Article Text

Abstract
Background: The magnitude and time course of effect of an acute exacerbation of chronic bronchitis (AECB) on health status are not known. Data from the GLOBE study, a randomised double blind trial of antibiotic therapy, were used to investigate these effects.
Methods: 438 patients with AECB received either gemifloxacin 320 mg once daily for 5 days (214 patients) or clarithromycin 500 mg twice daily for 7 days (224 patients) and were followed up for 26 weeks. St George’s Respiratory Questionnaire (SGRQ) scores were obtained at baseline and after 4, 12, and 26 weeks.
Results: At presentation during an exacerbation SGRQ scores were worse (Total score difference 5.4 units, 95% CI 1.9 to 8.8, p=0.002) in patients who had a subsequent exacerbation during follow up. The greatest improvement in SGRQ score occurred within the first 4 weeks (mean 8.9 units, 95% CI 6.5 to 11.5, p<0.0001). Subsequently, scores improved more rapidly in patients with no further exacerbations. At 26 weeks the difference between the two groups was 9.6 units (95% CI 5.7 to 13.4, p<0.0001). In patients with no further exacerbations the SGRQ score improved between 4 and 12 weeks by a further 4.1 units (95% CI 2.2 to 5.9, p<0.0001).
Conclusions: A single infective AECB has a sustained effect on health status. The recovery period is long even in patients who have no further exacerbations. A second episode within 6 months limits recovery markedly. Treatments that reduce exacerbation frequency could have a significant impact on health status.
- quality of life
- antibiotics
- chronic bronchitis
- exacerbations
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is one of the five leading causes of death worldwide and chronic bronchitis has been estimated to affect up to 13 million individuals (approximately 4–6% of adults in the USA1) and is associated with considerable morbidity and mortality. Patients with chronic bronchitis are susceptible to frequent exacerbations, characterised by increased dyspnoea, cough, sputum production and purulence2 which are frequently caused by bacterial pathogens.3 Chronic bronchitis is characterised by persistent daily sputum production, but many patients also have chronic airflow limitation making it difficult to distinguish the condition from COPD. Frequent exacerbations of COPD are associated with worse health status4; patients who had more than two exacerbations per year had significantly worse health than those with 0–2 exacerbations per year. Poor health status is also related to an increased likelihood of future admissions to hospital,5 and we have presented a preliminary analysis which shows that frequent exacerbations are associated with a faster rate of decline in health status.6
The rate of recovery of respiratory symptoms following an acute exacerbation has been described,7 but little is known of the recovery in health status. Our analysis was designed to characterise and measure its time course. We used data from a recent study of gemifloxacin versus clarithromycin in the treatment of acute infective exacerbations of chronic bronchitis. Gemifloxacin was as effective as the comparator, resulted in significantly fewer recurrences over 26 weeks, and was more cost effective. The data have been reported in detail elsewhere.8,9 Health status was measured using the St George’s Respiratory Questionnaire (SGRQ).10 The SGRQ has previously shown greater sensitivity to change following antibiotic treatment for an acute exacerbation than lung function parameters,11 and greater internal consistency compared with other outcome measures applied in a clinical trial of fluoroquinolone therapy.12 For the analysis presented in this paper our objectives were twofold: (1) to characterise the time course of recovery of health status over a 6 month period following initial presentation with an exacerbation, and (2) to test the hypothesis that further exacerbations will alter this time course.
