Article Text

Abstract
Background: Wheezing occurs in both atopic and non-atopic children. The characteristics of atopic and non-atopic wheeze in children at 10 years of age were assessed and attempts made to identify whether different mechanisms underlie these states.
Methods: Children were seen at birth and at 1, 2, 4 and 10 years of age in a whole population birth cohort study (n = 1456; 1373 seen at 10 years). Information was collected prospectively on inherited and early life environmental risk factors for wheezing. Skin prick testing, spirometry, and methacholine bronchial challenge were conducted at 10 years. Wheezing at 10 years of age was considered atopic or non-atopic depending on the results of the skin prick test. Independent significant risk factors for atopic and non-atopic wheeze were determined by logistic regression.
Results: Atopic (10.9%) and non-atopic (9.7%) wheeze were equally common at 10 years of age. Greater bronchial hyperresponsiveness (p<0.001) and airways obstruction (p = 0.011) occurred in children with atopic wheeze than in those with non-atopic wheeze at 10 years. Children with atopic wheeze more often received treatment (p<0.001) or an asthma diagnosis for their disorder, although current morbidity at 10 years differed little for these states. Maternal asthma and recurrent chest infections at 2 years were independently significant factors for developing non-atopic wheeze. For atopic wheeze, sibling asthma, eczema at 1 year, rhinitis at 4 years, and male sex were independently significant.
Conclusions: Non-atopic wheeze is as common as atopic wheeze in children aged 10 years, but treatment is more frequent in those with atopic wheeze. Different risk factor profiles appear relevant to the presence of atopic and non-atopic wheeze at 10 years of age.
- asthma
- atopy
- wheeze
- children
- risk factors
Statistics from Altmetric.com
Much attention has focused on the strong association between atopic tendency and childhood wheezing. Causal roles for atopic sensitisation1,2 in the pathogenesis of wheezing and asthma have been postulated as a result of numerous studies showing a higher frequency of asthmatic symptoms in atopic children than in non-atopic children.3–,6 Consequently, interventional strategies to prevent atopic sensitisation by allergen avoidance in early life have been applied in an attempt to modify the development of childhood allergy, wheeze, and asthma.7–,9 However, these measures have met with mixed results and have not shown definitive lasting benefit.2,7–,9 Given such evidence, Pearce et al10 recently questioned the role of atopy as a causative factor in asthma. Indeed, as amply shown by Martinez et al,11 there is growing evidence for the existence of several distinct wheezing phenotypes in childhood, not all of which are closely linked to atopy. Some forms of non-atopic wheeze such as early life transient wheeze have been well characterised,11 with associations with impaired lung function in infancy and maternal smoking. The nature of non-atopic wheeze in later childhood, however, remains unclear. In particular, the significance of such disease in terms of associated morbidity and the similarities or differences of its characteristics with atopic wheezing need confirmation. An understanding of whether different risk factors underlie atopic and non-atopic wheeze in later childhood could also provide fresh insight into the mechanisms underlying childhood wheezing and asthma. Here we describe findings that characterise non-atopic wheeze at 10 years of age and assess whether this differs in risk factor profile from atopic disease. The results were derived from our unselected whole population birth cohort which has been prospectively followed for the first decade of life.
METHODS
A whole population birth cohort was established on the Isle of Wight in 1989 to study prospectively the natural history of childhood wheezing and to identify risk factors relevant to the development of childhood wheezing states. Approval for the study was obtained from the local research ethics committee.
