Article Text

Abstract
Background The effects of low-dose CT screening on disease stage shift, mortality and overdiagnosis are unclear. Lung cancer findings and mortality rates are reported at the end of screening in the Danish Lung Cancer Screening Trial.
Methods 4104 men and women, healthy heavy smokers/former smokers were randomised to five annual low-dose CT screenings or no screening. Two experienced chest radiologists read all CT scans and registered the location, size and morphology of nodules. Nodules between 5 and 15 mm without benign characteristics were rescanned after 3 months. Growing nodules (>25% volume increase and/or volume doubling time<400 days) and nodules >15 mm were referred for diagnostic workup. In the control group, lung cancers were diagnosed and treated outside the study by the usual clinical practice.
Results Participation rates were high in both groups (screening: 95.5%; control: 93.0%; p<0.001). Lung cancer detection rate was 0.83% at baseline and mean annual detection rate was 0.67% at incidence rounds (p=0.535). More lung cancers were diagnosed in the screening group (69 vs 24, p<0.001), and more were low stage (48 vs 21 stage I–IIB non-small cell lung cancer (NSCLC) and limited stage small cell lung cancer (SCLC), p=0.002), whereas frequencies of high-stage lung cancer were the same (21 vs 16 stage IIIA–IV NSCLC and extensive stage SCLC, p=0.509). At the end of screening, 61 patients died in the screening group and 42 in the control group (p=0.059). 15 and 11 died of lung cancer, respectively (p=0.428).
Conclusion CT screening for lung cancer brings forward early disease, and at this point no stage shift or reduction in mortality was observed. More lung cancers were diagnosed in the screening group, indicating some degree of overdiagnosis and need for longer follow-up.
- Lung neoplasms
- mass screening
- randomised controlled trial
- mortality
- overdiagnosis
- bronchoscopy
- clinical epidemiology
- imaging/CT MRI
- lung cancer
- non-small cell lung cancer
- small cell lung cancer
- alpha1 antitrypsin deficiency
- inhaler devices
- pulmonary embolism
- clinical epidemiology
- lung cancer
- tobacco and the lung
- lung proteases
Statistics from Altmetric.com
- Lung neoplasms
- mass screening
- randomised controlled trial
- mortality
- overdiagnosis
- bronchoscopy
- clinical epidemiology
- imaging/CT MRI
- lung cancer
- non-small cell lung cancer
- small cell lung cancer
- alpha1 antitrypsin deficiency
- inhaler devices
- pulmonary embolism
- clinical epidemiology
- lung cancer
- tobacco and the lung
- lung proteases
Key messages
What is the key question?
To report lung cancer findings, disease stage shift, mortality rates at the end of screening in the Danish Lung Cancer Screening Trial.
What is the bottom line?
With screening, low-stage lung cancers are diagnosed more frequently but at this point no stage shift is observed and pooling of mortality data with European screening trials is needed.
Why read on?
The importance of stage shift in a screening setting and overdiagnosis is discussed from the results presented.
Introduction
In general, the purpose of screening for cancer is detecting the disease at a curable stage. Previous lung cancer screening studies have found a high frequency of early stage cancer compared with patients with symptomatic lung cancer.1–4 However, a high frequency of early stage cancers is not advantageous in itself. Experiences from other cancer screening programmes have indicated that incidence rate of early disease increased substantially with screening, while reduction in number of advanced cancers was negligible. This meant a decrease in relative proportion (relative stage shift) of advanced cancers but not in absolute numbers (absolute stage shift).5–7 A high frequency of early stage cancers is only beneficial if at the same time the frequency of late stage cancers is reduced, implying a reduction in mortality. Alternatively, a high frequency of early stage cancer may be due to ‘over-diagnosis’, that is, cancer that never would have progressed to clinical disease during a person's lifetime, and thus would not have been diagnosed without screening. Overdiagnosis is potentially harmful because it may imply unnecessary investigations and treatment. At present it is not clear to what extent the high frequencies of early stage lung cancer in screening trials are due to overdiagnosis and the degree to which they indicate a beneficial stage shift and reduced mortality.
In this paper, we report the lung cancer findings after five annual screening rounds in the randomised Danish Lung Cancer Screening Trial (DLCST). This includes the prevalence of lung nodules, stage and histology of lung cancers. We also report lung cancer specific mortality and all-cause mortality at the end of the 4-year screening period.
