Article Text

Abstract
Background: Previous studies have presented contradictory data concerning obstructive sleep apnoea syndrome (OSAS), lipid oxidation and nitric oxide (NO) bioavailability. This study was undertaken to (1) compare the concentration of 8-isoprostane and total nitrate and nitrite (NOx) in plasma of middle-aged men with OSAS and no other known co-morbidity and healthy controls of the same age, gender and body mass index; and (2) test the hypothesis that nasal continuous positive airway pressure (CPAP) therapy attenuates oxidative stress and nitrate deficiency.
Methods: A prospective, randomised, placebo controlled, double-blind, crossover study was performed in 31 consecutive middle-aged men with newly diagnosed OSAS and 15 healthy control subjects. Patients with OSAS were randomised to receive sham CPAP or effective CPAP for 12 weeks. Blood pressure, urinary catecholamine levels and plasma 8-isoprostane and NOx concentrations were obtained before and after both treatment modalities.
Results: Patients with OSAS had significantly higher 8-isoprostane levels (median (IQR) 42.5 (29.2–78.2) vs 20.0 (12.5–52.5) pg/ml, p = 0.041, Mann-Whitney test) and lower NOx levels (264 (165–650) vs 590 (251–1465) μmol/l, p = 0.022) than healthy subjects. Body mass index, blood pressure and urinary catecholamines were unchanged by CPAP therapy, but 8-isoprostane concentrations decreased (38.5 (24.2–58.7) pg/ml at baseline vs 22.5 (16.2–35.3) pg/ml on CPAP, p = 0.0001) and NOx levels increased (280 (177–707) vs 1373 (981–1517) μmol/l, p = 0.0001) after CPAP.
Conclusions: OSAS is associated with an increase in oxidative stress and a decrease in NOx that is normalised by CPAP therapy.
Statistics from Altmetric.com
Cardiovascular morbidity and mortality is increased in patients with obstructive sleep apnoea syndrome (OSAS).1–6 Oxidative and nitrosative stress are believed to contribute to this association7–9 because markers of lipid peroxidation appear to be increased in the plasma, exhaled breath condensate and urine of these patients.10–14 However, not all studies have been able to replicate these observations.15–17 Potential confounding factors explaining this discrepancy may include age differences between patients and controls, the smoking history of the patients and/or the presence of co-morbidities such as obesity, chronic obstructive pulmonary disease (COPD) or cardiovascular disease, all of which are common in OSAS and can be associated with oxidative stress by themselves.2 4 5 The effect of continuous positive airway pressure (CPAP) therapy on these biological abnormalities is also controversial. Whereas some uncontrolled studies have shown that CPAP therapy decreases oxidative stress in these patients,10 12 13 18–21 other groups have failed to demonstrate any significant change after CPAP.16 17
To address these limitations we designed a prospective, randomised, double-blind, placebo controlled, crossover study that sought to (1) compare the concentration of 8-isoprostane and total nitrate and nitrite (NOx) in plasma of middle-aged men with OSAS in whom lung and cardiovascular diseases were carefully excluded and in healthy controls of the same age, gender and body mass index (BMI); and (2) test the hypothesis that CPAP therapy improves oxidative stress and nitrate deficiency in these patients.
METHODS
Subjects
Thirty-one consecutive newly diagnosed men with OSAS and 15 healthy male volunteers were included in the study. All patients with OSAS fulfilled all the following inclusion criteria: (1) apnoea-hypopnea index (AHI) ⩾10/h; (2) excessive daytime sleepiness defined by an Epworth scale score of ⩾11 points; and (3) no treatment for OSAS. Inclusion criteria for healthy control subjects were AHI <5/h and Epworth sleepiness scale <10. Exclusion criteria for both study groups were: (1) unwillingness or inability to participate in the study; (2) obstructive or restrictive lung disease as identified by pulmonary function testing; (3) use of cardioactive drugs; (4) cardiac rhythm disturbances, including sinus bradycardia and sinus tachycardia; (5) known arterial hypertension or 24 h ambulatory blood pressure monitoring (ABPM) showing blood pressure values ⩾135/85 mm Hg; (6) left ventricular ejection fraction <50%, ischaemic or valve heart disease, hypertrophic, restrictive or infiltrative cardiomyopathy, pericardial disease or stroke by history, physical examination, ECG, chest radiography, conventional exercise stress testing and echocardiography; (7) diabetes mellitus by history or two random blood glucose levels ⩾126 mg/dl; (8) morbid obesity (BMI >40 kg/m2); and/or (9) daytime hypoxaemia (Pao2 <70 mm Hg) or hypercapnia (Paco2 >45 mm Hg). Other exclusion criteria during the study period were: (1) need to change medication; (2) hospital admission for 10 or more days; and (3) average nightly CPAP usage less than 3.5 h. Control subjects were recruited from a list of healthy subjects from our sanitary area who had had a routine health test in the previous 3 months. We randomly selected a control subject similar in gender, age (±2 years), weight (±2 kg) and height (±5 cm) with regard to the two preceding patients included in the study.
