Article Text

Abstract
Background Previous studies have suggested that long-term use of β agonists to treat chronic obstructive pulmonary disease (COPD) may increase the risk of cardiovascular adverse events. In this post hoc analysis, data from the TOwards a Revolution in COPD Health (TORCH) study were used to investigate whether use of the long-acting β2 agonist salmeterol over 3 years increased the risk of cardiovascular adverse events in patients with moderate to severe COPD.
Methods TORCH was a randomised, double-blind, placebo controlled study conducted at 444 centres in 42 countries. Patients (n=6184; safety population) received twice daily combined salmeterol 50 μg plus fluticasone propionate 500 μg (SFC), either component alone, or placebo. Adverse events were recorded every 12 weeks for 3 years.
Results The probability of having a cardiovascular adverse event by 3 years was 24.2% for placebo, 22.7% for salmeterol, 24.3% for fluticasone propionate and 20.8% for SFC. Although a history of myocardial infarction doubled the probability of cardiovascular adverse events, the event rates remained similar across treatment groups.
Conclusion Post hoc analysis of the 3-year TORCH dataset showed that salmeterol alone or in combination (SFC) did not increase the risk of cardiovascular events in patients with moderate to severe COPD.
- COPD Pharmacology
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is now recognised as being a highly prevalent condition1 that causes significant morbidity and mortality,2 and commonly coexists with cardiovascular disease.3 Cardiovascular events are one of the leading causes of mortality and hospitalisation in patients with COPD, particularly in those with mild to moderate disease.4 5 Moreover, COPD is a strong risk factor for cardiovascular events, independent of smoking,3 6 7 and impaired lung function is an important marker for cardiovascular mortality.8 9 However, it is unclear whether COPD interventions other than smoking cessation4 can modify the increased cardiovascular risk associated with COPD.
Recently there has been concern that the long-term use of inhaled bronchodilators commonly used in the treatment of COPD, including long-acting β2 agonist (LABA) and anticholinergic drugs, may increase the risk of cardiovascular complications.10–14 However, prospective data about the relative risk of therapy in patients with sufficient symptoms to be offered treatment with these drugs has, until recently, been lacking.
While the 3-year TOwards a Revolution in COPD Health (TORCH) study primarily investigated the effect of combination therapy with the LABA salmeterol (SAL) and the inhaled corticosteroid fluticasone propionate (FP) compared with placebo on all-cause mortality, other efficacy outcomes and adverse events (AEs) were also measured. The primary paper including the mortality analysis has already been published.15 It reported that long-term use of SAL or the SAL plus FP combination (SFC) did not increase the rate of cardiac death. In view of the continuing concerns about cardiovascular safety in COPD therapy, we extended this analysis (post hoc) to consider the occurrence of cardiovascular AEs and serious adverse events (SAEs) in the TORCH study. We also explored the factors that might determine the incidence of cardiovascular events in these patients. Some of these results have previously been presented in abstract form.16
Methods
Patients
Details of patient eligibility and study entry criteria have been published previously.15 Eligible patients were current or former smokers aged 40–80 years with a prebronchodilator forced expiratory volume in 1 s (FEV1) <60% of the predicted value and a ratio of prebronchodilator FEV1 to forced vital capacity (FVC) of ≤0.70. The only exclusion criterion with respect to comorbidities was that subjects were considered unlikely to die of something other than COPD in the subsequent 3 years.
Design overview
The study design has been described in detail previously.15 17 TORCH was a multicentre, randomised, double-blind, parallel-group, placebo controlled study conducted at 444 centres in 42 countries. After a 2-week run-in period, eligible patients were stratified by smoking status and randomised to receive either SFC 50/500 μg, SAL 50 μg, FP 500 μg or placebo twice daily for 3 years via a Diskus/Accuhaler inhaler (GlaxoSmithKline, Greenford, UK). Full details of the randomisation procedure have been reported elsewhere.15 17
The primary efficacy end point of the TORCH study was all-cause mortality. Other end points were rate of COPD exacerbations, health-related quality of life, lung function and AEs. After randomisation, patient visits occurred every 12 weeks to record any AE. At each visit the subject was allowed to spontaneously mention any problems, then the investigator asked the following standard questions: (1) ‘Have you had any (other) medical problems since your last visit/assessment?’ and (2) ‘Have you taken any new medicines other than those given to you within this study since your last visit/assessment?’ An AE was defined as any unfavourable and unintended sign (including a clinically significant abnormal laboratory finding), symptom or disease temporally associated with the use of the blinded study product, whether or not it was considered to be related to that product.
