Article Text

Abstract
Background: Proinflammatory leukotrienes, which are not completely inhibited by inhaled corticosteroids, may contribute to asthmatic problems. A 16 week multicentre, randomised, double blind, controlled study was undertaken to study the efficacy of adding oral montelukast, a leukotriene receptor antagonist, to a constant dose of inhaled budesonide.
Methods: A total of 639 patients aged 18–70 years with forced expiratory volume in 1 second (FEV1) ≥55% predicted and a minimum predefined level of asthma symptoms during a 2 week placebo run in period were randomised to receive montelukast 10 mg (n=326) or placebo (n=313) once daily for 16 weeks. All patients received a constant dose of budesonide (400–1600 μg/day) by Turbuhaler throughout the study.
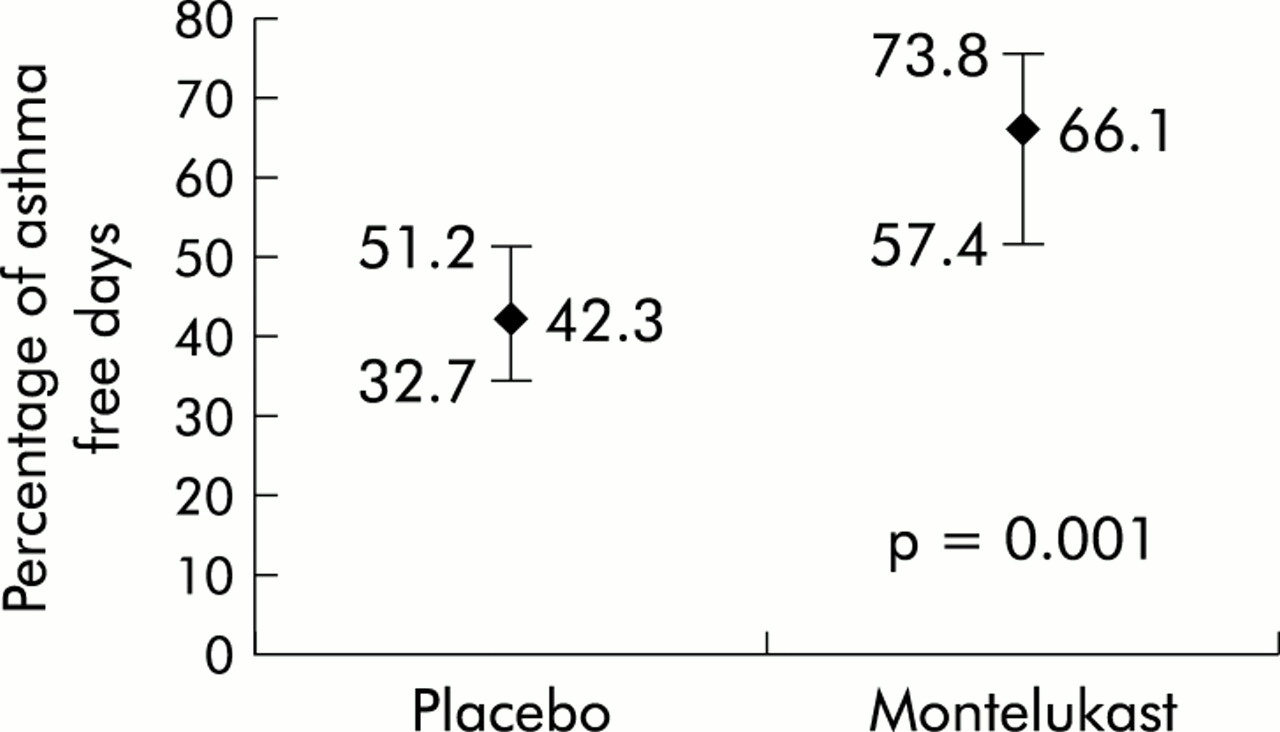
Results: Mean FEV1 at baseline was 81% predicted. The median percentage of asthma exacerbation days was 35% lower (3.1% v 4.8%; p=0.03) and the median percentage of asthma free days was 56% higher (66.1% v 42.3%; p=0.001) in the montelukast group than in the placebo group. Patients receiving concomitant treatment with montelukast had significantly (p<0.05) fewer nocturnal awakenings and significantly (p<0.05) greater improvements in β agonist use and morning peak expiratory flow rate (PEFR).
Conclusions: For patients with mild airway obstruction and persistent asthma symptoms despite budesonide treatment, concomitant treatment with montelukast significantly improves asthma control.