METHODS
Study population
A total of 438 patients (214 receiving gemifloxacin) were recruited. All had a history of chronic bronchitis (MRC criteria) and presented with an Anthonisen type 1 acute exacerbation of chronic bronchitis (AECB) characterised by purulent sputum, increased cough, and dyspnoea.2 Exclusion criteria were pregnancy, hypersensitivity to quinolone or macrolide antibacterials, those with a history of fluoroquinolone related tendonitis, patients with a complicating infection or disease, renal impairment, epilepsy, cystic fibrosis, TB, bronchiectasis or pneumonia, life threatening underlying disease, oral corticosteroids in excess of prednisolone 10 mg/day, and receipt of any other antibacterial within 7 days of entry. All patients gave informed consent to participate in the study. Full details of the acute phase of the study are reported elsewhere.8
Health status measurement
The SGRQ is a 50 item questionnaire with 76 weighted responses. It provides a Total score and three component scores: Symptoms (distress caused by respiratory symptoms), Activity (physical activities that cause or are limited by breathlessness), and Impacts (social and psychological effects of the disease). The SGRQ is scored from 0 to 100 where 0 indicates best and 100 indicates worst health. A change in the Total score of four units is consistent with a clinically significant change in the patient.10,13 An increase in score indicates worsening health. The SGRQ has been shown to be a valid and responsive measure of health impairment in chronic airflow limitation10,14 and bronchiectasis.11
Protocol
The study was a randomised, double blind, multicentre trial. In the acute phase of the study patients received either gemifloxacin 320 mg once daily for 5 days (n=214) or clarithromycin 500 mg twice daily for 7 days (n=224). During long term follow up patients were treated as deemed clinically appropriate by their physicians and followed for a maximum of 26 weeks. Economic outcomes were assessed during this period for the Gemifloxacin Long term Outcomes in Bronchitis Exacerbations (GLOBE) study. These are reported in detail elsewhere.9 Health status was assessed using the SGRQ at presentation and then after 4, 12, and 26 weeks. At presentation demographic data, peak expiratory flow (PEF), and signs and symptoms associated with the current AECB were recorded. Patients were free to withdraw from the study at any time. The need for further antibacterial treatment for another AECB after the end of the initial treatment was recorded. Health status was not included in the study as an efficacy outcome because the size and pattern of changes with treatment were unknown. The SGRQ was included in this study solely to permit the analysis now being presented.
Statistical analysis
Patients who had a further exacerbation after the initial episode were defined as “exacerbators” and those who did not have a recurrence were defined as “non-exacerbators”. A recurrent exacerbation was defined as a period of increased respiratory symptoms that, in the view of the patient’s physician, required further antibiotic treatment.
Differences between patient groups at presentation were examined using t tests. Improvement in health status was expected to be non-linear so an area under the curve (AUC) was used as the best estimate of the mean change in scores. The AUC was calculated using the trapezium rule (t2 – t1)(y1 + y2)/2 and then divided by the total number of days in study to obtain the average SGRQ score for each individual.15 An AUC was calculated for patients with at least the first two observations (at presentation and at 4 weeks) and only for patients with serial observations. Analysis of covariance (ANCOVA) was used to compare differences in health status scores between exacerbators and non-exacerbators, controlling for differences in the health status score at presentation. The following covariates were also included in the analyses: race (white, black, Asian, other), sex, country (USA, Canada), smoking status (ever smoked, never smoked), and age. Model residuals were examined for goodness of fit and found to conform with assumptions of normality. These tests were performed using SAS PROC GLM procedures and were two sided with a 5% level of significance unless stated otherwise. Results are given as mean with standard deviation or 95% confidence intervals.
RESULTS
Study enrolment and randomisation
At study enrolment—that is, at presentation with an acute Anthonisen type 1 exacerbation—the mean PEF was 58% predicted. Over half of the patients had wheeze and more than 75% had cough and dyspnoea of MRC grade 3 or worse. At presentation the SGRQ scores were high, at levels seen in patients with stable moderate to severe COPD.16 One hundred and thirty four patients had a further exacerbation after the initial episode. Of these, 92 had one further exacerbation, 21 had two, 14 had three, and seven had four recurrent exacerbations. Demographic data and patient characteristics at presentation, split into those who subsequently had further exacerbations and those who remained free from exacerbations, are shown in table 1. For all measures except the health status scores there were no significant differences at presentation between the two groups of patients. All of the SGRQ scores apart from the Symptoms score were higher (that is, worse) in patients who had a subsequent exacerbation during the 6 month follow up period. The difference of 5.4 units (95% CI 1.9 to 8.8) in SGRQ Total score between these two groups of patients was clinically and statistically significant (p=0.002).