SAEs were those that resulted in any of the following outcomes: (1) death; (2) an immediate risk of death; (3) hospitalisation or prolongation of an existing hospitalisation; or (4) any other important medical event which, in the opinion of the investigator, jeopardised the subject's health. An independent safety and efficacy data monitoring committee performed safety reviews of all SAEs every 6 months. Causes of death were independently adjudicated in a standardised fashion by a clinical end point committee.18
Cardiovascular safety evaluation
Cardiovascular AEs were classified based on the Medical Dictionary for Regulatory Activities (MedDRA) Version 8.1 terms. MedDRA is the AE classification dictionary endorsed by the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH). All events in the cardiac disorders system organ class plus selected events from the vascular disorders and nervous system disorders system organ classes were included (table 1). Further analysis was also conducted on the subset of ischaemic events and on events related to stroke (table 1). No specific information was collected about whether patient-reported AEs had been objectively verified.
List of MedDRA system organ class (SOC) high-level group terms (HLGT) used for analysis of cardiovascular events, ischaemic cardiovascular events and stroke events, and list of cardiovascular medications included in the analysis
Subjects receiving medications commonly used to treat cardiovascular disease were identified; these medications were selected from dictionary groupings (listed in table 1).
Statistical analysis
The study was powered for its primary all-cause mortality end point and was not formally powered to detect differences in numbers of AEs between treatments.
The safety population included all patients who took at least one dose of study medication. The number and proportion of patients reporting a cardiovascular AE over the 3 years were summarised by treatment group. To correct for differential treatment exposure between the treatments, the rate of cardiac events per 1000 treatment years was calculated by dividing the total number of AEs by the total number of years patients were exposed to study treatment, then multiplying by 1000. On-treatment deaths were defined as any death occurring up to 14 days after patients stopped their study medication.
The time to first cardiovascular AE was compared between treatment groups using Kaplan–Meier estimates and the log-rank test, stratified by smoking status; Kaplan–Meier cumulative incidence curves were also generated. Statistical significance was set at p<0.05.
Results
Study population
Of 8554 patients with COPD recruited, 6184 were randomised and evaluated for safety (figure 1). This included 72 patients from five sites excluded from the published efficacy analyses.15 One subject was randomised to placebo but took FP for the majority of the treatment period and was analysed with the FP group.

Patient flow. *The number of patients who underwent randomisation and the number of those included in the safety population differ in the placebo group and the fluticasone propionate group because one patient who was assigned to placebo received fluticasone propionate for more than half the study period; this patient was therefore included in the fluticasone propionate group for the safety analysis. AE, adverse event.
Demographic and baseline patient characteristics were balanced across treatment groups (table 2). The mean age was 65 years, 76% were male, mean smoking history was 48 pack-years and baseline postbronchodilator FEV1 was 44% of predicted. At baseline, 7% of patients reported a history of previous myocardial infarction (MI), 41% were taking cardiovascular medications and 60% were taking short-acting anticholinergic drugs. Use of the long-acting anticholinergic tiotropium bromide during the study was low (3%) and was similar across treatment groups. Of the 187 subjects receiving tiotropium, over half took it for 12 weeks or less.
Patient demographic and baseline characteristics of the safety population
The proportion of patients who withdrew from the study was highest in the placebo group (44%) and lowest in the SFC group (34%) (SAL 37%, FP 39%). The total number of patient-years of exposure to the study drugs was 3278 for placebo, 3531 for SAL, 3555 for FP and 3700 for SFC.
