Article Text

Abstract
Background Evidence suggests an association between HIV infection and the presence of obstructive lung disease (OLD). However, the associations between specific markers of HIV infection and OLD remain unclear. A study was undertaken to determine the independent associations of HIV infection, CD4 cell count and plasma HIV viral load with the presence of OLD in an urban cohort.
Methods Clinical, laboratory and spirometric data from the AIDS Linked to the Intravenous Experience (ALIVE) study, an observational study of current and former injection drug users in Baltimore, Maryland, were analysed. Multivariable logistic regression models were generated to identify HIV infection indices independently associated with OLD.
Results Of 1077 participants (mean±SD age 48±8 years), 89% were African-American, 65% were men and 86% were current smokers. A total of 303 (28%) were HIV infected and 176 (16%) had spirometry-defined OLD. Higher viral load was independently associated with OLD. HIV-infected individuals with viral load >200 000 copies/ml had a 3.4-fold increase in the odds of OLD compared with HIV-negative participants (95% CI 1.24 to 9.39; p=0.02). The association between higher HIV viral load and OLD persisted after accounting for antiretroviral therapy use (OR 4.06, 95% CI 1.41 to 11.7; p=0.01). No association was observed between HIV serostatus or CD4 cell count and the presence of OLD.
Conclusion In a cohort at risk for OLD and HIV infection, high viral load but not CD4 cell count was associated with an increased prevalence of spirometry-defined OLD. These findings suggest that higher viral load may contribute mechanistically to the increased risk of OLD in patients with HIV infection.
- HIV infection
- pulmonary disease
- chronic obstructive
- lung diseases
- obstructive
- asthma
- COPD mechanisms
- bronchiectasis
- COPD epidemiology
- COPD exacerbations
- COPD pathology
- COPD pharmacology
- emphysema
- ambulatory oxygen therapy
- asthma epidemiology
- lung physiology
Statistics from Altmetric.com
- HIV infection
- pulmonary disease
- chronic obstructive
- lung diseases
- obstructive
- asthma
- COPD mechanisms
- bronchiectasis
- COPD epidemiology
- COPD exacerbations
- COPD pathology
- COPD pharmacology
- emphysema
- ambulatory oxygen therapy
- asthma epidemiology
- lung physiology
Key messages
What is the key question?
What is the association between different indices of HIV infection and the presence of obstructive lung disease (OLD)?
What is the bottom line?
High viral load, but not CD4 cell count, is independently associated with an increased prevalence of spirometry-defined OLD in an urban high-risk cohort.
Why read on?
These findings suggest that the higher viral load may contribute mechanistically to the increased risk of OLD, offering insight into ways to decrease the risk of OLD in at-risk individuals with HIV.
Introduction
Obstructive lung disease (OLD), including asthma and chronic obstructive pulmonary disease (COPD), is associated with substantial morbidity and mortality in the USA.1 2 Risk factors for the development of OLD, such as tobacco use and low socioeconomic status, are prevalent in individuals at risk or infected with HIV.3 4 There has been an increased awareness of the association between HIV infection and the prevalence of COPD.5–7 Diaz and colleagues previously described an accelerated form of radiographic emphysema in HIV-infected smokers.5 Crothers and colleagues observed an increased odds of COPD diagnosed via ICD-9 diagnosis or self-report in HIV-infected individuals from a Veterans Administration (VA) cohort.6 Further analysis of this cohort demonstrated an increased risk of ICD-9 diagnosed COPD, but not asthma, in the combination antiretroviral era.8 While reports have described the prevalence and severity of airflow obstruction among HIV-infected individuals,9–11 it remains unclear which markers of HIV infection (CD4 cell count, plasma HIV viral load) are associated with spirometry-defined OLD.
The AIDS Linked to the Intravenous Experience (ALIVE) study has prospectively followed a cohort of injection drug users in Baltimore, Maryland since 1988.12 Clinical, laboratory and spirometric measurements have been collected longitudinally in this cohort at risk or with HIV infection. We have previously described the unrecognised burden of OLD and respiratory symptoms in this cohort,13 but the relationship between HIV infection and OLD was not investigated. The heavy smoking patterns and detailed information on HIV-related characteristics makes this cohort an ideal population in which to examine rigorously the relationship between HIV and OLD. In the current study we use cross-sectional and retrospective longitudinal data from the ALIVE study to determine the independent associations between HIV infection, CD4 count and plasma HIV viral load with prevalent OLD in an urban cohort with heavy tobacco use. We hypothesise that indices of more severe HIV infection will be independently associated with an increase in the odds of OLD.