Of 1536 children born between 1 January 1989 and 28 February 1990, informed consent was obtained for 1456 subjects to be enrolled. Enrolment took place at birth and information on family history of allergy (parental or sibling), household pets, parental smoking, social class (Registrar General’s classification), and birth weight were recorded. Children were followed at the ages of 1 (n = 1167; 80.2%), 2 (n = 1174; 80.6%), 4 (n = 1218; 83.7%) and 10 years (n = 1373; 94.3%). The results of cohort follow up at 1, 2, 4, and 10 years of age have been reported previously.12–,15 At each follow up detailed questionnaires were completed with the parents for each child regarding the prevalence of asthma and allergy. “Current wheeze” was recorded as having occurred on at least one occasion in the previous 12 months. Exposure to relevant environmental factors (domestic pets and tobacco smoke) was noted. The method of feeding was recorded at 1 and 2 years. A history of recurrent chest infections (more than one in the past year) was assessed at 1 and 2 years of age. Investigators’ diagnoses of eczema (chronic or chronically relapsing, itchy dermatitis lasting more than 6 weeks with characteristic morphology and distribution), recurrent nasal symptoms/rhinitis (recurrent nasal discharge or blockage with attacks of sneezing and itchy eyes), and food allergy (history of vomiting, diarrhoea, colic or rash within 4 hours of ingestion of a particular food on at least two occasions) were made each time. Further additional information was collected at 10 years about disease morbidity. Consultations with a hospital asthma specialist (“specialist referral”) were therefore recorded along with hospital admissions for wheezing episodes. Details of asthma treatment “ever used” such as bronchodilators, inhaled corticosteroids, other prophylactic medications (long acting β2 agonists, sodium cromoglycate, theophyllines, leukotriene antagonists or antihistamines), and oral corticosteroid therapy were also obtained. Several measures of “current wheezing morbidity” (within the preceding 12 months) were recorded at 10 years. These included “wheeze frequency” (number of wheezing episodes), “sleep disturbance from wheezing” (occurring more or less than once per week), “exercise induced wheezing”, “limitation of speech by wheezing” (severe enough to limit speech to one or two words between breaths), and “nocturnal cough” (dry cough at night not associated with cold or flu). At 10 years the parents were also asked to report suspected triggers (ever) for their child’s wheezing episodes.
At 10 years of age the questionnaire information was updated in 1373 children.15 Of these, 1043 individuals attended for further tests including skin prick testing (n = 1036), serum IgE measurement (n = 953), baseline spirometry (n = 981), and methacholine bronchial challenge (n = 784).
Skin prick testing was performed to a panel of common inhaled and food allergens (ALK, Denmark) which comprised house dust mite (Dermatophagoides pteronyssinus), grass pollen mix, tree pollen mix, cat and dog epithelia, Alternaria alternata, Cladosporium herbarum, milk, hen’s egg, soya, cod and peanut plus histamine and physiological saline which acted as positive and negative controls, respectively. An allergen skin test reaction with a mean wheal diameter of at least 3 mm more than the negative control was regarded as positive and the subject defined as atopic. Serum was analysed for total IgE and a qualitative inhalant screen (Phadiatop; Pharmacia Diagnostics, Uppsala, Sweden). The inhalant screen tested for common inhalant allergens: house dust mite (D pteronyssinus and D farinae), cat dander, dog dander, horse dander, timothy grass, Cladosporium, silver birch, olive, mugwort, and nettle. All children with past or current wheezing were invited to perform a methacholine bronchial challenge at 10 years to assess bronchial hyperresponsiveness (BHR) using a Koko dosimeter (Pds Instrumentation, Louisville, USA) with compressed air source at 8 l/min and nebuliser output of 0.8 l/min. Initial inhalation of 0.9% saline was followed 1 minute later by spirometric recordings to obtain a baseline value. Incremental concentrations from 0.0625 mg/ml to 16 mg/ml methacholine were then serially administered. The concentration causing a stable fall in forced expiratory volume in 1 second (FEV1) from the post-saline value of 20% was interpolated and expressed as PC20 FEV1. The intention was to perform bronchial challenge whenever possible in all children with wheezing histories plus a control group (n = 300) of children who had never wheezed.
Analysis of data
Data were double entered onto SPSS version 10.0 (SPSS Inc, Chicago, USA). Children were categorised at 10 years of age into the following four groups by the presence of “current wheeze” and atopic status at the 10 year skin prick test: (1) non-atopic non-wheeze; (2) non-atopic wheeze; (3) atopic non-wheeze; and (4) atopic wheeze.
Comparison of continuous variables for atopic and non-atopic wheeze was made (with transformation where necessary) using independent samples t testing. A continuous measure of BHR was estimated as the least square dose-response slope using least square regression of percentage change in FEV1 on methacholine concentration administered for each child. Inverse transformation of the resulting dose-response slope (inverse slope) was used to satisfy normality and homoscedasticity with low values of 1/(10 − slope) extrapolating to high BHR. Interval data were analysed using non-parametric tests (Mann-Whitney U test).