Cardiovascular AEs
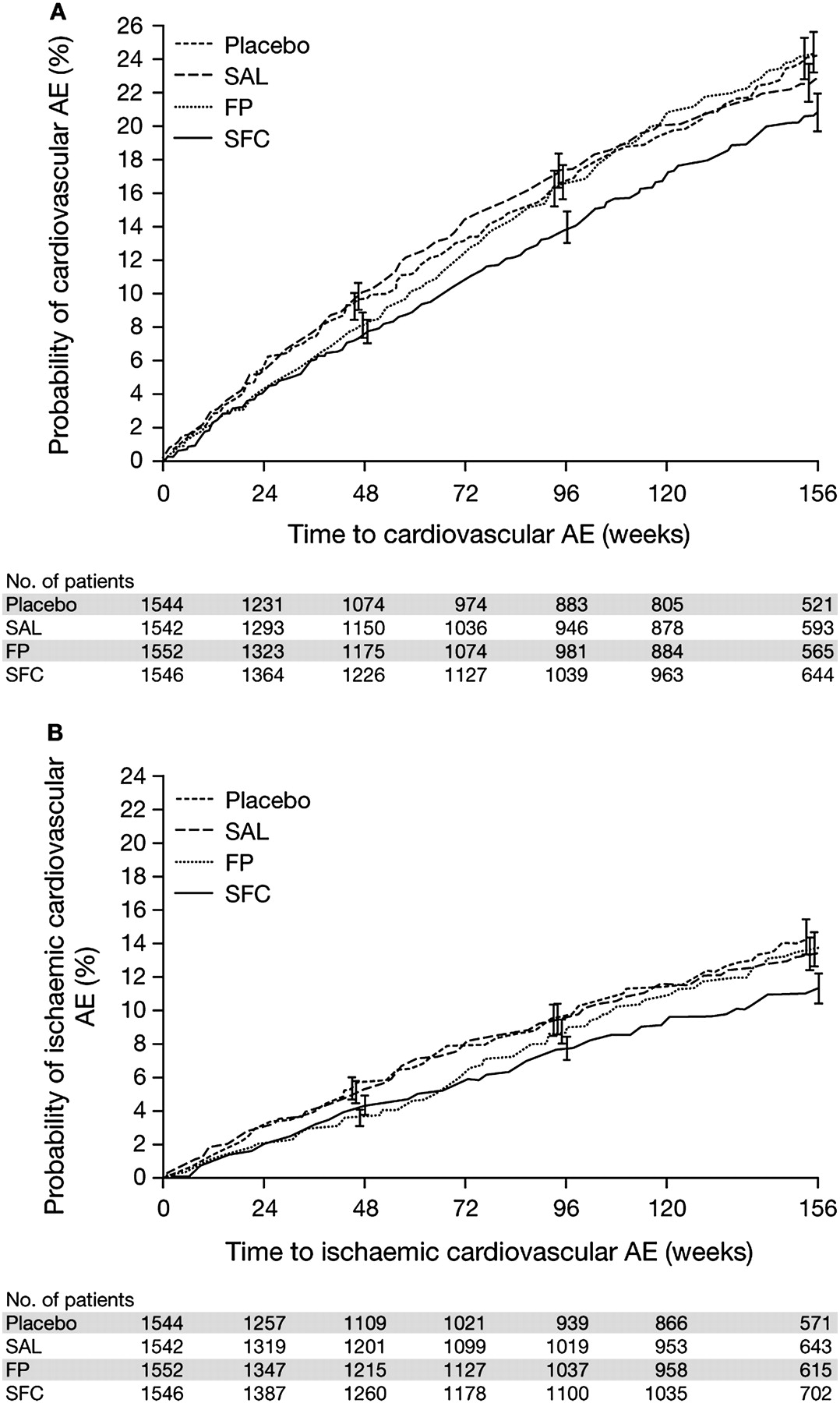
The proportion of patients who experienced a cardiovascular AE or cardiovascular SAE during the study was similar across treatment groups (17–20% and 10–12%, respectively) (table 3). When expressed as the number of events per 1000 treatment years, the rate of cardiovascular AEs was 142 in the placebo group and 110 in the SFC group. The probability of patients having a cardiovascular AE by 3 years was lowest for SFC at 20.8% (24.2% for placebo, 22.7% for SAL and 24.3% for FP; figure 2A; table 3). The probability of patients having a cardiovascular SAE by 3 years was lowest for SFC at 12.5% (15.4% for placebo, 13.6% for SAL and 14.7% for FP; table 3).