Patient characteristics at presentation with an acute exacerbation of chronic bronchitis (Anthonisen type 1)
Pattern of recovery
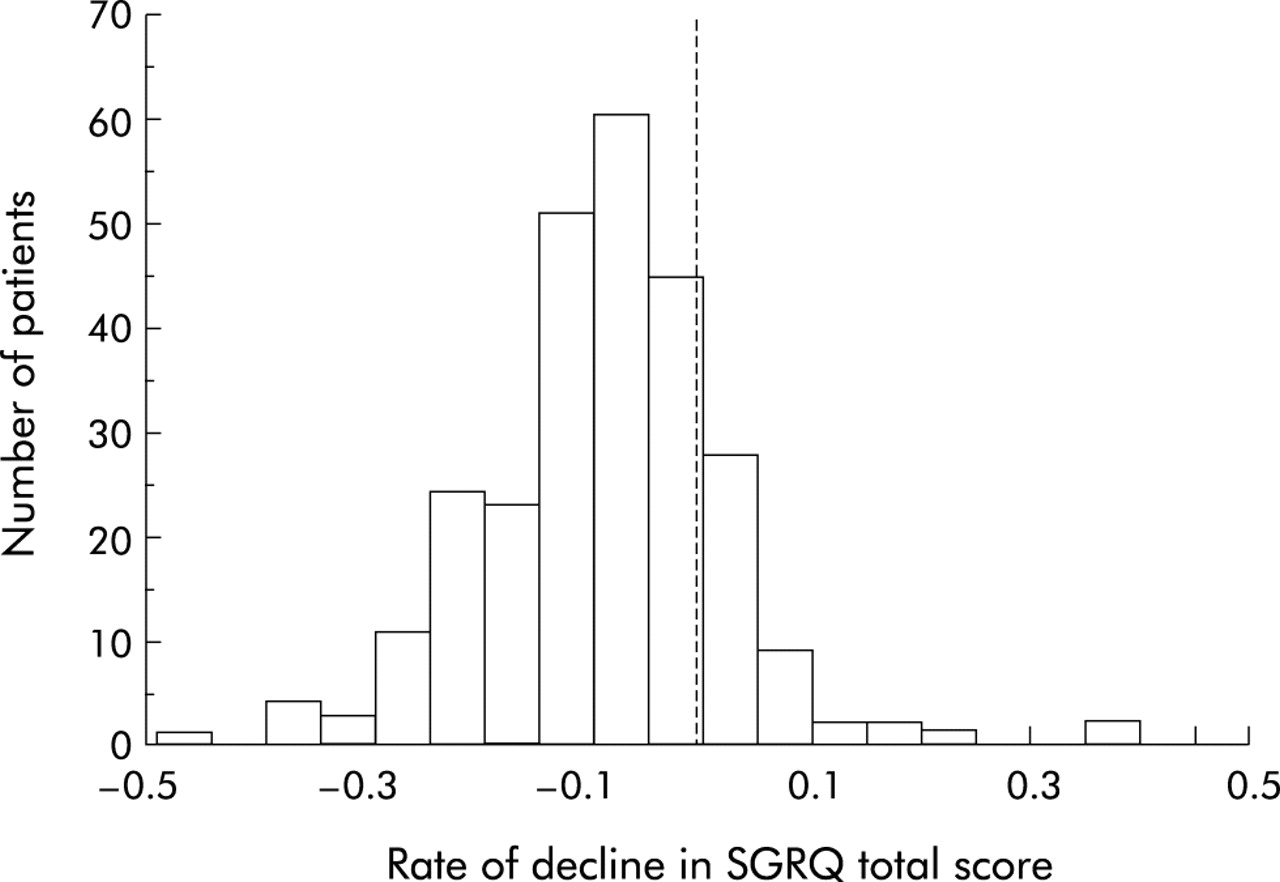
In both exacerbators and non-exacerbators the greatest improvement in SGRQ score (that is, the biggest fall) occurred within 4 weeks of initial presentation (fig 1). In the non-exacerbators the improvement was 11.8 (16) units and in the exacerbators it was 8.9 (14.6) units; the difference was not significant. In patients who had no further exacerbations the improvement in score over the first 4 weeks was greater than over the subsequent 5 months. For example, the Total score fell by 5.2 (14.3) units over this period. Most of this was due to a 4.1 unit improvement between weeks 4 and 12 (95% CI 2.2 to 5.9, p<0.0001). The pattern of recovery in patients who had no further exacerbations was non-linear (fig 1). There could be two explanations for this: either all the patients had this pattern, or the mean curves shown in fig 1 resulted from a combination of two subpopulations characterised by either a fast or a slow recovery speed. To investigate this possibility we plotted the frequency distribution of the rate of recovery of Total SGRQ scores calculated using linear regression (fig 2). This shows an almost normal distribution, with no evidence of subpopulations that recovered more or less slowly.