Material and methods
Study population
The overall design and baseline results of DLCST have previously been published.8 9
DLCST is a 5-year prospective randomised controlled screening trial. From October 2004 to March 2006, 4104 men and women were enrolled after written informed consent was acquired. They all volunteered after reading advertisements in local and regional free newspapers. Ads contained information about general study design, enrolment criteria and governmental funding.
We included men and women aged 50–70 years, who were current or former smokers with at least 20 pack years of smoking history. Former smokers should have quit after the age of 50 years and be abstinent for <10 years. Participants had to be able to climb two flights of stairs (36 steps) without pausing. Lung function was measured by spirometry and forced expiratory volume in the first second had to be at least 30% of predicted.
Exclusion criteria were weight over 130 kg, history of cancer diagnosis and treatment, lung tuberculosis, illness that would shorten life expectancy to <10 years and chest CT received during the last year for any reason.
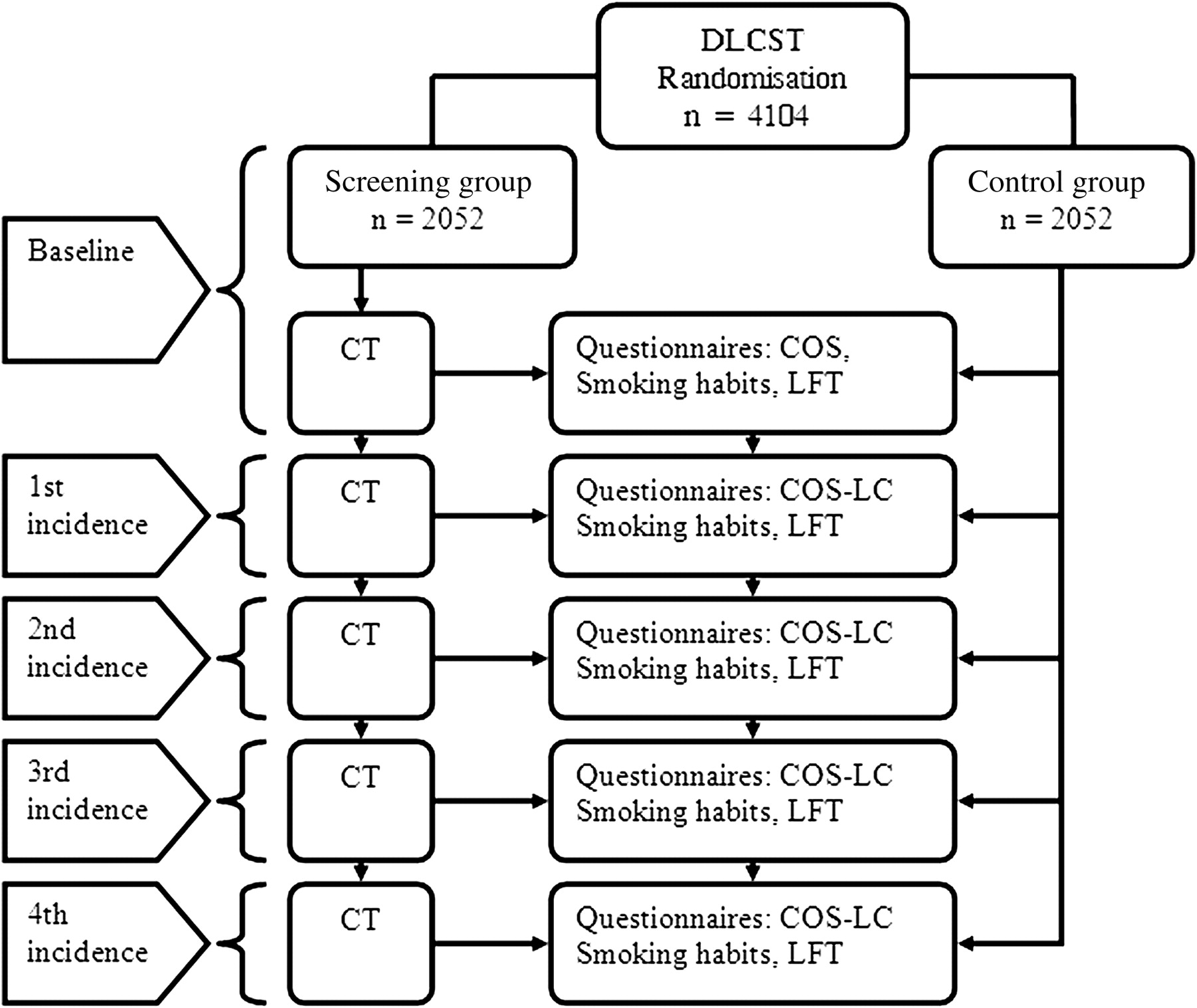
After inclusion, the participants were randomised to the screening group (n=2052) or the control group (n=2052). The screening group received five annual low-dose chest CT scans (one baseline scan and four subsequent incidence scans). All participants had an annual visit at the screening clinic, where lung function tests were performed, and questionnaires concerning health, lifestyle, smoking habits and psychosocial consequences of screening were completed.10–12 Figure 1 shows an overview of the DLCST design.