Summary of all cardiovascular AEs and SAEs

Cumulative incidence of (A) all cardiovascular adverse events and (B) ischaemic cardiovascular adverse events. Full details of the data presented in (A) and (B) including statistical testing are shown in tables 3 and 4, respectively. Vertical bars represent standard errors. AE, adverse event; FP, fluticasone propionate; SAL, salmeterol; SFC, salmeterol/fluticasone propionate combination.
The proportion of patients experiencing an ischaemic cardiovascular AE was similar across treatment groups (9–11%; table 4). The rate of ischaemic cardiovascular AEs per 1000 treatment years was 68 for placebo, 70 for SAL, 62 for FP and 54 for SFC. The probability of patients having an ischaemic cardiovascular AE by 3 years was lowest for SFC at 11.3%, 14.6% for placebo, 13.4% for SAL and 13.8% for FP (figure 2B and table 4).
Ischaemic cardiovascular AEs
The proportion of patients with a stroke-related AE over the 3-year course of the study was similar in each treatment group (3% placebo, 2% SAL, 3% FP and 3% SFC). The rate of stroke-related AEs per 1000 treatment years was 17 for placebo, 13 for SAL, 16 for FP and 12 for SFC.
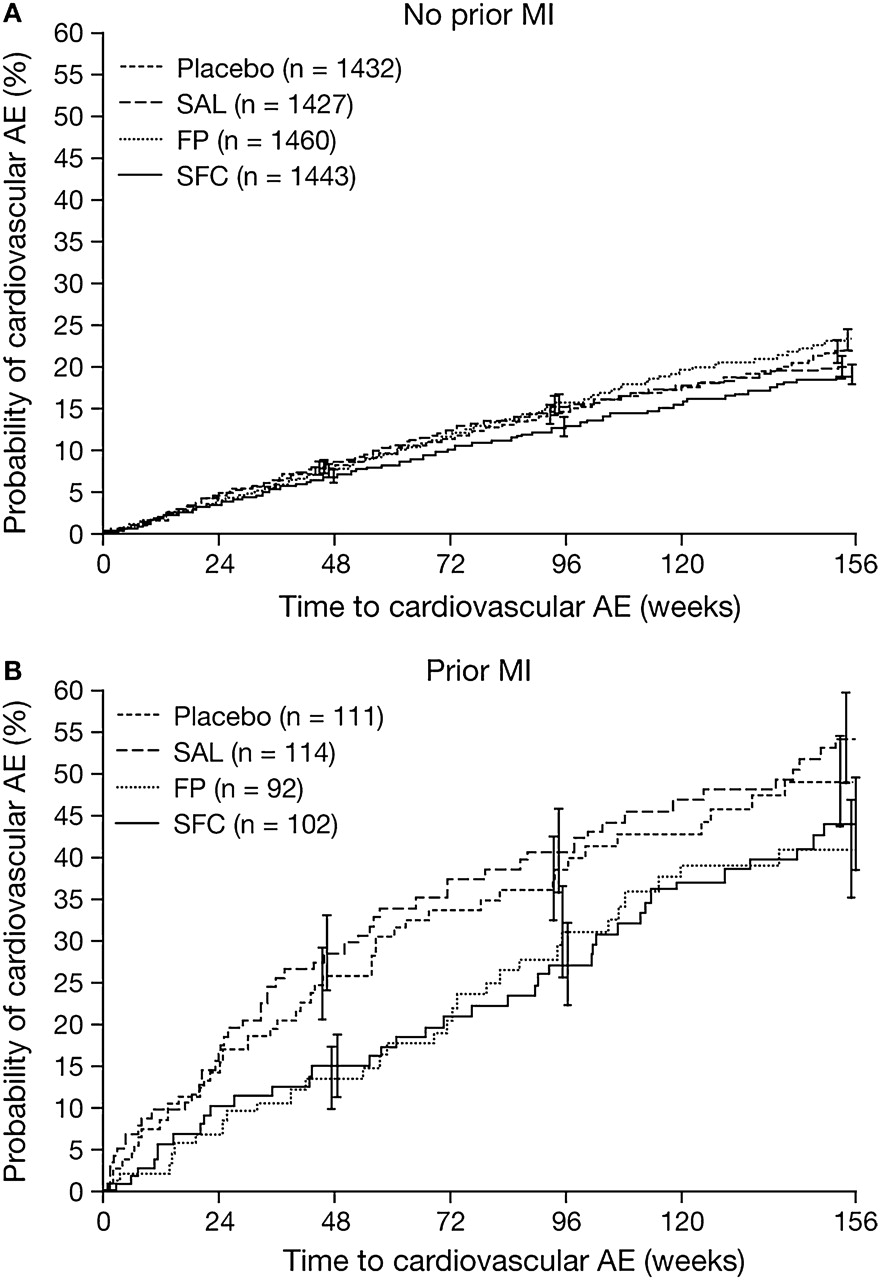
The likelihood of experiencing a cardiovascular AE was unaffected by gender and current smoking status (table 5). Patients who were on cardiovascular medications at baseline (figure 3), reported a previous MI (figure 4), were older or had lower baseline FEV1 (table 5) had a higher probability of having a cardiovascular AE. There were no significant differences between treatments in the likelihood of an event being reported, nor was there consistent evidence for an interaction between treatment and spirometrically-defined disease severity with respect to cardiac events (see table 1 in online supplement) . In patients who had previously had an MI, the likelihood of having a cardiovascular event over 3 years was 54.4% on salmeterol compared with 49.1% with placebo (p =0.51) and 44.1% with SFC (p=0.051 relative to salmeterol (figure 4B and table 5). However, the pattern of risk in other groups was inconsistent with salmeterol-treated