- asthma
- montelukast
- budesonide
- add-on therapy
- leukotriene receptor antagonists
Statistics from Altmetric.com
Inhaled corticosteroids are considered one of the first line treatments for patients with persistent asthma.1,2 These agents have proven efficacy in asthma, improving lung function and reducing asthma exacerbations, and their anti-inflammatory effects in the lungs are well established.3–5 Nonetheless, many patients receiving inhaled corticosteroids continue to experience asthma symptoms, possibly because corticosteroids do not completely inhibit the synthesis and release of cysteinyl leukotrienes in the lungs.6,7
The cysteinyl leukotrienes LTC4, LTD4, and LTE4 induce many of the pathophysiological changes present in the lungs of patients with asthma, including airflow obstruction, mucus secretion, reduced mucociliary clearance, and inflammatory cell infiltration.8,9 Antileukotriene drugs prevent provoked asthmatic responses and ameliorate asthma symptoms, improve lung function, and reduce β agonist use in patients with persistent asthma.10 Montelukast, a cysteinyl leukotriene type 1 (CysLT1) receptor antagonist, has been found to reduce airway eosinophilic inflammation in patients with chronic asthma.11
The anti-inflammatory effects of inhaled corticosteroids and montelukast may be complementary, as shown in previous studies in adults12 and children.13 These studies used lung function improvements as the predefined primary end point; there are no published studies of montelukast using reductions in asthma exacerbations as a primary end point, and this is a prominent goal of asthma treatment in national and international guidelines.1,2
The purpose of this 16 week randomised controlled study was to evaluate the efficacy of adding oral montelukast to a constant dose of inhaled budesonide for treating adult patients with mild to moderate asthma. Our hypothesis was that montelukast treatment would provide additional benefit and be safe and well tolerated for symptomatic asthmatic patients receiving inhaled budesonide, as measured by a reduction in the percentage of days of asthma exacerbations.
METHODS
Study design
This placebo controlled, randomised, parallel group study, conducted at 80 hospital centers in Spain, comprised a 2 week single blind placebo run in period and a 16 week double blind treatment period. Throughout the study all patients received a constant dosage of inhaled budesonide (Budesonide Turbuhaler, Astra, Lund, Sweden; 400–1600 μg/day administered twice daily). After the 2 week run in period, patients were randomly assigned, according to a central computer generated schedule, to receive concomitant montelukast 10 mg film coated tablets or matching placebo once daily at bedtime, irrespective of food. Treatment assignments (1:1) were stratified according to site and three budesonide dose levels (400– 800 μg/day, 801–1200 μg/day, and 1201–1600 μg/day). Participants, investigators, clinical monitors, and data coordinators were all blinded to treatment assignment. Patients used an inhaled short acting β agonist (salbutamol) as needed. The use of systemic corticosteroids, long acting antihistamines, and other antiasthmatic medications was not permitted.
Patients
Patients enrolled in the study were non-smoking male and female asthmatic outpatients aged 18–70 years who had been treated with inhaled corticosteroids at a clinically stable dose equivalent to budesonide 400–1600 μg/day for at least 8 weeks. Eligible patients had a forced expiratory volume (FEV1) of at least 55% of the predicted value and evidence of reversible airway obstruction (increase of at least 12% in FEV1 from the baseline value). During the 2 week run in period patients were required to have a minimum total daytime asthma symptom score of 64 (out of a possible maximum score in 14 days of 336) in addition to using a mean of at least 1 puff/day of β agonist. Women of childbearing age were required to have a negative pregnancy test (urine β-human chorionic gonadotropin) at screening and to use an appropriate contraceptive from 2 weeks before treatment until 14 days after the end of the study.
The study protocol was approved by each local ethical committee and all participants gave written informed consent.
Evaluations
All patients were issued a validated diary card for recording daily daytime asthma symptom scores, nocturnal awakenings, study medication use including as needed β agonist, morning and evening peak expiratory flow rate (PEFR), and the occurrence of asthma attacks. Daytime symptoms were evaluated each night before bed, and night time symptoms were evaluated in the morning on rising using validated measurement scales.14
Spirometric tests were performed at screening, at randomisation, and on completion of the study according to standardised procedures.15,16 Asthma specific quality of life was assessed before randomisation and at the end of the 16th week of treatment or on discontinuation of the study using a validated questionnaire containing 32 questions graded from 0 (worst response) to 6 (best response), evenly divided among four domains (activity, symptoms, emotions, and environment)17; the mean numerical response was calculated for each domain and for all domains. At the end of treatment patients and investigators also rated global asthma status relative to that on entering the study using a 7 point scale ranging from 0 (very much better) to 3 (unchanged) to 6 (very much worse).
Safety evaluations included adverse event reporting, physical examinations, 12 lead electrocardiograms, recording of vital signs, and clinical laboratory testing. The pregnancy test was repeated before randomisation and at the end of the study for women of childbearing age.