Methods
Study cohort
As described previously,12 since 1988 ALIVE has followed participants aged ≥18 years, living in inner city Baltimore, Maryland and with a history of injecting drugs. At biannual visits, participants complete HIV-specific questionnaires and provide blood samples. Since 2007, participants have performed pre-bronchodilator spirometry testing at each study visit. We performed a cross-sectional analysis nested within the ongoing cohort study of all participants undergoing spirometry between 9 January 2007 and 26 June 2009. The study was approved by the Institutional Review Board of Johns Hopkins University (NA_00020295) and all participants provided written informed consent.
Data collection
Cross-sectional data was collected on or within 6 months before the first spirometry visit, including demographic, laboratory and clinical data focused on smoking behaviour and respiratory symptoms. Smoking patterns, injection drug use habits and antiretroviral use were determined by self-report. Respiratory infections were identified through self-report and confirmed through medical records. Pre-bronchodilator spirometry was performed using KoKo pneumotachs (Pulmonary Data Services, Louisville, Colorado, USA) in accordance with American Thoracic Society guidelines.14 Percentage predicted values were calculated using standard formulae.15 The post-bronchodilator response was defined according to published guidelines.16 Separate analyses were performed defining OLD using two criteria: (1) ratio of the forced expiratory volume in 1 s (FEV1) to forced vital capacity (FVC) of ≤70%17; and (2) FEV1/FVC less than the predicted lower limit of normal (LLN).15 Analyses using fixed ratio criteria are presented here while analyses using LLN criteria are presented in the online supplement. We abstracted retrospective longitudinal CD4 and viral load data from prior ALIVE visits for additional modelling of HIV indices described below.
Statistical analysis