Study design
A single-centre, prospective, randomised, double-blind, placebo controlled, crossover clinical study was performed in which patients received CPAP and sham therapy22 for two 12-week periods. In healthy controls measurements were obtained once. At recruitment, ABPM, echocardiography, catecholamine concentration in urine and a sleep study were undertaken in all participants. After fasting overnight, a venous blood sample (anticoagulated with dipotassium EDTA for determination of 8-isoprostane and total nitrate and nitrite (NOx) concentrations) was collected from all participants between 08.00 and 10.00 h. Within 30 min of blood collection, plasma was obtained by centrifugation at 3000 rpm for 15 min. All plasma samples were stored at −60°C until analysis.
Patients with OSAS underwent a full-night CPAP titration study at home using an automated pressure setting device (Auto Set; ResMed, Sydney, Australia).23 Patients were given detailed instructions on the appropriate use of the CPAP equipment and were randomised to receive either effective or sham CPAP therapy for 12 weeks. The sham CPAP device was a modified conventional CPAP device in which the exhalation port diameter had been enlarged to nearly cancel nasal pressure and an orifice resistor was connected between the tubing and the CPAP unit that loads the blower with the same airflow resistance as in effective CPAP.22 No information about the type of therapy they were receiving was given. Compliance with therapy was obtained from a built-in run time counter. After 12 weeks the CPAP device was switched to the alternate mode of therapy and ABPM and plasma and urine sampling were repeated (fig 1).

Flow chart of study subjects. CPAP, continuous positive airway pressure; OSAS, obstructive sleep apnoea syndrome.
Measurements
A validated portable recording device (Sibel Home-300; Sibel SA, Barcelona, Spain)24 that records oronasal airflow using a thermistor and nasal cannula prongs, chest wall impedance, oxygen saturation, snoring and body position was used to perform a sleep study in patients and healthy controls. Respiratory events were classified as either obstructive or central on the basis of the presence or absence of respiratory effort. Respiratory events were scored as apnoeas when there was a cessation of oronasal airflow lasting ⩾10 s. Hypopnoea was defined as a decrease of 50% in oronasal airflow lasting >10 s associated with a fall in arterial oxygen saturation (Sao2) >4% of the preceding baseline level. Mean night time Sao2, minimum Sao2 (lowest values recorded during sleep), desaturation index and percentage of time with Sao2 <90% on nocturnal oximetry were computed as indices of nocturnal oxygen saturation.
Twenty-four hour ABPM data were obtained using an oscillometric method (Spacelabs device, Model 90207; Redmond, Washington, USA).25 Blood pressure was measured every 30 min during the day (08.00 to 23.00 h) and every 60 min during the night (23.00 to 08.00 h) on a workday. An appropriate cuff was placed on the non-dominant arm. Patients were instructed to carry out their ordinary daily activities, to go to bed no later than 23.00 h and not to move their arm during recordings.
Echocardiography was performed in the supine and left lateral positions after a minimum rest period of 30 min using a high quality echocardiograph with 2.0–4.0 MHz probes (Hewlett Packard Sonos 5500; Andover, Massachusetts, USA). Echocardiographic images were obtained in the parasternal long and short axes, apical two-chamber and four-chamber and subcostal views using two-dimensional, M-mode and Doppler echocardiographic techniques. The parameters were measured from at least three cardiac cycles. All echocardiograms were performed by the same experienced echocardiographer who was unaware of the subject group or the treatment assignment at each visit. Systolic function was assessed by left ventricular shortening fraction (LVSF) and left ventricular ejection fraction (LVEF);26 LVSF ⩾28% and LVEF ⩾50% were considered normal.
Forced spirometry was performed as previously described using a MasterScope system (Jaeger, Würtzburg, Germany).25
At each visit, subjects were requested to collect separate urine samples from 08.00 h until going to bed (day) and all urine during the night and the first sample after getting up in the morning (night). The urinary excretion of norepinephrine and epinephrine was determined as previously described.27
A specific enzyme immunoassay kit (Cayman Chemical, Ann Arbor, Michigan, USA) was used to measure 8-isoprostane concentrations in plasma. The intra-assay and inter-assay variability were 5% and 7%, respectively, and the detection limit of the assay was 5 pg/ml.