Statistical methods
All analyses were performed for the intention-to-treat patient population that included all randomised patients who had a baseline and at least one post-treatment assessment. The prespecified primary efficacy end point was the percentage of asthma exacerbation days, defined by Laviolette et al12 as days when any of the following occurred: awake all night (awake all night or recurrent episodes of awakening), increase from baseline in symptom score of >50%, increase from baseline in β agonist use of >70% (minimum increase 2 puffs/day), decrease from baseline of >20% in morning PEFR, morning PEFR <180 l/min, or an asthma attack (unscheduled medical care for asthma). Post hoc analyses were performed using two alternative definitions of an asthma exacerbation day, the first similar to that outlined by Wilding and coworkers18 and by Chan-Yeung and coworkers19—namely, a day when any of the following occurred: an asthma attack or, on two consecutive days, nocturnal waking, increase from baseline of more than 50% in symptoms score, use of at least 4 puffs/day of β agonist, decrease from baseline of more than 30% or more than 100 l/min in PEFR, or daily variability of more than 20% in PEFR. The second definition of an asthma exacerbation day was similar to that used by Pauwels et al for a mild exacerbation20—namely, a day when any of the following occurred: decrease from baseline of more than 20% in morning PEFR, increase from baseline in β agonist use of at least 3 puffs, or nocturnal waking because of asthma (single isolated days of exacerbations were not counted using this definition).
A secondary end point was the number of asthma free days, defined as a day when all of the following occurred: no nocturnal waking, use of two puffs or less of β agonist, no use of oral corticosteroids, and no unscheduled use of medical care for asthma. Other prespecified secondary end points were the daily use of β agonist and asthma specific quality of life. Tertiary end points were as follows: morning PEFR, daytime symptom score, discontinuations secondary to asthma, FEV1, and patient and physician global evaluations.
All patients, investigators, clinical monitors, and data coordinators were blinded throughout the study to the outcome measures of asthma exacerbation days and asthma free days. The percentages of asthma exacerbation days and asthma free days were non-normally distributed so the median and 95% confidence intervals (CI), calculated according to the method of Gardner and Altman,21 were used as the central measurement of data in both groups. The two sample median test attributed to Mood22 and the corresponding distribution-free CI for the difference between the two treatment groups were used to assess the treatment effect by non-parametric methods. The Breslow-Day test23 was used to assess the homogeneity of the treatment levels. The proportions of asthma exacerbation days and of asthma free days were calculated from the total number of follow up days in each treatment group. From these proportions the absolute risk reduction, relative risk, reduction in relative risk, and corresponding 95% CI were also calculated using the Wald method.23 The reciprocal of the absolute risk reduction—namely, the number needed to treat (NNT)—was then obtained for each end point (asthma exacerbation and asthma free days). The NNT is thus defined as the number of treatment days with montelukast needed to prevent either an asthma exacerbation day or a non-asthma free day (to gain an asthma free day).
For those efficacy end points with a baseline value, the mean changes from baseline and 95% CI during 16 weeks of treatment were computed. An analysis of variance (ANOVA) model containing terms for treatment, study centre, and dose of inhaled budesonide was used to evaluate between group differences and to construct the 95% CI for the least square (LS) means and the differences in LS means. The frequency of discontinuation secondary to asthma was compared between treatment groups using Fisher’s exact test. Patient and physician global evaluations were analysed using the ANOVA model and by reducing the 7 point scales into three categories of better (score of 0–3), unchanged (4), and worse (5–7). The proportion of patients in each category according to treatment group was summarised and tested using the Cochran-Mantel-Haenszel test, controlling for dose level where applicable.
Summary statistics were calculated for baseline characteristics of the two treatment groups, as well as for changes from baseline in laboratory values and vital signs. Adverse experiences were collected according to frequency of occurrence and the proportion of patients having any adverse experience was compared between treatment groups using Fisher’s exact test.
Prestudy power calculations yielded a sample size of 546 patients, equally divided between placebo and montelukast treatment groups, to have 90% power (at α=0.05, two sided test) to detect a 5% difference, assuming a standard deviation of 18% between treatment groups in the percentage of asthma exacerbation days.
RESULTS
Patients
Of 846 patients evaluated for inclusion in the study, 639 (76%) were randomly assigned to receive double blind treatment (fig 1). Of these 639 randomised patients, 573 (90%) completed the 16 week follow up planned for the study. Reasons for not randomising patients and for discontinuing patients before the planned 16 week follow up are shown in fig 1. Primary end point data were available for 98% of randomised patients, including 308 of 313 (98%) in the placebo group and 317 of 326 (97%) in the montelukast group.

Flow chart of study patients. Of the 207 patients who were not randomised, 63 deviated from the protocol, 38 experienced an adverse clinical event, 24 were not cooperative, five were lost to follow up, three did not have case report forms, one experienced an adverse laboratory event, and 73 were not randomised for other reasons.
Mean baseline characteristics were similar for randomised and non-randomised patients. For randomised patients, mean baseline characteristics were comparable for the two treatment groups (table 1). Approximately two thirds of patients in each treatment group received the lowest dose of budesonide (400–800 μg/day) and almost one third received the highest dose (1201–1600 μg/day). The mean baseline FEV1 was 81% predicted in both treatment groups.