patients having a similar incidence of events to patients treated with FP, as identified by their use of previous cardiac therapies (figure 3B). Patients who were taking short-acting anticholinergic treatment at baseline had a higher probability of cardiovascular events (table 5); however, these patients also had lower baseline percentage predicted FEV1. The pattern of cardiovascular events was similar across treatment groups irrespective of baseline anticholinergic use.
Kaplan–Meier probability of a cardiovascular adverse event by 3 years by subgroups

Cumulative incidence of all cardiovascular adverse events in patients who (A) did not receive or (B) did receive cardiovascular medication (listed in table 1) in the 12 months prior to screening. Full details of the data presented in this figure including statistical testing are shown in table 5. Vertical bars represent standard errors. AE, adverse event; CV, cardiovascular; FP, fluticasone propionate; SAL, salmeterol; SFC, salmeterol/fluticasone propionate combination.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative incidence of all cardiovascular adverse events in patients who (A) had not experienced or (B) had experienced a myocardial infarction prior to study entry. Full details of the data presented in this figure including statistical testing are shown in table 5. Vertical bars represent standard errors. AE, adverse event; FP, fluticasone propionate; MI, myocardial infarction; SAL, salmeterol; SFC, salmeterol/fluticasone propionate combination.
Cardiovascular deaths
There were 882 deaths (14%) during the 3-year study period, including those both on and off study treatment (see table 2 in online supplement). Of these, 239 were due to cardiovascular causes as adjudicated by the clinical end point committee. For placebo, 71 deaths (4.6%) were due to cardiovascular causes compared with 45 (2.9%) for SAL, 61 (3.9%) for FP and 62 (4.0%) for SFC. There were 468 deaths while on treatment, of which 172 were due to cardiovascular causes. For placebo, 47 (3.0%) deaths were due to cardiovascular causes compared with 33 (2.1%) for SAL, 43 (2.8%) for FP and 49 (3.2%) for SFC.