Clinical and demographic characteristics between groups were compared using the t test for normally distributed continuous variables and the Wilcoxon rank sum test for skewed data. All data are presented as mean (SD) for normally distributed data and median (IQR) for non-normally distributed data. Categorical variables were compared with Pearson χ2 and Fisher exact tests. A p value ≤0.05 was used to infer statistical significance.
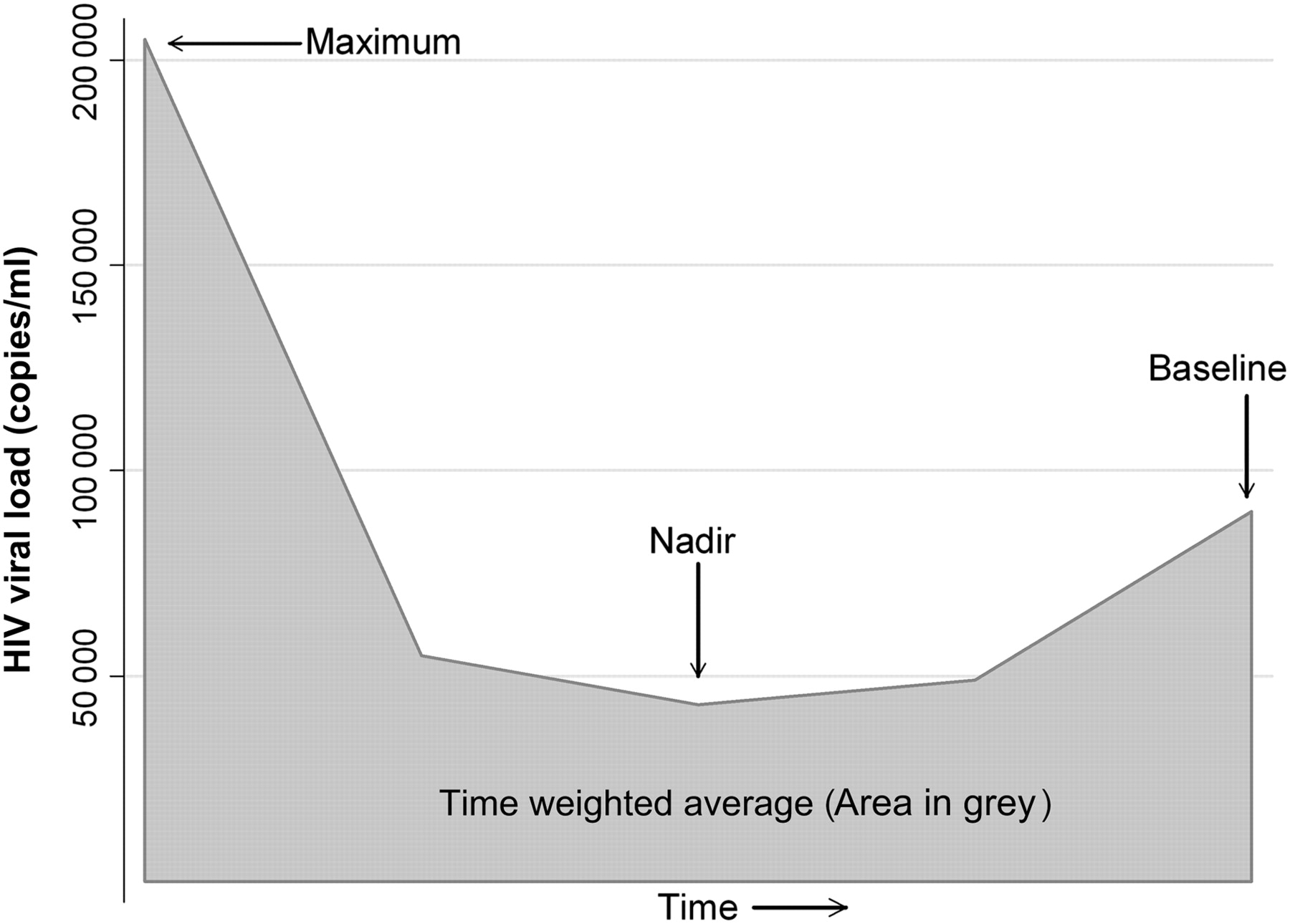
Logistic regression models were generated to explore associations between indices of HIV and the presence of OLD. The primary analysis included cross-sectional CD4 and viral load data from the 6-month window prior to the spirometry (baseline) visit. CD4 cell count was modelled continuously, dichotomously at clinically relevant thresholds (eg, 200, 350 cells/mm3) and in various increments (eg, per 50 cells/mm3, per 100 cells/mm3). HIV viral load was modelled continuously, dichotomously at different thresholds (eg, 75 000 copies/ml, 200 000 copies/ml) and categorically at clinical thresholds (<400 copies/ml vs 400–75 000 copies/ml vs >75 000 copies/ml; < or >100 000 copies/ml). Because HIV infection is a time-varying covariate, retrospective longitudinal data were used for secondary models (see figure 1). These models included nadir, maximum and time-weighted average (calculated as the area under the curve over follow-up time) CD4 count and HIV viral load. Significant relationships were then assessed with multivariable logistic regression models accounting for demographic and clinical covariates associated with OLD. Smoking history was modelled both continuously and dichotomously. Heavy smoking was defined as ≥40 pack-years, representing the 75th percentile of the cohort. Covariates were evaluated based upon relevance from clinical literature review and/or exploratory data analyses. Collinearity was assessed by measuring the variance inflation factor. Stata V.10.0 (Stata Corp) was used for statistical analysis.

{kind=link}
Idealised graph of viral load measurements. For analysis, the baseline HIV CD4 and viral load (obtained at the time of spirometry) were used. Additional measures from retrospective longitudinal data were used to determine the nadir, maximum and time-weighted average (calculated by the area under the curve in grey) over duration of follow-up.
