Article Text

Abstract
Rationale High resolution computed tomography (HRCT) is a more sensitive tool for detecting early cystic fibrosis (CF) lung disease than either spirometry or plain radiography, but its relationship to other measures of lung function has not been established in young children.
Objectives 1) To assess whether the lung clearance index (LCI) derived from multiple breath inert-gas washout (MBW) is as effective as HRCT in identifying pulmonary abnormalities; and 2) explore the relationships between abnormalities detected by HRCT and by spirometry, plethysmography and MBW (collectively, LFTs) in young children with CF.
Methods Children with CF underwent LFTs and volumetric HRCT on the same day. Healthy age-matched controls underwent identical LFTs without HRCT. Scans were anonymised, and scored using the Brody-II CT scoring system, to assess for presence and extent of bronchiectasis, airway wall thickening, mucus plugging, and parenchymal opacities.
Results Assessments were undertaken in 60 children with CF (mean (SD) 7.8 (1.3) years) and 54 healthy controls (7.9 (1.2) y). Among children with CF, 84% (47/56) had abnormal LCI, 58% (27/47) abnormal plethysmographic lung volumes (FRCpleth or RV), 35% (21/60) abnormal sRaw and 47% (28/60) abnormal spirometry (FEV1 or FEF25–75); whereas HRCT scans were abnormal in 85% (51/60): median total Brody-II score: 9.5% (range 0–51%). Total CT score correlated more strongly with LCI (Spearman correlation=0.77) than with spirometry (R=−0.43) or any other marker of lung function. Of the nine children with normal LCI, five had abnormalities on HRCT, whereas five children with normal HRCT had raised LCI.
Conclusions These results suggest that while LCI and HRCT have similar sensitivity to detect CF lung disease, complimentary information may be gained in individual patients.
- Pulmonary function tests
- child
- lung imaging
- CT
- cf
- multiple breath wash out
- cystics fibrosis
- imaging/CT MRI
Statistics from Altmetric.com
Key messages
What is the key question?
Is Lung Clearance index more sensitive than CT at detecting CF lung disease in young children?
What is the bottom line?
Both modalities are frequently abnormal in this age group with similar sensitivity, such that a normal LCI means that CT abnormalities are unlikely.
Why read on?
You will learn about the role of LCI as a novel sensitive means of detecting early airway disease in children with CF.
Introduction
Increasing emphasis on the importance of early detection and treatment of lung disease in young children with cystic fibrosis (CF) has created an urgent need for sensitive markers of early lung changes.1 High resolution computed tomography (HRCT) is known to be a sensitive means of detecting early lung disease in CF, demonstrating abnormalities prior to the development of clinical and spirometric abnormalities.2 3 HRCT has therefore been proposed as an important tool for the detection and monitoring of early lung disease in CF,4 5 with some authors proposing its use as a routine investigation.6 However, HRCT involves a significant delivered dose of ionising radiation7 and its routine use has therefore been questioned.8–10 The lung clearance index (LCI) is a non-invasive measure of ventilation inhomogeneity derived from multiple breath inert gas washout (MBW), which has been shown to be a far more sensitive measure of abnormal function in CF than spirometry.11–16 Retrospective analysis of clinical data in older children and adults has suggested that LCI may provide an alternative safer measure than HRCT for detecting early pulmonary abnormalities in CF, and indeed that LCI may be more sensitive than HRCT.17 The authors now report the first prospective study comparing simultaneous measurements of lung function using MBW, plethysmography and spirometry with volumetric HRCT in young children with CF. The authors hypothesised that LCI would detect relatively mild lung changes in CF as frequently as HRCT and be superior to other measurements of pulmonary function.
The primary aim of this study was to assess whether the LCI is as effective as volumetric HRCT in identifying pulmonary abnormalities in young children with CF. The secondary aim was to explore the relationships between the nature and severity of changes found on HRCT and functional abnormalities detected by spirometry, plethysmography and MBW.
Methods
Recruitment
Children with CF previously recruited to the London Cystic Fibrosis Collaborative Study (LCFC), together with healthy age-matched controls, were eligible for this study if aged between six and 10 years. Full details of recruitment, and inclusion and exclusion criteria have been reported previously,13 18 19 and are summarised in the online supplement (OLS). The study was approved by the Research Ethics Committee of UCL, Institute of Child Health and Great Ormond Street Hospital. Full informed written consent was obtained from the parents or guardians of the children, and the child's assent was also obtained.