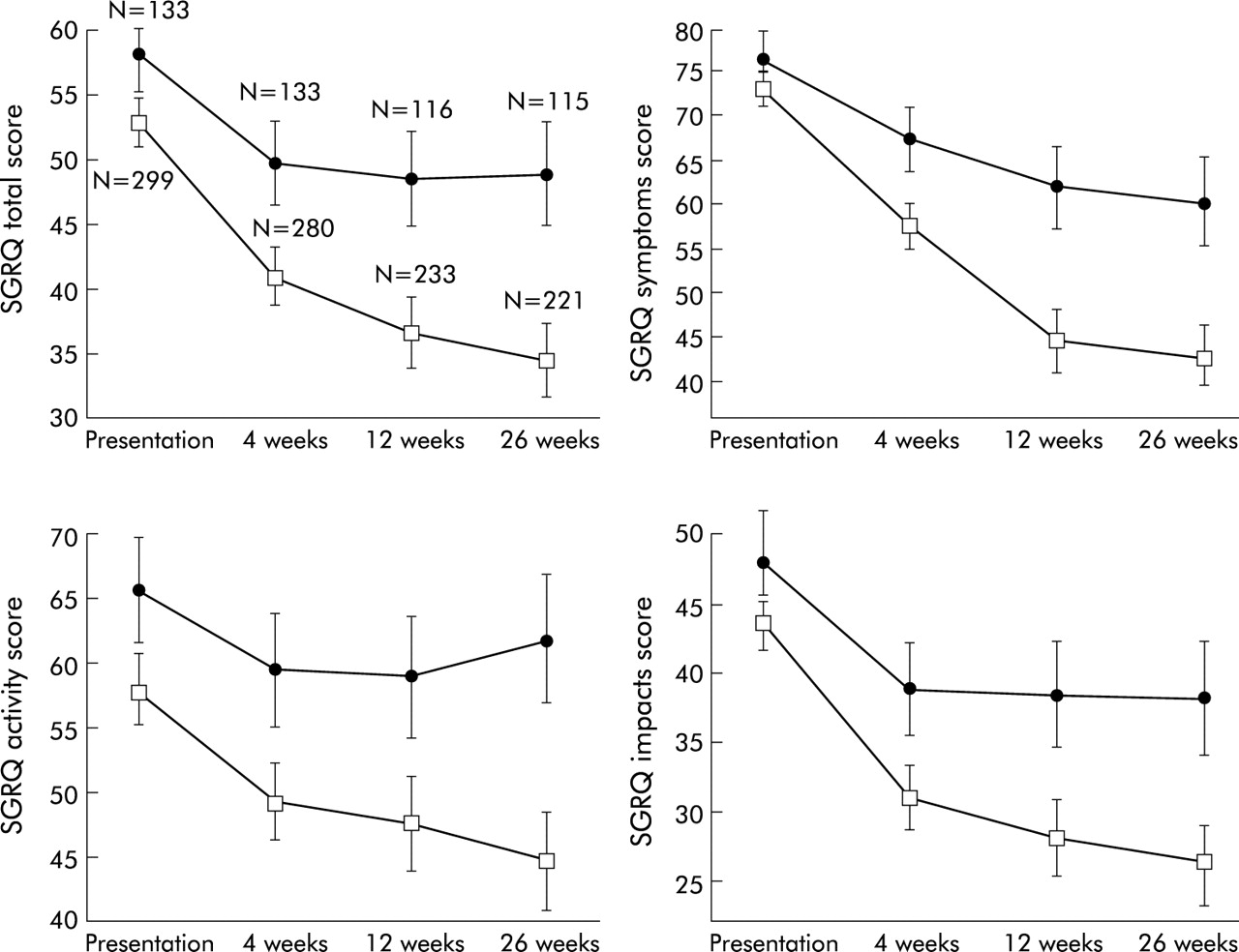
SGRQ study scores by exacerbation status (bars indicate 95% confidence intervals) in patients with no exacerbation (□) and patients with a further exacerbation during the follow up period (•). The numbers represent patients remaining in the study at that time point.

Frequency distribution for the decline in SGRQ score (that is, rate of recovery) calculated using a linear regression of change in SGRQ Total score from presentation to 26 weeks in patients who remained exacerbation free over this time.