Baseline characteristics of randomised patients
Efficacy
Treatment with montelukast produced a significant reduction of 35% in the percentage of asthma exacerbation days compared with placebo in patients receiving concomitant budesonide (table 2). These results were independent of the budesonide dose level (p=0.67).
Results for efficacy end points without baseline values
Our findings were consistent in post hoc analyses using the two alternative definitions, with reductions of 37% (first definition) and 32% (second definition) in the percentages of exacerbation days in the montelukast group compared with the placebo group (p=0.05 and p=0.07, respectively). Using the first definition,18,19 the median percentage of asthma exacerbation days during treatment was 13.4% (95% CI 9.9 to 18.0) in the montelukast group and 21.1% (95% CI 15.7 to 28.2) in the placebo group. With the second definition20 the median percentage of asthma exacerbation days during treatment was 8.9% (95% CI 6.3 to 12.2) in the montelukast group and 13.0% (95% CI 9.7 to 18.2) in the placebo group.
The median percentage of asthma free days was 56% higher in the montelukast group than in the placebo group (p=0.001; fig 2, table 2). These results were also independent of the budesonide dose level (p=0.70).
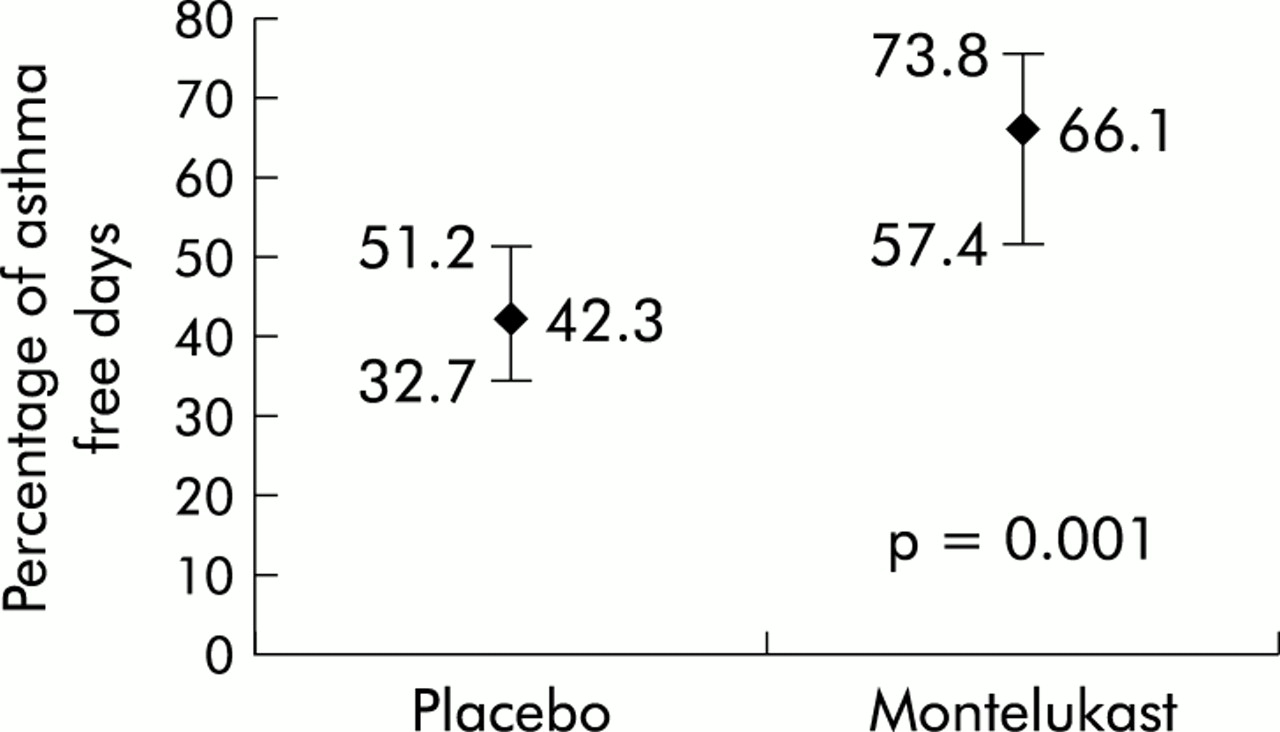
Median percentage (95% CI) of asthma free days during 16 weeks of treatment with inhaled budesonide plus concomitant once daily placebo or montelukast in patients with mild to moderate asthma. The percentage of asthma free days was significantly higher in patients receiving montelukast than in those receiving placebo (p=0.001).