Discussion
COPD is not simply a lung disease19 but is associated with an increased likelihood of complications outside the lungs. Support for this concept comes from recent studies that have shown significantly increased pulse wave velocity, independent of smoking status and other risk factors, in patients with stable COPD.20 In these circumstances it is no surprise that cardiovascular morbidity and mortality is high in COPD.
Both β agonists and antimuscarinic agents, the main classes of bronchodilator drugs used to treat COPD, have the potential to precipitate cardiac rhythm disturbances and other cardiac events; however, this has not been regarded as important in clinical practice until recently. Unfortunately, unlike the situation for cardiovascular disease, most studies of drug treatment in COPD have been relatively brief (≤1 year) and have only reported on-treatment data. These studies have made the largest contribution to the systematic reviews in this field, at least as far as patients receiving treatment for symptoms are concerned. As the TORCH study was conducted in a patient group likely to be prescribed inhaled LABAs, the TORCH dataset addresses some of the problems inherent in these earlier analyses. The current analysis provides generally reassuring results about the cardiovascular safety of inhaled LABA treatments in patients with COPD.
TORCH is the largest and longest prospective trial to examine the role of an inhaled LABA and an inhaled corticosteroid in COPD. Half of the >6000 patients were randomised to a regime containing SAL and, allowing for dropouts, this provides 7231 patient-years of exposure to these agents. Over the 3 years, approximately 1 in 5 patients experienced a cardiovascular AE. The event rate was lowest in those receiving SAL in combination with FP and not different from those patients treated with placebo or with LABA monotherapy. A SAE requiring hospitalisation and new cardiovascular ischaemic events were approximately half as common as the total cardiovascular event rate, but there was a similar pattern across treatment groups. Seven percent of patients had a history of previous MI. In this group the cardiovascular event rate, as would be expected, was higher. Again, no trend was seen for more AEs in those patients randomised to treatment with SAL in combination with FP. However, the data for SAL alone are inconclusive, possibly due to the small sample size in this smaller subgroup of patients.
Unlike other COPD studies, TORCH developed a rigorous methodology for determining the likely cause of death which was adjudicated by an expert panel blinded to the study medication.18 Moreover, there was effectively complete follow-up of the vital status of all patients 3 years after randomisation. In this data set, the patients randomised to LABA alone had the lowest rate of cardiovascular death while those who received placebo had the largest number of events. The number of on-treatment deaths, analogous to data included in earlier COPD studies, showed a similar pattern across treatments.
A range of predictable factors increases the cardiovascular event rate including higher age, a history of previous cardiac disease and worse lung function. None of these factors interacted with treatment to identify a specific ‘at-risk’ group. Somewhat surprisingly we saw no difference in event rate between current and ex-smokers, which may reflect our study entry criteria or possibly the nature of cardiovascular disease in patients with COPD. We did not control for the use of inhaled anticholinergic drugs although, when used, this was predominantly ipratropium as tiotropium was not available in most countries until TORCH was nearing completion. In those patients treated with an anticholinergic agent, there was a suggestion of a somewhat higher cardiovascular event rate but these patients also had lower baseline lung function. The association seen is therefore likely to represent the confounding influence of disease severity, an issue that has made interpretation of previous studies of COPD therapy particularly difficult. Patients in GOLD stage 4 receiving salmeterol appeared to have more cardiac events, although the differences between treatment groups were not significant. This finding is at odds with the lower than average reported incidence of events with salmeterol in GOLD stage 3 and probably reflects the lower sample size in the GOLD stage 4 population with correspondingly widened confidence intervals for these data.