Test procedure
All lung function measurements were performed in the paediatric respiratory laboratory at UCL, Institute of Child Health when all children had been free of acute respiratory infections for at least three weeks, and those with CF were clinically stable (at least 2 weeks since last exacerbation). Children with CF had their usual airway clearance therapy on the morning before assessments. All parents first answered a questionnaire about their child's recent symptoms, and the child underwent a physical examination. The parental questionnaire for children with CF was supplemented with additional information provided by the child's clinician. The authors recorded presence of cough in the week prior to testing, the number of additional courses of oral and intravenous antibiotics administered for increased respiratory symptoms in the preceding 12 months, and presence of wheeze or crackles on clinical examination at time of test.
Lung function
All children performed MBW, spirometry and plethysmography according to the standard laboratory protocols which adhere closely to ATS/ERS recommendations (see OLS for details). Four per cent sulphur hexafluoride via a bias flow apparatus was used as the tracer gas for MBW, these measurements being performed prior to spirometry or plethysmography to avoid any bias due to deep inhalation or forced expiration on recorded values. The primary outcome measure was the LCI, with functional residual capacity (FRCMBW) also being reported.20–22 Spirometry was performed as described previously,23 24 with FEV1, forced vital capacity (FVC) and forced expiratory flow between 25 and 75% of expired volume (FEF25–75) being reported. Plethysmographic measurements of specific airway resistance (sRaw)11 25 and partitioned lung volumes (FRCpleth, residual volume (RV) and total lung capacity (TLC))26 were also undertaken.
HRCT
All CT scans were performed at Great Ormond Street Hospital for Children, London on the same morning as the lung function tests. Scans were performed without sedation using a Siemens Sensation 16 detector unit (Siemens, Erlangen, Germany). HRCT was performed with isotropic volumetric acquisition during inspiration (rotation time: 0.5 s; pitch:1; collimation:16×0.75), with three additional 1 mm slices on expiration. Effective radiation doses varied from 1.2 to 2.0 mSv, depending on child's size. Two consultant paediatric radiologists with an interest in chest radiology (CMO, AC) reviewed scans, blinded to subject identification or clinical status. The Brody-II score was calculated; a total score of >5%; a gas trapping score >6; or any evidence of bronchial dilatation and bronchial wall thickening (bronchiectasis) was defined as abnormal.27 (see table E1, OLS for details). Inter-observer agreement for the CT scores was assessed (see OLS).
Birth weight and current height and weight were expressed in standard deviations as sex-specific z-scores.28 29 Values of LCI are relatively independent of height, age and sex in healthy subjects, with the upper limit of normal (mean+2SD) for school-aged children defined as 7.5.11 13 15 16 20 22 All remaining lung function outcomes were adjusted for sex, age and height by expressing results as z-scores.25 30–33 sRaw was calculated as both effective (sReff) and total (sRtot) airways resistance according to recent recommendations.25 Limits of normality for identifying abnormal lung function were set at ±1.96 z-scores for all tests except plethysmographic and MBW lung volumes, where results were classified as abnormal if they fell above the mean+1.96 SD z-scores derived from healthy controls, to adjust for the bias in published reference values for those outcomes that have been reported recently.34
Statistical analysis
Correlations between different LFT outcomes as well as between the various LFTs and HRCT were calculated using Spearman, non-parametric methods. Bland-Altman analysis35 was used to assess agreement between two different measures of the same outcome, for example FRC using MBW and plethysmography. Bland-Altman analysis was also used to assess agreement in total CT score between two observers, whereas a Kappa statistic was used to calculate agreement, corrected for chance, for the dichotomous CT outcome (normal/abnormal).
Results
Results were obtained in 60 clinically stable children with CF, mean (SD) 7.8 (1.3) years (range 6–10) details of whom are summarised in table 1. At the time of the test, three (5%) children with CF had any wheeze and six (10%) had crackles on auscultation, but 40 (67%) had coughed within the past seven days according to parental report. The study sample was generally representative of the clinical population from which it had been drawn (see OLS for details).13 Lung function was measured in 54 healthy controls who were of similar age (7.9 (1.2 y)), although taller and heavier than children with CF at the time of the test (table 2).