Total nitrate and nitrite (NOx) were measured in plasma by capillary electrophoresis using a Beckman capillary electrophoresis system (P/ACE MDQ). Absorbance was read at 200 nm and nitrate concentration was determined using a NaNO3 standard. The lower detection limit was 10 μmol/l and the intra-assay and inter-assay variability were 5% and 8%, respectively.
Statistical analysis
Values are expressed as mean (SD) or median (interquartile range, IQR) depending on their distribution. All statistical tests were two-sided. Comparisons between groups were performed using the Student t test or the Mann-Whitney U test. Categorical variables were compared using the χ2 test. Bivariate relationships between variables were determined by Pearson’s or Spearman’s correlation. To investigate the effect of CPAP therapy over time in patients with OSAS, repeated measures ANOVA was used with treatment (effective CPAP vs sham CPAP) as a within-subject factor and order of therapy as a between-subject factor. Whenever ANOVA results indicated the existence of significant differences between treatment conditions, post hoc multiple comparisons were performed with the Bonferroni test. A p value of <0.05 was considered statistically significant. All analyses were performed using the SPSS Version 11.0 software (SPSS, Chicago, Illinois, USA).
RESULTS
Characteristics of subjects
Seven subjects refused to take part in the study and three were deemed ineligible for inclusion after initial assessments (one had diabetes mellitus and two because they had unknown mitral stenosis), so 31 patients with OSAS were randomised for inclusion in the study (fig 1).
Table 1 shows the main demographic and functional characteristics of all participants at baseline. Demographic data, smoking habits, spirometric results and ABPM results did not differ between patients with OSAS and healthy controls. As expected, sleep parameters were abnormal (and consistent with the diagnosis of OSAS) in patients but were normal in healthy subjects. Patients with OSAS had higher nocturnal levels of norepinephrine and epinephrine than control subjects but LVSF and LVEF were similar in both groups.
Plasma concentrations of 8-isoprostane and total nitrate and nitrite (NOx)
At recruitment, before treatment with CPAP, patients with OSAS had higher median (IQR) plasma levels of 8-isoprostane (42.5 (29.2–78.2) vs 20.0 (12.5–52.5) pg/ml, p = 0.041) and lower plasma levels of NOx (264 (165–650) vs 590 (251–1465) μmol/l, p = 0.022) than healthy subjects. There were no correlations between plasma levels of 8-isoprostane or NOx and sleep parameters.
Effects of CPAP
Six patients failed to complete the trial, leaving 25 patients for the final analysis. Two were excluded because, on average, they used CPAP at night for <3.5 h, while the remaining four patients were lost to follow-up (fig 1). The baseline anthropometric characteristics, smoking habit, lung function data, sleep study indices, sympathetic tone, ABPM or left ventricular systolic function of these six patients were not significantly different from those who completed the trial. The mean (SD) CPAP pressure value was 10 (2) cm H2O and average nightly use of CPAP and sham CPAP was 6.2 (1.1) h and 6.3 (1.6) h, respectively.