Separate univariate risk factor analysis was conducted to identify risk factors present in early life (the first 4 years) that were associated with either atopic or non-atopic wheeze at 10 years of age. χ2 analysis (with Fisher’s exact test where indicated by low expected cell counts) was used for this purpose, comparing factors between the respective wheezing state and that of a non-atopic non-wheezer (common control). To obtain the independent effect of risk factors showing trends for significance at univariate testing (p<0.2), separate logistic regression models were created for atopic and non-atopic wheeze at 10 years. Stepwise backward (likelihood ratio) logistic regression was used for this purpose. Where more than one risk factor could explain a particular exposure of interest, only the most relevant was entered into the model.
RESULTS
At 10 years of age skin prick testing was performed in 1036 subjects (75.5% of 1373). Subjects attending for skin prick testing were more likely to have a personal or family history of allergy than those providing only questionnaire data at 10 years (table 1⇓). The prevalence of atopy—as defined by at least one skin test allergen positive response—was 26.9% (279/1036). Among the atopic children 159 (57.0%) were male. In the 1036 subjects who underwent skin prick tests, current wheeze was present at 10 years in 20.7% (n = 214), atopic wheeze in 10.9% (n = 113), and non-atopic wheeze in 9.7% (n = 101). Among non-wheezers at 10 years, 79.8% (n = 656) were non-atopic and 20.2% (n = 166) were atopic.
Characteristics of children at 10 years of age
The median age of onset did not differ between children with atopic and non-atopic wheeze at 10 years (median 2.0 years v 2.0 years; p = 0.954, Mann-Whitney U test). Immunological and lung function characteristics of children with atopic and non-atopic wheeze at 10 years are shown in table 2⇓. Total IgE was significantly higher in the atopic children. Positive IgE inhalant screen was also significantly greater for children with atopic wheeze than for those with non-atopic wheeze (100% v 8.6%; p<0.001). Children with atopic wheeze did not show significantly more impairment of baseline spirometric parameters (FEV1, FVC, or PEF) but they did have significantly more evidence of airways obstruction (FEV1/FVC), lower inverse slope measure of BHR, and a higher prevalence of greater BHR (PC20 FEV1<4.0 mg/ml) than those with non-atopic wheeze (64.5% v 23.1%; p<0.001, OR 6.07 (95% CI 3.25 to 11.34)). These findings did not vary with sex stratification (results not shown).
Mean (SE) characteristics of children with atopic and non-atopic wheeze at 10 years of age
Measures of current morbidity at 10 years of age were largely similar for children with atopic and non-atopic wheeze except for sleep disturbance from wheeze (table 3⇓). Similarly, measures that could be regarded as indices of severity—such as hospitalisation for wheezing illness or specialist referral—did not differ significantly between atopic and non-atopic wheeze. Children with atopic wheeze were more likely to have been diagnosed as asthmatic by a physician, treated with regular medications for wheezing, and to have received oral corticosteroids. However, when stratified into social classes, children in higher social classes at 10 years (I–IIInm) who had atopic wheeze were no more likely than those with non-atopic wheeze to be diagnosed as asthmatic (31.3% v 45.2%; p = 0.172; OR 0.55; (95% CI 0.23 to 1.30)) or to have used inhaled corticosteroids (52.1% v 48.8%; p = 0.756; OR 1.14 (95% CI 0.50 to 2.63)). Other patterns of morbidity did not differ by social class and there was also little variation in morbidity/disease severity with sex stratified analysis (results not shown). Boys with atopic wheeze had a higher wheeze frequency than those with non-atopic wheeze (50.7% v 29.2%; p = 0.020; OR 2.50 (95% CI 1.15 to 5.46)) but they had less exercise induced wheeze than non-atopic children (27.8% v 49.0%; OR 0.40 (95% CI 0.19 to 0.85)). Other patterns of morbidity in boys and girls were similar to the overall trends shown in table 3⇓.