Imaging and image review
Scanning procedures have been described previously.8 Two experienced chest radiologists (KB and HH) read all CT scans and registered the location, size and morphology of nodules. Scans with no nodules or nodules <5 mm (category 2) or nodules up to 15 mm in diameter with benign characteristics (category 1) were screening test negative. Participants with nodules with a diameter between 5 and 15 mm without benign characteristics (category 3) were rescanned after 3 months. Participants with nodules larger than 15 mm (category 4) or rapid growing nodules (>25% increase in volume) (category 5) were referred to chest physicians for diagnostic workup. Siemens syngo LungCARE CT version VE25A, a commercial computer-aided detection software, was used to measure nodule volumes when possible, and volume doubling time (VDT) was used to measure growth rate and was considered a supplement in decision making. Rapid growth (VDT <400 days) increased the suspicion of malignancy, whereas slow growth (VDT >400 days) decreased suspicion. The same software was used in the Dutch-Belgian screening trial (NELSON)13 and was validated in a double reading project.14
Findings were discussed at weekly consultations with participation of radiologists (KSB, HH), pulmonologists (AD, PFC) and a chest surgeon (JHP), and decisions were recorded in the project database.
Diagnostic workup
Participants with positive screening findings who needed further diagnostic workup were referred to chest physicians in two specialised lung cancer diagnostic centres at Gentofte University Hospital and Bispebjerg University Hospital in Copenhagen. An individual diagnostic strategy based on the characteristics of the radiological findings was followed with the possibility of CT with intravenous contrast, 18F-fluorodeoxyglucose-positron-emission-tomography-CT (PET-CT), bronchoscopy with biopsies, endobronchial ultrasound and endo-oesophageal ultrasound, CT-guided transthoracic biopsy and mediastinoscopy. If necessary, video-assisted thoracoscopic surgery was performed to obtain a final diagnosis and definitive treatment was sometimes performed in the same procedure. This was in accordance with European guidelines. Final staging of disease was made according to the cytology/histology of the cancers (pTNM) and the recommendations from the International Association for the Study of Lung Cancer (IASLC) seventh edition.15 Pathology was performed by BGS according to the EU-US pathology panel guidelines for screening detected lung tumours and subsequently confirmed by the panel.8
In the control group, lung cancers were diagnosed and treated outside the study by the usual clinical practice, which mostly involved the same lung cancer diagnostic centres and the same diagnostic and treatment strategy as for the screening group.
Follow-up
Both randomisation groups were followed annually at study visits, where information on imaging, history of diagnostic workup and treatment was gathered. Annual inquiries to the Danish Lung Cancer Register were made, and lung cancer data were included in the database. Subsequently relevant medical journals were retrieved from diagnosing and treating departments.
Mortality information was obtained annually from the Danish Civil Registration System, which contains information on all national deaths with a delay of a couple of weeks. Cause of death information was extracted from the Danish Causes of Death Register, which has a lag time in registry update of up to 2 years. Therefore, in addition to the registry inquiries, the medical history of the deceased was obtained, if possible, from general practitioners, medical records of hospitals, autopsy reports, police departments and the National Board of Health. The cause of death was established by a local death review board and categorised as ‘lung cancer’ or ‘other causes’ of death.
In this paper, the latest follow-up for both groups was set as end of screening, 31 March 2010. Participants who emigrated from Denmark were lost to follow-up.