The risk of an asthma exacerbation day or a “day not free of asthma” was lower in patients receiving montelukast than in those receiving placebo. Montelukast treated patients had a total of 9802 exacerbation days and 16 281 days not free of asthma out of 36 088 treatment days whereas the placebo treated patients had 11 930 exacerbation days and 18 884 days not free of asthma out of 34 318 treatment days. Patients treated with montelukast therefore had a relative risk (RR) of an asthma exacerbation day of 0.78 (95% CI 0.76 to 0.80) and an RR of a day not free of asthma of 0.82 (95% CI 0.81 to 0.83). The relative reduction in risk (RRR) of an asthma exacerbation day was 21.9% (95% CI 20.1 to 23.6) for patients receiving montelukast. Similarly, the RRR for a “day not free of asthma” was 18.0% (95% CI 16.8 to 19.2) for patients receiving montelukast. The number of days needed to treat (NNT) with montelukast to avoid one exacerbation day was 13, and the NNT to avoid one day not free of asthma—that is, to gain an asthma free day—was 10.
The results for other end points are summarised in tables 2 and 3. Patients receiving concomitant treatment with montelukast had significantly fewer nocturnal awakenings and showed significantly greater improvements in β agonist use and morning PEFR. The effect of montelukast on β agonist use was evident within the first day of treatment. The decrease from baseline in β agonist use was significantly lower in the montelukast group on the first day compared with the placebo group (p=0.04, fig 3) and remained consistent over the 16 weeks of treatment.
Change from baseline in efficacy end points

Mean percentage change from baseline in use of rescue β agonist treatment during the first 21 days of treatment with placebo or montelukast in patients receiving inhaled budesonide (mean adjusted according to treatment centre and dose level).
Improvements in daytime asthma symptom scores (fig 4), asthma specific quality of life scores, and FEV1 were numerically greater in the montelukast group but did not reach statistical significance compared with improvements in the placebo group (table 3). Only six patients (three in each group) discontinued treatment because of worsening asthma.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean change from baseline in daytime asthma symptom scores during 16 weeks of treatment with placebo or montelukast in patients receiving inhaled budesonide (mean adjusted according to treatment centre and dose level).
Results for the global evaluations were similar for the two treatment groups. Asthma status was rated as better during the study by 83–84% of patients in both groups, 12% rated it unchanged, and 4–5% rated it worse. Seventy six percent of physicians rated the patient’s asthma as better, 19% as unchanged, and 5% as worse for both treatment groups.
Safety
The overall incidence of adverse experiences was similar in the two treatment groups (table 4). Raised transaminase levels (>2 times above the upper limit of normal) occurred in a similar proportion of patients in both groups. Eight patients in the placebo group and six in the montelukast group discontinued treatment because of clinical adverse events (three in each group because of worsening asthma). No patient withdrew from the study because of laboratory adverse events.
Incidence of the most common adverse events
DISCUSSION
The addition of montelukast to budesonide Turbuhaler (400–1600 μg/day) improved asthma control for symptomatic patients with mild to moderate asthma, as measured by the significantly lower percentage of asthma exacerbation days compared with the placebo group during the 16 week study. Patients receiving concomitant montelukast experienced a decrease of 35% in asthma exacerbation days and a 56% increase in the percentage of asthma free days compared with those receiving placebo. Moreover, the need for β agonist reliever therapy, nocturnal awakenings, morning PEFR, and daytime asthma symptoms showed improvements in the montelukast treated patients. These improvements occurred despite the fact that patients had a mean baseline FEV1 of 81% predicted, indicating that patients receiving treatment with inhaled corticosteroids and with an FEV1 close to normal who remain symptomatic may need further control of asthmatic inflammation because of a lack of effect of inhaled corticosteroids on leukotrienes.6,7 Our findings suggest that the increase in asthma free days and the decrease in asthma exacerbation days with concomitant montelukast therapy can better detect improvements in control of asthmatic inflammation and thus may be a more sensitive clinical measure of inflammation control than changes in FEV1.
To understand better the clinical meaning of these results, we expressed our data in terms of the number of days needed to treat with montelukast to prevent one asthma exacerbation day or to gain one asthma free day. Our results showed that the addition of montelukast to budesonide in patients with mild to moderate asthma prevented one asthma exacerbation day and provided one asthma free day every 13 and 10 consecutive days of treatment, respectively.
This is the first published study of montelukast to use asthma exacerbation days as the primary end point. Asthma exacerbation days and asthma free days are clinically relevant end points that reflect the extent of asthma control experienced by patients on a daily basis, as well as the goals of asthma treatment according to national and international consensus guidelines.1,2 According to these guidelines, asthma treatment should aim to reduce or eliminate chronic symptoms and asthma exacerbations, minimise the need for β agonist reliever therapy, permit normal activity levels, and maintain nearly normal lung function. Our definition of an asthma free day corresponds to the guideline goals of treatment and is similar to that of the episode free day proposed by Sculpher and Buxton24—namely, a day when there is an absence of asthma attacks, need for rescue medication, sleep disturbance caused by asthma, or an adverse event. With regard to the definition of an asthma exacerbation day, several definitions have been published in the literature which differ from one another, making it difficult to compare the results from different studies using this end point. We tested our findings with post hoc analyses using two alternative definitions of asthma exacerbation days and found the effects of montelukast treatment to be consistent under the different definitions, with reductions in exacerbation days of 37% and 32%, respectively, compared with placebo.18–20
Patients received a constant dose of inhaled corticosteroids for at least 8 weeks before enrollment in the study and the same constant dose of inhaled budesonide during the 18 week study period. Patients were on different constant doses of inhaled budesonide (400–800 μg/day, 801–1200 μg/day, and 1201–1600 μg/day) and the mean baseline FEV1 was 81% predicted. The efficacy of concomitant montelukast was evident at both low and high budesonide doses, as improvements in asthma exacerbation days and asthma free days were independent of budesonide dose.