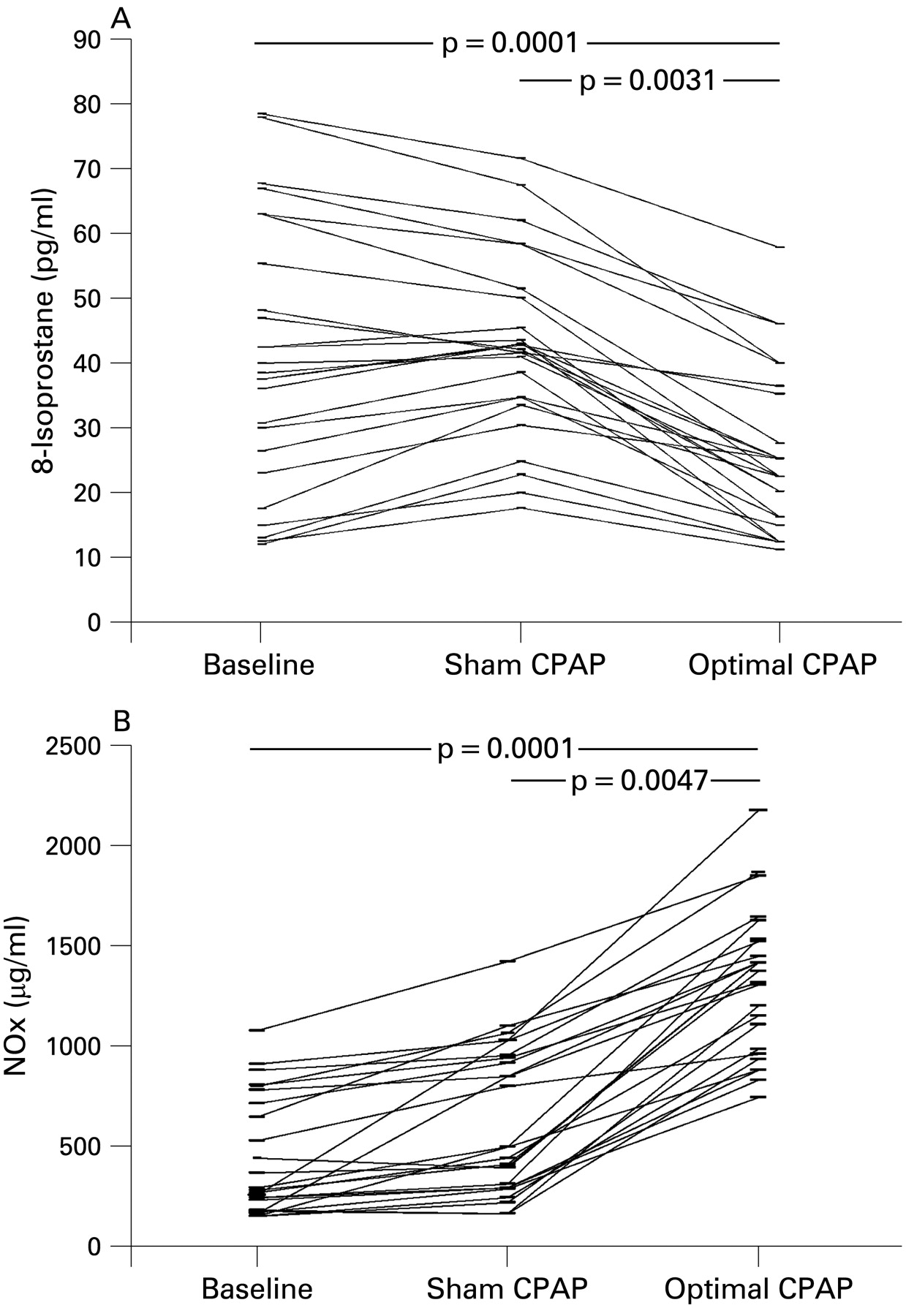
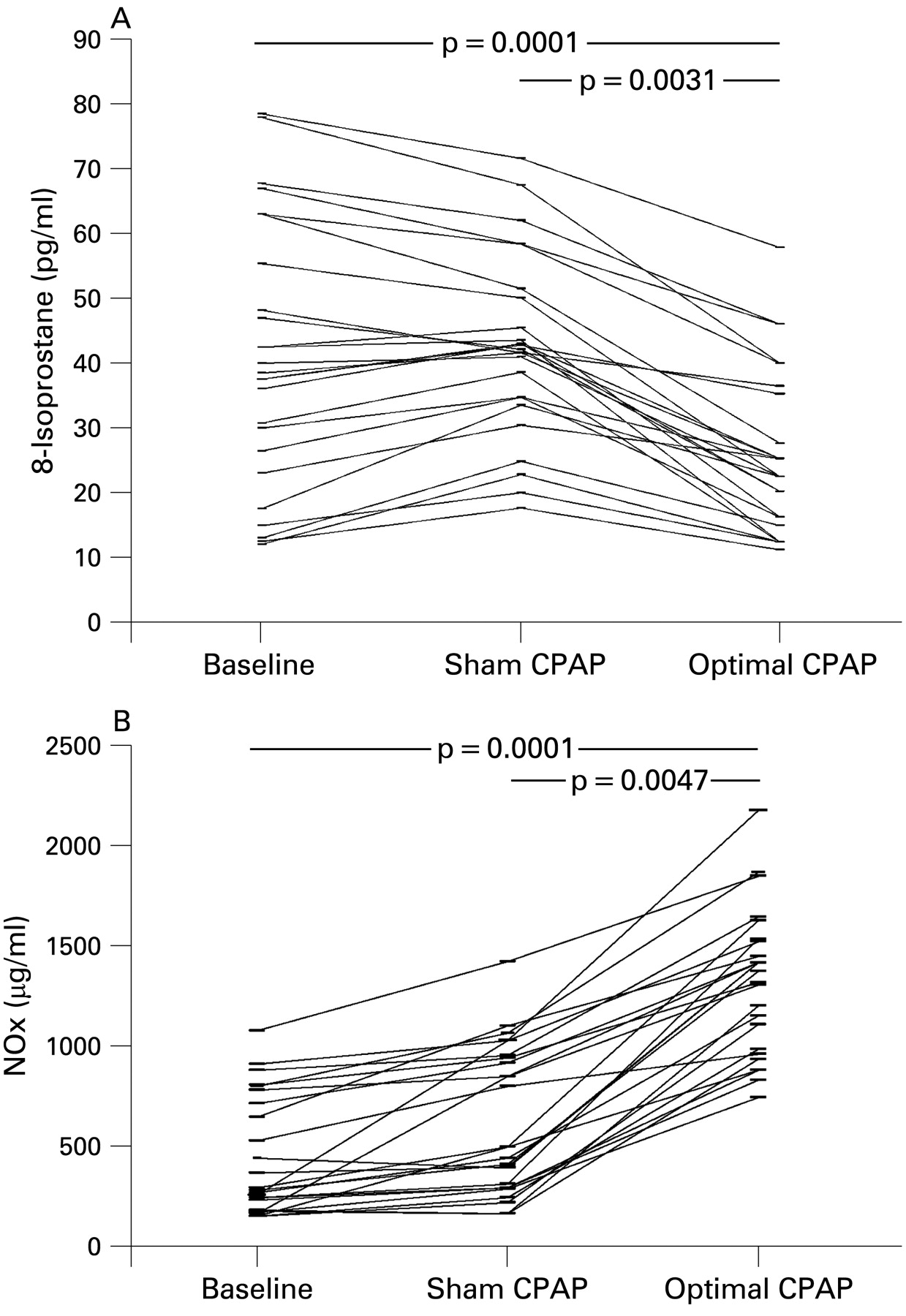
BMI, ABPM and urinary catecholamines were not modified by CPAP (table 2). However, effective CPAP (but not sham CPAP) significantly decreased the plasma concentration of 8-isoprostane (from 38.5 (24.2–58.7) pg/ml to 22.5 (16.2–35.3) pg/ml, p = 0.0001) and increased the plasma concentration of NOx (from 280 (177–707) μmol/l to 1373 (981–1517) μmol/l, p = 0.0001, fig 2). The decrease in 8-isoprostane concentration was similar in the OSAS subgroup treated with optimal CPAP and sham CPAP to that in the OSAS group treated with sham CPAP and optimal CPAP (18.3 (1.1–25.0) pg/ml vs 21.6 (4.0–25.6) pg/ml, p = 0.276). The increase in NOx concentration was also not affected by the treatment order (827 (563–974) μmol/l vs 961 (630–1309) μmol/l, p = 0.921). Values after CPAP therapy were not significantly different from those found in healthy subjects.
{kind=link}
{kind=link}
Individual plasma concentrations of (A) 8-isoprostane and (B) nitrate and nitrite (NOx) at baseline, after sham continuous positive airway pressure (CPAP) and optimal CPAP in patients with obstructive sleep apnoea syndrome.
DISCUSSION
Our study provides two main findings of interest. First, the plasma concentration of 8-isoprostane is higher and that of NOx is lower in patients with OSAS carefully selected to exclude pulmonary and cardiovascular disease than in healthy subjects matched for gender, age and BMI. Second, these abnormalities are normalised after 12 weeks of CPAP therapy. Despite the fact that some previous studies have provided similar results, to the best of our knowledge ours is the first prospective randomised placebo controlled crossover study to evaluate oxidative stress and NO bioavailability in patients with OSAS and the effects of CPAP therapy on these parameters. Our results therefore provide a definite answer to some still unanswered questions in this field.