Clinical characteristics of children with CF (n=60 unless otherwise indicated)
Background characteristics of children with CF and healthy controls (HC)
Lung function
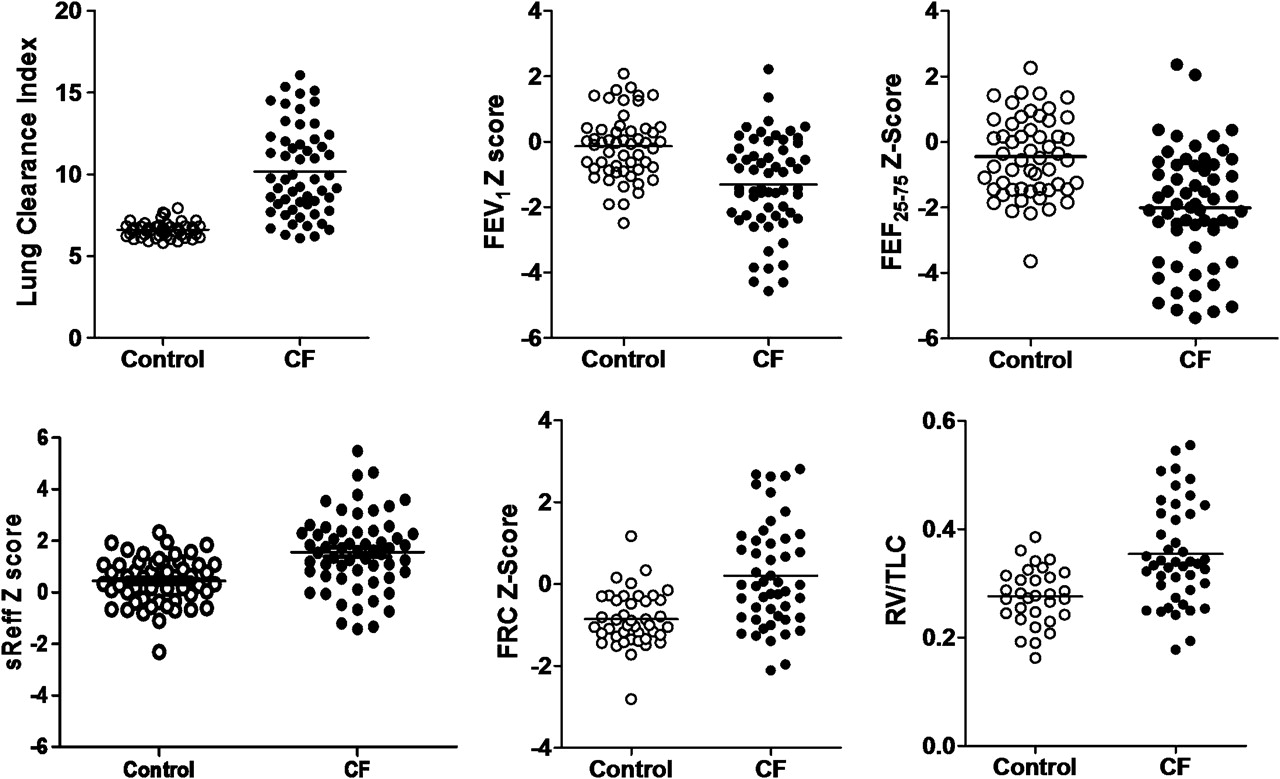
After adjustment for age, height and sex, there were highly significant differences in all lung function outcomes, except FRCMBW, between children with CF and healthy controls (table 3, figure 1). Among children with CF, more abnormalities were detected by LCI (85% (47/56)) than any other LF outcome (figure E1A, B). With the exception of a marginally reduced FEF25–75 in one child (figure E1), the presence of a normal LCI precluded abnormalities in any other LFT.
Comparison of lung function in children with CF and healthy controls

Comparison of Lung Function at ∼8 years in children with CF and healthy controls. There were significant differences (p<0.001) between children with CF and healthy controls for all the LFT outcomes illustrated above (see table 3 for additional details).