Results
Participant characteristics
Of 1348 ALIVE participants seen during the study period, a total of 1077 participated in the lung sub-study. The median (IQR) duration of follow-up for retrospective parameters was 7.1 (0.6–9.5) years. The characteristics of the participants included in the analysis were similar to those not included, with the exception of viral load which was higher in those not included (median (IQR) 8619 (142–76 300) vs 1190 (400–30 700). Overall, the mean age of participants was 48±8 years, nearly 90% were of black race, two-thirds were men and 303 (28%) were HIV infected. Of the cohort, 86% were current smokers and 9% were former smokers. The mean FEV1/FVC ratio of the entire cohort was 0.76±0.08, with a mean FEV1 of 92±18% predicted. Spirometry-defined obstruction was present in 176 (16%) of the entire cohort, with no difference by HIV serostatus. Of these 176 participants with spirometry-defined OLD, 86 (49%) reported no physician diagnosis of OLD, 13 (7%) COPD, 47 (27%) asthma, 24 (14%) both asthma and COPD and 6 (3%) had no response. A subset of 30 participants with OLD underwent pre- and post-bronchodilator spirometry to assess for reversible airflow obstruction. Eighteen (60%) did not have an acute bronchodilator response while 12 (40%) met ATS criteria for reversibility.
A total of 51 (4.7%) had both HIV and OLD. The median CD4 cell count of HIV-infected participants was 323 cells/mm3 (IQR 179–491) with 169 (56%) using antiretroviral therapy in the previous 6 months, 143 (47%) had HIV RNA levels ≤400 copies/ml (the lower limit of assay detection) and 79 (26%) ever had a viral load >200 000 copies/ml during follow-up. Higher viral load was associated with lower CD4 cell count (viral load <400 copies/ml: 459 CD4 cells/mm3; viral load 401–200 000 copies/ml: 302 CD4 cells/mm3; viral load >200 000 copies/ml: 132 CD4 cells/mm3; p<0.01).
When stratifying by OLD status, subjects with OLD were 2 years older, had lower body mass index (BMI) and heavier smoking exposure, but no differences were observed in gender, race, drug use habits or HIV status (table 1). Even fewer differences were observed among HIV-infected participants stratified by OLD status (table 2).
Clinical and demographic characteristics of study participants
Characteristics of HIV-infected participants
Analysis of factors associated with OLD
In univariate analysis, several clinical and demographic characteristics were associated with OLD including older age, history of bacterial pneumonia, lower BMI and pack-years smoking (table 3). HIV infection status was not associated with OLD (OR 1.05, 95% CI 0.74 to 1.50; p=0.786). When modelling baseline HIV RNA levels, there was a non-significant increase in the likelihood of OLD when evaluated continuously (OR 1.26 per 100 000 copies/ml, 95% CI 0.96 to 1.65; p=0.09). There was a significantly increased odds of OLD in the highest viral load group (OR 3.30, 95% CI 1.26 to 8.69; p=0.015) (table 3). There was no association between baseline absolute CD4 count (OR 1.00 per 50 cells/mm3, 95% CI 0.94 to 1.06; p=0.96). Nadir, maximum and time-weighted averaged CD4 and HIV RNA levels were not associated with OLD (data not shown). The absolute CD8 count and CD4/CD8 ratio were not associated with OLD. There was no association between hepatitis C virus (HCV) serostatus and OLD (OR 1.08, 95% CI 0.30 to 3.87; p=0.90).
Characteristics associated with OLD in entire cohort
After accounting for relevant characteristics identified in univariate analysis, the observed association between higher baseline HIV viral load and OLD persisted (table 3). Compared with HIV-negative participants, HIV-infected individuals with viral load >200 000 copies/ml had a 3.4-fold increase in the odds of OLD (OR 3.41, 95% CI 1.24 to 9.39; p=0.02). Other indices of HIV infection were not associated with an increased odds of OLD in separate models including HIV infection (OR 0.96, 95% CI 0.65 to 1.42; p=0.84) or baseline CD4 cell count <200 cell/mm3 (OR 1.08, 95% CI 0.57 to 2.04). Nadir, maximum and time-weighted average CD4 and HIV viral load levels were not associated with OLD. Selecting the 131 participants with longest follow-up time, we observed a non-significant increase in the odds of OLD in the highest quartile of time-weighted average HIV viral load (OR 1.81, 95% CI 0.61 to 5.33). Neither exclusion of BMI, incorporating markers of socioeconomic status (high school education, employment in the last 6 months), inclusion of CD4 or CD8 measurements, HCV serostatus nor modelling different types and durations of drug use altered the association between HIV viral load and OLD.