Oxidative stress
Many previous studies have identified an association between OSAS and cardiovascular disease.1 3 Oxidative stress is often proposed as a likely pathogenic mechanism.28 29 However, earlier studies of lipid peroxidation in OSAS provided conflicting results. Some of them could not find differences in the susceptibility to lipid peroxidation in these patients.15–17 This is best exemplified by the study of Svatikova et al16 who reported that the concentration of thiobarbituric acid-reactive substances, oxidised LDL autoantibodies and free isoprostane levels in 41 patients with severe OSAS without cardiovascular co-morbidity were similar to those of 35 healthy controls matched for BMI and age. However, they did not measure lung or left ventricular function, and controls were recruited from those who attended their sleep unit and had an AHI <5/h even though they had a relatively high sleep fragmentation index (22 (4)/h). Moreover, they employed a split-night protocol which is, in our opinion, unsuitable to investigate biomarker changes in these patients.16 On the other hand, several other studies reported abnormal lipid peroxidation in OSAS.10–14 For instance, Carpagnano et al11 found higher levels of 8-isprostane in plasma and exhaled breath condensate in patients with OSAS than in controls, and Minoguchi et al demonstrated that the urinary levels of 8-isprostane in OSAS were related to the AHI.14 Isoprostanes are a complex family of compounds produced from arachidonic acid via a free radical catalysed mechanism.30 They are often used as clinical markers of lipid peroxidation in human diseases because of their stability and specificity.29 We found that patients with OSAS in whom pulmonary and cardiac co-morbidities were carefully excluded had higher 8-isoprostane plasma levels than healthy controls, and that CPAP therapy (but not treatment with sham CPAP) normalised these values. The results of studies investigating the effects of CPAP therapy on oxidative stress in OSAS have also yielded conflicting results. On the one hand, several uncontrolled studies showed that short-term,11 medium-term12 14 21 and long-term10 13 20 CPAP reduces oxidative stress in patients with OSAS. In addition, Barceló et al18 found that treatment with CPAP for 1 year increased the plasma antioxidant status. In contrast, other groups failed to demonstrate that CPAP had any effect on oxidative stress and antioxidant capacity.16 17 The differences between the studies may be due to the effects of several potential confounders and the fact that none of them was controlled by sham CPAP. In our study we sought to avoid these limitations by selecting participants (both patients with OSAS and controls) very carefully so that all of them were free of any other co-morbid disease and none was receiving medication either before or during the study period. Furthermore, we recruited into the study healthy subjects in whom subclinical pulmonary or cardiac disease was carefully excluded and, most importantly, we designed a placebo controlled crossover study which is the most powerful design for testing the efficacy of any therapeutic intervention. Under these circumstances, our results clearly show that effective CPAP therapy improves oxidative stress in patients with OSAS (table 2, fig 2). Taking into account all the above-mentioned arguments, we postulate that our results clearly show that OSAS produces oxidative stress and that this is treatable with CPAP.
Nitrate and nitrite (NOx) deficiency
Impaired nitric oxide (NO) release from endothelial cells is also regarded as an initiator and promoter of cardiovascular disease in patients with OSAS. Nitrate and nitrite (NOx) are stable derivatives of NO and their levels reflect overall NO production.31 Previous studies have shown that NO production is lower in patients with OSAS than in controls.7–9 32 In keeping with these results, we also found that NOx levels were lower in OSAS than in an age- and BMI-matched control group. The mechanisms explaining this observation are unclear. Hypoxaemia is a likely candidate since it is known to suppress the expression of endothelial NO synthase,33 and previous studies have shown that NOx is inversely related to nocturnal desaturation8 9 and oxygen administration increases serum NOx in OSAS.9 On the other hand, previous studies have shown that effective CPAP therapy increases NO levels in OSAS.7 32 Furthermore, Lavie et al32 reported a significant decrease in circulating NO levels after CPAP withdrawal for just one night. Our study confirms these previous results using a highly robust design (randomised, placebo controlled, crossover trial). Thus, our results showed that treatment with CPAP for 3 months led to a significant improvement in NO metabolites compared with placebo.
Strengths and potential limitations
As discussed above, the main strengths of the study are the experimental design (randomised, placebo controlled, crossover trial) and the careful selection of patients and controls (in whom co-morbidities were carefully excluded). Yet, as in any study, there are some potential limitations that deserve comment. First, the sample size was relatively small. This was due to the difficulty of including only middle-aged patients with newly diagnosed OSAS who had no other diseases and were taking no cardiovascular medication. Second, because our study included only men, our results may not be directly applicable to women.
CONCLUSIONS
The results of this study show that OSAS causes oxidative stress and reduces NOx bioavailability, and that CPAP therapy normalises these biological abnormalities.
REFERENCES
Footnotes
Funding: This research was partially supported by a grant from the Fondo de Investigación Sanitaria (FIS; exp 01/0278).
Competing interests: None.
Ethics approval: The study was approved by the Institutional Ethics Committee at the hospital and all subjects gave their written informed consent.