Data analysis
χ2 test was used to compare frequencies of disease and participation rates between the screening and control group. Two sample t test was used to test the null hypothesis comparing means of follow-up years in the two groups. The log-rank test and Kaplan–Meier plot were used to assess mortality rates. We used a 95% CI and p values below 0.05 were considered statistically significant.
Power calculation was made assuming pooling of mortality data with the NELSON study. Assuming a 1:1 randomisation, a power of 80%, significance level of 5%, an annual incidence of lung cancer of 0.5%, a difference in 5-year mortality between screened and non-screened participants of at least 20%, 95% compliance in the screen group, 5% contamination in the control group, and 10 years of follow-up after randomisation, the required sample size was calculated as 2×2000 participants.
R statistical software version 2.12.1 was used as the statistical tool.
Ethical and legal approval
DLCST was approved by the Ethics Committee of Copenhagen County and the Danish Data Protection Agency, and registered in Clinical Trials.gov Protocol Registration System (identification no. NCT00496977).
Results
Participation
The baseline characteristics of all participants have been previously published.8 No statistical difference in age, gender, lung function, smoking status and pack-years was found in the two randomisation groups. The last screening scan was performed in March 2010.
The mean annual participation rate in the screening group was 95.5% (2047+1976+1944+1982+1851=9800)/(2052×5), and in the control group the mean rate of participation in the annual study visits was 93.0% (2052+1953+1877+1838+1820=9540)/(2052×5).
The difference in participation rate between the two groups was significant in second and third incidence rounds (χ2 test: p<0.001). No significant difference was found at baseline, and the first and fourth incidence rounds (χ2 test: p=0.073; 0.089; 0.127).
Total person-years of follow-up at last screening were 9769 person-years in the screening group; median 4.81, mean 4.76 (95% CI 3.64 to 5.88) and 9794 person-years in the control group, median 4.81, mean 4.77 (95% CI 3.73 to 5.82). No difference was seen between the groups (two sample t test; p=0.479) Twenty-nine participants were lost to follow-up due to emigration. Fifteen were in the screening group, and all screened negative at their last CT scan.
Radiological findings and management of nodules in the CT arm
During five screening rounds, 1029 (560 baseline + 469 incidence) non-calcified nodules (category 2–4) were registered 1404 times in 611 participants. Table 1 shows the categories of nodules detected during the five screening rounds in relation to the number of persons screened. Compared with baseline, the frequency of category 2–4 nodules was considerably lower during the incidence rounds (χ2 test: p<0.001).
Detection of non-calcified nodules during five annual screening rounds in 611 participants in the Danish Lung Cancer Screening Trial
At baseline recall rate for follow-up scan was 7.6% (155/2047). During the following years the rates were 20 (1.0%), 24 (1.2%), 18 (0.9%) and 24 (1.3%). A total of 198 of 9800 (2.02%) participants were referred for diagnostic evaluation by pulmonologists. Seven participants of 9800 (0.07%) had a diagnostic video-assisted thoracoscopic surgery procedure for benign disease. We plan to publish the types and extent of procedures and the economic costs separately. The diagnostic false positive rate at baseline was 7.9%,8 but at subsequent screening rounds the rates were 34 (1.7%), 39 (2.0%), 32 (1.6%), 35 (1.9%).
Lung cancers
The disease stages for both randomisation groups are presented in table 2. The baseline cancers have previously been reported8 and are updated according to IASLC classification recommendations.15
Disease stages in the Danish Lung Cancer Screening Trial after five annual CT scans and study visits
Screening group
A total of 69 lung cancers were diagnosed. The overall detection rate (baseline + incidence rounds) was 0.70% (69 of 9800). At baseline the detection rate was 0.83%, while the incidence rounds had a mean annual detection rate of 0.67% (χ2 test; p=0.535). Three were small cell lung cancers (SCLCs) and 66 were non-small cell lung cancers (NSCLCs). Forty-eight (70%) were early stage (I–IIB NSCLC and limited stage SCLC) and thus potentially curable. Twenty-two (30%) were diagnosed in late stage (IIIA–IV NSCLC and extensive stage SCLC). Fifty-eight (85%) of the lung cancers were pathologically verified within a year from the CT scan when they were first detected.