Other studies have shown the complementary activity of antileukotrienes with inhaled corticosteroids in patients with lower mean baseline FEV1 values. In one study patients receiving high doses of inhaled corticosteroids (1000–4000 μg/day beclomethasone or equivalent) with a mean baseline FEV1 of 63.5% predicted showed improved pulmonary function and asthma symptoms, as well as a lowered risk of asthma exacerbations, when a high dose of zafirlukast (80 mg/day) was added to the treatment regimen.25
Previous montelukast studies using FEV1 as a primary end point have shown that montelukast provides additional asthma control for adults receiving inhaled beclomethasone 400 μg/day12 and children receiving inhaled budesonide 400 μg/day by Turbuhaler.13 In these randomised controlled studies the mean baseline FEV1 values were 71.0% and 77.7% predicted, respectively, and asthma exacerbation days were significantly lower for montelukast treated patients (by 25% and 23%, respectively). Moreover, in both studies concomitant montelukast and inhaled corticosteroid treatment produced additive effects on peripheral blood eosinophil counts, with significantly lower counts than on corticosteroid alone, which suggests that corticosteroids and leukotriene receptor antagonists may have complementary anti-inflammatory activity. This complementary activity of montelukast may allow for the tapering of inhaled corticosteroid doses in stable patients while maintaining asthma control, as shown in a study by Löfdahl et al.26
In our study montelukast treated patients experienced symptomatic improvements, particularly in terms of decreased nocturnal waking because of asthma; 74% (three of four patients) in this group slept all night during the study. The improvements in FEV1 during the study period were minimal and were similar in the two treatment groups; however, this is not an unexpected finding because mean baseline FEV1 was close to normal (mean 81% predicted) in these patients who were receiving treatment with inhaled corticosteroids. There were no differences in the asthma specific quality of life scores between the groups, which may be explained by the large variability in data as shown in the standard deviation values.
International consensus guidelines have proposed antileukotrienes as an alternative to long acting β agonists for use as concomitant treatment with inhaled corticosteroids for patients with step 3 (moderate persistent) asthma.1 The NAEPP guidelines propose antileukotrienes as first line treatment for patients with step 2 (mild persistent) asthma.2 Antileukotrienes may have advantages over inhaled long acting β agonists as additive treatment with corticosteroids, including an established anti-inflammatory activity11 that is different from, yet complementary to, that of inhaled corticosteroids (which do not reduce leukotriene production) and which long-acting β agonists have not demonstrated in vivo.27–30 Other advantages may be the absence of tolerance to their bronchoprotective effects31–37 and the possibility that better patient compliance may be achieved with oral medications.38
There is little published information comparing antileukotrienes and long acting β agonists when concomitantly administered with inhaled corticosteroids. Two studies have shown that salmeterol was superior to montelukast when added to inhaled corticosteroids in terms of PEFR (primary end point), symptom control, and supplemental salbutamol use.39,40 Given the fact that salmeterol can be expected to have better bronchodilating properties than montelukast and because of the potential limitations of these studies,41 these results are neither surprising nor conclusive. There is a need for direct comparisons of antileukotrienes and long acting β agonists as complementary therapy with inhaled corticosteroids that focus on other sensitive clinical end points to measure asthma inflammation control such as asthma exacerbations and asthma free days.
The strengths of this study include its large size, the wide age range of enrolled patients, and the range of doses of inhaled budesonide, all features that make the results more readily applicable to daily clinical practice. A possible limitation could be that the patient eligibility criteria, as in other clinical trials, may have selected a specific group of asthma patients. However, it should be noted that the results were consistent across all different doses of inhaled budesonide, even though patients entered the study receiving the dose of inhaled corticosteroid that was considered adequate for them for at least the previous 8 weeks. Moreover, the additive effects of montelukast were clinically and statistically significant despite evidence of a large placebo effect, especially with regard to global evaluations. This placebo effect, often evident in clinical trials of asthma treatment,42,43 may result from the frequently repeated disease assessments and better adherence to treatment that occur in a clinical trial.
Montelukast was well tolerated with safety findings similar to those with placebo. The incidence of adverse events and of withdrawal because of an adverse event was similar in the two treatment groups.