Morbidity and treatment of children with atopic and non-atopic wheeze at 10 years of age
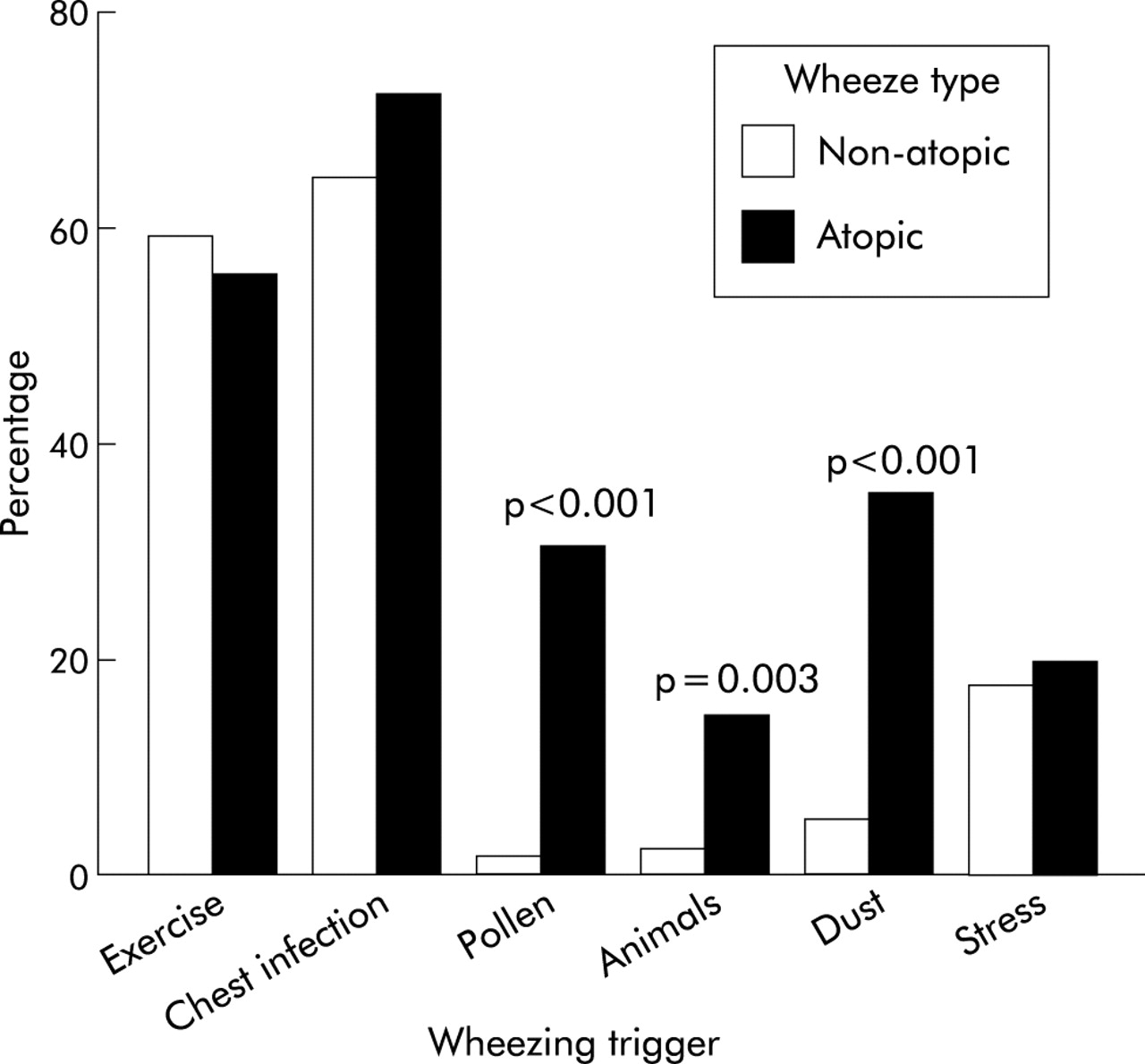
Figure 1⇓ shows parental reporting of suspected triggers (ever) for their child’s wheezing. Infections, exercise, and stress did not differ significantly in frequency between children with atopic wheeze and those with non-atopic wheeze.
{kind=link}
Wheezing triggers ever reported; p values denote comparison between children with non-atopic and atopic wheeze (χ2 test). Only significant p values are given.