One interval cancer was diagnosed 10 months after the third incidence scan when a 65-year-old man complained of hip pain, and he was admitted to the hospital where chest CT and skin biopsy showed disseminated adenocarcinoma originating from the lungs (CK7, TTF-1, CDX2 positive; CK5/6, CK20, PSA negative). He received palliative chemotherapy and radiation and died a month later. Even in retrospect, no primary focus could be identified in the lungs by visual inspection of the four previous screening scans.
Control group
Twenty-four participants were diagnosed with lung cancer. Six had extensive stage SCLC and one limited stage. Eight (33%) were in early stage and 16 (67%) in late stage. One of the participants with an early stage lung cancer had received a CT scan for screening purposes via the general practitioner (contamination). A stage IA lung cancer was found and was treated by surgery.
Significantly more lung cancers were diagnosed in the screening group (χ2 test: 69 vs 24; p<0.001) and more were low stage (χ2 test: 48 vs 21; p=0.002). The number of late stage lung cancers was the same in both groups (χ2 test: 21 vs 16; p=0.509). The absolute and relative stage distributions are shown in figure 2.

Overview of relative and absolute distribution of lung cancer stage.
The number of new lung cancers remained consistently high during all four incidence rounds in the screened group compared with the control group: 11+13+12+16 vs 4+6+7+6 (χ2 test p=0.001). Although the number of SCLCs was low in both groups (three vs seven), there was a tendency towards more advanced disease in the control group.
The majority of lung cancers in both study arms were adenocarcinomas. The histology distribution of lung cancers in the screening and control group is shown in table 3.
Histology of lung cancers in the Danish Lung Cancer Screening Trial
Mortality
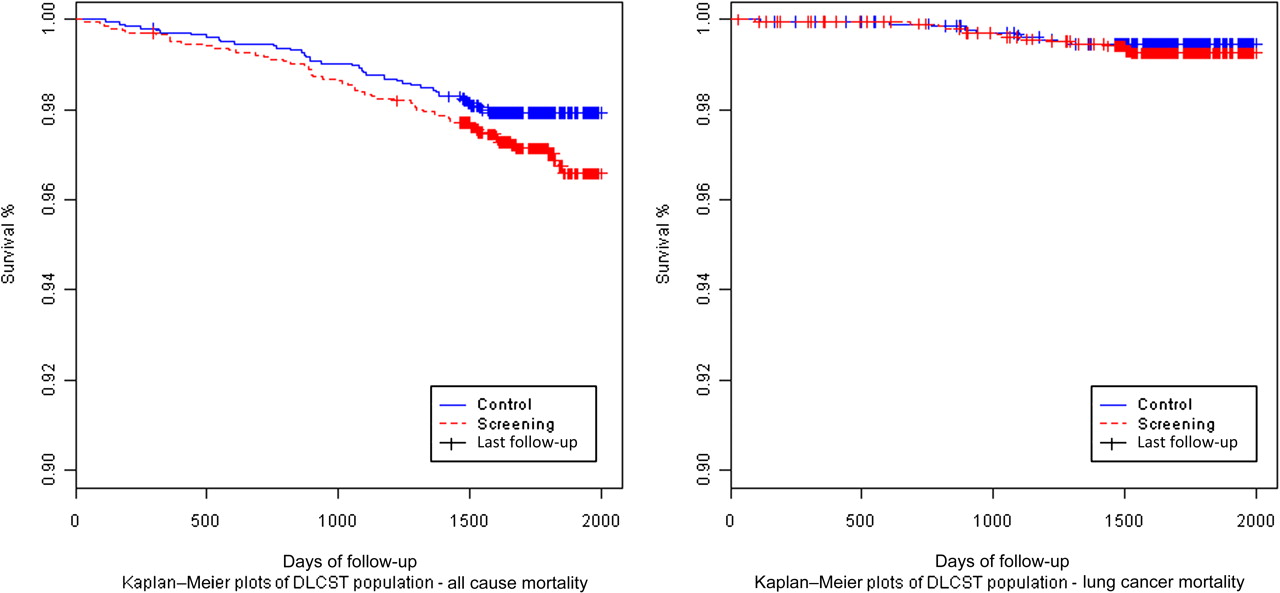
According to the Danish Civil Registration system, at the end of screening on 31 March 2010, 103 of 4104 participants had died. Sixty-one (2.97%) died in the screening group, while 42 (2.05%) died in the control group (log-rank test, all-cause mortality: p=0.059). Fifteen (0.73%) died of lung cancer in the screening group compared with 11 (0.54%) in the control group (log-rank test, lung cancer specific mortality: p=0.428). Thus, no differences in mortality were found. Figure 3 shows Kaplan–Meier plots of lung cancer and all-cause mortality.