Our study has strengths and some limitations. We monitored our patients regularly throughout the 3-year study, but events were self-reported rather than being in response to a predetermined diagnostic list. We did not undertake ECG or echocardiographic evaluations at the study outset and there was no requirement to provide objective documentation of the nature of any new cardiovascular episode. However, we did include patients with a history of cardiovascular disease provided it was not thought that this was the main cause for their symptoms or that they were likely to die from this during the study. This is an important difference from earlier studies where more restrictive eligibility criteria were applied. As in other large COPD studies, for example UPLIFT21 and TRISTAN,22 patients randomised to placebo tended to withdraw more frequently than those randomised to active therapy, probably reflecting their deteriorating condition. Thus, patients continuing in the placebo arm of our on-treatment analysis represent a relatively fitter group of patients with COPD. Despite this, we saw no suggestion that patients on treatment were more likely to experience adverse cardiovascular problems. Finally, we lack data about whether the use of these agents increases the risk of cardiovascular events during an acute exacerbation. Recent literature reviews have failed to report any association between use of high-dose β agonists and risk of arrhythmias in this setting.23
For some of our data the SFC combination appeared to be associated with important reductions in the incidence of adverse cardiovascular events. Although this difference may simply have been due to chance, other biologically plausible mechanisms exist which can account for this effect. It has been suggested that inflammation occurring in COPD might directly promote vascular damage24 and this may be reduced when airway inflammation is decreased, as has been demonstrated with a LABA/inhaled steroid combination.25 Our data cannot address this hypothesis, but this concept is supported by recent observations from a large database study that patients who used inhaled corticosteroids were less likely to experience cardiovascular deaths than those who received bronchodilators alone.12 This is consistent with the general conclusions of the TORCH study that there was a reasonable (but not conclusive probability that combination treatment with SAL plus FP prolongs life in COPD. An alternative explanation for the effect of SFC on cardiovascular outcomes may be its relative efficiency in preventing exacerbations of COPD which are associated with elevations in troponin T and a raised cardiac infarction injury score, at least in hospitalised patients.26 27 Further studies will be needed to address whether these potentially important mechanisms best explain the observed data.
In summary, in this large prospectively collected dataset, the occurrence of new cardiovascular AEs was no more frequent in patients treated with a LABA than in those treated with placebo. In addition, we saw some evidence that the combination of a LABA and an inhaled corticosteroid might offer a degree of cardioprotection. These data from patients with moderate to severe COPD provide reassurance that our current use of inhaled LABA therapies is not harmful to cardiovascular health.
Acknowledgments
The authors acknowledge medical writing support from David Cutler, a professional medical writer with Gardiner-Caldwell Communications, in the preparation of this manuscript; this support was funded by GlaxoSmithKline.
References
Supplementary materials
Web Only Data thx.2010.136077
Files in this Data Supplement:
Footnotes
Funding This work was supported by GlaxoSmithKline.
Competing interests PMAC has received consulting fees from AstraZeneca, GlaxoSmithKline, Nycomed and Pfizer; speaking fees from GlaxoSmithKline and Nycomed; and grant support from Boehringer-Ingelheim and GlaxoSmithKline. JAA, CC, LRW and JCY are employed by and hold stock in GlaxoSmithKline. BC has received consulting fees from Altana, AstraZeneca, Boehringer-Ingelheim and GlaxoSmithKline; speaking fees from Altana, AstraZeneca, Boehringer-Ingelheim and GlaxoSmithKline; and grant support from Boehringer-Ingelheim and GlaxoSmithKline. GTF has received consulting fees from Boehringer-Ingelheim, GlaxoSmithKline, Novartis and Schering Plough; speaking fees from Boehringer-Ingelheim, GlaxoSmithKline and Pfizer; and grant support from Altana, Boehringer-Ingelheim, Emphasys Medical Inc, Forrest, GlaxoSmithKline, Mannkind Corporation and Novartis. CJ has received consulting fees from Altana, AstraZeneca, Boehringer-Ingelheim and GlaxoSmithKline; speaking fees from Altana, AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline and Novartis; and grant support from GlaxoSmithKline. PWJ has received consulting fees from AstraZeneca, GlaxoSmithKline, Novartis and Roche; speaking fees from AstraZeneca and GlaxoSmithKline; and grant support from Boehringer-Ingelheim and GlaxoSmithKline. JV has received consulting fees from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Hoffman-LaRoche and Nycomed; speaking fees from AstraZeneca, Boehringer-Ingelheim and GlaxoSmithKline; and grant support from GlaxoSmithKline.
Ethics approval The study was approved by local ethics review committees and was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All patients gave written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.