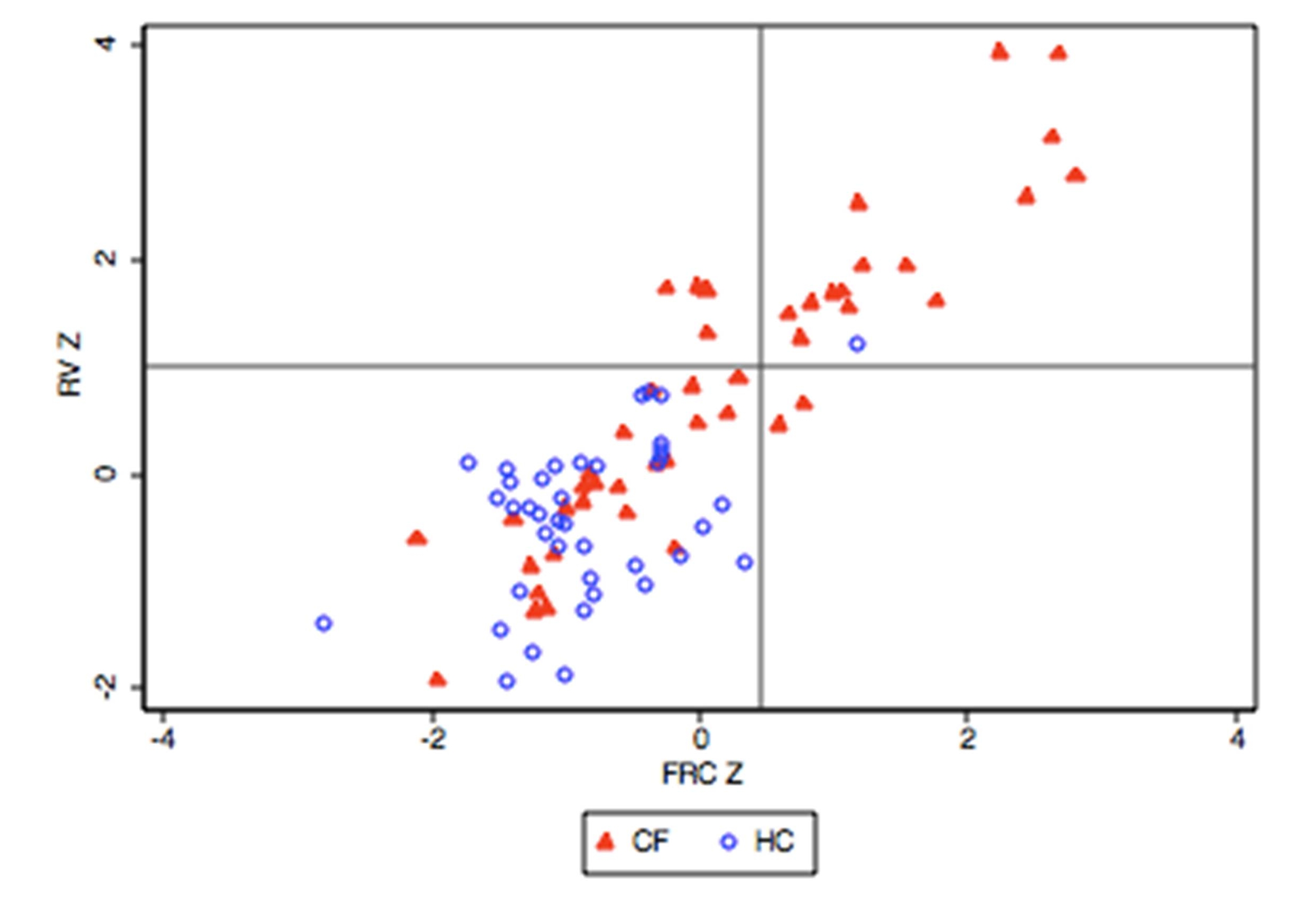
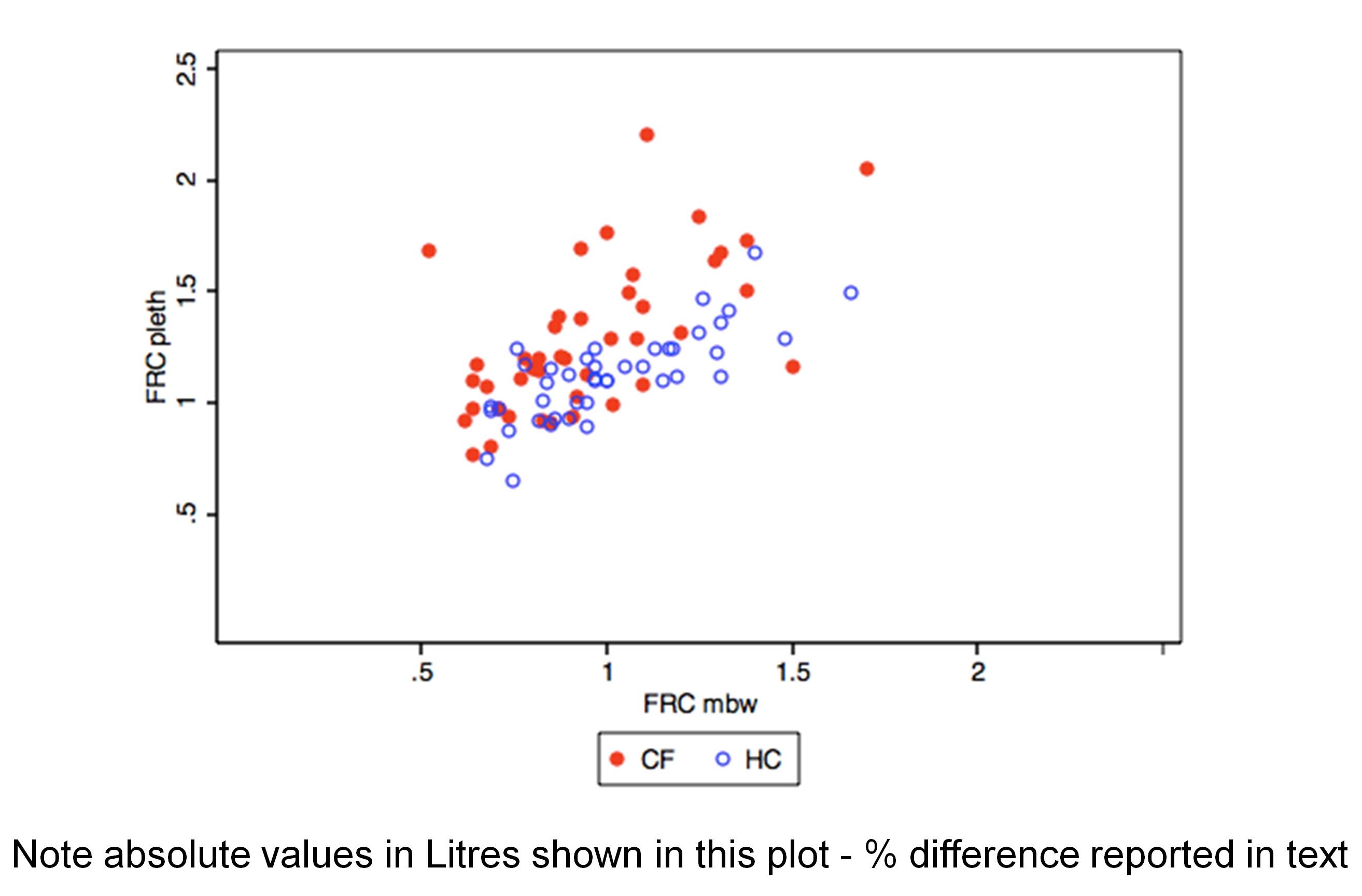
sReff and sRtot, as measures of increased resistance and/or hyperinflation secondary to airways obstruction, identified a similar proportion of abnormalities (35% & 30% respectively, data not shown). There was an inverse relationship between z-sReff and z-FEV1, (r=−0.47), both techniques detecting a similar proportion of abnormalities, though not necessarily in the same children (figure E2 OLS). Abnormalities with respect to elevated FRCpleth and RV, suggestive of hyperinflation, were identified in 19 children with CF (40% and 42% respectively of those with technically successful results, see table 3), whereas TLC was only abnormal in nine (20%). There was a significant correlation between FRCpleth and FRCMBW in both CF (r=0.63) and controls (r=0.76) (figure E4, OLS). FRCpleth was slightly higher than FRCMBW in healthy controls (mean (95% CI) difference: 13% (8 to 19%)), these differences being far more marked in children with CF (40% (28 to 51%)), indicating a significant degree of gas trapping in those with CF (figure E4 OLS).
HRCT
There was no significant difference in CT scores between observers during cross analysis: mean difference in total score (95% CI:1.2 (−0.2 to 2.7). When classifying scans dichotomously, the two observers agreed for 22/25 (88%) of the double-scored scans (18 abnormal and 4 normal; κ=0.66). When scoring individual components of the CT score there was good (R>0.7) correlation between observers for bronchial dilation, mucous plugging and peribronchial thickening, but this was lower for air trapping (R=0.59) and Parenchyma (R=0.4) (table E2, OLS).