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier plots of lung cancer and all-cause mortality. DLCST, Danish Lung Cancer Screening Trial.
Discussion
Lung cancer is by far the most lethal cancer type in the world with approximately 1.4 million deaths in 2008 according to WHO.16 Several efforts have been made to reduce lung cancer mortality. Prevention of risk factors, increased public awareness of symptoms, and early detection and treatment seem to be the cornerstones in the strategy against continuous high mortality.
Lung cancer screening may be a valuable tool in this strategy. However, psycho-social consequences, overdiagnosis, potentially harmful procedures and overtreatment are important drawbacks.
In this paper, we have reported the findings after five annual CT screenings in the DLCST. Participation rates were high in both groups throughout the trial. The rates are lower in the control group, which is probably due to disappointment of not getting screened. Despite this, the extent of contamination, defined as screening in the control group, was very limited in DLCST.9
The low recall and false positive rates observed in this study are comparable with those observed in the NELSON trial.13 This indicates that the very high recall rates observed in the National Lung Screening Trial (NLST) trial17 may be reduced and thereby one of the main obstacles to the implementation of CT screening may be overcome.
The number of early stage lung cancers was six times higher in the screening group compared with the control group. Early stage cancers were defined as stage I–IIB and were potentially curable with surgery alone or with adjuvant chemotherapy. The relative proportion of late stage cancers in the screening group was considerably lower than in the control group. However, no significant difference was seen in the absolute numbers of late stage cancers in both groups.
This suggests the absence of an absolute stage shift, and the excess proportion of early stage cancers (37%) may indicate some degree of overdiagnosis. Assuming that lung cancer arises with the same frequency in both groups after baseline, the consistently larger numbers of new cancers in the screening group at incidence rounds compared with the control group may indicate a considerable degree of overdiagnosis or a longer lead time until clinical diagnosis in the control group is made and registered. However, some of this overdiagnosis may be due to lag in registration. Information on lung cancer in the control group is not as up to date as in the screening group. Late onset of symptoms and diagnosis may be apparent during the following years and lead to a higher number of late stage cancers in the control group. Therefore, follow-up after several years may change the stage distribution, indicating an absolute stage shift and a subsequent increase in mortality, and also further clarify the extent of overdiagnosis.
Recently, colleagues from the NLST18 published their results and found a 20% lung cancer mortality reduction and 7% reduction in all-cause mortality.17 The NLST randomised 53 454 participants and compared low-dose chest CT with chest radiography. The screening began in 2002 and completed in 2006.
After five screening rounds, the mortality data in the DLCST showed no difference in lung cancer or all-cause mortality. This is explained by the small sample size and shorter follow-up time. However, we expect that a possible screening effect on mortality may be apparent during the next 4–5 years when the follow-up time will be approximately the same as in NLST. If screening reduces mortality, one should expect that the screened participants will eventually have fewer incurable high-stage lung cancers than the non-screened population. According to IASLC, survival data for high-stage lung cancers (pathologic stage IIIB–IV) show a median survival time of 13–17 months.15 Thus, in principle, a stage shift should precede mortality reduction with 1–2 years only. However, as lung cancer growth may show great heterogeneity, lead time may be much longer and perhaps even up to 4–5 years.19
To gain more statistical power, efforts are being made to pool all mortality data in the European randomised trials.2 13 20 These efforts are challenging due to differences in study design and time span. However, it is our hope that within the next decade, data from DLCST together with data from other randomised European trials will substantially improve our knowledge on potential harms and benefits of lung cancer screening with low-dose CT.
References
Footnotes
See Editorial, p 283
Funding This study was supported by the Danish Ministry of Interior and Health.
Competing interests None.
Ethics approval Ethics approval was provided by Committee of Copenhagen County and the Danish Data Protection Agency.
Provenance and peer review Not commissioned; externally peer reviewed.