Univariate analysis showed a significant association between non-atopic wheeze and parental (particularly maternal) allergic history, sibling asthma, personal allergy in the first year of life (eczema and food allergy) plus rhinitis at 2 years (table 4⇓). Similarly, significant effects were observed for parental smoking throughout early life and recurrent chest infections in infancy. Exclusive formula feeding in the first 3 months of life also conferred a significant increased risk of having non-atopic wheeze, while exclusive breastfeeding in the first 3 months of life provided a significant reduction in risk.
Univariate analysis of early life risk factors for non-atopic wheeze in children at 10 years of age (p<0.05)
Univariate analysis examining risk factors for atopic wheeze at 10 years showed significant associations with parental and sibling allergic histories (especially asthma and rhinitis), personal histories of eczema and food allergy throughout early life plus rhinitis and urticaria at 4 years (table 5⇓). There was also a positive association with male sex. Early life environmental factors showed minimal effect on the development of atopic wheeze. Only recurrent chest infections at 2 years showed univariate significance, with social class at birth, method of infant feeding, pet exposure and parental smoking not having a statistically significant influence on the presence of atopic wheeze at 10 years of age.
Univariate analysis of early life risk factors for atopic wheeze at 10 years of age (p<0.05)
Many of the factors showing significant effects by univariate analysis for these wheezing states at 10 years may have been linked. To determine independently significant variables associated with atopic and non-atopic wheeze, multivariate logistic regression analysis was used (table 6⇓). For non-atopic wheeze at 10 years only maternal asthma and recurrent chest infections at 2 years were found to be independently significant factors while, for atopic wheeze, independent significance was found for male sex, diagnosed eczema at 1 year, diagnosed rhinitis at 4 years, and sibling asthma.
Multivariate analysis of early life risk factors for atopic and non-atopic wheeze at 10 years (p<0.2)
DISCUSSION
This study shows that non-atopic wheezing is as frequent as atopic wheezing in an unselected cohort of 10 year old British children. Current morbidity for atopic and non-atopic wheezing at 10 years of age was also not dissimilar. However, BHR, all levels of treatment, and being diagnosed as asthmatic were significantly more frequent in children with atopic wheeze. Characterisation of early life risk factor profiles for these two states revealed different patterns. Male sex, heredity, and allergic traits were independently significant for atopic wheezing while the environmental factors examined had little effect of their own on this state. Heredity in the form of maternal asthma also had a significant effect on the presence of non-atopic wheeze. In contrast to atopic wheeze, recurrent chest infections at 2 years of age were found to have a significant independent association with non-atopic wheeze.
A higher prevalence of wheeze and asthma in atopic children has previously been shown.3–,6 It has recently been reported that 32% of subjects with wheeze aged 11 years and over are non-atopic as defined by serum IgE criteria.16 Defining atopy by skin test positivity, we found that half the children with wheeze at 10 years of age did not have an atopic tendency. In support of this definition of atopy, we found good concordance between atopy by skin prick testing and a positive IgE inhalant screen. However, it is possible that our definition of wheeze—at least one episode of wheezing in the last year regardless of duration—could have led to a high estimation of non-atopic wheeze. Some might consider that our figures for non-atopic wheeze include “insignificant” single episodes of viral induced wheeze which conventionally may not be considered to have the same importance as that associated with persistent atopic wheeze. However, it is worth reflecting that both atopic and non-atopic wheeze in our 10 year old children had their origins in infancy and were therefore “persistent” states. It is also noteworthy that chest infections were not reported more frequently as wheezing triggers by parents of the non-atopic children in our study. This is different from previous findings from Tucson which suggest that non-atopic childhood asthma is largely associated with early life chest infections and remits after the age of 6 years.17 This discrepancy could plausibly reflect the different environment encountered by our population.