The median (range) total Brody score was 9.5% (range 0–51%). Scans were classified as abnormal in 51/60 (85%) of children with CF: 39 scored >5% of maximum, while nine with a score of <5% had bronchial dilatation, and a further three with no bronchial dilatation had an air-trapping subscore of ≥6. All children with total CT scores >5% also had evidence of bronchiectasis and/or an air-trapping subscore of ≥6. Measurements could not be completed on the same day in three children due to technical difficulties with the mass spectrometer. Comparisons between HRCT and LFT findings in the following section have been limited to children in whom both tests were performed on the same morning.
Lung function indices compared with CT
Of the 57 CF children in whom CTs were performed on the same day as lung function, scans were classified as abnormal in 48 (84%). Of the 53 children in whom both LCI and CT were available, 44 had an abnormal LCI (ie, >7.5) and 44 had abnormal CT results. The results were concordant and abnormal for 39/53 (74%) children, whereas they were concordant and normal for four children (ie, overall concordance 81% for total CT score). Of the nine children with a normal LCI, five (56% (95% CI (27 to 81%)) had an abnormal CT, and similarly 5/9 with a normal CT had an abnormal LCI (table 4; figure 2A). By contrast, abnormal results from both CT and spirometry were only observed in 32% (18/57) of children with CF when using FEV1 (figure 2B, table 4) and 40% (23/57) if based on FEF25–75. Similar results were obtained when concordance between the various LF outcomes and the bronchiectasis subscore were examined (table 5). Although fewer abnormalities were detected by FRCpleth and/or RV than when using the LCI, both total CT score and bronchiectasis subscore were always abnormal in the presence of hyperinflation detected by plethysmography (tables 4 and 5).
Concordance between total CT score and lung function results in children with CF

Relationship between A) LCI and B) FEV1 with total CT score measured on the same day in children with CF. FEV1 is expressed as z-scores to adjust for height, age and sex. Seventy four per cent of children had abnormal results from both CT and LCI (>7.5), whereas an abnormal FEV1 (<1.96 z-scores) was only found in 32% of those with abnormal CT. Solid triangles denote those with evidence of air trapping and/or bronchiectasis despite a total CT score <5. Brody scores in those with normal LCI ranged from 0 to 6.7%. LCI among those with normal HRCT ranged from 6.1 to 8.7.
Concordance between bronchiectasis on CT and lung function results in children with CF
The correlation between the total Brody score and LCI (R=0.77, figure 2A) was stronger than with any other lung function outcome (see table E3, OLS), those with the highest CT scores also having higher LCI values. Similarly, the LCI showed the strongest correlations with the bronchial dilatation, mucous plugging, air trapping and peribronchial thickening components of the CT (figure 3), followed by measures of hyperinflation (FRCpleth, RV and RV/TLC, table E3). Although statistically significant, the relationships between CT sub-scores and either specific resistance or spirometric outcomes were weaker, whereas those between CT and TLC or FRCmbw were not significant. (table E3, OLS).

{kind=link}
{kind=link}
{kind=link}
Relationship between LCI and individual elements of the CT score. In addition to the relationship with total score, LCI was significantly related to all individual elements except the parenchyma score (data not shown, r=0.16). For further details see table E3 OLS.
Discussion
The main findings of this study are that, among six to 10 year old children with CF who have been diagnosed clinically: a) very few had either a normal HRCT or LCI; b) LCI was far more sensitive than any spirometric or plethysmographic outcome to the presence of HRCT abnormalities (both with respect to total score and individual abnormalities); and (c) contrary to previous work,17 a normal LCI cannot exclude the presence of HRCT abnormalities in this population. The major novel finding is that while HRCT is almost invariably abnormal (39/44, 89%) if LCI is abnormal, a normal result on either measure is not predictive of a normal result on the other. Since radiation dosage is an issue with HRCT, the authors suggest that in clinical practice, LCI should be performed first, and, only if it is normal should the child have an HRCT. Adoption of this policy would have reduced the number of HRCTs performed in this population by 83%, that is from 53 to only nine subjects.