In conclusion, for patients with mild airway obstruction and persistent asthma symptoms despite treatment with budesonide in doses of 400–1600 μg/day by Turbuhaler, concomitant treatment with montelukast provides significant additional benefit and is well tolerated. Improved asthma control is evident in the increased percentage of asthma free days, the decreased percentage of asthma exacerbation days, and decreased β agonist use.
APPENDIX
The Casiopea Study Group (CApacidad de SIngulair Oral en la Prevención de Exacerbaciones Asmáticas (the ability of oral Singulair to prevent exacerbations of asthma)) for this clinical trial comprised the following investigators per study site:
H Dr Peset, Valencia (R Blanquer Oliva, I Inchaurraga Alvarez, J Palop Medina); H de Sagunto, Valencia (F Ripolles Peris, E Fernández Zabrellas, E Martínez Moragón, G Ruiz Jareño); H Xeral de Galicia, La Coruña (J R Rodríguez Suarez, M R Arias Castells, M Salgueiro Rodríguez, C Zamarron Sanz); H Provincial de Santiago, La Coruña (L G Valdés Cuadrado, D Alvarez García, P Penela Penela); H General de Elche, Alicante (C Shum Funk, J A Carratala Torregrosa, J C Padilla Estrada, V Romero Sanz); H Clínico y Provincial de Barcelona (C Picado Vallés, M T Luengo Planas); H General de Guadalajara (F Carrillo Arias, I Sánchez Hernández, J L Izquierdo Alonso); H Mutua de Terrassa, Barcelona (J L Heredia Budó); H Ntra Sra de Covadonga, Asturias (A Bango Alvarez, J Palicio Sopeña, J Martinez del Río); H Gran Canaria Dr Negrin, Las Palmas (P Cabrera Navarro, M V Medina Cruz, M F García Cabrera); H Virgen del Puerto, Cáceres (J A Riesco Miranda); H Carlos Haya, Málaga (A Valencia, J M García Jiménez, F Paez Codeso); H de la Princesa, Madrid (J Ancochea Bermúdez, M J Espinosa de los Monteros Garde); H Arnau de Vilanova, Valencia (B Brotons Brotons, J A Pérez Fernández, F Sánchez-Toril López); H Germans Trias i Pujol, Barcelona (J Morera Prat, C Martínez Rivera); H Arquitecto Marcide, La Coruña (M J Mejuto Marti, R de los Reyes Cruz, J M Moreno Barragan); H San Jorge, Huesca (L Borderías Clau, J Garrapiz López, P Val Adan); H de la Serranía, Málaga (J M Ignacio García); H San Juan, Alicante (E Chiner Vives, J Marco Such); H Valle de Hebron, Barcelona (P Lloberes Canadell, D N Aristizabal Roa, M L De Souza Galvao); H La Inmaculada, Almería (J Calvo Bonachera, J F Pascual Lledo); H Universitario La Fe, Valencia (M Perpiña Tordero, L Compte Torrero, A de Diego Damia); Fundación Jiménez Díaz, Madrid (J Sastre Domínguez, M Lluch Bernal, A Novalbos Wischer); H de Basurto, Vizcaya (J A Crespo Notario, A Lahuerta Castro); H Virgen del Rocío, Sevilla (J Castillo Gómez, F Alvarez Gutierrez, G Soto Campos, J Sánchez Gómez); H Infanta Cristina, Badajoz (F Fuentes Otero, A M Castañar Jover, P Cordero Montero, P Iñigo Naranjo); H Francisco de Borja, Valencia (C Pellicer Ciscar, J Fullana Monllor, M J Cremades Romero); Consorci Sanitari de Mataro, Barcelona (S Bardaji, X Vila Giralte); H de Cruces, Vizcaya (V Sobradillo Peña, V Achotegui Iraolagoitia, E Ciruelos Ayuso, P Marin, E Zenarruzabeitia Urigoitia); H Gregorio Marañon, Madrid (A Ventura Alvarez, T Vargas Hidalgo); H Santa Creu i Sant Pau, Barcelona (J Sanchis Aldás, P Casan Clara, V Plaza Mora, F Rodríguez Jerez); H Marques de Valdecilla, Santander (R Agüero Balbín); H Puerta del Mar, Cádiz (A León Jiménez, A Arnedillo Muñoz); H Universitario Lozano Blesa, Zaragoza (F Duce Gracia, C Colas Sanz, M A Domínguez Fuentes, J Fray Lazaro, A Lezaun Alfonso); Consorsi Sanitari de Terrassa, Barcelona (J Armengol Sánchez, A Llunell Casanova); H Clínico Virgen de la Victoria, Málaga (M Rosales Jaldo, N Avisbal Portillo, V Hidalgo San Juan); H de Requena, Valencia (J J Soler Cataluña); H Cristal Piñor, Orense (J Lamela López, E Toubes Navarro, M Blanco Aparicio, J