Several demographic characteristics remained strong independent factors associated with OLD. Each 10-year increase in age was associated with an approximately 40% increase in the odds of OLD (OR 1.38, 95% CI 1.08 to 1.76; p=0.01). Black race and highest BMI category were both associated with a reduced odds of OLD (OR 0.43, 95% CI 0.25 to 0.72, p=0.002 and OR 0.50, 95% CI 0.29 to 0.85, p=0.01, respectively). Both a history of heavy smoking and a history of bacterial pneumonia were independently associated with the presence of OLD. The smoking effect was present when smoking was modelled categorically (≥40 vs <40 pack-years) or continuously (per 10 pack-years). Similarly, the association between pneumonia and OLD was present when pneumonia was modelled in a categorical (<1, ≥1) or continuous (0, 1, 2, 3) manner.
To determine the impact of antiretroviral therapy on the association between HIV and OLD, we separately evaluated 303 HIV-infected participants (table 4). Participants with a viral load >200 000 copies/ml had a fourfold higher likelihood of OLD than those with a viral load ≤200 000 copies/ml (OR 4.06, 95% CI 1.41 to 11.7; p=0.01). As observed in the total cohort, black race was associated with lower odds of OLD. Inclusion of CD4 or CD8 measures did not alter the association between HIV viral load and OLD among HIV-infected individuals.
Characteristics associated with OLD among HIV-infected participants only
When defining OLD with LLN criteria rather than a fixed ratio definition, nine additional participants met the criteria for OLD. Multivariate models using LLN criteria attenuated the age and race effects in the overall cohort and the race effect in the HIV-only analysis. However, using LLN criteria did not alter the associations between higher HIV viral load and OLD (see tables 1 and 2 in online supplement).
Discussion
In this study of more than 1000 current and former injection drug users with nearly ubiquitous smoking exposure, we found that high HIV viral load, but not CD4 cell count, was independently associated with an increased odds of spirometry-defined OLD. Specifically, viral load exceeding 200 000 copies/ml increased the odds of OLD more than threefold. After accounting for antiretroviral use among HIV-infected participants, high viral load remained independently associated with a fourfold increase in the odds of OLD.
Our observations of the relationship between higher HIV viral load and OLD expand the current understanding of the interaction between HIV infection and the development of OLD. To our knowledge, this is the first report to describe a viral load threshold at which the likelihood of spirometry-defined OLD was increased. Previous studies have described the association between HIV seropositivity and radiographic emphysema or ICD-9/self-reported OLD, but not an association with viral load.5 6 Our analysis revealed similar risk estimates for other predictors of OLD (age, race, bacterial pneumonia, use of antiretroviral therapy) in the VA study. In contrast to the VA cohort, ALIVE represents a community-based cohort with more limited use of antiretroviral therapy and more heterogeneous disease severity not easily captured by HIV serostatus. Our contrasting observations may also be related to differing characteristics of the study populations (male and female injection drug users vs male veterans) and the definition of OLD (spirometry-based vs ICD-9/self-report). The lack of an association between longitudinal measures of viral load may reflect challenges in modelling viral exposure in a cohort with heterogeneous disease severity and differential follow-up.
Despite an association between HIV viral load levels and CD4 cell count, we did not observe an association between CD4 levels and OLD, although our study may have been underpowered to detect such a relationship. In the VA study, increasing CD4 cell count and lower odds of OLD was of borderline significance with ICD-9 diagnosis but was not present when OLD was diagnosed via self-report. Although an association between use of antiretroviral therapy and the presence10 and severity9 of airflow obstruction has been described, we did not observe similar effects in our analysis.
