for example, patients may be presenting with earlier stage disease, less comorbidity and better performance status. We were unable to assess these parameters due to the limited availability of stage information and a lack of information on performance status. Further analysis on staging, comorbidity and performance status may improve our understanding of the possible impact on the increase in surgery. An interesting contrasting study to note in this context was carried out in the East of England, which reported a decrease in surgery between 1995 and 2006 and attributed this decrease to improved patient selection due to improved staging procedures.19 However, it is likely that the increase in the lung cancer resection rate is brought about by changes in staffing (an increase in lung cancer specialist surgeons), clinical infrastructure (multidisciplinary team meetings), access to less invasive surgical techniques and an increasing propensity to operate on patients with significant comorbidity and less-than-ideal fitness characteristics. Our observation that over time patients were less likely to undergo a pneumonectomy and more likely to undergo a sleeve resection seems to reflect this.
In conclusion, the proportion of patients with NSCLC who underwent a surgical resection increased materially from 1998 to 2008, and especially in patients in their 70s and 80s.
Acknowledgments
This paper is a contribution from the National Cancer Intelligence Network and is based on the information collected and quality assured by the regional cancer registries in England (http://www.ukacr.org; http://www.ncin.org.uk).
References
Footnotes
Linked article 202006.
Funding This work was carried out by the Thames Cancer Registry, King's College London, which receives funding from the Department of Health for England. The research was supported by the National Institute for Research (NIHR) Biomedical Research Centre based at Guy's and St Thomas' NHS Foundation Trust and King's College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.