Tabara Rodríguez); H San Pedro Alcántara, Cáceres (J F Masa Jiménez, M J Martín Vicente, A Sojo González); H Universitario La Paz, Madrid (C Villasante Fernández-Montes, M S Serrano Peña, F J García Río); H Montecelo, Pontevedra (A Baloira Villar); Instituto Nacional de Silicosis, Asturias (J A Mosquera Pestaña, B Rodríguez Cocina); H San Eloy, Vizcaya (L Alberto Ruiz Iturriaga); H Juan Canalejo, La Coruña (H Verea Hernando, F Molina Nieto, I Otero González, A Veres Racamonde); H General de Albacete (J Martínez Moratalla); H Universitario de Canarias, Tenerife (I González Martín); H General Vic, Barcelona (J Serra Batlles); H 12 de Octubre, Madrid (P Martín Escribano, C Melero Moreno); H Joan March, Baleares (F Renom Sotorra, I Mir Viladrich, S Pons Vives); H General Yagüe, Burgos (J L Viejo Bañuelos, J García Muñoz, L Rodríguez Pascual); H de Mendaro, Guipuzcoa (M Azpiazu Blocona); H Militar de Burgos (I de Granda Orive, M T Peña Miguel, M C Reinares Ten, A Velayos Mayos); H Virgen de la Concha, Zamora (E Gutierrez Maire-Richard, J Muñiz Giron, T Antolín García, M Izquierdo Patron); Hospital Santa María Nai, Orense (M Tumbeiro Novoa, A Acuña Fernández, J M García Pazos); H Reina Sofía, Córdoba (A Cosano Povedano, J Cosano Povedano); H Ramón y Cajal, Madrid (A Sueiro Bendito, R Esteban Calvo, J Tamayo Sicilia); H General de Alicante (S Romero Candeira, A Candela Blanes); H Santa Marina, Vizcaya (E Ruiz de Gordejuela, L Zaldumbide Cacho); H Virgen de la Candelaria, Tenerife (J Batista Martín, I García Talavera); H Río Carrión, Palencia (M A Fernández Jorge, L Ramos Casado); H Virgen de la Luz, Cuenca (J M Peña Herrera, B Sánchez Sánchez); H Xeral-Cies, Vigo (L Piñeiro Amigo, J C Barros Tizón); H General Provincial de Pontevedra (E Temes Montes); H de Guipuzcoa (G Zubillaga Garmendia); H Axarquía, Málaga (A Domenech del Río, M Bentabol Manzanares); H General de Jerez, Cádiz (J F Carbonero de la Fuente); H Rio Hortega, Valladolid (J L Carretero Sastre, T Ruiz Albi); H Xeral-Calde de Lugo (L A Pérez del Llano); Clínica Puerta de Hierro, Madrid (J Estada Girauta, M J Ferreiro Alvarez, M T Lázaro Carrasco, A de Pablo Gafas); H de Manacor, Mallorca (R Irigaray Canals); H Ntra Sra de Valme, Sevilla (I Alfajeme Michavila, S Umbría Domínguez); H Severo Ochoa, Madrid (C Barbosa Ayucar, J de Miguel Díez); H de la Merced, Sevilla (R Vahí Maqueda, A Beiztegui Sillero); H Ciudad de Jaen (B Alcázar Lanagran); H Principe de Asturias, Madrid (F Canseco Gonzalez, E Alonso Peces); Hospital Santa Ana de Motril, Granada (F Cañizares Sevilla); H Univ Puerto Real, Cádiz (C García Vadillo); H de Mérida, Badajoz (G García de Vinuesa, J F Medina Gallardo ); H Torrecárdenas, Almería (A Maresca García-Esteller, G Villegas Sánchez); H Juan Ramón Jiménez, Huelva (J Maldonado Pérez); H Clínico San Carlos, Madrid (C Fernández).
Acknowledgments
The authors are indebted to Nieves Blanco for her excellent coordination of drug management and administrative aspects and to Dr Jonathan Leff for his continuous support and guidance. The study was supported by a grant from Merck Sharp & Dohme Spain.
REFERENCES
Supplementary materials
Effect of montelukast added to inhaled budesonide on control of mild to moderate asthma
M J Vaquerizo, P Casan, J Castillo, M Perpiña, J Sanchis, V Sobradillo, A Valencia, H Verea, J L Viejo, C Villasante, J Gonzalez-Esteban, and C Picado
Publisher's Correction
Please note that there is an error in the first sentence of the abstract. The correct sentence reads:
Background:
Proinflammatory leukotrienes, which are not completely inhibited by inhaled corticosteroids, may contribute to asthmatic problems.
The error is much regretted
Footnotes
-
↵* A complete list of members of the CASIOPEA Study Group is provided in the Appendix.
Linked Articles
- Airwaves
- Miscellaneous