Several potential biological mechanisms may explain the association between high HIV viral load and increased odds of OLD. Plasma HIV RNA levels are independently correlated with the percentage and activation of CD8 T cells as well as with progression of HIV infection.18 19 HIV-infected smokers with radiographic emphysema have an increased percentage of cytotoxic CD8 lymphocytes compared with HIV-infected smokers without emphysema and HIV-negative smokers.5 CD8 alveolitis is also correlated with the presence and severity of airflow obstruction in smokers with OLD.20 Although we did not observe an association between peripheral CD8 lymphocyte levels and OLD, the correlation between peripheral and lung CD8 levels has not been extensively examined in the literature. Twigg and colleagues observed a strong correlation between serum viral load, bronchoalveolar lavage viral load and CD8 alveolitis.21 The most robust CD8 alveolitis was seen in participants with CD4 cell counts ranging from 200 to 500, suggesting that HIV virus may be acting independently of immune suppression. Moreover, in lung autopsy studies of HIV-infected individuals, areas of histological emphysema have greater numbers of HIV-infected cells than normal lung.22 Finally, HIV-infected individuals have increased levels of inflammatory cytokines which have been implicated in the pathogenesis of COPD.23–26 Taken together, these data suggest that uncontrolled HIV infection with elevated viral load may increase susceptibility to OLD. Our cross-sectional study cannot determine a causal relationship between higher HIV RNA levels and OLD. There could also be an effect of OLD in increasing CD8 T cell activation27 28 and thereby secondarily increasing HIV RNA levels. Irrespective of the direction, this association with a plausible biological mechanism could have substantial clinical implications for HIV-infected persons with OLD.
It is possible that the observed association between higher plasma viral load and OLD represents behavioural rather than biological effects. Individuals with a high viral load in the effective antiretroviral era may represent persons less likely to seek medical care or more likely to engage in higher-risk behaviours which could potentially increase the odds for developing OLD. We adjusted for several measured variables (eg, income, educational level, illicit drug behaviour) that could generate this bias and observed no impact on the observed associations. However, unmeasured confounders, which we are unable to account for, may still potentially exist.
In addition to the association between elevated HIV viral load and OLD, we also observed several negative associations between covariates and OLD. Compared with BMI <21 kg/m2, BMI >27 kg/m2 was associated with a 50% reduction in the odds of OLD. Low BMI is a known risk factor for COPD as well as a marker of poor prognosis in COPD.29 30 While BMI <18 kg/m2 may be a marker of advanced HIV infection or intense drug use in our cohort, we did not observe collinearity between BMI and high viral load. Moreover, excluding BMI from our multivariate models did not affect the relationship between high viral load and OLD. Despite a lack of association in univariate analysis, we observed a strong protective effect of black race on the presence of OLD in multivariate analysis. This effect is consistent with the earlier VA study.6 Although reports have described an association between HCV and OLD,31–33 we found no association in our cohort with a high HCV prevalence. HCV is a strong surrogate marker for a history of injection drug use, and studies which do not fully account for behavioural differences (eg, smoking) among injection drug users compared with other HIV risk groups may incorrectly associate HCV with OLD.
Besides the cross-sectional nature of our analysis, our study has other limitations. We are unable to fully determine airflow reversibility; a sample with pre-/post-bronchodilator spirometry suggests a mix of reversible and fixed airflow obstruction is present. Nonetheless, use of spirometric criteria to define OLD extends prior self-reported and administrative diagnoses of HIV-associated lung diseases. Participants not included in the lung sub-study had a statistically higher viral load than those included in the analysis. If the prevalence of OLD in those not included is also different, our estimate of the association between OLD and viral load may be biased. The differential follow-up time in this cohort makes accurate estimates of longitudinal viral load exposure difficult. Our population of urban injection drug users may limit the generalisability of our findings, although this homogeneity may decrease the likelihood that unmeasured exposures confound the association between higher viral load and OLD.
In summary, we have observed a strong independent association between high plasma HIV viral load and the presence of OLD among current and former drug users with a heavy burden of smoking. In addition to biological plausibility, this association was robustly observed with numerous subgroup and sensitivity analyses. These findings suggest that the higher viral load associated with uncontrolled HIV infection may contribute mechanistically to the increased risk of OLD reported in previous studies.
Acknowledgments
The authors acknowledge the contributions of the study participants and of the ALIVE and SHIELD study staff.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding This study was funded in part by grants from the National Institutes of Health (Grants HL090483, DA04334 and DA12568). MBD by a grant from the National Institutes of Health National Heart, Lung and Blood Institute (K23HL103192).
Competing interests None.
Ethics approval Johns Hopkins Hospital Institutional Review Board (Approval NA_00020295).
Provenance and peer review Not commissioned; externally peer reviewed.