There was little improvement in patients who had further exacerbations. Since the SGRQ scores were different between exacerbation groups at presentation, for subsequent analysis the scores were adjusted for their presentation level using ANCOVA. The magnitude of differences in scores between the groups increased over time (table 2). The difference in Total scores was greater than the 4 unit threshold for clinical significance after 4 weeks and even larger by 26 weeks.
Mean (SD) SGRQ scores for exacerbators and non-exacerbators adjusted for scores at randomisation
Area under the curve (AUC) analysis
Since the recovery of health status during the study period was non-linear, AUC estimates were used to summarise health status scores during the recovery period. These were calculated if at least two consecutive observations were available. All scores were significantly higher during the study in patients who had a recurrence compared with those who did not (table 3). To test the relationship between the severity of airflow limitation during the initial exacerbation and the subsequent recovery of health status, we examined the correlation between PEF at presentation and the AUC estimates of health status. Correlations were weak but significant (Total, r=–0.25, p<0.0001; Symptoms, r=–0.11, p=0.03; Activity, r=–0.32, p<0.0001; Impacts, r=–0.21, p<0.0001), showing that worse PEF was associated with worse health status throughout the study. Multivariate analysis showed that this relationship did not differ between exacerbators and non-exacerbators (p>0.05).
Area under the curve (AUC) estimates for exacerbators and non-exacerbators controlling for race, sex, country, smoking status, and age
Effect of re-exacerbation on changes in health status
To examine the relationship between re-exacerbation and health status more closely, we compared the change in SGRQ Total score between each successive measurement in patients who had a documented exacerbation during that period and those who did not (fig 3). Over the first 4 weeks the rate of recovery in SGRQ score was lower in patients who had an exacerbation requiring treatment during that period than in those who did not. Between weeks 4 and 12 there was a further improvement in the patients who remained exacerbation-free compared with those who had a recurrence. Between 12 and 26 weeks there was no significant change in either group.

{kind=link}
{kind=link}
{kind=link}
Change (and 95% confidence interval) in SGRQ Total score by exacerbation status at different times during the follow up period. The numbers apply to the number of patients for whom data were available during that period. Open bars=no exacerbation during that period; closed bars=patients who had an exacerbation during that period.
Effect of smoking
Multivariate analysis showed that smokers had worse SGRQ scores throughout the study than ex-smokers (p<0.0001). An interaction analysis was used to test the relationship between exacerbation status and smoking status. Statistical significance for this exploratory analysis was set, a priori, at p<0.01. Although there was a trend toward a greater improvement in scores in non-smoking patients who did not have recurrent exacerbations, this was not statistically significant. For example, the p value for a test of an interaction between exacerbation status, health status, and smoking was 0.2.
Effect of antibiotic choice
The study was not designed or powered to test for an effect of antibiotic on health status as a trial outcome, but to aid the design of any future studies we have carried out an exploratory post hoc analysis. There was no statistically significant (p<0.05) difference between the health status scores at any stage in the study. At the end of the study the Total SGRQ score in the gemifloxacin group was lower than in the clarithromycin treated patients (difference = –3.3 units, p=0.09). We also carried out an analysis of the effect of antibiotic on outcome in patients who had no further exacerbations; 121 patients receiving gemifloxacin and 102 receiving clarithromycin completed the study and had no further exacerbations. SGRQ scores at first presentation were not significantly different between the two groups (p<0.7). Thereafter, the scores, adjusted for their level at presentation, showed a progressive widening of the difference between the two treatment groups so that, at 26 weeks, the Total SGRQ score was 4.6 units (95% CI 9.1 to 0.1) lower in the gemifloxacin treated patients.
DISCUSSION
We have shown that the time course of recovery from an acute infective exacerbation of chronic bronchitis in patients with airflow limitation is very prolonged. It appears to be in two phases—a fast improvement over the first 4 weeks followed by a slower phase that continues for several months. The size of the overall improvement is large, but only if the patient remains free from any further exacerbation. During the second and third months following the initial event the improvement in SGRQ is still above the threshold considered to be clinically significant.13 However, if a further exacerbation occurs at any time in the following 6 months, the degree of recovery is small. The difference in scores between those patients who had further exacerbations and those who did not was both clinically and statistically significant after 4 weeks. This difference continued to widen, so that by 6 months it was more than twice that required for a clinically significant difference.