Previous studies in this area
Both HRCT and LCI have been suggested as possible markers of early CF lung disease. Both measures have been shown to be abnormal in young children with CF who still have normal spirometry;2 11–13 17 37 38 to worsen with increasing age on cross sectional studies,11 15 17 37 and with time on longitudinal studies;14 39 40 and to improve with CF therapy.41 42 It is therefore very likely that both these measures can detect early CF lung disease. It should, however, be noted that the two measures detect different, albeit overlapping, aspects of CF pathology. HRCT detects mostly early structural changes, including those that are not yet visible on plain radiograph; air trapping is a surrogate for distal airway obstruction. LCI is a measure of lung function, and specifically a measure of inhomogeneous ventilation distribution. Several other lung function measures were used in this study. As expected, spirometry did not detect abnormality as frequently as either HRCT or LCI. A previous study from the authors demonstrated that plethysmographic specific airway resistance was superior to spirometry but inferior to LCI for detecting functional abnormality in preschool children with CF,12 However, in this population of young school children, the authors found that measures of hyperinflation (FRCpleth and RV) (which are generally not measurable in preschool children) were superior to sReff with respect to detecting lung function abnormalities (tables 4 and 5), confirming previous reports from older school-age children.40 43 Similarly, although the associations between FRCpleth and RV and structural changes on CT were weaker than those seen for the LCI, they were both considerably stronger than that seen with either specific airways resistance or Spirometric outcomes (table E3, OLS).
There have been two previous studies comparing LCI with HRCT in individuals with CF. Gustafsson and colleagues retrospectively analysed clinical data collected in 44 subjects with CF aged five to 20 years.17 All subjects had spirometry, MBW, and HRCT data collected at annual review, although it is not clear if all scans and LFTs were performed on the same date. The data from Gustafsson's study17 were collected and analysed using different methods from this study. First, whereas Gustafsson's study employed an intermittent sampling protocol for CT, the authors of this study collected a low dose complete inspiratory volumetric dataset to minimise the risk of missing abnormalities. Second, the comparisons of CT and lung function data in this study have aimed to identify both overall concordance between methods and also, by recruiting a contemporary control group, to identify the extent to which children with normal results by one method are likely to have normal/abnormal results by another. In a smaller study, Ellemunter and colleagues reported CT and LCI in a highly selected group of 34 subjects aged six to 26 years, all with a normal FEV1.38 Although these data were collected prospectively, the scans were performed according to a clinical protocol, with up to 243 days separating the two investigations. In contrast to the present study, it was not possible to calculate the Brody II score, which is currently considered to be the most comprehensive, systematic and robust system for use in CF, from either of these previous studies, making it difficult to make direct comparisons of results. In addition, neither of these studies had a contemporary control group, and their structure-function comparisons were limited to spirometry and LCI, whereas in this study, the range of functional assessments was extended to include plethysmographic measures of lung volume and resistance, which have been shown to be sensitive markers of early lung disease in children with CF.11 40 43
Strengths and weaknesses
There are some important aspects of this study’s design that need to be highlighted. First, this study was targeted at a specific age group of children in early school-age. This age range was selected because of the relative ease of testing compared with infants or preschoolers, and the likelihood that many of these children would only have mild disease. As discussed in the OLS, the children with CF were generally representative of those attending clinics in London at the time of study.13
Data were collected prospectively, with HRCT and lung function testing being performed within hours of each other. The HRCT protocol was designed to provide a balance of the maximum information with the lowest radiation dose. The radiation dose is significantly higher where all of the thoracic volume is included within the scanned range, (thin section 0.6 mm collimated volumetric scanning), compared to the traditional method of ‘sampling’ thin slices of lung (eg, 1 mm slices at 10 or 20 mm intervals). The latter technique will bypass sections of lung, which will not be irradiated, which is particularly important where highly radiation sensitive tissue (eg, breast tissue) is within the direct incident radiation beam. On the other hand, in a disorder which affects the lung in a patchy distribution (especially in the early stages of the disease process) contiguous whole volume data acquisitions will help interrogate the whole volume of tissue and hence detect early small volume change in a more sensitive manner. In this study, the inspiratory data set was acquired as a whole lung volumetric study at low radiation dose enabling interrogation and scoring of the entire lung volume at TLC. As a compromise the expiratory phase acquisition included only three thin sections of lung with scans performed through the upper, mid and lower thoracic anatomical sections.
A potential methodological problem when using CT to evaluate lung parenchymal disease is that of defining what constitutes ‘normal’ appearances, since such imaging is rarely justified in subjects with normal lungs. Minor abnormalities of lung structure, such as small areas of linear atelectasis and post infective nodular consolidation, are common incidental findings. The problem of air-trapping is perhaps the most challenging: although air-trapping on CT is an important marker of distal airways disease in children with CF and in other types of non-CF airways diseases,44 45 Tanaka et al have shown that extensive air-trapping can be identified on expiratory CT in apparently healthy individuals.46 Consequently, using a score of zero to define ‘normal,’ may result in otherwise healthy subjects being classified as ‘abnormal’. To overcome this problem, recent publications have defined ‘abnormal’ as being a composite modified Brody HRCT score of >5%, or the presence of any bronchial dilatation, or air-trapping involving >30% of the lung.17 47 Similar definitions were used in this study, differing only in the definition of air-trapping. In fact, the inclusion of the 5% criterion was superfluous in this study, as all patients with a composite score of >5% had evidence of bronchiectasis and/or an air-trapping subscore of >6. These definitions do, however, remain arbitrary and, in the absence of studies on control subjects, essentially unvalidated.