Is the disease state in our unexpectedly large group of children with non-atopic wheeze as significant as in those with atopic wheeze? Clough et al18 showed that atopic children aged 7–8 years with cough and wheeze had lower FEV1, greater BHR, and greater peak flow variability as well as increased symptom severity than non-atopic children. Ponsonby et al19 also found greater wheeze frequency and hospital attendance in 8–10 year old children with atopic wheeze than in those with non-atopic wheeze. In some respects our findings support suggestions of worse disease among those with atopic wheeze. Our study confirms greater BHR and obstructive patterns of airflow limitation among children with atopic wheeze. Disease severity as indicated by physician diagnosed asthma ever and receiving all levels of treatment for wheezing disorders might also appear to be greater for those with atopic wheeze in our study. However, we found that diagnosed asthma and inhaled steroid usage was no different between children with atopic and non-atopic wheeze in the highest three social classes. Furthermore, among the boys, current morbidity measures such as exercise induced wheeze were greater in non-atopic children. Overall, we found that most measures of current morbidity as well as hospitalisation and specialist referral for wheezing illness did not vary significantly by atopic status. There is therefore a discrepancy between morbidity and levels of treatment in our children with atopic and non-atopic wheeze. One explanation may be that children with atopic wheeze do indeed have more severe disease but that successful treatment prevents significantly more morbidity than in those with non-atopic wheeze. An alternative view might be that atopic wheeze is more recognisable (owing to family and personal history of allergy) and therefore is more readily treated, while non-atopic wheeze is not necessarily always milder but is being relatively overlooked and undertreated. In this context, a recent report from Australia suggests that the non-atopic status may be associated with underdiagnosis of adult asthma.20
Combinations of genetic and environmental influences are believed to underlie the development of wheezing and asthma. Court et al16 recently proposed that IgE and non-IgE mediated asthma might have distinctive aetiological mechanisms. We have confirmed different risk factor profiles for atopic and non-atopic wheeze in our children. Univariate analysis showed that parental smoking at all stages within early life, exclusive formula feeding in the first 3 months, and recurrent chest infections in infancy were significant factors for non-atopic but not for atopic wheeze. No effect of animal exposure or social class was observed for either state. Many significant factors may have been interlinked, and multivariate analysis found only recurrent chest infections at 2 years to have persisting independent significance for non-atopic wheeze. Whether this reflects a causal role for respiratory pathogens in non-atopic wheeze or merely increased susceptibility to infection because of intrinsic airway disease remains uncertain. Oddy et al21 identified wheezing lower respiratory illnesses as a significant risk factor for current asthma at 6 years of age in both atopic and non-atopic children. However, we did not find an independent association between such infections and development of atopic wheeze. This is consistent with findings reported by Von Mutius et al22 who found a higher risk of childhood asthma from repeated early childhood infections for non-atopic asthma. It also supports work from Tucson23 showing no significant association between early life lower respiratory tract illness and allergic sensitisation at the ages of 6 or 11 years.
Work by Lowe et al24 has suggested that there is a significant interaction between maternal asthma, the child’s atopic status, and lung function in 3 year olds. Our findings illustrate an important role for asthmatic family history in the manifestation of wheeze, regardless of whether or not the subject is atopic. Thus, even in the absence of personal atopy, we have found that maternal asthma is independently associated with wheezing at 10 years of age. This agrees with the findings from Tucson associating maternal asthma with asthma in Alternaria negative (the predominant local aeroallergen) children.17 The mechanism behind such relationships remains obscure but, as Halonen et al suggest, it may involve in utero factors.17
Analysis by Pearce et al10 has shown that the population attributable risk for asthma in relation to atopy in a variety of studies is typically less than 50%. Our findings confirm that a substantial burden of non-atopic wheezing exists at 10 years of age and further question a predominant role for atopy in childhood wheezing. Whether a model of wheezing and asthma as a primary epithelial disorder that facilitates airway allergen sensitisation is a better explanation of the associations between atopy and wheeze is worth considering.25 The high prevalence of non-atopic wheeze in our population and the risk factor profile associated with it might provide some clues as to the rising prevalence of wheeze and asthma in recent years. Whether the increasing prevalence of non-atopic wheeze is one explanation for this phenomenon needs to be considered. Certainly, our findings indicate that non-atopic wheeze should not be ignored as a disease entity in later childhood.
Acknowledgments
The authors acknowledge the cooperation of the children and parents who have participated in this ongoing study. The 10 year follow up was funded with the assistance of the National Asthma Campaign, UK (grant no 364). The authors also note the valued contributions of Linda Terry, Gail Poulton, Linda Waterhouse, Heidi Savory, Tessa Booth, Andrew Gallini, Cathy Wilby, Rosemary Lisseter and Roger Twiselton to the 10 year follow up of this study, and highlight the role of the late Dr David Hide in starting the study.