The SGRQ score at presentation during the initial exacerbation was significantly worse in patients who had further exacerbations than in those who remained exacerbation-free. This finding is consistent with a previous observation that SGRQ scores were higher (that is, worse) in patients who subsequently died or were admitted to hospital with an exacerbation of COPD during a 1 year follow up period.5 There are number of possible explanations for this. It is known that patients with frequent exacerbations have worse health.4 Also, patients with frequent exacerbations may have had one in the months before entry to this study, so might have been in the recovery phase following the previous episode. This may have inflated the health status effects of the episode that precipitated admission to the study. Finally, the underlying disease processes that are reflected in poor health scores may increase the likelihood of further exacerbations.
The time course of recovery appears to be very long, with a small change evident even between 12 and 26 weeks in patients who had no further exacerbations. At first sight this appears to be longer than the time course of recovery of respiratory symptoms reported by Seemungal et al,7 but their study differed from ours in many respects. They recorded respiratory symptoms (cough, dyspnoea, and symptoms of the common cold) whereas we measured health status using an instrument designed to capture a wide range of effects of the disease. They also presented their results differently, expressing them as percentages of patients with a given symptom presence rather than as a numerical estimate of symptom level. Their findings are not inconsistent with ours, however. While they measured the median time to recovery of symptoms and PEF to be 6 and 7 days respectively, inspection of their figures show that, on average, full recovery of PEF or symptoms in patients presenting with increased dyspnoea had not occurred by 5 weeks (the end of their study period). They appeared to find patients who recovered or did not (by 35 days), but we found no evidence of defined populations of patients who may be called “fast” or “slow” recoverers. The mechanism of the prolonged time course of recovery in health status is not clear. It was seen in all components of impaired health—symptoms, physical activity, social, and psychological functioning. One possibility is that the increased level of symptoms leads to reduced physical activity with resulting effects on physical fitness and muscle strength. This effect may be magnified by the presence of increased levels of circulating proinflammatory cytokines.17
The study was carried out in patients who had previous symptoms of chronic bronchitis and had airflow limitation at the time of presentation with an acute exacerbation. We were unable to make the measurements necessary to confirm airway obstruction at the end of the study, but it is likely that the majority of these patients did have COPD. The PEF at presentation was only 58% of predicted normal, and it has been shown that exacerbations have only a small effect on PEF in patients with COPD.7 It has also been shown that exacerbation frequency increases with the severity of airway obstruction.18 Finally, the SGRQ scores at the end of the study were well above the values for a normal population.19
The study has confirmed a previous observation that patients with COPD who smoke have significantly worse health than ex-smokers.20 In this study, as in the previous one, this difference was maintained over the entire follow up period, irrespective of changes in health status score over time. The mechanism responsible for this effect of smoking is not clear, but it is not related to differences in forced expiratory volume in 1 second (FEV1).20
It is clear that exacerbation frequency has a marked effect on health status and may influence the decline in FEV1,21 so effective prevention and treatment is important. The study was not powered to test for a difference in effect on health status between antibiotics but, to test the feasibility of any future studies, we carried out an exploratory post hoc analysis of SGRQ scores in the two treatment groups. These were lower (that is, better) in gemifloxacin treated patients at 6 months (p=0.09), but we cannot exclude the presence of a type 2 statistical error because the study was underpowered to detect a significant difference between treatments. We also observed that health status at the end of the study in patients who remained exacerbation-free for the whole period was better in those who received gemifloxacin than in those treated with clarithromycin (p<0.05). The results of this post hoc analysis should be interpreted with care, but they do not firmly refute the hypothesis that the choice of antimicrobial therapy in acute exacerbations of chronic bronchitis may influence subsequent health status. Appropriately designed and powered studies to test this hypothesis appear to be justified on the basis of these analyses.
In conclusion, this study has shown that a single infective exacerbation of chronic bronchitis has a large and sustained effect on health status. While the initial recovery is fast, the recovery period is long even in patients who have no further exacerbations over a 6 month period. Early re-exacerbation is more common in patients with worse health during an exacerbation and results in a marked attenuation of the degree of recovery. Treatments that reduce exacerbation frequency could have a clinically significant impact on health status.
REFERENCES
Footnotes
-
This study was funded by GlaxoSmithKline.