A range of measures were employed to assess functional changes, and a prospective healthy control group was recruited. The extent of hyperinflation in children with CF was evident not only from the discrepancy between plethysmographic and gas washout assessments of FRC but from the elevated z-scores for FRCpleth and RV. The latter would, however, have been severely underestimated had the authors simply expressed results according to published reference data rather than in direct comparison to healthy controls (table 3, figure E1 OLS). Interestingly, with the exception of the LCI, it was these measures of hyperinflation which showed the strongest concordance and correlations with both the total CT scores and the bronchiectasis subscore (tables 4 and 5, table E3 OLS).
Finally, when interpreting these results, the authors have avoided presenting sensitivity and specificity calculations, as this implies the existence of a gold standard for the detection of CF lung disease. The authors suggest that such a standard does not currently exist. While abnormal HRCT or LCI in young children with CF almost certainly reflects the presence of lung disease, this does not necessarily mean that a normal result from one or both measures confirms the absence of disease. The authors have therefore presented these results as frequency of abnormality and concordance between measures.
Clinical implications and conclusions
It has already been demonstrated that HRCT and LCI are both sensitive to early CF lung disease. In contradistinction to previous work, this study has shown that a normal LCI is not predictive of a normal HRCT. While concordance in children with more severe lung disease is very good, it is less strong in children with very mild disease. In other words, some children with normal LCI have minor abnormalities on HRCT, and vice versa.
For both measures there are challenges still to be addressed. The advantage of LCI is that it is relatively easy to measure, safe, and inexpensive. For the last decade, the majority of research in this area has been performed in a small number of specialised laboratories, as no commercially manufactured MBW systems were available. That situation is very likely to change in the next few years. In contrast, HRCT scanning is widely available, and a well accepted and validated scoring system has been developed. However there is some controversy over whether a more sensitive scoring system might be more appropriate, or whether quantitative automated scoring would be more appropriate.48 Perhaps most importantly, there is concern regarding the radiation exposure related to repeated CT scanning.7 9 10 This concern will limit the number of CT scans that can be performed in an individual patient for monitoring purposes, and also limit its use as a clinical outcome following interventions.
It is not yet possible to identify whether one of these tests is ‘better’ than the other. Long-term follow-up will be required to identify which test more accurately predicts the clinical course of children with very mild or early disease, and which test is more sensitive to change in lung disease, and it is likely that different approaches will be required according to the specific research or clinical question being posed. Many centres are now advocating annual HRCT scans in CF. However, given the potential risk of cumulative radiation exposure, the authors suggest, on the basis of the data reported here, that LCI should be performed as the first investigation in school age children to assess the presence of CF lung disease. Only if LCI is normal may HRCT be necessary. This approach would allow much more frequent monitoring for early CF lung disease, with enhanced safety. This policy would result in a substantial reduction in the radiation burden to the CF population, and considerable cost savings.
Acknowledgments
The authors thank all the members of the LCFC and the children and families that participated in this study. They also thank Sooky Lum for invaluable help with data management, Carol Young and Yvonne Sullivan for their unswerving enthusiasm and assistance during the CT scans, Prof Per Gustafsson for his ongoing support and advice regarding the MBW technique and Prof K Costeloe, Dr J Hawdon and staff at the Homerton University and University College London Hospitals for their assistance in recruiting many of the healthy controls. This study was funded by the CF Trust, Smiths Medical and Asthma UK.
References
Supplementary materials
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Footnotes
Members of the London Cystic Fibrosis Collaboration P Aurora, I Balfour Lynn, A Bush, S Carr, J Davies, R Dinwiddie, A-F Hoo, W Kozlowska, S Lum, C Oliver, C Owens, A Prasad, J Price, S Ranganathan, M Rosenthal, G Ruiz, A Shankar, S Stanojevic, J Stocks, J Stroobant, R. Suri, A Wade, C Wallis and H Wyatt
Funding This study was funded by the CF Trust, Smiths Medical and Asthma UK.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.